")
Back to Journals » International Journal of Women's Health » Volume 10
Correlates of individual-level abortion stigma among women seeking elective abortion in Nigeria
Authors Oginni A , Ahmadu SK , Okwesa N, Adejo I, Shekarau H
Received 6 June 2017
Accepted for publication 14 December 2017
Published 12 July 2018 Volume 2018:10 Pages 361—366
DOI https://doi.org/10.2147/IJWH.S143388
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Ayodeji Oginni,1 Sikiratu Kailani Ahmadu,2 Nkiruka Okwesa,1 Isaac Adejo,3 Hauwa Shekerau3
1Research and Evaluation Unit, Ipas Nigeria, 2Maternal, Newborn, and Child Health Program (MNCH2), Ipas Nigeria, 3Program Unit, Ipas Nigeria, Abuja, Nigeria
Objective: This study aimed to measure individual-level abortion stigma (ILAS) and determine its correlates among women receiving safe elective abortion services.
Patients and methods: Data were collected from a cross-section of women who received safe elective abortion services in select intervention health facilities. Respondents were recruited through a self-selection sampling. ILAS was assessed using a 16-item scale (Cronbach’s alpha =0.9122). Respondents were categorized as high (summed score >40) or low ILAS (summed score ≤40) on a spectrum of a summed minimum score of 16 to a maximum score of 64. A log-binomial regression model was constructed to determine the ILAS correlates.
Results: Among 382 respondents, 43% expressed high ILAS. Women’s age and education, provider’s cadre and type of abortion procedure were significant correlates in the model. Older women (age 25–34 and age ≥35) were less likely (prevalence ratio [PR]=0.60 and 0.39, p<0.001) to express high ILAS than the younger women (age ≤24); those with higher educational status were more likely to express (PR=1.64, p<0.05) high ILAS than those with None/Primary education; those who had medical abortion were less likely (PR=0.54, p<0.01) to express high ILAS than those who had surgical abortion; and lastly, those who received care from midlevel providers were more likely (PR=1.31, p<0.05) to express high ILAS than those who received care from physicians.
Conclusion: High ILAS still exists among women accessing safe elective abortion care in Nigeria. Therefore, interventions at all levels of the socioecological model of abortion stigma need to be considered to address this societal problem that affects and impacts women.
Keywords: abortion, stigma, individual-level, women, factors
Introduction
Abortion stigma is the discrediting of individuals as a result of their association with abortion.1 The individuals include women who have had abortions, individuals who work in facilities that provide abortion, and supporters of women who have had abortions, including partners, family, and friends, as well as abortion researchers and advocates.1 Abortion stigma is a global phenomenon that exists in both the developed and the developing countries. Its impact on women’ health and well-being is grave most especially in the developing countries with restrictive abortion laws. Even in a developed country such as the USA, many abortion patients perceive and internalize stigma2 and the stigma hurts women despite the availability of legal abortion services in the country.3 Abortion stigma plays a significant role in women’s decision on whether to have a safe or unsafe abortion4 and in the disclosure of individual abortion behavior.5 It may cause some women to carry their pregnancies to term and assume a disproportionate economic burden for care; it can lead women to seek unsafe abortions clandestinely to avoid judgment by society1,6 or contribute to women avoiding or delaying safe postabortion care.7 Understanding abortion stigma is, therefore, essential to inform strategies to reduce it and, thus, has direct implications for improving access to care and better health for those whom stigma affects.1
Nigeria is still ranked in the Category I of countries with most restrictive abortion laws that permit abortion only to save a woman’s life or ban the procedure entirely.8 The Criminal Code (Sections 228, 229, and 230) and the Penal Code (Sections 232 and 233) criminalize abortion services in Nigeria.9 Abortion is permitted (Section 297) only for the preservation of the mother’s life. The Criminal Code applicable in southern Nigeria prescribes a penalty of 7 years imprisonment while the Penal Code, applicable in northern Nigeria, prescribes 14 years imprisonment. The law criminalizes the woman seeking abortion services, the provider, as well as any person who aids either the woman or the provider in the process.
