")
Back to Journals » Clinical Ophthalmology » Volume 13
Consensus on the management of astigmatism in cataract surgery
Authors Núñez MX, Henriquez MA, Escaf LJ, Ventura BV, Srur M , Newball L, Espaillat A , Centurion VA
Received 28 June 2018
Accepted for publication 12 October 2018
Published 11 February 2019 Volume 2019:13 Pages 311—324
DOI https://doi.org/10.2147/OPTH.S178277
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Maria X Núñez,1 Maria A Henriquez,2 Luis J Escaf,3 Bruna V Ventura,4 Miguel Srur,5 Lyle Newball,6 Arnaldo Espaillat,7 Virgilio A Centurion8
1Unit of Cornea, Cataract and Refractive Surgery, Grupo de Investigacion Vision Sana, Clinica de Oftalmología de Cali, Universidad Javeriana, Cali, Colombia; 2Department of Cataract, Department of Research, Oftalmosalud Instituto de Ojos, Lima, Peru; 3Clinica Oftalmologica del Caribe (Cofca), Universidad Javeriana, Barranquilla, Colombia; 4Department of Cataract, Altino Ventura Foundation, HOPE Eye Hospital, Recife, Brazil; 5Centro de la Visión, Filial Clínica Las Condes, Universidad de Los Andes, Santiago de Chile, Chile; 6Lynd Newball Clinic, San Andres Islas, Colombia; 7Cataract and refractive surgery service, Espaillat Cabral Institute, Santo Domingo, Dominican Republic; 8Cataract service, IMO – Instituto de Moléstias Oculares, São Paulo, Brazil
Abstract: This project was aimed at achieving consensus on the management of astigmatism during cataract surgery by ophthalmologists from Latin America using modified Delphi technique. Relevant peer-reviewed literature was identified, and 21 clinical research questions associated with the definition, classification, measurement, and treatment of astigmatism during cataract surgery were formulated. Twenty participants were divided into seven groups, and each group was assigned three questions to which they had to respond in written form, after thoroughly reviewing the literature. The assigned questions with corresponding responses by each group were discussed with other participants in round 4 – presentation of findings. The consensus was achieved if approval was obtained from at least 80% of participants. The present paper provides several agreements and recommendations for management of astigmatism during cataract surgery, which could potentially minimize the variability in practice patterns and help ophthalmologists adopt optimal practices for cataract patients with astigmatism and improve patient satisfaction.
Keywords: management of astigmatism, astigmatism correction during cataract surgery, cataract patients with astigmatism, measurement and treatment of astigmatism, consensus on managing astigmatism
Introduction
Ocular astigmatism is a refractive condition which occurs because of unequal curvatures of the cornea and the crystalline lens, decentration or tilting of the lens, or unequal refractive indices across the crystalline lens,1 and in some cases, alterations of the geometry of the posterior pole. Several studies have reported the prevalence of corneal astigmatism in cataract patients of different age groups. In general, nearly 35%–40% of the cataract patients have astigmatism ≥1.0 D and 19%–22% have astigmatism ≥1.5 D.2–4
The advances in intraocular lens (IOL) designs and surgical technique have increased the patient expectations after cataract surgery. Since resultant astigmatism after phacoemulsification can leave the patient spectacle-dependent and significantly decreases patient satisfaction, it is important to address astigmatism as well during cataract surgery, so as to achieve optimal postoperative refractive outcomes and/or spectacle independence.
There are several ways to measure and treat astigmatism at the time of cataract surgery. Techniques to measure astigmatism include keratometry (manual or automated), corneal topography (eg, placido-based or based on the reflection of multicolor light-emitting diode [LED] points), and corneal tomography (eg, slit-scan imaging, Scheimpflug imaging).5 Additionally, the use of intraoperative aberrometry has been documented to improve the astigmatic outcomes.6 Some of the techniques used to correct astigmatism during cataract surgery include selective positioning of the phacoemulsification incision, corneal relaxing incisions, limbal relaxing incisions, and toric IOL implantation.7 Every procedure has its own limitations, advantages, and disadvantages. As such, no single device/surgical approach has been identified as the most accurate for measuring and correcting astigmatism during cataract surgery. Since there is a lack of well-defined approach to astigmatic planning and treatment, there is a necessity to develop a consensus on the best practices to manage astigmatism during cataract surgery.
The purpose of this paper is to present the consensus achieved on the evaluation and correction of astigmatism during cataract surgery by a panel of experts in the Latin American region using a modified Delphi method. The consensus covers the most relevant questions regarding the definition, measurement, and treatment of astigmatism during cataract surgery.
Methods
We used a modified Delphi technique to obtain consensus on the management of astigmatism during cataract surgery. The Delphi method8,9 is a technique used to collate the opinions of the panelists through iterations with multiple rounds of a structured questionnaire. As a modification to the Delphi method, we included an additional round of presentation of findings, in which the participants presented their responses to the assigned questions, which were discussed and approved by the panelists using the voting method.
The Colombian Association of Cataract and Refractive Surgeons (ASOCCYR), a nonprofit organization that promotes academic research of general interest in cataract and refractive surgery, was the leader of the project. Consensus process began with the development of a research question using the PICOT methodology10 in the first round. This means population (P) – patients diagnosed with cataract and preexisting corneal astigmatism, intervention (I) – surgical management of both cataract and astigmatism, comparison (C) – surgical methodologies, outcomes (O) – postoperative astigmatism and cataract outcomes, and time (T) – postoperative 3 months. Using this methodology, appropriate search words were used to identify relevant peer-reviewed literature.
The second round involved the formulation of clinical research questions, based on the base question developed in the previous round. Overall 21 questions associated with the definition, classification, measurement, and treatment of astigmatism during cataract surgery were prepared. Ophthalmologists from different countries of Latin America with experience in the field of cataract and/or astigmatism and scientific publications in ophthalmic journals were enlisted as potential panelists. The criteria to determine experience were number of cataract surgeries performed using toric and multifocal IOLs, number of cataract surgeries performed using relaxing incisions, experience in a clinical setup that has all the preoperative and intraoperative technologies required to do premium surgery, university professor position, and experience in research. An e-mail invitation was sent to these experts requesting their participation, explaining the aim of the study and the methodology. Twenty experts who were willing to comply with the initial question rounds and the final round involving presentation of findings were selected to participate in this project. Considering the multiplicity of themes, the participants were divided into seven groups with two or three participants in each. The groupwise distribution of the panelists with their respective countries is shown in Table 1.
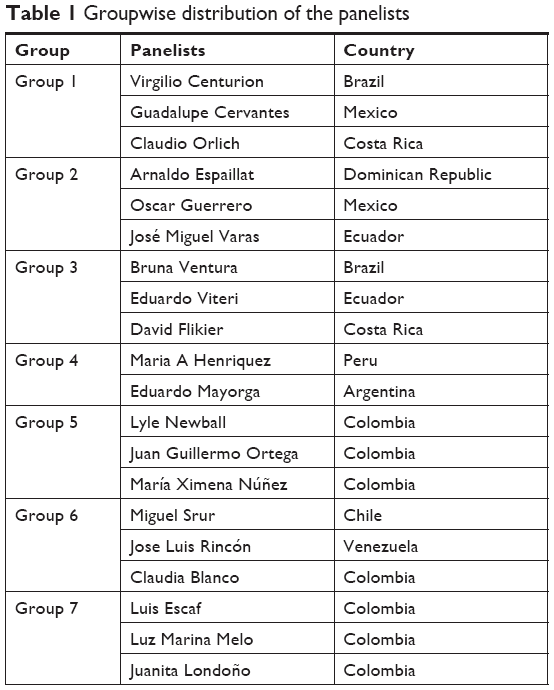 | Table 1 Groupwise distribution of the panelists |
In the third round, the participants were provided with the bibliography and literature regarding the diagnosis and management of astigmatism. The experts of each group were assigned three questions (of the total 21), and they were required to respond to those questions in written form after thoroughly reviewing the literature.
In the fourth round, each group of participants presented their assigned questions with corresponding responses, which were discussed with the remaining panelists. The consensus on each statement was obtained by voting method (raising hands in favor of the statement). The consensus was considered to be achieved if at least 80% of the participants approved the statement. In case of a disagreement, the statement was revised, and a new voting was performed.
Results and discussion
All participants responded to their assigned questions and attended the last round of presentation of findings. The items addressed throughout the rounds and the consensus obtained are hereby presented by their major topic.
Classification of cataract and astigmatism
The first set of questions was aimed at discussing the methods used to classify cataract and astigmatism. To evaluate cataracts, different methods have been described in the literature, such as the Lens Opacities Classification System (LOCS)11 and the Age-Related Eye Disease Study System.12 Some objective methods for measuring nuclear density have also been described;13–19 however, the experts agreed that in the absence of a validated classification system, such methods do not add much value to the clinical decision making. Despite the technical limitations related to the slit lamp and subjectivity of the evaluator, LOCS III remains the most established subjective method for cataract grading.14,15 The experts suggested that the LOCS III can be complemented with the Barraquer Cataract Nuclear Classification (BCN 10),20 which divides the nuclear cataract progression into a baseline clear lens (N0) and 10 grades of opacification (N1 to N10), where N10 corresponds to a completely dark lens (cataracta nigra). The grading chart shows a large slit-lamp cross-sectional image, a smaller frontal view image, and the relative color for each stage of cataract development.
The panelists also agreed on the different ways described in the literature to classify ocular astigmatism based on the refractive component, magnitude, orthogonality, anatomy, and location of the steepest meridian, and in terms of wavefront aberrations (Table 2).
