")
Back to Journals » Clinical Ophthalmology » Volume 16
Compliance of Soft Contact Lens Care and Bacterial Contamination Among University Students in Palestine
Authors Beshtawi IM , Qaddumi J, Suboh N , Zaid A, Mansour H , Zeyadeh T
Received 4 December 2021
Accepted for publication 14 March 2022
Published 13 December 2022 Volume 2022:16 Pages 4121—4134
DOI https://doi.org/10.2147/OPTH.S352209
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Ithar M Beshtawi,1 Jamal Qaddumi,2 Nabeela Suboh,1 Aesha Zaid,3 Hiba Mansour,1 Thana Zeyadeh3
1Optometry Department, Faculty of Medicine and Health Sciences, An-Najah National University, Nablus, West Bank, State of Palestine; 2Nursing Department, Faculty of Medicine and Health Sciences, An-Najah National University, Nablus, West Bank, State of Palestine; 3Medicine Department, Faculty of Medicine and Health Sciences, An-Najah National University, Nablus, West Bank, State of Palestine
Correspondence: Ithar M Beshtawi, Optometry and Nursing Building, New Campus, An-Najah National University, P.O. Box 7, Al-Juneid Street, Nablus, West Bank, State of Palestine, Tel +972 92345116 ext. 2155 ; +972 592586273, Fax +970 92345982, Email [email protected]
Purpose: This study investigated the contact lens care compliance, noncompliance reasons, bacterial contamination rate, and the behaviors associated with contamination among university students in Palestine.
Patients and Methods: 133 Habitual soft contact lens wearers were recruited in this study and interviewed using a face-to-face questionnaire, to obtain data on demographics, contact lenses, modifiable lens care behaviors and the reasons for non-compliance. High, moderate, and low lens care behaviors were identified. Additionally, a sample of the participant’s storage cases was collected for bacterial contamination testing.
Results: The participants’ mean age was 22.4± 4.4, with female predominance (62.4%). The average compliance rate was 76.8%. Total CL care compliance (100%) was found in filling the case with adequate solution, not sharing the lenses or storage case with others, while the poorest compliance (> 40%) was found in attending after-care visits, checking the solution’s expiry, and re-disinfecting the lenses with a fresh solution before insertion after prolonged storage. Poor understanding of the instructions contributed significantly to a low level of compliance (P≤ 0.05). Gram-positive and gram-negative bacteria were detected in 19.55% of the participants’ cases. Poor hand and case hygiene, no replacement of lens cases (monthly), and water exposure were linked to bacterial contamination of storage cases.
Conclusion: This study indicated moderate to high compliance in CL care, averaging 76.8%. Poor compliance was found in attending after-care visits, checking the solution’s expiry, and re-disinfecting the lenses with a fresh solution after an extended storage interval. 19.55% of the cases had bacterial contamination, with Staphylococcus Aureus being the most common. Poor hand and lens case hygiene and water exposure are found to be associated with lens case contamination. These findings emphasize the importance of patient education on safer lens wear modalities, proper wearing schedules, and hygiene regimens to reduce the risks of developing contact lens complications.
Keywords: modifiable-behaviors, hygiene, microbiology, risk factors, attitude
Introduction
Compliance in the contact lens (CL) field is referred to the adherence of CL care instructions provided by eye care practitioners.1 Unfortunately, compliance with recommended care strategies is generally poor. Previous research reported a low level of compliance in CL care and hygiene in both young and adult wearers1–7 even when the instructions were adequately provided along with the possible complications.8,9 Laziness, rising costs, a lack of understanding of instructions, and intermittent use of CL are all factors that may contribute to poor compliance.1,10
Non-compliance with CL and accessory care has been linked to an increased risk of contact lens-related complications and discomfort,6,11,12 which could lead to CL dropout.13 Previous research has looked at a range of CL non-compliant behaviors that contribute to corneal infection, such as poor hand hygiene and storage case hygiene,14 un-prescribed overnight wear,12,14,15 longer replacement schedules, smoking14 and contact lens exposure to water.12
Non-compliance increases the possibility of microorganisms, particularly bacteria, to adhere to hydrogel CL,1,12,16 because the bacteria has an ability to form a biofilm with strong adherence to the CL or case surfaces17 and resistance to multipurpose solutions.18,19 Some bacteria are known to cause ocular inflammation when the ocular surface is disrupted.20 For instance, CL contamination with Staphylococcus Aureus, Streptococcus Pneumonia and others are associated with CL peripheral ulcers (CLPU),21 contamination with Haemophilus Influenzae, Pseudomonas Aeruginosa, Pseudomonas Putida, Serratia Marcescens, Serratia Liquefaciens, and others are associated with CL acute red eye (CLARE)11 and Pseudomonas Aeruginosa, Serratia Marcescens and Staphylococcus Aureus are associated with microbial keratitis (MK).12,20