Although there are few empirical studies on abortion stigma in Nigeria, the fact still remains that abortion stigma exists and persists in the country and it may be one of the leading reasons women seek unsafe abortion services in the country.5,10 The level of unsafe abortion continues to be high in Nigeria. Nigeria has the highest number of women treated in health facilities for pregnancy termination complications in Africa and ranks fourth to countries like Pakistan (622, 564), Bangladesh (309, 397), and Mexico (219, 430).11 In 2012, about 212,000 women were treated for complications of unsafe abortion, representing a treatment rate of 5.6 per 1,000 women of reproductive age.12 According to a conservative estimate, more than 3,000 women die annually in Nigeria as a result of unsafe abortion, which is twice as high as the entire estimate (1,290) for the Europe, the Latin America, and the Carribean, and the Oceania.13,14 For a country such as Nigeria, it is important that the understanding of abortion stigma becomes more precise through empirical research to understand and measure abortion stigma, design interventions to mitigate it, and evaluate those interventions.15
Although female-focused abortion stigma is a negative perception of women who seek to terminate a pregnancy as inferior to ideals of womanhood; in this study, individual-level abortion stigma (ILAS) is defined as an individual’s lived experiences with and feelings about an abortion decision.16 Therefore, the objective of this study was to measure the level of ILAS among women seeking elective abortion care services and determine the correlates of ILAS among those women.
Patients and methods
This study is a secondary analysis of the data collected from the cross-sectional survey (client exit interviews) of women accessing safe abortion care services at Ipas intervention sites in 2016. Self-selection sampling technique was used to recruit the women as study participants. The data collection was done with an interviewer-administered questionnaire which contained the 16-item ILAS scale adapted from Cockrill et al.17 The ILAS Scale is a theory-based, multidimensional, validated scale to measure stigma among women who have had abortions. Reliability analysis was conducted on the 16-item ILAS scale used in this study. The analysis shows that the 16-item scale has a very reliable internal consistency with Cronbach’s alpha statistics of 0.9122 (Table 1). Each item has four mutually exclusive responses and each of these responses had a score of 1, 2, 3, or 4 depicting the increasing intensity or severity of the response to the question. Each respondent, thus, had the summed response score that spanned from a minimum of 16 to a maximum of 64. A score of 40, ie, midpoint of the possible score range, was set as the cutoff point and was thus used to categorize the respondents into having high (>40) or low (≤40) ILAS (Figure 1). The data were analyzed with Stata/SE 14.2 for Windows. Descriptive (frequencies and percentages), bivariate (chi-square test), and multivariate (log-binomial regression) analyses were conducted. The log-binomial regression model was used to estimate a prevalence ratio (PR) with its 95% CIs for each category of the covariates in the multivariate model.
