")
Back to Journals » International Journal of General Medicine » Volume 15
Construction and Validation of a Prediction Model for Identifying Clinical Risk Factors of Lateral Lymph Node Metastasis in Medullary Thyroid Carcinoma
Authors Huang Y, Min Y, Yang G, Wang H , Yin G , Zhang L
Received 15 December 2021
Accepted for publication 17 February 2022
Published 1 March 2022 Volume 2022:15 Pages 2301—2309
DOI https://doi.org/10.2147/IJGM.S353497
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yizhou Huang,1,* Yu Min,2,* Gangyi Yang,1 Hanghang Wang,3 Guobing Yin,2 Lili Zhang1
1Department of Endocrinology, The Second Affiliated Hospital, Chongqing Medical University, Chongqing, 400010, People’s Republic of China; 2Department of Breast and Thyroid Surgery, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, 400010, People’s Republic of China; 3Department of Respiratory and Critical Care Medicine, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, 400010, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lili Zhang, Department of Endocrinology, The Second Affiliated Hospital of Chongqing Medical University, No. 74, Linjiang Road, Yuzhong Dist, Chongqing, 404100, People’s Republic of China, Email [email protected]; [email protected] Guobing Yin, Department of Breast and Thyroid Surgery, The Second Affiliated Hospital of Chongqing Medical University, No. 74, Linjiang Road, Yuzhong Dist, Chongqing, 404100, People’s Republic of China, Email [email protected]
Purpose: Medullary thyroid carcinoma (MTC) is a rare but highly invasive malignancy, especially in terms of cervical lymph node metastasis. However, the role of prophylactic lateral lymph node dissection (LLND) is still controversial. We hereby aim to explore the risk factors of lateral lymph node metastasis (LLNM) in patients with MTC to guide clinical practice.
Patients and Methods: The clinicopathological characteristics of patients with MTC from the Surveillance, Epidemiology, and End Results (SEER) Program and the Second Affiliated Hospital of Chongqing Medical University were reviewed and analyzed. Univariate and multivariate logistics regression analyses were used to screen the risk factors of LLNM in patients with MTC.
Results: Four variables, including male gender, multifocality, extrathyroidal invasion (EI), and large tumor size (all p < 0.05), were identified as potential independent factors of LLNM in patients with MTC. Based on these results, an individualized prediction model was subsequently developed with a satisfied C-index of 0.798, supported by both internal and external validation with a C-index of 0.816 and 0.896, respectively. We also performed the decision curve analysis (DCA) and calibration curve, which indicated a remarkable agreement in our model for predicting the risk of LLNM.
Conclusion: We determined that various clinical characteristics, male gender, multifocality, EI, and large tumor size, were significantly associated with LLNM in patients with MTC. Thus, a validated prediction model utilizing readily available variables was successfully established to help clinicians make individualized clinical decisions on MTC management, especially regarding whether the LLND is necessary for patients with clinical negative lateral lymph node involvement and the frequency of follow-up without LLND.
Keywords: medullary thyroid carcinoma, lateral lymph node metastasis, risk factors, SEER, predicting model
Introduction
Over the past years, medullary thyroid carcinoma (MTC), which accounted for approximately 1%- 2% of thyroid cancer, has aroused wide concern as a result of its worse prognosis and high mortality when compared with papillary thyroid carcinoma (PTC).1,2 It is gradually accepted that a more conservative therapeutic modality could benefit PTC patients with small primary tumor size (cT1) or clinical negative lymph node involvement (cN0), including no prophylactic cervical lymph node dissection (LND), lobectomy, and even active surveillance (AS). However, these agreements were not adapted to patients with MTC. MTC is a neuroendocrine tumor that derives from the calcitonin-producing parafollicular C-cells and represents more aggressive than differentiated thyroid cancer (DTC). To date, surgical intervention, especially total thyroidectomy (TT) combined with the prophylactic central LND, was the first-line in dealing with MTC patients. However, there was still a lack of consensus regarding whether prophylactic lateral LND was appropriately warranted for cN0 patients. Notably, some previous studies had determined that LLNM (cervical lymph nodes levels II to V) was related to the abnormal serum calcitonin (Ctn) and carcinoembryonic antigen (CEA) levels3,4 and played a pivotal role in predicting the prognosis of patients with MTC. For instance, high circulating serum levels of Ctn, CEA, and neuron-specific enolase (NSE), larger primary tumor size, irregular shape, spiculated margins, and subcapsular locations in the neck ultrasonography were prone to appear LLNM metastasis, and log odds of positive lymph nodes (LODDS) was determined to be independent prognostic factors for MTC.5–7 Nevertheless, some clinicopathological results might also be of great significance to help us determine more effective predicting variables for stratifying the different risk levels of LLNM in patients with MTC.
