")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Correlation Between Recovery of Menstrual Cycle and Improvement of Glucose and Lipid Metabolism in Patients with Sleeve Gastrectomy in a Small Chinese Cohort Sample
Received 6 October 2020
Accepted for publication 17 November 2020
Published 1 December 2020 Volume 2020:13 Pages 4711—4715
DOI https://doi.org/10.2147/DMSO.S285114
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Yu Ran, Qiang Yi, Cong Li
Department of Gynecology, The First Affiliated Hospital of Chongqing Medical University, Chongqing City, People’s Republic of China
Correspondence: Cong Li
Department of Gynecology, The First Affiliated Hospital of Chongqing Medical University, YuZhong District, Chongqing City 400010, People’s Republic of China
Tel +8615334506105
Fax +86(23) 89011080
Email [email protected]
Objective: To analyze the status of insulin resistance and hyperlipidemia in the regulation of menstrual cycle in patients undergoing sleeve gastrectomy (LSG).
Materials and Methods: Retrospective analysis of a typical metabolic syndrome population: 65 cases of sexually mature women underwent weight reduction surgery from January 2015 to June 2018, and for 35 of these cases we collected all clinical data including age, menstrual status, body mass index (BMI), waist-to-hip ratio (WHR), blood lipid level, homeostasis model assessment in insulin resistance (HOMA-IR) and free androgen index (FAI). Sixteen of these patients had menstrual disorder that was characterized by oligomenorrhea and their menstrual cycle was > 2 months or < 24 days before operation, while their menstrual cycle recovered approximately 1 month to one year after sleeve gastrectomy.
Results: The age of our 35 patients with metabolic syndrome was 15– 40 years; 19 cases were in the menstrual regularity group and 16 cases in the menstrual disorder group. On analysis of metabolic factors in the two groups, only BMI and FAI distribution in the two groups were statistically different, while lipid levels and insulin resistance levels for abnormal menstrual cycle were not statistically significant. The analysis of blood lipid components showed that high triglyceride levels and high cholesterol levels increased the occurrence of menstrual disorders.
Conclusion: BMI can be used as one of the important metabolic indicators of menstrual disorders in patients with metabolic syndrome. Excess androgen can increase the occurrence of menstrual disorders, leading to polycystic ovarian syndrome (PCOS). Although insulin resistance is universal in patients with metabolic syndrome, it is not a specific factor that affects menstrual cycle. Hyperlipidemia, especially triglyceride composition, may be one of the driving factors of menstrual disorder.
Keywords: sleeve gastrectomy, metabolic syndrome, menstrual cycle, hyperlipidemia
Introduction
Sleeve gastrectomy (LSG) is the most important operation for the treatment of obesity and type 2 diabetes.1 Metabolic syndrome (MS) associated with obesity, such as type 2-diabetes, fatty liver, hypertension, hyperglycemia and hyperlipidemia, can be effectively treated.2 As a clinical syndrome of metabolic syndrome in females, polycystic ovary syndrome (PCOS) has been unclear for a long time. Most studies have confirmed that insulin resistance-dominated glucose metabolism disorders play an important role in the occurrence and development of PCOS.3 However, the importance and necessity of insulin resistance therapy (such as metformin) has not been found in the efficacy analysis, and no independent treatment has been shown to be effective in regulating menstrual cycle.4 Obesity is the main clinical manifestation of dyslipidemia, which plays an important role in PCOS patients. Improving lifestyle and controlling body weight can improve the clinical symptoms of PCOS and improve the menstrual cycle to a certain extent, and this clinical effect has been confirmed by the literature.5 But the components of blood lipids that affect the adjustment of menstrual cycle have not been reported.
In this study, we selected a typical metabolic syndrome population: sexually mature women who underwent weight loss surgery. Firstly, the patients diagnosed with metabolic syndrome have three major pathological links of PCOS: androgen, hyperlipidemia and insulin resistance, which could be important for the progress of PCOS.6 Secondly, not all patients have abnormal menstrual cycle, but the proportion of patients with abnormal menstrual cycle is high, which can be analyzed as typical cases. Finally, the level of glucose and lipid metabolism were improved in varying degrees after weight-loss surgery. The menstrual cycle could be significantly recovered by more than 90%, but the serum androgen concentration was not significantly decreased. This conclusion can be used to analyze the possible proportion of glucose and lipid metabolism in improving menstrual cycle.