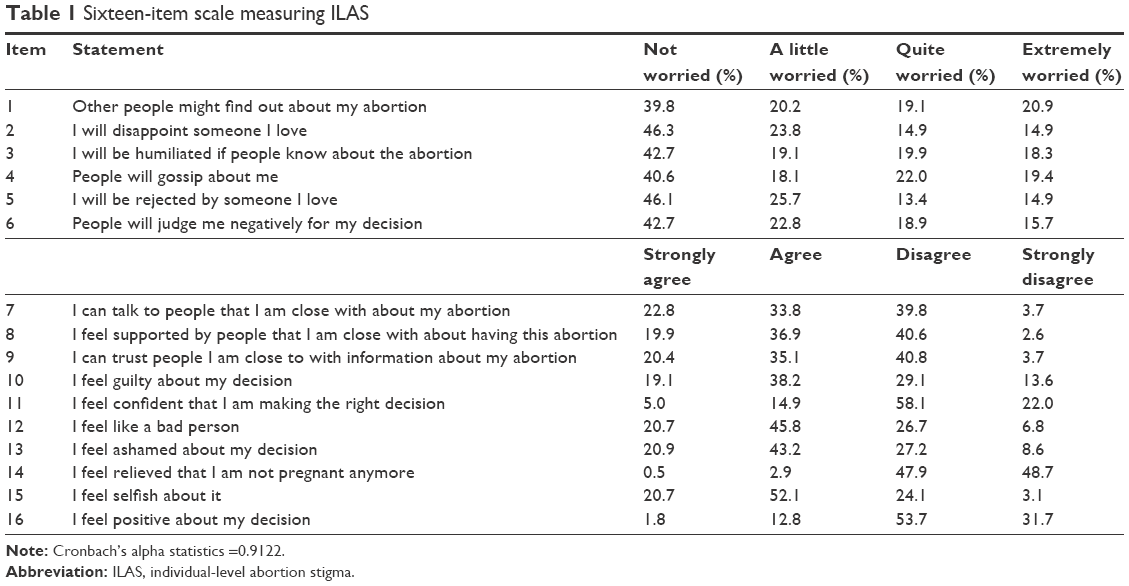 | Table 1 Sixteen-item scale measuring ILAS |
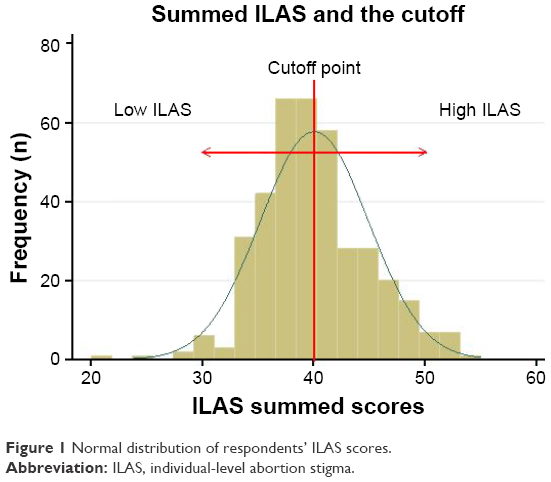 | Figure 1 Normal distribution of respondents’ ILAS scores. |
The protocol and all data collection tools for the primary research were reviewed for adherence to ethical standards by Allendale Institutional Review Board (USA). The primary research was approved by the Review Board. In accordance with the principle of respect for persons, the risks and benefits of the study were explained to the participants and the consent provided by the participants was written informed consent. All data were collected anonymously so that data and results could not be traced back to individual respondents. All informed consent forms and questionnaires were kept in a locked cabinet in the investigator’s office.
Results
A total of 404 women seeking safe elective abortion care services were interviewed, out of which 22 were excluded at the analysis stage because of the incompleteness of data for the outcome variable (ILAS) and the type of provider. Of the 382 women studied, about 45% and 42% were aged ≤24 years and 25–34 years, respectively; and about 46% were currently married or cohabiting. While about 16% of the respondents had no more than primary education, about 40% and 41% had secondary and higher education, respectively. Looking at the number of lifetime pregnancies, about 44% of the respondents had had three or more pregnancies, while about one-third had had one (Table 2).
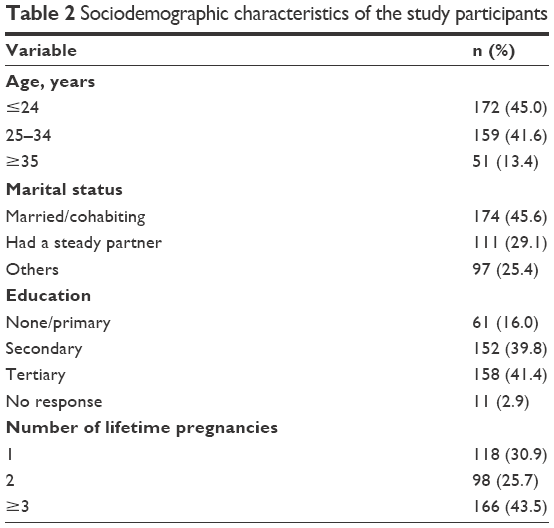 | Table 2 Sociodemographic characteristics of the study participants |
More than two-thirds of the respondents reported that they received surgical abortion procedure (with and without medical abortion [MA]), while about 14% admitted they received only MA care. About two-thirds (65%) of the respondents reported that they received care from physicians and others from the midlevel providers (midwives and nurses). The majority (80%) of the respondents also reported that they experienced cordial client–facility staff interaction (Table 3).