In the present study, we aim to determine the independent risk factors associated with the LLNM in patients with MTC based on the clinicopathological characteristics of patients from the SEER database. SEER program is established to comprehensively collect clinical data on malignant and in situ cancers, including patient demographics, primary tumor site, tumor morphology and stage at diagnosis, first course of treatment, and mortality outcomes, for correlated incidence, prevalence, and prognosis.8 Furthermore, we develop and validate a risk prediction model for predicting LLNM in patients with MTC. Patients with MTC are scored through each item in the model, and total points are calculated to obtain the probability of LLNM. Based on our prediction model, MTC patients with a high probability of LLNM could benefit from LLND in the absence of structural lateral neck disease.
Materials and Methods
Data Collection
The patients we had analyzed were from two databases. Firstly, patients diagnosed with MTC between 2010–2015 years were retrieved from the SEER database (http://seer.cancer.gov/). All patients included satisfied the histopathology codes of the International Classification of Diseases for Oncology, 3rd edition (ICD-O-3):8345/3, 8346/3, 8347/3, 8510/3. Besides, other inclusion criteria for the study were as follows: aged between 18 and 80 years; MTC was confirmed positive by postoperative histological results. Exclusion criteria were as follows: no lymph nodes found in the final pathological report (n = 90); history or coexistence of other head and neck cancer, incomplete or missing Medical records. After exclusion, there were 924 patients ultimately enrolled in our study. Secondly, the data of 22 patients were extracted from the Department of Breast and Thyroid Surgery of the Second Affiliated Hospital of Chongqing Medical University between 2012–2021 years. The specific exclusion criteria were as follows:1 patients without histologically proven MTC,2 patients undergoing biopsy without further thyroid resection,3 patients without lymph nodes examined,4 patients with a history or coexistence of other head and neck cancer. The study was approved by the Chongqing Medical University Ethics Committee, and all the procedures being performed were part of the routine care.
Assessment of Variables
The variables screened as risk factors of lateral cervical regional lymph node involvement of MTC patients included age, gender, race, extrathyroidal invasion, multifocality, and tumor size. Patients in our study were classified as younger patients (18–54 years) and older patients (≥ 55 years) according to the 8th revision of TNM by the American Joint Committee on Cancer (AJCC). The race was divided into white, black, and other (American Indian/Alaska Native, Asian, or Pacific Islander). The EI category was defined as patients with extrathyroidal invasion (T3-T4) and patients without extrathyroidal invasion (T1-T2). Meanwhile, multifocality was classified as more than one lesion within the thyroid, while a solitary tumor represented only one lesion within the thyroid. Tumor size was divided into three parts, including > 0mm largest diameter ≤ 10mm, > 10mm largest diameter ≤ 20mm, and > 20mm largest diameter ≤ 40mm because of the possibility that lateral cervical regional lymph node metastasis was high for oversized tumors (> 40mm).
Statistical Analysis
Logistic-regression analyzed models were used for binary variables, including both univariate and multivariate analyses. We divided the data extracted from SEER into two groups according to the diagnosis year of MTC patients: years of 2010–2012 for a training data set and years of 2013–2015 for an internal validation data set. The data retrieved from our Department was used as the external validation set. Then logistic regression analysis was used to establish a risk model and develop a nomogram. The C-index, which was in accordance with the area under the curve (AUC) and calibration curves as well as the decision curve analysis (DCA), was performed for assessing the accuracy of predicting the LLNM in training data set and testing data set and determining the clinical value of the risk model by quantifying the net benefits under different threshold probabilities. All statistical analyses were performed via the “R” software (https://www.r-project.org). The statistical significance was defined as p < 0.05.
Results
Clinicopathological Characteristics of Patients
Generally, in our study, 924 patients with MTC between 2010 and 2015 were retrieved from the SEER database. Moreover, 22 patients with MTC between 2012 and 2021 were extracted from the medical record of the Second Affiliated Hospital of Chongqing Medical University. In patients collected from the SEER database, the age range was between 18–85 years, and the entire cohort encompassed 346 males (37.4%) and 578 females (62.6%). Besides, 204 patients (22.1%) confirmed LLNM in the whole population. Approximately 86.1% of the cancer foci were confined within the thyroid capsule. Then, patients with MTC were divided into two groups which were consisted of a training set (n = 450) and an internal validation set (n = 474). Among patients with MTC, about 21.8% patients were confirmed LLNM in the training group (170 males and 280 females), whereas 22.4% patients in the internal validation group (176 males and 298 females) and 45.5% were in the external validation group (6 males and 4 females). Demographic and clinicopathologic characteristics of patients were summarized in Table 1.