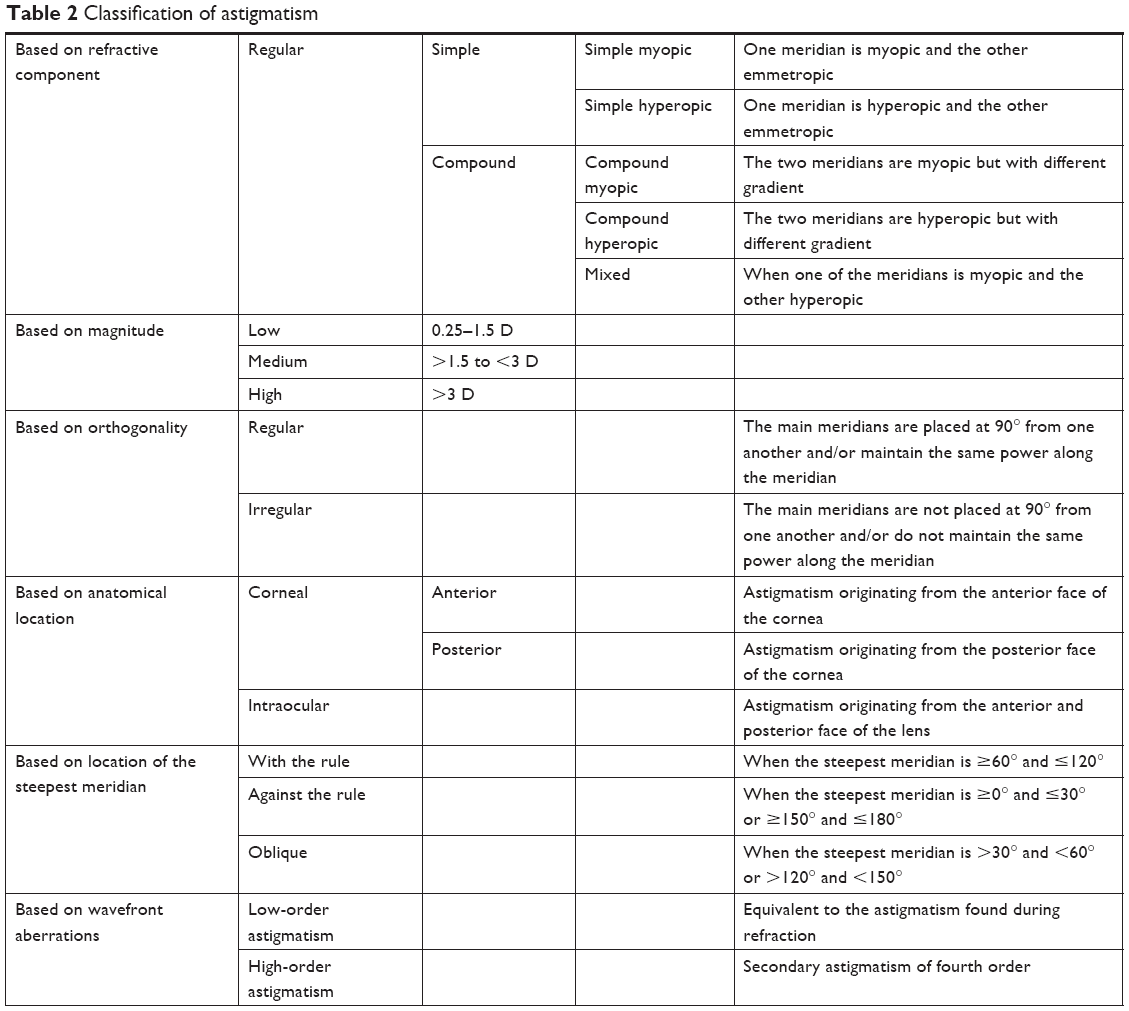 | Table 2 Classification of astigmatism |
Measurement of corneal astigmatism in cataract patients
Several devices based on different technologies are available to measure corneal power and astigmatism, which include manual keratometers, automated keratometers, placido-based corneal topographers, point-source color LED topographers, Scheimpflug image-based topographers, low-coherence reflectometers, and scanning-slit corneal topographers.21–26
Anterior corneal astigmatism: devices and calculators
Manual keratometers, automatic keratometers, and placido ring-based topographers offer direct measurements of the anterior cornea.23–26 Since each device has its own characteristics, measurements obtained from different devices may not be comparable due to the use of different refractive indices or measurement area. Measurements can also be influenced by unstable tear film, ocular surface disease, etc.27,28 These factors may compromise the accuracy of measurements. Therefore, evaluating the quality of each measurement before using it to plan the surgery is critical to obtain precise postoperative results.
Some investigators have suggested that combining keratometry techniques may improve the precision of preoperative keratometry. For example, Browne and Osher demonstrated that measurement errors can be substantially reduced by carefully taking measurements with a manual keratometer and an automated keratometer, and then averaging the measurements.29 It was found that using the average of the measurements reduced the outliers and led to more precise results. It is important to note that axis location and magnitude of astigmatic measurements should be obtained with at least three different measurement methods (manual keratometry, automated keratometry, and topography/tomography). If no two measurements are fairly consistent, there can be ambiguity in deciding correct measurement and calculating toric IOL power. In such conditions, toric IOL should be avoided.
Conventionally, only anterior corneal surface was measured, assuming that the posterior cornea induces minimal refractive astigmatism.30 However, recent studies have demonstrated that both the anterior and posterior corneal surfaces contribute to the total corneal astigmatism (TCA), and that ignoring posterior corneal astigmatism may induce errors in astigmatic treatment calculations.31,32 Koch et al determined that the posterior corneal astigmatism (average −0.3 D) affects the value of TCA. This value may decrease (in cases of with-the-rule [WTR] astigmatism) or increase (in cases of against-the-rule [ATR] astigmatism) TCA.30,32–35 If the posterior corneal astigmatism is not considered, it may overestimate WTR astigmatism by 0.5–0.6 D and underestimate ATR astigmatism by 0.2–0.3 D.30 It has also been documented that ignoring the astigmatism of the posterior cornea can produce an axis error of 7.4°±10.3°.36 The panel agreed that in addition to the evaluation of the anterior corneal surface, posterior corneal surface should be considered in patients undergoing astigmatism correction during cataract surgery.
Various nomograms, adjustment coefficients,35,37 and calculators37–39 are being used to factor in the effect of posterior cornea in the anterior corneal measurements. The Koch et al30 and Goggin et al37 nomograms are being used for selecting the toric power for astigmatic correction that factors in posterior corneal astigmatism. The Baylor nomogram recommends a 0.7 D shift in toric IOL threshold to compensate for posterior corneal astigmatism. However, the method is likely to suffer from inaccuracies due to inherent problems with the measuring device and/or by assuming a fixed location of the steep meridian of the posterior corneal astigmatism. The Goggin nomogram adjusts the anterior corneal astigmatism based on the orientation of the anterior cornea (ie, WTR or ATR) and on the toric lens power for astigmatism correction up to 2.0 D.37 According to this nomogram, the cylindrical component is multiplied by an adjustment factor of 0.75 for WTR astigmatism and by 1.41 if the astigmatism is ATR. Although these methods may improve the accuracy of the surgical planning, they remain inherently inaccurate for not using vector analysis to determine TCA.
Barrett’s toric calculator uses the Universal II formula40 to calculate effective position of the lens and predicts posterior corneal astigmatism based on a theoretical model to provide toric IOL power.40 The Abulafia–Koch formula aims to adjust the measured anterior corneal astigmatism to factor in posterior corneal astigmatism; the net corneal astigmatism thus calculated is used for toric IOL calculations. The Abulafia–Koch formula and Barrett’s toric calculator provide net corneal astigmatism using vector analysis.38,39
Posterior corneal astigmatism and TCA: devices and calculators
The point-source color LED topographer and Scheimpflug image-based tomographers measure both anterior and posterior cornea. Devices based on these technologies, which include the Galilei (Ziemer Ophthalmic Systems AG, Port, Switzerland), the Pentacam (Oculus Optikgeräte GmbH, Wetzlar, Germany), and the Cassini (i-Optics BV, Hague, the Netherlands) provide TCA by directly measuring the anterior as well as the posterior corneal astigmatism. The total corneal power can be used to determine corneal topographic astigmatism (CorT) value,41 which is calculated using summated vector mean of the astigmatism values using all the valid data captured during topography. Additionally, toric calculators, such as Panacea IOL & Toric Calculator, consider real measurements of anterior and posterior toricity with the correction from keratometric to real corneal refractive index.42 Although the use of direct measurements of the anterior and posterior cornea is helpful in decreasing resultant astigmatism after toric IOL implantation,33,43,44 there are studies demonstrating that the outcomes achieved using these measurements or software are not better than those achieved with the Barrett’s toric calculator.24,45
Recently, to obtain net corneal power measurement, intraoperative methods were made available, such as the ORA (Alcon Laboratories, Inc., Fort Worth, TX, USA) and the Holos (Clarity Medical Systems, Inc., Pleasanton, CA, USA). During aphakic measurements, intraoperative aberrometry provides net corneal astigmatism that incorporates posterior corneal astigmatism, thus allowing for better estimation of toric IOL power and its axis of implantation. Although variables such as eyelid speculum pressure, intraocular pressure, corneal hydration, and the viscoelastic used to fill the anterior chamber can influence the net corneal power measurements, several studies have shown promising results.6,46
Although none of the methods is perfect, surgical results have improved over the years. The experts agreed that there is no gold standard technique for measuring posterior corneal astigmatism until now. While the direct measurements of anterior and posterior cornea are helpful, these do not demonstrate high reliability. The panel also agreed that the use of predictive nomograms that use vectorial analysis, such as Barrett’s toric calculator and Abulafia–Koch formula, is safe and reliable, as was demonstrated in a study by Ferreira et al.47
Treatment of corneal astigmatism during cataract surgery
Among various surgical techniques used for cataract extraction, phacoemulsification continues to be the universal choice. It can be either manual or femtosecond laser assisted. However, several investigators have reported that femtosecond laser-assisted cataract surgery (FLACS) does not yield better visual or refractive outcomes than conventional phacoemulsification.4,48 Although the increasing use of robotics is highly anticipated as an effect of technification in the field of health care, the panelists believed that the FLACS is still evolving and will take time to become the mainstream cataract procedure.
