")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Correlation Study of Short-Term Mental Health in Patients Discharged After Coronavirus Disease 2019 (COVID-19) Infection without Comorbidities: A Prospective Study
Authors Guo L , Lin J, Ying W, Zheng C , Tao L, Ying B, Cheng B , Jin S , Hu B
Received 30 August 2020
Accepted for publication 5 October 2020
Published 6 November 2020 Volume 2020:16 Pages 2661—2667
DOI https://doi.org/10.2147/NDT.S278245
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Lei Guo,1,* Jingjing Lin,2,* Weiyang Ying,3 Chanfan Zheng,4 Linshuang Tao,2 Binyu Ying,1 Bihuan Cheng,1 Shengwei Jin,4 Beilei Hu2
1Department of Critical Care Medicine, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou 325000, Zhejiang, People’s Republic of China; 2Department of Neurology, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou 325000, Zhejiang, People’s Republic of China; 3Department of Pain Medicine, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou 325000, Zhejiang, People’s Republic of China; 4Clinical Research Unit, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Beilei Hu
Department of Neurology, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou 325000, Zhejiang, People’s Republic of China
Email [email protected]
Shengwei Jin
Department of Anesthesia and Critical Care Medicine, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou 325000, Zhejiang, People’s Republic of China
Email [email protected]
Objective: The WHO has upgraded the status of coronavirus disease 2019 (COVID-19) from epidemic to global pandemic. The psychometric properties aspects of COVID-19 patients without comorbidities in the short term after discharge have not been reported. In this study, the Short Form 36 (SF-36) was used to evaluate the psychometric properties and to find relevant risk factors.
Methods: The study was conducted in seven hospitals from January 2020 to April 2020. The SF-36 questionnaire was administered one month after discharge. Univariate analysis and multivariate regression model were used to analyze the risk factors of psychometric properties impairment.
Results: In univariate analysis of independent risk factors, according to the comparison of whether the duration of positive nucleic acid was greater than 20 days, the positive nucleic acid duration was independently related to the decreased role-emotional value [100, IQR (66– 100) vs 100, IQR (0, 100); p = 0.0156]. In addition, multivariable linear regression model showed that male sex and positive nucleic acid duration were related to decreased role-emotional value (p = 0.03< 0.05; p = 0.01< 0.05, respectively). Mental health was associated with age (p= 0.0435). Subsequently, we divided into three subgroups: less than seven days, 7 to 14 days and more than 14 days according to the positive nucleic acid duration. The results revealed that there were significant differences in the vitality value and mental health value of patients aged 46 to 69 in the subgroup where the positive nucleic acid duration longer than 14 days (p= 0.0472; p= 0.0311< 0.05, respectively). Similarly, there are also significant differences in role-emotional value in different genders (p= 0.0316).
Conclusion: The study described the psychometric properties of COVID-19 patients without comorbidities shortly after discharge. Risk factors for psychometric properties damage included age, male sex, and nucleic acid duration.
