")
Back to Journals » Infection and Drug Resistance » Volume 15
Correlation Between Drug Resistance and Virulence of Candida Isolates from Patients with Candidiasis
Authors Yang Z, Zhang F , Li D, Wang S, Pang Z, Chen L, Li R, Shi D
Received 3 September 2022
Accepted for publication 23 November 2022
Published 15 December 2022 Volume 2022:15 Pages 7459—7473
DOI https://doi.org/10.2147/IDR.S387675
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Suresh Antony
Zhiya Yang,1,* Fangfang Zhang,2,* Dongmei Li,3 Sisi Wang,1 Zhiping Pang,1 Liu Chen,1 Renzhe Li,4 Dongmei Shi1,5
1The Laboratory of Medical Mycology, Jining No.1 People’s Hospital, Jining, Shandong, 272111, People’s Republic of China; 2Department of Dermatology, Jining Dermatosis Prevention and Treatment Hospital, Jining, Shandong, 272000, People’s Republic of China; 3Department of Microbiology & Immunology, Georgetown University Medical Center, Washington, DC, 20057 USA; 4The Laboratory of Clinical Medicine, Jining No.1 People’s Hospital, Jining, Shandong, 272111, People’s Republic of China; 5Department of Dermatology, Jining No.1 People’s Hospital, Jining, Shandong, 272001, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Dongmei Shi, The Laboratory of Medical Mycology and Dermatology Department of Jining No.1 People’s Hospital, Shandong, 272011, China, Tel +86 537-6051008, Email [email protected] Renzhe Li, Clinical Laboratory of Jining No.1 People’s Hospital, 272111, People’s Republic of China, Tel +86 13563704987, Email [email protected]
Purpose: This article aims to provide a theoretical basis for new or adjuvant strategies to facilitate the early diagnosis and treatment of candidiasis and to determine if drug-resistant Candida would affect virulence.
Patients and Methods: Our strains were collected from patients diagnosed with candidiasis in our hospital. The strains were identified by MALDI-TOF system and ITS sequencing. Antifungal sensitivity testing in vitro was performed to evaluate susceptibility of these isolates to current widely used antifungal drugs. The Galleria mellonella larvae model infected by Candida spp. was used to compare the virulence of drug-resistant and susceptible Candida spp.
Results: A total of 206 Candida strains were collected from clinical specimens. Candida albicans was the most common species among them, and was predominantly isolated from male patients aged over 40 years in ICU environments suffering from pulmonary and/or cerebral conditions. The accuracy rate of MALDI TOF-MS identification was 92.72% when compared with ITS sequencing as the standard method. Most Candida species, except for C. tropicalis which showed high resistance to micafungin, showed high susceptibilities to voriconazole, itraconazole, amphotericin B and micafungin but were highly resistant to terbinafine. For each specific Candida species, the G. mellonella larvae model revealed that the virulence of drug-resistant Candida isolates did not markedly differ from that of the drug-susceptible isolates, however, the virulence was dose-dependent on inoculated fungal cells in this model.
Conclusion: The possibility of Candida infection should not be neglected in patients at critical care hospital settings and C. albicans is the most common causative agent. MALDI-TOF MS has the advantages of rapidity and high accuracy, and should be a preferred method for identification of Candida spp. in a clinical laboratory. Voriconazole, itraconazole, amphotericin B and micafungin can still be recommended as the first line antifungals to treat candidiasis.
Keywords: Candida, antifungal susceptibility testing, fungal infection, MALDI-TOF MS
Introduction
Fungal infections increased significantly in the past few decades, and are now responsible for over 1.5 million deaths globally per year. These infections occur primarily in hosts with a history of overuse of broad-spectrum antibiotics, hormones or immunosuppressive agents, or having a history of invasive treatment.1 The yeasts of Candida species (spp.) are the most common pathogen in fungal infections and also one common cause of nosocomial infections.2 In Europe, the genus Candida ranks in the top ten most common nosocomial blood pathogens with a reported annual incidence of 1.9~4.8 per 100,000 persons and is the fourth of most common hospital-acquired bloodstream infection pathogens in the United States.3 Today, the global prevalence of candidemia is 6.9/1000 persons4 and approximately 250,000 new cases of IC are reported per year, of which more than 50,000 result in death, although others have reported a mortality rate of up to 60%.5–7
There are more than 15 species of Candida spp. identified as human pathogens.5,8 According to many worldwide surveys, Candida albicans (C. albicans) is still the most common causative agent of IC,1,9 although the number of non-albicans Candida (NAC) species such as Candida glabrata (C. glabrata), Candida tropicalis (C. tropicalis) and Candida parapsilosis (C. parapsilosis) have been increasing significantly. With the widespread and long-term use of broad-spectrum antibiotics, the likelihood of resistance in Candida spp. is quickly increasing year by year. Antifungal susceptibility tests are still widely used for guiding empirical treatment in clinics.10 Since the susceptibility of different species to antifungal drugs varies significantly,11 this fact underscores not only the importance of accurate identification of the pathogens12–14 but also suggests our obligations to test all Candida strains isolated from cases of candidiasis.15
Methods for identifying yeast species from clinical specimens have improved significantly in the past decades,2 with emphasis on developing a rapid, economical and accurate technology for identification of Candida species. Traditional methods based on the morphological and physiological characteristics of the species are time-consuming and only moderately accurate,16 and yet are routinely used by most laboratories despite these drawbacks.17 In recent years, molecular identification methods have been explored for developing a fast and accurate diagnosis in clinical laboratories for microbial infections. Like other fungal pathogens, a PCR-based DNA sequencing technique has been carried out for Candida species identification. The second diagnostic method is using matrix-assisted laser desorption/ionization-time-of-flight (MALDI-TOF) mass spectrometry (MS)-based strategies. This technique identifies the pathogenic organisms through their protein profiles18 and specimen preparation for MALDI-TOF analysis can be simply extracted from agar plate.19,20 As PCR-based diagnosis requires DNA extraction, PCR amplification and sequencing, MALDI-TOF MS technology should have more advantages than the DNA-based method for a rapid identification of Candida species.
The Galleria mellonella (G. mellonella) model has been widely used in the study of fungal infections, including Candida infections. In this invertebrate model of G. mellonella, fungal virulence and efficacy and antifungal resistance are studied.21–23 Because of the structural and functional similarities between the immune systems of insects and the innate immune response of mammals, this larva is seen as an effective and useful model for evaluating the virulence of other human pathogens.24 Through this model, evaluation of drug resistance, the virulence of drug-resistant strains and the efficacy of antifungal drugs are expected to be more fruitful than those the classical vertebrate model. In this study, the G. mellonella larvae model was used to evaluate the virulence of our collected drug-resistant strains from clinical specimens. The purpose of this study was to explore the epidemiological, mycological and virulent characteristics of drug-sensitive and drug-resistant Candida spp., which we hoped to provide useful information in the diagnosis and treatment of candidiasis.
Materials and Methods
Study Population Selection
A total of 206 strains from 206 patients were recruited in this study, which included 55 yeast isolates from clinical specimens collected from June 2019 to June 2021 and 151 stored strains of 151 patients. All these isolates were collected from Jining No.1 People’s Hospital. All strains were cultured on Sabouraud’s dextrose agar (SDA, Oxoid, UK) and preserved at the Laboratory of Clinical Medicine, Jining No.1 People’s Hospital. For each fungal isolate, the medical record of each patient was retrieved for further analysis. Inclusive criteria for recruiting cases followed the revised and updated consensus definitions of invasive fungal disease by yeasts that was published by the European Organization for Research and Treatment of Cancer and the Mycoses Study Group and Research Consortium (EORTC/MSG) in 2019.25 Specifically, patients were included if they were in-patients with comprehensive medical conditions and were clinically suspected to have invasive candidiasis; Candida spp. were successfully recovered from sterile specimens of each patient, including blood, central venous catheter (CVC) tips, cerebrospinal fluid (CSF), hydrothorax, ascites, synovial fluid, sterile tissue (eg, bone) and freshly placed (within 24 hours) drains such as abdominal drainage fluid, pleural drainage fluid, abscess drainage and bile; Candida spp. recovered from normally non-sterile materials of inpatients, such as sputum, bronchoalveolar lavage fluid (BALF) and urine were also included if clinically suspected IC patients responded to antifungal treatment well and failed to antibacterial treatments. All IC outpatients and inpatients with missing records or/and if they were infected with non-Candida yeast were excluded.