The prevalence of preoperative astigmatism in cataract patients has been reported to be 86.6%, of which 35%–40% of the cataract patients have astigmatism ≥1.0 D and 19%–22% have astigmatism ≥1.5 D.2–4 While preexisting astigmatism of <0.5 D does not need correction,49 resultant astigmatism should be <0.75 D in patients seeking spectacle independence after cataract surgery especially with multifocal IOLs.50–52 The experts agreed that, whether manual or femtosecond assisted, the following intraoperative techniques are currently being used to correct astigmatism during cataract surgery: 1) creating clear corneal incision (CCI) on the steepest meridian, 2) paired opposite clear corneal incisions (POCCIs) on the steepest meridian, 3) corneal relaxing incisions, and 4) toric IOL implantation. It is important to recognize that these treatment options correct regular astigmatism; as such, it is important to do thorough preoperative work-up to identify and rule out the presence of corneal conditions that cause irregular or asymmetric astigmatism. Corneal tomographic imaging, in addition to topography, is valuable for decision making.53,54
CCI on the steepest meridian
During cataract surgery, the placement of CCI on the steep meridian has a flattening effect on the corneal curvature, which helps control astigmatism.55 The total astigmatic effect of an incision on the corneal astigmatism is quantified by its surgically induced astigmatism (SIA) vector.56 Conceptually, SIA can be calculated as a double-angle vector difference between the postoperative astigmatism and the preoperative astigmatism at the corneal plane. This SIA can be decomposed into a component with a pure flattening/steepening effect, which changes the magnitude of the astigmatism, and a component that induces torque, which changes the orientation of the preoperative astigmatism.57
The incision on the steep meridian has been reported to correct astigmatism of 0.85±0.75 D.58 The mean surgically induced astigmatism for a 3.0–3.2 mm CCI may range from 0.50 to 0.67 D.7,59,60 The superior incisions tend to produce greater SIA than the temporal incisions, due to greater proximity of the superior incisions to the corneal center than the temporal incisions because of the oval shape of the cornea.61 With the advancing technology, the width of CCI has been decreasing. While there are reports that a CCI of 2.2 mm produces some flattening effect,62 the panel agreed that incisions smaller than 2.4 mm (SIA 0.35±0.21),60 whether created manually or with femtosecond laser, do not produce much astigmatic effect.
Paired opposite corneal incisions at the steepest meridian
Performing an additional CCI opposite (180°) to the first CCI to enhance the flattening effect has also been reported.63 This method is called POCCI. When compared to the single CCI, POCCIs (3.2 mm incision) have been documented providing an enhanced effect of 1.66±0.5058 and 1.3±0.9 D64 for correcting preexisting corneal astigmatism during cataract surgery using POCCIs of 3.2 mm.58,63,64 The experts agreed that POCCI on the most curved meridian has the potential to correct preexisting regular astigmatism of up to 1.5 D and is more effective than performing a single CCI.61,64 However, the technique has not become popular due to its lack of predictability, absence of nomogram, and increased risk of endophthalmitis.65
Corneal/limbal relaxing incisions
Corneal/limbal relaxing incisions flatten the cornea in the incised meridian; therefore, they are created on the steepest meridian. Additionally, these incisions produce a coupling effect on the meridian 90° away.66–68 Although relaxing incisions can be performed manually employing inexpensive instrumentation, the efficacy of reducing astigmatism is limited to low keratometric astigmatism as compared to procedures using an excimer laser or toric lens implantation.69,70 The maximum length of relaxing incision suggested in different nomograms is 90°.71,72 This type of incision can be single or paired and can potentially correct up to 1.5 D of astigmatism. The corneal/limbal relaxing incisions are associated with transient effects of foreign body sensation, decreased corneal sensitivity, and increased ocular dryness after surgery.
The clinical application of the femtosecond laser for creating relaxing incisions of precise length, depth, and radius presumably improves clinical outcomes.73–75 With integrated optical coherence tomography/Scheimpflug imaging, the depth of the incision can be controlled accurately, which allows making precise incisions at a depth equivalent to 85%–90% of the corneal thickness. While some surgeons choose to open the incisions at the time of surgery, it can be done up to a month later, in the office, depending on visual acuity, refraction, and topography.76 When existing nomograms71,72 of manual incisions were attempted for femtosecond laser-assisted corneal relaxing incisions, tendency for hypo-correction was observed. As such, there is a need to refine the nomograms to optimize the outcomes of laser-assisted corneal relaxing incisions.
The experts agreed that although corneal relaxing incisions are helpful in correcting astigmatism, they do not offer the predictability and stability provided by a toric IOL.69 As such, the panelists recommend performing corneal relaxing incisions only in select cases, particularly those with low astigmatism (<1.5 D), without exceeding 90° arc. Furthermore, they should not be performed in corneas which have suspicious topographic features of ectasia.59
Toric IOL implantation
Toric IOL implantation can correct preexisting astigmatism as low as 0.75 D and is the method of choice for correcting high levels of astigmatism. In addition, it is considered the most predictable method to correct astigmatism in cataract surgery, as was demonstrated in a multicenter study involving five centers, three in Europe and two in South America.77 Monofocal and presbyopia-correcting (extended depth of focus, bifocal, and trifocal) toric IOLs are available, offering high patient satisfaction and significantly reducing spectacle dependence for distance as well as near vision, when using the latter lens.78 However, they are not suitable for cases with irregular astigmatism or zonular instability. In addition, toric IOL implantation should be avoided in patients with severe dry eye, not responding to treatment. Although toric IOLs have been documented to yield promising results, a review of the literature reveals that there is high variability in visual outcomes. The prevalence of spectacle independence for distance vision following unilateral toric IOL implantation ranges from 60% to 85%,79–82 and following bilateral toric IOL implantation from 69% to 97%.30,83,84 The experts believed that this high variability in postoperative visual and refractive outcomes is due to the several factors affecting preoperative planning, surgical technique, and postoperative IOL rotation.
The experts agreed on the key factors affecting resultant refractive astigmatism following toric IOL implantation. They are shown in Table 3.
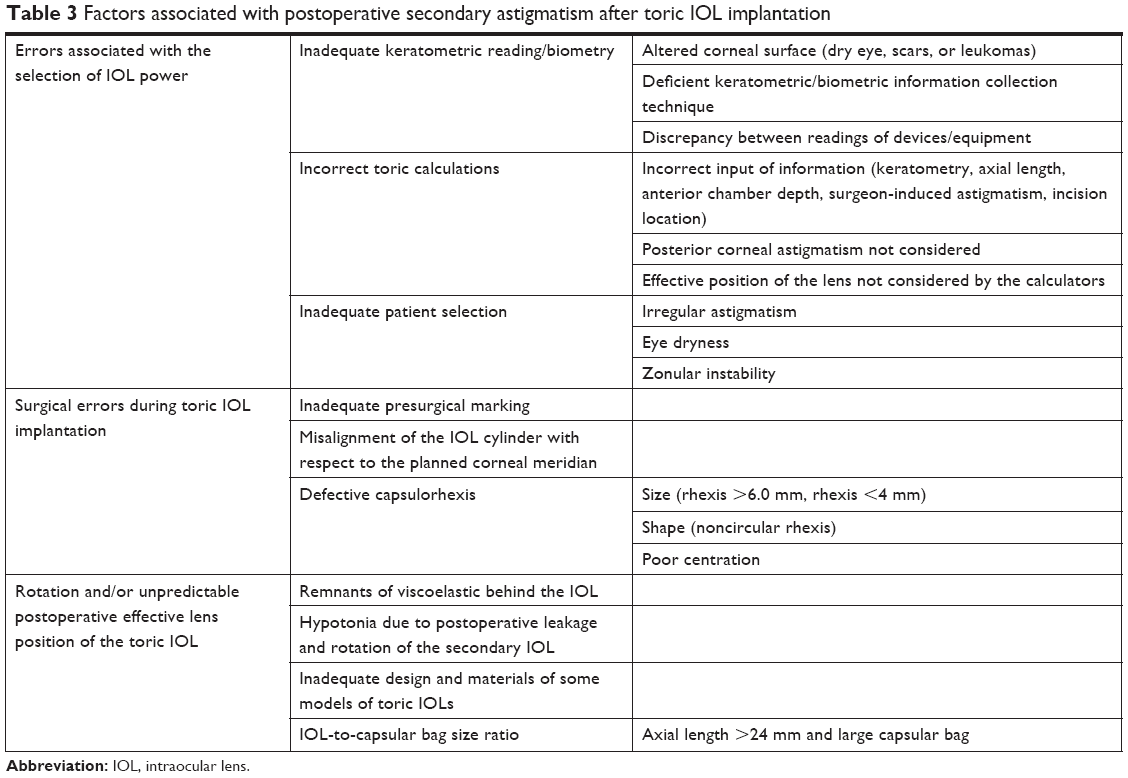 | Table 3 Factors associated with postoperative secondary astigmatism after toric IOL implantation |
Differences in the magnitude and axes of preoperative corneal astigmatism from different devices are fundamental to the high variability of resultant astigmatism observed in the literature. For example, difference between the standard keratometric astigmatism and the Scheimpflug-derived readings can be up to 0.5 D and 10° in 25% of the population.85 Similarly, the comparison of keratometric findings obtained using Lenstar LS 900 and IOL Master 500 has shown that the differences are significant.86 Likewise, the findings obtained using Lenstar LS 900 and IOL Master 500 or Topcon autokeratometer KR-8100 are found to be different.87 The axes of astigmatism measured using different devices can be highly variable. For example, a difference of >20° has been demonstrated between the measurements obtained using the Verion™ and IOL Master 500 in 21% of cases and between Verion™ and Topcon KR-8900 in 17% of cases.88 Incorrect position of the patient’s head while performing keratometry may be a possible reason for variable keratometric measurements. In addition, increased tear osmolarity due to the presence of dry eye in the patient may produce variability in mean keratometry and in astigmatism of the anterior corneal surface.27
Further, some instruments, such as Verion™ (Alcon Laboratories, Inc.), use only anterior corneal measurements for the calculations and others like Oculus Pentacam or Galilei consider an integrated value of the anterior and posterior power of the cornea.89 Ignoring posterior corneal astigmatism may yield incorrect estimation of TCA.
