")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 12
Coping with transitions in life: a four-year longitudinal narrative study of single younger people with dementia
Authors Johannessen A , Engedal K, Haugen PK, Dourado MCN , Thorsen K
Received 12 March 2019
Accepted for publication 15 May 2019
Published 28 June 2019 Volume 2019:12 Pages 479—492
DOI https://doi.org/10.2147/JMDH.S208424
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Aud Johannessen,1,2 Knut Engedal,1 Per Kristian Haugen,1 Marcia CN Dourado,3 Kirsten Thorsen1,4
1Norwegian National Advisory Unit on Ageing and Health, Vestfold Hospital Trust, Tønsberg, Norway; 2Campus Vestfold, University of South-Eastern Norway, Tønsberg, Norway; 3Center for Alzheimer’s disease, Institute of Psychiatry, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil; 4Norwegian Social Research, Oslo Metropolitan University, Oslo, Norway
Background: People with younger onset dementia (YOD <65 years) experience a great transformation of existential life. Living alone, they lack the support of a partner, and have a higher risk of moving into a residential care facility.
Aim: To explore how people living alone with YOD experience and cope with transitions during the progression of dementia.
Method: A longitudinal qualitative approach was used. From 2014 to 2018, we interviewed 10 persons with YOD every 6 months for up to four years.
Findings: Two significant main transitions and themes were registered under the perspective; experiencing and coping with (1) receiving the diagnosis of dementia and (2) moving to a residential care facility, which covers two subthemes: moving to a supported living accommodation and moving to a nursing home. To get the diagnosis was initially experienced as a dramatic disaster, while moving to residential care were mainly experienced as positive. With efficient cognitive and emotion-focused coping strategies, the participants adapted and experienced a mostly good life for a long time.
Conclusion: People with dementia can describe their lived experiences for a long time after receiving the diagnosis. They adapt and preserve a feeling of a rather good life by the efficient use of various coping strategies. High-quality public support is of significant importance to assist them in sustaining quality of life and vitality.
Keywords: early-onset dementia, existential needs, health care services, health promotion, qualitative study, transition
Introduction
To get a diagnosis of dementia in younger age (YOD<65 years) is abruptly transforming a normal expected life course, impacting on identity, everyday life and future prospects.
The number of people with YOD in Norway is estimated to be 4,500 to 5,000 people, whereas the number of people above the age of 65 with dementia is estimated to be 80,000.1–3 In most cases, dementia is caused by progressive neurodegenerative disorders, which imply radical changes and transitions in the life situation and prospects for the future.
Dementia affects the person’s cognition, which gradually declines and threatens his or her self-image and self-confidence. The disease reduces an individual’s abilities to take care of daily activities and herself or himself and to be oriented in the environment. It also implies a gradual transition from being independent to becoming cared for, often in a residential care facility.4–7
Qualitative studies show in more detail how people experience living with the disease.
The process of receiving a diagnosis of dementia for everyone is, reasonably, followed by uncertainty and concerns about the future.4,8–12
Little attention has been given to how persons with dementia, not only people with YOD, experience their situation over time, how they cope and how their abilities to manage everyday life can be supported when dementia progresses. Losing functional and coping abilities may lead to an experience of loss of dignity and later to a sense of shame and despair.5,13,14 The social response of others can support or undermine social wellbeing.15 Maintaining meaningful activities may help the person with dementia to preserve dignity and the sense of self.16
Knowledge is also limited regarding how persons, during the progression of dementia, experience various transitions, including receiving the diagnosis, stopping their working lives, being cared for, and eventually moving to a residential care facility. There is a need for more knowledge about how people with dementia respond and adapt to the disease over time with their resources and abilities, especially in radical transitions that change the life course.4–6,8,17 Such information is of importance as many persons with YOD living alone experience increasing isolation, loneliness and vulnerability, and needs for assistance and services like day care centres or residential care facilities.4,5,9
Summing up: There are still scarce qualitative studies, based on interviews/dialogues with people with dementia – in younger or older age – on how they experience living with dementia. There is great lack of studies exploring their existential living over time, which is the background for our longitudinal study.
According to public policies in Norway, people with dementia should remain living at home for as long as possible,18,19 in line with the policy advocated by the World Health Organization.20 People living alone with dementia have a greater risk for unmet needs21 than those living with a partner, and a higher risk of moving to a nursing home.22
During challenging changes and transitions in the life situation, it is important to realize that health care personnel’s evaluation of what persons with YOD experience and need is not necessarily in accordance with the person’s subjective needs.10,23,24 Thus, people with dementia should be given opportunities to express their perceptions of their life world and needs.4,5,8,9,25–27
The concept transition, which is used as a focal concept in our analysis, is an integral part of life course theory.28 Transitions are defined as “changes in roles and statuses that represent a distinct departure from prior roles and statuses. They are discrete and bounded; when they happen, an old phase of life ends and a new phase begins.”29 Transition theory, also define a transition as any experienced event, or non-event, that results in changed relationships, routines, assumptions, and roles.30 We will apply this concept of transitions.
Vital transitions are thus not only “outer”, they are filtered through the experiences and the personality of the individual. They transform inner life, social relations, habits, life plans and the self, and challenge coping capacities.
Studies have shown that ageing people have amazing coping capacities for thriving in spite of losses, reduced resources and diseases.31 The theory of selective optimization with compensation (SOC)32,33 presents the strategies ageing people use to preserve thriving. They concentrate on what is vital and significant in their lives, invest their engagement in these fields and try to compensate for fewer resources and capacities and less strength. In short, they demonstrate resilience.34 People also have the capacity to perceive continuity in the life course where others see breaks and disruptions.35 Resources, adaptation and resilience34,36–40 change the outcome.
To the best of our knowledge, no study has followed people with YOD and listened to their own stories over a span of four years. Therefore, we have performed a longitudinal study aiming to explore how people living alone with YOD experiences of coping with transitions during the progression of dementia.
Methods
Design
The study is a longitudinal explorative, narrative descriptive study with a duration of four years. The period of four year was decided after evaluation of the project`s resources and further output. Then six out of ten participants had dropped out (more information later), the information in the last interviews were rather meagre, shrinking and mostly covered in earlier interviews.
Individual qualitative interviews were conducted every six months with a series of up to eight interviews with the participants. The first took place at inclusion in 2014, three to six months after the diagnosis was ascertained, and the remaining seven interviews took place every six months thereafter.
We have thoroughly considered the time interval, and the six months period between the interviews was considered optimal, covering experiences of significant transitions during the interviews, but not too often to overtax the energy and willingness of the individuals to participate. An important consideration was to preserve trust and positive relations to the participants and avoid exhausting them. All interviews covered what the persons had experienced on the day of the interview, as well as earlier experiences and reactions to them.
