")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Correlation of Alcohol Use Disorders with Common Mental Disorders and Its Association with Socio-demographic Characteristics Among Community in Ethiopia: A Cross-sectional Study
Received 31 August 2020
Accepted for publication 11 November 2020
Published 8 December 2020 Volume 2020:13 Pages 2909—2917
DOI https://doi.org/10.2147/RMHP.S279590
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Zakir Abdu, Mohammedamin Hajure
Department of Psychiatry, Faculty of Health and Medical Sciences, Mettu University, Mettu, Ethiopia
Correspondence: Zakir Abdu Tel +251 (0) 913845371
Email [email protected]
Background: Alcohol use disorders occurring together with common mental disorders are common and have been recognized worldwide as a crucial public health concern. However, there is a scarcity of data about the correlation of alcohol use disorders with common mental disorders and its association with socio-demographic characteristics among community in Ethiopia, especially in the study area. The aim of the study is to assess the correlation of alcohol use disordesr with common mental disorders and its association with socio-demographic characteristics among adults of selected woredas of the Ilu Aba Bor zone.
Methods: Community-based cross-sectional study was employed on 690 participants selected by using the multistage sampling technique. Data were collected by using the alcohol use disorder identification test (AUDIT) and self-reporting questionnaire (SRQ-20) scale. Data analysis were done using SPSS version 20. Pearson correlation was used to see the relation of two variables. The strength of the association was determined at p-value < 0.005.
Results: 14.1% of the study sample positive for alcohol use disorders and 27.2% for common mental disorders. There is a significant positive relationship between alcohol use disorders and common mental disorders, r(688)=0.314, p=0.001. From socio-demographic characteristics, multivariable logistic regression analysis revealed marital status being single, orthodox religion followers, and living in urban had a significant association with alcohol use disorders.
Conclusion: In the Ilu Aba Bor zone, 14.1% of participants reported alcohol use disorders, and 27.2% have a common mental disorders. There is a significant positive relationship between alcohol use disorders and common mental disorders. Being single, orthodox religion, and living in urban had a significant association with alcohol use disorders. Detection and treatment of people with alcohol use disorders and common mental disorders in the community have been recommended at the same time through integrated treatment.
Keywords: alcohol use disorders, common mental disorders, Ilu Aba Bor
Introduction
Alcohol is one of the most commonly used and misused substances by people with mental disorders.1 Alcohol use disorders’ (AUDs) occurring together with common mental disorders (CMDs) are common and have been recognized worldwide as a crucial public health concern.2–7 CMDs are the most common prevalent mental disorders in both developed and developing countries.8 It is a group of distress states manifesting with anxiety, depressive, and unexplained somatic symptoms typically encountered in community and primary care settings.9 Recently, CMDs account for 14% of the total burden of disease.2 The number of persons with CMDs globally is going up, particularly in lower-income countries, because the population is growing and more people are living to the age of 20 years when depression and anxiety most commonly occurs.10 It is predicted to be the first leading cause of disease burden by the year 2030.2
Four of the six leading causes of years lived with disability are due to neuropsychiatric disorders including AUDs and CMDs.2 More than four out of eleven people with AUDs have at least one mental disorders, especially CMDs.11 More than 3 million deaths in 2016 were attributed to alcohol-related risks.12 Half of the world’s population drink alcohol13 and over 75 million are diagnosed with AUDs.14 AUDs are the third leading cause of ill health and premature death globally.13 Worldwide, the overall prevalence of AUDs were 2.2% to 44%.15,16 Alcohol-related health and social problems are on the rise in sub-Saharan Africa.17
Different kinds of literatures described associations between AUDs and CMDs as follows: 1) CMDs are the primary disorder and alcohol is used to cope with the symptoms of CMDs;18–30 2) AUDs are the primary disorders, and CMDs symptoms develop as a consequence of AUDs;3,5,12,20,26,28,30–35 3) CMDs and AUDs are unrelated but may interact with each other; 4) Both CMDs and AUDs share a common genetic or psychosocial cause;28 5) The causality and nature of the associations between AUDs and CMDs remain complex and unclear;20,32,36 6) A vicious cycle of increasing CMDs symptoms and alcohol use that could result in comorbidity; once both alcohol use and mental disorders are present, each disorders could promote the maintenance or exacerbation of the other;3,20,26,37 or 7) Other study confirmed as AUDs were not associated with CMDs.38
Alone or combined, AUDs and CMDs can lead to problems like damaged relationships, poor academic performance, problems with the law, and reduced overall health conditions.32 Generally, AUDs and CMDs can greatly affect the health of individuals, as well as their families and their community.3 Coexistence of harmful use of AUDs and CMDs affect the course, severity, and outcomes of both disorders as well as treatment outcomes and contributes to a negative prognosis of both sets of disorders.19,20,39,40
Correlation of alcohol use disorders with common mental disorders and its association with socio-demographic characteristics are relatively well explored in high-income countries. But, there have been fewer studies on low and middle-income countries, especially in Ethiopia. Therefore, the finding of this study will show the correlation of alcohol use disorders with common mental disorders and its association with socio-demographic characteristics among residents of the Ilu Aba Bor zone, which will be vital for regional health office to link with hospitals and health centers and manage it. And also this study will reveal important factors associated with alcohol use disorders; therefore, from the result of this study, Ministry of health and non-governmental organizations who are working on alcohol use disorders and mental health can be benefited. In addition, this study will be vital to investigate problem and important recommendation to reduce the morbidity, mortality and other consequences associated with the alcohol use disorders and to enhance the health status of the community. Furthermore, the finding of the study will serve as the baseline for the study on similar topic and also input for policy makers, planners and those who are working in higher institution to indicate appropriate methods to tackle the problem regarding correlation of alcohol use disorders with common mental disorders and associated factors in the community. That is why we are interested to conduct this research. The aim of the study is to assess the correlation of alcohol use disorders with common mental disorders and its association with socio-demographic characteristics among adults of selected woredas of the Ilu Aba Bor zone.