The panel agreed that it is important to accurately estimate SIA for optimal correction of astigmatism during cataract surgery. SIA can be influenced by several factors, such as corneal radius, size, depth, and location of the incision.90–93 Other factors include suture use, patient age, biomechanical properties of the cornea, intraoperative complications of the incision, previous surgeries in the cornea,94 and the laterality of the eye. Commonly used vector methods for calculating SIA are the polar value system,95 the Alpins method,56,96 the Holladay method,97,98 and the Thibos method.99,100 The most accepted method to calculate SIA is the vectorial sum method described by Alpins.56,96 When analyzing SIA for a case series (aggregate analysis), two methods are commonly used. One of the methods determines the mean vector magnitude by calculating arithmetic mean and disregarding the orientation of the vectors.96 In the second method, the magnitudes of the vectors are added with regard to each vector’s orientation to determine a summated vector mean of the group. This analysis is done by converting the polar values (power and axis) into Cartesian values (x/y). The centroid, thus obtained, provides the power and axis of the induced astigmatism in the aggregate of patients.98
Accurate alignment of the toric IOLs intraoperatively, after correcting for any cyclorotation, is fundamental to achieving good refractive astigmatism outcomes. This can be guided by making ink marks on the corneal limbus using the horizontal light beam on the slit lamp or the advanced manual markers (eg, pendulum marker), or using automated references in iris patterns or conjunctival vessels of the limbus. A comparative study of three types of presurgical marking methods – iridian pattern references, a pendulum marker, and a three-point corneal marker – found comparable results between the first two, which were better than the three-point corneal marker, particularly in eyes with ATR astigmatism.101 Insufficient visibility due to either dissolution of the ink or marks that are too wide and imprecise may also alter refractive astigmatism accuracy. Manual methods are also prone to corneal epithelial damage by involuntary movement of the patient.102
To overcome such problems with conventional marking system, automated image-guided systems, such as Verion™ and Callisto (Carl Zeiss Meditec AG, Jena, Germany), are helpful. Verion™ is an image-guided system, which is designed to accurately measure the eye, image anterior segment landmarks, perform IOL calculations including astigmatic corrections, and then guide the surgeon in the placement of corneal incisions and toric IOL alignment. In a single step, it measures both keratometry and pupil size and captures a high-resolution reference image of the eye, detecting anatomical landmarks (scleral vessels, limbus, pupil, and iris features) that are used for intraoperative tracking and registration. The data are automatically transferred to the Verion™, which is compatible with the LenSx Laser system (Alcon LenSx Lasers Inc., Aliso Viejo, CA, USA) and most surgical microscopes. In addition, the system tracks for eye movement and automatically adjusts for cyclotorsion. By eliminating the need for manually placed, astigmatic ink markings and the imprecisions inherent with that technique, the Verion™ system increases the accuracy of toric IOL alignment resulting in less postoperative deviation from targeted induced astigmatism.103 However, major disadvantages with this technique are that it uses an image divider in the microscope, which reduces the amount of light intended for the surgeon’s visualization. In addition, this technique does not consider posterior corneal measurements for IOL power calculation.
Callisto is another device available for precise and markerless alignment of toric IOL. Unlike Verion™, it does not require an additional planning station for data transfer from biometry to surgery. It also does not require an external image divider but is rather designed to be used directly under the microscope. However, with Callisto, it is required to have an IOL Master 700 to use the necessary images for the identification of the axis of implantation and a Zeiss Lumera microscope.
The use of intraoperative aberrometers in the aphakic state provides net corneal power, which helps to guide the selection of the IOL toric power and alignment.104 However, as was previously mentioned, factors such as edema of the incision during surgery and intraocular pressure at the time of measurement may affect its final outcome.
Toric IOLs can rotate after implantation, especially in the early postoperative period. The toric IOL offset or inclination effect may induce high-order aberrations that negatively impact the patient’s postoperative visual outcomes.105 This may be due to several reasons, which include presence of residual viscoelastic between the IOL and the posterior capsule at the end of the surgery, postoperative changes in pressure (hypotonia) that destabilize the anterior chamber, capsulorhexis size and centering, the design and material of the toric IOL, axial lengths >24 mm, and large capsular bag. There is a sinusoidal relationship between resultant cylinder and meridional misalignment of toric IOL.57 However, within 15° of off-axis rotation of the toric IOL, there is loss of astigmatic correction of ~3.5% per degree.104 If the IOL rotates by 30°, the astigmatism remains unchanged, but aligned at a meridian different from the original steep meridian.
The longer the axial length of the eye, the greater is the size of the capsular bag, which may decrease the equatorial friction on the lens, potentially reducing the IOL rotational stability. While some studies have reported a positive correlation of IOL rotation with axial length ≥24 mm,106 this relationship has not been found in other studies.107 Additionally, high myopia is associated with weak zonules, which may also affect rotational stability of the IOL.108 The IOLs with smaller diameter tend to rotate more.104,109
There are very few studies which compared the rotational stability of IOLs with regard to haptic design and optic material. Patel et al compared two IOLs with silicone optic but different haptic designs (plate and “C” loop) and found that rotational stability was higher in plate haptic IOLs as compared to loop haptic IOLs.110 Another study compared open-loop, hydrophobic acrylic IOL, and plate haptic hydrophilic acrylic IOL and found that both the IOLs had similar rotational stability.111 As such, there is not enough evidence to conclude if IOL material or haptic design affects the rotational stability of lens.
Some authors have suggested that epithelial cells of the anterior capsule should be left in situ while implanting a toric IOL.108 The fibrotic contraction of the capsular bag decreases the free space between the capsule and the lens, which may increase the rotational stability of the IOL. In addition, the panel recommended that single-piece acrylic toric IOLs must be implanted in the capsular bag; if implanted in the sulcus, there is a higher risk of iris chafing112 and rotation of the IOL, resulting in loss of astigmatism correction.
The panel concluded that the most predictable method to correct preexisting astigmatism is toric IOL implantation. However, the postoperative outcomes depend on several factors related to the measurement accuracy of the preoperative meridian and magnitude of astigmatism, type and location of CCI, accurate estimation of surgeon’s SIA, precise alignment of IOL intraoperatively, absence of IOL rotation postoperatively, etc. There are different platforms of toric IOLs that have proven to be effective and predictable; however, there are not enough prospective, randomized studies that demonstrate the superiority of one platform over another. Regarding the matter of astigmatism that must be corrected with a toric IOL, the panel recommends putting every case of cataract surgery through toric IOL calculator taking into account the type and location of the incision, the surgeon’s SIA, the existing astigmatism, and the sphere of the lens to be implanted. Finally, we should choose the suggested toric IOL, such that the resultant astigmatism is close to 0 without flipping the astigmatism axis and knowing that resultant astigmatism should be <0.75 D especially in multifocal IOLs.
Use of toric IOLs in specific conditions
Glaucoma
Several studies have suggested that glaucoma affects contrast sensitivity to a greater extent than visual acuity.113 In fact, contrast sensitivity has been found to inversely correlate with visual field loss. In glaucoma patients undergoing cataract surgery, contrast sensitivity may potentially be improved with aspheric IOLs; however, if these lenses decenter, they may induce more aberrations than non-aspheric IOLs.114 For the management of astigmatism in such patients, aspheric monofocal toric IOLs can be used. However, caution must be taken when performing combined cataract and filtering surgery.115
Pseudoexfoliation (PXF) syndrome
Patients with PXF have zonular weakness and may not respond to pharmacologic pupil dilation preoperatively.116 These patients are also predisposed to intraoperative zonular dialysis. Toric IOL implantation in such patients may not be successful, as the lens and bag may rotate, or tilt once implanted, altering the patients’ vision.117 For this reason, the use of toric IOL in patients with PXF should be avoided.
Fuchs’ dystrophy
Although toric IOL implantation has been used successfully for astigmatism correction at the time of triple Descemet’s membrane endothelial keratoplasty procedure in patients with Fuchs’ dystrophy, the use of toric IOL is less predictable in such patients.118 As such, the authors recommend avoiding toric IOL implantation in such cases.