Therefore, given the vast number of people who wear contact lenses around the world,22 and in the Middle East,23 including in Palestine, the ocular inflammation induced by bacterial contamination of the hydrogel CL would be higher than in non-CL wearers1,12,16 due to CL care non-compliance. To date, there is no data available on the CL care compliance rate and non-compliance behaviors among SCL wearers in Palestine, as well as the non-compliance behaviors associated with bacterial contamination. Awareness and educational programs regarding the proper use and care of contact lenses are lacking in Palestine as well. Therefore, an understanding of the risks and contributory factors to contact lens non-compliance is important so eye care practitioners in Palestine can develop strategies to educate patients on safer lens wear modalities, proper wearing schedules, and hygiene regimens, which in turn could reduce the CL patients drop out in Palestine. Especially when access to medical examinations and council is temporarily suspended, as was the case during the COVID 19 pandemic, which highlighted the importance of providing patients with detailed and clear instructions.24,25
The purpose of this study, which used direct patient interviews and contact lens case cultures, was to determine, for the first time, the CL compliance rate and non-compliant behaviors among daily soft CL users in Palestine, and to investigate the participants’ thoughts on the reasons for non-compliance. It also aimed to look into non-compliant behaviors associated with bacterial contamination and underlying bacterial pathogens in contaminated storage cases. The results of this study will give valuable information to eye care professionals in Palestine on how to improve patient education and CL care compliance in order to avoid related ocular risks and infections, based on the common non-compliant behaviors of SCL wearers in Palestinian society.
Material and Methods
Participants
133 habitual soft contact lens wearers from both genders who were at least 18 years old with good general health and wearing soft lenses for refractive error correction were invited to participate in this study. Participants who were using therapeutic CL or wearing CL for less than one month were excluded. All participants were students at An-Najah National University who were approached through the university email, announcement on the university portal page and social media.
Eligible participants were asked to visit the optometry clinic at An-Najah National University (30 ± 10 min) to illustrate the nature of the study, check the eligibility of the participants based on the inclusion and exclusion criteria, answer the direct survey questions and provide a sample for bacterial culture.
Ethical Considerations
This study was conducted in compliance with the tenets of the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board (IRB) committee at An-Najah National University. The objectives, procedure and the significance of the study were explained verbally and in written format to all participants. Informed consent was obtained from all participants prior to the start of the study.
The Questionnaire
This questionnaire was designed by the study team in accordance with past research targeted at determining contact lens wearer compliance with contact lens care.1,2,4–9,26,27 The questionnaire was first administered to 15 contact lens wearers to check comprehensibility, and it was further modified according to the feedback of a group of contact lens optometrists to ensure that the questionnaire was written in a clear and understandable language. The final version of the questionnaire was used in the study, excluding the data collected from the first 15 participants.
The participants were interviewed by a trained researcher. It was composed of four main parts; the first part was demographic information (ie, age, gender, educational level, and smoking habit). The second part asked about contact lenses information (ie, power, duration of wearing CL (in months), average wearing time (hours per day), wearing modality, prescribed by whom and purchase place). The third part was about modifiable behaviors of CL care. Questions related to the care of contact lenses, care solution, storage case, lens and hand hygiene, water exposure, and aftercare visits were included. Each question was supplied with four set answers (always, frequently, occasionally, and rarely), and each answer was given a score from 1–4 where lower scores indicate high compliance and higher scores indicate low compliance. According to previous studies,5,26,27 scores 1 and 2 were considered complaints, and scores 3 and 4 were regarded as non-compliant for statistical purposes. The compliance rate will be calculated using the sum of score 1 and 2 frequencies, and the non-compliance rate will be calculated using the sum of score 3 and 4 frequencies for each CL care procedure. Frequencies greater than 80% are defined as high levels of compliance, frequencies between 40% and 80% are defined as moderate levels of compliance, and frequencies less than 40% are defined as low levels of compliance.5,26,27
The last part of the questionnaire asked about the participants’ opinions of reasons behind non-compliance. These include; complexity of procedures recommended, poor understanding of verbal and/or written instructions, poor patient-practitioner relationship, time needed to perform the prescribed tasks correctly, costs, insufficient instruction, forgetfulness, laziness, and intermittent use of CL. The participants’ response to the nine yes/no questions for reasons of non-compliance in this part were recorded.