Methods and Materials
Study Design and Setting
A cross-sectional community based study was carried out in various woredas in the Ilu Aba Bor zone between 1 July and 30 August 2018.
Source Population
All residents of the Ilu Aba Bor zone during 2018.
Study Population
All residents of the Ilu Aba Bor zone included in the frame in order to obtain an equal opportunity to be selected during the data collection period.
Inclusion and Exclusion Criteria
Inclusion Criteria
All persons aged 18 years and above.
Exclusion Criteria
A severely ill person was excluded.
Sample Size Determination
The sample size was determined based on a one-population proportion formula. The total sample size was 690, based on the assumption of 21%17 prevalence and a design effect of 1.5x, a tolerance of 0.04 sampling error and a 15% non-response rate.
Sampling Technique
A multi-stage stratified sampling technique was used to choose study participants. Stratification was initially carried out at woreda level, then at kebele level. Participants were selected through systematic randomization. Kebele and woreda are a small group of administrators in Ethiopia. Ethiopia currently has 9 regional states and 2 administrative cities. Of nine regional states, Oromia is one and the largest regional state. There are approximately 22 zones. In Ethiopia, different kebeles come together to wear woredas. Different woredas come together and form zones. Different zones gather and form one regional state. Different regional states gather and form one country, Ethiopia. The Ilu Aba Bor zone has 13 woredas. Because the study was a survey study, based on the rule of thumb, 30% of the total woreda were included in the study which is 4 woreda.
These 4 woredas were randomly selected from 13 woredas in total. This is the first stratification at woreda level. Below these four woredas a total of 93 kebeles found. Seventeen kebeles from Hurumu woreda representing 18.28%, 34 kebeles from Alge Sachi woreda representing 36.56%, 18 kebeles from Yayo woreda representing 19.35% and 24 kebeles from Bure woreda representing 25.8%. Kebeles were selected from each woreda on the basis of representative percentage or proportional distribution. This means that woreda that has more kebeles, selected participants are also more and whereas woreda that has less kebeles, selected participants are also less. For instance, Alge Sachi woreda who has 34 kebeles, 248 participants were included in the study, while Hurumu woreda who has 17 kebeles, 126 participants were included in the study. Therefore, 18.28% of 17 kebeles meaning 3 kebeles in the Hurumu woreda (126 participants), 36.56% of 34 kebeles meaning 13 kebeles in the Alge Sachi woreda (248 participants), 19.35% of 18 kebeles meaning 4 kebeles in the Yayo woreda (136 participants) and 25.8% of 24 kebeles meaning 6 kebeles in the Bure woreda (180 participants) was randomly selected by simple random sampling (lottery) method. This is a second stratification for the kebele. Participants were chosen based on households. On average, every kebele has 350 homes. For example, to obtain a kebele 01 household from Bure woreda that we obtained from participants, we first divided a total of Kebele 01 households by a number of allocated households (180/30). We randomly selected a household of 1 to 6; we obtained household #2. So, for the kebele 01 from Bure woreda, a household found in the #2 list was a first household we were selected participants. At each of the six intervals, households were selected. For Bure woreda kebele 01, the first household was registered at #2, a second household was registered at #8, the third was at #14, the fourth was at #22 and so on until we received 30 households from kebele 01 for Bure woreda.
The technique was applied to all selected kebeles. Once the household was identified or selected by a systematic random sampling technique using kebeles, one participant per household was invited to participate in the study using the Kish method and the inclusion and exclusion criteria.