Keywords: COVID-19, psychometric factor, SF-36
Introduction
The global epidemic of the coronavirus disease 2019 (COVID-19) was expanding rapidly, raising widespread concern in the international organization. The cases were initially reported in Wuhan, China, and quickly spread in other area of China, as well as other countries, such as Korea, Europe and so on. As of 25 August 2020, there have been 23,518,343 confirmed cases of COVID-19 globally, including 810,492 deaths, reported to WHO.1 On the aspect of epidemiology, pathogenicity and clinical features, COVID-19 is similar to severe acute respiratory syndrome coronavirus (SARS-CoV). Between November 2002 and June 2003, the severe acute respiratory syndrome (SARS) broked out in Guangdong, China.2 There were 8422 cases worldwide, including 916 deaths (case fatality rate 11%).3 However, the 1ab polyprotein and surface glycoprotein or S protein of the amino acid sequence of COVID-19 is different from the other coronaviruses.4 COVID-19’s clinical features include fever, radiology change or acute respiratory distress, decreased or normal leukocytes and lymphocytes, and not responding to 3 to 5 days of antibiotic treatment. Most cases are reported as a mild illness course.5 Most human coronaviruses are mainly transmitted through the respiratory tract or in contact with infected secretions. Viruses have also been detected in patient stool samples.6 The management of COVID-19 treatment in Zhejiang Province, China, is rigorous. Discharge requirements include: more than three days of normal body temperature, significant improvement of respiratory symptoms, and nucleic acid test results for respiratory pathogens are negative twice consecutively (sampling time at least one day apart). All patients need another 14-day isolation after discharge. Many patients presented abnormal mood and behavior while hospitalized. Therefore, we conducted a follow-up evaluation of patients with COVID-19 one month after discharge. Some studies have shown the clinical characteristics of the COVID-19, especially the impact of the patient’s age on the prognosis.7 In addition, psychological disorders during the epidemic have also attracted the attention of many scholars,8 but no one has implemented the follow-up analysis of COVID-19 patients in the short term after they are discharged from the hospital.
The clinical outcome of a disease is not only described in terms of survival and mortality. However, it can also be measured by subjective results, such as health-related quality of life (HRQOL). It is reported that survivors of other epidemic diseases such as the Middle East respiratory syndrome (MERS) and H1N1 Influenza have a short-term or long-term quality of life problems.9–11 Short-Form General Health Survey 36 (SF-36) is the most widely used tool to evaluate HRQOL, and it is often used to evaluate the health status of the population, the effect of treatment and the disease burden.12 SF-36 has been proven to have excellent psychometric characteristics, retested reliability values, and a high degree of internal consistency for people of different ages and health conditions from the United States and around the world.13 SF-36 measures the two main components of health, including Likert-type and dichotomous items, each composing of four subforms. The physical component summary (PCS) contains role-physical (RP), physical functioning (PF), general health (GH), and bodily pain (BP). The mental component summary (MCS) contains social functioning (SF), vitality (VT), mental health (MH), and role-emotional (RE).14 Some researchers employed the SF-36 scale to evaluate the quality of life of survivors in intensive care units (ICU) one year after discharge. During the follow-up period, the overall SF-36 score of patients after discharge was lower than that of normal people, and up to 31.6% of survivors developed symptoms of post-traumatic stress disorder, and up to 31.5% of survivors were diagnosed with clinical significance anxiety or depression symptoms.7 Therefore, we used the SF-36 to evaluate the psychometric properties of COVID-19 patients in short-term after discharge.
Methods
Patients
The study was conducted in seven hospitals in southern Zhejiang, China, from January 2020 to April 2020. There were 504 patients receiving COVID-19 treatment in the hospital, 380 of them completed the questionnaire. These hospitals are tertiary hospitals designated to treat COVID-19 patients. We followed up in one month after hospital discharge.
Setting and Samples
Patients diagnosed as COVID-19 positive in the aforementioned hospitals were eligible to join in this study. If the patient had epidemiological risk, typical clinical manifestations, and met one of the following two criteria, they can be diagnosed as COVID-19: 1) blood or airway samples were tested to be SARS-CoV-2 positive by real-time polymerase chain reaction (PCR). 2) Viral gene sequencing shows that blood or respiratory samples are highly homologous to known SARS-CoV-2.15 The following patients will be excluded: 1) patients younger than 18; 2) patients who were pregnant at the time of diagnosis; 3) unable to participate; 4) lost to follow-up (SF-36 questionnaire is not available); 5) the main reason for admission is not COVID-19, and there were also serious diseases including metastatic malignant tumors, weakness, and serious injuries.
Ethical Considerations
The study conducted in accordance to the Helsinki Declaration, was permitted by the Ethics Committee of the Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University (2020–002), with informed consent of participants.
