")
Back to Journals » Local and Regional Anesthesia » Volume 13
Control of Spinal Anesthesia-Induced Hypotension in Adults
Authors Ferré F, Martin C, Bosch L, Kurrek M , Lairez O , Minville V
Received 2 December 2019
Accepted for publication 27 March 2020
Published 3 June 2020 Volume 2020:13 Pages 39—46
DOI https://doi.org/10.2147/LRA.S240753
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Stefan Wirz
Fabrice Ferré,1 Charlotte Martin,1 Laetitia Bosch,1 Matt Kurrek,1,2 Olivier Lairez,3,4 Vincent Minville1
1Department of Anesthesia and Intensive Care Medicine, CHU Purpan, Toulouse, France; 2Department of Anesthesia, University of Toronto, Toronto, ON M5S 3E2, Canada; 3Department of Nuclear Medicine, Toulouse University Hospital, Toulouse Cedex 9 31059, France; 4Department of Cardiology, Toulouse University Hospital, Toulouse Cedex 9 31059, France
Correspondence: Vincent Minville
Department of Anesthesia and Intensive Care Medicine, Purpan University Hospital, Hôpital Purpan, Place du Dr Baylac, TSA 40 031, Toulouse Cedex 9 31059, France
Email [email protected]
Abstract: Spinal anesthesia-induced hypotension (SAIH) occurs frequently, particularly in the elderly and in patients undergoing caesarean section. SAIH is caused by arterial and venous vasodilatation resulting from the sympathetic block along with a paradoxical activation of cardioinhibitory receptors. Bradycardia after spinal anesthesia (SA) must always be treated as a warning sign of an important hemodynamic compromise. Fluid preloading (before initiation of the SA) with colloids such as hydroxyethyl starch (HES) effectively reduces the incidence and severity of arterial hypotension, whereas crystalloid preloading is not indicated. Co-loading with crystalloid or colloid is as equally effective to HES preloading, provided that the speed of administration is adequate (ie, bolus over 5 to 10 minutes). Ephedrine has traditionally been considered the vasoconstrictor of choice, especially for use during SAIH associated with bradycardia. Phenylephrine, a α1 adrenergic receptor agonist, is increasingly used to treat SAIH and its prophylactic administration (ie, immediately after intrathecal injection of local anesthetics) has been shown to decrease the incidence of arterial hypotension. The role of norepinephrine as a possible alternative to phenylephrine seems promising. Other drugs, such as serotonin receptor antagonists (ondansetron), have been shown to limit the blood pressure drop after SA by inhibiting the Bezold–Jarisch reflex (BJR), but further studies are needed before their widespread use can be recommended.
Keywords: spinal anesthesia, arterial hypotension, vasopressor, phenylephrine, ondansetron
Introduction
The maintenance of arterial blood pressure is felt to be important to ensure adequate regional perfusion. While spinal anesthesia (SA) may confer significant benefits when compared to general anesthesia, it is frequently associated with arterial hypotension. The aim of this article is to review the mechanisms responsible for spinal anesthesia-induced hypotension (SAIH) as well as to discuss the different approaches to prevent and treat SAIH.
Mechanisms of Arterial Hypotension
While the cardiovascular effects of SA are proportionate to the extent of the associated sympathetic block the extent of the resulting sympathetic block can vary significantly between individual patients.
Effect of SA on the Resistive and Capacitive Vascular Systems
The sympathetic block created by SA rapidly leads to arterial and arteriolar vasodilation in the regions concerned which in turn leads to an augmentation of sympathetic arterial vascular tone in the regions not subject to the block through a baroreflex. These compensatory mechanisms are generally more effective in younger patients.1
The hemodynamic consequences of SA also result in a sympathetic block of the venous reservoir2 which then leads to pooling of blood in the capacitance vessels in the lowermost regions.3 When the level of the sensory block is higher than or equal to T6, this pooling in the hepatosplanchnic region can affect up to 20% of the circulating blood volume and this volume can be mobilized by the use of vasopressors.
Effects of SA on the Cardiac System
SA leads to bradycardia and a drop in blood pressure by causing a sympathovagal imbalance in favor of the parasympathetic tone. This bradycardia/hypotension could represent a dysregulation of cardiovascular function or could alternatively be interpreted as an adaptive response (lengthening of the duration of diastole to promote ventricular filling).
Physiologically, it is well established that the cardioinhibitory receptors of the Bezold–Jarisch reflex (BJR), in conjunction with the aortic and carotid baroreceptors, participate in the regulation of arterial blood pressure.4 In conditions of moderate hypovolemia, the activity of the BJR is lowered with a concomitant stimulation of the baroreflex leading to an increase in arterial blood pressure. In conditions of severe hypovolemia like profound hemorrhage, a brutal drop in venous return leads to a paradoxical activation of the BJR with a sustained hypotension and bradycardia, the latter could be an adaptative mechanism to preserve diastolic filling time.5
Approximately 13% of non-obstetrical patients experience bradycardia during SA,6 generally without significant consequences as long as corrective measures are immediately taken.7 However severe bradycardia can rapidly progress to asystole8 and bradycardia induced by SA should therefore always be considered a warning sign of an impending hemodynamic collapse.
Studies of cardiac output under SA have shown a biphasic effect of SA: cardiac output initially increases due to a decrease in afterload through arterial vasodilatation (reaching a maximum after about 7 minutes), and subsequently decreases secondary to a decrease in preload.9,10 This decrease in cardiac output is one of the determinants for the decrease in arterial blood pressure observed in 15% to 50% of patients.
