")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
CONQUEST Quality Standards: For the Collaboration on Quality Improvement Initiative for Achieving Excellence in Standards of COPD Care
Authors Pullen R , Miravitlles M , Sharma A, Singh D, Martinez F , Hurst JR , Alves L , Dransfield M, Chen R, Muro S , Winders T, Blango C, Muellerova H , Trudo F, Dorinsky P , Alacqua M, Morris T , Carter V, Couper A , Jones R , Kostikas K , Murray R , Price DB
Received 1 April 2021
Accepted for publication 30 June 2021
Published 12 August 2021 Volume 2021:16 Pages 2301—2322
DOI https://doi.org/10.2147/COPD.S313498
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Rachel Pullen, 1, 2 Marc Miravitlles, 3 Anita Sharma, 4 Dave Singh, 5 Fernando Martinez, 6 John R Hurst, 7 Luis Alves, 8, 9 Mark Dransfield, 10 Rongchang Chen, 11 Shigeo Muro, 12 Tonya Winders, 13 Christopher Blango, 14 Hana Muellerova, 15 Frank Trudo, 16 Paul Dorinsky, 17 Marianna Alacqua, 15, 18 Tamsin Morris, 19 Victoria Carter, 1, 2 Amy Couper, 1, 2 Rupert Jones, 20 Konstantinos Kostikas, 1, 21 Ruth Murray, 1 David B Price 1, 2, 22
1Observational and Pragmatic Research Institute, Singapore, Singapore; 2Optimum Patient Care, Cambridge, UK; 3Pneumology Dept, Hospital Universitari Vall d’Hebron, Vall d’Hebron Institut de Recerca (VHIR), Vall d’Hebron Barcelona Hospital Campus, CIBER de Enfermedades Respiratorias (CIBERES), Barcelona, Spain; 4Platinum Medical Centre, Chermside, QLD, Australia; 5Division of Infection, Immunity & Respiratory Medicine, University of Manchester, Manchester University NHS Foundation Trust, Manchester, UK; 6New York-Presbyterian Weill Cornell Medical Center, New York, NY, USA; 7UCL Respiratory, University College London, London, UK; 8EPI Unit, Institute of Public Health, University of Porto, Porto, Portugal; 9Laboratory for Integrative and Translational Research in Population Health (ITR), Porto, Portugal; 10Division of Pulmonary, Allergy, and Critical Care Medicine, Lung Health Center, University of Alabama at Birmingham, Birmingham, AL, USA; 11Key Laboratory of Respiratory Disease of Shenzhen, Shenzhen Institute of Respiratory Disease, Shenzhen People’s Hospital (Second Affiliated Hospital of Jinan University, First Affiliated Hospital of South University of Science and Technology of China), Shenzhen, People’s Republic of China; 12Department of Respiratory Medicine, Nara Medical University, Nara, Japan; 13USA & Global Allergy & Airways Patient Platform, Vienna, Austria; 14Janssen Pharmaceutical Companies of Johnson & Johnson, Philadelphia, PA, USA; 15AstraZeneca, Cambridge, UK; 16AstraZeneca, Wilmington, DE, USA; 17AstraZeneca, Durham, NC, USA; 18CSL Behring SpA, Milan, Italy; 19AstraZeneca, Luton, UK; 20Research and Knowledge Exchange, Plymouth Marjon University, Plymouth, UK; 21Respiratory Medicine Department, University of Ioannina School of Medicine, Ioannina, Greece; 22Centre of Academic Primary Care, Division of Applied Health Sciences, University of Aberdeen, Aberdeen, UK
Correspondence: David B Price
Centre of Academic Primary Care, Division of Applied Health Sciences, University of Aberdeen, Polwarth Building, Foresterhill, Aberdeen, AB25 2ZD, UK
Tel +65 3105 1489
Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) are managed predominantly in primary care. However, key opportunities to optimize treatment are often not realized due to unrecognized disease and delayed implementation of appropriate interventions for both diagnosed and undiagnosed individuals. The COllaboratioN on QUality improvement initiative for achieving Excellence in STandards of COPD care (CONQUEST) is the first-of-its-kind, collaborative, interventional COPD registry. It comprises an integrated quality improvement program focusing on patients (diagnosed and undiagnosed) at a modifiable and higher risk of COPD exacerbations. The first step in CONQUEST was the development of quality standards (QS). The QS will be imbedded in routine primary and secondary care, and are designed to drive patient-centered, targeted, risk-based assessment and management optimization. Our aim is to provide an overview of the CONQUEST QS, including how they were developed, as well as the rationale for, and evidence to support, their inclusion in healthcare systems.
Methods: The QS were developed (between November 2019 and December 2020) by the CONQUEST Global Steering Committee, including 11 internationally recognized experts with a specialty and research focus in COPD. The process included an extensive literature review, generation of QS draft wording, three iterative rounds of review, and consensus.
Results: Four QS were developed: 1) identification of COPD target population, 2) assessment of disease and quantification of future risk, 3) non-pharmacological and pharmacological intervention, and 4) appropriate follow-up. Each QS is followed by a rationale statement and a summary of current guidelines and research evidence relating to the standard and its components.
Conclusion: The CONQUEST QS represent an important step in our aim to improve care for patients with COPD in primary and secondary care. They will help to transform the patient journey, by encouraging early intervention to identify, assess, optimally manage and followup COPD patients with modifiable high risk of future exacerbations.
Keywords: identification, assessment, intervention, follow-up
Plain Language Summary
Under-diagnosis and under-treatment of COPD results in significantly higher risk of exacerbations, morbidity and death. Early identification and appropriate management should mitigate that risk. The COllaboratioN on QUality improvement initiative for achieving Excellence in STandards of COPD care (CONQUEST) aims to improve the management of patients at greater risk of future COPD exacerbations by developing and implementing quality standards (QS) into routine care and measuring implementation success. This is an area where important improvements in patient care and outcomes can be made and measured.
Four QS were developed: 1) identification of COPD target population, 2) assessment of disease and quantification of future risk, 3) appropriate non-pharmacological/pharmacological intervention, and 4) appropriate follow-up. The target population are patients with COPD (or potential COPD) with ≥2 moderate, or ≥1 severe exacerbations in the last 24 months (≥1 of these in the last 12 months) AND with scope for management optimization. Each QS is followed by a rationale statement and summary of current guidelines/evidence to support it and its components.
These QS represent a first step in empowering primary and secondary care providers to identify, assess, quantify risk, treat, and follow-up the millions of people living with COPD (both diagnosed and undiagnosed) at increased risk of exacerbations, morbidity and mortality. By incorporating these QS into routine care, CONQUEST aims to affect sustained change to COPD patient care. The QS will be used as a benchmark to monitor the impact of quality improvement on COPD outcomes in two planned CRTs in the UK and the USA.
Introduction
Despite being a largely preventable disease, the global burden of chronic obstructive pulmonary disease (COPD) is high and remains a public health priority in the 21st century.1 COPD affects approximately 384 million people worldwide and is the third leading cause of death.2,3 It is frequently under-diagnosed, under-treated, and has high morbidity, including a greater risk of cardiovascular (CV) disease and death.3–5 COPD is projected to be responsible for a loss of 45 million quality-adjusted life years, 315 million exacerbations, and 9 million deaths cumulatively in the USA over the next 20 years, assuming current patterns of treatment and smoking rates.6 The socio-economic burden of COPD is also high, with projected 20-year (2019–2038) discounted direct and indirect costs estimated at $801 billion and $101 billion, respectively, in the USA.6 Similarly, the average total annual per patient cost of COPD management (excluding medications) in the United Kingdom has been estimated at £3396 for those experiencing ≥2 moderate-to-severe exacerbations. Primary care associated costs contribute most to overall expenditure.7
COPD is initially managed predominantly in primary care, but key opportunities to optimize management are often not realized due to unrecognized disease and delayed implementation of appropriate interventions for both diagnosed and undiagnosed individuals.8,9 A study carried out in the UK found that opportunities for diagnosis were missed in 85% of the patients in the 5 years immediately preceding COPD diagnosis.8 As a consequence, many patients receive no treatment or delayed initiation of maintenance therapy, even after diagnosis.9 This is important since interventions such as smoking cessation and pulmonary rehabilitation10,11 may improve prognosis and drugs such as inhaled corticosteroids (ICS) may improve current symptoms and exacerbations that are associated with rapid lung function loss.12 Furthermore, patients who experience a greater exacerbation burden after initiation of maintenance therapy have worse lung function at diagnosis and a more rapid lung function decline thereafter, emphasizing the need for better treatment strategies.13 These findings highlight the importance of earlier intervention among patients with COPD, to more proactively diagnose and manage optimally. Current gaps in COPD management and the need for improved quality of care have been recognized both in the UK and the USA.14–18 In the USA, specific goals of the COPD national action plan14 are to raise public awareness of COPD, educate key stakeholders in diagnosis, prevention, and treatment, and encourage data sharing/dissemination. In the UK, the Department of Health has similar goals for COPD management.16,18
The COllaboratioN on QUality improvement initiative for achieving Excellence in STandards of COPD care (CONQUEST) is a new program providing a roadmap to improved quality of COPD care,19 and aligns with the aims of both the COPD National Action Plan and the UK Department of Health. CONQUEST is the first-of-its-kind collaborative, interventional, COPD registry with an integrated quality improvement program. Its vision is to drive change in the management of patients (both diagnosed and undiagnosed) at a greater risk of future COPD exacerbations and to measure the success of implementing this change in cluster randomized trials. This vision will be achieved by closing gaps in current COPD care provision, imbedding quality standards (QS) in routine primary care, integrating information from these patients, and presenting it to clinicians in a way that drives patient-centered, targeted, risk-based assessment and treatment optimization, thus empowering both patients and physicians to improve COPD care.19 The registry will be populated from local and global data sources and will hold anonymized data from over 200,000 primary and secondary care COPD patients (both diagnosed and undiagnosed) at modifiable high risk for COPD exacerbations. Patients will be identified through, and data collected from, electronic medical records (EMR). These data will be further supplemented through patient questionnaires and enhanced clinical assessments.19
The first step in the CONQUEST program is the development of QS. The aim of this article is to provide an overview of the CONQUEST QS, including how they were developed, as well as the rationale for, and evidence to support, their inclusion.
Methods
Quality Standard Design
These QS are core research and evidence-based statements that underpin the CONQUEST initiative and are intended to cover care for a targeted COPD population (see CONQUEST target patients below), a large proportion of whom may be positively impacted by quality COPD care. When developing these QS, consideration was given to 1) practicality and ease of use by all stakeholders (eg, clinicians, policy makers, advocacy groups), 2) future-proofing the QS, by advocating general principles rather than a stringent and didactic approach, 3) feasibility of implementation in routine clinical practice, 4) the need to compare QS adherence and impact on disease outcomes across healthcare systems and 5) inter-country differences in COPD burden (morbidity, mortality, socio-economic), and patterns of treatment and access to care. Ethical approval from an Independent Review Board was not required as this article outlines QS informed by review of evidence in the public domain, no participants were recruited and data were neither collected nor analyzed.