An identical Candida species from two concessive culture results within one month or by different Candida species within two weeks were considered as one episode of infection.
Data Collection
Patients’ records were reviewed to collect demographic information, hospitalized period, underlying diseases, infected sites, mycological results and antifungal therapies.
DNA Molecular Identification
DNA was extracted using the EZNA Fungal DNA Mini Kit (Omega bio-tek, USA). In brief, tissues were resuspended in a proprietary bead-containing solution and used lysis solution to break the cell wall. The lysed DNA were purified and finally washed with sterile water to obtain DNA. PCR reaction mixtures were carried out as previously described26 in a MyCycler thermal cycler (Bio-Rad). The PCR reaction was repeated three times. The molecular identification of Candida was performed by sequencing the internal transcribed spacer (ITS) region as follows: ITS1 (5′-TCCGTAGGTGAACCTGCGG-3′) and ITS4 (5′-TCCTCCGCTTATTGATATGC-3′) primers, next, using NCBI for sequence alignment to identify. The consensus sequences were annotated and deposited in the GenBank, and the accession numbers of the sequences were received.27
MALDI-TOF MS
A colony of yeast was picked using an inoculation loop and was dissolved in formic acid. One microliter of cell suspension was then added onto the MALDI plate, allowed to dry and then overlaid with the matrix solution consisting of 40 g of α-cyano-4-hydroxycinnamic acid (CHCA; Sigma-Aldrich, Buchs, Switzerland) in 33% ethanol, 33% deionized water, 33% acetonitrile (ACN; Sigma-Aldrich) and 3% trifluoroacetic acid (TFA). The mixture was then dried at room temperature. The MALDI plate was loaded onto the equipment for analysis.
Antifungal Susceptibility Testing In Vitro
Antifungal susceptibility tests were performed by broth microdilution method as described in the CLSI M27-Ed4 document.28 A series of conidial suspensions (two times of the final inoculums) in RPMI 1640 medium were obtained ranging from 0.5×105 to 2.5×105 CFU/mL. C. parapsilosis (ATCC 22019) was used in parallel as a quality control. Amphotericin B, micafungin, voriconazole, itraconazole and terbinafine (MedChemExpress company, America) were provided as clinical formulations. The drugs were serially diluted at two-fold in a 96-well plate with the same medium. The ranges of concentrations of these drugs were 0.0313~16 μg/mL for amphotericin B, 0.015~8 μg/mL for micafungin, 0.0313~16 μg/mL for voriconazole, 0.0313~16 μg/mL for itraconazole and 0.001~0.5 μg/mL for terbinafine. Antifungal drug dilutions were filled into columns 1 through 10 of each 96-well culture plate, column 11 as positive control without drug and column 12 serves as a negative control. The plates were stored at −80 °C and thawed on the day of the experiment.
Using G. mellonella Larvae to Construct Animal Model Infected with Drug-Resistant Candida Spp
Final sixth instar G. mellonella larvae were acquired from Tianjin Huiyude Biotechnology Company. Larvae of approximately 300–500 mg showing no discoloration were selected for the experiments. According to the results of the drug susceptibility test in vitro, 49 resistant strains (Table 1) were selected and used for the following virulence assay in G. mellonella. At the same time, 4 ATCC or CBS reference Candida strains (C1S: C. albicans, C2F: C. tropicalis, C4E: C. parapsilosis, C6G: C. glabrata) in Table 1 were used as controls. All strains were sub-cultured on SDA at 37 °C for 1 day before conidia were transferred into phosphate-buffered saline (PBS) and kept still for 3–5 minutes to allow the heavy particles to settle. The supernatant was then transferred to a new sterile tube and vortexed thoroughly. Spores were quantified with a hemocytometer (Burker-Turk). To confirm fungal viability and to exclude bacterial contamination, 50 μL of each suspension was cultured on blood agar and SDA for 1 week at 37 °C.
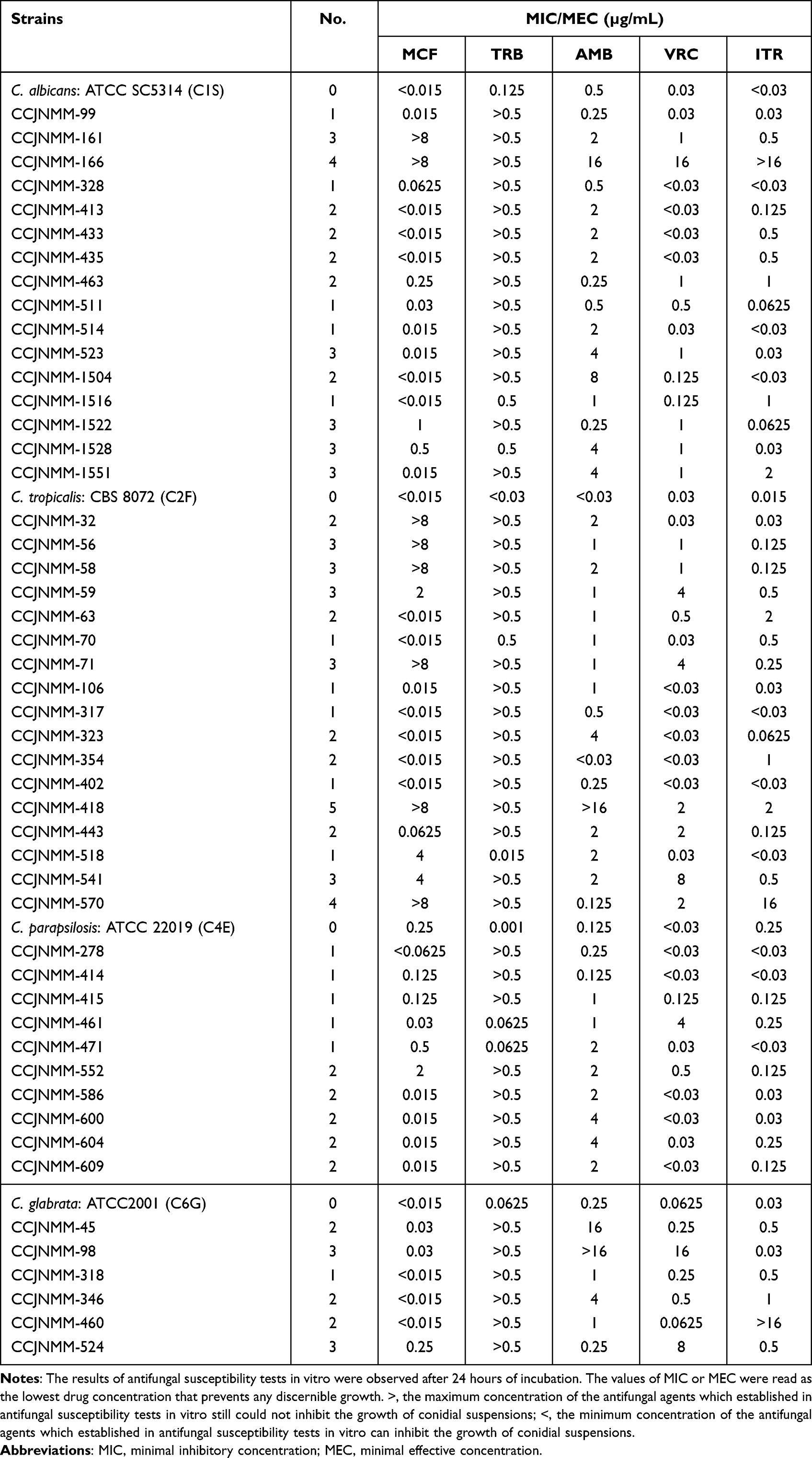 |
Table 1 The Results of the Drug Susceptibility Test of These 53 Strains |
Survival Assay in G. mellonella
Wax moth larvae killing assays were carried out as described previously.29 A total of 20 larvae were used for each testing group. Larvae were first infected each strain with different concentrations of conidia (5×106, 2.5×106, 1.25×106, 5×105 and 1×105 conidia per larva). Inoculation was performed by injecting 50 μL of the fungal suspension at the last left pro-leg with an insulin 29G U-100 needle (BD diagnostics, Sparks, USA). For control larvae, larvae were also pricked with the needle and injected with PBS. Larvae were checked daily for survival for 7 days at 37 °C.