Bacterial Assessment
A sample from the participant’s storage cases was collected to be tested against bacterial contamination. This was chosen as the storage case provides a favorable place to build up a bacterial biofilm than on the CL,17 in addition to the previously approved cross-contamination between the CL, cleaning solution and storage case.28 Therefore, a single extract from any of these sites would be sufficient to provide evidence of a positive bacterial culture.
The CL case was first emptied of any reaming solution, and one chamber was then filled with 2 mL of sterile phosphate buffered saline (PBS). The case was then capped and vortexed for 30 seconds. The PBS was transferred to a labeled bijou bottle to be used for microbiological culture within 30 min of collection. Collected samples were then cultured on blood agar, chocolate agar and nutrient agar (Oxoid Ltd, Basingstoke, UK) at 35°C for 72 hours to investigate bacterial contamination.
The number of colony types on the agar plate and the morphology of the detected colonies were noted for the samples which exhibited culture growth. A standardized biochemical test for microbiological identification was then applied using API Rapid 20E and API 20NE (bioMerieux, Marcyl’Etoile, Rhône, France).29
Statistical Analysis
The Statistical Package of Social Sciences version 20.0 (SPSS Inc., Chicago, IL, USA) was utilized for data entry and statistical analysis. Based on a medium-sized effect and an alpha level of 0.05, this study had 80% or higher power to identify CL compliance rates, common non-compliant behaviors, and cases bacterial contamination rate assuming data from 133 participants was analyzed. Descriptive analysis and simple frequencies (expressed in percentages) were used to describe the participants’ demographics and their contact lens characteristics. Non-parametric statistics were applied as the data was not normally distributed. Multivariate logistic regression was applied to investigate the association between the participants’ characteristics and non-compliant behaviors. Odd ratios (OR) along with 95% confidence intervals (CI) were calculated for each factor. Further, the association between the non-compliant behaviors and bacterial contamination was also studied using Chi-squared test. A P-value of ≤ 0.05 with a 95% confidence level was considered statistically significant.
Results
Participants and CL Usage
A total of 133 university students participated in this study. Mean age was 22.4 ± 4.4 (range 18–45 years) with female predominance (62.4%) as shown in Table 1. 128 participants (96.2%) were undergraduate students while five participants (3.8%) were postgraduate students. Most participants were from the Faculty of Medicine and Health Sciences, the Faculty of Sciences, and the Faculty of Fine Arts. All participants were using reusable hydrogel soft contact lenses which is commonly used in the local market due to its lower cost as found in a nearby country,23 and various types of commercially available MPS, for refractive error correction. The CL replacement rate was every 3–6 months (89, 66.9%), yearly (27, 20.3%), monthly (14, 10.5%) and weekly (3, 2.3%). The participants mostly wore CL for more than 6 months (122, 91.7%) and on an average of 5 days per week (115, 86.5%), 5–12 hours per day (124, 93.2%). The students mainly visit optometry centers to prescribe (113, 85%) and purchase CLs (132, 99.2%).