The CONQUEST Target Patients
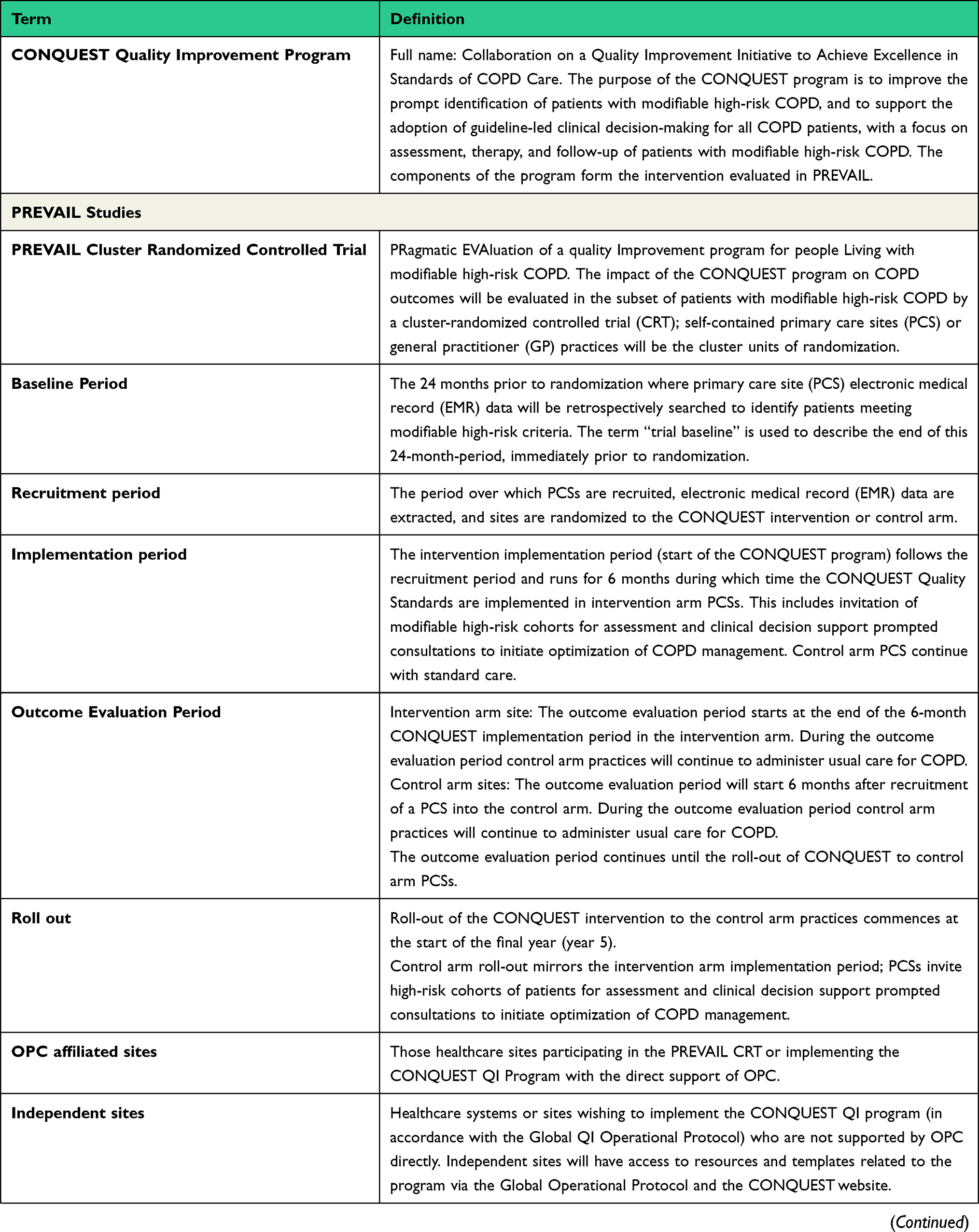
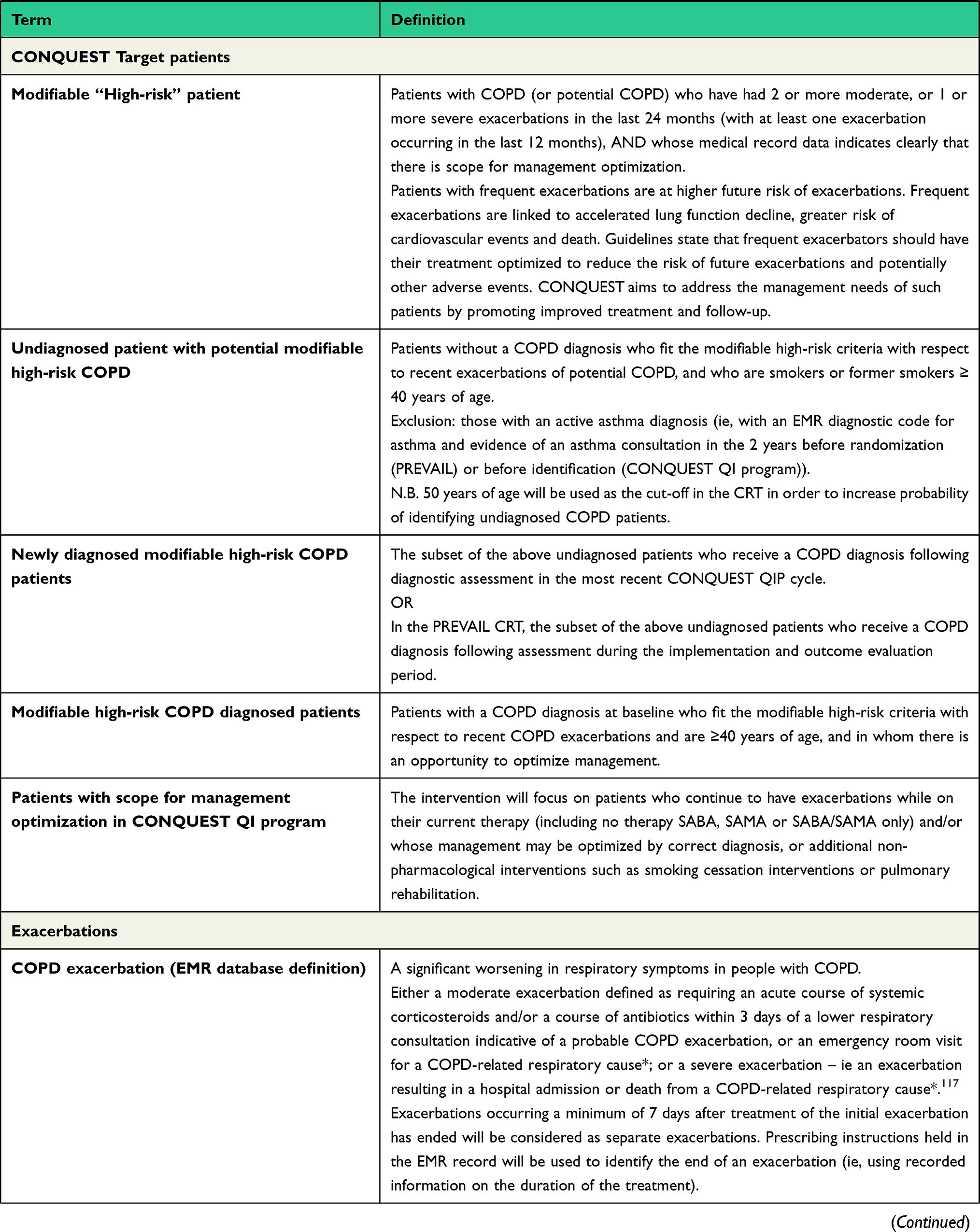
Two CONQUEST groups have been identified: those with a COPD diagnosis at baseline and those without a COPD diagnosis who fit the modifiable high-risk criteria. Please refer to Table 1 for a summary of CONQUEST key terms. Modifiable high-risk patients are those with COPD (or potential COPD) who have had ≥2 moderate or ≥1 severe (hospitalized) exacerbation in the last 24 months (with at least one exacerbation occurring in the last 12 months) AND whose medical record data clearly indicates scope for management optimization. Management optimization focuses on patients who continue to have exacerbations while on their current therapy (including no therapy or short-acting β2-agonist only) and/or whose management may be optimized by correct diagnosis or additional non-pharmacological interventions. COPD exacerbations are defined as a significant worsening in respiratory symptoms in people with COPD (or an event analogous to a COPD exacerbation in people with suspected but undiagnosed COPD) and are categorized as moderate or severe. CONQUEST patients are required to be ≥40 years of age and, for those with potential COPD, to have a current or previous smoking history (ie, current or ex-smokers with ≥10 pack-year history or ≥10 years smoking duration).
 |
 |
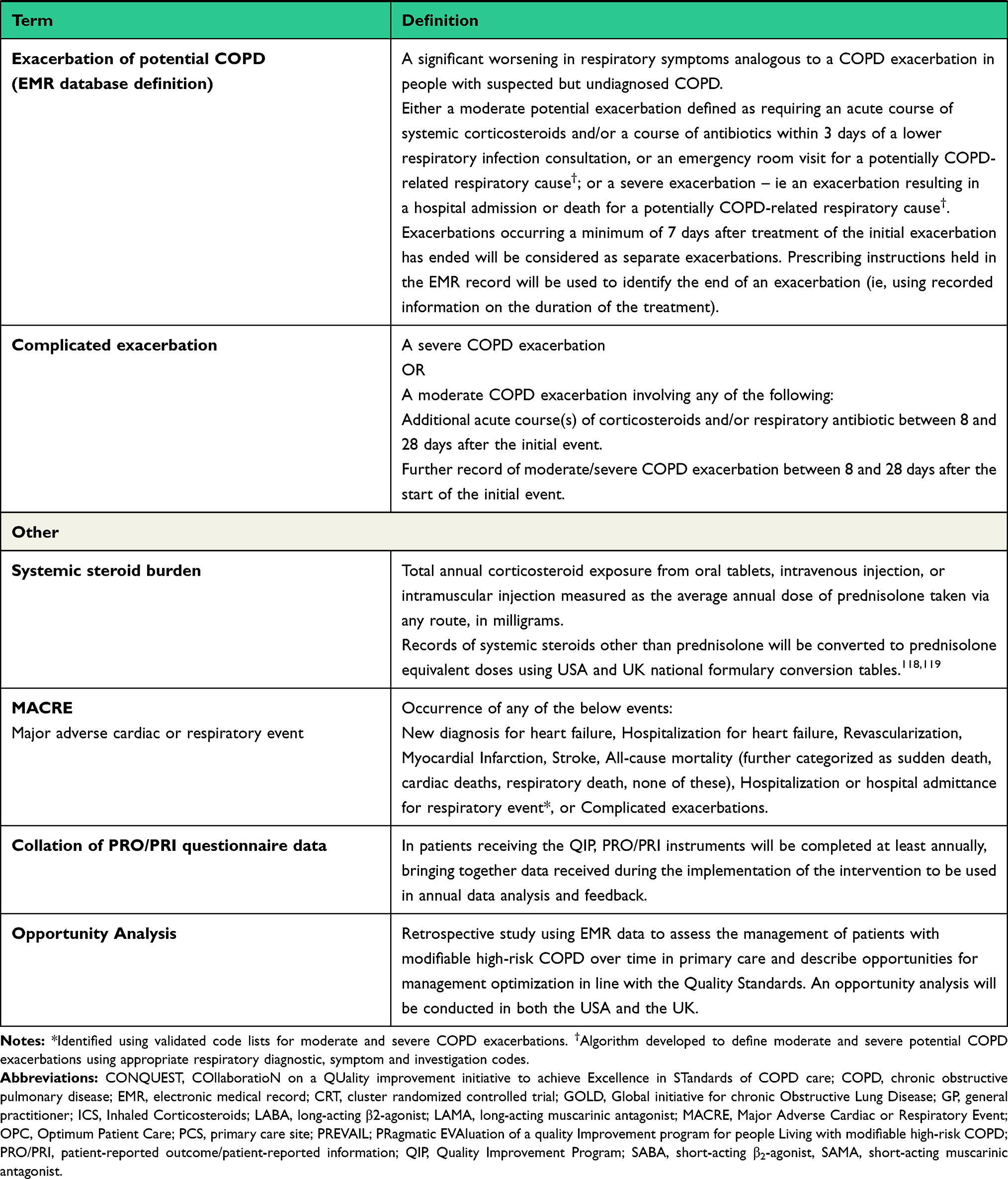 |
Table 1 Lexicon of CONQUEST Key Terms |
CONQUEST Task Force
The CONQUEST QS task force comprises the Global Steering Committee, including 11 internationally recognized experts with a specialty and research focus in COPD from 8 countries across 4 continents, as well as 2 AstraZeneca members (Table 2). Membership of the task force was weighted towards the UK and the USA as it is in these countries where the QS will be initially implemented and trialed, before rolling out to other countries. Task force members are all experts in the field of COPD. Criteria for task force membership included 1) publication history; 2) leadership of national or international initiatives that have focused on high-risk COPD patients; or 3) experience as a primary care medical provider, patient representative or with cardiology expertise. Their role is to provide scientific advice on CONQUEST research projects and quality improvement program implementation, and to ensure that CONQUEST research is ethical, clinically appropriate, and continues to bring value to patients and physicians.
 |
Table 2 Members of the CONQUEST Quality Standard Task Force |
Quality Standard Development
The process included an extensive literature review as well as discussions with, and consensus of, experts of the CONQUEST Global Steering Committee and is summarized in Figure 1. Eight QS were initially identified, predominantly based on the National Institute for Health and Care Excellence (NICE) and Global initiative for chronic Obstructive Lung Disease (GOLD) recommendations, but also informed by the American Thoracic Society (ATS)/European Respiratory Society guidelines.3,20–22 Relevant references cited within these guidelines were also reviewed in addition to research identified through literature review.3,25–27 These eight QS were prioritized, consolidated (following several rounds of review by Optimum Patient Care medical experts) and sent to the CONQUEST QS Task Force for review and comment. The process consisted of three iterative rounds, and consensus was achieved following several meetings and via email correspondence. The process began in November 2019 and concluded in December 2020.