Measurements
Our research applied SF-36 form, which contains 8 scales, to assessed physical and mental health. The mental health indicators were composed of social functioning (SF, 2 items), vitality (VT, 4 items), mental health (MH, 5 items), and role-emotional (RE, 3 items). The physical health indicators include four scales of role-physical (RP, 4 items), physical functioning (PF, 10 items), general health (GH, 5 items), and bodily pain (BP, 2 items). In our study, SF-36 was recalled at the standard time (4 weeks), and Likert scales or Yes/no options were used to evaluate well-being and function on this 36-item questionnaire. In order to make SF-36 scores comparable, the scale is standardized using a scoring algorithm to obtain a score. The score range is 0–100 points, the higher the score means the better your health. The Chinese version of SF-36 has been well verified among the Chinese population.16–18
We recorded demographic data such as age and gender. Then comparisons of SF-36 value by the duration of positive nucleic acid for longer than 20 days, or whether the use of corticosteroids and compared whether the patients have a drinking or smoking history.
Statistical Analysis
Demographic and baseline characteristics were summarized using descriptive statistics. In univariate analysis, continuous variables were summarized as medians and interquartile ranges, while categorical variables were expressed as the counts and percentages of patients in each category. Kruskal–Wallis rank sum test was used for group comparison among the continuous variables, and Fisher’s Exact test or the chi-squared test was used to determine the association among categorical data.19 The estimates of regression coefficients and their corresponding 95% confidence intervals were calculated by multivariable linear regression model. All statistical tests were two-sided, and a p-value of less than 0.05 was considered statistically significant. We use SPSS software for statistical analysis (version 22.0; SPSS Inc., Chicago, IL).
Results
Patient Characteristics
A total of 504 patients from 7 hospitals were included in this study, and 380 patients completed follow-up one month after discharge. In order to eliminate the psychological influence of chronic diseases, we excluded 121 patients with chronic diseases, and finally, 259 patients were included in the study. Among them, male and female patients accounted for 46.9% and 53.1%, respectively. The proportions of each age groups are 1.6% for younger than 18 years old,53.1% for the group between18–46 years old, and 43.3% for the group between 46 and 69 years old (Table 1).
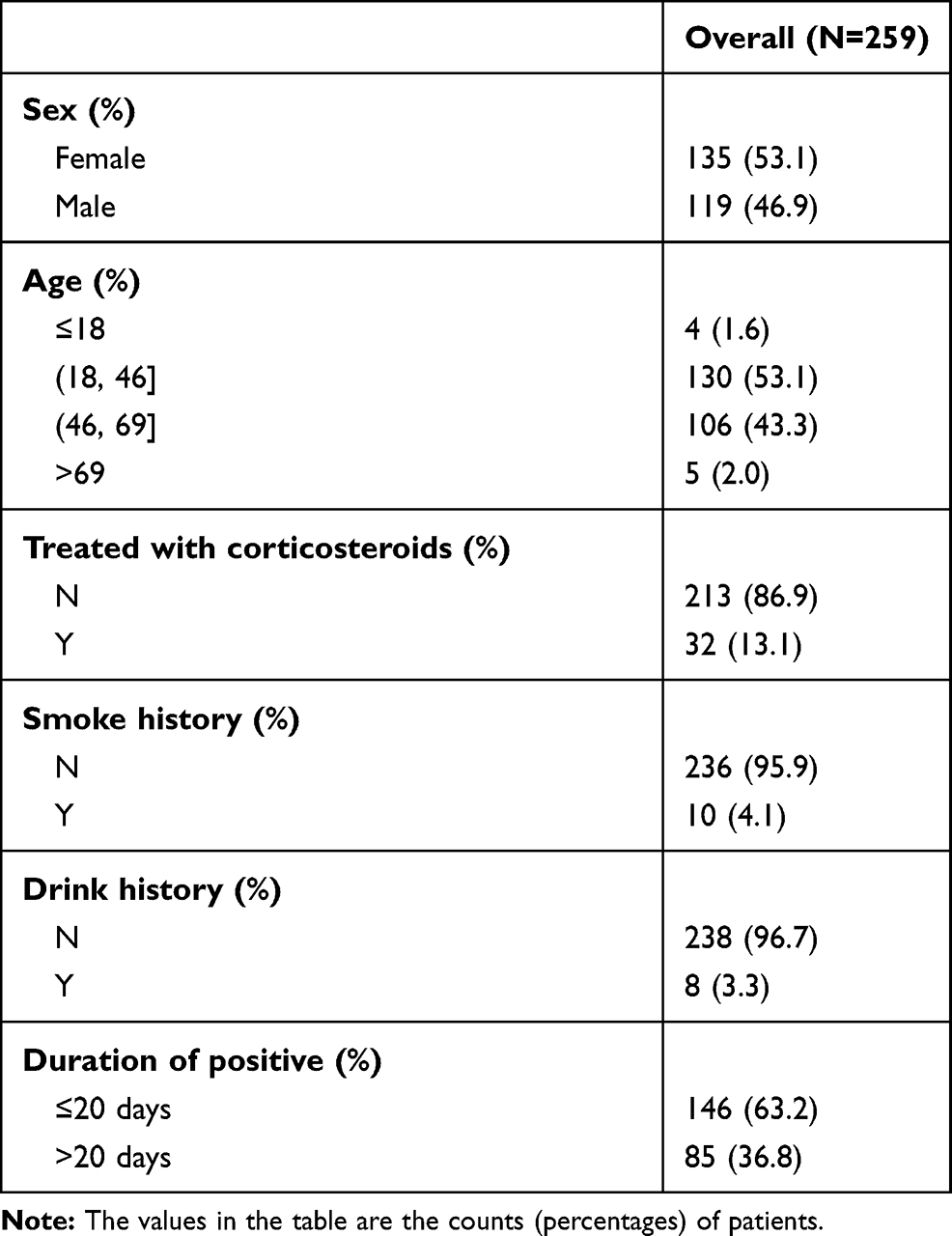 |
Table 1 Clinical Characteristics |
Univariate Analysis of SF-36 Score Decline