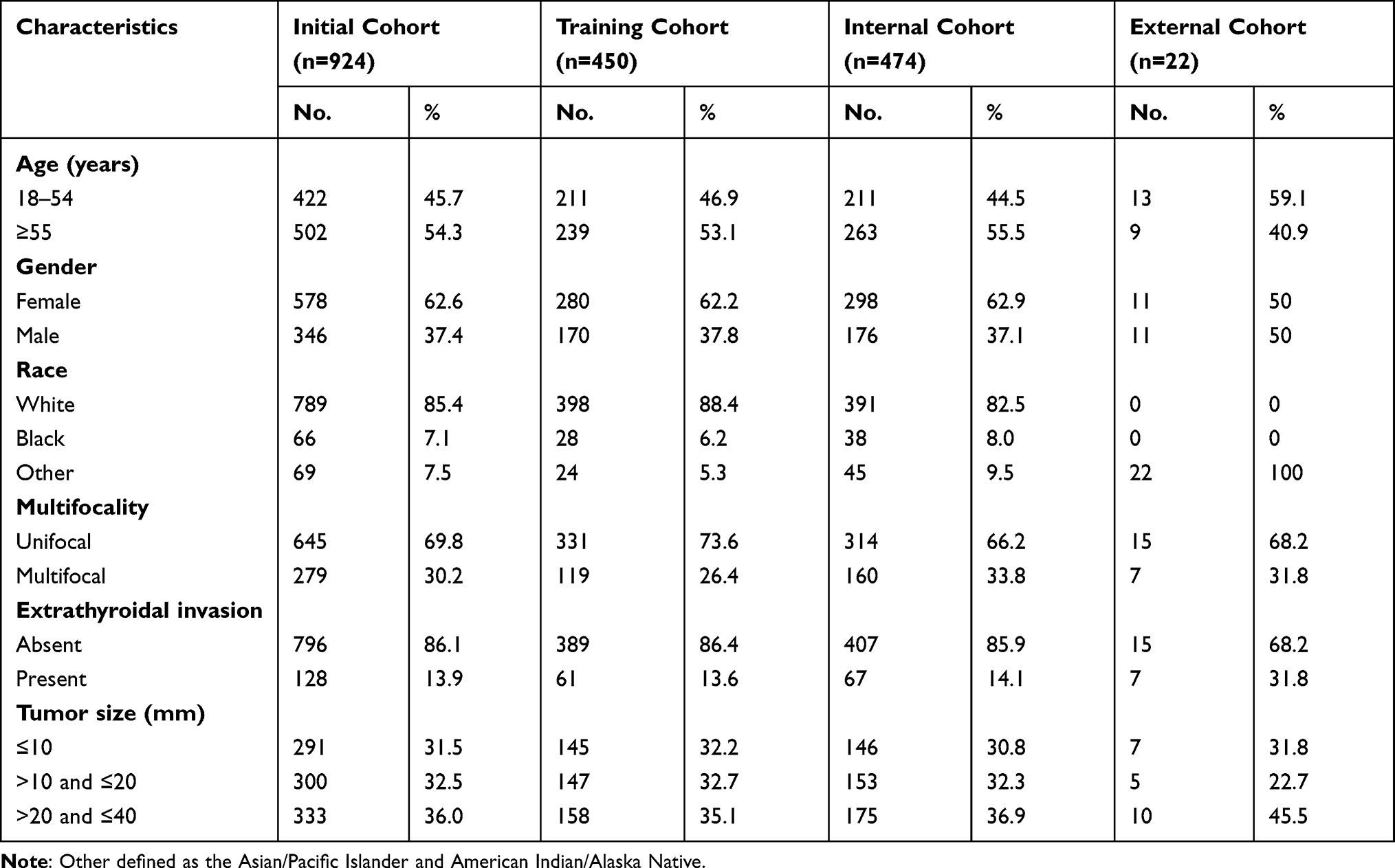 |
Table 1 Clinicopathological Characteristics of Patients with Medullary Thyroid Carcinoma |
Univariate and Multivariate Logistic Regression Analyses
There were four variables being observed to be independent predictive factors of LLNM in patients with MTC via univariate and multivariate logistic regression analyses. At univariate analysis, gender (p < 0.001), multifocality (p < 0.001), EI (p < 0.001) and tumor size (p = 0.002 and p < 0.001, respectively) were screened as predictive factors associated with LLNM in patients with MTC. Multivariate logistic regression was further performed to screen for significant variables associated with LLNM, which were in line with the results of univariate analysis. Specifically, male gender (hazard ratio (HR) = 2.414; 95% confidence interval (CI): (1.425–4.090); p = 0.001), multifocality (HR = 2.234; 95% CI: (1.246–4.004); p = 0.007), EI (HR = 8.969; 95% CI: (4.660–17.265); p < 0.001), and tumor size lager than 10mm (10 mm < largest diameter ≤ 20 mm HR = 2.878; 95% CI: (1.367–6.059); p = 0.005; 20 mm < largest diameter ≤ 40 mm HR = 3.684; 95% CI: (1.789–7.588); p < 0.001) were regarded as risk factors (Table 2).