Participants
To attain heterogeneity, we included persons with YOD (age at onset of dementia before 65 years of age) of both genders and living alone, from the southern and western parts of Norway. They were recruited from six memory clinics. The participants could have different dementia diagnoses and various comorbidities. Frontotemporal dementia was an exclusion criterion because people with this diagnosis have less insight into their disease and situation. A total of 10 people with YOD were asked to participate, and none declined. The sample comprised participants 49 to 67 years of age (mean of 60 years), including seven women and three men. At the time of the four-year follow-up, six persons had dropped out; one died; one had severe dementia and was no longer able to answer the interviewer’s questions; three declined further interviews; and one was excluded because of the value of the collected information at the last interview (see Table 1). Eight persons were divorced; one was a widow; and one was unmarried. Three participants were childless. Only three of them had children living close by but not in the same household. Some characteristics of the informants are described in Table 1. Due to strict principles for protecting anonymity, with few people with YOD in each region, we do not individualize more the personal characteristics.
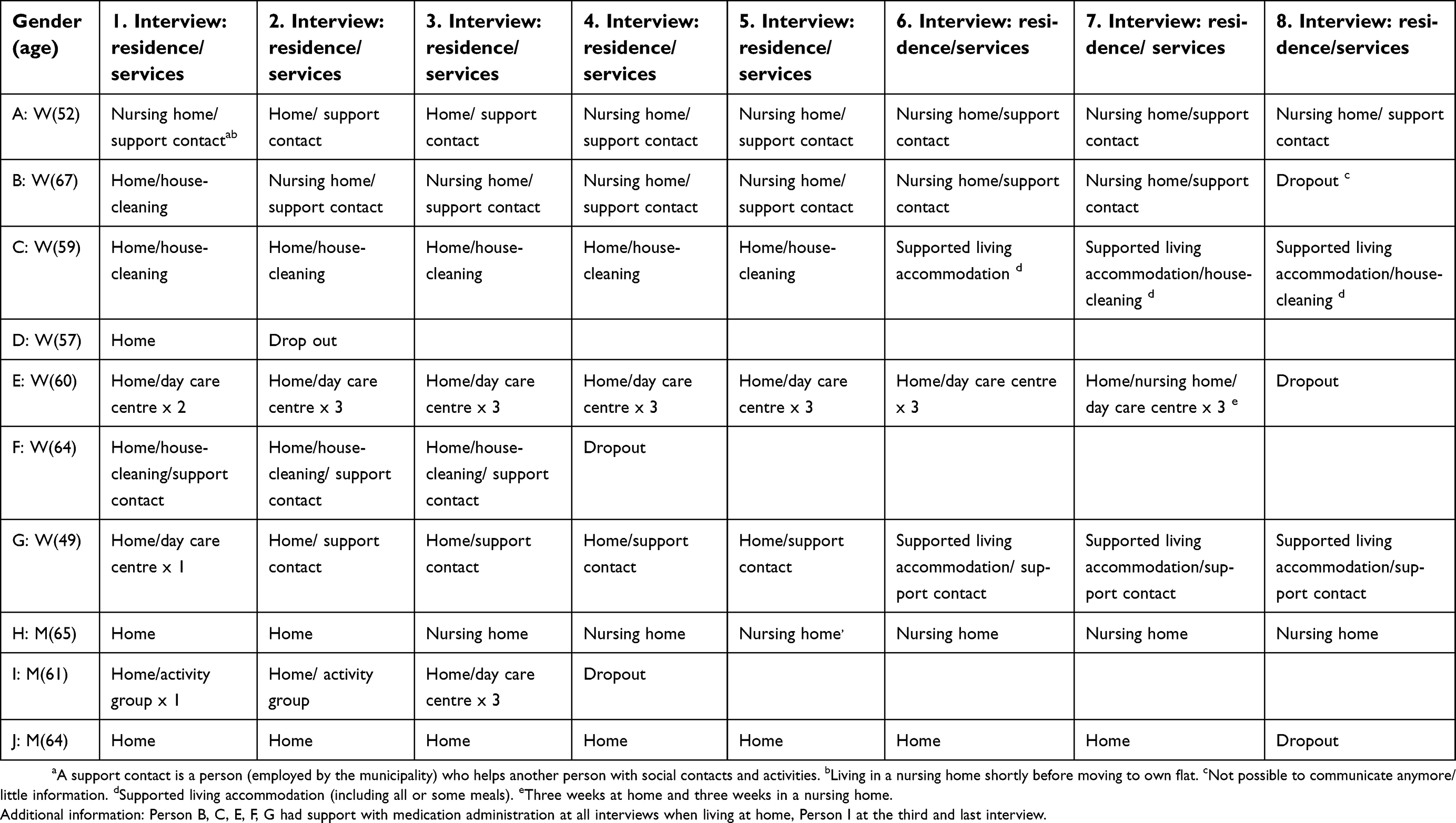 |
Table 1 Characteristics of the informants, their living situation and use of support contact |
At the time of the follow-up, two persons had moved to a supported living accommodation; one had respite stay in a nursing home; and three had moved to a nursing home. In this study, a supported living accommodation is a private flat in a complex of flats organized for people needing more assistance that in ordinary flats. There, residents are offered varied types of activities, social gatherings and support, according to their preferences, but the complex is not fully staffed 24/7 like a nursing home.
The interviews
The 60 interviews lasted for 7 to 63 mins each (mean 28 mins), and the total time for all the interviews was 1, 693 mins. Some of the interviews were rather short. One reason was that the person was not “verbal” and narrative in style, but matter-of-factual in their descriptions. Their talk may represent a habitual sociolect.41 The participants` verbal fluency and vocabulary become reduced during the progression of the dementia. Another reason may be that the same stories are told several times. They are shared, known and later touched upon with short referrals.
The interviews, conducted by the first author (AJ), were performed at the most convenient place for the participants.42 Two of the interviews were conducted at a hospital (see Table 2); all the remaining interviews were carried out in the participants’ private rooms/homes. Some field-notes were taken as supplement for memory and interpretation, but the basic data material is the transcribed interviews with the person`s own wording.