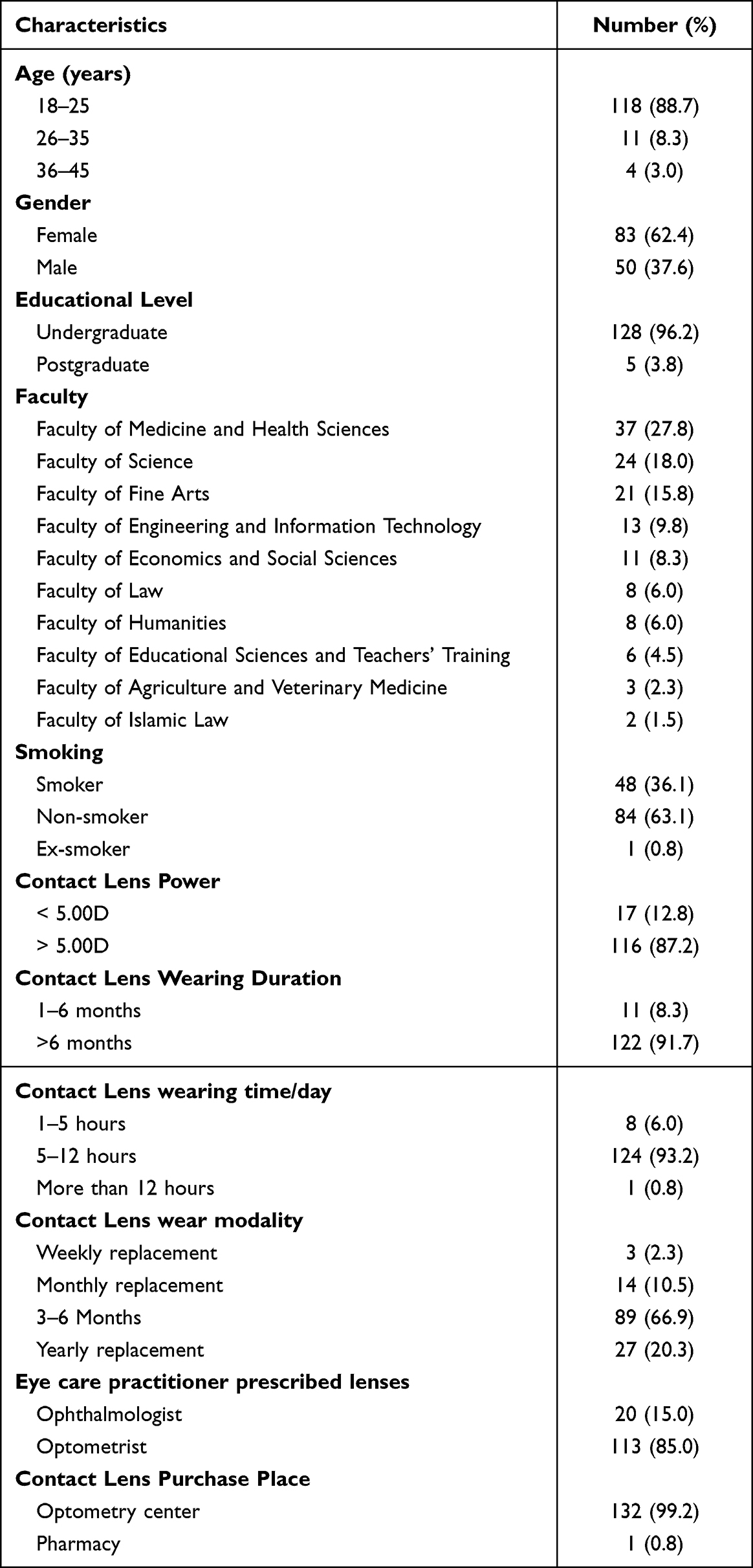 |
Table 1 Study Participants Demographics and Lens-Wearing Pattern (N=133) |
Aspects of Contact Lens Care
Table 2 displays the study participants’ attitudes on CL hygiene, cleaning solutions use, contact lens use, water exposure while wearing the CL and attending after care visits.
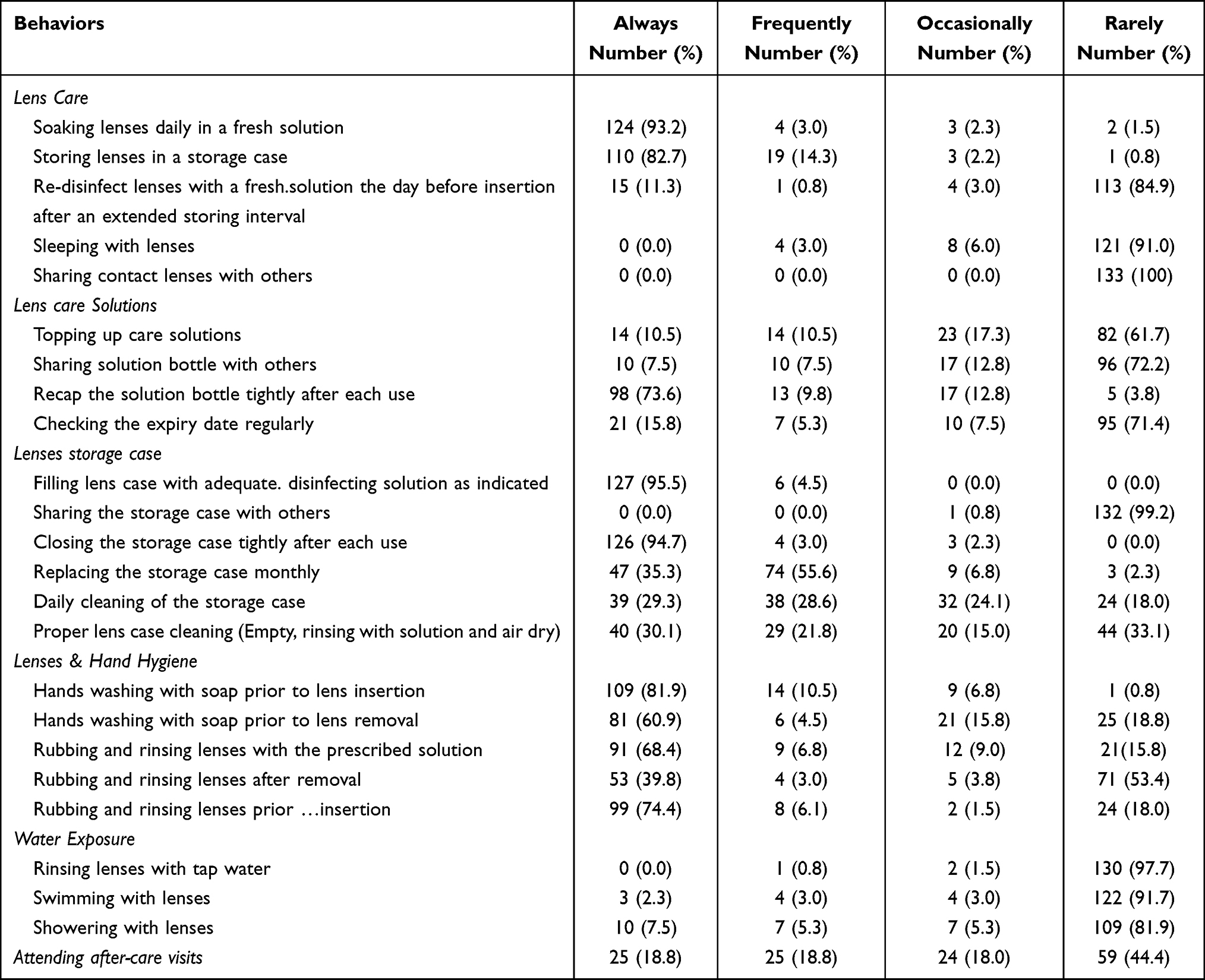 |
Table 2 Frequency of Reported Compliant Behaviors Related to Contact Lens Wear (N=133) |
The rates of compliance and non-compliance for each lens care procedure are shown in Table 3. The frequencies of scores 1 and 2 were added together to compute the compliance frequencies and the frequencies of scores 3 and 4 were added together to compute the non-compliance frequencies. The compliance rate in this study ranged between 12.1%-100%. Participants showed high compliance with; filling the lens case with adequate disinfecting solution as indicated, not sharing the lenses or storage case with others, not rinsing lenses with tap water, closing the storage case tightly after each use, storing lenses in a storage case, not sleeping with lenses, soaking lenses daily in a fresh solution, not swimming with lenses, hands washing with soap prior to lens insertion, monthly replacement of the storage case, not showering with lenses, not sharing the solution bottle with others, recapping the solution bottle tightly after each use, and rubbing and rinsing lenses prior insertion. A moderate compliance level was found in; no topping up care solutions, rubbing and rinsing lenses with prescribed solution, hand washing with soap prior to lens removal, daily cleaning of the storage case, proper lens case cleaning (empty, rinsing with solution and air dry) and rubbing and rinsing lenses after removal. A low level of compliance was found in attending after-care visits, checking the expiry date of the care solution regularly, and re-disinfecting the lenses with a fresh solution the day before insertion after an extended storage interval.