Fungal Burden
The resistant strains were used to determine the fungal burden and measured as described earlier.30 Four larvae of G. mellonella from each group were sacrificed at 2 h, 24 h, 72 h and 168 h post infection. 10 μL body fluid of each larva was repeatedly taken and mixed evenly. SDA culture spreading with 20 μL of homogenized undiluted, 1:10-diluted and 1:100-diluted larva body fluid with PBS was incubated at 37 °C and the number of colonies forming units (CFUs) per larvae was determined after 24–48 h growth.
Statistical Analysis
All experiments were performed on three independent occasions. Data were collected and analyzed using GraphPad prism 8 and p<0.05 was considered to be significant.
Results
Patient Age and Gender
We collected data from 206 patients with suspected invasive candidiasis in this study. Among them, 61.65% (127/206) were male and 38.35% (79/206) were female (Figure 1A). Patient’s age ranged from less than 1 to 96 years old with the mean age at 68.64±16.98 and the median age at 71. Most patients were over 40 years old (95.63%, 197/206), of which over 60-year-old patients accounted for 72.82% (150/206) and over 60-year-old male patients accounted for 46.12% (95/206, 46.12%) (P=0.764) (Figure 1B).
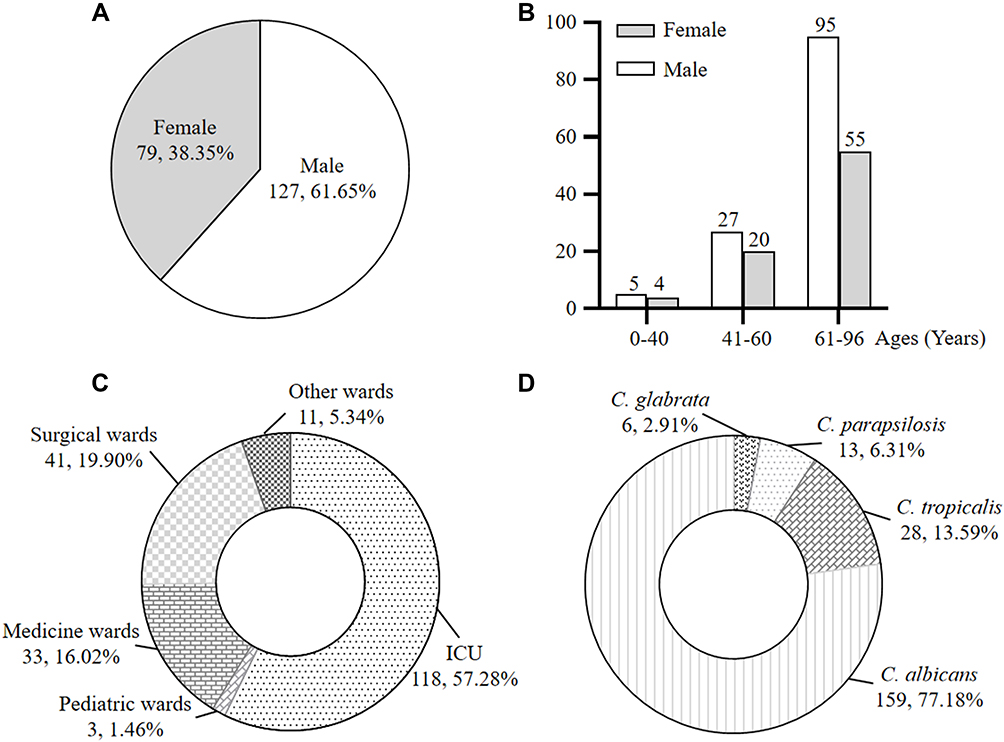 |
Figure 1 (A, B and C) Gender, ages and department distribution of 206 patients with Candida infection, respectively. (D) Distribution of Candida species in 206 clinical isolates. |
Underlying Diseases of IC Patients
The first admitting hospital units were different in these 206 patients. Of them, 118 patients (57.28%) were admitted in the ICU, accounting for more than half of patients (Figure 1C). The second group contains 41 patients (19.90) who stayed in general surgery unit. Thirty-three patients (16.02%) were recruited from the department of internal medicine and 3 patients (1.46%) were pediatric patients. The remaining 11 cases, accounting for a total of 5.34%, were collected from other hospital units.
The incidence of Candida infections was mainly found in patients with the diseases involved in lung (101 cases) and brain (75 cases) functions. The incidence of patients with a history of surgery or trauma was also high (65 cases). The patients with tumors accounted for 45 cases. Patients with two and more underlying diseases accounted for the majority of this studying population (67.48%, 139/206) by contrast to relatively few (32.52%, 67/206) patients with one single disease (Figure 2). For the patients recruited from the past, there were 12 patients were clinically diagnosed as IC, of which 10 cases were suffering from candidemia, and 1 case of each suffered from intra-abdominal candidiasis and bronchopulmonary candidiasis. The demographic data of these patients are shown in Table 2.