Materials and Methods
Study Design and Clinical Data Collection
From January 2015 to June 2018, 65 cases of sexually mature women underwent sleeve gastrectomy due to severe obesity and metabolic syndrome, in the Department of Gastroenterology, the First Affiliated Hospital of Chongqing Medical University, China. Among them, 28 cases had menstrual cycle disorder (menstrual cycle length > 2 months or < 24 days) before operation, and 24 cases recovered their menstrual cycle without sex hormone treatment within 1 year after operation. We collected their body mass index (BMI), waist-to-hip ratio (WHR), blood lipid level, free androgen index (FAI), total cholesterol (TC) and triacylglycerol (TG), which were measured by fully automatic biochemical analyser Alcyon300, fasting blood-glucose (FPG), fasting insulin (FINS) measured by enzyme immune chemical radiation assay, and calculated their homeostasis model assessment in insulin resistance (HOMA-IR = fasting glucose*insulin/22.5). Among them, 16 cases with menstrual cycle disorder and complete clinical and sufficient follow-up data constituted the experimental group, while 19 cases were chosen as control group with regular cycle and complete data (see Figure 1). Each patient’s results were compared at three points: before surgery, 6 months and 12 months after surgery.
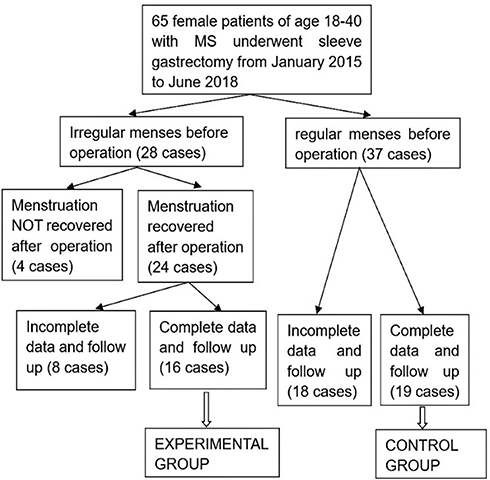 |
Figure 1 Patient recruitment and grouping process. |
All effective follow-up patients gave informed consent to this clinical retrospective analysis through the Ethics Committee of First Affiliated Hospital of Chongqing Medical University (number 2020–636). Reviewed by the Ethics Committee, the research program and informed consent form and other information submitted by the project meet the requirements of medical ethical principles and the Helsinki Declaration; the experimental design has scientific basis and there is no unnecessary risk to the subjects, and the safety and privacy of the subjects are given a maximum of protection. Approval was received for the implementation of the project according to the predetermined plan.
We confirm that our study was approved by the Ethics Committee of the First Affiliated Hospital of Chongqing Medical University, and complied with the Declaration of Helsinki. We confirm that all participants provided informed consent to participate.
Statistical Analysis
Statistical analysis was performed on SPSS 23. Shapiro–Wilk tests were used to test whether there was a normal distribution of our quantitative variables. Comparison of variables with a normal distribution was performed by parametric Student’s t-test, continuous variables were presented as n ± SD. Parameters that did not fit normal distribution were analyzed using a median (Me) and an interquartile range and the Mann–Whitney U-test. Qualitative variables were analyzed with chi-square test. P < 0.05 indicated that there was statistical significance.
Result
The Differences of BMI, WHR, Blood Lipid and Blood Glucose Between the Two Groups
Sixteen women with abnormal menstrual cycle and 19 women with normal menstrual cycle were selected. The metabolic indexes of the two groups, including BMI, WHR, FAI, HOMA-IR, TC and TG, were compared (Table 1). There were significant differences in BMI between the two groups (F 8.519, P < 0.05), and the analysis of variance of FAI was statistically significant (F 5.994, P < 0.05), but there was no difference in the mean value (P > 0.05). There was no significant difference in the other four indexes of WHR, HOMA-IR, TC and TG between the two groups. It shows that the disorder of menstrual cycle can be measured by BMI, which is related to hyperandrogenemia. But it has no direct correlation with insulin resistance and hyperlipidemia.