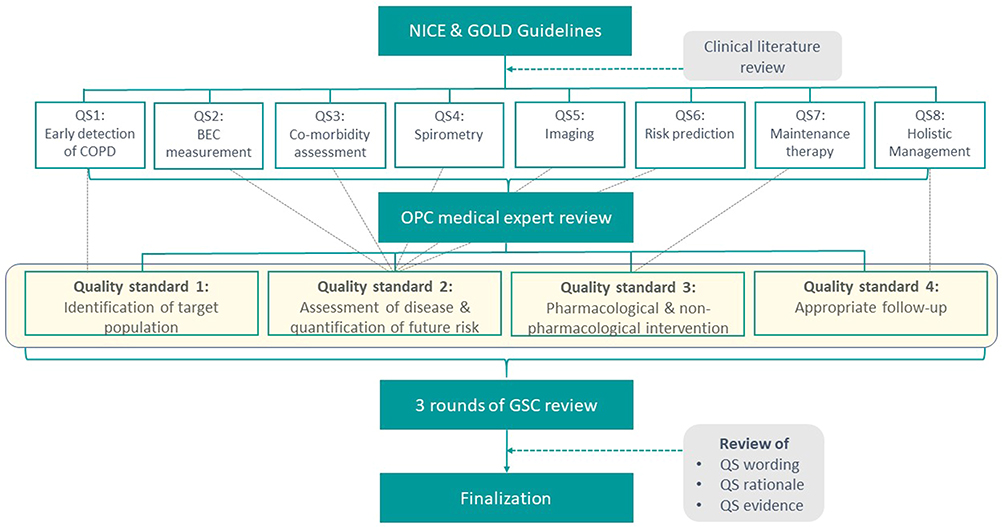 |
Figure 1 CONQUEST quality standards development process. Abbreviations: BEC, blood eosinophil count; CONQUEST, COllaboratioN on QUality improvement initiative for achieving Excellence in STandards of COPD care; COPD, chronic obstructive pulmonary disease; GOLD, Global initiative for chronic Obstructive Lung Disease; GSC, Global Steering Committee; NICE, National Institute for Health and Clinical Excellence; OPC, optimum patient care; QS, quality standard. |
Global steering committee consensus was achieved for each of the four CONQUEST QS. Each QS is followed by a short statement explaining the rationale behind it and a summary of current guidelines and research evidence relating to the standard and its components.
Results
Quality Standard 1: Identification of Target Population
Identify individuals ≥40 years of age (with or without a pre-existing COPD diagnosis) with a history of smoking or relevant environmental exposure, at increased risk of exacerbations, morbidity, and mortality and with scope for COPD management optimization.
And, within this population, identify those with greater cardiovascular risk (Figure 2).
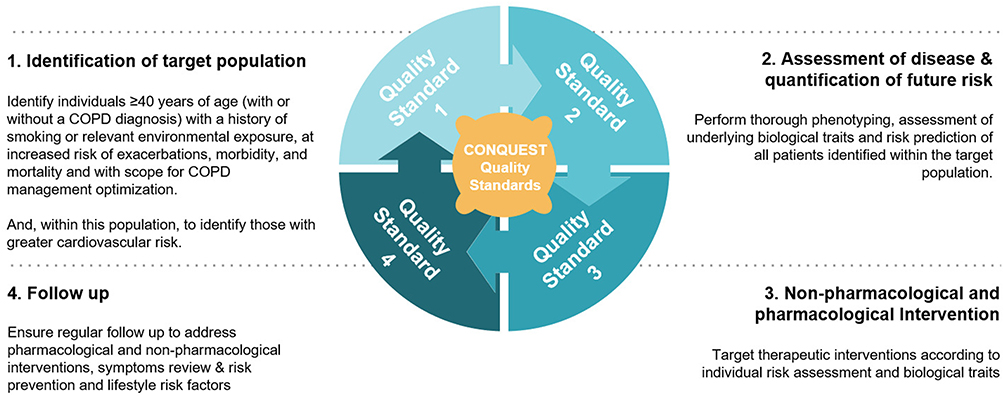 |
Figure 2 CONQUEST quality standards for the identification and management of patients with COPD at risk of exacerbations or acute respiratory events. Abbreviations: CONQUEST, COllaboratioN on QUality improvement initiative for achieving Excellence in STandards of COPD care; COPD, chronic obstructive pulmonary disease. |
Rationale
The lives of COPD patients are significantly impacted by the disease. This informed the CONQUEST decision to focus our efforts on those individuals (both diagnosed and undiagnosed) at risk of exacerbating and to intervene earlier in the COPD journey in order to slow the speed of COPD progression (eg, accelerated lung function decline, increased exacerbation frequency, deterioration in co-morbidity control). A focus on patients at higher risk of exacerbating is an area in which large and important improvements in patient care and outcomes can be made and measured. These patients require more intense focus on identification and assessment in order to optimize management. The goal of optimized management is to reduce the number of exacerbations and consequent lung function decline and disease progression, thereby improving patient health-related quality of life (HRQoL) and decreasing CV risk associated with exacerbations.
Supporting Evidence
Evidence to support QS 1 is summarized in Table 3 and described in more detail here.
- Diagnostic delay: COPD diagnosis is often delayed.8,23 Data from the Optimum Patient Care Research Database found that 85% of patients had consulted primary or secondary care for lower respiratory symptoms in the 5 years prior to their diagnosis, and 58% had consulted in the 10 years prior to diagnosis.8 Diagnosing COPD early (feasibly 5–10 years earlier based on UK data)8 in the disease progression is important, since undiagnosed patients have an increased risk of exacerbations and pneumonia, compared to their non-COPD counterparts.24 Use of a targeted approach (focused case-finding methods) using characteristics such as age, smoking history, and respiratory symptoms may help to find these undiagnosed COPD patients.25,26 Physicians are more than seven times more likely to detect undiagnosed COPD in the targeted group (vs a routine care group), translating into one new case identified for every 21 targeted individuals assessed (after risk difference adjustment).26 Undiagnosed patients who present to their health care provider (HCP) form part of the target population for CONQUEST, particularly those with a smoking history, who consult with lower respiratory symptoms, who received medication for lower respiratory illness or who were admitted to hospital or treated in an outpatient setting with respiratory symptoms.
- Management optimization: COPD often remains undertreated, with a gap between guideline recommendations and real world practice.9,27,28 Medical and pharmacy claims data in the USA found that >65% of COPD patients were receiving no maintenance therapy,27 whereas in the UK, three quarters of patients with a modified Medical Research Council (mMRC) dyspnea score <2 but ≥2 exacerbations/year were considered under-treated.9 Although patients hospitalized with severe exacerbations usually receive recommended care, once discharged, most patients receive inappropriate support and medications.29
- Exacerbation frequency: Many patients with COPD experience ≥2 exacerbations/year.30 For example, 22% of patients with moderate COPD had frequent exacerbations in the ECLIPSE study.31 Furthermore, real-world data found that COPD patients who had ≥2 lower respiratory prescribing consultations in the 2 years preceding diagnosis were over three times more likely to have ≥2 exacerbations in the year after diagnosis.8 Earlier identification and treatment of patients who frequently exacerbate is likely to protect lung function, reduce CV risk and improve patients’ HRQoL since 1) frequent exacerbations accelerate lung function decline,12,32 2) exacerbations of COPD increase the risk of major adverse CV events,33–36 and 3) frequency of exacerbation is associated with worse HRQoL.37,38 COPD patients with CV disease are four times more likely to have a subsequent CV event if they exacerbate, and 10 times more likely to have a subsequent CV disease (eg, cardiovascular death, myocardial infarction, stroke, unstable angina or transient ischemic attack) if the exacerbation required hospitalization.36
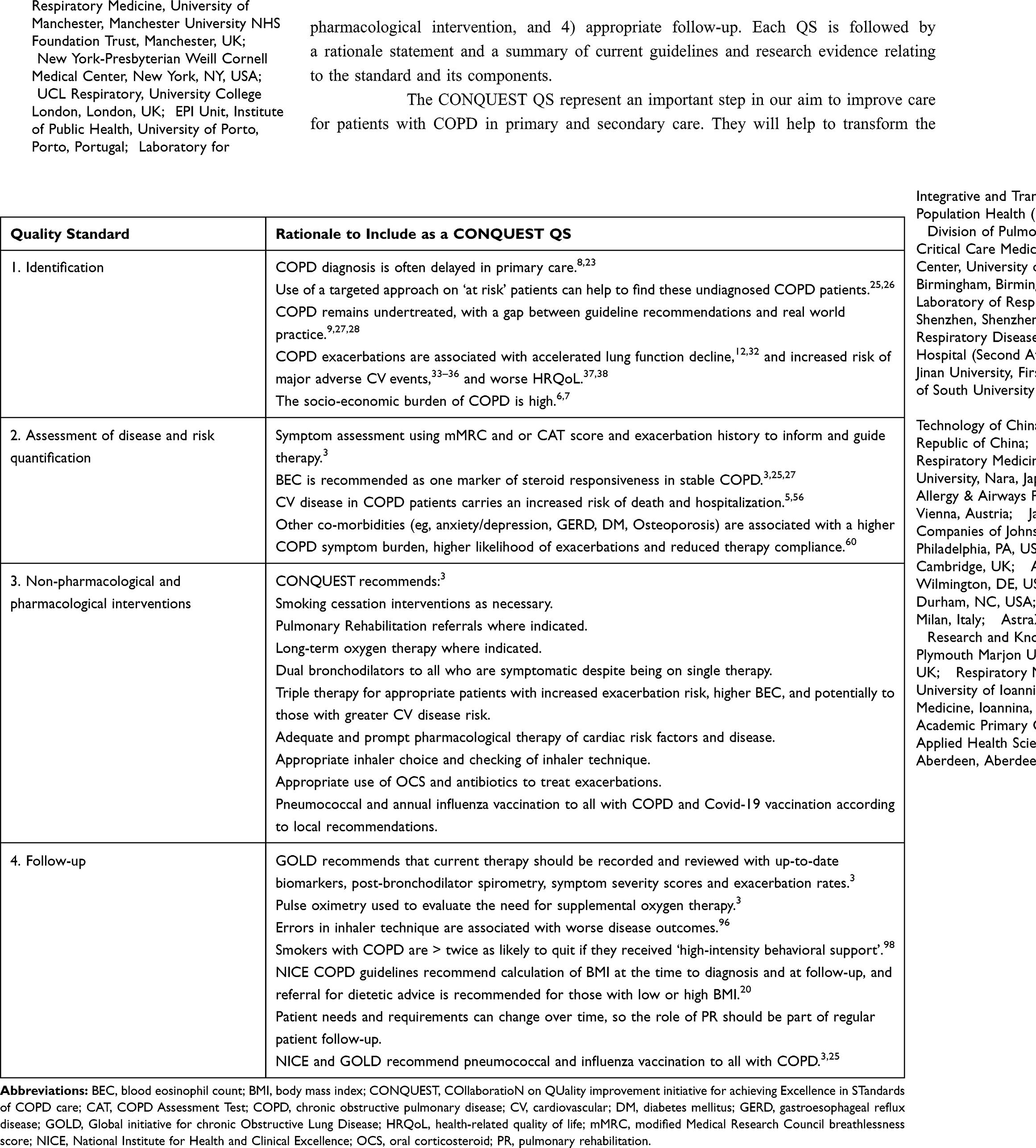 |
Table 3 COPD Quality Standards and Rationale for Their Inclusion in CONQUEST |
Quality Standard 2: Assessment of Disease and Quantification of Future Risk
Perform thorough phenotyping, assessment of underlying biological traits and risk prediction of all patients identified within the target population (Figure 2).