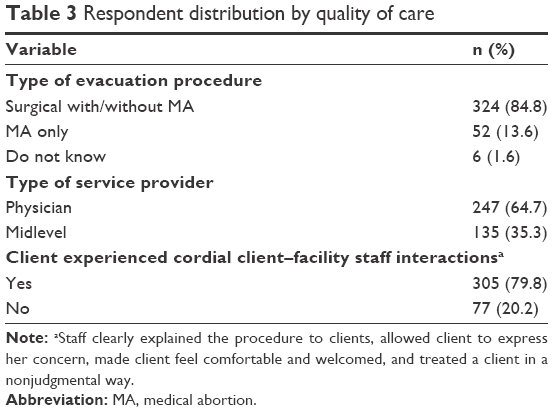 | Table 3 Respondent distribution by quality of care |
The categorization of the respondents’ ILAS scores into high (summed score >40) and low (summed score ≤40) as shown in Figure 1 shows that 43% of the respondents had high ILAS, while the remaining 57% expressed low ILAS. The bivariate analysis (Table 4) identified client age, number of lifetime pregnancies and type of procedure as factors significantly associated with having a high the ILAS catergories. However, all the variables that were not significantly associated with ILAS at bivariate level were still included in the multivariate regression model to control for the confounding effect of each covariate in the model. The model identified client age, education, type of procedure, and type of provider as significant correlates of ILAS among the respondents. The model (Table 4) shows that high ILAS that reduced significantly with increasing age was inversely associated with high internalized stigma as older women (age ≥35) were less likely (PR =0.32, p<0.001) to express high abortion stigma than the younger women (age ≤24). Those with higher education were found more likely (PR =1.64, p<0.05) to express high ILAS than those with no more than primary education. The model also shows that those who had MA only were less likely (PR =0.54, p<0.05) to express high ILAS than those who had a surgical abortion (with or without MA). Finally, those who received services from the midlevel were more likely (PR =1.31, p<0.01) to express high ILAS than those who received care from physicians.
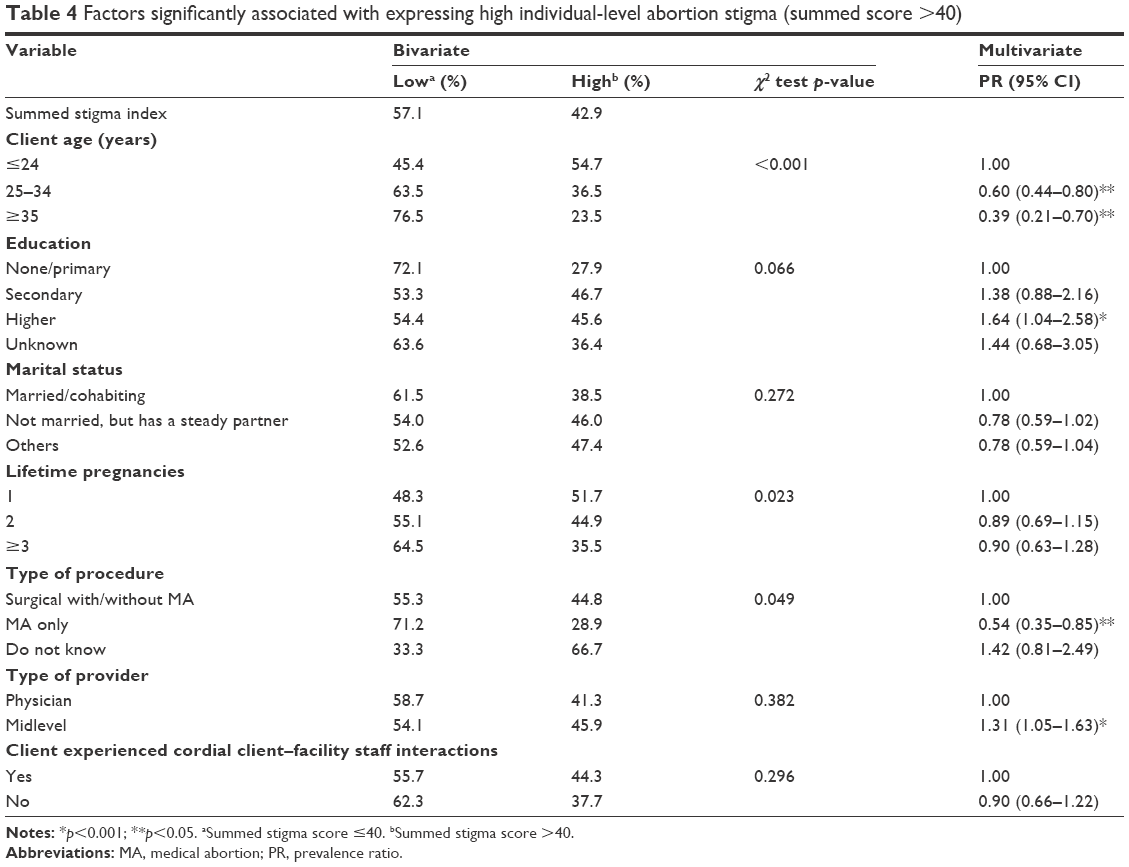 | Table 4 Factors significantly associated with expressing high individual-level abortion stigma (summed score >40) |
Discussion