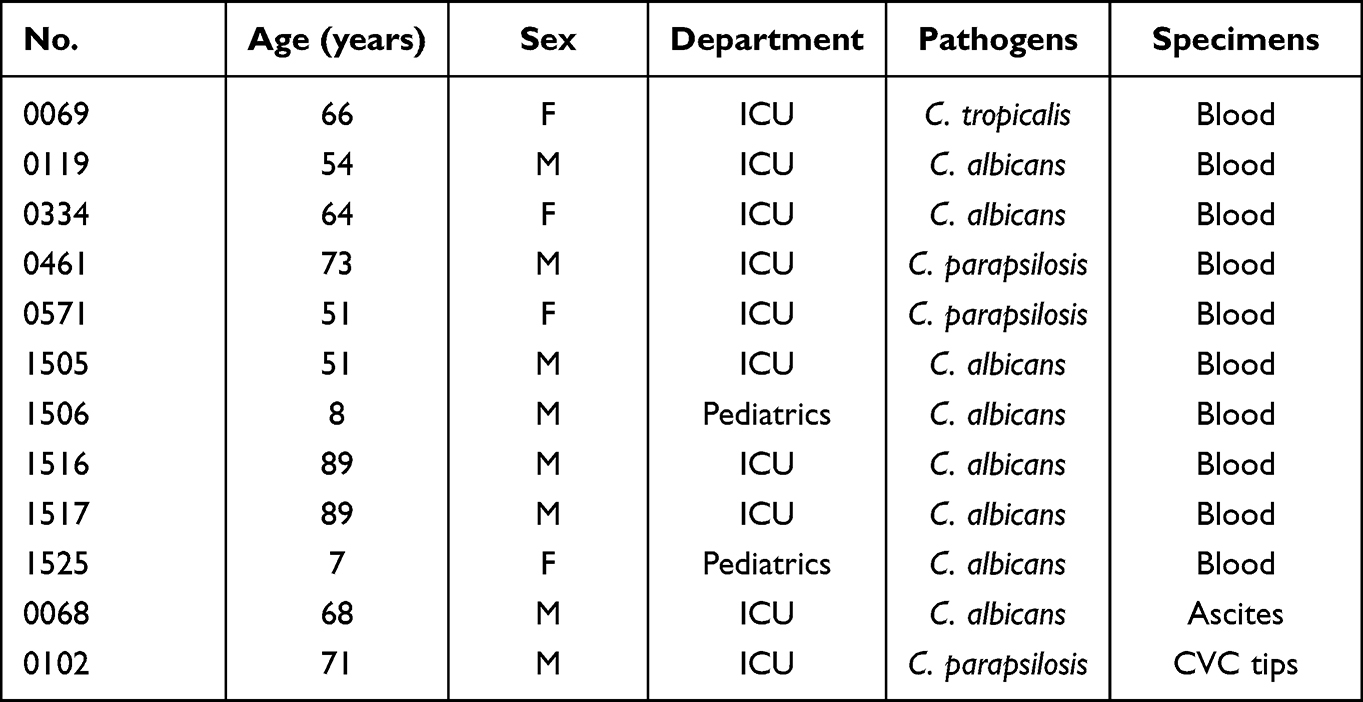 |
Table 2 The Distribution of IC |
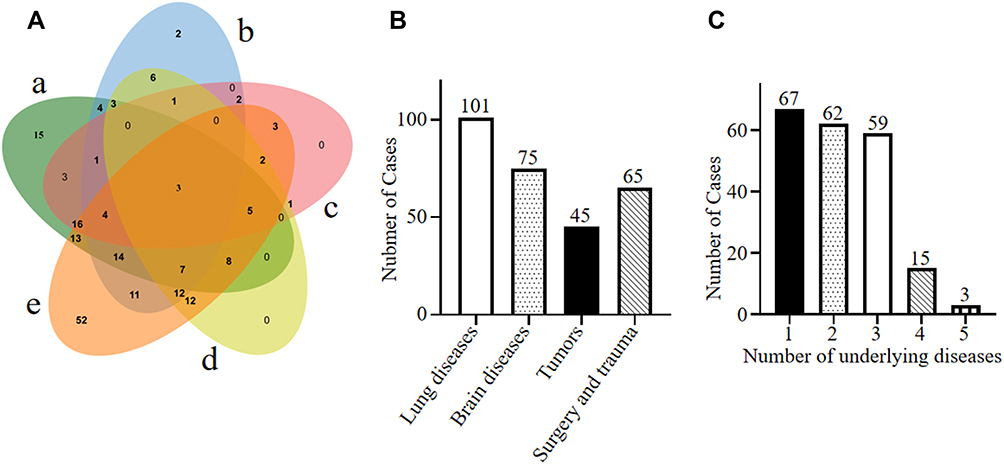 |
Figure 2 Distribution of diseases involved in 206 patients with Candida infection. (A) a Patients suffering from pulmonary conditions, b Patients suffering from cerebral conditions, c Patients with the history of tumor, d Patients with the history of surgery and trauma, e Patients with other conditions. (B) 206 patients were collected and among them, 101 patients suffered from pulmonary conditions (101/206, 49.03%), 75 patients suffered from cerebral conditions (75/206, 36.41%), 45 patients had the history of tumor (45/206, 21.84%) and 65 patients had the history of surgery and trauma (65/206, 31.55%). (C) The numbers of underlying diseases that patients suffered from. There were 67 patients (67/206, 32.52%) who suffered from 1 underlying disease, 62 patients (62/206, 30.10%) who suffered from 2 underlying diseases, 59 patients (59/206, 28.64%) who suffered from 3 underlying diseases, 15 patients (15/206, 7.28%) who suffered from 4 underlying diseases and 3 patients (3/206, 1.46%) who suffered from 5 underlying diseases. |
Taken together, these data demonstrated that the ICU patients, particularly aged with two and more medical conditions, are at high risk for invasive candidiasis.
Type of Specimens and Distribution of Candida Species
The specimen sources for Candida isolates from 206 patients are shown in Table 3. The most common specimen type was sputum, accounting for 61.65% (127/206), which was followed by variant body secretion (22.33%, 46/206), urine (7.28%, 15/206), blood (4.85%, 10/206) and others (3.88%, 8/206). Among these 206 clinical isolates, C. albicans was the most prevalent species, contributing to 77.18% (159/206) of the cases, followed by C. tropicalis (13.59%, 28/206), C. parapsilosis (6.31%, 13/206) and C. glabrata (2.91%, 6/206) (Figure 1D).
 |
Table 3 The Distribution of Specimen Sources of 4 Candida Species |
Molecular-Based Strain Identification Methods
Results of the ITS sequencing was used in this study to confirm Candida species in 206 clinical isolates. When compared with this gold standard method, the accuracy of MALDI-TOF MS reached to 92.72% of the DNA molecular identification method (Table 4). Both methods were performed with a pure culture on the SDA plates. This identification process of MALDI-TOF MS only took a few minutes to perform a species-level’s identification, which was much shorter than the process of DNA extraction, PCR and sequencing. Our results demonstrated that MALDI-TOF MS system is an effective and less time-consuming method for identification of Candida species.
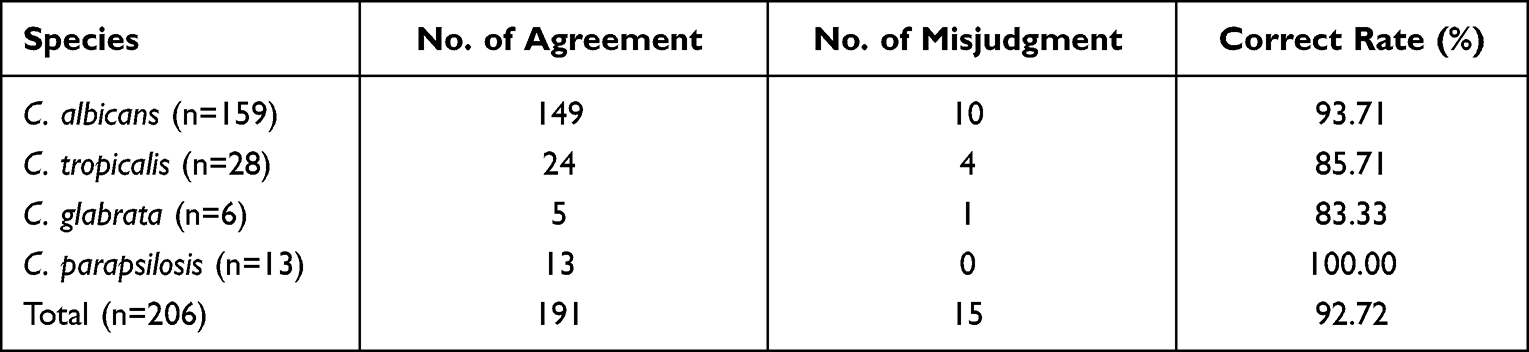 |
Table 4 Results of Two Identification Methods |
Resistance to Terbinafine Was High in Candida Isolates
Antifungal susceptibility test in vitro was used to evaluate the drug resistance in this cohort study. Our data showed that 17.61% (28/159) of C. albicans isolates were resistant to voriconazole, and 5.03% of C. albicans (8/159) were resistant to micafungin. Unexpectedly, there were 45.91% (73/159) of C. albicans resistant to amphotericin B. Resistance of C. albicans and other three species to all testing antifungals are shown in Table 5. We also noted that most of the Candida isolates except C. glabrata were non-WT to terbinafine and the resistant rates of C. albicans, C. tropicalis and C. parapsilosis to terbinafine were 88.05%, 82.14% and 61.54%, respectively.