Data Collection Procedure and Tools
The data were gathered using a semi-structured paper questionnaire by face-to-face interview. Initially, the tools and developed a structured questionnaire in English was translated to Afan Oromo and back to English by an independent person to verify the consistency and understanding of the tools. Socio-demographic questionnaires were developed after a thorough review of similar literatures and research. The alcohol use disorder identification test (AUDIT) was used to assess alcohol use disorders and is developed by the World Health Organisation (WHO). The overall rating for AUDIT is 40. A score of 8 or greater is considered to be a drinking disorder.41,42 The self-reported questionnaire (SRQ-20), prepared by the WHO, was used to assess the absence and presence of CMDs. The SRQ-20 was originally designed as a self-administered scale, but was also deemed appropriate for the questionnaire administered by the interviewer because of low literacy rates in developing countries.43 Each of the 20 elements came up with 0 or 1. A score of 1 indicates the presence of the symptom during the previous month, a score of 0 indicates the absence of the symptom. A cutoff point of 7/8 (7“yes’s’ a non-case, 8 ‘yes’s” a case) was used which is the most commonly used cut off point in developing countries.43 Its validity was done in low and middle-income countries44 and in Eritrea.45
Data Processing, Analysis, Interpretation and Presentation
Once all necessary data were obtained, data were checked for completeness. Data were coded, entered to Epi Data version 3.1, exported to SPSS and cleaned. The collected data were analyzed using SPSS version 20.0. The data were processed by using descriptive analysis, bivariate analysis and multi-variable logistic regression. Descriptive analysis was used to compute demographic characteristics of participants. In addition, bivariate and multi-variable logistic regression analysis was used to see the significance of the association. Pearson correlation was used to see the relation of AUDs and CMDs. Statistical significance was declared at p-value less than 0.05. Significance of association of the variables was described using AOR with 95% confidence interval.
Ethical Considerations
This study was carried out according to the Helsinki Declaration. Ethics approval was obtained from the Ethics Review Committee of the Faculty of Health Sciences at Mettu University. Then the letter of authorization was obtained from the Department of Health of the Ilu Aba Bor zone. The selected participants were informed of the nature, goals, benefits and negative impacts of the study and invited to participate. Privacy was ensured and all related issues were raised. Participation was entirely voluntary, with no economic or other rationale, and each participant signed a written informed consent for participation. The right of participants to decline or terminate their participation at all times was strictly respected.
Operational Definition
Based on this study, the definition of CMDs is as follows.
The SRQ-20 contains 20 items and each item has a yes (1) or no (0) response. The minimum score is 0, while the highest score is 20. Participants who score 8 and above are considered to have a CMDs, while participants who score 7 or below do not have a CMDs.43
Critically ill: subjectively, participants complain of the pain of any type of illness or objectively of participants, called ill and unable to communicate due to illness during data collection. Data collectors and trained supervisors identified or measured critically ill participants prior to commencing the interview.
Results