Rationale
Different COPD phenotypes require different therapeutic interventions. Thorough assessment will enable accurate individual prediction of future risk of exacerbations, disease progression, mortality and CV risk, with the goal to guide therapy.
The assessment of individuals with COPD (both diagnosed and undiagnosed) with modifiable high risk of morbidity (including exacerbations) and mortality should include assessment of 1) symptoms and exacerbation history, 2) spirometry and other measures of lung function, 3) body mass index (BMI), 4) blood eosinophil count (BEC), 5) chest imaging, 6) cardiovascular risk assessment, 7) identification of co-morbidities, 8) use of relevant risk prediction tools and 9) smoking exposure and physical activity.
Supporting Evidence
Evidence to support QS 2 is summarized in Table 3 and described in more detail here.
- Symptoms: NICE guidelines recommend the use of the MRC dyspnea scale for grading breathlessness at annual follow-up and when diagnosing COPD (in conjunction with other symptoms). The COPD Assessment Test is a method of assessing symptom burden in COPD that incorporates common symptoms.20,22 The results of symptom assessment measures can be used to guide pharmacological therapy in accordance with GOLD recommendations.3
- Post-bronchodilator spirometry: Recommended in clinical guidelines to be used in conjunction with clinical assessment to confirm the diagnosis of COPD,3,22 and is incentivized as part of the Quality Outcomes Framework in the UK. Longitudinal spirometry results can be used to measure lung function decline and response to therapy and can help guide therapy interventions.3,12
- Body mass index: BMI is associated with COPD prognosis,20 and included in several risk prediction tools and models to determine exacerbation risk and/or mortality risk.39,40 Low BMI (ie, <21.75 kg/m2) has been associated with increased risk of pneumonia and mortality in COPD patients.41,42 Obesity, with BMI >30 kg/m2, is a risk factor for the development of type II diabetes,43 a relevant comorbidity for those who frequently exacerbate and require oral corticosteroids (OCS).
- Blood eosinophil count: In stable COPD, BEC is recommended as a marker of steroid responsiveness, with higher BEC used as an indicator for ICS therapy.3,25,27 This recommendation is informed by the fact that those with higher BEC have less exacerbations when treated with ICS/long acting β2-agonist (LABA) versus LABA alone,44,45 or with ICS/LABA/long acting muscarinic agonist (LAMA) vs LAMA/LABA.46–48 Similarly, ICS are beneficial in reducing the number of exacerbations in those with elevated BEC, with exacerbation rate reductions increasing with increasing BEC.49 Real-life data also showed that elevated BEC was associated with better outcomes for those on triple therapy (vs dual bronchodilator therapy),50 and in frequent exacerbators is associated with more rapid lung function decline.12 Higher BEC (ie, >200 cells/µL) may also be a predictor of OCS success in those experiencing exacerbations,51 and eosinophil guided therapy has been shown to reduce OCS exposure in patients admitted to hospital with acute exacerbation of COPD.52 Taken together, these results suggest the value of BEC to tailor treatments to specific COPD phenotypes and endotypes. However, BEC is commonly not available and/or underused in primary care and is not routinely considered in treatment decisions. More work on implementation in everyday clinical care is needed.
- Imaging: Such as chest x-ray or CT scan is useful in suspected and/or confirmed COPD to exclude other respiratory pathologies.3,20 Chest CT scans are necessary when considering lung volume reduction,3,25 for the detection of bronchiectasis and for those requiring lung cancer assessment.3 CT chest scans (paired insp-exp) can aid early diagnosis of COPD by identifying air trapping, and standard CT scans can identify airway wall thickening, and can discriminate between emphysematous and non-emphysematous phenotypes.53,54 The former is a predictor for reduced survival as is pulmonary artery:aorta ratio.55 However, it is recognized that CT scanning in all patients with COPD may not be feasible in the real-life setting.
- CV risk assessment: CV diseases are perhaps the most important co-morbidities in COPD and carry an increased risk of death and hospitalization.5,56 COPD patients have a twofold higher risk of having CV disease (including ischemic heart disease, arrhythmias and heart failure) than their non-COPD counterparts.57 Furthermore, cardiac mortality in patients with moderate COPD is higher than mortality due to respiratory failure,58 and prognosis following an acute cardiac event is worse for those who also have a diagnosis of COPD.35
- Identification of co-morbidities: Co-morbidities besides CV disease (eg, anxiety/depression, gastroesophageal reflux disease, diabetes mellitus, and osteoporosis) are common in COPD and may be encountered at any level of disease severity.3,9,59 These co-morbidities are associated with a higher COPD symptom burden, higher likelihood of exacerbations and reduced therapy compliance.60 Although the GOLD strategy document advises that, in general, the presence of co-morbidities should not change COPD treatment, these comorbidities can have a significant impact on disease course.3
- Risk prediction tools: For example, the BODE index, which integrates BMI, airflow limitation (forced expiratory volume in one second (FEV1)), dyspnea and 6-minute walk distance, are useful to predict COPD mortality.61 Another multicomponent index, DOSE (dyspnea, obstruction, smoking, exacerbations), has been shown to identify COPD patients with a greater risk of future worsening in health status and exacerbations.62,63 Others have found that risk of developing COPD in adulthood can be identified using lifetime lung function trajectory patterns and is 57% greater in those individuals with a parental history.64,65 These risk prediction tools may be used to guide therapy and highlight those most at risk of exacerbations, disease progression, and mortality within the target population.
- Smoking (tobacco, e-cigarette/vaping), exposure and physical activity: The NICE guidelines suggest a multifactorial approach to assess risk of exacerbations including ongoing smoking, exposure to pollutants, infection, insufficient physical activity, seasonal variation and frequency of exacerbations.20 GOLD acknowledge that smoking cessation is key for COPD prevention and for maintenance therapy. However, the effectiveness of e-cigarettes as a smoking cessation aid is uncertain since e-cigarette use has been associated with severe acute lung injury, eosinophilic pneumonia, alveolar hemorrhage, respiratory bronchiolitis and other lung abnormalities.3,66,67
Quality Standard 3: Non-Pharmacological and Pharmacological Intervention
Target therapeutic interventions according to individual risk assessment and biological traits (Figure 2).
Rationale
Both non-pharmacological and pharmacological interventions are essential for effective COPD management. These are used to reduce symptoms, reduce the frequency and severity of exacerbations, and improve exercise tolerance and health status.3 In accordance with published literature and expert opinion, the GOLD strategy document, and NICE and ATS guidelines, the CONQUEST program recommends the following3,22:
Non-Pharmacological Interventions
- Smoking cessation interventions as appropriate
- Pulmonary rehabilitation referrals, where indicated
- Long-term oxygen therapy, where indicated
- Pneumococcal and annual influenza vaccination to all with COPD
- Patient motivation and engagement enhanced by patient-reported outcome information and shared decision-making.
Pharmacological Interventions
- Dual bronchodilators (LABA/LAMA) to all who are symptomatic on long-acting bronchodilator monotherapy.
- Triple therapy (ICS/LABA/LAMA) for appropriate patients with exacerbations and elevated BEC, and potentially to those with greater CV disease risk and greater risk of mortality (ie, severe exacerbations).
- In line with national guidelines for initial and follow-up therapy. Follow-up therapy should reflect both background therapy, symptom response and exacerbation risk based on actual exacerbations and COPD control.
- Adequate and prompt pharmacological therapy of cardiac risk factors and disease according to latest guideline recommendations.
- Regularly assess inhaler choice and technique.
- Short courses of OCS and/or antibiotics during exacerbations as per GOLD or other national/international guideline recommendations.
Supporting Evidence
Evidence to support QS 3 is summarized in Table 3 and described in more detail here.
Non-Pharmacological Interventions
- Smoking cessation: Has the greatest capacity to influence the natural history of COPD. The earlier smoking cessation is achieved the greater the impact on preventing lung function decline.68 There is also an associated reduction in symptoms following smoking cessation.69
- Pulmonary rehabilitation: Improves dyspnea, health status and exercise tolerance in stable patients.3,10,11 Started soon after an exacerbation of COPD, pulmonary rehabilitation is safe, effective and associated with fewer subsequent hospital admissions for exacerbations.70 It is recommended by NICE to all “who view themselves as functionally disabled by COPD (usually MRC of grade 3 or above)”,25 and by GOLD as part of integrated COPD patient management.3
- Long-term oxygen therapy: Has been shown to increase survival in patients with severe resting hypoxemia. GOLD recommend it for patients who have 1) PaO2 ≤7.3 kPa or SaO2 ≤88% with or without hypercapnia confirmed twice over a 3-week period or 2) for those with PaO2 7.3–8.0 kPa or SaO2 of 88% if there is evidence of pulmonary hypertension, peripheral edema suggesting congestive cardiac failure or polycythemia (hematocrit >55%).3 Domiciliary non-invasive ventilation has proven utility in those with more severe disease.71
- Vaccination: NICE and GOLD recommend offering pneumococcal and annual influenza vaccination to all with COPD.3,20 More recently, people with more severe COPD have been prioritized for COVID-19 vaccine, and as these become available, local recommendations should be followed. Influenza vaccinations have been shown to reduce death and illness, such as lower respiratory tract infections, in COPD patients.72,73 An updated Cochrane review also concluded that inactivated influenza vaccine led to fewer COPD exacerbations, but noted that there were a limited number of randomized controlled trials available on the topic.74 Pneumococcal vaccination also reduces the likelihood of COPD exacerbation.75 While not currently part of any COPD guidelines, there has been some recent discussion regarding the role of pertussis booster vaccination in COPD patients, due to a resurgence of pertussis and evidence that COPD patients are at high risk of contracting the disease.76
- Patient motivation and engagement: GOLD recognizes the benefit of personalized, multi-component, education and training for patients with COPD (rather than simply providing information and advice).3 Shared decision-making and patient engagement have been shown to significantly improve perceived health status, COPD knowledge, adherence to pharmacological treatment, general functionality and healthy lifestyle measures for COPD patients hospitalized for acute exacerbations.77
Pharmacological Interventions
The GOLD strategy document classifies COPD patients initiating therapy into ABCD groups based on health status as assessed by CAT, mMRC dyspnea score and exacerbation history, and recommends appropriate targeted pharmacological intervention for each group.3 The CONQUEST cohort are likely to fall within GOLD groups C or D. A dyspnea or exacerbation directed step up approach is advised if response to this initial treatment is not sufficient. Patients with dyspnea as their predominant symptom should be stepped up to dual LABA/LAMA (if on LABA or LAMA monotherapy) and consider switching inhaler device or investigation of other causes of dyspnea for those who remain symptomatic on dual bronchodilators.3 De-escalation of ICS should only be considered for those who become low risk over time or have reasons to be cautious of ICS use, including low eosinophil count and pneumonia.3,78 Exacerbating patients on LABA or LAMA mono-therapy should be stepped up to LABA/LAMA or ICS/LABA (if BEC≥300 or BEC ≥100 plus ≥2 exacerbations), and then to triple therapy if response is insufficient.3
- Dual bronchodilators (to all who are symptomatic on long-acting bronchodilator monotherapy): Multiple studies have found improvements in lung function, symptoms and HRQoL with dual bronchodilators when compared to single therapy or placebo.79
- Triple therapy (ICS/LABA/LAMA) for appropriate patients with exacerbations and higher BEC, and potentially to those with greater CV disease risk and greater risk of mortality): Most beneficial to symptomatic COPD patients with an exacerbation history despite dual therapy. Also recommended for those patients with higher BEC (ie, ≥300 cells/µL).80,81 COPD patients with a history of exacerbations treated with triple therapy experienced better HRQoL, better lung function and fewer moderate-to-severe exacerbations, compared to those treated with either LABA/LAMA or ICS/LABA; with 25% and 16% less exacerbations, respectively.82 ICS-containing regimens were associated with a lower rate of death from CV and respiratory causes and lower all-cause mortality.82,83 However, in keeping with other studies,84,85 an increased incidence of pneumonia was noted for those on ICS.82 For example, studies of salmeterol/fluticasone in COPD found that the number needed to treat to induce one case of pneumonia ranged from 16 to 20.86 More recently, the ETHOS study also found that compared to those on dual therapy, patients on ICS triple therapy experienced a significantly lower annual exacerbation rate (budesonide/glycopyrronium/formoterol) vs LAMA/LABA: (number needed to treat) (NNT)=3 and vs ICS/LABA: NNT=7],87 with lower mortality rates (any cause) noted in the higher ICS group.47 Pneumonia rates across triple and dual therapies were low, between 0.02 and 0.05 per patient-year and were lower for budesonide/glycopyrronium/formoterol than budesonide/formoterol (number needed to harm=58), suggesting a low pneumonia risk for budesonide/glycopyrronium/formoterol relative to its benefits on exacerbations.87
- Adequate and prompt pharmacological therapy of cardiac risk factors and disease: Although CV medications can cause concerns among prescribers over possible side effects or interactions in COPD patients leading to under-treatment of CV disease,88 the overall principle advocated by current COPD guidelines is that treatment of comorbidities should not be altered by the presence of COPD.3 The use of cardio-selective β1-blockers where indicated in ischemic heart disease and heart failure is considered safe with the benefits of treatment outweighing any potential risks.89 The current GOLD report advises that heart failure should be treated no differently in COPD patients and use of cardio-selective β-blockers is recommended.3
- Regularly assess inhaler choice and technique: While ensuring the right drug is prescribed to the patient at the correct dose is important for treatment success, method of delivery and inhaler training are often overlooked. Choice of inhaler should be tailored to the individual patient where possible and consideration given not only to what the inhaler contains (eg, drug class/particle size) but also inspiratory flow, ease of use, patient preference, age, cognition, manual dexterity and coordination.90 Regular checking of inhaler technique is also important and has been associated with improved therapy adherence.91
- Short course of OCS for exacerbations (when clinically indicated): GOLD strategy suggests consideration of a course of OCS of between 5 and 7 days for moderate or severe acute exacerbations.3 Use of OCS in these situations is associated with improved lung function, oxygenation and recovery time.92 Similarly for those with raised BEC, treatment with OCS during an acute exacerbation has been associated with a reduction in treatment failure and hospitalization.51 The NICE guidelines also recommend short-term OCS use (typically 5 days) in all people admitted to hospital with an exacerbation of COPD (if no contraindications) and to consider their use in community settings when an exacerbation is associated with “a significant increase in breathlessness that interferes with daily activities”.13 OCS can be associated with significant side effects in both the short and long term.93
Quality Standard 4: Appropriate Follow-Up
Ensure regular follow-up to address non-pharmacological and pharmacological intervention by symptoms review and assessing risk prediction and lifestyle risk factors (Figure 2).