In the elderly, age-related changes (alteration in systolic function, diastolic relaxation) can aggravate the decrease in cardiac output in this setting.11–14
Arterial Hypotension
The consequence of the effects of SA on the cardiovascular system is the occurrence of arterial hypotension. Intraoperative arterial hypotension has been linked to an increase in patient mortality and morbidity.15,16 In the literature, the most commonly used definition for SAIH is a systolic arterial blood pressure less than 80% of the baseline. The incidence of SAIH increases with age, being about 36% of younger patients and increasing to 75% of patients over the age of 50.17 Even with low doses (ie, 7.5 mg of bupivacaine), the incidence of SAIH remains high in older patients.12 Furthermore, SAIH can be amplified by an impairment of mechanisms of homeostasis; even more so in patients with an altered neuro-humoral regulation of cardiac function, with a rapid extension of the block, or simultaneously administered sedation (increased dysautonomia).
Control of Arterial Blood Pressure
Unilateral SA
Even if recently the dose in SA was drastically reduced,9,18 In orthopedic surgery, SA can be lateralized to the side to be operated on in order to create a predominantly unilateral sympathetic bloc and thus to minimize its hemodynamic consequences.19,20 This can be particularly helpful in patients at higher risk of SAIH (ie, elderly patients). This can be achieved by injecting the local anesthetic with the orifice of the needle towards the side to be operated on and by placing the patient in the lateral decubitus position (for hyperbaric solutions the limb to be operated on would be towards the bottom, and for hypobaric solutions with the limb to be operated on towards the top). This position should then be maintained for approximately 20 minutes until a predominantly unilateral block is obtained. Bupivacaine remains one of the most commonly used local anesthetics for SA with doses recommended between 3.5 and 8 mg when used this way.21 One of the major drawbacks of any techniques using a small-dose single injection is the risk of an insufficiently high block or the block wearing off prematurely.
Titrating SA
One possible approach is the use of a spinal catheter through which it is possible to titrate the local anesthetic, thus allowing some control over both the extent and the rapidity of onset of the associated sympathetic block.22–25 Compared with conventional SA, titrating SA induces less hypotension and reduces the need for vasopressor agents, in comparison to even low dose single shot SA.22–24,26 Such a use of spinal catheters has been described with the use of a small size Tuohy needle via paramedian approach27 and by inserting the catheter no more than 2 centimetres into the intrathecal space.28 The local anesthetic (2.5 mg of isobaric bupivacaine) is then injected and can be re-administered every 15 minutes so as to obtain a sufficient sensory level. The resulting hemodynamic profile is more stable compared to both a traditional spinal and general anesthesia,23,24 even in higher-risk patients where it resulted in fewer hypotensive episodes and less myocardial ischemia than the other anesthetic techniques.
The size of the needle during puncture of the spinal canal has been shown to be an important predictor of post-dural-puncture headaches and since this technique uses a relatively large Tuohy needle, the possibility of a post-dural-puncture headache is expected to be much higher when compared to a traditional SA. However, since this technique is used mostly used in elderly patient (due to their increased risk of SAIH), the increase in post-dural-puncture headaches may not be clinically significant, since elderly patients are much less prone to this complication and the overall risk/benefit profile may be favourable for this patient population.
The Effect of Circulating Blood Volume and Body Position
Pre-existing hypovolemia can lead to cardiovascular collapse during SA29 and putting the patient level from Trendelenburg can precipitate a cardiac arrest.30 The possible cephalad extension of any hyperbaric solution must be carefully considered and its hemodynamic effects anticipated. In the parturient, the left lateral tilt position (5–10°) after SA favours venous return by limiting aortocaval compression by the gravid uterus.31
Fluid Loading
The type and amount of intravenous fluid must take into account the effects of the sympathetic block, the patient’s volume status before the SA as well as any intraoperative and postoperative fluid losses.
In obstetrical patients, during caesarean section, fluid loading (FL) is frequently used either alone (44%) or in association with a vasopressor (53%).32 Different types of iv fluid and the timing of its administration have been studied.33 While crystalloid preloading (ie, before the SA) is ineffective and not clinically indicated, colloid preloading (using hydroxyethyl starch, HES) can effectively reduce the incidence and severity of maternal hypotension34 decrease the quantity of vasopressors required.35 HES co-loading is as effective as HES preloading, when administered rapidly after placing the SA (within 5 to 10 minutes). Crystalloid co-loading is a less costly alternative, but its effectiveness appears to be less, especially when administered at slower speeds. For some special clinical cases, such as patient with pre-eclampsia FL should only be performed as absolutely necessary (after onset of SA) in order to avoid fluid overload.34 For fluid loading, studies showed that crystalloid co-loading reduced the incidence of hypotension in SA for cesarean delivery.36 As crystalloids are more widely used, without the disadvantages related to colloids, like allergic reactions, coagulation changes and cost.
Atropine
Atropine is widely used to treat bradycardia but little data are available concerning its use to prevent SAIH. Lim et al have investigated atropine (given intravenously 1 min after SA) and shown a dose-dependent increase in heart rate and reduction in the need for vasopressors.35 Although routine pretreatment with atropine in patients undergoing SA is not recommended at this time, small-dose atropine (5 μg/Kg) may help in patients with low baseline heart rate or in patients who are hypotensive and relatively bradycardic after SA.