Socio-Demographic Characteristics of Respondents
A total of 690 participants were surveyed, most of whom were men 60.8% (n=420). The median age of respondents was 31 years and the inter-quartile range was 15 years. Of the participants, 43.1% (n=298) were Orthodox by religion, with about three-quarters living in rural residences (Table 1).
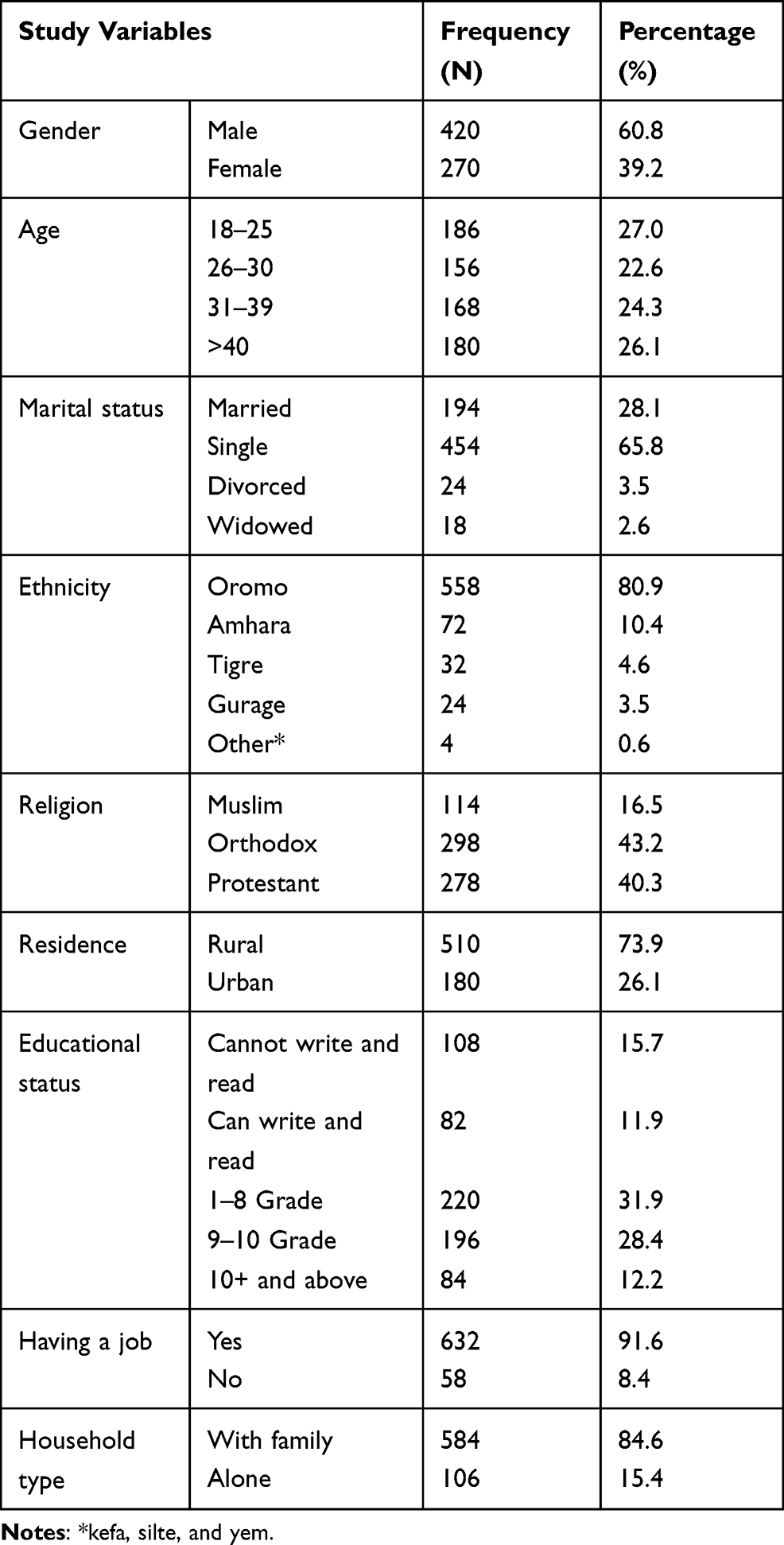 |
Table 1 General Characteristics of Study Participants Among Selected Woreda Adults from the Ilu Aba Bor zone of Southwestern Ethiopia |
Prevalence of Alcohol Use Disorders and Common Mental Disorders
In the overall sample, the prevalence of alcohol use disorders was 14.1% (n=97; 95% CI: 11.2, 16.7) and the prevalence of abstinence was 85.9% (n=593; 95% CI: 83.3, 88.8). Among participants (n=188) with CMDs, 31.9% (n=60) had AUDs, whereas among participants (n=502) without CMDs, 7.4% (n=37) had AUDs.
The one-month prevalence of the study showed that 3 out of 11 participants, 27.2% (n=188) had a common mental disorders.
There is a significant positive relationship between alcohol use disorders and common mental disorders, r(688)=0.314, p=0.001.
The socio-demographic characteristics of respondents such as gender, age, education and employment did not reveal any link to alcohol use disorders in the bivariate analysis. However, residence, marital status, religion, living alone and having a common mental disorders were associated with a drinking disorder in a bivariate analysis. Multivariate logistic regression analysis found that marital status was single, orthodox in religion, urban, and with common mental disorders were significantly associated with alcohol use disorders (Table 2).
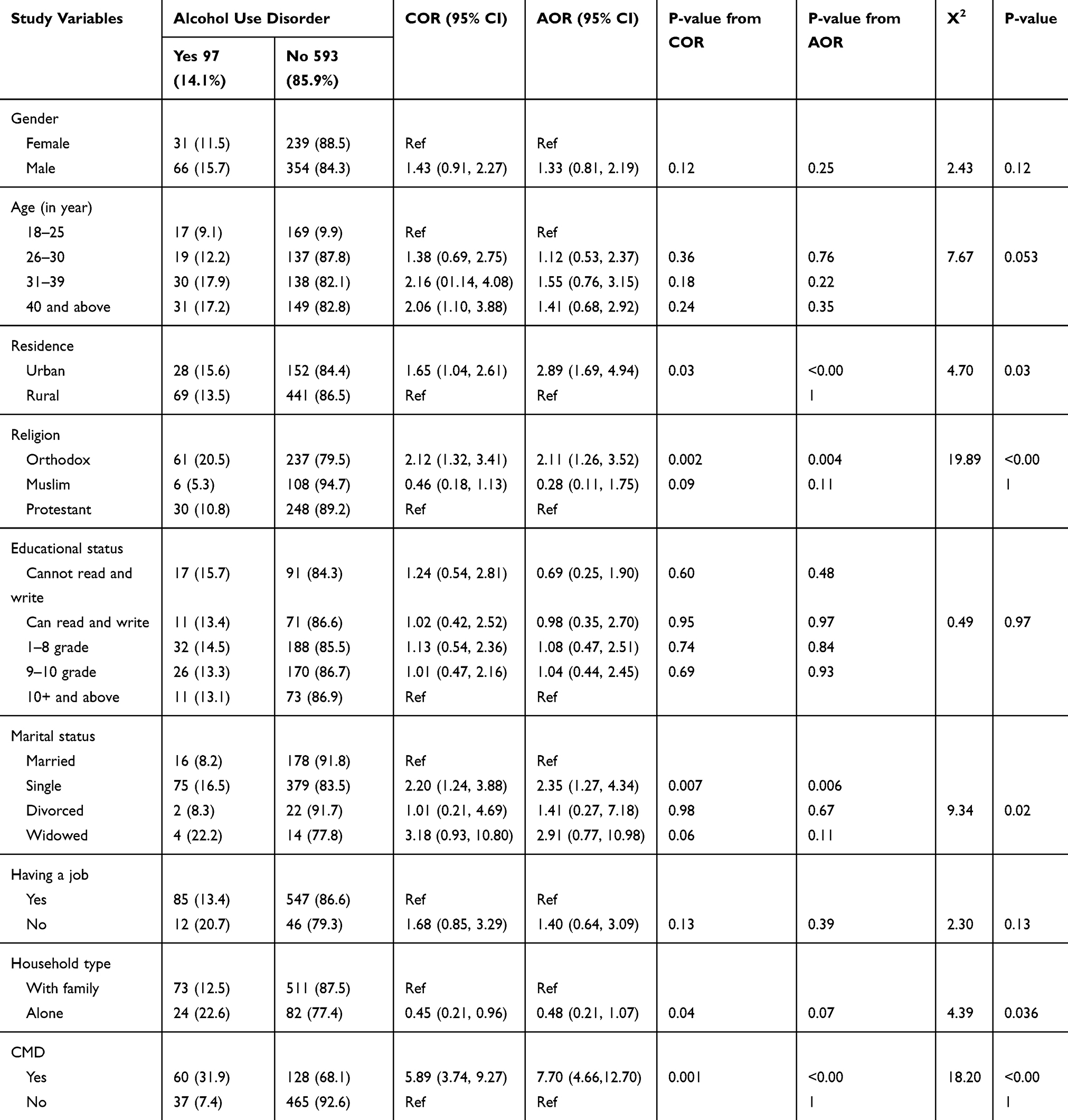 |
Table 2 Factors Associated with Alcohol Use Disorders by Bivariate and Multivariable Logistic Regression and Chi‐square Test Among Selected Woreda Adults from the Ilu Aba Bor zone of Southwestern Ethiopia |
Discussion
The results of this study showed a prevalence of AUDs of 14.1% (n=97; 95% CI: 11.2, 16.7). This was consistent with studies carried out in Ethiopia (14.2%),46 in Iraq 12.2%47 and Brazil 13.1%.48 The probable reason could be studies conducted on the same population46,48 and the tools used46–48 in the current and previous studies are same.
However, it was lower than the finding of the studies done in Ethiopia 17.4%49 and 38.9%,50 Ghana 43%,51 Eastern Africa 29%,52 Nigeria 39.5%,53 Turkey 29.7%,54 Brazil 18.4%,55 28.6%56 and 26.9%,21 and US 67.8%.57
The first probable reason for difference of the result could be some of the previous studies conducted hospital based,49,50 but the current study was community based. On other hand, the previous study was done only among youth and sample size was half of the current study51 and the previous study done among outdoor drinkers in public open places,53 but the current study was conducted on the general population. Another reason for difference in result could be the previous study was systematic review,52 while, the current was community-based cross-sectional study. The other probable reason could be the previous study was conducted among students, tool they used was CAGE, and sample size was lower than the current study.54
The current study was higher than the finding of the studies done in South Africa 9%58 and 3.6% of men and 1.4% of women,59 Nepal 7.3%,60 Uganda 4.1%,61 China 2.2%.15