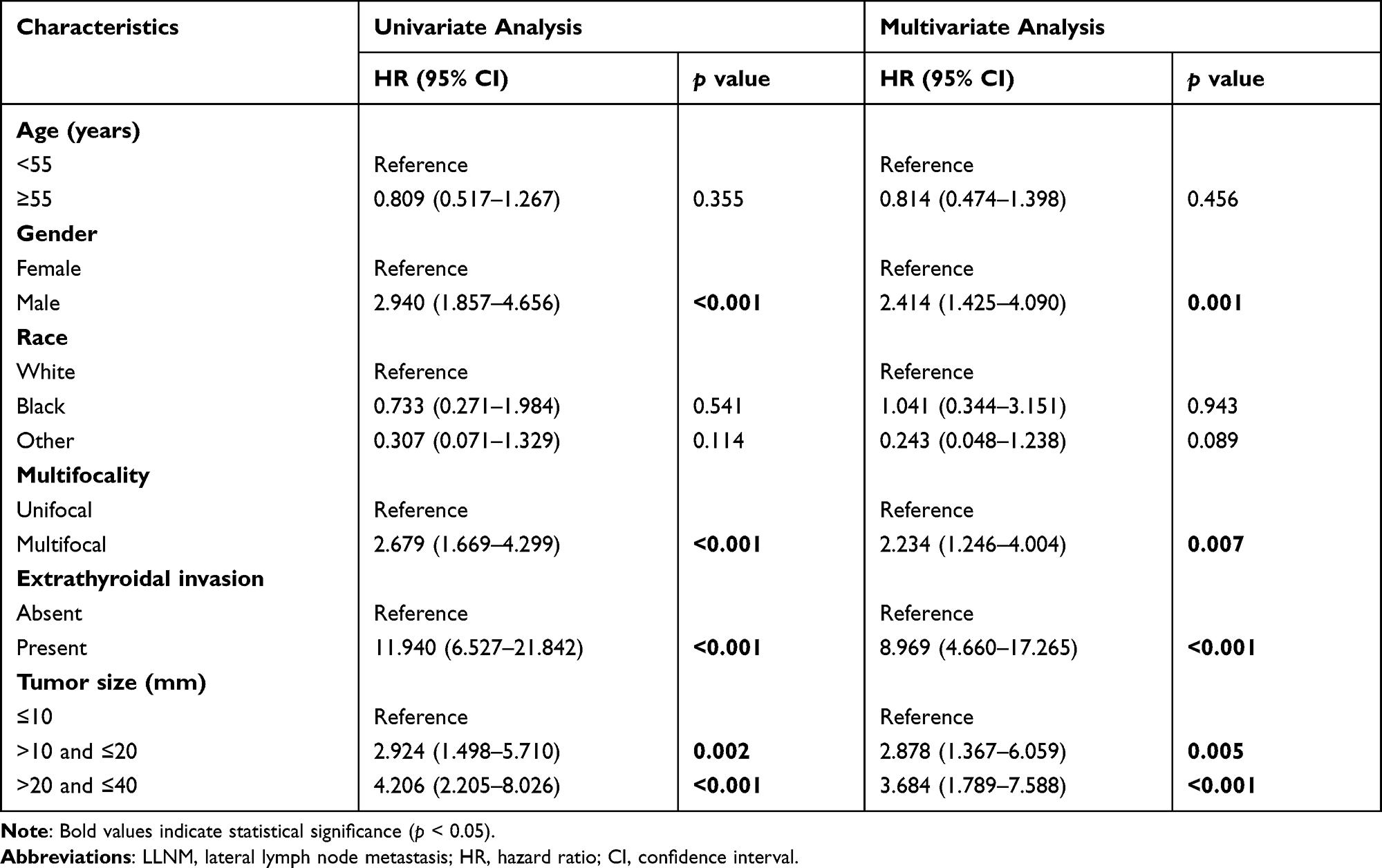 |
Table 2 Univariate and Multivariate Analyses of Risk Factors Related to LLNM |
Construction and Validation of Individualized Risk Model for Predicting LLNM
We have constructed a risk model and visualized it to help clinical practice (Figure 1). The calibration curve of our model showed great consistency in the training data set and internal validation data set (Figure 2A; mean absolute error = 0.015). The C-index of the training model, equally to the AUC, was reached 0.798 (Figure 3A) and further supported by both the internal validation cohort (C-index of 0.816) and external validation cohort (C-index of 0.896) (Figure 3B and C), which indicated that the model we developed had a satisfied predictive capability. Moreover, the DCA results showed that applying this model to predict the risk of LLNM would be better than using this model to treat all patients or none patients, with which threshold probability between >9% and <78% (Figure 2B).