Maculopathy
When there is a risk of retinal/macular disease, toric IOL should be avoided due to unpredictable stability over time.
Keratoconus
As discussed above, postoperative outcomes after toric IOL implantation depend on the repeatability of keratometric measurements. Since keratoconus is a progressive disorder, toric IOL implantation should only be considered in patients with stable corneal topography over a period of at least 1 year. Hashemi et al compared the repeatability of keratometry measurements with five different devices in keratoconus eyes and reported that in cases with maximum keratometry reading >55.0 D, all devices had reduced repeatability.119 As such, toric IOL implantation should be avoided in keratoconus eyes with maximum keratometry >55 D.
Management of resultant astigmatism
Despite the use of advanced technology and the best efforts to plan and execute the surgery, resultant astigmatism may still occur. The experts recommended that resultant astigmatism (≥0.75 D) should be corrected if it generates significant patient dissatisfaction with symptoms, such as blurred vision, dysphotopsia, photophobia, and diplopia.120 Alpins et al have described several reasons of refractive surprises after toric IOL implantation, which include incision effect, incision position, IOL power, and IOL orientation.121 Understanding these factors may enable surgeons to choose appropriate methods of managing resultant astigmatism. Online toric calculators, such as ASSORT (http://www.assort.com/assort-vector-calculator-0; accessed October 5, 2018), can be used for rotational analysis of the implanted toric IOL to calculate any required rotation that may minimize the refractive cylinder postoperatively. The panel agreed that for correction of resultant refractive error post-cataract surgery, corneal ablation procedures,122–124 arcuate keratotomy, or IOL replacement can be considered. Of the ablative procedures, although both photorefractive keratectomy (PRK) and LASIK yield similar outcomes, LASIK is the preferred option as it offers faster visual rehabilitation along with good results.125–129 However, LASIK should only be performed if the patients are younger than 60 years, do not have dry eye symptoms, have a healthy cornea without corneal ectasia or secondary irregular astigmatism, and sufficient estimated residual bed thickness. Additionally, the refraction should be stable; usually, about 3 months is a prudent and appropriate period after cataract surgery.130 The experts recommended that if a patient is not eligible for LASIK, PRK is the second option. Arcuate keratotomy can also be considered to correct resultant astigmatism; however, the predictability of this procedure is relatively low. Replacement of the IOL should be considered in cases of high refractive surprises, and in such cases, the replacement should be immediate. If a patient is eligible neither for corneal ablation nor for IOL replacement, a piggyback IOL can be considered.
Astigmatism and dysfunctional lens syndrome (DLS)
With the advancing technology and increasing awareness about DLS, interest in offering clear lens extraction (CLE) for DLS is increasing. Some authors even classify this syndrome as stages 1, 2, and 3 based on degree of loss in accommodation, optical aberrations, and densitometry of the crystalline lens.131
Given that the treatment of DLS stage 2 is essentially the same as cataract, that is, implantation of IOL but following extraction of clear (yet dysfunctional) lens, it was pertinent to ask whether DLS with preexisting astigmatism can be treated with same methods as cataract with preexisting astigmatism. The experts felt that although the technologies that currently exist for the treatment of cataract with preexisting astigmatism can also be used for the treatment of DLS, ophthalmic surgeons are advised to make extensive preoperative assessments for appropriate patient selection weighing the risks vs the benefits of the procedure. For example, DLS patients with preexisting high myopia with long axial length and partial posterior vitreous detachment have an increased risk of retinal detachment (ranging from 0.0% to 7.3%),132–140 as compared to cataract patients (ranging from 0.005% to 0.0179%).141–144 In addition, the use of premium IOLs, in general, leads to a reduction in contrast sensitivity especially at high spatial frequencies.145–148 In such cases, exhaustive questioning about the family history may reveal individual risk factors which could predict possible future occurrence of the retinal, corneal, or glaucomatous diseases. Such patients should be treated cautiously. It is important to note that following CLE surgery, patients report greater discomfort in their daily lives postoperatively due to secondary visual effects compared to patients with cataract surgery, probably, due to the absence of photic phenomenon preoperatively.147 Such patients need substantial preoperative counseling to reinforce the notion that most of these symptoms cause discomfort at the beginning of the process and tend to decrease or disappear after 6 months. Due to the abovementioned challenges associated with CLE, the panelists recommend that such surgeries should be performed by experienced surgeons who have adequate technology available to achieve satisfactory visual outcomes.
Practice patterns related to measurement and treatment of preexisting astigmatism during cataract surgery vary across the world. This project provides several agreements and recommendations for the measurement and treatment of astigmatism during cataract surgery, which would help ophthalmic surgeons adopt optimal practices for cataract patients with preexisting astigmatism and improve patient outcomes.
Acknowledgments
The authors thank the Colombian Association of Cataract and Refractive Surgeons (ASOCCYR) for its support and Omar Salamanca, the epidemiologist who participated in the  bibliographic search for evidence. Raman Bedi, MD, critically reviewed the manuscript, and IrisARC – Analytics, Research & Consulting (Chandigarh, India) provided editorial assistance in the preparation of the manuscript. This project was primarily funded by an educational grant by Alcon – a Novartis Division – through the Colombian Association of Cataract and Refractive Surgeons (ASOCCYR). The funding body had no role in the design, contents, implementation, or interpretation of the results of this project. This funding defrayed the cost of epidemiologist, statistical analysis, rounds of the Delphi Panels, printed materials, portfolio, supplements, questionnaires, and travel of panelists to the presentation of findings in Cali, Colombia, and potential publication expenses.
bibliographic search for evidence. Raman Bedi, MD, critically reviewed the manuscript, and IrisARC – Analytics, Research & Consulting (Chandigarh, India) provided editorial assistance in the preparation of the manuscript. This project was primarily funded by an educational grant by Alcon – a Novartis Division – through the Colombian Association of Cataract and Refractive Surgeons (ASOCCYR). The funding body had no role in the design, contents, implementation, or interpretation of the results of this project. This funding defrayed the cost of epidemiologist, statistical analysis, rounds of the Delphi Panels, printed materials, portfolio, supplements, questionnaires, and travel of panelists to the presentation of findings in Cali, Colombia, and potential publication expenses.
Disclosure
MXN serves as a consultant to Ziemer Ophthalmic Systems and as a speaker to Alcon Inc. and receives travel funding from Alcon Inc. LJE receives research funding from Alcon Inc., Asico LLC, Katena Products, Inc., and Epsilon Eyecare. LN serves as a speaker to Glaukos Corp. and Abott Medical Optics. MS, AE, and VAC serve as consultants to Alcon Inc. and receive travel funding. MAH and BVV have no conflicts of interest to disclose in this work. The authors report no other conflicts of interest in this work.