The probable reason for the difference between the current and previous outcome could be the result of an earlier study conducted 8 years ago15,58,59 that alcohol consumption could increase from time to time. The other reason might be that the participants in the previous study were 15 years old and over half were women,58 indicating that there may have been fewer alcohol-related disorders prior to age 15 and that women were less likely to report alcohol-related disorders. The other likely reason might be the result of the difference is the different usage of the cutoff note for AUDIT, which is the cutoff note of 9 in the previous study60 and 8 in the current study.
In this study, sex did not exhibit any association with alcohol consumption disorders in the bivariate analysis. This finding is inconsistent with previous studies, in the Netherlands alcohol dependence was associated with the male sex,29 in Nigeria, men were associated with current drinking,62 and in Ethiopia, females were least likely to develop AUDs.50 The probable reason for the difference in outcomes could be previous clinical studies29,50 while the current study was a community study. Another probable reason could be a large variation in sample size between current and previous studies.29,62 Another probable reason for the difference in outcomes may be the use of different study tools and the difference in study design between the previous study62 and the current study. Finally, the reason for the difference in results could be the present study, which was conducted in a rural community setting and compared with the previous study.
The outcome of this study found that participants in urban dwellings were more likely to have a drinking disorder than their counterparts. This finding was corroborated by the previous South African study.58 It could be due to the availability of alcohol is higher in urban areas and also explained by the fact that many people have consumed alcohol for different purposes, routinely used for social and relaxation purposes with friends followed by to relieve stress in urban areas. On the other hand, this finding was inconsistent with the study done in Nigeria,53 the possible reason could be that the previous study was carried out among outdoor drinkers in public open places and subjects were recruited with non-probability purposive sampling method.53 In this case, the rural dwellers may more drink alcohol at open public places and enter to study with non-probability purposive sampling.
The risk of alcohol use problems for unmarried participants was 2.35 times higher than for married participants. This result is in line with the study carried out in Nigeria62 and in Brazil.55 This could be explained by the fact that non-married persons were free of family control and consumed alcohol as married persons. In addition, they were able to make independent decisions throughout their lives and results in participating in alcoholic beverages. The other reason might be single in marital status had less responsibility to their family than married one and they participated in drinking than their counterparts.
The chances of obtaining AUDs among members of the Orthodox religion were higher than among members of the Protestant religion. This finding corresponds to a clinical study carried out in Jimma, Ethiopia.50
In addition, to our knowledge, no similar research has been conducted in Ethiopia on this title. Thus, the conclusion of the study will be important to indicate appropriate methods to address the problems concerning the correlation of alcohol use disorders with common mental disorders and the associated factors for the Ethiopian community. In treating alcohol use disorders and common mental health disorders in the community according to their characteristics, we can change the health outcomes of individuals and communities and the investment the research community has made in developing new treatment options that are more effective.