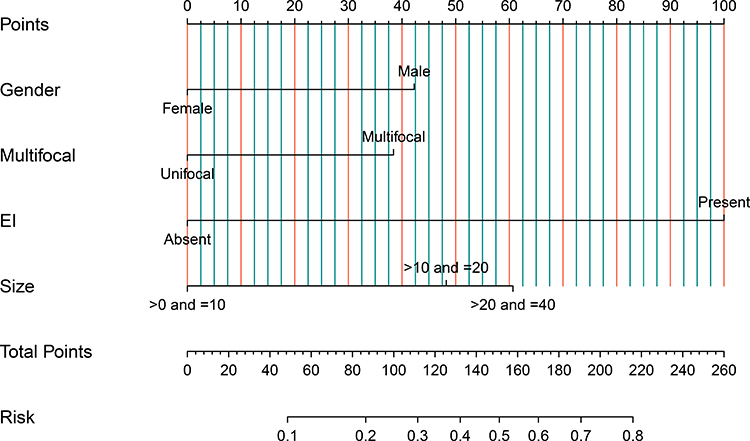 |
Figure 1 Nomogram for predicting lateral lymph node metastasis in patients with MTC. Patients were scored through each item, and total points are calculated to obtain the probability of LLNM. Abbreviations: EI, extrathyroidal invasion, LNM, lymph node metastasis. |
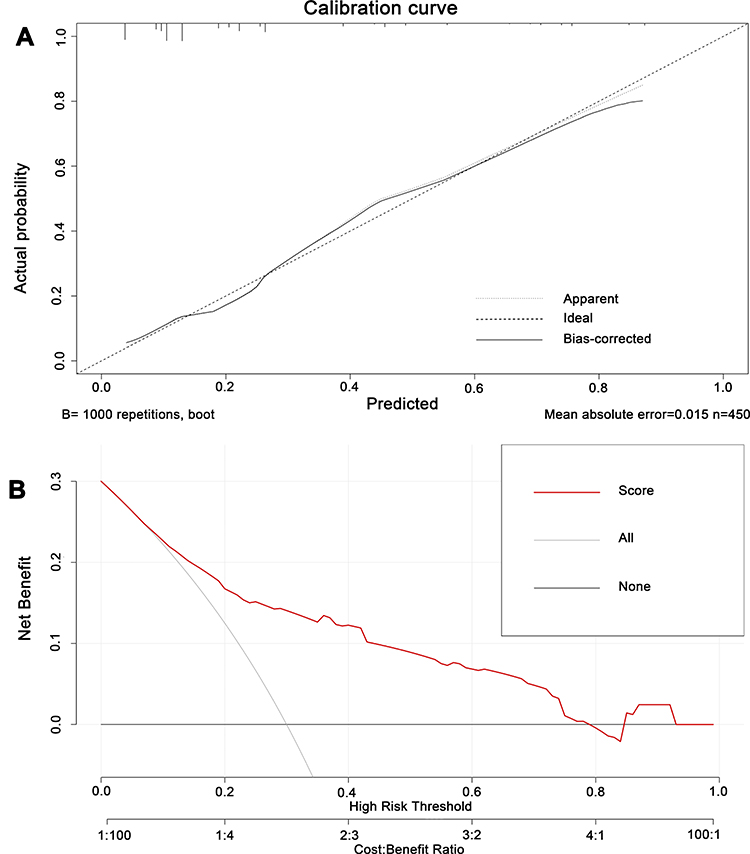 |
Figure 2 (A) Calibration curve of the nomogram for the verification of training set. The x-axis represents the predicted LLNM. The y-axis represents the actual LLNM. The dotted line stands for a perfect prediction using an ideal model. The solid line was drawn to represent the performance of the nomogram, of which the closer fit to the dotted line represents the better prediction of the nomogram. (B) Decision curve analysis for LLNM in MTC patients. The black line (None) represents the assumption of net benefit that no patient has LLNM. The gray line (All) shows the assumption of net benefit that all patients have LLNM. The red line (Score) represents the assumption of net benefit of nomogram for LLNM considering clinical risk factors (gender, multifocal, extrathyroidal invasion and tumor size). |
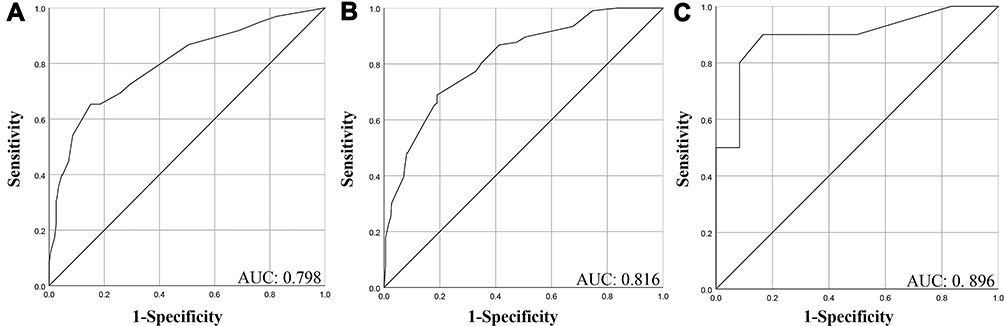 |
Figure 3 The receiver operating characteristics (ROC) curve and area under the ROC curve (AUC). (A) AUC for the training group; (B) AUC for the internal validation group; (C) AUC for the external validation group. |
Discussion
Medullary thyroid carcinoma is a rare histological subtype of thyroid cancer, characterized by early lymphatic and systemic dissemination of tumor cells. Compared with PTC and follicular thyroid carcinoma (FTC), the prognosis of medullary thyroid cancer is worse, and over 50% of MTC patients suffered from the biopsy confirmed recurrence within 10 years during the postoperative follow-up.9,10 According to the latest management guideline of the American Thyroid Association (ATA), there is no doubt that therapeutic dissection of lateral lymph node compartments is suitable for clinically lateral lymph node metastasis (cN1b) patients with MTC. However, concerning the patients with cN0 status, there was still controversy on the role of