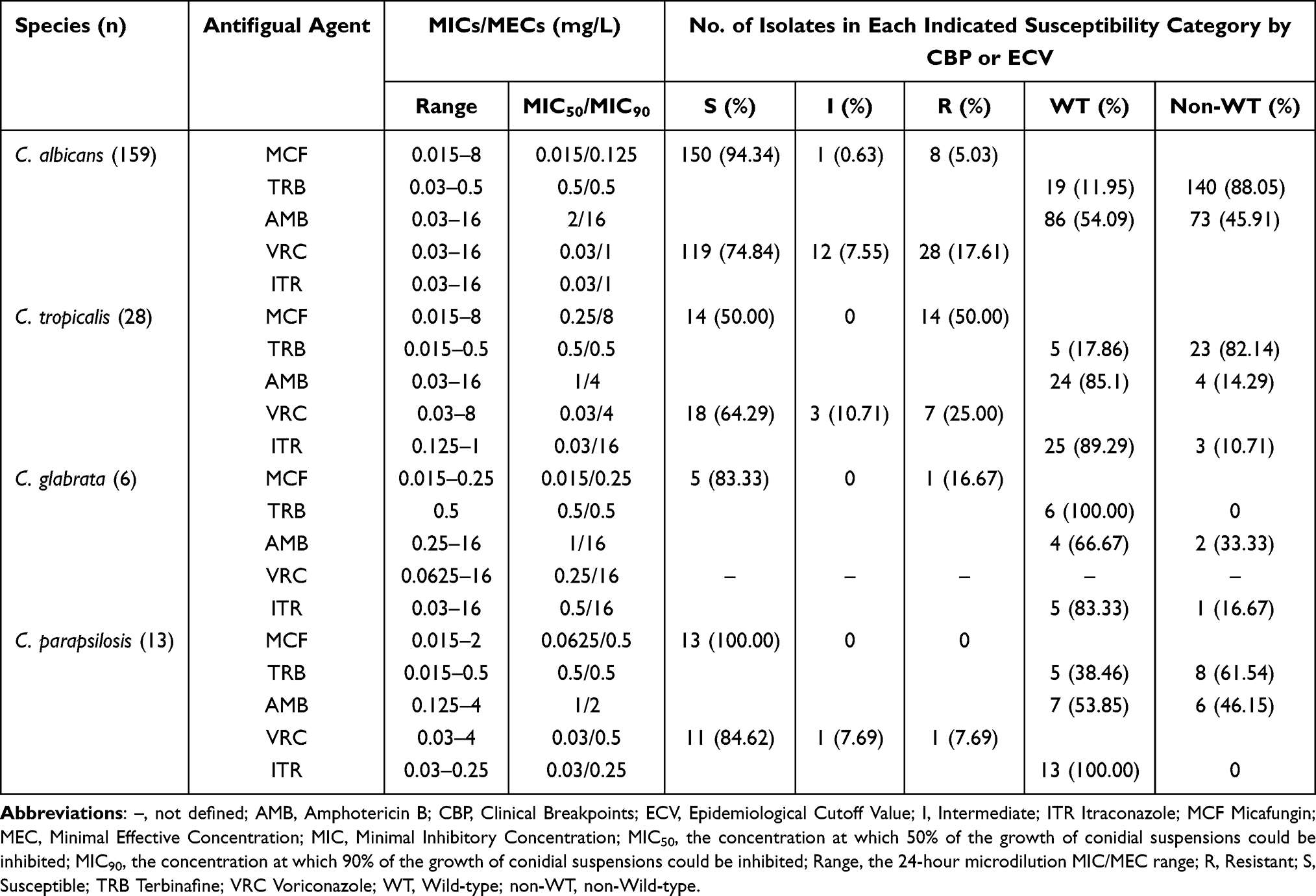 |
Table 5 Ranges of MIC/MEC, MIC50/MIC90 and Susceptibility Category of 5 Antifungal Agents Against 206 Candida Isolates |
Treatment and Follow-Up
Twelve patients who were clinically diagnosed as IC were treated with micafungin injection. After taking the antifungal micafungin treatment, the symptoms such as fever improved markedly the next day. Other suspected cases of Candida infection were not followed up, but the relationship between the bacteria and virulence was further studied.
Virulence in G. mellonella Model Was Dose-Dependent of Fungal Inoculums
To better estimate the virulence of Candida spp. in this animal model, we studied the fungal burdens of these clinical collected strains at different harvest points with different inoculated concentrations. We found that the fungal colonies were not high when sampling at 2 h. The yeast-like colonies occurred on the SDA plate at the first day (24 h) and continually increased in numbers by the third day (72 h) and diapered by the seventh day (168 h) regardless that the test strains were from patients with different underlying conditions or with different antifungal resistance patterns. Generally, the more the inoculums of the strains were, the more yeast-like colonies appeared (Figure 3).
 |
Figure 3 (A) Fungal burden at different times of the strain C1S showed that the fungal load was not high when sampling at 2 h, but on the 1st or 3rd day, the number of high-concentration spores injected into the SDA plate showed more yeast-like colonies. On the 7th day, fungal burden was not observed on the SDA plate. (B and C) C. albicans (C1S, 511 and 166) and C. tropicalis (C2F, 402 and 418) had the same trend as C1S. |
The G. mellonella larvae were then infected with Candida spp. to evaluate the virulence of the strains from different patients with different antifungal resistant pattern. The results showed that the mortality of G. mellonella larvae increased with initial concentration of inoculums, presenting in a dose-dependent manner (Figure 4). Again, there were no significant differences among mortalities (LD50 CFU) of G. mellonella larvae infected by strains having multiple-drug resistance (to 2, 3, 4, or 5 antifungals), single-drug resistance (to 1 antifungal) and susceptible standard strains (0 antifungal) (Figure 5). However, LD50 CFU values of C. glabrata were generally lower than those in C. albicans (Figure 5), while the CFU values of C. tropicalis and C. parapsilosis were more similar to C. albicans. Our results indicated that C. albicans, C. tropicalis and C. parapsilosis are more virulent than C. glabrata in this invertebrate animal model. Nevertheless, the resistance of Candida species had no correlation with their virulence.