Strength of the Study
- Nationally, this study is a first and could be used as a reference point for researchers in the future.
- In this study, the tools used to evaluate alcohol-related disorders and common mental disorders are standardized and validated.
- Data were obtained from four woredas of the area administration.
- There was a 100% response rate.
Limitations of the Study
- Given its cross-sectional nature, the study could not explore the causal relationship between the variables.
- The other limitation of this study is the absence of search for variables such as other substances (such as cocaine, heroin and amphetamine).
- Another limitation of the study is information bias, the use of survey tools, and the misclassification of variables such as educational attainment.
Conclusion
This study showed that alcohol consumption disorders (14.1%) and common mental disorders (27.2%) are common in the Ilu Aba Bor community. There is an important positive relationship between drinking disorders and common mental disorders. Being single, following an orthodox religion, and living in an urban setting were strongly associated with alcohol-related disorders.
Recommendations
- The detection and treatment of individuals with AUDs and CMDs in the community was simultaneously recommended through integrated treatment. Target follow up of AUDs and CMDs screening and treatment should be done as needed.
- In addition, large-scale longitudinal research should be needed to discuss and infer a temporal relationship between the AUDs and the CMDs.
Acknowledgments
We wish to thank Mettu University and the Department of Health of the Ilu Aba Bor zone for giving us this opportunity. We are also grateful to the study participants, data collectors and supervisors, the Woredas Health Units and the Department Head for their great contribution and support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gordon A, et al. Comorbidity of mental disorders and substance use: a brief guide for the primary care clinician. In: Drug and Alcohol Services South Australia. Government of South Australia; 2008:P3–4653.
2. Investing in mental health by department of mental health and substance dependence, noncommunicable diseases and mental health. World Health Organization [Internet]. Geneva; 2003. Available from: www.who.int/mental_health.
3. Barnes BN. Compulsive comorbidities: links between generalized anxiety disorder and substance use disorders among African American women. 2016.
4. Man H, Lai X, Cleary M, Sitharthan T, Hunt GE. Prevalence of comorbid substance use, anxiety and mood disorders in epidemiological surveys, 1990–2014: a systematic review and meta-analysis. Drug alcohol depend [Internet]; 2015. Available from: http://dx.doi.org/10.1016/j.drugalcdep.2015.05.031.
5. Stewart SH Anxiety disorders and substance use disorders; 2010. Available from: https://www.researchgate.net/publication/283910858.
6. Nicolas Clark, et al. Prevention of Drug Use and Treatment of Drug Use Disorders in Rural Settings, Revised Version. New York, Vienna: UNODC, UNITED NATIONS; 2017. [Internet]. Available from: www.unodc.org.
7. Van DW, et al. Validation of the self reporting questionnaire 20-item (SRQ-20) for use in a low- and middle-income country emergency centre setting. Int J Ment Heal Addict. 2017;14(1):37–48.
8. Haile YG, Alemu SM, Habtewold TD. Common mental disorder and its association with academic performance among Debre Berhan University students, Ethiopia. Int J Ment Health Syst. 2017;8–12.
9. Lopes CS, Abreu GA, Santos DF, et al. ERICA: prevalence of common mental disorders in Brazilian adolescents. Rev Saude Publica. 2016;50(Suppl1): 1–9.
10. Depression and other common mental disorders global health estimates. WHO [Internet]; 2017. Available from: https://creativecommons.org/licenses/by-nc-sa/3.0/igo.).
11. NAMi hearts & minds, mental illness and substance abuse [Internet]. Vol. 1; 2010. Available from: www.nami.org.
12. Global status report on alcohol and health, World Health Organization [Internet]. Geneva; 2018. Available from: www.who.int/substance_abuse.
13. European action plan to reduce the harmful use of alcohol 2012–2020 79. World Health Organization [Internet]; 2012. Available from: http://www.euro.who.int/pubrequest.
14. Prevention of Mental Disorders, a Report of the World Health Organization, Department of Mental Health and Substance Abuse in Collaboration with the Prevention Research Centre of the Universities of Nijmegen and Maastricht. Geneva: World Health Organization; 2004.
15. Cheng HG, Deng F, Xiong W, Phillips MR. Prevalence of alcohol use disorders in mainland China: a systematic review. Addiction. 2015;110:761–774. doi:10.1111/add.12876
16. Weaver T, Madden P, Charles V, et al. Comorbidity of substance misuse and mental illness in community mental health and substance misuse services. Br J Psychiatry. 2003;183:304–313. doi:10.1192/bjp.183.4.304
17. Teferra S, Medhin G, Selamu M, Bhana A, Hanlon C, Fekadu A. Hazardous alcohol use and associated factors in a rural Ethiopian district: a cross-sectional community survey. BMC Public Health. 2016;16:1–7. doi:10.1186/s12889-016-2911-6
18. Mancebo MC, Grant JE, Pinto A, Eisen JL, Rasmussen SA. Journal of anxiety disorders substance use disorders in an obsessive compulsive disorder clinical sample §. J Anxiety Disord Subst. 2009;23:429–435. doi:10.1016/j.janxdis.2008.08.008
19. Gentil AF, Alice M, Mathis D, et al. Alcohol use disorders in patients with obsessive – compulsive disorder: the importance of appropriate dual-diagnosis. Drug Alcohol Depend J. 2009;100:173–177. doi:10.1016/j.drugalcdep.2008.09.010
20. Harmful use of alcohol, alcohol dependence and mental health conditions: a review of the evidence for their association and integrated treatment approaches, World Health Organization [Internet]. Denmark; 2019. Available from: http://www.euro.who.int/pubrequest.