References
Read SA, Collins MJ, Carney LG. A review of astigmatism and its possible genesis. Clin Exp Optom. 2007;90(1):5–19. | ||
Ferrer-Blasco T, Montés-Micó R, Peixoto-de-Matos SC, González-Méijome JM, Cerviño A. Prevalence of corneal astigmatism before cataract surgery. J Cataract Refract Surg. 2009;35(1):70–75. | ||
Khan MI, Muhtaseb M. Prevalence of corneal astigmatism in patients having routine cataract surgery at a teaching hospital in the United Kingdom. J Cataract Refract Surg. 2011;37(10):1751–1755. | ||
Michelitsch M, Ardjomand N, Vidic B, Wedrich A, Steinwender G. [Prevalence and age-related changes of corneal astigmatism in patients before cataract surgery]. Ophthalmologe. 2017;114(3):247–251. | ||
Kanellopoulos AJ, Asimellis G. Distribution and repeatability of corneal astigmatism measurements (magnitude and axis) evaluated with color light emitting diode reflection topography. Cornea. 2015;34(8):937–944. | ||
Davison JA, Potvin R. Preoperative measurement vs intraoperative aberrometry for the selection of intraocular lens sphere power in normal eyes. Clin Ophthalmol. 2017;11:923–929. | ||
Buckhurst PJ, Wolffsohn JS, Davies LN, Naroo SA. Surgical correction of astigmatism during cataract surgery. Clin Exp Optom. 2010;93(6):409–418. | ||
Jones J, Hunter D. Qualitative research: consensus methods for medical and health services research. BMJ. 1995;311(7001):376–380. | ||
Asua Batarrita J. Entre El consenso Y La evidencia científica. Gaceta Sanitaria. 2005;19(1):65–70. | ||
Guyatt G, Rennie D, Meade M, Cook D. Users’ Guides to the Medical Literature: Essentials of Evidence-Based Clinical Practice, Second Edition. New York: Mcgraw-hill; 2008. | ||
Chylack LT Jr, Wolfe JK, Singer DM, et al. The lens opacities classification system III. The longitudinal study of cataract Study Group. Arch Ophthalmol. 1993;111(6):831–836. | ||
Age-Related Eye Disease Study Research Group. The Age-Related eye Disease Study (AREDS) system for classifying cataracts from Photographs: AREDS report no. 4. Am J Ophthalmol. 2001;131(2):167–175. | ||
Cheung CY, Li H, Lamoureux EL, et al. Validity of a new computer-aided diagnosis imaging program to quantify nuclear cataract from slit-lamp Photographs. Invest Ophthalmol Vis Sci. 2011;52(3):1314–1319. | ||
Domínguez-Vicent A, Birkeldh U, Laurell CG, Carl-Gustaf L, Nilson M, Brautaset R. Objective assessment of nuclear and cortical cataracts through scheimpflug images: agreement with the LOCS III scale. PLoS One. 2016;11(2):e0149249. | ||
Grewal DS, Brar GS, Grewal SP. Correlation of nuclear cataract lens density using scheimpflug images with lens opacities classification system III and visual function. Ophthalmology. 2009;116(8):1436–1443. | ||
Li H, Lim JH, Liu J, et al. A computer-aided diagnosis system of nuclear cataract. IEEE Trans Biomed Eng. 2010;57(7):1690–1698. | ||
Magalhães FP, Costa EF, Cariello AJ, Rodrigues EB, Hofling-Lima AL. Comparative analysis of the nuclear lens opalescence by the lens opacities classification system III with nuclear density values provided by oculus Pentacam: a cross-section study using Pentacam nucleus staging software. Arq Bras Oftalmol. 2011;74(2):110–113. | ||
Pei X, Bao Y, Chen Y, Li X. Correlation of lens density measured using the Pentacam scheimpflug system with the lens opacities classification system III grading score and visual acuity in age-related nuclear cataract. Br J Ophthalmol. 2008;92(11):1471–1475. | ||
Hall NF, Lempert P, Shier RP, Zakir R, Phillips D. Grading nuclear cataract: reproducibility and validity of a new method. Br J Ophthalmol. 1999;83(10):1159–1163. | ||
Barraquer RI, Pinilla Cortés L, Allende MJ, et al. Validation of the nuclear cataract grading system BCN 10. Ophthalmic Res. 2017;57(4):247–251. | ||
Aramberri J, Araiz L, Garcia A, et al. Dual versus single scheimpflug camera for anterior segment analysis: precision and agreement. J Cataract Refract Surg. 2012;38(11):1934–1949. | ||
Hoffmann PC, Abraham M, Hirnschall N, Findl O. Prediction of residual astigmatism after cataract surgery using swept source Fourier domain optical coherence tomography. Curr Eye Res. 2014;39(12):1178–1186. | ||
Reinstein DZ, Gobbe M, Archer TJ. Anterior segment biometry: a study and review of resolution and repeatability data. J Refract Surg. 2012;28(7):509–520. | ||
Shirayama M, Wang L, Koch DD, Weikert MP. Comparison of accuracy of intraocular lens calculations using automated keratometry, a Placido-based corneal Topographer, and a combined Placido-based and dual scheimpflug corneal Topographer. Cornea. 2010;29(10):1136–1138. | ||
Shirayama M, Wang L, Weikert MP, Koch DD. Comparison of corneal powers obtained from 4 different devices. Am J Ophthalmol. 2009;148(4):528.e1–535.e1. | ||
Ventura BV, Al-Mohtaseb Z, Wang L, Koch DD, Weikert MP. Repeatability and comparability of corneal power and corneal astigmatism obtained from a point-source color light-emitting diode Topographer, a Placido-based corneal Topographer, and a low-coherence reflectometer. J Cataract Refract Surg. 2015;41(10):2242–2250. | ||
Epitropoulos AT, Matossian C, Berdy GJ, Malhotra RP, Potvin R. Effect of tear osmolarity on repeatability of keratometry for cataract surgery planning. J Cataract Refract Surg. 2015;41(8):1672–1677. | ||
Lee H, Kim TI, Kim EK. Corneal astigmatism analysis for toric intraocular lens implantation: precise measurements for perfect correction. Curr Opin Ophthalmol. 2015;26(1):34–38. | ||
Browne AW, Osher RH. Optimizing precision in toric lens selection by combining keratometry techniques. J Refract Surg. 2014;30(1):67–72. | ||
Koch DD, Jenkins RB, Weikert MP, Yeu E, Wang L. Correcting astigmatism with toric intraocular lenses: effect of posterior corneal astigmatism. J Cataract Refract Surg. 2013;39(12):1803–1809. | ||
Nemeth G, Berta A, Lipecz A, Hassan Z, Szalai E, Modis L Jr. Evaluation of posterior astigmatism measured with scheimpflug imaging. Cornea. 2014;33(11):1214–1218. | ||
Savini G, Versaci F, Vestri G, Ducoli P, Næser K. Influence of posterior corneal astigmatism on total corneal astigmatism in eyes with moderate to high astigmatism. J Cataract Refract Surg. 2014;40(10):1645–1653. | ||
Savini G, Næser K. An analysis of the factors influencing the residual refractive astigmatism after cataract surgery with toric intraocular lenses. Invest Ophthalmol Vis Sci. 2015;56(2):827–835. | ||
Gundersen KG, Potvin R. Clinical outcomes with toric intraocular lenses planned using an optical low coherence reflectometry ocular biometer with a new toric calculator. Clin Ophthalmol. 2016;10:2141–2147. | ||
Koch DD, Ali SF, Weikert MP, Shirayama M, Jenkins R, Wang L. Contribution of posterior corneal astigmatism to total corneal astigmatism. J Cataract Refract Surg. 2012;38(12):2080–2087. | ||
Ho JD, Tsai CY, Liou SW. Accuracy of corneal astigmatism estimation by neglecting the posterior corneal surface measurement. Am J Ophthalmol. 2009;147(5):788–795.e1–2. | ||
Goggin M, Zamora-Alejo K, Esterman A, van Zyl L. Adjustment of anterior corneal astigmatism values to incorporate the likely effect of posterior corneal curvature for toric intraocular lens calculation. J Refract Surg. 2015;31(2):98–102. | ||
Abulafia A, Hill WE, Franchina M, Barrett GD. Comparison of methods to predict residual astigmatism after intraocular lens implantation. J Refract Surg. 2015;31(10):699–707. | ||
Abulafia A, Koch DD, Wang L, et al. New regression formula for toric intraocular lens calculations. J Cataract Refract Surg. 2016;42(5):663–671. | ||
Barrett GD. An improved universal theoretical formula for intraocular lens power prediction. J Cataract Refract Surg. 1993;19(6):713–720. | ||
Alpins N, Ong JK, Stamatelatos G. Corneal topographic astigmatism (CorT) to quantify total corneal astigmatism. J Refract Surg. 2015;31(3):182–186. | ||
Panacea IOL and Power Calculator [homepage on Internet]. Available from: www.panaceaiolandtoriccalculator.com. Accessed June 3, 2018. | ||
Zhang L, Sy ME, Mai H, Yu F, Hamilton DR. Effect of posterior corneal astigmatism on refractive outcomes after toric intraocular lens implantation. J Cataract Refract Surg. 2015;41(1):84–89. | ||
Klijn S, Reus NJ, van der Sommen CM, Sicam VA. Accuracy of total corneal astigmatism measurements with a scheimpflug imager and a color light-emitting diode corneal Topographer. Am J Ophthalmol. 2016;167:72–78. | ||
Ferreira TB, Ribeiro P, Ribeiro FJ, O’Neill JG. Comparison of methodologies using estimated or measured values of total corneal astigmatism for toric intraocular lens power calculation. J Refract Surg. 2017;33(12):794–800. | ||
Hatch KM, Woodcock EC, Talamo JH. Intraocular lens power selection and positioning with and without intraoperative aberrometry. J Refract Surg. 2015;31(4):237–242. | ||
Ferreira TB, Ribeiro P, Ribeiro FJ, O’Neill JG. Comparison of astigmatic prediction errors associated with new calculation methods for toric intraocular lenses. J Cataract Refract Surg. 2017;43(3):340–347. | ||