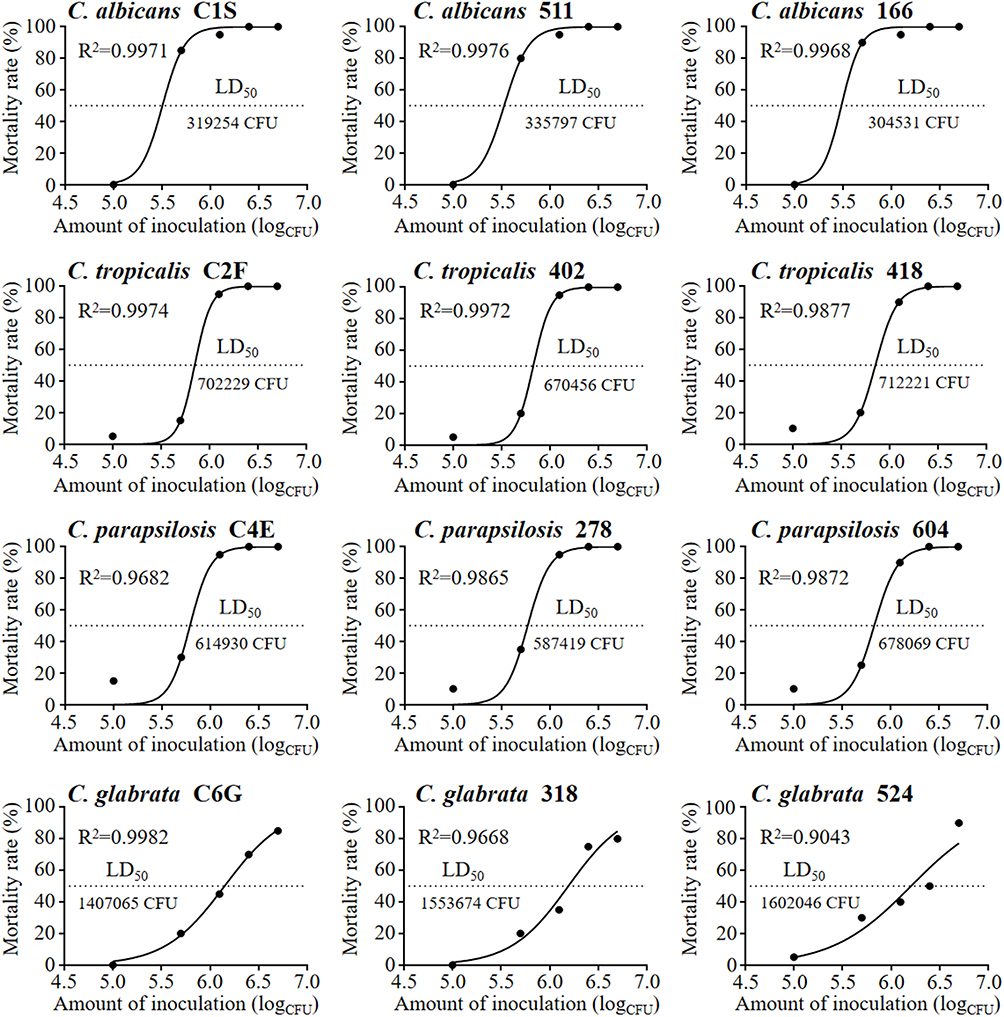 |
Figure 4 The mortality of G. mellonella larvae enhanced with strain concentration. The results of these following strains include C. albicans (C1S, 511 and 166), C. tropicalis (C2F, 402 and 418), C. parapsilosis (C4E, 278 and 604) and C. glabrata (C6G, 318 and 524). |
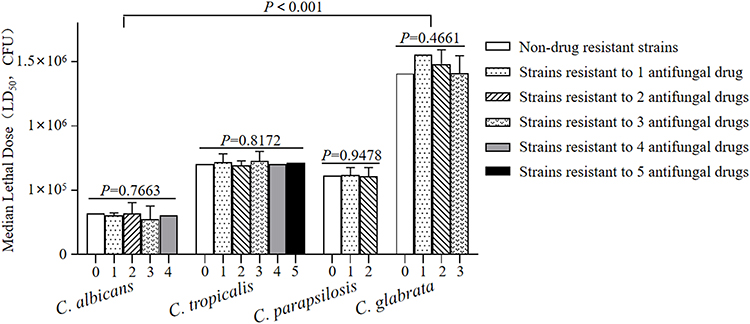 |
Figure 5 For C. albicans, C. tropicalis, C. parapsilosis or C. glabrata, there was no significant difference in median lethal dose (LD50) of G. mellonella larvae among infection models of multiple-drug resistant strains, single-drug resistant strains and non-drug resistant standard strains. But the difference among these four candida species was statistically significant (P<0.001). |
Discussion
Members of the genus Candida are commensal flora of humans, a frequent resident of the skin as well as gastrointestinal and genital tracts that can become pathogenic and cause severe invasive infections in susceptible (ie, elderly, hospitalized or immunosuppressed) patients.31 In the United States, candidiasis was reported to be one of the leading causes of healthcare-associated infections.32 In a ten-year retrospective study conducted in a tertiary hospital, patients aged over 65 accounted for more than half of a total of 183 invasive candidiasis (IC) episodes (54.1%, 99/183).6 Our data show a similar age effect for IC, even though our sample is smaller. Several explanations are possible here. First, the elderly are more likely to have impaired immune function and carry a higher Candida load even under normal commensal circumstances. Second, underlying diseases in these patients require a longer hospitalization or even a stay in the ICU. Third, the widespread use of broad-spectrum antibiotics and increasingly aggressive anti-inflammatory (and therefore immunosuppressive) treatments will promote fungal infections.33–35 Four, the treatment procedures associated with arteriovenous catheters, tracheal cannula, etc., are likely to promote biofilm formation and decrease antifungal susceptibility.36 All of these risk factors are potentially contributors to an increased candidiasis rate in these elderly patients – especially those admitted to the ICU.37–40 In this study, we found patients primarily hospitalized in the ICU accounting for 57.28% of the total number infected (118/206). We were unable to determine the size of the two base populations (ICU vs non-ICU), however, and so we cannot determine how great a risk factor for candidiasis placement in the ICU might be.
Although at least 15 distinct Candida species have been reported to cause human disease, more than 95% of reported cases of invasive candidiasis were confirmed to be caused by the following 6 species: C. albicans, C. glabrata, C. tropicalis, C. parapsilosis, C. krusei and, in some regions, C. auris.41 Epidemiological data also indicate that there has been a shift over the past decade to non-albicans species for candidiasis.42,43 In our 206 collections, we identified 4 species (C. albicans, C. tropicalis, C. parapsilosis and C. glabrata), in which the most commonly-found species was still C. albicans, which accounted for 77.18% of isolated strains. The dominance of C. albicans from our and other studies suggests that C. albicans is more pathogenic than other Candida species.4,44 Studies on virulence factors of C. albicans have found that many proteins and biological characters are required for its host invasion, including extracellular acid protease, adhesion, germ tube formation, hydrophobicity and other toxic factors.45 Owing to its stronger adherence capacity, C. albicans is found more often than other Candida species.46
The early detection of Candida is an indispensable prerequisite for proper treatment.47,48 In this study, the MALDI-TOF MS method had showed some advantages over the DNA-based PCR and sequencing method although the accuracy is slightly lower. However, since it is easy to operate and fast, the MALDI-TOF MS method is still a preferred method in clinical laboratories to identify Candida spp. For a PCR amplification procedure today, the fungal DNA must be extracted from yeast-like colonies in a culture medium; the subsequent PCR and sequencing then further delay the diagnosis despite offering better accuracy. On the other hand, specimen preparation for MALDI-TOF analysis can be simply extracted from agar plate.19,20 This greater ease of use in the MALDI-TOF MS method also shows an advantage over the PCR-based method in rapid identification of Candida.
In high antifungal use settings, others have noted an increasing number of Candida species resistant to first line antifungals such as azoles and echinocandins, and an increased clinical prevalence of multidrug-resistant isolates (eg, azole and echinocandin resistant C. glabrata) has also being identified.49 The emergence of these multidrug-resistant species eliminates almost all current treatment options. While we did not find multidrug-resistant strains in this study, we did find that most of our C. albicans isolates were susceptible to amphotericin B and voriconazole, which agrees with previous reports.50,51 Except for C. tropicalis which showed high resistance to micafungin, all other Candida strains were sensitive to micafungin. Non-C. albicans species in our collection are also susceptible to voriconazole, itraconazole, and amphotericin B but are highly resistant to terbinafine. Therefore, terbinafine should not be considered for the treatment of Candida-specific infectious diseases.
The ability to correctly identify pathogenic fungi, along with a better understanding of their pathogenicity and susceptibility to antifungals, is extremely important for the efficient management of appropriate prophylactics and therapies. Whether drug resistance affects virulence in Candida is still open to question, since it is well known that the etiological agent and its interaction with the host play an important role in the pathogenicity of Candida beyond “simple” virulence factors.52 Virulence factors such as adhesion to inert and biological substrates, germ tube, exoenzymes and biofilm formation are exhibited by Candida species and are important aspects of pathogen–host interaction to aid in colonization of host tissues, disease onset and the evasion of host defenses.53 Larvae of the greater wax moth G. mellonella are widely used for the study of pathogenesis and virulence mechanisms of various microbial pathogens54 due to the economic and ethical advantages and short lifespan. For Candida infections, Andrew M. Borman et al55 successfully used G. mellonella as an animal model to compare the pathogenicity of 19 multidrug-resistant Candida auris strains with other common pathogenic yeast species. They found that virulence did not differ significantly among strains exhibiting different antifungal susceptibility. There is also no correlation between drug resistance and virulence in our collection. We agree that the virulence of Candida has no obvious correlation with its drug resistance. The failure to treat an infection caused by drug-resistant Candida is then simply due to the proliferation of fungi while the antifungal drug fails to effectively inhibit growth. The overgrowth of fungi then aggravates the infectious course and often leads to patient death. Nevertheless, the relationship between the virulence and drug resistance of the Candida spp. needs further study including other resistant strains and different models.