prophylactic lateral LND for this particular subpopulation. Recently, some studies discovered that the serum Ctn was maintained at a high level when the lateral lymph nodes were involved.11 Furthermore, they suggested that the fewer regional lymph nodes dissected were significantly related to the poorer postoperative overall survival (OS) of patients with MTC.12 Although poor prognosis was frequently observed in patients with lymph nodes involvement, the false-negative results might occur in approximately one-third of patients during the preoperative neck ultrasonography examination.13 For this reason, the prophylactic CLND seemed to be an alternative plan to reduce this risk. However, the defects of prophylactic CLND had been recognized by clinicians, including but not limited to nerve injury and hypoparathyroidism during cervical lymph node dissection. Notably, Calò et al found that patients with DTC performing TT combined with CLND were involved in a higher incidence of permanent hypoparathyroidism than patients performing TT alone (10/220 vs.7/65) as well as a higher risk of recurrent laryngeal nerve injury in Conzo et al study.14,15 Therefore, prophylactic CLND was not routinely recommended for DTC patients with cN0 status.16 Interestingly, the cost-effective value of prophylactic CLND was still controversial in the latest guideline of ATA.16 Namely, clinicians performed overtreatment frequently because of the will to protect patients’ necks from residual tumor invasion. However, the tumor recurrence rate concerning the inadequate scope of dissection often increases because of the high frequency of lateral cervical lymph nodes residual in MTC.17 Referring to previous studies on this topic, some scholars found that the LLNM in patients with MTC was correlated with serology results, including serum Ctn level and CEA level or the frequency of central compartment lymph node metastases.3,18,19 Nevertheless, to our best of knowledge, there was still a lack of reliable predictive factors for guiding surgeons to make better clinical decisions on the necessity of lateral LND in patients with MTC, based on their clinicopathological characteristics.