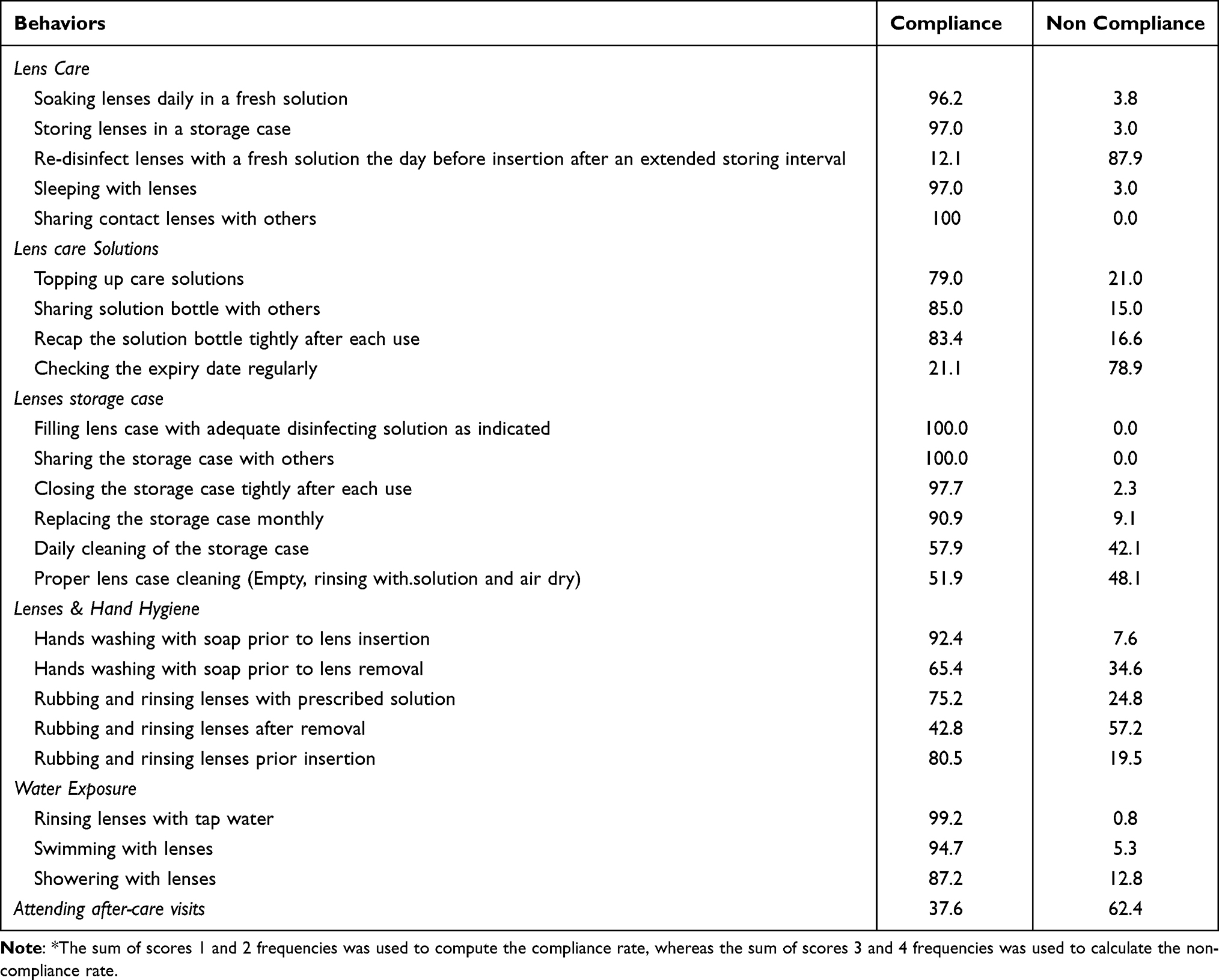 |
Table 3 Compliance and Non-Compliance Rates* of Contact Lens Care Behaviors |
Factors Affecting Contact Lens Compliance
Faculty, CL power, practitioner prescribed the lenses and, purchase place were not significantly associated with low compliance in any of CL behaviors (P>0.05), whereas male gender, youth age (18–25), smoking, CL wearing duration longer than six months, 5–12 hours of daily CL wearing, and the use of 3–6 months replacement rate CL were significantly associated with low compliance in some of the CL care behaviors, as shown in Table 4.