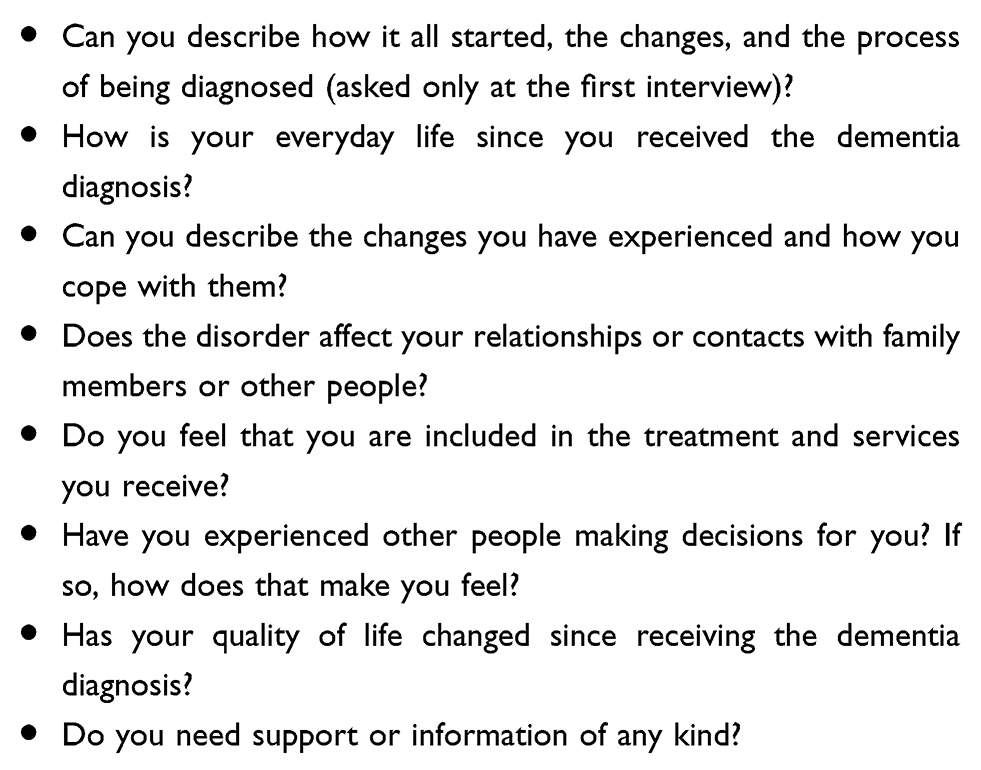 |
Table 2 Questions and themes from the interviews with the people with younger onset dementia living alone |
The interviews were tape recorded and transcribed verbatim by a professional typist within two weeks. A quality control check was performed by interviewer AJ, who listened to the tapes while reading the interviews. This procedure was considered to be sufficient and satisfactory, since the quality check was to see if the research assistant has understood and transcribed the interview accurate. As recommended for longitudinal qualitative studies, the interviewer was the same through all interviews, and she was the one who could best understand what was said during the conversation/interview.43
The interview guide is listed in Table 2. The first question in Table 2 was asked only at the first interview. Detailed follow-up questions explored what had happened since the last interview.
Analysis
As underlined that narrative inquiry is a particular type, a subtype of qualitative inquiry. It revolves around an interest in life experiences as narrated by those who live them.44
We used a reformulated analytical method approach of Grounded Theory.45 The modified method is particularly fruitful for the study of people’s living experiences of personal development and their social relationships, making it the preferred method for this study. The method has been applied, without an intention of formulating a theory, to acquire more-detailed knowledge about how people with YOD experience their life situation.
At first, an initial approach – “open coding” – was to read all the interviews with an open mind whilst searching for themes concerning the significant experiences of transitions of the participants. The interpretation was both inductive and deductive, as recommended in a study43 for longitudinal analyses of large quantity of qualitative data. We searched for remarks and narratives about the important event of getting the diagnosis of dementia and other vital transitions. Remarks like “It is very difficult. Sometimes I cry a lot. Transitions are part of life. Now I am very afraid of the future”, (cited in the empirical part), signify the emotional, cognitive and life changing impact also for the future of getting the dementia diagnosis. Moving from own private home was another important transition. We explored these significant themes “vertically” over time for each person. Did the first reactions persist, or reside, and how did the person manage the challenges of the transformations in daily life? Some described the transitions by using this word and were stressing the change between “before” and “after” the event.
Then, the themes were compared by “axial coding” to identify the most relevant higher-level themes for the whole group. Agreement on higher-level themes was reached by discussion among the researchers. In the process, the researchers continuously related the themes to the empirical material, analysed it vertically – going back and forth in the material of one participant. We also analysed it horizontally, comparing the participant’s situation and experiences with the others, in line with the method’s constant comparative approach. The processes of open and axial coding, as Corbin and Strauss emphasized (2008), are intertwined empirically. The axis of our empirical analysis is the time perspective, that is, how the dementia process has changed the participants’ narrated experiences of their life situation.45
The first five interviews were analysed and published in an article aiming to explore the existential experiences of people with YOD.4 A case study analysed the experiences over time of one single person with YOD.5 In this study, we have expanded the analysis to examine what happened in the later stages and, thus, have included all the participants. All interviews have been analysed and reframed under the perspective of coping with transitions.
Ethics
The study followed the ethical guidelines outlined in the revised Declaration of Helsinki46 and was approved by the Regional Committee for Ethics in Medical Research, Southern Norway (number 2013/2149). The Norwegian Data Protection Authority also approved the study (number 36,797). The participants received oral and written information about the study and gave their written consent before they were interviewed. Protecting the anonymity of the participants has been an important consideration.
Findings
The findings of the analyses are captured by two main themes, condensing the experiences of the most significant events and transitions during the progression of dementia. Experiencing and coping with (1) Receiving the diagnosis of dementia (2) Moving to a residential care facility. This theme covers the two subthemes: Moving to a supported living accommodation and Moving to a nursing home.
Receiving the diagnosis of dementia
For many of the participants, dementia started with increasing memory problems, from rather imperceptible changes in cognitive functions going on for years, like forgetting names, how to handle things, and having problems with orientation and localization. Increasing cognitive problems and compensation efforts gradually interfered with everyday functioning.
For some persons, difficulties with performing tasks were observed at the workplace.
Often, it was their employer who recommended that they see a doctor, or they felt that something was “wrong”, which led to being referred to a memory clinic for assessment. A woman expressed: “It felt almost like that I had ants inside my head. It was like that the ants were creeping inside my head (…). I went to the doctor, but he did not find out. After a while he sent me to further examination, and the diagnosis was confirmed.” The procedures, tests and assessment for the diagnosis are mentioned as stressful.
The diagnosis and the consequences were, according to most of the participants, experienced as a serious life event, turning their existence “upside-down”. A man says: “When the process first started, I really felt bad, you know. I was just lying on the sofa here and felt sorry for myself. It was not okay.” A woman experienced various changes in her life situation when she got the diagnosis of dementia. At the first interview, she says: “It is very difficult. Sometimes I cry a lot. Transitions are part of life. Now I am very afraid of the future. How will I be able to take care and manage my life? I often sit down very depressed, can just be sitting there for 2–3 hours, and don’t know how time [has] passed away.” The persons still working when the assessment process began were offered sick leave, a disability pension or retirement. One person was still working (with partial sick leave) at the first interview; two had old-age retirement; the rest had disability pensions. Some had experienced the unexpected loss of work as a great loss in their life. A woman, still employed, exclaimed: “After many years at work (…), it will be a terrible transition. I expected to work for many more years. It will be very difficult.”
How did the participants initiate adaptation and coping efforts to handle life after the first shock of the diagnosis had subsided? Some adapted to the prospects of a future with dementia rather quickly. A man who said that he “went deeply down” when he got the diagnosis, at the next interview says: “But now I feel very well. I am completely another boy than I was just after the diagnosis. I have many buddies. I think my life now is fine.” A woman talks about her active decision to take control of her reactions and plan her future life with dementia:
In autumn, I got the diagnosis, and went just down. I cried and was very upset. Then I read an article in a newspaper about a girl who had had a very traumatic life. Then I thought, I have to decide that I must make myself happy. No other can. The decision gave me a push. What am I to complain? I can go skiing; I live in a wonderful flat; I have close family, people who care about me, and hobbies that I love, like taking photos. I do not have to go to work; I can avoid the stress. I have decided to be glad since it is good for my health (…). I have a very good situation.