We first investigated some univariate correlations with risk factors related to the SF-36 score one month after discharge. Gender and different ages had nothing to do with related psychometric factors (including SF, VT, MH and RE) in the SF-36 score. In patients with smoking or drinking, as well as whether the use of corticosteroids, there was no statistically significant variation in the influence of psychometric factors in univariate analysis. The extension of positive nucleic acid duration was related to the decreased RE scores [100, IQR (66–100) vs. 100, IQR (0, 100); p = 0.0156] (Table 2).
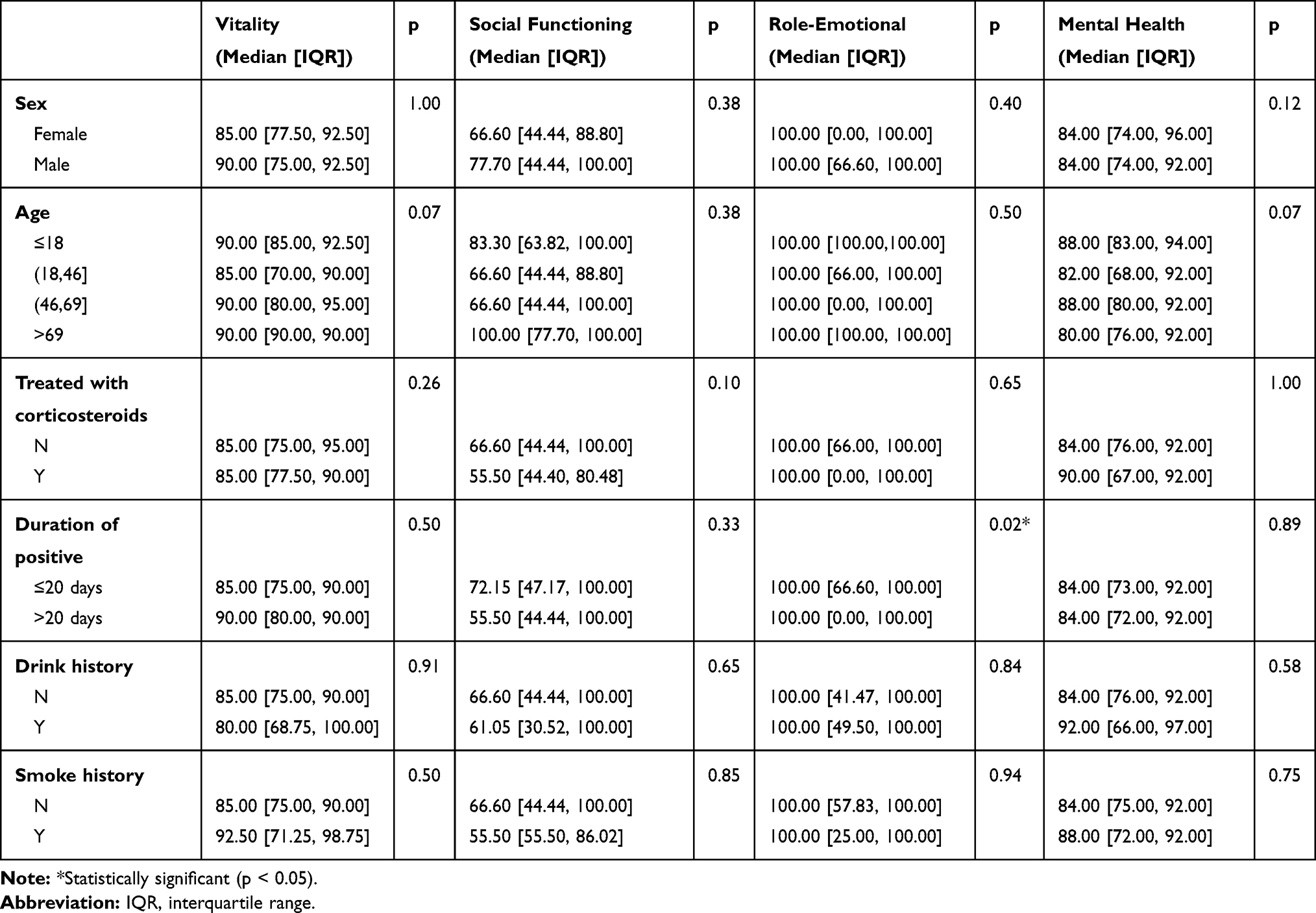 |
Table 2 Comparisons of SF-36 Scales by Univariate Analysis |
Multivariable Linear Regression Model Analysis of Independent Risk Factors for Decreased SF-36 Scales
A multiple linear regression model was established to find the independent risk factors for the decline of the SF-36 scores. Male sex and positive nucleic acid duration were related to decreased RE scores (p= 0.03; p= 0.01, respectively) (Table 3). Subsequently, we divided into three subgroups: less than seven days, 7 to 14 days and more than 14 days according to the positive nucleic acid duration. Linear regression analysis was performed on these three subgroups. The results revealed that there were significant differences in the VT scores and MH scores of patients aged 46 to 69 in the subgroup of the positive nucleic acid duration longer than 14 days (p = 0.0472; p = 0.0311, respectively). Similarly, there are also significant differences in RE scores in different genders (p = 0.0316) (Table 4).