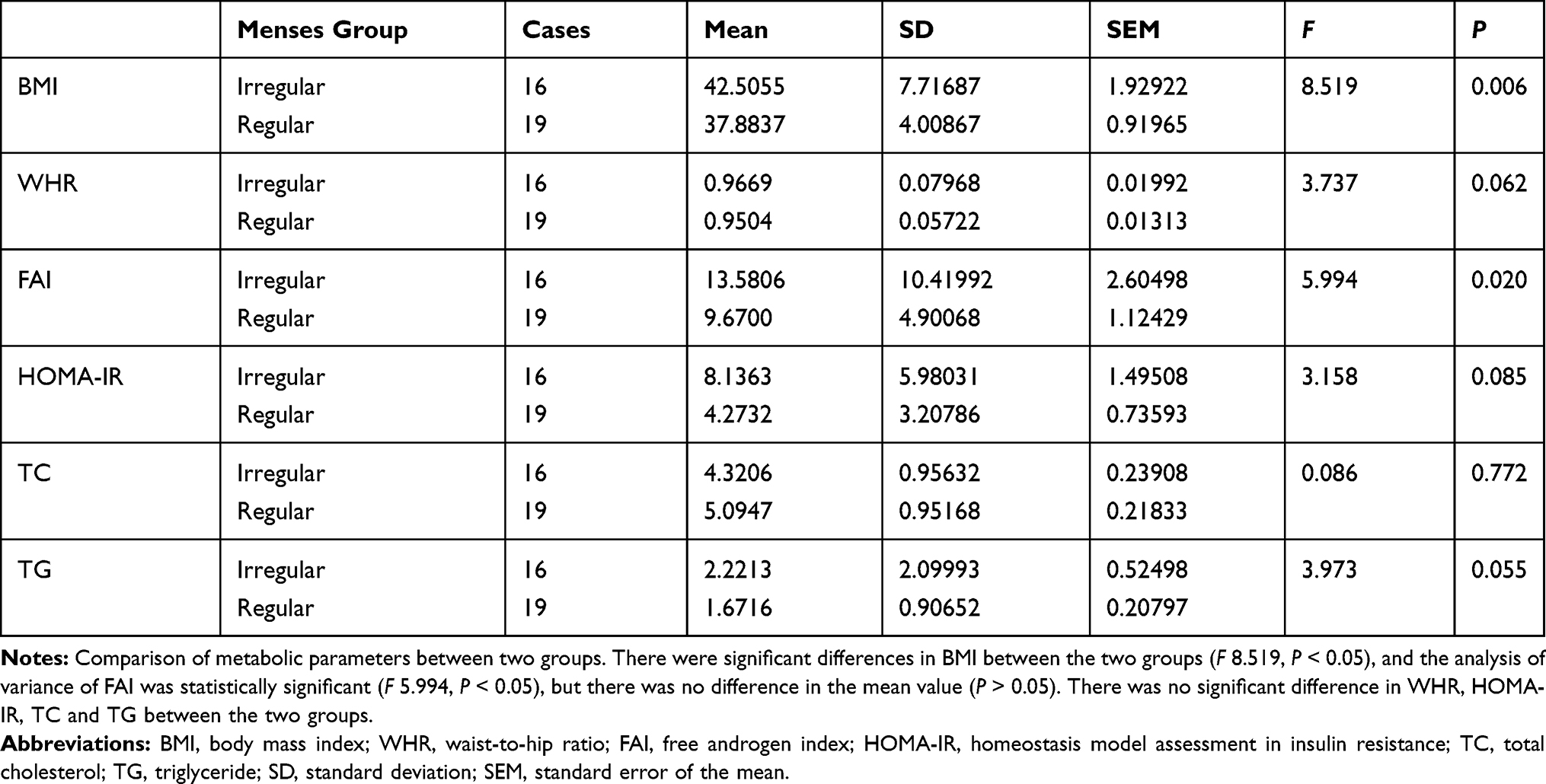 |
Table 1 Correlation of Glucose and Lipid Metabolism Parameters and Menstrual Cycle |
The Influence of Total Dyslipidemia and Dyslipidemia on Menstrual Regulation
Hyperlipidemia is mainly composed of serum cholesterol and triglyceride levels. There is no common phenomenon in the distribution of all patients. We investigated whether there is statistical difference in the number of menstrual disorders between the hyperlipidemia group (including high cholesterol and high triglyceride) and the normal blood lipid group. The results showed that there was no significant difference between menstrual disorder and dyslipidemia (Table 2).
 |
Table 2 Chi-Square Test for Menstrual Cycle and Hyperlipidemia |
We carried out a stratified analysis of 23 patients with hyperlipidemia, through hypercholesterolemia and hypertriglyceridemia, to count the number of patients with menstrual disorder. The results showed that the proportion of menstrual disorder in the high triglyceride group was more than 50%, reaching 53.85%, while that in the high cholesterol group was only 20%, which was statistically significant. It is suggested that triglyceride levels may play an important role in the regularity of the menstrual cycle; as possible metabolic factors they affect the menstrual cycle (Table 3).