She took a review of her “assets”, her resources for making her life happy: Her network, family and friends, interests and prospects. She is the only participant reporting such a decisive moment in her way of seeing the future with dementia and making a plan for how to act and cope. She left her grieving behind and took action to make herself happy. Her description of all her “good things in life” is detailed in the following interviews. Her social resources are many and varied.
The participants underline that they have a strategy of looking at the bright side of life, avoiding thoughts and situations that remind them of the dementia and their shortcomings.
A man – like others – emphasizes his optimistic outlook on what happens: “I am a person who always look at the bright side of life – that it is better than bad. Then I function well, and I do not go and pity myself”. However, at the same time, most of them are realistic in their view of the progression of dementia. The woman cited above says: “I realize that it will be worse, but I will make the best out of it for as long as I can!”
Some participants live in the centre of the capital of Norway, others in remote regions far from local centres and services. The availability of support and local resources differs. A woman says: “What I think is the worst is that I am not allowed to drive a car any longer. Here at my place, there are long distances to everything. I have been dependent on a car.” However, whatever their resources, they share the main coping strategy of making the best of it.
The participants mention that they have controlled their outer image by concealing their diagnosis and have presented their difficulties as a “memory problem.” Their reasons are to be seen as “normal”, to be able to relate to others as usual, and to diminish the impact of the disease, for themselves as well as others. “I want to live my life as well as possible and not talk very much about it. Yes, not enlarge it by talking.” In the early stages, their problems may be minor, and some disguise them with jokes and self-irony. A man comments: “I do not talk much about illness in general. I think I maybe get more ill by talking.”
A woman living in a remote part of the country compares her life to others and says: “I manage on my own, I buy what I need, I make my food. (…). It is a normal life. Sometimes it is a little boring; other times it is okay. So, it is for most people, I think. And I do not have pain.” She focuses on her everyday life, which is seen as an ordinary life, like most others`.
What happened to person who were staying at home? Two persons, a man and a woman, were living alone at home during all completed interviews (seven in total). The man, at the first visit after the diagnosis, deeply regretted losing his engaging job. He thinks he is stamped, has lost his “badge”, his main role in life, and he is feeling miserable. His down period is followed by a gradual adaptation. At the next interview, he says: “The dementia is not bothering me.” He has decided not to complain about anything. However, his adaptation to the status as a pensioner becomes remarkably more positive when some of his friends also retire: “Suddenly, I am a member of the club again. It is very usual. So, I am not completely alone any longer.” At the following interviews, he states that he feels excellent, “very okay” and “has no problems.” At the last interview visit, he even says: “I feel very well. I think. It gets better and better (…). I feel no changes, except my local orientation (…). The only disaster is that I have lost my certificate. I think it is terrible.”
The woman living in her private home in the countryside enjoys visiting a day care centre three times a week. She says, “We joke. It keeps me up.” At the seventh interview, the last, she is also at respite stay at a nursing home – three weeks at home and three at the nursing home. She expresses that she does not experience her stay at the nursing home as a transition – she has no feeling that things are changing. “It is the same.” Her life is “as usual.” The basis for her experience of continuity is that she has not made a definite move out of her home. She does not think about the dementia, sees no problems, and finds that “life is good, really.” At this time, she even thinks that something has improved: “I remember a little better.”
The persons living at home describe experiences of life with dementia for the time they participated in the project as a continual, slow, sometimes almost-imperceptible change. With coping strategies, they accept and adapt to the progressing dementia. Most of them continue to express for a long time that life is reasonably good. However, they admit a sneaking feeling of boredom when their energy decreases.
Moving to a residential care facility
Moving to a supported living accommodation
Two participants have reluctantly moved to supported care accommodations. The woman who made the resolute decision to emphasize all the good things in life is, at the fifth interview, preparing for a move to a supported care accommodation. She does not feel “so much” that she has Alzheimer’s disease. She says: “Except for the pain in my leg, life as such I am very satisfied with.” She feels she is being pushed to move by the local municipality, which has built a new building complex with supported care accommodations that they must fill up. “They want me to move, and I had no good arguments to say no.”
However, already at the next interview, which took place just after she moved, she is very enthusiastic. She talks about her activities, social relations and all the interesting arrangements. She does not regret moving at all. On sunny days, the residents sit outside. “It is very different from sitting in my former home; there I was completely alone, see?” Her retrospective narrative about her former social life has changed, and now it is presented as a darker background for her new positive situation: “The first time I came here I said: I won’t move, I won`t move! Now I am very satisfied. Others have seen it too. They say: “You are always so satisfied. (…) Yes, I have that personality.” She has adapted to the transition, even if she did not choose it, or wish it, and sees it as progress. Still, she does not feel she has a disease. Her basic coping strategy, “making herself happy,” is successfully transferred to life in the new flat. Her conclusion stands firm after four years of living with dementia: “Life is very good.”
Another woman living alone at home has been increasingly depressed during follow-up. She senses that her dementia is progressing, and she finds life meaningless. After the fifth interview, she moves, reluctantly, into a supported care accommodation. Her quality of life changes radically and positively after the transition. She reports at the next interview: “So many say to me: “Don’t you miss your old flat?” I say: “Not a minute! I am so happy (…). In the beginning I did not want to have any contact with the others here. It changed.” However, she differentiates her life experiences: “I do thrive more and more here. I do so. At the same time, I feel that I get worse. Then I become very annoyed.” Her remarks illustrate the contrasting, sometimes contradictory “outer” and “inner” experiences: her joy and satisfaction over her living conditions and her sorrow that the dementia has progressed.
Both women demonstrate the great coping abilities and adapting capacities of people with YOD, even in “pushed” transitions to another way of living – to a new, supported flat – which they have not wanted or chosen. However, the participants discover and appreciate the breadth of activities and social contact where they are now, and perceive the support, and opportunities they did not have in their former homes. They have changed their evaluation.
Moving to a nursing home
Three participants moved to a nursing home. We will analyse the experiences of this radical transition of two of them in greater detail, a woman and a man.
The woman says that to be living alone in her own flat was extremely difficult. The autonomy she wanted, trying to manage on her own, turned out to be a lonely and scary existence. She had “morning anxiety”, frightened about the day to come. At the fourth interview, after moving to the nursing home, she talks about her experiences of the transition from living in a private flat. “I was so terribly scared of everything, and many things that are normal for human beings – I feared them. But now I am not scared any longer, and it is wonderful to end being so afraid and so exhausted.”
She experiences a great sense of relief and describes her new life: “Now I am fine, feel safe, can even sit quietly and knit, which I have not done for a long time, and sense that it is quiet, even if the old residents chat a lot.” (She laughs). She is very active and vital, enjoys her hobbies, sits in the living room and attends social gatherings. Being accepted as the person she is, with dementia, getting assistance to do what she wants, and being able to avoid the things she has not mastered, has restored her autonomy. However, it is a different autonomy – an assisted autonomy performed in safe surroundings.