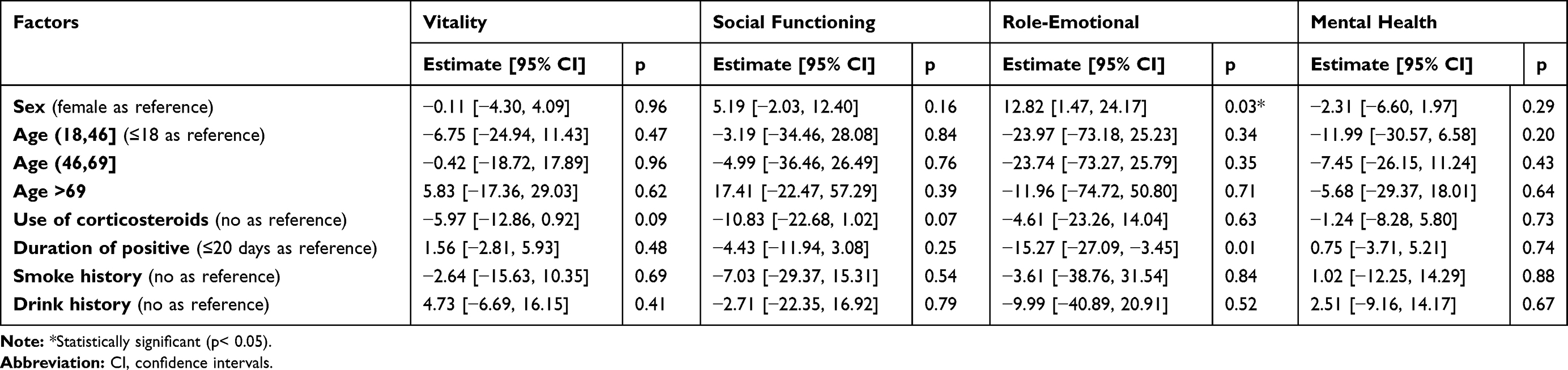 |
Table 3 Investigation of Independent Risk Factors for SF-36 Value Reduction by Multivariable Linear Regression Model |
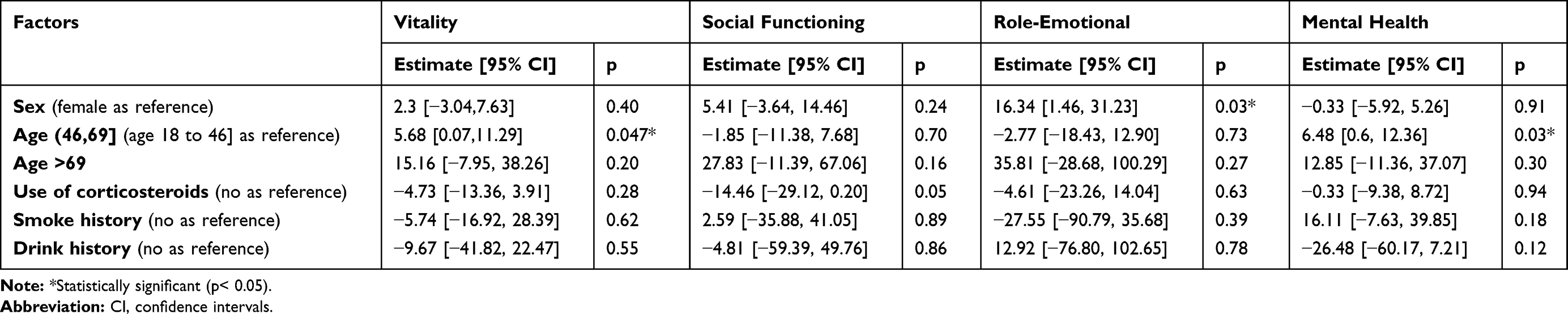 |
Table 4 Investigation of Independent Risk Factors for SF-36 Value Reduction in the Positive Nucleic Acid Duration Longer Than 14 Days by Multivariable Linear Regression Model |
Discussion
Our study reported for the first time, the HRQL test results of COVID-19 patients one month after discharge. The results showed that after the hospitalization of COVID-19 patients, the mental health was damaged. Based on the above results, we can find that the related factors that affect the patient’s psychometric properties include gender, age and the positive nucleic acid duration. These data provide a more sensitive and meaningful experience in assessing the mental state of patients and can help improve the quality of care.