Ephedrine
Ephedrine has for a long time been considered the standard vasoconstrictor for SAIH.37 It is sympathomimetic amine acting directly on both α- and β- adrenergic receptors as well as indirectly by increasing the release of endogenous catecholamine (norepinephrine). Since the storage of endogenous norepinephrine is depleted in patients under long-term treatment with ACE inhibitors (or angiotensin II receptor antagonists) the effects of ephedrine in those patients can be diminished. This lead to the proposal that these patients would benefit from the use of a direct-acting sympathomimetic drug, such as phenylephrine37–39 or even adrenaline. The pharmacodynamics of phenylephrine (a pure α- adrenergic agonist) along with its lack of placental transfer and effect on foetal metabolism make it the vasoconstrictor of choice (see next section), while ephedrine remains the recommended treatment for patients with parasympathetic hyperactivity (bradycardia associated with hypotension).4
Phenylephrine
Phenylephrine, a direct-acting α (1)-adrenergic receptor agonist, has largely been used to treat intraoperative arterial hypotension. Even though physiological studies suggest that the use of α-adrenergic agonists increases cardiac afterload and reduces venous compliance,40 the effect of phenylephrine on cardiac output is very dependent on the starting conditions of venous return.41 If left ventricular function is normal, an increase in left ventricular afterload has only a small effect on cardiac output. If the intravascular volume status of the patient is good, phenylephrine can mobilize volume and increase venous return which in turn increase cardiac output42 according to Starling’s law.43 However, if the patient’s sympathetic tone is already increased, then the volume in the venous capacitance vessels has already been recruited, and phenylephrine can actually increase arterial resistance and diminish cardiac output especially if the patient has an impairment of cardiac function.42
However, numerous publications report the use of phenylephrine to treat or prevent hypotension during SA.
Different modes of administering phenylephrine have been tested. Compared to rescue administration (ie, a bolus of 100 μg phenylephrine each time the systolic blood pressure drops below 80% of base-line), the prophylactic administration of phenylephrine (ie, immediately after the intrathecal injection of local anesthetic to maintain a systolic blood pressure of at least 80% of base-line) often leads to higher phenylephrine use and better prevention of arterial hypotension in the parturient as in the elderly.11,34,44,45 Among the prophylactic administration regimens, fixed-rate continuous infusions, as compared to repeated boluses, do not appear to be beneficial.46 A variable rate, prophylactic infusion of phenylephrine leads to greater hemodynamic stability, less nausea and vomiting, and reduced the number of interventions required to maintain blood pressure.47 Closed-loop computer-controlled continuous infusion of phenylephrine has also been studied and shown to lead to better control of blood pressure than manually controlled continuous infusion.48
In conclusion, the prophylactic administration of phenylephrine (ie, immediately after intrathecal injection) by continuous, rate adjusted intravenous infusion of phenylephrine appears optimal to limit the decrease in blood pressure after SA. Alternatively, a fixed rate of 50 μg/minute (with repeated boluses of 100 μg for a blood pressure below 80% of the base-line) appears to be acceptable. Should neither of these two options be feasible, then the clinician could choose prophylactic treatment with repeated boluses of phenylephrine.34,44,47
Norepinephrine
Phenylephrine is a potent and pure α-adrenergic receptor agonist (without acting on β-adrenergic receptors), its use has been linked to a dose-dependent slowing of heart rate, and even a decrease in cardiac output (see discussion above). Some authors have therefore proposed norepinephrine because it has, an additional weak β-adrenergic receptor agonist activity. Ngan Kee et al recently published the results of a randomized controlled trial comparing norepinephrine with phenylephrine to maintain arterial blood pressure of parturients scheduled for elective caesarean sections under SA.49 Computer-controlled continuous infusion of norepinephrine (5 μg/mL) was equally effective to phenylephrine in controlling blood pressure, but lead to less bradycardia and decrease in cardiac output (albeit with no difference in neonatal outcome) due to the activity of norepinephrine on β-adrenergic receptors. A range from 0.07 to 0.08 μg kg−1 min−1 norepinephrine infusion may be optimum for initiating norepinephrine infusions for preventing SAH for cesarean section.50,51
Further studies are necessary before it can be considered that norepinephrine is preferable to phenylephrine for the prevention of SA induced hypotension. It is not yet the time for a paradigm shift as to the choice of vasopressor agent52–54 even if some preliminary results are interesting.55
Serotonin Antagonists
During SA, arterial hypotension and bradycardia have sometimes been observed to be related to the activation of the cardioinhibitory receptors via the BJR4,5 and chemoreceptors, activated by the serotonin (ie, 5-hydroxytryptamine (5-HT)), from circulating platelets, have been implicated in this setting. Animal studies have revealed that serotonin could be one of the factors favouring the BJR in the case of hypovolemia by activating peripheral Type 3 receptors located on intracardial vagal nerve terminations.56 Indeed, the administration of serotonin activated the BJR in rats, which was further antagonized by a blockade of 5-HT3 receptors.57
In humans, a single case report of asystole occurring during SA which responded to atropine and ondansetron (a serotonin 5-HT3 receptor antagonist) lead to considering the possible relation between the BJR and the serotonergic and cholinergic receptors in the afferent and efferent fibers of this vagally mediated reflex during SAIH.58 Several authors have since proposed the administration of ondansetron in order to limit the hypotension and bradycardia induced by SA. But it is worth noting that while the injection of 4 to 8 mg of ondansetron several minutes before SA has been shown to limit the decreases in blood pressure, a decrease in the incidence of SAIH has never clearly been demonstrated.59–62 A meta-analysis published by Gao et al in 2015, which included 10 randomized controlled studies, suggested that a prophylactic injection of ondansetron may be beneficial.63 However since then, two publications, one in parturients64 and the other in patients over 70 years old,61 have failed to show.