The present study shows that ILAS not only exists but is also high among women seeking safe elective abortion care service in Nigeria. In a country with a restrictive abortion law, the implication of the observed high ILAS is the influence it has on women’s decision on whether to have a safe or unsafe abortion4 and it may lead women to seek unsafe abortions to avoid judgment by society.4,6 Four factors, therefore, emerged as significant correlates of the ILAS among the women; the factors included age, education, provider’s cadre, and type of evacuation procedure.
A proper understanding of factors influencing ILAS is necessary for its prevention. Situating these four factors in the socioecological model of abortion stigma can give a better understanding of the ILAS and the effect of its potential prevention strategies. At the individual level, the ILAS varied significantly with the women’s age and education.17 In specific terms, the present study suggests that the likelihood of expressing high ILAS may reduce with increasing age.18 In line with this position, a study reported that young unmarried women bore the brunt of being stigmatized and lacked a supportive environment that could provide guidance on correct information on how to prevent unwanted pregnancy and where to get help.4 Although it seems counterintuitive that higher education correlates with higher internalized stigma in this study contrary to other studies one possible explanation for the higher ILAS among women with higher education could be the tendency to feel disappointed for the inability to prevent the pregnancies despite the higher level of educational attainment.4,17 The fact that the observed associations were noncausal suggests that there could be some other individual-level factors not investigated in the present study, but which could have influenced the associations. Some previous studies have identified religious conservatism and norms that place a high value on motherhood as factors that could perpetuate abortion stigma.17,18 At this individual level, it is necessary to ensure that strategies designed to promote positive attitudes, beliefs, and behaviors towards safe abortion.