However, at the sixth interview, her experiences have led to more ambivalent feelings. Her opening comment is: “I am happy to live here. I am! (…).” But she misses people of her own age, and activities for this group. She says that she does not attend when the other old residents have coffee breaks. Also, her health is deteriorating; she emphasizes that her knee is “outworn” and hurts. Still, she is performing some of her former activities, preserving continuity. She is a gardener at the nursing home, planting seeds and nurturing plants. “They are my babies. To plant a seed gives meaning to life. To see it be a beautiful flower”. She takes a lot of photos, but the meaning and context have changed. She lies in her bed and looks at the pictures, which are functioning as her diary and supporting her memory. For the most part, she stays alone in her room. “But I just have to feel the safety that there is somebody there.”
Dementia has progressed in the way that, she reports: “I get so very tired of being me. It is so many silly small things that become huge heaps in my head.” She abstains from social contacts that provoke experiences of chaos, conversations she can’t participate in, especially with people who do not know her disease, and contacts where she feels miserable. Then she can cry afterwards, often for a long time. “Everything is felt so strongly and strange.” She mourns that she cannot write any more. “If I had been able, I would have written a book. About life. About how everything changes in the head. It is important to get it (the story) out. To people.” She avoids thinking about the future. “I do not despair. What comes, will come. If the disease will be so that you forget the people you love and the small things you enjoy, okay, then I hope that you don’t care at all. I hope it is like that.”
At the last interview, she is, as ever, elegant: “You have to smarten up, even if you feel awful.” She repeats her persistent opinion about the nursing home. Dementia and her situation have deteriorated further. She continues some of her hobbies but with less energy and commitment. Now, “the best place is in bed. At least here nothing happens.” She prefers to be alone, avoids the other pensioners, but at the same time, she longs for someone to talk with who sees her as an individual. She now comments about the personnel: “They have no time to listen. I have no occasion to talk about what is in my head and heart. I am often sad. Earlier, some of those working here would come and look at my pictures and have a chat. No more.”
At this point in life, she hopes she will have a short future in the nursing home. Her last remark is: “My future? I shall not live here for 40 years. I am not afraid of dying. I think it will be fine. Everything finished. No life, you know.”
Also another woman, at the second interview, just after moving into a nursing home, expresses great enthusiasm about her new life: “It is very, very nice here. I call them angels, those working here.” The same enthusiasm is maintained during the whole period. “I think that everything is getting better and better.” At some point, she even thinks she remembers much better.
The man, moving into a nursing home, was divorced rather late in life. He has been living alone in a remote part of the country, “in the woods.” He is a former leader of a job “with very much to keep track of.” He was informed that he seemed to be unfocused at work, which he did not feel himself, and it was proposed that he take sick leave. After a medical assessment, he got the diagnosis of dementia and lost his job. This event has left a great gap in his life. At the first interview, he talks about trying to find new activities, “somewhere to go.” He says: “Having ended working, you have to engage yourself. It is very easy to be lying in bed until 10:30. It is the way it is (…). It is a way of life you have to try to be accustomed to. I read a lot.”
His narrative is mainly retrospective. He prefers to talk about his former life, his education, his previous job, with events and travels all over the world. His life story is his career life, presented as the core of his identity. In the second interview, his quality of life is unchanged, as he sees it: “Full freedom, full salary, without work.” He does not think about the dementia. He is worried about losing his car: “It will be a crisis.”
However, his private doctor had advised that he should apply for an intermittent stay at a nursing home, which became permanent. The car was sold. He finds his new life in the nursing home boring and the days empty: “24 hrs are a terrible long time if you have nothing to do.” He misses his earlier life. There he could wake up and see a moose or a deer outside his window. On the other hand, he is positive about eating all his meals together with others, compared to having only a squirrel or a moose as company. “It is very nice here. Unproblematic. You get up, get your clothes washed and get food four times a day, but it is not the same freedom any longer. You have lost your freedom.” He has not given up hope of returning to his former home. He has found a friend from his school years here, and they are sharing memories about their former lives. He still does not “feel” his illness or think about it.
Half a year later, he takes a short walk every day, and his buddy visits him regularly. He reads a lot. Daily life has gotten a structure, and he finds that life is okay: “I do not complain.”
In the next interview, he mentions that he has much time on his own – being alone. His good friend has passed away. However, a female resident is sharing his interest in nature and travelling. They have a chat every day. “She is a light in my day. She means rather much to me.” Concerning living in the nursing home, he says: “I see no reason for complaining of life in the nursing home, the personnel are kind and considerate, and the food is good. I am very comfortable. Do not have to make any decisions. Long live laziness.” Every day he thinks that he has to take on a more active life, like bicycling or cross-country skiing, but he is lacking the means to do it, like a car.
At the following two interviews, he is still not bothered “at all” by the dementia – he only has a “hint” of dementia. He continues his coping strategies. Now his wishes for returning home, have gone.
At the last interview, he recounts his master strategy for life: “I have never thought of being bored. Consequently, I try to find the positive sides of life and pass on from there. I think I am rather clever.” Despite his plans, ambitions and coping strategy, he has become less active. He does not read any longer, since there is “something wrong with the glasses”. He just “fumble and fumble and fumble.” Suddenly, in the course of the interview, he fell asleep. After a short nap, the interview continued. Now his story about why he moved to the nursing home has changed: “From time to time, it was lonesome up there in the wood. When the doctor suggested I should move to the nursing home, I agreed, and I have not regretted it a second.” Loneliness now has a more prominent place in his story about his former life, contrasting his more-positive life situation now.
What he misses most is driving, and the great transition in his life – mentioned several times – has been losing his driving license, “and the freedom a car gives. You could just take your car, and in a moment, you were [in] another place. I used to say that I miss the car more than I miss the wife.” Otherwise, he has adapted to life in the nursing home. Life there is comfortable and social.
Discussion
The study has shown that people with YOD are able to talk about how they experience life with progressing dementia, even at later stages when they are greatly handicapped by problems with cognitive deficiencies, shrinking language and loss of memory. This aligns with several exceptional books written by people with dementia47–49 as well as reports and recorded stories.50,51
We find that the participants are very open-minded in their interviews and demonstrate trust for the interviewer, visiting them eight times at most. The stories are presented in their narrative style, consistent throughout the study period, in line with their social and educational background, their cognitive status and with their local dialect.41 During the interview period, the stories get shorter, less detailed and refined. As mentioned, one reason may be that the same stories are told earlier, few new events happen. Their vocabulary seems to shrink somewhat during the progression of the dementia, but it is preserved for all of them to adequately present their experiences and reflections about their life situation. As demonstrated by the citations, they use words and sentences to describe their experiences, including important emotions, habitual strategies, contextualized reactions and evaluations as well as their feelings of the progression of the dementia. This is their narrated existential experience, which may not be in accordance with what “outsiders” – family members or health care personnel – would say is “adequate” or “realistic”. Their narratives are essential in their way of handling progressive dementia.44
To find a positive way of looking at life when experiencing progressing dementia, ending in death, is one of the most demanding coping challenges people can face. The stories are highly consistent and continuous concerning their main coping styles. The significant transitions they emphasize are few, in accordance with what they find important related to their identity. Certainly, to receive a diagnosis of dementia in mid-life is experienced as a great and dramatic transition, met with strong emotional reactions. They “fell down”, “cried and cried.” However, already at the first interview, 3–6 months after the diagnosis, most of them had made a reorientation in life, were in an adaptation process, and expressed the coping strategies they were using. The informants use both problem-focused and emotional-focused coping strategies,52 or what has been denoted by Heckhausen and Schulz53 as primary and secondary control. The first has been considered as “active” coping, changing the stressing situation, the other “passive”, modifying personal reactions.