Even if the values of arterial blood pressure seem better with the administration of ondansetron, the tendency to privilege the control of directly measurable variables, such as arterial blood pressure, rather than non-measurable but otherwise essential variables, such as tissue oxygenation, presents a tangible bias.65
A recent study has shown that intravenous ondansetron 4 mg reduced the ED50 of a prophylactic phenylephrine infusion by approximately 26% in patients undergoing cesarean delivery under combined spinal-epidural anesthesia.66
In summary, further studies are necessary before ondansetron can be recommended for the prevention of SAIH.
Cafedrine and Theodrenaline
In Germany, a combination of cafedrine (covalently linked norephedrine and theophylline) and theodrenaline (covalently linked noradrenaline and theophylline) called Akrinor® is used for the treatment of hypotension in adults that occurs during emergency situations, especially during cesarean sections.67
German anesthesiologists often use cafedrine/theodrenaline and have gained a lot of practical experience with the substance. 86.2% of German hospitals use cafedrine/theodrenaline for the treatment of hypotension during regional anesthesia for cesarean section.68
Cafedrine/theodrenaline can be administered via bolus while catecholamines normally need to be diluted and administered via syringe pumps. Bolus injection is faster, which may be beneficial in emergency situations. Sole administration of theodrenaline increases vascular resistance, while cafedrine exhibits an inotropic effect.69 By administering the two substances in combination the optimal ratio of cafedrine and theodrenaline can be used. Sakai et al tested different ratios in dogs and rats and concluded that 20:1 is the ideal ratio for both a rapid onset and a long-lasting hypertensive effect.70
Also, this drug combination has a very good safety record, as it has been used widely in Germany since the 1960s. However, it should be noted that there are only few safety data from controlled trials available.
The drug strategies for the control of spinal anesthesia-induced hypotension (SAIH) in adults are summarized in Table 1.
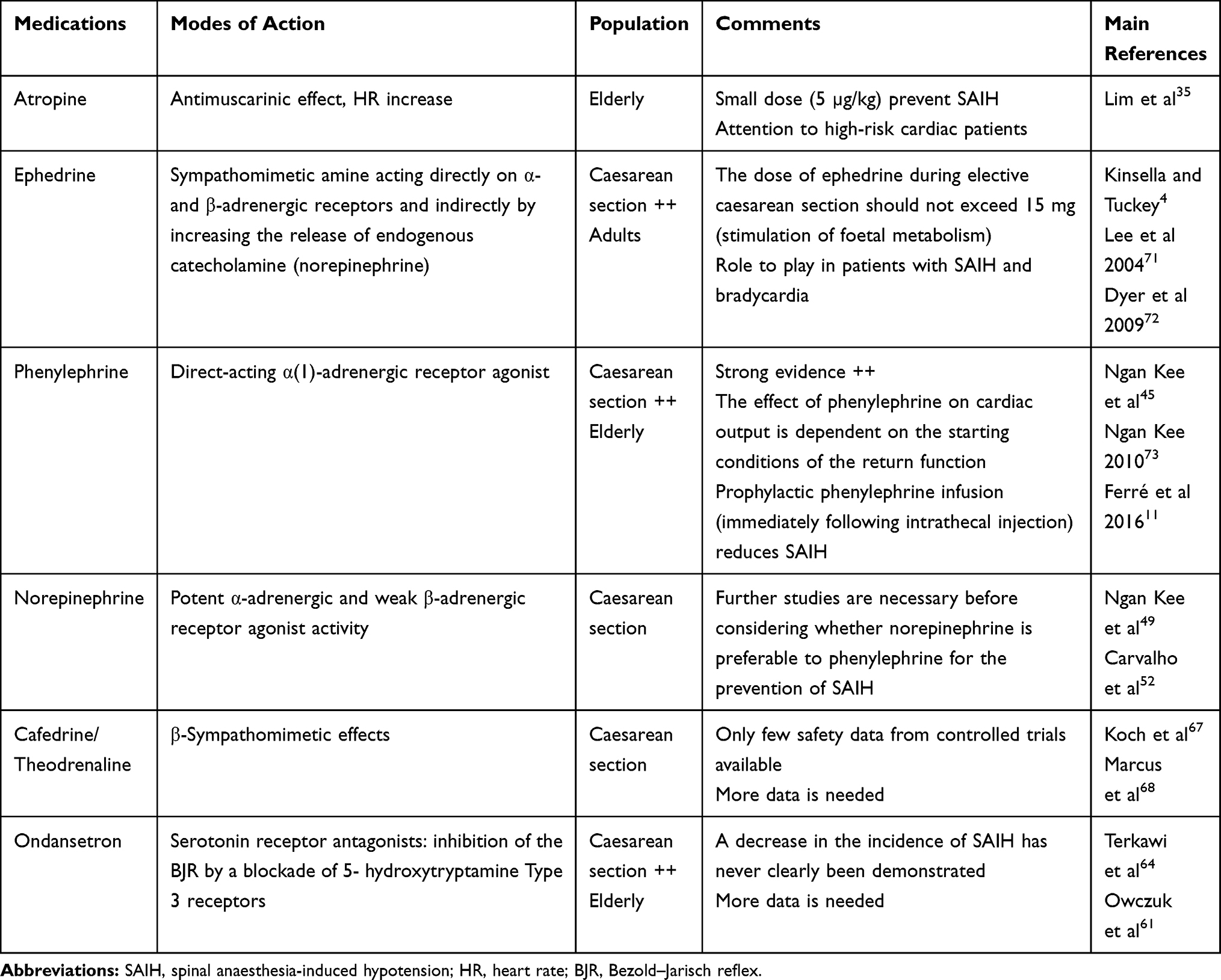 |
Table 1 Drug Strategies for the Control of Spinal Anaesthesia-Induced Hypotension (SAIH) in Adults |
Conclusion
Spinal anesthesia-induced hypotension (SAIH) is frequently occurring, particularly in the elderly and in the parturient undergoing caesarean section. Several strategies for decreasing its incidence have been studied, but no one measure has been sufficiently effective. Contrary to co-loading, crystalloid preloading (ie, before the SA) is not effective. Phenylephrine is currently the standard vasopressor agent. Its prophylactic injection (ie, immediately after the intrathecal injection) by continuous intravenous infusion (at fixed or adjusted rate) or by way of titrating repeated boluses limits the incidence of SAIH observed in this setting. More data are needed before serotonin receptor antagonists, such as ondansetron, can be recommended for the prevention of arterial hypotension. Whatever strategy is to be used, bradycardia induced by SA must always be considered as a warning sign of a critical hemodynamic situation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Arndt JO. The low pressure system: the integrated function of veins. Eur J Anaesthesiol. 1986;3(5):343–370.
2. Butterworth JF, Piccione W, Berrizbeitia LD, Dance G, Shemin RJ, Cohn LH. Augmentation of venous return by adrenergic agonists during spinal anesthesia. Anesth Analg. 1986;65(6):612–616. doi:10.1213/00000539-198606000-00009