Rationale
Ongoing effort over time is required to change behavior and determine the appropriate course of therapy. Not all aspects of COPD care can be discussed and addressed in an initial consultation or risk assessment and therefore require a long-term patient treatment strategy.
Supporting Evidence
Evidence to support QS 4 is summarized in Table 3 and described in more detail here.
To improve quality of care for COPD patients, efforts to provide individualized treatment plans and interventions must be ongoing.3 This cycle of ongoing review and assessment involves pharmacological, clinical, and non-pharmacological components as outlined below:
- Medication, inhaler device and symptom review: Current therapy should be recorded and reviewed with up-to-date biomarkers, spirometry, symptom severity scores and exacerbation rates. Pulse oximetry (at rest, during a 6-minute walk or overnight) can be used to estimate a patient’s arterial oxygen saturation and need for supplemental oxygen therapy, and is important in all patients with clinical signs suggestive of respiratory failure or right heart failure.3 Use of the COPD control tool may help to achieve appropriate and faster clinical review to evaluate response to therapy and escalate treatment where appropriate.94,95
- Inhaler technique: There is evidence that errors in inhaler technique are associated with worse disease outcomes in both asthma and COPD.96 Conversely, significant improvement in inhaler technique has been associated with improved COPD control,97 and checking of inhaler technique (within the last 2 years) is associated with better adherence.91
- Smoking cessation: A Cochrane review in 2016 found evidence that smokers with COPD were more than twice as likely to quit if they received “high-intensity behavioral support” as well as medication, compared to those receiving only behavioral support.98 There was no clear evidence that any one form of support or medication was better than another.
- Nutrition: NICE COPD guidelines recommend calculation of BMI at the time of diagnosis and at follow-up, and referral for dietetic advice is recommended for those with low or high BMI.20
- Pulmonary rehabilitation: Patient needs and requirements can change over time, so the role of pulmonary rehabilitation should be part of regular patient follow-up. Patients should be referred if the therapy is likely to be beneficial. Considerations regarding patients suitable for referral include discussion of patient goals and their ability to perform the exercises, as well as noting the need to commit to a course of therapy lasting at least 6 to 8 weeks.3,99 The likely benefits of the program should be emphasized to the patient. The ability of clinicians to refer patients to a suitable pulmonary rehabilitation program may be limited by resources and availability.
- Vaccination: Should be offered to COPD patients at review in accordance with local policies (please also see point 4 of QS 3 supporting evidence for non-pharmacological intervention).
- Motivation and engagement: For quality improvement initiatives of this kind to be successful, there must be motivation to drive long-term behavioral changes, from both the physician/clinical team and the patient. In the past, therapeutic nihilism has been a feature of COPD care, but there is evidence that this feeling that little can be done for COPD patients is changing, with improving primary care physician knowledge and awareness of COPD guidelines.100 Ensuring that motivation is sustained beyond the trial phase is a critical part of the CONQUEST initiative. Patients may not be motivated to seek medical help due to a lack of understanding of the disease itself, feelings of guilt and stigma associated with a COPD diagnosis,101,102 the feeling that it is “too late” to change or simply due to ignoring symptoms and/or attributing them to another cause.103,104 Greater public awareness and knowledge of the condition and the possibilities for its treatment are needed to counter these issues. Implementing behavior-targeted interventions with the aim of improving physical activity should also be considered as physical activity is often significantly reduced in COPD patients.105 According to GOLD (2021),3 “This can lead to a downward spiral of inactivity, predisposing patients to reduced QoL, increased rates of hospitalization and mortality”.106,107
Discussion
These CONQUEST QS represent a roadmap to improved quality of care for people with COPD (both diagnosed and undiagnosed). People with modifiable disease and higher risk of exacerbations, morbidity and mortality, are individuals for whom there is an opportunity to optimize management. The QS presented in the current article represent a first step in empowering primary and secondary care providers to identify, assess, quantify risk, treat, and follow-up the millions of people living with COPD who fall into this category, and differ from previous QS in that they are internationally agreed. They are important, as better identification of those at risk of exacerbating and those requiring management optimization is needed to reduce lung function decline and disease progression and improve patient HRQoL. Phenotyping disease using clinical, CV risk and biomarker variables should facilitate the identification of treatable traits, bringing us one step closer to the practice of precision medicine and selection of targeted phenotype-specific treatments to optimize COPD outcomes. Finally, regular follow-up of COPD patients is critical to modify risks (with appropriate diagnosis and treatment), lock in behavior change(s), measure treatment successes, and encourage re-assessment of the patient (eg, identification of clinical, non-pharmacological and pharmacological interventions/issues, making adjustments to treatment when necessary). By engaging physicians and patients, and then incorporating and embedding a process of quality improvement into routine care, we aim to bring about sustained change to COPD patient care. The QS will be used as benchmark to monitor the impact of quality improvement in COPD management.
Although, many of the components of our initiative may be intuitive, data showing that it can be implemented successfully, in a way which can be scaled up globally, and improve disease outcomes is less apparent. Other initiatives to improve quality of care and guideline adherence in COPD management have shown some success.17,108–115 Specific quality improvement initiatives have included financial incentives,108 national clinical audits,17 COPD diagnosis questionnaires,109 educational programs for patients and physicians,111,114 introduction of care bundles to COPD management112 and utilization of EMR for clinical decision-making support.110 For example, introduction of a COPD flow sheet into EMR at a tertiary care clinic resulted in significant improvement of clinical assessment and use of LABA.110 Use of a web-based disease management system to provide point-of-care support and information on primary care COPD management in the USA led to a significant reduction in exacerbations and improvement in COPD control medication prescription.111 In the UK, a national clinical audit for hospitalized exacerbations of COPD found improvements in process indicators when continuous audit was combined with quality improvement support and, in particular, financial incentives.17 These studies contain elements that are similar to planned components of CONQUEST and suggest that providing information and guidance at the point-of-care can lead to closer adherence to clinical guidelines. However, overall, results have been mixed and a reduction in mortality has not yet been shown. This may have been because of the short-term nature of some of these initiatives, their tendency to focus on severe disease, and failure to fully integrate into healthcare systems. Patient-reported outcomes and information were also under-utilized and quality improvement methodologies were of mixed quality and heterogenous.116
CONQUEST overcomes many of these limitations. It promotes more proactive and hence earlier diagnosis, since undiagnosed COPD patients have an increased risk of exacerbations and pneumonia, compared to those without COPD. Targeting undiagnosed patients at risk (≥40 years old and ever smokers) including the presence of previous respiratory symptoms and exacerbations, should increase diagnostic yield, improve disease outcomes, reduce healthcare resource utilization, and help to inform national/international guidelines and policies to support earlier prevention and treatment intervention in COPD.
Limitations to CONQUEST QS implementation include the fact that global and local quality improvement protocols for implementation may need to be modified depending on the country adopting these standards. Any modifications required would be based on the various nuances of healthcare policy and differences in national recommendations and guidelines, which may impact a global delivery of the program. Moreover, variability in availability of technology and/or access to electronic record systems for patient identification (especially in lower income countries) may also impact ability to implement CONQUEST QS. As the QS will be implemented, and their impact assessed in the UK and the USA initially, we acknowledge that these countries may not be representative of the situation elsewhere. Challenges encountered in each country may be different (eg, data protection issues, completeness of EMRs and differentiation between primary and secondary care), particularly with respect to socio-economic burden of lower income countries, and also differences in access to, and availability of, pharmacological treatments. On the strengths side of the equation, CONQUEST QS have been informed by 11 key thought leaders from a variety of backgrounds, including representation from primary and specialist care, academics, patient advocacy groups and the pharmaceutical industry. The QS will help to address potential disconnects between local/national and global approaches, are consensus and evidence-based, will be reviewed and updated as new evidence emerges or whenever necessary, and will be embedded into primary and secondary care processes.
Next steps for CONQUEST include the translation of these QS into Quality Improvement Program operational protocols, which describe the core components of the program required to implement CONQUEST in a healthcare system or practice. The USA and the UK have been identified for the initial delivery of the intervention, as these countries have a well-documented burden of COPD, existing quality improvement programs, and EMR integration into healthcare systems. An Opportunity Analysis using retrospective analysis of EMRs to compare the QS with current practice in each of these countries will be undertaken to describe the opportunities for management optimization. The impact of the CONQUEST intervention on COPD outcomes (eg, rate of exacerbations and major adverse cardiac or respiratory events, COPD control, lung function, systemic corticosteroid burden) will be evaluated by a cluster randomized controlled trial (CRT) in each country (PREVAIL study).
Conclusions
The CONQUEST QS are the first step on an international journey to improve care of the COPD patient in primary and secondary care. They aim to transform the patient pathway, by identifying patients with modifiable high risk of future exacerbations, optimizing management and follow-up of patients with diagnosed COPD to reduce symptoms, exacerbations, co-morbidity, and mortality. Moving forward CONQUEST will advocate for appropriate and early treatments to slow disease progression, optimize patient outcomes including improved HRQoL, encourage follow-up with patients and HCPs utilizing shared decision-making to lock in behavior change, and generate transformational evidence to measure treatment success.
Abbreviations
ATS, American Thoracic Society; BEC, blood eosinophil count; BMI, body mass index; BODE, Body-mass index, airflow Obstruction, Dyspnea, and Exercise; CONQUEST, COllaboratioN on QUality improvement initiative for achieving Excellence STandards of COPD care; COPD, chronic obstructive pulmonary disease; CV, cardiovascular; DOSE, dyspnea, obstruction, smoking, exacerbations; ECLIPSE, Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints; EMR, electronic medical record; ETHOS, Efficacy and Safety of Triple Therapy in Obstructive Lung Disease; FEV1, forced expiratory volume in one second; GOLD, Global initiative for chronic Obstructive Lung Disease; HCP, health care providers; HRQoL, health-related quality of life; ICS, inhaled corticosteroids; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist; mMRC, modified Medical Research Council; NICE, National Institute for Health and Care Excellence; OCS, oral corticosteroids; QS, quality standards.