Repeatedly, the participants expressed a rather coherent adaptation strategy of coping with the progression of dementia, a situation they cannot change. They adapt their cognitive and emotional reactions. They will live in “the here and now”, take one day at a time, and avoid the thoughts and situations that remind them of the negative and depressing progression of the disease. They even try to refrain from thinking about the disease. As shown, one woman does not accept the diagnosis, and a man has “just a hint of dementia” several years after the diagnosis.
The context, the culture and other people’s reactions to dementia, is important to their coping strategies. The participants are well aware of the stigma of dementia, as other studies and reports from people with dementia have documented.4,47,54,55 To avoid stigmatization and social exclusion, they present their memory problems as “forgetfulness” – more socially acceptable. Some of the eldest choose “older people” as their reference group since forgetfulness is associated with getting older.
The participants decide to look at the bright side of life and to value the resources they have and the positive aspects of their lives – in other words, to live well with dementia, which is also the slogan of the British National Dementia Strategy.19 A few mentioned that they have to accept what will come as a part of a full life, with both good and bad days – a meaning-focused strategy. They use selective ignoring in response to the stress and avoid being reminded of a frightening future.56 In this way, they practice proactive coping57 and practice self-regulation.36 The way some of the participants avoid courses and meetings for people with dementia, as well as stressing social gatherings, illustrates coping by avoidance. The strategy may be seen as active coping, even if it does not change the basic cause – the disease. It lessens the social consequences. But they also actively participate in activities in new and safe social surroundings, like in supported living, tailored to their resources.
Some participants point to personality traits. They mention that they have always been in a good mood, with an optimistic outlook on what happens.58 Research has established that optimism minimizes the risks for several diseases and depressive symptoms,59 increasing longevity.60 Individuals can change their mind-set.61 We find that people with YOD have done that, to preserve positive ageing for as long as possible.29,62
One of the most significant transitions described by the participants is giving up a job involuntarily. Only one person was still in job at the start of the project, some others told about their reactions to retiring in retrospect. The loss of work is a radical break in the normal expected life course for younger people,63 falling out of step with their age-mates. To try to accept and accommodate to the message that they are not proficient enough to perform their former job, which represents a central identity, seems to be very difficult.29 Loss of job is not presented as a main transition here, since our study is prospective of what happens after the diagnosis, not a retrospective life history study.
Another central transition was the experience of one of the implications of dementia – losing one’s driver’s license – an unexpected finding. Two persons mentioned that. The loss is felt as a crisis and a dramatic shift in life – meaning a loss of mobility, freedom and connectedness. We had not fully understood how a good social life in rural areas depends on driving a car.
During the progression of dementia, the participants are modifying or reducing goals for the future64 as a way of performing proactive coping. They plan for some “last time event”. They may give up goals like planning a trip abroad and accept that travelling close to home may also be nice. Or they admit that their plans to take up former hobbies will probably not happen because they are “lacking the energy” or the abilities. Their method of social coping is to retract from difficult or destructive social contacts, that are undermining their selves and their self-confidence. We have seen that some participants report becoming more and more isolated and lonely when being on their own; others, in retrospect, later admit a lack of contact at home after having moved into a supported living accommodation or nursing home. They modify their evaluation of former life.
Entering a residential care facility is one of the most feared transitions in later life.29 Five participants moved into supported care accommodations or nursing homes during the project period. We found that they all valued the transition of moving to a nursing home or a supported living accommodation, which gave them social contacts, acceptance as a person with dementia, adapted assistance, and support for their capacities. They felt revitalized after moving into a residential care facility, now more congruent with their abilities. This is also in line with another study.65 Even the man who valued his lonely life in the woods, with animals as his company, after some time felt the joy of human companionship, he found in the nursing home. However, after some time, the stories of the residents in the nursing home seem to become more ambivalent. They more often stress several negative aspects, such as a lack of younger or more-agreeable people, or attention from the personnel. When dementia is progressing and energy is declining, participation and contact with others become more problematic. The participants in later stages differentiate their quality of life; their “outer life” may be mostly okay, but their “inner life” worsens and their capacities shrink.
A review of qualitative studies on the experience for older people of a permanent move into a residential care accommodation,66 found themes of loss and suffering, but also a sense of relief and security, passive acceptance, making the best of available choices, and reframing. Another study emphasized that residents have left not only their homes but also a part of who they are.67 Our study has shown that some single people with YOD have lost a robust feeling of who they are already at home, living in depression and anxiety. That there might be significantly higher levels of well-being among residents than those living at home with dementia in general was reported in a study.65 We have shown how important feelings of support and security in the nursing home are for the informants’ relief and revitalization of their selfhood.
A study emphasizes that there is a need for better understanding by the health care personnel in nursing homes regarding the former habits and interests of persons with dementia.68 This is also true for people with YOD. We have demonstrated the vitalizing effect of support to practice former hobbies and activities, a strengthening of identity. We strongly underline that it is important to hear vulnerable persons’ voices to be able to tailor person-centred care to them, especially in situations with transitions, in line with this study.69
We emphasize that our study has demonstrated that the participants’ use active, persistent and continual coping in the existential situation of unavoidable, progressive dementia and the transitions they meet. They combine a variety of coping strategies – emotional, cognitive and social – and use selective optimization, to protect their selves: In a sum do the best out of it and live here and now. Their efficient coping strategies have preserved a feeling of a good life for a long time. Some participants preserve a feeling of having a good life even at the end. However, for others, this gradually gives way in the last stages of serious dementia.
Strengths and limitations
Our study has been following single people with YOD for an exceptional long time – four years – and got their own stories of their experiences, formulated with their own word. The study attests that people, even in late stages of dementia, are able to inform about their experiences – joys, sorrows and needs.
Performing a longitudinal in-depth study using interviews with people with dementia depends on trust between the informant and the interviewer.70 Trust has laid the foundation of this study and made possible continuing interviews, even when a participant’s dementia has progressed decisively, and the person has moved to a nursing home. The narrated stories are remarkable and rare documents about existential life over a long period with dementia.
The stage of the dementia will influence the narratives people may give, and the progression of the disease restricts the sample and the duration of time that people can be followed. Recruiting subjects shortly after their diagnosis was affirmed made it possible to follow them over a longer period, several into the late-stage dementia. Four persons participated throughout the whole four-year period.
We claim that, even if the sample is small, the themes have broader validity and offer new insights, showing the longitudinal experiences of single people living with YOD. The findings may contribute to a better understanding of how to contribute to the development and organization of services for people with dementia.
People who live in a partnership will have other experiences, such as receiving assistance from their partners. The experiences of old people with dementia will also differ. They will not experience the radical break from a “normal” expected life course in the midst of their life, losing their job and a future of ageing.
The study was conducted in the prosperous Norwegian welfare state characterized by dominant public health care. Research is needed from other contexts with other private and public systems for support for people with dementia.