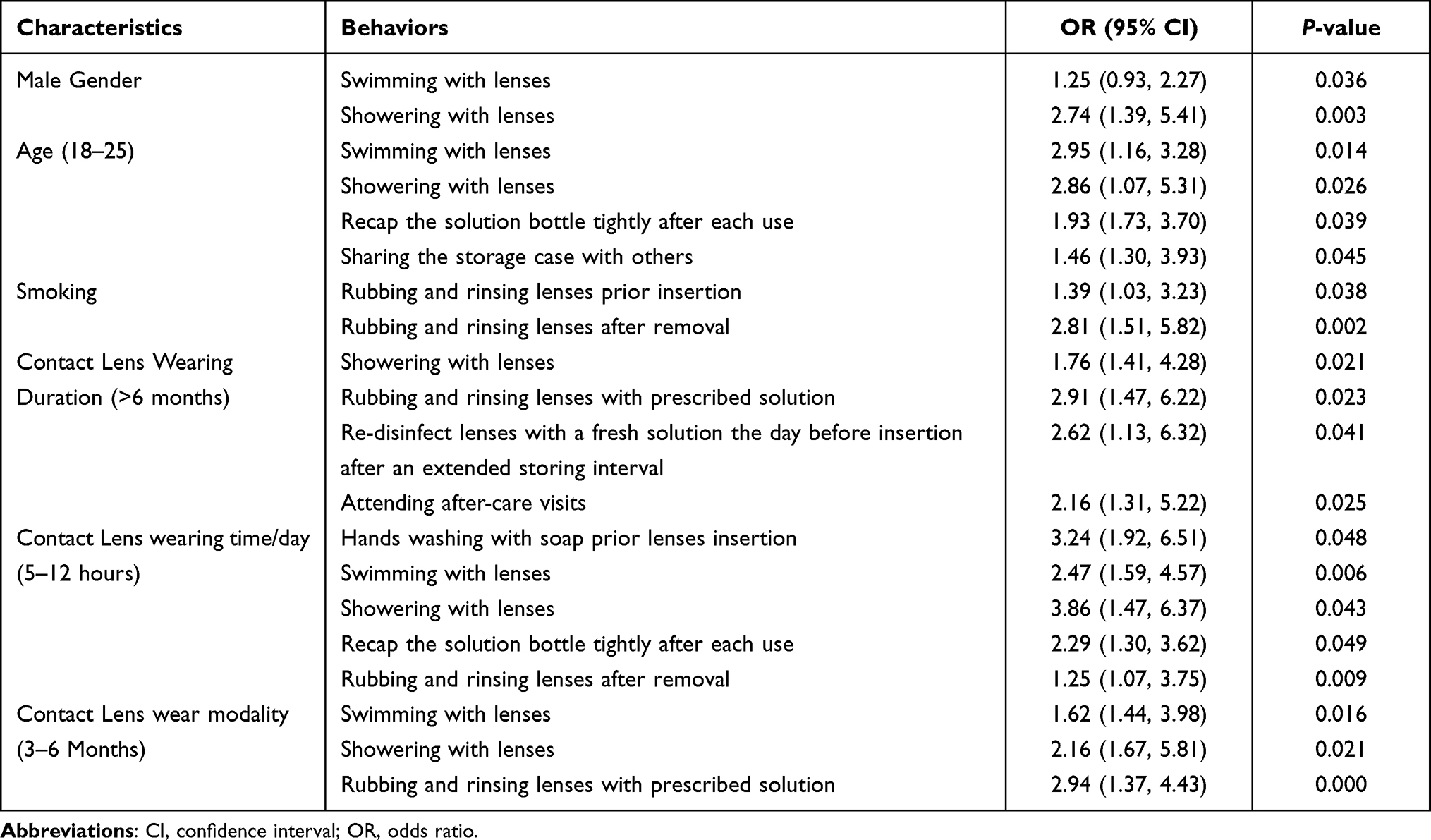 |
Table 4 Factors That are Attributed Significantly to a Low Level of Contact Lens Compliance |
Reasons for CL Non-Compliance
The possible reasons for CL care non-compliance indicated by the participants of this study are shown in Table 5. The most common reported reasons include: complexity of procedures recommended, poor understanding of verbal and/or written instructions, poor patient-practitioner relationship, and time needed to perform the prescribed tasks. Only poor understanding of the instructions contributed significantly to low level of non-compliance in re-disinfect lenses with a fresh solution the day before insertion after an extended storing interval (P=0.046) and proper lens case cleaning (P=0.031).