In the end, the rapid detection of pathogenic Candida and determination of drug susceptibility are necessary steps to earlier antifungal intervention, which we expect will reduce antifungal resistance and save lives in clinical settings. In effect, this offers a somewhat chilling outlook, since there appears to be a point in time beyond which intervention is pointless, and so speed of detection and therapy remain paramount.
Data Sharing Statement
The original contributions presented in the study are included in the article/supplementary material; further inquiries can be directed to the corresponding authors.
Ethics Statement
The studies involving human participants were reviewed and approved by Medical Ethics Committee of Jining No.1 People’s Hospital (TRECKY2019-130). The study complied with the Declaration of Helsinki. The patients/participants provided their written informed consent to participate in this study.
Acknowledgments
We are extremely grateful to all the participants and their authorized relatives who participated in this study, as well as the entire psychiatric medical teams.
Funding
This work was supported in part by grants from the National Natural Science Foundation of China (NM 81773337), China Medical Fungi Alliance, (CMFA-2021-06). “Qihang” Plan of Jining No.1 People’s Hospital (2021-QHM-026).
Disclosure
The authors declare that they have no potential conflicts of interest to disclose in this work.
References
1. Lee Y, Puumala E, Robbins N., et al. Antifungal drug resistance: molecular mechanisms in Candida albicans and beyond. Chem Rev. 2021;121(6):3390–3411. doi:10.1021/acs.chemrev.0c00199
2. Neppelenbroek KH, Seó RS, Urban VM, et al. Identification of Candida species in the clinical laboratory: a review of conventional, commercial, and molecular techniques. Oral Dis. 2014;20(4):329–344. doi:10.1111/odi.12123
3. Cao B, Wang H, Wu L, et al. Epidemiological study of invasive nosocomial candidiasis in 2 teaching hospitals in Beijing. Zhonghua Yi Xue Za Zhi. 2008;88(28):1970–1973.
4. Pfaller MA, Diekema DJ. Epidemiology of invasive candidiasis: a persistent public health problem. Clin Microbiol Rev. 2007;20(1):133–163. doi:10.1128/CMR.00029-06
5. Guo LN, Yu SY, Xiao M, et al. Species Distribution and Antifungal Susceptibility of Invasive Candidiasis: a 2016-2017 Multicenter Surveillance Study in Beijing, China. Infect Drug Resist. 2020;13:2443–2452. doi:10.2147/IDR.S255843
6. Yang ZH, Song YG, Li RY, Ten-year Retrospective A. Study of Invasive Candidiasis in a Tertiary Hospital in Beijing. Biomed Environ Sci. 2021;34(10):773–788. doi:10.3967/bes2021.107.
7. Zeng ZR, Tian G, Ding YH, et al. Surveillance study of the prevalence, species distribution, antifungal susceptibility, risk factors and mortality of invasive candidiasis in a tertiary teaching hospital in Southwest China. BMC Infect Dis. 2019;19(1):939. doi:10.1186/s12879-019-4588-9.
8. Ken AB, Ma ZH, Xiong DQ, et al. Clinical features of invasive candidiasis and risk factors for Candida bloodstream infection in children: a multicenter study in Urumqi, China. Zhongguo Dang Dai Er Ke Za Zhi. 2017;19(4):414–418. doi:10.7499/j.issn.1008-8830.2017.04.011.
9. Asadzadeh M, Ahmad S, Al-Sweih N, et al. Rapid and Accurate Identification of Candida albicans and Candida dubliniensis by Real-Time PCR and Melting Curve Analysis. Med Princ Pract. 2018;27(6):543–548. doi:10.1159/000493426
10. Dagi HT, Findik D, Senkeles C, et al. Identification and antifungal susceptibility of Candida species isolated from bloodstream infections in Konya, Turkey. Ann Clin Microbiol Antimicrob. 2016;15(1):36. doi:10.1186/s12941-016-0153-1
11. Sanguinetti M, Posteraro B, Lass-Flörl C. Antifungal drug resistance among Candida species: mechanisms and clinical impact. Mycoses. 2015;58:2–13. doi:10.1111/myc.12330
12. Ruan SY, Huang YT, Chu CC, et al. Candida glabrata fungaemia in a tertiary centre in Taiwan: antifungal susceptibility and outcomes. Int J Antimicrob Agents. 2009;34(3):236–239. doi:10.1016/j.ijantimicag.2009.02.021
13. Silva S, Negri M, Henriques M, et al. Candida glabrata, Candida parapsilosis and Candida tropicalis: biology, epidemiology, pathogenicity and antifungal resistance. FEMS Microbiol Rev. 2012;36(2):288–305. doi:10.1111/j.1574-6976.2011.00278.x
14. Cleveland AA, Harrison LH, Farley MM, et al. Declining incidence of candidemia and the shifting epidemiology of Candida resistance in two US metropolitan areas, 2008-2013: results from population-based surveillance. PLoS One. 2015;10(3):e0120452. doi:10.1371/journal.pone.0120452
15. Hedayati MT, Tavakoli M, Zakavi F, et al. In vitro antifungal susceptibility of Candida species isolated from diabetic patients. Rev Soc Bras Med Trop. 2018;51(4):542–545. doi:10.1590/0037-8682-0332-2017
16. Relloso MS, Nievas J, Fares Taie S, et al. Evaluation of mass spectrometry: MALDI-TOF MS for fast and reliable yeast identification. Rev Argent Microbiol. 2015;47(2):103–107. doi:10.1016/j.ram.2015.02.004
17. Maldonado I, Cataldi S, Garbasz C, et al. Identification of Candida yeasts: conventional methods and MALDI-TOF MS. Rev Iberoam Micol. 2018;35(3):151–154. doi:10.1016/j.riam.2018.02.002
18. Croxatto A, Prodhom G, Hom G, et al. Applications of MALDI-TOF mass spectrometry in clinical diagnostic microbiology. FEMS Microbiol Rev. 2012;36(2):380–407. doi:10.1111/j.1574-6976.2011.00298.x.
19. Oviaño M, Rodríguez-Sánchez B. MALDI-TOF mass spectrometry in the 21st century clinical microbiology laboratory. Enferm Infecc Microbiol Clin. 2021;39(4):192–200. doi:10.1016/j.eimc.2020.02.027
20. Tsuchida S, Umemura H, Nakayama T. Current Status of Matrix-Assisted Laser Desorption/Ionization-Time-of-Flight Mass Spectrometry (MALDI-TOF MS) in Clinical Diagnostic Microbiology. Molecules. 2020;25:20. doi:10.3390/molecules25204775
21. Six A, Krajangwong S, Crumlish M, et al. Galleria mellonella as an Infection Model for the Multi-Host Pathogen Streptococcus Agalactiae Reflects Hypervirulence of Strains Associated with Human Invasive. Dis Virulence. 2019;10(1):600–609. doi:10.1080/21505594.2019.1631660
22. Maurer E, Hörtnagl C, Lackner M, et al. Galleria mellonella as a Model System to Study Virulence Potential of Mucormycetes and Evaluation of Antifungal Treatment. Med Mycol. 2019;57(3):351–362. doi:10.1093/mmy/myy042
23. de Castro Spadari C, Da Silva de Bastiani FWM, Pisani PBB, de Azevedo Melo AS, Ishida K. Efficacy of voriconazole in vitro and in invertebrate model of cryptococcosis. Arch Microbiol. 2020;202(4):773–784. doi:10.1007/s00203-019-01789-8
24. Ratcliffe NA. Invertebrate immunity--a primer for the non-specialist. Immunol Lett. 1985;10(5):253–270. doi:10.1016/0165-2478(85)90100-2
25. Donnelly JP, Chen SC, Kauffman CA, et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis. 2020;71(6):1367–1376. doi:10.1093/cid/ciz1008
26. Romeo O, Criseo G. First molecular method for discriminating between Candida africana, Candida albicans, and Candida dubliniensis by using hwp1 gene. Diagn Microbiol Infect Dis. 2008;62(2):230–233. doi:10.1016/j.diagmicrobio.2008.05.014
27. Abastabar M, Hosseinpoor S, Hedayati MT, et al. Hyphal wall protein 1 gene: a potential marker for the identification of different Candida species and phylogenetic analysis. Curr Med Mycol. 2016;2(4):1–8. doi:10.18869/acadpub.cmm.2.4.1