Interestingly, our data found that in univariate analysis, only the extension of positive nucleic acid duration was related to the decreased RE scores. Moreover, in the multivariable linear regression model of RE, it can be seen that the positive nucleic acid duration is negatively correlated with the declined of the values, and the age is positively correlated with the increased of the values. The extension of positive nucleic acid duration is related to the decreased RE value; it might be associated with anxiety and depression. Some studies have shown that the RE scale can be used for outpatient screening for depression and anxiety, and the sensitivity and specificity of the results are acceptable.20–22 Under strict regulation in Zhejiang Province, China, hospital discharge should meet the following criteria: more than three days of normal body temperature; significant improvement of respiratory symptoms; the nucleic acid test results for respiratory pathogens should turn as negative twice consecutively (sampling time at least one day apart); and another 14 days of isolation after discharge. As a result, many recovered patients have to be isolated or long-term hospitalized, which may cause depression and anxiety. Studies have found that COVID-19 can cause a certain degree of anxiety symptoms in the community population,23 so specific COVID-19 patients, such as patients with longer positive nucleic acid duration, should receive psychological intervention as much as possible. We also noticed that there were significant differences in the VT scores and MH scores of patients aged 46 to 69 in the subgroup of the positive nucleic acid duration were longer than 14 days. Compared with other age groups, the group which positive nucleic acid duration was longer than 14 days was more likely to have psychometric properties. This may be because people in this group assume more important responsibilities in the family or society. The pressure they bear is greater than that of other groups. Similarly, there are also significant differences in RE scores in male. These results gave us some hints that COVID-19 infection might have more psychometric properties impact in middle age and males, who need psychological management as early as possible.
The advantage of this study lies in the collection of information on patients diagnosed in all designated hospitals for the treatment of COVID-19 in Wenzhou. The medical information and changes are complete. The quality of data management is well controlled. At the same time, we must also acknowledge a few limitations. First of all, our lost to follow-up rate was high. Because the patients were scattered around, some of them were unable to be contacted or unwilling to participate in the follow-up studies. Second, we lacked a dedicated mental assessment scale, so only the four aspects SF, VT, MH and RE, were evaluated. However, in the data analysis, the relevant parts of interest were still found. Finally, through data analysis, we found that the positive nucleic acid duration was negatively correlated with psychometric properties, but this was only a preliminary result and needed to be further verified.
In summary, this study described for the first time, the psychometric properties of COVID-19 patients without comorbidities in the short term after recovery. Related factors affecting psychometric properties included age, male sex, and the positive nucleic acid duration. Our findings are useful for early psychological intervention for such health emergencies in the future. Similarly, it is also recommended to measure relevant psychological scales in subsequent related studies.
Acknowledgments
Thanks to the doctors and nurses who assisted in the completion of the study, the patients who joined in the study, and the teachers who made suggestions to modify the manuscript.
Funding
This work was supported by the Wenzhou Municipal Sci-Tech Bureau Programs of China [grant number Y20180136]; Wenzhou Science and technology key problem program of China [grant number ZY2020001]; and The Special Project for Significant New Drug Research and Development in the Major National Science and Technology Projects of China [grant number 2020ZX09201002].
Disclosure
The authors report no conflicts of interest for this work.
References
1. World Health Organization. WHO Coronavirus Disease (COVID-19) dashboard. Available from: https://covid19.who.int/.
2. Peiris JS, Guan Y, Yuen KY. Severe acute respiratory syndrome. Nat Med. 2004;10(12 Suppl):S88–S97. doi:10.1038/nm1143
3. Chan-Yeung M, Xu R-H. SARS: epidemiology. Respirology. 2003;8(s1):S9–S14. doi:10.1046/j.1440-1843.2003.00518.x
4. Kannan S, Shaik Syed Ali P, Sheeza A, Hemalatha K. COVID-19 (novel coronavirus 2019) - recent trends. Eur Rev Med Pharmacol Sci. 2020;24(4):2006–2011.
5. Lake MA. What we know so far: COVID-19 current clinical knowledge and research. Clin Med (Lond). 2020;20(2):124–127. doi:10.7861/clinmed.2019-coron
6. Holshue ML, DeBolt C, Lindquist S, et al. First case of 2019 novel coronavirus in the United States. N Engl J Med. 2020;382(10):929–936. doi:10.1056/NEJMoa2001191
7. Liu Y, Mao B, Liang S, et al. Association between ages and clinical characteristics and outcomes of coronavirus disease 2019. Eur Respir J. 2020.