3. Shimosato S, Etsten BE. The role of the venous system in cardiocirculatory dynamics during spinal and epidural anesthesia in man. Anesthesiology. 1969;30(6):619–628. doi:10.1097/00000542-196906000-00009
4. Kinsella SM, Tuckey JP. Perioperative bradycardia and asystole: relationship to vasovagal syncope and the Bezold-Jarisch reflex. Br J Anaesth. 2001;86(6):859–868. doi:10.1093/bja/86.6.859
5. Campagna JA, Carter C. Clinical relevance of the Bezold-Jarisch reflex. Anesthesiology. 2003;98(5):1250–1260. doi:10.1097/00000542-200305000-00030
6. Carpenter RL, Caplan RA, Brown DL, Stephenson C, Wu R. Incidence and risk factors for side effects of spinal anesthesia. Anesthesiology. 1992;76(6):906–916. doi:10.1097/00000542-199206000-00006
7. Caplan RA, Ward RJ, Posner K, Cheney FW. Unexpected cardiac arrest during spinal anesthesia: a closed claims analysis of predisposing factors. Anesthesiology. 1988;68(1):5–11. doi:10.1097/00000542-198801000-00003
8. Auroy Y, Narchi P, Messiah A, Litt L, Rouvier B, Samii K. Serious complications related to regional anesthesia: results of a prospective survey in France. Anesthesiology. 1997;87(3):479–486. doi:10.1097/00000542-199709000-00005
9. Asehnoune K, Larousse E, Tadié JM, Minville V, Droupy S, Benhamou D. Small-dose bupivacaine-sufentanil prevents cardiac output modifications after spinal anesthesia. Anesth Analg. 2005;101(5):1512–1515. doi:10.1213/01.ANE.0000180996.91358.CC
10. Meyhoff CS, Hesselbjerg L, Koscielniak-Nielsen Z, Rasmussen LS. Biphasic cardiac output changes during onset of spinal anaesthesia in elderly patients. Eur J Anaesthesiol. 2007;24(9):770–775. doi:10.1017/S0265021507000427
11. Ferre F, Marty P, Bruneteau L, et al. Prophylactic phenylephrine infusion for the prevention of hypotension after spinal anesthesia in the elderly: a randomized controlled clinical trial. J Clin Anesth. 2016;35:99–106. doi:10.1016/j.jclinane.2016.07.020
12. Lairez O, Ferre F, Portet N, et al. Cardiovascular effects of low-dose spinal anaesthesia as a function of age: an observational study using echocardiography. Anaesth Crit Care Pain Med. 2015;34(5):271–276. doi:10.1016/j.accpm.2015.02.007
13. Hofhuizen C, Lemson J, Snoeck M, Scheffer G-J. Spinal anesthesia-induced hypotension is caused by a decrease in stroke volume in elderly patients. Local Reg Anesth. 2019;12:19–26. doi:10.2147/LRA.S193925
14. Ferre F, Delmas C, Carrié D, Cognet T, Lairez O, Minville V. Effects of spinal anaesthesia on left ventricular function: an observational study using two-dimensional strain echocardiography. Turk J Anaesthesiol Reanim. 2018;46(4):268–271. doi:10.5152/TJAR.2018.48753
15. Charlson ME, MacKenzie CR, Gold JP, et al. The preoperative and intraoperative hemodynamic predictors of postoperative myocardial infarction or ischemia in patients undergoing noncardiac surgery. Ann Surg. 1989;210(5):637–648. doi:10.1097/00000658-198911000-00012
16. Dalton JE, Kurz A, Turan A, Mascha EJ, Sessler DI, Saager L. Development and validation of a risk quantification index for 30-day postoperative mortality and morbidity in noncardiac surgical patients. Anesthesiology. 2011;114(6):1336–1344. doi:10.1097/ALN.0b013e318219d5f9
17. Graves CL, Underwood PS, Klein RL, Kim YI. Intravenous fluid administration as therapy for hypotension secondary to spinal anesthesia. Anesth Analg. 1968;47(5):548–556. doi:10.1213/00000539-196809000-00018
18. Gentili M, Senlis H, Houssel P, Monnier B, Bonnet F. Single-shot spinal anesthesia with small doses of bupivacaine. Reg Anesth. 1997;22(6):511–514.