Acknowledgments
We thank Dr Seyi Soremekun, Jonathan Marshall, Jennie Medin and Irena Brookes-Smith for their valuable contributions to the design of the study. We would also like to acknowledge Ms Andrea Teh Xin Yi (BSc, Hons) of the Observational and Pragmatic Research Institute (OPRI), Singapore, for editorial and formatting assistance which supported the development of this publication. Professor Dave Singh is supported by the National Institute for Health Research (NIHR) Manchester Biomedical Research Centre (BRC).
Funding
CONQUEST is conducted by Optimum Patient Care Global and Observational and Pragmatic Research Institute and is co-funded by Optimum Patient Care Global and AstraZeneca.
Disclosure
Rachel Pullen and Amy Couper are employees of the Observational and Pragmatic Research Institute, which is a research collaborator of the CONQUEST initiative with Optimum Patient Care and AstraZeneca. Marc Miravitlles reports speaker fees from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, Menarini, Rovi, Bial, Sandoz, Zambon, CSL Behring, Grifols and Novartis, consulting fees from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Bial, Gebro Pharma, Kamada, CSL Behring, Laboratorios Esteve, Ferrer, Mereo Biopharma, Verona Pharma, TEVA, Spin Therapeutics, pH Pharma, Novartis, Sanofi and Grifols and research grants from GlaxoSmithKline and Grifols. Anita Sharma is a practising Primary Care Physician and Senior Lecturer, School of Clinical Medicine-Primary Care Clinical Unit, University of Queensland. She supervises clinical training of primary care doctors and serves on advisory boards for Diabetes, Heart Failure and Osteoporosis for Novartis, Merck Sharp & Dohme and Boehringer Ingelheim, Eli Lilley and Amgen. Dave Singh has received personal fees from Aerogen, AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, CSL Behring, Epiendo, Glenmark, Gossamerbio, Kinaset, Menarini, Novartis, PulmatrixSanofi, Theravance and Verona. Fernando Martinez has received personal fees and non-financial support from the American College of Chest Physicians, AstraZeneca, Boehringer Ingelheim, ConCert, Genentech, GSK, Inova Fairfax Health System, Miller Communications, National Society for Continuing Education, Novartis, Pearl Pharmaceuticals, PeerView Communications, Prime Communications, Puerto Rico Respiratory Society, Chiesi, Sunovion, Theravance, Potomac, University of Alabama Birmingham, Physicians Education Resource, Canadian Respiratory Network, Teva and Dartmouth; non-financial support from ProterrixBio, Gilead, Nitto and Zambon; and personal fees from Columbia University, Integritas, MD magazine, Methodist Hospital Brooklyn, New York University, UpToDate, WebMD/MedScape, Western Connecticut Health Network, Patara/Respivant, PlatformIQ, American Thoracic Society, Rockpointe, Rare Disease Healthcare Communications and France Foundation; grant support from NIH; and is a member of steering committees for Afferent/Merck, Biogen, Veracyte, Prometic, Bayer, Bridge Biotherapeutics and ProMedior. John Hurst has received personal payment and payment to his institution (UCL), including research grants, reimbursement for advisory work and educational activities, and support to attend meetings from pharmaceutical companies that make medicines to treat COPD, which includes AstraZeneca, Boehringer Ingelheim, Chiesi and Novartis. ; Luís Alves has served as an advisor or consultant for AstraZeneca, GlaxoSmithKline; served as a speaker or a member of a speakers bureau for Astra-Zeneca, BIAL, GlaxoSmithKline, and Novartis Pharmaceuticals Corporation. Luis Alves also reports personal fees from Optimum Patient Care Global Limited, during the conduct of the study. He is also a member of the Education Subcommittee of the International Primary Care Respiratory Group and a member of the of GRESP, the Portuguese Primary Care Study Group for Respiratory Diseases. Mark Dransfield has received grant support from the Department of Defense and NIH; personal fees from AstraZeneca, Boehringer Ingelheim, PneumRx/BTG, Genentech, BostonScientific, Quark Pharmaceuticals, Teva, and GSK; and contracted clinical trial support from Boehringer Ingelheim, Novartis, AstraZeneca, Yungjin, PneumRx/BTG, Pulmonx, Boston Scientific and GSK. Rongchang Chen has received grant support from AstraZeneca, Boehringer Ingelheim, and GSK; and reimbursement for advisory work and educational activities from AstraZeneca, Boehringer Ingelheim, GSK, Novartis. Shigeo Muro reported lecture and advisory fees from Novartis Pharma and AstraZeneca; lecture fees and grants from Boehringer Ingelheim and Fukuda Life Tech; advisory fees from GlaxoSmithKline; grants from Eisai Pharmaceutical, Otsuka Pharmaceutical and Fuji Film Medical; and lecture fees from Astellas Pharmaceutical, Kyorin Pharmaceutical and Meiji Seika Pharma. Tonya Winders has received personal fees from AstraZeneca, GSK, Novartis, Genentech, and Sanofi/Regeneron alliance. Allergy & Asthma Network & Global Allergy & Airways Patient Platform has received funds for unbranded disease awareness and education from AZ, BI, GSK, Novartis, Genentech, Viatris and Sanofi/Regeneron. Christopher Blango was an employee of AstraZeneca and hold stock and/or stock options in the company. Currently employed at the Janssen Pharmaceutical Companies of J&J. Hana Müllerová, Tamsin Morris, Frank Trudo and Paul Dorinsky are employees of AstraZeneca and hold stock and/or stock options in the company. AstraZeneca is a co-funder of the CONQUEST initiative. Marianna Alacqua was an employee of AstraZeneca at the time of manuscript development. Currently employed at CSL Behring SpA. Victoria Carter is an employee of Optimum Patient Care, a co-funder of the CONQUEST initiative. Rupert Jones declares grants from Astra Zeneca, Glaxo Smith Kline, Novartis and Teva and personal fees for consultancy, speakers fees or travel support from Astra Zeneca, Boehringer Ingelheim, Glaxo Smith Kline, Novartis and OPRI. Konstantinos Kostikas was an employee and shareholder of Novartis Pharma AG until 31.10.2018. He has received honoraria for presentations and consultancy fees from AstraZeneca, Boehringer Ingelheim, Chiesi, ELPEN, GSK, Menarini, Novartis and Sanofi. His department has received funding and grants from AstraZeneca, Boehringer Ingelheim, Chiesi, Innovis, ELPEN, GSK, Menarini, Novartis and NuvoAir. He is a member of the GOLD Assembly. Ruth Murray reports personal fees from OPC, during the conduct of the study. David B Price has board membership with AstraZeneca, Boehringer Ingelheim, Chiesi, Mylan, Novartis, Regeneron Pharmaceuticals, Sanofi Genzyme, Thermofisher; consultancy agreements with Airway Vista Secretariat, AstraZeneca, Boehringer Ingelheim, Chiesi, EPG Communication Holdings Ltd, FIECON Ltd, Fieldwork International, GlaxoSmithKline, Mylan, Mundipharma, Novartis, OM Pharma SA, PeerVoice, Phadia AB, Spirosure Inc, Strategic North Limited, Synapse Research Management Partners S.L., Talos Health Solutions, Theravance and WebMD Global LLC; grants and unrestricted funding for investigator-initiated studies (conducted through Observational and Pragmatic Research Institute Pte Ltd) from AstraZeneca, Boehringer Ingelheim, Chiesi, Mylan, Novartis, Regeneron Pharmaceuticals, Respiratory Effectiveness Group, Sanofi Genzyme, Theravance and UK National Health Service; payment for lectures/speaking engagements from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, GlaxoSmithKline, Kyorin, Mylan, Mundipharma, Novartis, Regeneron Pharmaceuticals and Sanofi Genzyme; payment for travel/accommodation/meeting expenses from AstraZeneca, Boehringer Ingelheim, Mundipharma, Mylan, Novartis, Thermofisher; stock/stock options from AKL Research and Development Ltd which produces phytopharmaceuticals; owns 74% of the social enterprise Optimum Patient Care Ltd (Australia and UK) and 92.61% of Observational and Pragmatic Research Institute Pte Ltd (Singapore); 5% shareholding in Timestamp which develops adherence monitoring technology; is peer reviewer for grant committees of the UK Efficacy and Mechanism Evaluation programme, and Health Technology Assessment; and was an expert witness for GlaxoSmithKline. The authors report no other conflicts of interest in this work.
References
1. Criner RN, Han MK. COPD: care in the 21st century: a public health priority. Respir Care. 2018;63(5):591–600. doi:10.4187/respcare.06276
2. World Health Organization: the top 10 causes of death. Available from: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
3. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease; 2021. Available from:https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf.
4. Diab N, Gershon AS, Sin DD, et al. Underdiagnosis and overdiagnosis of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(9):1130–1139. doi:10.1164/rccm.201804-0621CI
5. Morgan AD, Zakeri R, Quint JK. Defining the relationship between COPD and CVD: what are the implications for clinical practice? Ther Adv Respir Dis. 2018;12:1753465817750524. doi:10.1177/1753465817750524
6. Zafari Z, Li S, Eakin MN, Bellanger M, Reed RM. Projecting long-term health and economic burden of chronic obstructive pulmonary disease in the United States. Chest. 2020;159(4):1400–1410. doi:10.1016/j.chest.2020.09.255
7. Punekar YS, Shukla A, Müllerova H. COPD management costs according to the frequency of COPD exacerbations in UK primary care. Int J Chron Obstruct Pulmon Dis. 2014;9:65–73. doi:10.2147/COPD.S54417
8. Jones RCM, Price D, Ryan D, et al. Opportunities to diagnose chronic obstructive pulmonary disease in routine care in the UK: a retrospective study of a clinical cohort. Lancet Respir Med. 2014;2(4):267–276. doi:10.1016/S2213-2600(14)70008-6
9. Halpin DMG, de Jong HJI, Carter V, Skinner D, Price D. Distribution, temporal stability and appropriateness of therapy of patients with COPD in the UK in relation to GOLD 2019. EClinicalMedicine. 2019;14:32–41. doi:10.1016/j.eclinm.2019.07.003
10. McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015;(2):CD003793. doi:10.1002/14651858.CD003793.pub3
11. Puhan MA, Gimeno-Santos E, Scharplatz M, Troosters T, Walters EH, Steurer J. Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2011;(10):CD005305. doi:10.1002/14651858.CD005305.pub3
12. Kerkhof M, Voorham J, Dorinsky P, et al. Association between COPD exacerbations and lung function decline during maintenance therapy. Thorax. 2020;75(9):744–753. doi:10.1136/thoraxjnl-2019-214457
13. Kerkhof M, Voorham J, Dorinsky P, et al. The long-term burden of copd exacerbations during maintenance therapy and lung function decline. Int J Chron Obstruct Pulmon Dis. 2020;15:1909–1918. doi:10.2147/COPD.S253812
14. COPD National Action Plan. COPD.NIH.Gov; 2017. Available from: https://www.nhlbi.nih.gov/sites/default/files/media/docs/COPD%20National%20Action%20Plan%20508_0.pdf.
15. Rightcare pathway: COPD. NHS RightCare; 2017. Available from: https://www.england.nhs.uk/rightcare/wp-content/uploads/sites/40/2017/12/nhs-rightcare-copd-pathway-v18.pdf.
16. Stockley RA. COPD service delivery in the UK. Lancet Respir Med. 2016;4(6):426–428. doi:10.1016/S2213-2600(16)30082-0
17. Hurst JR, Quint JK, Stone RA, Silove Y, Youde J, Roberts CM. National clinical audit for hospitalised exacerbations of COPD. ERJ Open Res. 2020;6:3. doi:10.1183/23120541.00208-2020
18. Department of Health. An outcomes strategy for chronic obstructive pulmonary disease (COPD) and asthma. NHS companion document; 2012. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/216531/dh_134001.pdf.