Conclusion
This longitudinal study shows that people with dementia can talk about their lived experiences, needs and ways of coping with progressing dementia for a long time. They adapt and preserve a feeling of a rather good life through the efficient use of various coping strategies. High-quality public assistance will support coping, quality of life and vitality for a long time during the progression of dementia.
Acknowledgments
The authors wish to thank the participants for sharing their experiences, along with the Research Council of Norway, and Norwegian National Advisory Unit on Ageing and Health, who supported the study through funding. The authors would also like to thank Anne-Lise Eriksen, who transcribed the interviews.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
Marcia CN Dourado is a researcher funded by the National Council for Scientific and Technological Development (NCPq). The authors report no other conflicts of interest in this work.
References
1. Engedal K, Laks J. Forekomst av og risikofaktorer for demenssykdom i ung alder [Occurrence of and risk factors for dementia at a young age]. In: Johannessen A, Barca ML, Engedal K, Haugen P, editors. Yngre Personer Med Demens [Younger People with Dementia]. Tønsberg: Forlaget Aldring og helse [Publisher Ageing and Health]; 2017:31–39.
2. Zhu XC, Tan L, Wang HF, et al. Rate of early onset Alzheimer’s disease: A systematic review and meta-analysis. Ann Transl Med. 2015;3(3):38.
3. Prince M, Bryce R, Albanese E, Wimo A, Ribeiro W, Ferri CP. The global prevalence of dementia: A systematic review and metaanalysis. Alzheimers Dement. 2013;9(1):63–75.e62. doi:10.1016/j.jalz.2012.11.007
4. Johannessen A, Engedal K, Haugen PK, Dourado MCN, Thorsen K. “To be, or not to be”: experiencing deterioration among people with young-onset dementia living alone. Int J Qual Stud Health Well-Being. 2018;13(1):1490620. doi:10.1080/17482631.2018.1490620
5. Thorsen K, Dourado MCN, Johannessen A. Developing dementia: the existential experience of the quality of life with young-onset dementia - A longitudinal case study. Dementia. Epub 2018 Jul 30 .
6. Borley G, Sixsmith J, Church S. How does a woman with alzheimer’s disease make sense of becoming cared for? Dementia. 2016;15(6):1405–1421. doi:10.1177/1471301214561647
7. Koedam EL, Pijnenburg YA, Deeg DJ, et al. Early-onset dementia is associated with higher mortality. Dement Geriatr Cogn Disord. 2008;26(2):147–152. doi:10.1159/000149585
8. Spreadbury JH, Kipps C. Measuring younger onset dementia: what the qualitative literature reveals about the ‘lived experience’ for patients and caregivers. Dementia. 2017;18(1):135–156. https://doi.org/10.1177/1471301216684401
9. Johannessen A, Moller A. Experiences of persons with early-onset dementia in everyday life: A qualitative study. Dementia. 2013;12(4):410–424. doi:10.1177/1471301211430647
10. Haugen PK. Demens Før 65 År. Fakta, Utfordringer Og Anbefalinger [Dementia Befor the Age of 65 Years. Facts, Demands and Suggestions]. Tønsberg: Forlaget Aldring og helse [Publisher Ageing and Health]; 2012.
11. Caddell LS, Clare L. The impact of dementia on self and identity: A systematic review. Clin Psychol Rev. 2010;30(1):113–126. doi:10.1016/j.cpr.2009.10.003
12. Manthorpe J, Samsi K, Campbell S, et al. From forgetfulness to dementia: clinical and commissioning implications of diagnostic experiences. Br J Gen Pract. 2013;63(606):e69–75. doi:10.3399/bjgp13X660805
13. Norberg A. Identitetsverdighet hos personer med demens [Identity worthiness of people with dementia]. Demens & Alderspsykiatri. 2016;20(4):26–29.
14. Tranvåg O. I verdighetens navn” - om verdighetsbevarende omsorg for personer med demens [In the name of dignity” - about the preservation of dignity for persons with dementia]. Demens & Alderspsykiatri. 2017;21(1):35–39.
15. Patterson KM, Clarke C, Wolverson EL, et al. Through the eyes of others - the social experiences of people with dementia: a systematic literature review and synthesis. Int Psychogeriatr. 2018;30(6):791–805. doi:10.1017/S1041610216002374
16. Roach P, Drummond N. ‘It’s nice to have something to do’: early-onset dementia and maintaining purposeful activity. J Psychiatr Ment Health Nurs. 2014;21(10):889–895. doi:10.1111/jpm.12154
17. Robinson L, Gemski A, Abley C, et al. The transition to dementia-individual and family experiences of receiving a diagnosis: A review. Int Psychogeriatr. 2011;23(7):1026–1043. doi:10.1017/S1041610210002437
18. Helse- og omsorgsdepartementet [Ministry of Health and Care Services]. Dementia Plan 2015. Oslo: Norwegian Ministry of Health and Care Services; 2015.
19. Health Do. Living Well with Dementia: A National Dementia Strategy. Department of Health and Social Care: London; 2009.
20. International AsD. Dementia: A Public Health Priority. World Health Organization (WHO); 2012.
21. Miranda-Castillo C, Woods B, Orrell M. People with dementia living alone: what are their needs and what kind of support are they receiving? Int Psychogeriatr. 2010;22(4):607–617. doi:10.1017/S104161021000013X
22. Luppa M, Luck T, Weyerer S, Konig HH, Brahler E, Riedel-Heller SG. Prediction of institutionalization in the elderly: A systematic review. Age Ageing. 2010;39(1):31–38. doi:10.1093/ageing/afp202
23. Frank C, Forbes RF. A patient’s experience in dementia care: using the “lived experience” to improve care. Can Fam Physician. 2017;63(1):22–26.
24. Chemali Z, Schamber S, Tarbi E, Acar D, Avila-Urizar M. Diagnosing early onset dementia and then what? A frustrating system of aftercare resources. Int J Gen Med. 2012;5:81–86. doi:10.2147/IJGM.S26523
25. Svanstrom R, Sundler AJ. Gradually losing one’s foothold-a fragmented existence when living alone with dementia. Dementia. 2015;14(2):145–163. doi:10.1177/1471301213494510
26. Rostad D, Hellzén O, Enmarker I. The meaning of being young with dementia and living at home. Nurs Rep. 2013;3:1. doi:10.4081/nursrep.2013.e3
27. Mayrhofer A, Mathie E, McKeown J, Bunn F, Goodman C. Age-appropriate services for people diagnosed with young onset dementia: A systematic review. Aging Ment Health. 2018;22(8):927–935. doi:10.1080/13607863.2017.1334038
28. Giele JZ, Elder GH. Methods of Life Course Research. London: Sage Publications; 1998.
29. Robertson G. Transitions in later life: a review of the challenges and opportunities for policy development. Working Older People. 2014;18(4):186–196. doi:10.1108/WWOP-08-2014-0022
30. Schlossberg NK, Waters EB, Goodman J. Counseling Adults in Transition: Linking Practice with Theory. New York: Springer Publishing Company; 1995.