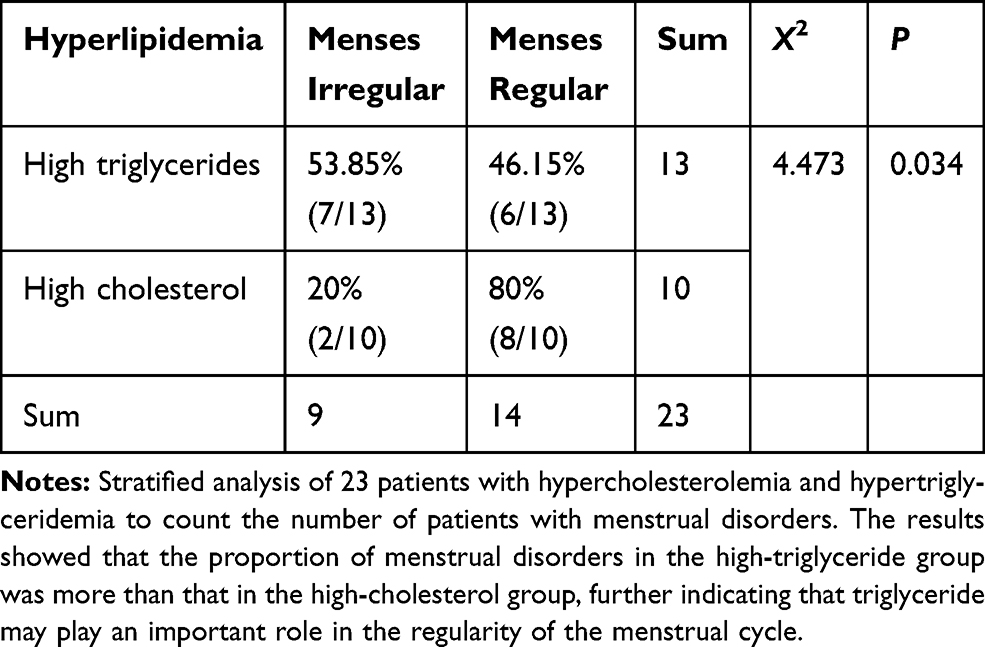 |
Table 3 Chi-Square Test of Four Tables for Hyperlipidemia and Menstrual Cycle Disorder |
Discussion
Polycystic ovary syndrome (PCOS) is the most common female disease which combines irregular menstrual cycle and metabolic syndrome, and also it is the most common cause of menstrual disorders and infertility in adolescent and reproductive age women. Its pathological mechanisms include hyperandrogenemia, insulin resistance and hyperlipidemia.7 In the 16 cases that had menstrual cycle disorder with complete clinical data, 10 cases had hyperandrogenism (TT≥0.5ng/mL in our hospital) and were diagnosed with PCOS, and 6 cases only had irregular menstrual cycle. The concentration of androgen can regulate menstrual cycle, but ovulation cannot be restored during treatment.8 At the same time, once the drug is stopped, menstrual disorder will return, with no long-term treatment effect. Metformin, which can improve insulin resistance, has been proved to be an adjuvant therapy for ovulation induction and androgen reduction, but cannot completely regulate the menstrual cycle.9 Lipid-lowering drugs have been proved to improve glucose and lipid metabolism in obese patients with PCOS, and can assist in improving ovulation induction effect.10 It is difficult to achieve clinical effect with a single treatment for the three major pathological parts.
For PCOS patients, the first recommendation is to adjust lifestyle, namely introduce proper exercise and reasonable diet structure, which is beneficial to long-term management of menstruation. Insisting on exercise and a reasonable three-meal diet can regulate menstrual cycle, to some extent; it is no less effective than drug treatment.11 Therefore, glucose and lipid metabolism has a definite effect on the adjustment of menstrual cycle, and the recovery degree of metabolic syndrome can also be used as one of the evaluation criteria for the efficacy of PCOS.
In this clinical trial we found that: insulin resistance in the two groups was not significantly different, that is, the recovery of menstrual cycle after surgery and the insulin resistance level are not significantly correlated. In the hyperlipidemia group, more patients had irregular menstruation, and after the blood lipid level returned to normal, the natural recovery rate of menstrual cycle was the highest. It is suggested that the components of blood lipids may be used as a metabolic index for the recovery of menstrual cycle.
Cholesterol and triglyceride are the two most important components of blood lipids. Cholesterol has the function of synthesizing hormone.12 The main physiological function of triglyceride is to provide a necessary heat source for human life activities. When triglyceride is absorbed by the human body, it will combine with lipoprotein to form chylous particles, which are mainly stored in the subcutaneous and visceral adipose tissue around the human body, and provide heat for the human body at any time. According to the statistical results, triglyceride is more important than cholesterol in regulating menstrual cycle.
Triglycerides exist in the body as a form of heat storage. When PCOS patients adjust their lifestyle and exercise actively,13 they consume excess fat, reduce BMI and also reduce the concentration of triglycerides in serum, thus partially improving the menstrual cycle. This clinical inference needs to be further confirmed by basic research.