21. Trettim P, Jansen K, Silva RA, et al. Psychoactive substance abuse and dependence and its association with anxiety disorders: a population-based study of young adults in Brazil. Brazilian J Psychiatry. 2018;40:349–353. doi:10.1590/1516-4446-2017-2258
22. Gilman SE, David H. A longitudinal study of the order of onset of alcohol dependence and major depression. Drug Alcohol Depend. 2001;63:277–286. doi:10.1016/S0376-8716(00)00216-7
23. Fröjd S, Ranta K, Kaltiala-heino R, Marttunen M. Associations of social phobia and general anxiety with alcohol and drug use in a community sample of adolescents. Alcohol Alcohol. 2011;46(2):192–199. doi:10.1093/alcalc/agq096
24. Swendsen JD, Tennen H, Carney MA, et al. Mood and alcohol consumption: an experience sampling test of the self-medication hypothesis. J Abnorm Psychol. 2000;109(2):198–204. doi:10.1037/0021-843X.109.2.198
25. Thomas SE, Randall CL, Carrigan MH. Drinking to cope in socially anxious individuals: a controlled study. Alcohol Clin Exp Res. 2003;27:12. doi:10.1097/01.ALC.0000100942.30743.8C
26. Sabourin BC, Stewart SH. Alcohol use and anxiety disorders. Anxiety Heal Behav Physical Illness. 2007;29–55.
27. Po-Hsiu Kuo CO, Gardner J, Kenneth S, Kendler CAP. The temporal relationship of the onsets of alcohol dependence and major depression: using a genetically informative study design. Psychol Med. 2006;36:1153–1162. doi:10.1017/S0033291706007860
28. Bacon AK, Ham LS. Addictive behaviors attention to social threat as a vulnerability to the development of comorbid social anxiety disorder and alcohol use disorders: an avoidance-coping cognitive model. Addict Behav. 2010;35(11):925–939. doi:10.1016/j.addbeh.2010.06.002.
29. Boschloo L, Vogelzangs N, Smit JH, et al. Comorbidity and risk indicators for alcohol use disorders among persons with anxiety and/or depressive disorders: findings from the Netherlands Study of Depression and Anxiety (NESDA). J Affect Disord. 2011;131(1–3):233–242. doi:10.1016/j.jad.2010.12.014.
30. Marmorstein N. Anxiety disorders and substance use disorders: different associations by anxiety disorder. J Anxiety Disord. 2012;26(1):88–94. doi:10.1016/j.janxdis.2011.09.005
31. Swendsen JD, Merikangas KR, Canino GJ, Kessler RC, Rubio-stipec M. The comorbidity of alcoholism with anxiety and depressive disorders in four geographic communities. Compr Psychiatry. 1998;39(4):176–184. doi:10.1016/S0010-440X(98)90058-X
32. Canadian Centre on Substance Abuse (ISBN 978-1-927467-92-3). When mental health and substance abuse problems collide [internet]; 2013. Available from: www.ccsa.ca.
33. Hasin DS, Goodwin RD, Frederick S, Stinson BFG. Epidemiology of major depressive disorder. Arch Gen Psychiatry. 2005;62:1097–1106. doi:10.1001/archpsyc.62.10.1097
34. Fidalgo TM. Psychiatric comorbidity related to alcohol use among adolescents. Am J Drug Alcohol Abuse. 2008;34(1):83–89. doi:10.1080/00952990701764664
35. Pickering RP, Kaplan K. Prevalence and co-occurrence of substance use disorders and independent mood and anxiety disorders. Arch Gen Psychiatry. 2006;61(2):807–816.
36. Pasche S. Exploring the comorbidity of anxiety and substance use disorders. Curr Psychiatry Rep. 2012;14:176–181. doi:10.1007/s11920-012-0264-0
37. Boden JM, Fergusson DM. Alcohol and depression. Addiction. 2010;106:906–914. doi:10.1111/j.1360-0443.2010.03351.x
38. Wang J, Pat SB. Alcohol consumption and major depression: findings from a follow-up study. Can J Psychiatry. 2001;46:632–638. doi:10.1177/070674370104600708
39. Roy-byrne P. Understanding and treating comorbid anxiety disorders in substance users review and future directions. J Addict Med. 2011;5(4):233–247.