28. CLSI. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts.
29. Mesa-Arango AC, Forastiero A, Bernal-Martínez L, et al. The non-mammalian host Galleria mellonella can be used to study the virulence of the fungal pathogen Candida tropicalis and the efficacy of antifungal drugs during infection by this pathogenic yeast. Med Mycol. 2013;51(5):461–472. doi:10.3109/13693786.2012.737031
30. Kloezen W, van Helvert-van Poppel M, Fahal AH, et al. A Madurella mycetomatis Grain Model in Galleria mellonella Larvae. PLoS Negl Trop Dis. 2015;9(7):e0003926. doi:10.1371/journal.pntd.0003926
31. Bhattacharya S, Sae-Tia S, Fries BC. Candidiasis and Mechanisms of Antifungal Resistance. Antibiotics. 2020;9:6. doi:10.3390/antibiotics9060312
32. Soulountsi V, Schizodimos T, Kotoulas SC. Deciphering the epidemiology of invasive candidiasis in the intensive care unit: is it possible? Infection. 2021;49(6):1107–1131. doi:10.1007/s15010-021-01640-7
33. Wang SA, Jia JH, Bai FY. Candida alocasiicola sp. nov., Candida hainanensis sp. nov., Candida heveicola sp. nov. and Candida musiphila sp. nov., novel anamorphic, ascomycetous yeast species isolated from plants. Antonie Van Leeuwenhoek. 2008;94(2):257–265. doi:10.1007/s10482-008-9238-y
34. Alam MZ, Alam Q, Jiman-Fatani A, et al. Candida identification: a journey from conventional to molecular methods in medical mycology. World J Microbiol Biotechnol. 2014;30(5):1437–1451. doi:10.1007/s11274-013-1574-z
35. Ambaraghassi G, Dufresne PJ, Dufresne SF, et al. Identification of Candida auris by Use of the Updated Vitek 2 Yeast Identification System, Version 8.01: a Multilaboratory Evaluation Study. J Clin Microbiol. 2019;57(11):548. doi:10.1128/JCM.00884-19
36. Dekkers B, Veringa A, Marriott D, et al. Invasive Candidiasis in the Elderly: considerations for Drug Therapy. Drugs Aging. 2018;35(9):781–789. doi:10.1007/s40266-018-0576-9
37. Vincent JL, Rello J, Marshall J, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;302(21):2323–2329. doi:10.1001/jama.2009.1754
38. Cuenca-Estrella M, Kett DH, Wauters J. Defining standards of CARE for invasive fungal diseases in the ICU. J Antimicrob Chemother. 2019;74(Suppl2):ii9–ii15. doi:10.1093/jac/dkz038
39. Bassetti M, Giacobbe DR, Vena A, et al. Incidence and outcome of invasive candidiasis in intensive care units (ICUs) in Europe: results of the EUCANDICU project[J]. Crit Care. 2019;23(1):219. doi:10.1186/s13054-019-2497-3
40. Bassetti M, Azoulay E, Kullberg BJ, et al. EORTC/MSGERC Definitions of Invasive Fungal Diseases: summary of Activities of the Intensive Care Unit Working Group[J]. Clin Infect Dis. 2021;72(Suppl 2):S121–S127. doi:10.1093/cid/ciaa1751
41. McCarty TP, White CM, Pappas PG. Candidemia and Invasive Candidiasis[J]. Infect Dis Clin North Am. 2021;35(2):389–413. doi:10.1016/j.idc.2021.03.007
42. Pristov KE, Ghannoum MA. Resistance of Candida to azoles and echinocandins worldwide[J]. Clin Microbiol Infect. 2019;25(7):792–798. doi:10.1016/j.cmi.2019.03.028
43. Sadeghi-Ghadi Z, Vaezi A, Ahangarkani F, et al. Potent in vitro activity of curcumin and quercetin co-encapsulated in nanovesicles without hyaluronan against Aspergillus and Candida isolates[J]. J Mycol Med. 2020;30(4):101014. doi:10.1016/j.mycmed.2020.101014
44. Arendrup MC. Epidemiology of invasive candidiasis[J]. Curr Opin Crit Care. 2010;16(5):445–452. doi:10.1097/MCC.0b013e32833e84d2
45. Staniszewska M. Virulence Factors in Candida species[J]. Curr Protein Pept Sci. 2020;21(3):313–323. doi:10.2174/1389203720666190722152415
46. Lohse MB, Gulati M, Johnson AD, et al. Development and regulation of single- and multi-species Candida albicans biofilms[J]. Nat Rev Microbiol. 2018;16(1):19–31. doi:10.1038/nrmicro.2017.107
47. Delavy M, Dos Santos AR, Heiman CM, et al. Investigating Antifungal Susceptibility in Candida Species With MALDI-TOF MS-Based Assays[J]. Front Cell Infect Microbiol. 2019;9:19. doi:10.3389/fcimb.2019.00019
48. Meena S, Mohanty A, Kaistha N, et al. Comparative Assessment of Matrix-assisted Laser Desorption Ionization-time of Flight Mass Spectrometry (MALDI-TOF-MS) and Conventional Methods in the Identification of Clinically Relevant Yeasts[J]. Cureus. 2021;13(6):e15607. doi:10.7759/cureus.15607
49. Murphy SE, Drug Resistance BT. Novel Therapeutic Approaches in Invasive Candidiasis[J]. Front Cell Infect Microbiol. 2021;11:759408. doi:10.3389/fcimb.2021.759408
50. Mohammadi F, Ghasemi Z, Familsatarian B, et al. Relationship between antifungal susceptibility profile and virulence factors in Candida albicans isolated from nail specimens[J]. Rev Soc Bras Med Trop. 2020;53:e20190214. doi:10.1590/0037-8682-0214-2019
51. Nasri E, Fakhim H, Vaezi A, et al. Airway colonisation by Candida and Aspergillus species in Iranian cystic fibrosis patients. Mycoses. 2019;62(5):434–440. doi:10.1111/myc.12898
52. Fakhim H, Vaezi A, Javidnia J, et al. Candida africana vulvovaginitis: prevalence and geographical distribution. J Mycol Med. 2020;30(3):100966. doi:10.1016/j.mycmed.2020.100966
53. Mello VG, Escudeiro H, Weckwerth A, et al. Virulence Factors and Antifungal Susceptibility in Candida Species Isolated from Dermatomycosis Patients. Mycopathologia. 2021;186(1):71–80. doi:10.1007/s11046-020-00509-x
54. Cutuli MA, Petronio Petronio G, Vergalito F, et al. Galleria mellonella as a consolidated in vivo model hosts: new developments in antibacterial strategies and novel drug testing. Virulence. 2019;10(1):527–541. doi:10.1080/21505594.2019.1621649
55. Borman AM, Szekely A, Johnson EM. Comparative Pathogenicity of United Kingdom Isolates of the Emerging Pathogen Candida auris and Other Key Pathogenic Candida Species. mSphere. 2016;1(4):448. doi:10.1128/mSphere.00189-16
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.