19. Press Release: optimum Patient Care Collaborates with AstraZeneca to Launch a Quality Improvement Initiative for Achieving Excellence in Standards of COPD Care; 2020. Available from: https://optimumpatientcare.org/news/conquest/.
20. National Institute for Health and Care Excellence. Chronic obstructive pulmonary disease in over 16s: diagnosis and management; 2019. Available from: www.nice.org.uk/guidance/ng115.
21. Qaseem A, Wilt TJ, Weinberger SE, et al. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann Intern Med. 2011;155(3):179–191. doi:10.7326/0003-4819-155-3-201108020-00008
22. Nici L, Mammen MJ, Charbek E, et al. Pharmacologic Management of Chronic Obstructive Pulmonary Disease. An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2020;201(9):e56–e69. doi:10.1164/rccm.202003-0625ST
23. Kostikas K, Price D, Gutzwiller FS, et al. Clinical impact and healthcare resource utilization associated with early versus late COPD diagnosis in patients from UK CPRD database. Int J Chron Obstruct Pulmon Dis. 2020;15:1729–1738. doi:10.2147/COPD.S255414
24. Çolak Y, Afzal S, Nordestgaard BG, Vestbo J, Lange P. Prognosis of asymptomatic and symptomatic, undiagnosed COPD in the general population in Denmark: a prospective cohort study. Lancet Respir Med. 2017;5(5):426–434. doi:10.1016/S2213-2600(17)30119-4
25. Tinkelman DG, Price D, Nordyke RJ, Halbert RJ. COPD screening efforts in primary care: what is the yield? Prim Care Respir J. 2007;16(1):41–48. doi:10.3132/pcrj.2007.00009
26. Jordan RE, Adab P, Sitch A, et al. Targeted case finding for chronic obstructive pulmonary disease versus routine practice in primary care (TargetCOPD): a cluster-randomised controlled trial. Lancet Respir Med. 2016;4(9):720–730. doi:10.1016/S2213-2600(16)30149-7
27. Make B, Dutro MP, Paulose-Ram R, Marton JP, Mapel DW. Undertreatment of COPD: a retrospective analysis of US managed care and Medicare patients. Int J Chron Obstruct Pulmon Dis. 2012;7:1–9. doi:10.2147/COPD.S27032
28. Price D, West D, Brusselle G, et al. Management of COPD in the UK primary-care setting: an analysis of real-life prescribing patterns. Int J Chron Obstruct Pulmon Dis. 2014;9:889–904. doi:10.2147/COPD.S62750
29. Yip NH, Yuen G, Lazar EJ, et al. Analysis of hospitalizations for COPD exacerbation: opportunities for improving care. COPD. 2010;7(2):85–92. doi:10.3109/15412551003631683
30. Le Rouzic O, Roche N, Cortot AB, et al. Defining the “frequent exacerbator” phenotype in copd: a hypothesis-free approach. Chest. 2018;153(5):1106–1115. doi:10.1016/j.chest.2017.10.009
31. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
32. Halpin DMG, Decramer M, Celli BR, Mueller A, Metzdorf N, Tashkin DP. Effect of a single exacerbation on decline in lung function in COPD. Respir Med. 2017;128:85–91. doi:10.1016/j.rmed.2017.04.013
33. Crisan L, Wong N, Sin DD, Lee HM. Karma of cardiovascular disease risk factors for prevention and management of major cardiovascular events in the context of acute exacerbations of chronic obstructive pulmonary disease. Front Cardiovasc Med. 2019;6:79. doi:10.3389/fcvm.2019.00079
34. Halpin DMG, Decramer M, Celli B, Kesten S, Leimer I, Tashkin DP. Risk of nonlower respiratory serious adverse events following COPD exacerbations in the 4-year UPLIFT® trial. Lung. 2011;189(4):261–268. doi:10.1007/s00408-011-9301-8
35. Rothnie KJ, Smeeth L, Herrett E, et al. Closing the mortality gap after a myocardial infarction in people with and without chronic obstructive pulmonary disease. Heart. 2015;101(14):1103–1110. doi:10.1136/heartjnl-2014-307251
36. Kunisaki KM, Dransfield MT, Anderson JA, et al. Exacerbations of chronic obstructive pulmonary disease and cardiac events. a post hoc cohort analysis from the SUMMIT randomized clinical trial. Am J Respir Crit Care Med. 2018;198(1):51–57. doi:10.1164/rccm.201711-2239OC
37. Anzueto A, Leimer I, Kesten S. Impact of frequency of COPD exacerbations on pulmonary function, health status and clinical outcomes. Int J Chron Obstruct Pulmon Dis. 2009;4:245–251. doi:10.2147/copd.s4862
38. Seemungal TA, Donaldson GC, Paul EA, Bestall JC, Jeffries DJ, Wedzicha JA. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157(5 Pt 1):1418–1422. doi:10.1164/ajrccm.157.5.9709032
39. Celli BR, Cote CG, Marin JM, et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(10):1005–1012. doi:10.1056/NEJMoa021322
40. Chen X, Wang Q, Hu Y, et al. A nomogram for predicting severe exacerbations in stable COPD patients. Int J Chron Obstruct Pulmon Dis. 2020;15:379–388. doi:10.2147/COPD.S234241
41. Prudente R, Franco EAT, Mesquita CB, Ferrari R, de Godoy I, Tanni SE. Predictors of mortality in patients with COPD after 9 years. Int J Chron Obstruct Pulmon Dis. 2018;13:3389–3398. doi:10.2147/COPD.S174665
42. Crim C, Calverley PMA, Anderson JA, et al. Pneumonia risk with inhaled fluticasone furoate and vilanterol in COPD patients with moderate airflow limitation: the SUMMIT trial. Respir Med. 2017;131:27–34. doi:10.1016/j.rmed.2017.07.060
43. Boles A, Kandimalla R, Reddy PH. Dynamics of diabetes and obesity: epidemiological perspective. Biochim Biophys Acta Mol Basis Dis. 2017;1863(5):1026–1036. doi:10.1016/j.bbadis.2017.01.016
44. Pascoe S, Locantore N, Dransfield MT, Barnes NC, Pavord ID. Blood eosinophil counts, exacerbations, and response to the addition of inhaled fluticasone furoate to vilanterol in patients with chronic obstructive pulmonary disease: a secondary analysis of data from two parallel randomised controlled trials. Lancet Respir Med. 2015;3(6):435–442. doi:10.1016/S2213-2600(15)00106-X
45. Bafadhel M, Peterson S, De Blas MA, et al. Predictors of exacerbation risk and response to budesonide in patients with chronic obstructive pulmonary disease: a post-hoc analysis of three randomised trials. Lancet Respir Med. 2018;6(2):117–126. doi:10.1016/S2213-2600(18)30006-7
46. Cazzola M, Rogliani P, Calzetta L, Matera MG. Triple therapy versus single and dual long-acting bronchodilator therapy in COPD: a systematic review and meta-analysis. Eur Respir J. 2018;52:6. doi:10.1183/13993003.01586-2018
47. Rabe KF, Martinez FJ, Ferguson GT, et al. Triple Inhaled Therapy at Two Glucocorticoid Doses in Moderate-to-Very-Severe COPD. N Engl J Med. 2020;383(1):35–48. doi:10.1056/NEJMoa1916046
48. Pascoe S, Barnes N, Brusselle G, et al. Blood eosinophils and treatment response with triple and dual combination therapy in chronic obstructive pulmonary disease: analysis of the IMPACT trial. Lancet Respir Med. 2019;7(9):745–756. doi:10.1016/S2213-2600(19)30190-0
49. Bafadhel M, Pavord ID, Russell REK. Eosinophils in COPD: just another biomarker? Lancet Respir Med. 2017;5(9):747–759. doi:10.1016/S2213-2600(17)30217-5
50. Voorham J, Corradi M, Papi A, et al. Comparative effectiveness of triple therapy versus dual bronchodilation in COPD. ERJ Open Res. 2019;5(3):00106–02019. doi:10.1183/23120541.00106-2019
51. Kerkhof M, Chaudhry I, Kocks J, et al. Eosinophil counts as a biomarker of oral corticosteroid treatment success for patients with COPD. Am Thoracic Soc. 2019;17–22.
52. Sivapalan P, Lapperre TS, Janner J, et al. Eosinophil-guided corticosteroid therapy in patients admitted to hospital with COPD exacerbation (CORTICO-COP): a multicentre, randomised, controlled, open-label, non-inferiority trial. Lancet Respir Med. 2019;7(8):699–709. doi:10.1016/S2213-2600(19)30176-6
53. Gonçalves I, Guimarães MJ, van Zeller M, Menezes F, Moita J, Simão P. Clinical and molecular markers in COPD. Pulmonology. 2018;24(4):250–259. doi:10.1016/j.pulmoe.2018.02.005
54. Lowe KE, Regan EA, Anzueto A, et al. COPDGene® 2019: redefining the Diagnosis of Chronic Obstructive Pulmonary Disease. Chronic Obstr Pulm Dis. 2019;6(5):384–399. doi:10.15326/jcopdf.6.5.2019.0149
55. Zulueta JJ, Wisnivesky JP, Henschke CI, et al. Emphysema scores predict death from COPD and lung cancer. Chest. 2012;141(5):1216–1223. doi:10.1378/chest.11-0101
56. Divo M, Cote C, de Torres JP, et al. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(2):155–161. doi:10.1164/rccm.201201-0034OC
57. Chen W, Thomas J, Sadatsafavi M, FitzGerald JM. Risk of cardiovascular comorbidity in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. Lancet Respir Med. 2015;3(8):631–639. doi:10.1016/S2213-2600(15)00241-6
58. André S, Conde B, Fragoso E, Boléo-Tomé JP, Areias V, Cardoso J. COPD and Cardiovascular Disease. Pulmonology. 2019;25(3):168–176. doi:10.1016/j.pulmoe.2018.09.006
59. Agusti A, Calverley PMA, Celli B, et al. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir Res. 2010;11(1):122. doi:10.1186/1465-9921-11-122
60. Hillas G, Perlikos F, Tsiligianni I, Tzanakis N. Managing comorbidities in COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:95–109. doi:10.2147/COPD.S54473
61. Marin JM, Cote CG, Diaz O, et al. Prognostic assessment in COPD: health related quality of life and the BODE index. Respir Med. 2011;105(6):916–921. doi:10.1016/j.rmed.2011.01.007
62. Rolink M, van Dijk W, van den Haak-rongen S, Pieters W, Schermer T, van den Bemt L. Using the DOSE index to predict changes in health status of patients with COPD: a prospective cohort study. Prim Care Respir J. 2013;22(2):169–174. doi:10.4104/pcrj.2013.00033
63. Jones RC, Price D, Chavannes NH, et al. Multi-component assessment of chronic obstructive pulmonary disease: an evaluation of the ADO and DOSE indices and the global obstructive lung disease categories in international primary care data sets. NPJ Prim Care Respir Med. 2016;26:16010. doi:10.1038/npjpcrm.2016.10
64. Bui DS, Lodge CJ, Burgess JA, et al. Childhood predictors of lung function trajectories and future COPD risk: a prospective cohort study from the first to the sixth decade of life. Lancet Respir Med. 2018;6(7):535–544. doi:10.1016/S2213-2600(18)30100-0
65. Li LSK, Paquet C, Johnston K, Williams MT. “What are my chances of developing COPD if one of my parents has the disease?” A systematic review and meta-analysis of prevalence of co-occurrence of COPD diagnosis in parents and offspring. Int J Chron Obstruct Pulmon Dis. 2017;12:403–415. doi:10.2147/COPD.S123933
66. He T, Oks M, Esposito M, Steinberg H, Makaryus M. “Tree-in-bloom”: severe acute lung injury induced by vaping cannabis oil. Ann Am Thorac Soc. 2017;14(3):468–470. doi:10.1513/AnnalsATS.201612-974LE
67. Henry TS, Kanne JP, Kligerman SJ. Imaging of vaping-associated lung disease. N Engl J Med. 2019;381(15):1486–1487. doi:10.1056/NEJMc1911995
68. Welte T, Vogelmeier C, Papi A. COPD: early diagnosis and treatment to slow disease progression. Int J Clin Pract. 2015;69(3):336–349. doi:10.1111/ijcp.12522
69. Kanner RE, Connett JE, Williams DE, Buist AS. Effects of randomized assignment to a smoking cessation intervention and changes in smoking habits on respiratory symptoms in smokers with early chronic obstructive pulmonary disease: the Lung Health Study. Am J Med. 1999;106(4):410–416. doi:10.1016/s0002-9343(99)00056-x