In the present study, during the univariate logistic regression and multivariate logistic regression analyses, we determined that male gender, multifocality, extrathyroidal invasion, and tumor size larger than 1cm were the independent risk factors of LLNM, and a prediction model was subsequently developed. We propose a hypothetical MTC patient to illustrate the utility of the model designed in this study. A male MTC patient with multifocality and tumor size of 40mm confined to the thyroid presents the risk of lateral cervical lymph node metastasis of approximately 45%. Expressly in our analysis, the number of 204 patients (22.1%) being confirmed LLNM in the whole population, which was lower than our data (45.5%) and the previous study (35.6%).5 Reasons for this difference may be the disparate sample size (924 vs 22 vs 73) or dominating composition of the race (American vs Chinese vs Korean). Although limited studies could be found to confirm our results directly, previous studies had found that tumor size and extrathyroidal invasion were related to the decline in the survival rate of patients with MTC, and MTC tumors with larger size (>1.5 cm) were at higher risk for lateral cervical lymph node metastasis.5,20–22 Gender was proved to be a risk factor by Scopsi et al and Saad et al with the conclusion of a female having a better prognosis than a male, which was in accord with our study.23,24 Many studies have confirmed that age is an independent predictor for MTC patients.25 Roman et al found that if the patients were aged >65 at the time of diagnosis, the mortality risk increased by 5.2% for each additional year.26 However, the result of our study suggested that age was not statistically significantly associated with the LLNM, which was only consistent with a seventy-three-sample-size study. We speculate the reason may be that MTC itself was relatively rare, and data from the SEER database were strictly screened, which resulted in our small sample size. Moreover, we divided the sample into the training data set and internal validation data sets, reducing the statistical sample size and leading to such differences. Consequently, we cannot rule out the possibility that age was associated with lateral neck lymph node metastasis. Furthermore, an individualized risk model concerning four potential independent risk factors was well established and validated based on our discovered results. A C-index of 0.798 in the training cohort presented excellent applicability in this model and was in high agreement with the internal validation cohort (C-index of 0.816) and external validation cohort (C-index of 0.896). Moreover, the DCA results displayed a good clinical utility as well.
Nonetheless, several limitations in this present study needed to be addressed. First, the cases in the external validation cohort are relatively insufficient, which would lead to a bias in the results. Second, the model was based on retrospective data collected from the SEER database, leading to the difficulty of comparing sporadic and hereditary MTC. Patients with sporadic MTC are more likely to have lateral lymph node metastasis.27 Finally, previous studies determined that some serum indicators such as CEA, Ctn, NSE were significantly associated with the increasing risk of LLNM in MTC patients but missing in the SEER program.
Conclusion
In summary, based on the clinicopathological characteristics of patients from the SEER program, we established an individualized prediction model for evaluating LLNM for MTC. This model might be of great clinical value (follow-up frequency, etc.) and helpful for formulating an operative method for MTC patients. For cN0 MTC patients with a high score according to the model, clinicians should consider the dissection of the lateral cervical lymph node or closer follow-up without LLND.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
Ethical approval was approved by the local Ethics Committee of the Chongqing Medical University, and our study was complied with the Declaration of Helsinki. All the procedures being performed were part of the routine care. Informed consents were obtained from the participants prior to study commencement.
Acknowledgment
Yizhou Huang and Yu Min are co-first authors for this study.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gundara JS, Zhao J, Gill AJ, et al. Noncoding RNA blockade of autophagy is therapeutic in medullary thyroid cancer. Cancer Med. 2015;4:174–182. doi:10.1002/cam4.355
2. Wells SA
3. Machens A, Dralle H. Biomarker-based risk stratification for previously untreated medullary thyroid cancer. J Clin Endocrinol Metab. 2010;95:2655–2663. doi:10.1210/jc.2009-2368
4. Turkdogan S, Forest VI, Hier MP, Tamilia M, Florea A, Payne RJ. Carcinoembryonic antigen levels correlated with advanced disease in medullary thyroid cancer. J Otolaryngol Head Neck Surg. 2018;47:55. doi:10.1186/s40463-018-0303-x