19. Casati A, Moizo E, Marchetti C, Vinciguerra F. A prospective, randomized, double-blind comparison of unilateral spinal anesthesia with hyperbaric bupivacaine, ropivacaine, or levobupivacaine for inguinal herniorrhaphy. Anesth Analg. 2004;99(5):. doi:10.1213/01.ANE.0000132972.61498.F1
20. Casati A, Fanelli G. Restricting spinal block to the operative side: why not? Reg Anesth Pain Med. 2004;29(1):4–6. doi:10.1016/j.rapm.2003.09.014
21. Atef H, El-Kasaby A, Omera M, Badr M. Optimal dose of hyperbaric bupivacaine 0.5% for unilateral spinal anesthesia during diagnostic knee arthroscopy. Local Reg Anesth. 2010;3:85–91. doi:10.2147/LRA.S11815
22. Juelsgaard P, Sand NP, Felsby S, et al. Perioperative myocardial ischaemia in patients undergoing surgery for fractured hip randomized to incremental spinal, single-dose spinal or general anaesthesia. Eur J Anaesthesiol. 1998;15(6):656–663. doi:10.1097/00003643-199811000-00006
23. Minville V, Asehnoune K, Delussy A, et al. Hypotension during surgery for femoral neck fracture in elderly patients: effect of anaesthetic techniques. A retrospective study. Minerva Anestesiol. 2008;74(12):691–696.
24. Minville V, Fourcade O, Grousset D, et al. Spinal anesthesia using single injection small-dose bupivacaine versus continuous catheter injection techniques for surgical repair of hip fracture in elderly patients. Anesth Analg. 2006;102(5):1559–1563. doi:10.1213/01.ane.0000218421.18723.cf
25. Lux EA. Continuous spinal anesthesia for lower limb surgery: a retrospective analysis of 1212 cases. Local Reg Anesth. 2012;5:63–67. doi:10.2147/LRA.S35535
26. Favarel-Garrigues JF, Sztark F, Petitjean ME, Thicoïpé M, Lassié P, Dabadie P. Hemodynamic effects of spinal anesthesia in the elderly: single dose versus titration through a catheter. Anesth Analg. 1996;82(2):312–316. doi:10.1097/00000539-199602000-00017
27. Rabinowitz A, Bourdet B, Minville V, et al. The paramedian technique: a superior initial approach to continuous spinal anesthesia in the elderly. Anesth Analg. 2007;105(6):. doi:10.1213/01.ane.0000287655.95619.fa
28. Biboulet P, Jourdan A, Van Haevre V, et al. Hemodynamic profile of target-controlled spinal anesthesia compared with 2 target-controlled general anesthesia techniques in elderly patients with cardiac comorbidities. Reg Anesth Pain Med. 2012;37(4):433–440. doi:10.1097/AAP.0b013e318252e901
29. Bonica JJ, Kennedy WF, Akamatsu TJ, Gerbershagen HU. Circulatory effects of peridural block: 3. Effects of acute blood loss. Anesthesiology. 1972;36(3):219–227. doi:10.1097/00000542-197203000-00006
30. Nishikawa T, Dohi S. [The effects of a small dose of atropine upon sinus bradycardia during spinal anesthesia]. Masui. 1990;39(7):833–838. Japanese.
31. Holmes F. The supine hypotensive syndrome. Its importance to the anaesthetist. Anaesthesia. 1960;15:298–306. doi:10.1111/j.1365-2044.1960.tb13341.x
32. Allen TK, Muir HA, George RB, Habib AS. A survey of the management of spinal-induced hypotension for scheduled cesarean delivery. Int J Obstet Anesth. 2009;18(4):356–361. doi:10.1016/j.ijoa.2009.03.014
33. Mercier FJ. Cesarean delivery fluid management. Curr Opin Anaesthesiol. 2012;25(3):286–291. doi:10.1097/ACO.0b013e3283530dab
34. Mercier FJ, Diemunsch P, Ducloy-Bouthors A-S, et al. 6% Hydroxyethyl starch (130/0.4) vs Ringer’s lactate preloading before spinal anaesthesia for Caesarean delivery: the randomized, double-blind, multicentre CAESAR trial. Br J Anaesth. 2014;113(3):459–467. doi:10.1093/bja/aeu103
35. Lim HH, Ho KM, Choi WY, Teoh GS, Chiu KY. The use of intravenous atropine after a saline infusion in the prevention of spinal anesthesia-induced hypotension in elderly patients. Anesth Analg. 2000;91(5):1203–1206. doi:10.1097/00000539-200011000-00029
36. Ni H-F, Liu H-Y, Zhang J, Peng K, Ji F-H. Crystalloid coload reduced the incidence of hypotension in spinal anesthesia for cesarean delivery, when compared to crystalloid preload: a meta-analysis. Biomed Res Int. 2017;2017:3462529. doi:10.1155/2017/3462529
37. Lee A, Ngan Kee WD, Gin T. A quantitative, systematic review of randomized controlled trials of ephedrine versus phenylephrine for the management of hypotension during spinal anesthesia for cesarean delivery. Anesth Analg. 2002;94(4):. doi:10.1097/00000539-200204000-00028 French.