8. Tran BX, Ha GH, Nguyen LH, et al. Studies of novel Coronavirus Disease 19 (COVID-19) pandemic: a global analysis of literature. Int J Environ Res Public Health. 2020;17:11. doi:10.3390/ijerph17114095
9. Pérez Vela JL, Martín Benítez JC, Carrasco González M, et al. Clinical practice guide for the management of low cardiac output syndrome in the postoperative period of heart surgery. Med Intensiva. 2012;36(4):e1–e44. doi:10.1016/j.medin.2012.02.007
10. Skinner EH, Haines KJ, Howe B, et al. Health-related quality of life in australasian survivors of H1N1 influenza undergoing mechanical ventilation. a Multicenter Cohort Study. Ann Am Thorac Soc. 2015;12(6):895–903. doi:10.1513/AnnalsATS.201412-568OC
11. Batawi S, Tarazan N, Al-Raddadi R, et al. Quality of life reported by survivors after hospitalization for Middle East respiratory syndrome (MERS). Health Qual Life Outcomes. 2019;17(1):101. doi:10.1186/s12955-019-1165-2
12. Gandek B, Sinclair SJ, Kosinski M, Ware JE
13. McHorney CA, Ware JE
14. Hu J, Gruber KJ, Hsueh KH. Psychometric properties of the Chinese version of the SF-36 in older adults with diabetes in Beijing, China. Diabetes Res Clin Pract. 2010;88(3):273–281. doi:10.1016/j.diabres.2010.03.005
15. Jin YH, Cai L, Cheng ZS, et al. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version). Mil Med Res. 2020;7(1):4.
16. Zhou BCK, Wang J-F WY, Zheng W-J. Reliability and validity of a Short-Form health survey scale (SF-36), Chinese version used in an elderly population of Zhejiang province in China. Zhonghua Liu Xing Bing Xue Za Zhi. 2008;29:1193–1198.
17. Yan S, Lian Z, Sun G, Bao Y, Ge Y, Liu Z. Assessment of the Chinese-version SF-36 in the Chinese opiate addicts. Subst Use Misuse. 2011;46(13):1561–1568. doi:10.3109/10826084.2011.589880
18. Zhou K, Li M, Wang W, et al. Reliability, validity, and sensitivity of the Chinese Short-Form 36 health survey version 2 (SF-36v2) in women with breast cancer. J Eval Clin Pract. 2019;25(5):864–872. doi:10.1111/jep.13088
19. Zhang Z, Gayle AA, Wang J, Zhang H, Cardinal-Fernández P. Comparing baseline characteristics between groups: an introduction to the CBCgrps package. Ann Transl Med. 2017;5(24):484. doi:10.21037/atm.2017.09.39
20. Walsh TL, Homa K, Hanscom B, Lurie J, Sepulveda MG, Abdu W. Screening for depressive symptoms in patients with chronic spinal pain using the SF-36 health survey. Spine J. 2006;6(3):316–320. doi:10.1016/j.spinee.2005.11.004
21. Vilagut G, Forero CG, Pinto-Meza A, et al. The mental component of the short-form 12 health survey (SF-12) as a measure of depressive disorders in the general population: results with three alternative scoring methods. Value Health. 2013;16(4):564–573. doi:10.1016/j.jval.2013.01.006
22. Matcham F, Norton S, Steer S, Hotopf M. Usefulness of the SF-36 health survey in screening for depressive and anxiety disorders in rheumatoid arthritis. BMC Musculoskelet Disord. 2016;17:224. doi:10.1186/s12891-016-1083-y
23. Zhang Y, Ma ZF. Impact of the COVID-19 pandemic on mental health and quality of life among local residents in Liaoning Province, China: a Cross-Sectional Study. Int J Environ Res Public Health. 2020;17(7):2381.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.