5. Oh HS, Kwon H, Song E, et al. Preoperative Clinical and Sonographic Predictors for Lateral Cervical Lymph Node Metastases in Sporadic Medullary Thyroid Carcinoma. Thyroid. 2018;28:362–368. doi:10.1089/thy.2017.0514
6. Tang J, Jiang S, Gao L, et al. Construction and Validation of a Nomogram Based on the Log Odds of Positive Lymph Nodes to Predict the Prognosis of Medullary Thyroid Carcinoma After Surgery. Ann Surg Oncol. 2021;28(8):4360–4370. doi:10.1245/s10434-020-09567-3
7. Ye L, Zhou X, Lu J, Wang Y, Xie X, Zhang J. Combining serum calcitonin, carcinoembryonic antigen, and neuron-specific enolase to predict lateral lymph node metastasis in medullary thyroid carcinoma. J Clin Lab Anal. 2020;34:e23278. doi:10.1002/jcla.23278
8. Cronin KA, Ries LA, Edwards BK, Surveillance T. Epidemiology, and End Results (SEER) Program of the National Cancer Institute. Cancer. 2014;120(Suppl 23):3755–3757. doi:10.1002/cncr.29049
9. Ho AS, Wang L, Palmer FL, et al. Postoperative Nomogram for Predicting Cancer-Specific Mortality in Medullary Thyroid Cancer. Ann Surg Oncol. 2015;22:2700–2706. doi:10.1245/s10434-014-4208-2
10. Chen L, Wang Y, Zhao K, Wang Y, He X. Postoperative Nomogram for Predicting Cancer-Specific and Overall Survival among Patients with Medullary Thyroid Cancer. Int J Endocrinol. 2020;2020:8888677. doi:10.1155/2020/8888677
11. Kim J, Park J, Park H, et al. Metastatic Lymph Node Ratio for Predicting Recurrence in Medullary Thyroid Cancer. Cancers. 2021;14:13. doi:10.3390/cancers14010013
12. Moses LE, Oliver JR, Rotsides JM, et al. Nodal disease burden and outcome of medullary thyroid carcinoma. Head Neck. 2021;43:577–584. doi:10.1002/hed.26511
13. Kouvaraki MA, Shapiro SE, Fornage BD, et al. Role of preoperative ultrasonography in the surgical management of patients with thyroid cancer. Surgery. 2003;134:946–954. doi:10.1016/S0039-6060(03)00424-0
14. Calò PG, Pisano G, Medas F, et al. Total thyroidectomy without prophylactic central neck dissection in clinically node-negative papillary thyroid cancer: is it an adequate treatment? World J Surg Oncol. 2014;12:152. doi:10.1186/1477-7819-12-152
15. Conzo G, Calò PG, Sinisi AA, et al. Impact of prophylactic central compartment neck dissection on locoregional recurrence of differentiated thyroid cancer in clinically node-negative patients: a retrospective study of a large clinical series. Surgery. 2014;155:998–1005. doi:10.1016/j.surg.2014.02.010
16. Haugen BR, Alexander EK, Bible KC, et al. American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2015;2016(26):1–133.
17. Machens A, Lorenz K, Dralle H. Histology-proven recurrence in the lateral or central neck after systematic neck dissection for medullary thyroid cancer. Endocrine. 2018;61:428–439. doi:10.1007/s12020-018-1625-1
18. Machens A, Hauptmann S, Dralle H. Prediction of lateral lymph node metastases in medullary thyroid cancer. Br J Surg. 2008;95:586–591. doi:10.1002/bjs.6075
19. Chen L, Zhao K, Li F, He X. Medullary Thyroid Carcinoma With Elevated Serum CEA and Normal Serum Calcitonin After Surgery: a Case Report and Literature Review. Front Oncol. 2020;10:526716. doi:10.3389/fonc.2020.526716
20. Nguyen XV, Roy Choudhury K, Tessler FN, Hoang JK. Effect of Tumor Size on Risk of Metastatic Disease and Survival for Thyroid Cancer: implications for Biopsy Guidelines. Thyroid. 2018;28:295–300. doi:10.1089/thy.2017.0526
21. Kebebew E, Greenspan FS, Clark OH, Woeber KA, Grunwell J. Extent of disease and practice patterns for medullary thyroid cancer. J Am Coll Surg. 2005;200:890–896. doi:10.1016/j.jamcollsurg.2004.12.011
22. Guan YJ, Fang SY, Chen LL, Li ZD. Development and validation of prognostic nomograms for medullary thyroid cancer. Onco Targets Ther. 2019;12:2299–2309. doi:10.2147/OTT.S196205
23. Scopsi L, Sampietro G, Boracchi P, et al. Multivariate analysis of prognostic factors in sporadic medullary carcinoma of the thyroid. A retrospective study of 109 consecutive patients. Cancer. 1996;78:2173–2183. doi:10.1002/(SICI)1097-0142(19961115)78:10<2173::AID-CNCR20>3.0.CO;2-V
24. Saad MF, Ordonez NG, Rashid RK, et al. Medullary carcinoma of the thyroid. A study of the clinical features and prognostic factors in 161 patients. Medicine. 1984;63:319–342. doi:10.1097/00005792-198411000-00001
25. Park H, Park SY, Park J, et al. Prognostic Value of Preoperative Serum Calcitonin Levels for Predicting the Recurrence of Medullary Thyroid Carcinoma. Front Endocrinol (Lausanne). 2021;12:749973. doi:10.3389/fendo.2021.749973
26. Roman S, Lin R, Sosa JA. Prognosis of medullary thyroid carcinoma: demographic, clinical, and pathologic predictors of survival in 1252 cases. Cancer. 2006;107:2134–2142. doi:10.1002/cncr.22244
27. Qu N, Shi RL, Luo TX, et al. Prognostic significance and optimal cutoff of age in medullary thyroid cancer. Oncotarget. 2016;7:15937–15947. doi:10.18632/oncotarget.7556
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.