Given the fact that abortion stigma exists within multiple facets of every society including churches, communities, and health care systems the emergence of provider’s cadre and type of evacuation procedure as correlates of ILAS is not unlikely.7 There is need for a caution in interpreting the association between the type of providers and the women’s ILAS given the importance of task-shifting and empirical evidence that the mid-level providers could provide services that are comparable in safety and efficacy to those provided by physicians. Nonetheless, empirical studies have shown that health care system contributes significantly to women’s abortion stigma and that women’s perception is such that stigma-related mistreatment in health care settings frequently occurs.7,20,21 We, therefore, share the view that ILAS may reduce if health professionals and abortion service providers attend not only to clinical/technical aspects of the abortion procedure but also to women’s psychological and emotional sensitivities surrounding abortion process.22 Regarding the association of ILAS and type of procedure, a probable explanation for the association is that MA is considered more natural because it happens in women’s own bodies and can take place at anywhere before 9 weeks of pregnancy.23 All the identified associations, however, need to be explored further to fully understand the relationships and the implications for the design and implementation of ILAS reduction interventions.
It is necessary to acknowledge the scope and the limitations of this study. This study focuses on ILAS experiences among women receiving safe abortion care, exclusive of those receiving unsafe abortion care. The study was based on secondary analysis of data collected in a cross-sectional survey; therefore, the analysis was constrained to the available variables in the primary dataset and other possible factors that were not in the primary dataset could not be explored. Being a cross-sectional study, therefore, all the associations thus found cannot be proven casual. The use of convenience sample because of the sensitive nature of the subject matter also limits the generalization of the study findings to all women receiving safe abortion care in the country. Other limitations of the study include the use of midpoint of the range as the cutoff point which might have an implication for over- or under-estimating the prevalence of high ILAS and the lumping of all the ILAS items together into one score that does not allow for more nuanced suggestion of interventions that would target the more salient domains from the scale.
Conclusion
High ILAS does not only exists but it is also preponderant among women accessing safe elective abortion services in Nigeria. The authors align with the view that if ILAS develops from public stigma, interventions could be developed to interrupt the process at the individual level to reduce or eliminate ILAS despite the perceptions of public stigma.24 However, there are evidence-based interventions that have been shown to reduce stigma.25 Perhaps interventions and techniques such as self-awareness assessments, peer counseling, decision aids, encouraging active client participation, supporting decision satisfaction, support groups, Internet-based support, ongoing telephone counseling, and public artistic expression could be considered as some of the specific approaches to address this societal problem that affects and impacts women. However, there are a variety of other interventions at other levels of the socioecological model, that can also be explored.
Acknowledgments
We appreciate and acknowledge the effort of Dr Kristen Shellenberg for her meticulous review of the manuscript and her invaluable contributions to the final version. We also appreciate the effort of Emily Madsen who validated the results of the data analysis.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Norris A, Bessett D, Steinberg JR, Kavanaugh ML, De Zordo S, Becker D. Abortion Stigma: a reconceptualization of constituents, causes, and consequences. Womens Health Issues. 2011;21 (3 Suppl):S49–S54. | ||