38. Mercier FJ, Bonnet M-P, la Dorie De A, et al. [Spinal anaesthesia for caesarean section: fluid loading, vasopressors and hypotension]. Ann Fr Anesth Reanim. 2007;26(7–8):688–693. doi:10.1016/j.annfar.2007.05.003.
39. Saravanan S, Kocarev M, Wilson RC, Watkins E, Columb MO, Lyons G. Equivalent dose of ephedrine and phenylephrine in the prevention of post-spinal hypotension in Caesarean section. Br J Anaesth. 2006;96(1):95–99. doi:10.1093/bja/aei265
40. Thiele RH, Nemergut EC, Lynch C. The clinical implications of isolated alpha(1) adrenergic stimulation. Anesth Analg. 2011;113(2):297–304. doi:10.1213/ANE.0b013e3182120ca5
41. Guyton AC. Determination of cardiac output by equating venous return curves with cardiac response curves. Physiol Rev. 1955;35(1):123–129. doi:10.1152/physrev.1955.35.1.123
42. Magder S. Phenylephrine and tangible bias. Anesth Analg. 2011;113(2):211–213. doi:10.1213/ANE.0b013e318220406a
43. Rebet O, Andremont O, Gérard J-L, Fellahi J-L, Hanouz J-L, Fischer M-O. Preload dependency determines the effects of phenylephrine on cardiac output in anaesthetised patients: a prospective observational study. Eur J Anaesthesiol. 2016;33(9):638–644. doi:10.1097/EJA.0000000000000470
44. Mercier FJ, Augè M, Hoffmann C, Fischer C, Le Gouez A. Maternal hypotension during spinal anesthesia for caesarean delivery. Minerva Anestesiol. 2013;79(1):62–73.
45. Ngan Kee WD, Khaw KS, Ng FF, Lee BB. Prophylactic phenylephrine infusion for preventing hypotension during spinal anesthesia for cesarean delivery. Anesth Analg. 2004;98(3). doi:10.1213/01.ANE.0000099782.78002.30
46. Doherty A, Ohashi Y, Downey K, Carvalho JCA. Phenylephrine infusion versus bolus regimens during cesarean delivery under spinal anesthesia: a double-blind randomized clinical trial to assess hemodynamic changes. Anesth Analg. 2012;115(6):1343–1350. doi:10.1213/ANE.0b013e31826ac3db
47. Siddik-Sayyid SM, Taha SK, Kanazi GE, Aouad MT. A randomized controlled trial of variable rate phenylephrine infusion with rescue phenylephrine boluses versus rescue boluses alone on physician interventions during spinal anesthesia for elective cesarean delivery. Anesth Analg. 2014;118(3):611–618. doi:10.1213/01.ane.0000437731.60260.ce
48. Ngan Kee WD, Khaw KS, Lau TK, Ng FF, Chui K, Ng KL. Randomised double-blinded comparison of phenylephrine vs ephedrine for maintaining blood pressure during spinal anaesthesia for non-elective Caesarean section*. Anaesthesia. 2008;63(12):1319–1326. doi:10.1111/j.1365-2044.2008.05635.x
49. Ngan Kee WD, Lee SWY, Ng FF, Tan PE, Khaw KS. Randomized double-blinded comparison of norepinephrine and phenylephrine for maintenance of blood pressure during spinal anesthesia for cesarean delivery. Anesthesiology. 2015;122(4):736–745. doi:10.1097/ALN.0000000000000601
50. Wei C, Qian J, Zhang Y, Chang X, Hu H, Xiao F. Prospective, randomised, double-blind, dose-finding study of norepinephrine for preventing spinal-induced hypotension during caesarean delivery under combined spinal-epidural anaesthesia. Eur J Anaesthesiol. 2020. doi:10.1097/EJA.0000000000001152
51. Fu F, Xiao F, Chen W, et al. A randomised double-blind dose-response study of weight-adjusted infusions of norepinephrine for preventing hypotension during combined spinal-epidural anaesthesia for Caesarean delivery. Br J Anaesth. 2020;124:e108–e114. doi:10.1016/j.bja.2019.12.019
52. Carvalho B, Dyer RA. Norepinephrine for spinal hypotension during cesarean delivery: another paradigm shift? Anesthesiology. 2015;122(4):728–730. doi:10.1097/ALN.0000000000000602
53. Sharwood-Smith G, Drummond GB. Hypotension in obstetric spinal anaesthesia: a lesson from pre-eclampsia. Br J Anaesth. 2009;102(3):291–294. doi:10.1093/bja/aep003
54. Heesen M, Hilber N, Rijs K, et al. A systematic review of phenylephrine vs. noradrenaline for the management of hypotension associated with neuraxial anaesthesia in women undergoing caesarean section. Anaesthesia. 2020;75:800–808. doi:10.1111/anae.14976
55. Singh PM, Singh NP, Reschke M, Ngan Kee WD, Palanisamy A, Monks DT. Vasopressor drugs for the prevention and treatment of hypotension during neuraxial anaesthesia for Caesarean delivery: a Bayesian network meta-analysis of fetal and maternal outcomes. Br J Anaesth. 2019. doi:10.1016/j.bja.2019.09.045