As a specific manifestation of metabolic syndrome in ovarian dysfunction, the disorder of menstrual cycle is the main goal of PCOS management in clinical, and also the main appeal of patients. As a metabolic syndrome, its treatment is also a long-term management process. In clinical practice, if we improve glucose and lipid metabolism and adjust the level of key metabolic factors, we can achieve the goal of regulating menstrual cycle. This is undoubtedly the most comprehensive treatment for patients and can prevent long-term complications. What role does glucose and lipid metabolism play in regulating menstrual cycle, one relationship is conducive to the effective guidance of follow-up treatment.
Acknowledgments
The authors thank professor Jun Zhang and MengHua Zen, Department of Gastroenterology, the First Affiliated Hospital of Chongqing Medical University for sharing the data needed for the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding supported.
Disclosure
The authors declare that there is no conflict of interest.
References
1. Beydoun HA, Beydoun MA, Hossain S, et al. Patterns of bariatric surgeries among U.S. women diagnosed with polycystic ovarian syndrome. J Womens Health (Larchmt). 2020;29(4):585–595. doi:10.1089/jwh.2019.7947
2. Yheulon CG, Millard AJ, Balla FM, et al. Laparoscopic sleeve gastrectomy outcomes in patients with polycystic ovary syndrome. Am Surg. 2019;85(3):252–255. doi:10.1177/000313481908500327
3. Pergialiotis V, Trakakis E, Chrelias C, et al. The impact of mild hypercholesterolemia on glycemic and hormonal profiles, menstrual characteristics and the ovarian morphology of women with polycystic ovarian syndrome. Horm Mol Biol Clin Investig. 2018;34(3). doi:10.1515/hmbci-2018-0002
4. De Sousa SM, Norman RJ. Metabolic syndrome, diet and exercise. Best Pract Res Clin Obstet Gynaecol. 2016;37:140–151. doi:10.1016/j.bpobgyn.2016.01.006
5. Khorshidi A, Azami M, Tardeh S, et al. The prevalence of metabolic syndrome in patients with polycystic ovary syndrome: a systematic review and meta-analysis. Diabetes Metab Syndr. 2019;13(4):2747–2753. doi:10.1016/j.dsx.2019.06.008
6. Li J, Wu Q, Wang CC, et al. Endocrine characteristics, body mass index and metabolic syndrome in women with polycystic ovary syndrome. Reprod Biomed Online. 2019;39(5):868–876. doi:10.1016/j.rbmo.2019.06.014
7. Otaghi M, Azami M, Khorshidi A, et al. The association between metabolic syndrome and polycystic ovary syndrome: a systematic review and meta-analysis. Diabetes Metab Syndr. 2019;13(2):1481–1489. doi:10.1016/j.dsx.2019.01.002
8. Jun TJ, Jelani AM, Omar J, et al. Serum anti-müllerian hormone in polycystic ovary syndrome and its relationship with insulin resistance, lipid profile and adiponectin. Indian J Endocrinol Metab. 2020;24(2):191–195. doi:10.4103/ijem.IJEM_305_19
9. Behboudi-Gandevani S, Amiri M, Bidhendi YR, et al. The risk of metabolic syndrome in polycystic ovary syndrome: a systematic review and meta-analysis. Clin Endocrinol (Oxf). 2018;88(2):169–184. doi:10.1111/cen.13477
10. Hallajzadeh J, Khoramdad M, Karamzad N, et al. Metabolic syndrome and its components among women with polycystic ovary syndrome: a systematic review and meta-analysis. J Cardiovasc Thorac Res. 2018;10(2):56–69. doi:10.15171/jcvtr.2018.10
11. Skiba MA, Islam RM, Bell RJ, et al. Understanding variation in prevalence estimates of polycystic ovary syndrome: a systematic review and meta-analysis.Hum. Reprod Update. 2018;24(6):694–709.
12. Satitpatanapan P, Jaruratanasirikul S, Sriplung H. Menstrual cycle, reproductive function, body mass index, and metabolic profiles of women with former central precocious puberty: 10–20-year longitudinal cohort study in southern Thailand. J Pediatr Endocrinol Metab. 2020;33(7):933–940. doi:10.1515/jpem-2020-0019
13. Kyrkou G, Trakakis E, Attilakos A, et al. Metabolic syndrome in Greek women with polycystic ovary syndrome: prevalence, characteristics and associations with body mass index. A prospective controlled study. Arch Gynecol Obstet. 2016;293(4):915–923. doi:10.1007/s00404-015-3964-y
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.