Shellenberg KM, Tsui AO. Correlates of perceived and internalized stigma among abortion patients in the USA: an exploration by race and Hispanic ethnicity. Int J Gynecol Obstet. 2012;118 (Suppl 2):S152–S159. | ||
Harris LH. Stigma and abortion complications in the United States. Obstet Gynecol. 2012;120(6):1472–1474. | ||
Yegon EK, Kabanya PM, Echoka E, Osur J. Understanding abortion-related stigma and incidence of unsafe abortion: experiences from community members in machakos and trans Nzoia counties Kenya. Pan Afr Med J. 2016;24:258. | ||
Shellenberg KM, Moore AM, Bankole A, et al. Social stigma and disclosure about induced abortion: results from an exploratory study. Glob Public Health. 2011;6 (Suppl 1):S111–S125. | ||
McMurtrie SM, García SG, Wilson KS, Diaz-Olavarrieta C, Fawcett GM. Public opinion about abortion-related stigma among Mexican Catholics and implications for unsafe abortion. Int J Gynecol Obstet. 2012;118 (Suppl 2):S160–S166. | ||
Berry-Bibee E, Jean CJ, Telemaque Y, Nickerson NM, Jean-Louis S, Lathrop E. Stigma surrounding illegal self-induced abortion in urban Haiti. Int J Gynecol Obstet. 2015;131. | ||
Bank W. The World’s Abortion Laws Map 2013 Update. 2013:60–61. Available from: https://www.reproductiverights.org/sites/crr.civicactions.net/files/documents/AbortionMap_Factsheet_2013.pdf. Accessed January 19, 2018. | ||
Okagbue I. Pregnancy termination and the law in Nigeria. Stud Fam Plann. 1990;21(4):197–208. | ||
Omideyi AK, Akinyemi AI, Aina OI, et al. Contraceptive practice, unwanted pregnancies and induced abortion in Southwest Nigeria. Glob Public Health. 2011;6 (Suppl 1):S52–S72. | ||
Singh S, Maddow-Zimet I. Facility-based treatment for medical complications resulting from unsafe pregnancy termination in the developing world, 2012: a review of evidence from 26 countries. BJOG. 2016;123(9):1489–1498. | ||
Bankole A, Adewole IF, Hussain R, Awolude O, Singh S, Akinyemi JO. The incidence of abortion in Nigeria. Int Perspect Sex Reprod Health. 2015;41(4):170–181. | ||
Sudhinaraset M. Reducing unsafe abortion in Nigeria. Issues Brief (Alan Guttmacher Inst). 2008;3:1–3. | ||
World Health Organization. WHO|Unsafe abortion: global and regional estimates of the incidence of unsafe abortion and associated mortality in 2008. 5th ed. WHO; 2014:1–67. | ||
Kumar A. Everything is not abortion stigma. Womens Health Issues. 2013;23(6):e329–e331. | ||
Kumar A, Hessini L, Mitchell EM. Conceptualising abortion stigma. Cult Health Sex. 2009;11(6):625–639. | ||
Cockrill K, Upadhyay UD, Turan J, Greene Foster D. The stigma of having an abortion: development of a scale and characteristics of women experiencing abortion stigma. Perspect Sex Reprod Health. 2013;45(2):79–88. | ||
Yegon E, Mwaniki P, Echoka E, Osur J. Correlates of individual-level stigma and unsafe abortions among women seeking abortion care in Trans Nzoia and Machakos Counties, Kenya. Ann Trop Med Public Heal. 2016;9(4):226–234. | ||
Sorhaindo AM, Juárez-Ramírez C, Olavarrieta CD, Aldaz E, Mejía Piñeros MC, Garcia S. Qualitative evidence on abortion stigma from Mexico city and five States in Mexico. Women Health. 2014;54(7):622–640. | ||
Izugbara CO, Egesa C, Okelo R. “High profile health facilities can add to your trouble”: Women, stigma and un/safe abortion in Kenya. Soc Sci Med. 2015;141:9–18. | ||
Tagoe-Darko E. “Fear, shame and embarrassment”: the stigma factor in post abortion care at Komfo Anokye Teaching Hospital, Kumasi, Ghana. Asian Soc Sci. 2013;9(10):134–141. | ||
Astbury-Ward E, Parry O, Carnwell R. Stigma, abortion, and disclosure-findings from a qualitative study. J Sex Med. 2012;9(12):3137–3147. | ||
Berer M. Medical abortion: issues of choice and acceptability. Reprod Health Matters. 2005;13(26):25–34. | ||
Vogel DL, Bitman RL, Hammer JH, Wade NG. Is stigma internalized? The longitudinal impact of public stigma on self-stigma. J Couns Psychol. 2013;60(2):311–316. | ||
Upadhyay UD, Cockrill K, Freedman LR. Informing abortion counseling: an examination of evidence-based practices used in emotional care for other stigmatized and sensitive health issues. Patient Educ Couns. 2010;81(3):415–421. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.