31. Hansen T, Slagsvold B. Alder og livskvalitet [Age and quality of life]. In: Næss S, Moum T, Eriksen J, editors. Research on the Good Life. Bergen: Fagbokforlaget [Publisher Fagbok]; 2011
32. Baltes M, Carstensen L. The process of successful aging: selection, optimization and compensation. In: Baltes M, Carstensen L, editors. Understanding Human Development. Heidelberg: Springer; 2003:81–104.
33. Baltes P, Baltes M. Psychological perspectives on successful aging: the model of selective optimization with compensation. In: Baltes P, Baltes M, editors. Successful Aging: Perspectives from the Behavioral Sciences. New York: Cambridge University Press; 1990:1–31.
34. Bonanno G. Loss, trauma, and human resilience: have we underestimated the human capacity to thrive after extremely aversive events? Am Psychologist. 2004;59(1):20–28. doi:10.1037/0003-066X.59.1.20
35. Atchley RC. A continuity theory of normal aging. Gerontologist. 1989;29(2):183–190. doi:10.1093/geront/29.2.183
36. Brandstädter J. Goal pursuit and goal adjustment: self-regulation and intentional self-development in changing developmental contexts. Adv Life Course Res. 2009;14(1–2):52–62. doi:10.1016/j.alcr.2009.03.002
37. Smith G, Hayslip B. Resilience in adulthood and later life: what does it mean and where are we heading? Annu Rev Gerontol Geriatr. 2012;32(1). doi:10.1891/0198-8794.32.3
38. Wiles JL, Wild K, Kerse N, Allen RES. Resilience from the point of view of older people: ‘There’s still life beyond a funny knee’. Soc Sci Med. 2012;74(3):416–424. doi:10.1016/j.socscimed.2011.11.005
39. Gallacher J, Mitchell C, Heslop L, Christopher G. Resilience to health related adversity in older people. Qual Ageing Older Adults. 2012;13(3):197–204. doi:10.1108/14717791211264188
40. Brandstädter J. The Resiliency of the Aging Self: Strategies and Mechanisms of Adaptation. Amsterdam: European Congress of Gerontology; 1995.
41. Uri H. Hvem Sa Hva? Kvinner, Menn Og Språk. Oslo: Gyldendal; 2018.
42. Denzin N, Lincoln Y. The SAGE Handbook of Qualitative Research. London: Sage Publications Ltd; 2011.
43. Solomon P, Nixon S, Bond V, Cameron C, Gervais N. Two approaches to longitudinal qualitative analyses in rehabilitation and disability research. Disabil Rehabil. 2019;1–7. doi:10.1080/09638288.2019.1602850
44. Chase SE. Still the field in the making. In: Denzin N, Lincoln YS, editors. The Sage Handbook of Qualitative Research. London: Sage; 2011:421–434.
45. Corbin J, Strauss A. A Basics of Qualitative Research. Los Angeles CA: Sage Publications Ltd; 2008.
46. World Medical Association. Declaration of helsinki; 2013. http://www.wma.net/en/30publications/10policies/b3/index.html. Accessed May 15, 2019.
47. Taylor R. Alzheimer’s from the inside Out. Baltimore: Health Professions Press; 2007.
48. de Baggio T. Losing My Mind: An Intimate Look at Life with Alzheimer’s Disease. New Yoek: Free Press; 2002.
49. de Baggio T. When It Gets Darker: An Enlightened Reflection on Life with Alzheimer’s. New York: Free Press; 2003.
50. Voris E, Shabahangi N, Fox P. Conversation with Ed: Waiting for Forgetfulness. Why are We so Afraid of Alzheimer’s Disease? San Fransisco: Elders Academy Press; 2009.
51. Rose L. Larry’s Way: Another Look at Alzheimer’s from the Inside. New York: iUniverse Inc; 2003.
52. Folkman S, Lazarus RS. An analysis of coping in a middle-aged community. J Health Soc Behav. 1980;21(3):219–239.
53. Heckhausen J, Schulz R. A life-span theory of control. Psychol Rev. 1995;102(2):284–304.
54. Behuniak S. The living dead? The construction of people with alzheimer’s disease as zombies. Ageing Soc. 2011;31:1. doi:10.1017/S0144686X10000693
55. Aquilina C, Hughes J. The return of living dead. Agency lost and found? In: Hughes J, Louw S, Sabat S, editors. Dementia: Mind, Meaning, and the Person. Oxford: Oxford University Press; 2006:143–161.
56. Pearlin LI, Schooler C. The structure of coping. J Health Soc Behav. 1978;19(1):2–21.
57. Bode C, de Ridder DT, Kuijer RG, Bensing JM. Effects of an intervention promoting proactive coping competencies in middle and late adulthood. Gerontologist. 2007;47(1):42–51. doi:10.1093/geront/47.1.42
58. Kim E, Park N, Peterson C. Dispositional optimism protects older adults from stroke: the health and retirement study. Stroke. 2011;42(10):2855–2859. doi:10.1161/STROKEAHA.111.613448
59. Giltay EJ, Zitman FG, Kromhout D. Dispositional optimism and the risk of depressive symptoms during 15 years of follow-up: the zutphen elderly study. J Affect Disord. 2006;91(1):45–52. doi:10.1016/j.jad.2005.12.027
60. Diener E, Chan M. Happy people live longer: subjective well‐being contributes to health and longevity. Applied Psychol. 2011;3(1):1–43.
61. Seligman M. Learned Optimism: How to Change Your Mind and Your Life. Vintage. The New York Times Book Review Vintage Books: Vintage; 2006.
62. Robertson G. How to Age Positively: A Handbook for Personal Development in Later Life. Bristol: Positive Ageing Associates; 2013.
63. Hagestad G. Interdependent lives and relationships in changing times. A life course view of families and aging. In: Setters R, editor. Invitation to the Life Course: Toward New Understandings in Later Life. New York: Baywood Publishing Company Inc.; 2003:297–307.
64. Brandtstädter J, Rothermund K, Kranz D, Kühn W. Final decentrations: personal goals, rationality perspectives, and the awareness of life’s finitude. Eur Psychol. 2010;15(2):152–163. doi:10.1027/1016-9040/a000019
65. Böckerman P, Johansson E, Saarni S. Institutionalisation and subjective wellbeing for old-age individuals: is life really miserable in care homes? Ageing Soc. 2012;32(7):1176–1192. doi:10.1017/S0144686X1100081X
66. Lee DT, Woo J, Mackenzie AE. A review of older people’s experiences with residential care placement. J Adv Nurs. 2002;37(1):19–27.
67. Heliker D, Scholler-Jaquish A. Transition of new residents to long-term care: basing practice on residents’ perspective. J Gerontol Nurs. 2006;32(9):34–42.
68. Cronfalk BS, Norberg A, Ternestedt BM. They are still the same - family members’ stories about their relatives with dementia disorders as residents in a nursing home. Scand J Caring Sci. 2018;32(1):168–176. doi:10.1111/scs.12442
69. Rustad EC, Furnes B, Cronfalk BS, Dysvik E. Older patients’ experiences during care transition. Patient Prefer Adherence. 2016;10:769–779. doi:10.2147/PPA.S97570
70. Kvale S, Brinkmann S. Det Kvalitative Forskningsintervju [The Qualitative Research Interview]. Oslo: Gyldendal akademisk [Gyldendal academic]; 2009.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.