Popovic M, Campos-Möller X, Schlenker MB, Ahmed II. Efficacy and Safety of Femtosecond Laser-Assisted Cataract Surgery Compared with Manual Cataract Surgery: A Meta-Analysis of 14567 Eyes. Ophthalmology. 2016;123(10):2113–2126. | ||
Villegas EA, Alcón E, Artal P. Minimum amount of astigmatism that should be corrected. J Cataract Refract Surg. 2014;40(1):13–19. | ||
Chiam PJ, Quah SA. The refractive outcome of toric lentis mPLUS implant in cataract surgery. Int J Ophthalmol. 2016;9(5):699–702. | ||
de Vries NE, Webers CA, Touwslager WR, et al. Dissatisfaction after implantation of multifocal intraocular lenses. J Cataract Refract Surg. 2011;37(5):859–865. | ||
Woodward MA, Randleman JB, Stulting RD. Dissatisfaction after multifocal intraocular lens implantation. J Cataract Refract Surg. 2009;35(6):992–997. | ||
Delrivo M, Ruiseñor Vázquez PR, Galletti JD, et al. Agreement between placido topography and scheimpflug tomography for corneal astigmatism assessment. J Refract Surg. 2014;30(1):49–53. | ||
Hamer CA, Buckhurst H, Purslow C, Shum GL, Habib NE, Buckhurst PJ. Comparison of reliability and repeatability of corneal curvature assessment with six keratometers. Clin Exp Optom. 2016;99(6):583–589. | ||
Comez AT, Ozkurt Y. Surgical correction of astigmatism during cataract surgery. In: Goggin M, editor. Astigmatism – Optics, Physiology and Management. London: InTech; 2012. | ||
Alpins NA. A new method of analyzing vectors for changes in astigmatism. J Cataract Refract Surg. 1993;19(4):524–533. | ||
Alpins NA. Vector analysis of astigmatism changes by flattening, steepening, and torque. J Cataract Refract Surg. 1997;23(10):1503–1514. | ||
Khokhar S, Lohiya P, Murugiesan V, Panda A. Corneal astigmatism correction with opposite clear corneal incisions or single clear corneal incision: comparative analysis. J Cataract Refract Surg. 2006;32(9):1432–1437. | ||
Amesbury EC, Miller KM. Correction of astigmatism at the time of cataract surgery. Curr Opin Ophthalmol. 2009;20(1):19–24. | ||
Masket S, Wang L, Belani S. Induced astigmatism with 2.2- and 3.0-mm coaxial phacoemulsification incisions. J Refract Surg. 2009;25(1):21–24. | ||
Hashemi H, Khabazkhoob M, Soroush S, Shariati R, Miraftab M, Yekta A. The location of incision in cataract surgery and its impact on induced astigmatism. Curr Opin Ophthalmol. 2016;27(1):58–64. | ||
Alpins N, Ong JK, Stamatelatos G. Asymmetric corneal flattening effect after small incision cataract surgery. J Refract Surg. 2016;32(9):598–603. | ||
Lever J, Dahan E. Opposite clear corneal incisions to correct pre-existing astigmatism in cataract surgery. J Cataract Refract Surg. 2000;26(6):803–805. | ||
Ben Simon GJ, Desatnik H. Correction of pre-existing astigmatism during cataract surgery: comparison between the effects of opposite clear corneal incisions and a single clear corneal incision. Graefe’s Arch Clin Exp Ophthalmol. 2005;243(4):321–326. | ||
Bazzazi N, Barazandeh B, Kashani M, Rasouli M. Opposite clear corneal incisions versus steep Meridian incision phacoemulsification for correction of pre-existing astigmatism. J Ophthalmic Vis Res. 2008;3(2):87–90. | ||
Carvalho MJ, Suzuki SH, Freitas LL, Branco BC, Schor P, Lima AL. Limbal relaxing incisions to correct corneal astigmatism during phacoemulsification. J Refract Surg. 2007;23(5):499–504. | ||
Ouchi M, Kinoshita S. Prospective randomized trial of limbal relaxing incisions combined with microincision cataract surgery. J Refract Surg. 2010;26(8):594–599. | ||
Wang L, Misra M, Koch DD. Peripheral corneal relaxing incisions combined with cataract surgery. J Cataract Refract Surg. 2003;29(4):712–722. | ||
Hirnschall N, Gangwani V, Crnej A, Koshy J, Maurino V, Findl O. Correction of moderate corneal astigmatism during cataract surgery: toric intraocular lens versus peripheral corneal relaxing incisions. J Cataract Refract Surg. 2014;40(3):354–361. | ||
Nanavaty MA, Bedi KK, Ali S, Holmes M, Rajak S. Toric Intraocular Lenses Versus Peripheral Corneal Relaxing Incisions for Astigmatism Between 0.75 and 2.5 Diopters During Cataract Surgery. Am J Ophthalmol. 2017;180:165–177. | ||
Nichamin LD. Astigmatism management for modern phaco surgery. Int Ophthalmol Clin. 2003;43(3):53–63. | ||
Johnson and Johnson vision. Available from: www.lricalculator.com. Accessed June 3, 2018. | ||
Mozayan E, Lee JK. Update on astigmatism management. Curr Opin Ophthalmol. 2014;25(4):286–290. | ||
Rubenstein JB, Raciti M. Approaches to corneal astigmatism in cataract surgery. Curr Opin Ophthalmol. 2013;24(1):30–34. | ||
Rückl T, Dexl AK, Bachernegg A, et al. Femtosecond laser-assisted intrastromal arcuate keratotomy to reduce corneal astigmatism. J Cataract Refract Surg. 2013;39(4):528–538. | ||
Trikha S, Turnbull AM, Morris RJ, Anderson DF, Hossain P. The journey to femtosecond laser-assisted cataract surgery: new beginnings or a false dawn? Eye (Lond). 2013;27(4):461–473. | ||
Alfonso JF, Knorz M, Fernandez-Vega L, et al. Clinical outcomes after bilateral implantation of an apodized +3.0 D toric diffractive multifocal intraocular lens. J Cataract Refract Surg. 2014;40(1):51–59. | ||
Agresta B, Knorz MC, Donatti C, Jackson D. Visual acuity improvements after implantation of toric intraocular lenses in cataract patients with astigmatism: a systematic review. BMC Ophthalmol. 2012;12:41. | ||
Mingo-Botín D, Muñoz-Negrete FJ, Won Kim HR, Morcillo-Laiz R, Rebolleda G, Oblanca N. Comparison of toric intraocular lenses and peripheral corneal relaxing incisions to treat astigmatism during cataract surgery. J Cataract Refract Surg. 2010;36(10):1700–1708. | ||
Ho JD, Tsai CY, Tsai RJ, Kuo LL, Tsai IL, Liou SW. Validity of the keratometric index: evaluation by the Pentacam rotating scheimpflug camera. J Cataract Refract Surg. 2008;34(1):137–145. | ||
Holland E, Lane S, Horn JD, Ernest P, Arleo R, Miller KM. The Acrysof toric intraocular lens in subjects with cataracts and corneal astigmatism: a randomized, subject-masked, parallel-group, 1-year study. Ophthalmology. 2010;117(11):2104–2111. | ||
Srivannaboon S, Soeharnila, Chirapapaisan C, Chonpimai P. Comparison of corneal astigmatism and axis location in cataract patients measured by total corneal power, automated keratometry, and simulated keratometry. J Cataract Refract Surg. 2012;38(12):2088–2093. | ||
Ahmed II, Rocha G, Slomovic AR, et al. Visual function and patient experience after bilateral implantation of toric intraocular lenses. J Cataract Refract Surg. 2010;36(4):609–616. | ||
Lane SS, Ernest P, Miller KM, Hileman KS, Harris B, Waycaster CR. Comparison of clinical and patient-reported outcomes with bilateral Acrysof toric or spherical control intraocular lenses. J Refract Surg. 2009;25(10):899–901. | ||
Zheng T, Chen Z, Lu Y. Influence factors of estimation errors for total corneal astigmatism using keratometric astigmatism in patients before cataract surgery. J Cataract Refract Surg. 2016;42(1):84–94. | ||
Cruysberg LP, Doors M, Verbakel F, Berendschot TT, De Brabander J, Nuijts RM. Evaluation of the Lenstar LS 900 non-contact biometer. Br J Ophthalmol. 2010;94(1):106–110. | ||
Jasvinder S, Khang TF, Sarinder KK, Loo VP, Subrayan V. Agreement analysis of LENSTAR with other techniques of biometry. Eye (Lond). 2011;25(6):717–724. | ||
Asena L, Güngör SG, Akman A. Comparison of keratometric measurements obtained by the Verion image guided system with optical biometry and auto-keratorefractometer. Int Ophthalmol. 2017;37(2):391–399. | ||
Davison JA, Potvin R. Refractive cylinder outcomes after calculating toric intraocular lens cylinder power using total corneal refractive power. Clin Ophthalmol. 2015;9:1511–1517. | ||
Alió J, Rodríguez-Prats JL, Galal A, Ramzy M. Outcomes of microincision cataract surgery versus coaxial phacoemulsification. Ophthalmology. 2005;112(11):1997–2003. | ||
Altan-Yaycioglu R, Akova YA, Akca S, Gur S, Oktem C. Effect on astigmatism of the location of clear corneal incision in phacoemulsification of cataract. J Refract Surg. 2007;23(5):515–518. | ||
Borasio E, Mehta JS, Maurino V. Torque and flattening effects of clear corneal temporal and on-axis incisions for phacoemulsification. J Cataract Refract Surg. 2006;32(12):2030–2038. | ||
Tejedor J, Murube J. Choosing the location of corneal incision based on preexisting astigmatism in phacoemulsification. Am J Ophthalmol. 2005;139(5):767–776. | ||
Lyhne N, Corydon L. Two year follow-up of astigmatism after phacoemulsification with adjusted and unadjusted sutured versus sutureless 5.2 MM superior scleral incisions. J Cataract Refract Surg. 1998;24(12):1647–1651. | ||
Naeser K. Assessment and statistics of surgically induced astigmatism. Acta Ophthalmol. 2008;86(3):349. | ||
Alpins N. Astigmatism analysis by the Alpins method. J Cataract Refract Surg. 2001;27(1):31–49. | ||
Holladay JT, Dudeja DR, Koch DD. Evaluating and reporting astigmatism for individual and aggregate data. J Cataract Refract Surg. 1998;24(1):57–65. | ||
Holladay JT, Moran JR, Kezirian GM. Analysis of aggregate surgically induced refractive change, prediction error, and intraocular astigmatism. J Cataract Refract Surg. 2001;27(1):61–79. | ||