70. Spruit MA, Singh SJ, Garvey C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–64. doi:10.1164/rccm.201309-1634ST
71. Criner GJ, Dreher M, Hart N, Murphy P. COPD home oxygen therapy and home mechanical ventilation: improving admission-free survival in persistent hypercapnic COPD. Chest. 2018;153(6):1499–1500. doi:10.1016/j.chest.2018.03.053
72. Nichol KL, Margolis KL, Wuorenma J, Von Sternberg T. The efficacy and cost effectiveness of vaccination against influenza among elderly persons living in the community. N Engl J Med. 1994;331(12):778–784. doi:10.1056/NEJM199409223311206
73. Wongsurakiat P, Maranetra KN, Wasi C, Kositanont U, Dejsomritrutai W, Charoenratanakul S. Acute respiratory illness in patients with COPD and the effectiveness of influenza vaccination: a randomized controlled study. Chest. 2004;125(6):2011–2020. doi:10.1378/chest.125.6.2011
74. Kopsaftis Z, Wood-Baker R, Poole P. Influenza vaccine for chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2018;6(6):CD002733. doi:10.1002/14651858.CD002733.pub3
75. Froes F, Roche N, Blasi F. Pneumococcal vaccination and chronic respiratory diseases. Int J Chron Obstruct Pulmon Dis. 2017;12:3457–3468. doi:10.2147/COPD.S140378
76. Blasi F, Bonanni P, Braido F, Gabutti G, Marchetti F, Centanni S. The unmet need for pertussis prevention in patients with chronic obstructive pulmonary disease in the Italian context. Hum Vaccin Immunother. 2020;16(2):340–348. doi:10.1080/21645515.2019.1652517
77. Granados-Santiago M, Valenza MC, López-López L, Prados-Román E, Rodríguez-Torres J, Cabrera-Martos I. Shared decision-making and patient engagement program during acute exacerbation of COPD hospitalization: a randomized control trial. Patient Educ Couns. 2020;103(4):702–708. doi:10.1016/j.pec.2019.12.004
78. Chalmers JD, Laska IF, Franssen FME, et al. Withdrawal of inhaled corticosteroids in COPD: a European Respiratory Society guideline. Eur Respir J. 2020;55:6. doi:10.1183/13993003.00351-2020
79. Price D, Østrem A, Thomas M, Welte T. Dual bronchodilation in COPD: lung function and patient-reported outcomes - a review. Int J Chron Obstruct Pulmon Dis. 2017;12:141–168. doi:10.2147/COPD.S116719
80. Papi A, Vestbo J, Fabbri L, et al. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary disease (TRIBUTE): a double-blind, parallel group, randomised controlled trial. Lancet. 2018;391(10125):1076–1084. doi:10.1016/S0140-6736(18)30206-X
81. Chapman KR, Hurst JR, Frent S-M, et al. Long-term triple therapy de-escalation to indacaterol/glycopyrronium in patients with chronic obstructive pulmonary disease (SUNSET): a randomized, double-blind, triple-dummy clinical trial. Am J Respir Crit Care Med. 2018;198(3):329–339. doi:10.1164/rccm.201803-0405OC
82. Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378(18):1671–1680. doi:10.1056/NEJMoa1713901
83. Martinez FJ, Rabe KF, Ferguson GT, et al. Reduced all-cause mortality in the ETHOS trial of budesonide/glycopyrrolate/formoterol for COPD: a randomized, double-blind, multi-center parallel-group study. Am J Respir Crit Care Med. 2020. doi:10.1164/rccm.202006-2618OC
84. Calverley PMA, Jones PW. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. n Engl j Med. 2007;15.
85. Tashkin DP, Miravitlles M, Celli BR, et al. Concomitant inhaled corticosteroid use and the risk of pneumonia in COPD: a matched-subgroup post hoc analysis of the UPLIFT® trial. Respir Res. 2018;19(1):196. doi:10.1186/s12931-018-0874-0
86. Suissa S. Number needed to treat in COPD: exacerbations versus pneumonias. Thorax. 2013;68(6):540–543. doi:10.1136/thoraxjnl-2012-202709
87. Rabe KF, Martinez FJ, Ferguson GT, et al. COPD exacerbation benefits relative to pneumonia risk with budesonide/glycopyrronium/formoterol metered dose inhaler: analysis from ETHOS. Eur Respir J. 2020;56(Suppl 64):5230.
88. Lipworth B, Skinner D, Devereux G, et al. Underuse of β-blockers in heart failure and chronic obstructive pulmonary disease. Heart. 2016;102(23):1909–1914. doi:10.1136/heartjnl-2016-309458
89. Salpeter S, Ormiston T, Salpeter E. Cardioselective beta-blockers for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2005;(4):CD003566. doi:10.1002/14651858.CD003566.pub2
90. Rogliani P, Calzetta L, Coppola A, et al. Optimizing drug delivery in COPD: the role of inhaler devices. Respir Med. 2017;124:6–14. doi:10.1016/j.rmed.2017.01.006
91. Price D, Keininger DL, Viswanad B, Gasser M, Walda S, Gutzwiller FS. Factors associated with appropriate inhaler use in patients with COPD - lessons from the REAL survey. Int J Chron Obstruct Pulmon Dis. 2018;13:695–702. doi:10.2147/COPD.S149404
92. Walters JAE, Tan DJ, White CJ, Gibson PG, Wood-Baker R, Walters EH. Systemic corticosteroids for acute exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014;(9):CD001288. doi:10.1002/14651858.CD001288.pub4
93. Walters JA, Tan DJ, White CJ, Wood-Baker R. Different durations of corticosteroid therapy for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2018;3(3):CD006897. doi:10.1002/14651858.CD006897.pub4
94. Soler-Cataluña JJ, Marzo M, Catalán P, Miralles C, Alcazar B, Miravitlles M. Validation of clinical control in COPD as a new tool for optimizing treatment. Int J Chron Obstruct Pulmon Dis. 2018;13:3719–3731. doi:10.2147/COPD.S178149
95. Miravitlles M, Sliwinski P, Rhee CK, et al. Changes in control status of COPD over time and their consequences: a prospective international study. Arch Bronconeumol. 2021;57(2):122–129. doi:10.1016/j.arbres.2020.06.003
96. Kocks JWH, Chrystyn H, van der Palen J, et al. Systematic review of association between critical errors in inhalation and health outcomes in asthma and COPD. NPJ Prim Care Respir Med. 2018;28(1):43. doi:10.1038/s41533-018-0110-x
97. Dudvarski Ilic A, Zugic V, Zvezdin B, et al. Influence of inhaler technique on asthma and COPD control: a multicenter experience. Int J Chron Obstruct Pulmon Dis. 2016;11:2509–2517. doi:10.2147/COPD.S114576
98. van Eerd EAM, van der Meer RM, van Schayck OCP, Kotz D. Smoking cessation for people with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2016;1(8):CD010744. doi:10.1002/14651858.CD010744.pub2
99. Garvey C, Bayles MP, Hamm LF, et al. Pulmonary rehabilitation exercise prescription in chronic obstructive pulmonary disease: review of selected guidelines: an official statement from the American Association of Cardiovascular and Pulmonary Rehabilitation. J Cardiopulm Rehabil Prev. 2016;36(2):75–83. doi:10.1097/HCR.0000000000000171
100. Yawn BP, Wollan PC, Textor KB, Yawn RA. Primary care physicians’, nurse practitioners’ and physician assistants’ knowledge, attitudes and beliefs regarding COPD: 2007 To 2014. Chronic Obstr Pulm Dis. 2016;3(3):628–635. doi:10.15326/jcopdf.3.3.2015.0168
101. Strang S, Farrell M, Larsson L-O, et al. Experience of guilt and strategies for coping with guilt in patients with severe COPD: a qualitative interview study. J Palliat Care. 2014;30(2):108–115. doi:10.1177/082585971403000206
102. Lundell S, Wadell K, Wiklund M, Tistad M. Enhancing confidence and coping with stigma in an ambiguous interaction with primary care: a qualitative study of people with COPD. COPD. 2020;17(5):533–542. doi:10.1080/15412555.2020.1824217
103. Jönsson A, Fedorowski A, Engström G, Wollmer P, Hamrefors V. High prevalence of undiagnosed COPD among patients evaluated for suspected myocardial ischaemia. Open Heart. 2018;5(2):e000848. doi:10.1136/openhrt-2018-000848
104. Goldman RE, Mennillo L, Stebbins P, Parker DR. How do patients conceptualize chronic obstructive pulmonary disease? Chron Respir Dis. 2017;14(3):245–255. doi:10.1177/1479972316680845
105. Albarrati AM, Gale NS, Munnery MM, Cockcroft JR, Shale DJ. Daily physical activity and related risk factors in COPD. BMC Pulm Med. 2020;20(1):60. doi:10.1186/s12890-020-1097-y
106. Watz H, Pitta F, Rochester CL, et al. An official European Respiratory Society statement on physical activity in COPD. Eur Respir J. 2014;44(6):1521–1537. doi:10.1183/09031936.00046814
107. Garcia-Aymerich J, Lange P, Benet M, Schnohr P, Antó JM. Regular physical activity reduces hospital admission and mortality in chronic obstructive pulmonary disease: a population based cohort study. Thorax. 2006;61(9):772–778. doi:10.1136/thx.2006.060145
108. Falzon C, Elkin SL, Kelly JL, Lynch F, Blake ID, Hopkinson NS. Can financial incentives for improvements in healthcare quality enhance identification of COPD in primary care? Thorax. 2011;66(7):630. doi:10.1136/thx.2010.140913
109. Martinez FJ, Mannino D, Leidy NK, et al. A new approach for identifying patients with undiagnosed chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;195(6):748–756. doi:10.1164/rccm.201603-0622OC
110. Terasaki J, Singh G, Zhang W, Wagner P, Sharma G. Using EMR to improve compliance with clinical practice guidelines for management of stable COPD. Respir Med. 2015;109(11):1423–1429. doi:10.1016/j.rmed.2015.10.003
111. Morganroth M, Pape G, Rozenfeld Y, Heffner JE. Multidisciplinary COPD disease management program: impact on clinical outcomes. Postgrad Med. 2016;128(2):239–249. doi:10.1080/00325481.2016.1129259
112. Markun S, Rosemann T, Dalla-Lana K, Steurer-Stey C. Care in Chronic Obstructive Lung Disease (CAROL): a randomised trial in general practice. Eur Respir J. 2018;51:5. doi:10.1183/13993003.01873-2017
113. Shah SA, Velardo C, Farmer A, Tarassenko L. Exacerbations in chronic obstructive pulmonary disease: identification and prediction using a digital health system. J Med Internet Res. 2017;19(3):e69. doi:10.2196/jmir.7207
114. Farmer A, Williams V, Velardo C, et al. Self-management support using a digital health system compared with usual care for chronic obstructive pulmonary disease: randomized controlled trial. J Med Internet Res. 2017;19(5):e144. doi:10.2196/jmir.7116
115. Royal College of Physicians. National Asthma and Chronic Obstructive Pulmonary Disease Audit Programme (NACAP). Wales primary care clinical audit 2017/18; 2020. Available from: https://www.hqip.org.uk/wp-content/uploads/2020/03/Ref-179-Primary-Care-Report-National-Report-Wales-Only-FINAL.pdf.
116. Kruis AL, Smidt N, Assendelft WJJ, et al. Integrated disease management interventions for patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2013;10:CD009437. doi:10.1002/14651858.CD009437.pub2
117. Wedzicha JA, Miravitlles M, Hurst JR, et al. Management of COPD exacerbations: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2017;49:3. doi:10.1183/13993003.00791-2016
118. NICE/BNF. British National Formulary: glucocorticoid therapy. Available from: https://bnf.nice.org.uk/treatment-summary/glucocorticoid-therapy.html.
119. USPNF. United States Pharmacopeia (USP) and the National Formulary (NF). Available from: https://www.uspnf.com/purchase-usp-nf.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.