40. Myrick H, Brady K. Current review of the comorbidity of affective, anxiety, and substance use disorders. Curr Opin Psychiatry. 2003;16:261–270. doi:10.1097/01.yco.0000069080.26384.d8
41. Babor TF, Higgins-Biddle JC, John B, Saunders MGM. The Alcohol Use Disorders Identification Test Guidelines for Use in Primary Care
42. The Alcohol Use Disorders Identification Test (AUDIT): interview Version. Available from: http://whqlibdoc.who.int/hq/2001/who_msd_msb_01.6a.pdf. 2001.
43. Beusenberg M. A User’s Guide to the Self Reporting Questionnaire (SRQ). Geneva: World Health Organization; 1994.
44. van der Westhuizen C, Wyatt G, Williams JK, Stein DJ. HHS public access. Int J Ment Heal Addict Author. 2017;14(1):37–48. doi:10.1007/s11469-015-9566-x
45. Netsereab TB, Kifle MM, Tesfagiorgis RB, Habteab SG. Validation of the WHO self-reporting questionnaire-20 (SRQ −20) item in primary health care settings in Eritrea. Int J Ment Health Syst. 2018;12(61):1–9. doi:10.1186/s13033-018-0242-y
46. Bultum JA, Yigzaw N, Demeke W, Alemayehu M. Alcohol use disorder and associated factors among human immunodeficiency virus infected patients attending antiretroviral therapy clinic at Bishoftu General Hospital, Oromiya region, Ethiopia. PLoS One. 2018;13(3):1–12. doi:10.1371/journal.pone.0189312.
47. Al-Ameri RJK, Husham J, RKL AA-B. Prevalence of alcohol consumption among university students in Baghdad: a cross-sectional survey from Iraq. Epidemiol Biostat Public Heal. 2016;13(4):1–8.
48. Barros MBA, et al. Prevalence of alcohol abuse and associated factors in a population-based study. Rev Saúde Pública. 2007;41(4):502–509. doi:10.1590/S0034-89102006005000032
49. Waja, et al. Prevalence of alcohol use disorders and associated factors among people with epilepsy attending Amanuel Mental Specialized Hospital. Neuropsychiatr Dis Treat. 2016;12:2989–2996. doi:10.2147/NDT.S122296
50. Zenebe Y, Negash A, Gt F, Krahl W. Alcohol use disorders and its associated factors among psychiatric outpatients in Jimma University Specialized Hospital, Southwest Ethiopia. J Alcohol Drug Depend. 2015;3:3.
51. Osei-Bonsu E. Prince Kubi Appiah Idn. prevalence of alcohol consumption and factors influencing alcohol use among the youth in Tokorni-Hohoe, Volta Region of Ghana. Sci J Public Heal. 2017;5:3.
52. Francis JM, Grosskurth H, Changalucha J, Kapiga SH, Weiss HA. Systematic review and meta-analysis: prevalence of alcohol use among young people in eastern Africa. Trop Med Int Heal. 2014;19(4):476–488. doi:10.1111/tmi.12267
53. Lasebikan VO, Ayinde O, Odunleye M, Adeyefa B, Adepoju S, Fakunle S. Prevalence of alcohol consumption and alcohol use disorders among outdoor drinkers in public open places in Nigeria. BMC Public Health. 2018;18(400):1–10. doi:10.1186/s12889-018-5344-6
54. Demİrbaş H. Substance and alcohol use in young adults in turkey as indicated by the cage questionnaire and drinking frequency. Arch Neuropsychiatry. 2015;52:29–35. doi:10.5152/npa.2015.6916
55. Reisdorfer E, et al. Prevalence and associated factors with alcohol use disorders among adults: a population-based study in southern Brazil. Rev Bras Epidemiol. 2012;15(3):582–594. doi:10.1590/S1415-790X2012000300012
56. Moss C, Mendoza-sassi RA, Dias L, Nader MM, Maria A, De MB. Alcohol use disorders among people living with HIV/AIDS in southern Brazil: prevalence, risk factors and biological markers outcomes. BMC Infect Dis. 2017;17(263):1–8.
57. Klein H, Sterk CE, Elifson KW. The prevalence of and factors associated with alcohol-related problems in a community sample of African American Women. Hindawi Publ Corp J. 2016;2016.
58. Peltzer K, Davids A, Njuho P. Alcohol use and problem drinking in South Africa: findings from a national population-based survey. Afr J Psychiatry. 2011;1:30–37.
59. Pengpid S, Peltzer K, Heever H, Der V. Prevalence of alcohol use and associated factors in urban hospital outpatients in South Africa. Int J Environ Res Public Heal. 2011;8:2629–2639.
60. Luitel NP, Baron EC, Kohrt BA, Komproe IH, Jordans MJD. Prevalence and correlates of depression and alcohol use disorder among adults attending primary health care services in Nepal: a cross sectional study. BMC Health Serv Res. 2018;18(215):1–10.
61. Nalwadda O, Rathod SD, Nakku J, Lund C, Prince M, Kigozi F. Alcohol use in a rural district in Uganda: findings from community based and facility based cross sectional studies. Int J Ment Health Syst. 2018;12(12):. doi:10.1186/s13033-018-0191-5
62. Lasebikan VO, Ola BA. Prevalence and correlates of alcohol use among a sample of nigerian semi rural community dwellers in Nigeria. Hindawi Publ Corp. 2016. doi:10.1155/2016/2831594
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.