Thibos LN, Horner D. Power vector analysis of the optical outcome of refractive surgery. J Cataract Refract Surg. 2001;27(1):80–85. | ||
Thibos LN, Wheeler W, Horner D. Power vectors: an application of Fourier analysis to the description and statistical analysis of refractive error. Optom Vis Sci. 1997;74(6):367–375. | ||
Onishi H, Torii H, Watanabe K, Tsubota K, Negishi K. Comparison of clinical outcomes among 3 marking methods for toric intraocular lens implantation. Jpn J Ophthalmol. 2016;60(3):142–149. | ||
Popp N, Hirnschall N, Maedel S, Findl O. Evaluation of 4 corneal astigmatic marking methods. J Cataract Refract Surg. 2012;38(12):2094–2099. | ||
Elhofi AH, Helaly HA. Comparison between digital and manual marking for toric intraocular lenses: a randomized trial. Medicine (Baltimore). 2015;94(38):e1618. | ||
Ventura BV, Wang L, Weikert MP, Robinson SB, Koch DD. Surgical management of astigmatism with toric intraocular lenses. Arq Bras Oftalmol. 2014;77(2):125–131. | ||
He L, Applegate RA. Predicting crystalline lens fall caused by accommodation from changes in wavefront error. J Cataract Refract Surg. 2011;37(7):1313–1322. | ||
Shah GD, Praveen MR, Vasavada AR, Vasavada VA, Rampal G, Shastry LR. Rotational stability of a toric intraocular lens: influence of axial length and alignment in the capsular bag. J Cataract Refract Surg. 2012;38(1):54–59. | ||
Mencucci R, Favuzza E, Guerra F, Giacomelli G, Menchini U. Clinical outcomes and rotational stability of a 4-haptic toric intraocular lens in myopic eyes. J Cataract Refract Surg. 2014;40(9):1479–1487. | ||
Zhu X, He W, Zhang K, Lu Y. Factors influencing 1-year rotational stability of Acrysof toric intraocular lenses. Br J Ophthalmol. 2016;100:263–268. | ||
Chang DF. Early rotational stability of the longer Staar toric intraocular lens: fifty consecutive cases. J Cataract Refract Surg. 2003;29(5):935–940. | ||
Patel CK, Ormonde S, Rosen PH, Bron AJ. Postoperative intraocular lens rotation: a randomized comparison of plate and loop haptic implants. Ophthalmology. 1999;106(11):2190–2195; discussion 2196. | ||
Scialdone A, De Gaetano F, Monaco G. Visual performance of 2 aspheric toric intraocular lenses: comparative study. J Cataract Refract Surg. 2013;39(6):906–914. | ||
Chang DF, Masket S, Miller KM, et al; ASCRS Cataract Clinical Committee. Complications of sulcus placement of single-piece acrylic intraocular lenses: recommendations for backup IOL implantation following posterior capsule rupture. J Cataract Refract Surg. 2009;35(8):1445–1458. | ||
Hawkins AS, Szlyk JP, Ardickas Z, Alexander KR, Wilensky JT. Comparison of contrast sensitivity, visual acuity, and Humphrey visual field testing in patients with glaucoma. J Glaucoma. 2003;12(2):134–138. | ||
Teichman JC, Ahmed II. Intraocular lens choices for patients with glaucoma. Curr Opin Ophthalmol. 2010;21(2):135–143. | ||
Paletta Guedes RA, Paletta Guedes VM, Aptel F. [Multifocal, toric, and aspheric intraocular lenses for glaucoma patients]. J Fr Ophtalmol. 2011;34(6):387–391. | ||
Belovay GW, Varma DK, Ahmed II. Cataract surgery in pseudoexfoliation syndrome. Curr Opin Ophthalmol. 2010;21(1):25–34. | ||
Ichhpujani P, Bhartiya S, Sharma A. Premium IOLs in glaucoma. J Curr Glaucoma Pract. 2013;7(2):54–57. | ||
Yokogawa H, Sanchez PJ, Mayko ZM, Straiko MD, Terry MA. Astigmatism correction with toric intraocular lenses in Descemet membrane endothelial keratoplasty triple procedures. Cornea. 2017;36(3):269–274. | ||
Hashemi H, Yekta A, Khabazkhoob M. Effect of keratoconus grades on repeatability of keratometry readings: comparison of 5 devices. J Cataract Refract Surg. 2015;41(5):1065–1072. | ||
Alio JL, Abdelghany AA, Fernández-Buenaga R. Enhancements after cataract surgery. Curr Opin Ophthalmol. 2015;26(1):50–55. | ||
Alpins N, Ong JK, Stamatelatos G. Refractive surprise after toric intraocular lens implantation: graph analysis. J Cataract Refract Surg. 2014;40(2):283–294. | ||
Sánchez-Galeana CA, Smith RJ, Rodriguez X, Montes M, Chayet AS. Laser in situ keratomileusis and photorefractive keratectomy for residual refractive error after phakic intraocular lens implantation. J Refract Surg. 2001;17(3):299–304. | ||
Macsai MS, Fontes BM. Refractive enhancement following presbyopia-correcting intraocular lens implantation. Curr Opin Ophthalmol. 2008;19(1):18–21. | ||
Kuo IC, O’Brien TP, Broman AT, Ghajarnia M, Jabbur NS. Excimer laser surgery for correction of ametropia after cataract surgery. J Cataract Refract Surg. 2005;31(11):2104–2110. | ||
Alfonso JF, Fernández-Vega L, Montés-Micó R, Valcárcel B. Femtosecond laser for residual refractive error correction after refractive lens exchange with multifocal intraocular lens implantation. Am J Ophthalmol. 2008;146(2):244–250. | ||
Ayala MJ, Pérez-Santonja JJ, Artola A, Claramonte P, Alió JL. Laser in situ keratomileusis to correct residual myopia after cataract surgery. J Refract Surg. 2001;17(1):12–16. | ||
Jendritza BB, Knorz MC, Morton S. Wavefront-guided excimer laser vision correction after multifocal IOL implantation. J Refract Surg. 2008;24(3):274–279. | ||
Jin GJ, Merkley KH, Crandall AS, Jones YJ. Laser in situ keratomileusis versus lens-based surgery for correcting residual refractive error after cataract surgery. J Cataract Refract Surg. 2008;34(4):562–569. | ||
Kim P, Briganti EM, Sutton GL, Lawless MA, Rogers CM, Hodge C. Laser in situ keratomileusis for refractive error after cataract surgery. J Cataract Refract Surg. 2005;31(5):979–986. | ||
Moshirfar M, McCaughey MV, Santiago-Caban L. Corrective techniques and future directions for treatment of residual refractive error following cataract surgery. Expert Rev Ophthalmol. 2014;9(6):529–537. | ||
Dysfunctional lens syndrome, a new way to educate patients. Eye Net. 2016. Available from: https://www.aao.org/eyenet/academy-live/detail/dysfunctional-lens-syndrome-educate-patients. Accessed May 14, 2018. | ||
Barraquer C, Cavelier C, Mejía LF. Incidence of retinal detachment following clear-lens extraction in myopic patients. Retrospective analysis. Arch Ophthalmol. 1994;112(3):336–339. | ||
Gris O, Güell JL, Manero F, Müller A. Clear lens extraction to correct high myopia. J Cataract Refract Surg. 1996;22(6):686–689. | ||
Lee KH, Lee JH. Long-term results of clear lens extraction for severe myopia. J Cataract Refract Surg. 1996;22(10):1411–1415. | ||
Jiménez-Alfaro I, Miguélez S, Bueno JL, Puy P. Clear lens extraction and implantation of negative-power posterior chamber intraocular lenses to correct extreme myopia. J Cataract Refract Surg. 1998;24(10):1310–1316. | ||
Fernández-Vega L, Alfonso JF, Villacampa T. Clear lens extraction for the correction of high myopia. Ophthalmology. 2003;110(12):2349–2354. | ||
Pucci V, Morselli S, Romanelli F, Pignatto S, Scandellari F, Bellucci R. Clear lens phacoemulsification for correction of high myopia. J Cataract Refract Surg. 2001;27(6):896–900. | ||
Alió JL. Lens surgery (cataract and refractive lens exchange) and retinal detachment risk in myopes: still an issue? Br J Ophthalmol. 2011;95(3):301–303. | ||
Neuhann IM, Neuhann TF, Heimann H, Schmickler S, Gerl RH, Foerster MH. Retinal detachment after phacoemulsification in high myopia: analysis of 2356 cases. J Cataract Refract Surg. 2008;34(10):1644–1657. | ||
Ravalico G, Michieli C, Vattovani O, Tognetto D. Retinal detachment after cataract extraction and refractive lens exchange in highly myopic patients. J Cataract Refract Surg. 2003;29(1):39–44. | ||
Algvere PV, Jahnberg P, Textorius O. The Swedish retinal detachment register. I. A database for epidemiological and clinical studies. Graefes Arch Clin Exp Ophthalmol. 1999;237(2):137–144. | ||
Haimann MH, Burton TC, Brown CK. Epidemiology of retinal detachment. Arch Ophthalmol. 1982;100(2):289–292. | ||
Lois N, Wong D. Pseudophakic retinal detachment. Surv Ophthalmol. 2003;48(5):467–487. | ||
Rowe JA, Erie JC, Baratz KH, et al. Retinal detachment in Olmsted County, Minnesota, 1976 through 1995. Ophthalmology. 1999;106(1):154–159. | ||
Anton A, Böhringer D, Bach M, Reinhard T, Birnbaum F. Contrast sensitivity with bifocal intraocular lenses is halved, as measured with the Freiburg vision test (FrACT), yet patients are happy. Graefes Arch Clin Exp Ophthalmol. 2014;252(3):539–544. | ||
Gil MA, Varón C, Cardona G, Vega F, Buil JA. Comparison of far and near contrast sensitivity in patients symmetrically implanted with multifocal and monofocal IOLs. Eur J Ophthalmol. 2014;24(1):44–52. | ||
Hida WT, Motta AF, Kara-José Junior N, et al. Comparison between OPD-Scan results and visual outcomes of monofocal and multifocal intraocular lenses. Arq Bras Oftalmol. 2009;72(4):526–532. | ||
Venter JA, Pelouskova M, Bull CE, Schallhorn SC, Hannan SJ. Visual outcomes and patient satisfaction with a rotational asymmetric refractive intraocular lens for emmetropic presbyopia. J Cataract Refract Surg. 2015;41(3):585–593. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.