56. Villalón CM, Centurión D. Cardiovascular responses produced by 5-hydroxytriptamine: a pharmacological update on the receptors/mechanisms involved and therapeutic implications. Naunyn Schmiedebergs Arch Pharmacol. 2007;376(1–2):45–63. doi:10.1007/s00210-007-0179-1
57. Yamano M, Kamato T, Nishida A, et al. Serotonin (5-HT)3-receptor antagonism of 4,5,6,7-tetrahydrobenzimidazole derivatives against 5-HT-induced bradycardia in anesthetized rats. Jpn J Pharmacol. 1994;65(3):241–248. doi:10.1254/jjp.65.241
58. Martinek RM. Witnessed asystole during spinal anesthesia treated with atropine and ondansetron: a case report. Can J Anaesth. 2004;51(3):226–230. doi:10.1007/BF03019100
59. Ortiz-Gómez JR, Palacio-Abizanda FJ, Morillas-Ramirez F, Fornet-Ruiz I, Lorenzo-Jiménez A, Bermejo-Albares ML. The effect of intravenous ondansetron on maternal haemodynamics during elective caesarean delivery under spinal anaesthesia: a double-blind, randomised, placebo-controlled trial. Int J Obstet Anesth. 2014;23(2):138–143. doi:10.1016/j.ijoa.2014.01.005
60. Owczuk R, Wenski W, Polak-Krzeminska A, et al. Ondansetron given intravenously attenuates arterial blood pressure drop due to spinal anesthesia: a double-blind, placebo-controlled study. Reg Anesth Pain Med. 2008;33(4):332–339. doi:10.1016/j.rapm.2008.01.010
61. Owczuk R, Wenski W, Twardowski P, et al. Ondansetron attenuates the decrease in blood pressure due to spinal anesthesia in the elderly: a double blind, placebo-controlled study. Minerva Anestesiol. 2015;81(6):598–607.
62. Sahoo T, SenDasgupta C, Goswami A, Hazra A. Reduction in spinal-induced hypotension with ondansetron in parturients undergoing caesarean section: a double-blind randomised, placebo-controlled study. Int J Obstet Anesth. 2012;21(1):24–28. doi:10.1016/j.ijoa.2011.08.002
63. Gao L, Zheng G, Han J, Wang Y, Zheng J. Effects of prophylactic ondansetron on spinal anesthesia-induced hypotension: a meta-analysis. Int J Obstet Anesth. 2015;24(4):335–343. doi:10.1016/j.ijoa.2015.08.012
64. Terkawi AS, Tiouririne M, Mehta SH, Hackworth JM, Tsang S, Durieux ME. Ondansetron does not attenuate hemodynamic changes in patients undergoing elective cesarean delivery using subarachnoid anesthesia: a double-blind, placebo-controlled, randomized trial. Reg Anesth Pain Med. 2015;40(4):344–348. doi:10.1097/AAP.0000000000000274
65. Thiele RH, Nemergut EC, Lynch C. The physiologic implications of isolated alpha(1) adrenergic stimulation. Anesth Analg. 2011;113(2):284–296. doi:10.1213/ANE.0b013e3182124c0e
66. Xiao F, Wei C, Chang X, et al. A prospective, randomized, double-blinded study of the effect of intravenous ondansetron on the effective dose in 50% of subjects of prophylactic phenylephrine infusions for preventing spinal anesthesia-induced hypotension during cesarean delivery. Anesth Analg. 2019. doi:10.1213/ANE.0000000000004534
67. Koch T, Wenzel V. [Old drugs and new approval procedures: akrinor remains marketable and an application for reapproval of Arginin Vasopressin has been made]. Anaesthesist. 2006;55(6):708–710. doi:10.1007/s00101-006-1011-x. German.
68. Marcus HE, Behrend A, Schier R, et al. [Anesthesiological management of Caesarean sections: nationwide survey in Germany]. Anaesthesist. 2011;60(10):916–928. doi:10.1007/s00101-011-1931-y. German.
69. Sternitzke N, Schieffer H, Rettig G, Bette L. [Mechanism of action of oxyfedrine as a partial beta receptor agonist]. Z Kardiol. 1984;73(9):586–593. German.
70. Sakai K, Shioya A, Hashimoto K. Effect of combining noradrenalinetheophylline and norephedrinetheophylline in various ratios on renal circulation. Arzneimittelforschung. 1972;22(4):698–701.
71. Lee A, Ngan Kee WD, Gin T. A dose-response meta-analysis of prophylactic intravenous ephedrine for the prevention of hypotension during spinal anesthesia for elective cesarean delivery. Anesth Analg. 2004;98(2):483–90.
72. Dyer RA, Reed AR. Spinal hypotension during elective cesarean delivery: closer to a solution. Anesth Analg. 2010;111(5):1093–5.
73. Ngan Kee WD. Prevention of maternal hypotension after regional anaesthesia for caesarean section. Curr Opin Anaesthesiol. 2010;23(3):304–309. doi:10.1097/ACO.0b013e328337ffc6
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.