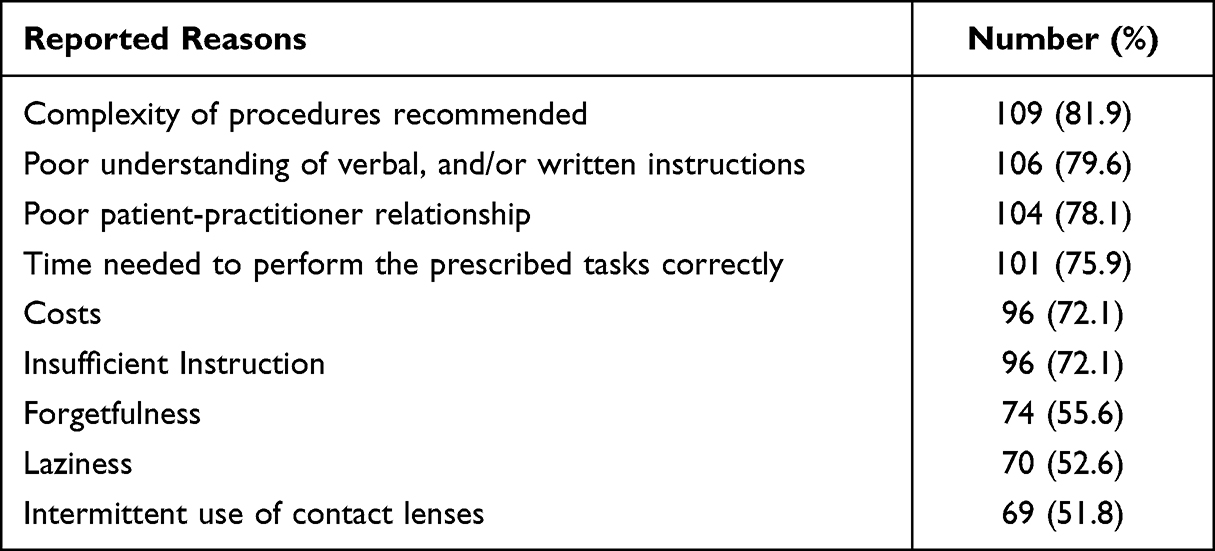 |
Table 5 Reasons for Contact Lens Compliance from the Participants’ Point of View (N=133) |
Bacterial Contamination
A sample from each participant’s CL storage was tested for bacterial contamination. A positive contamination was found in 26 cases (19.55%) of the collected samples and 107 cases (80.45%) did not show any positive sign of contamination. Eight different species of bacteria were isolated from the contaminated samples (Table 6). The predominant contaminants were Staphylococcus Aureus (5.3%) followed by Pseudomonas Aeruginosa (3.0%), Serratia Marcescens (3.0%), and Pseudomonas Pneumonia (2.3%).
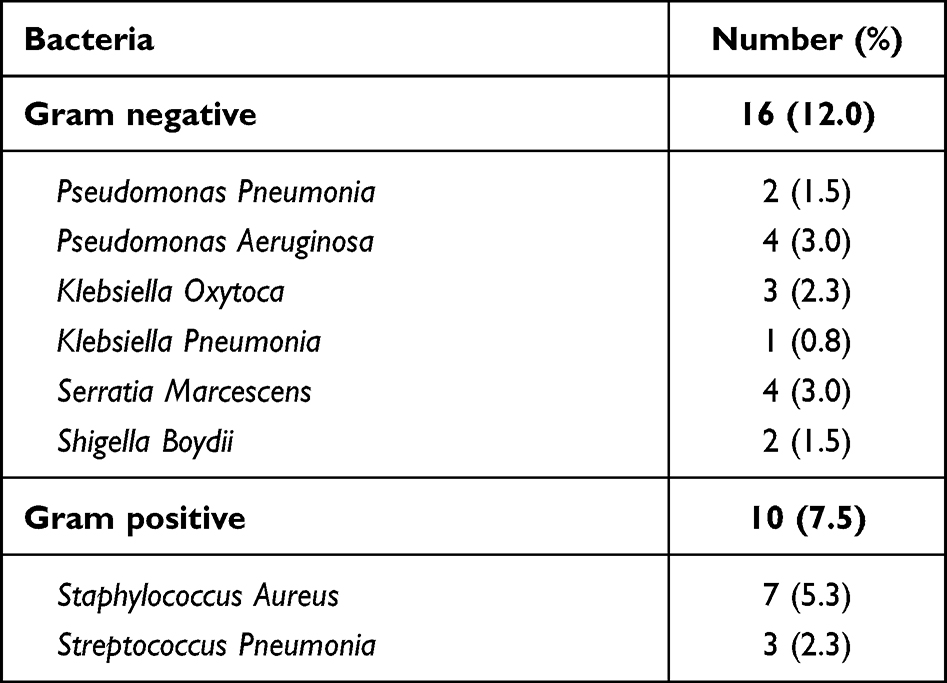 |
Table 6 Incidence of Bacterial Contaminants in Lens Cases Isolated from Collected Samples (N = 26) |
The CL care behaviors and their association with bacterial contamination are shown in Table 7. The CL care behaviors which showed a statistically significant impact on inducing bacterial contamination were; poor hand washing prior to CL insertion and removal (P=0.043), swimming (P=0.012) and showering (P=0.016) with CL, storing lenses in places other than the storage case (P=0.036), poor CL case cleaning (P=0.033), no replacement of CL case (monthly) (P=0.024) and inadequate CL disinfection after prolonged storage (P=0.048).
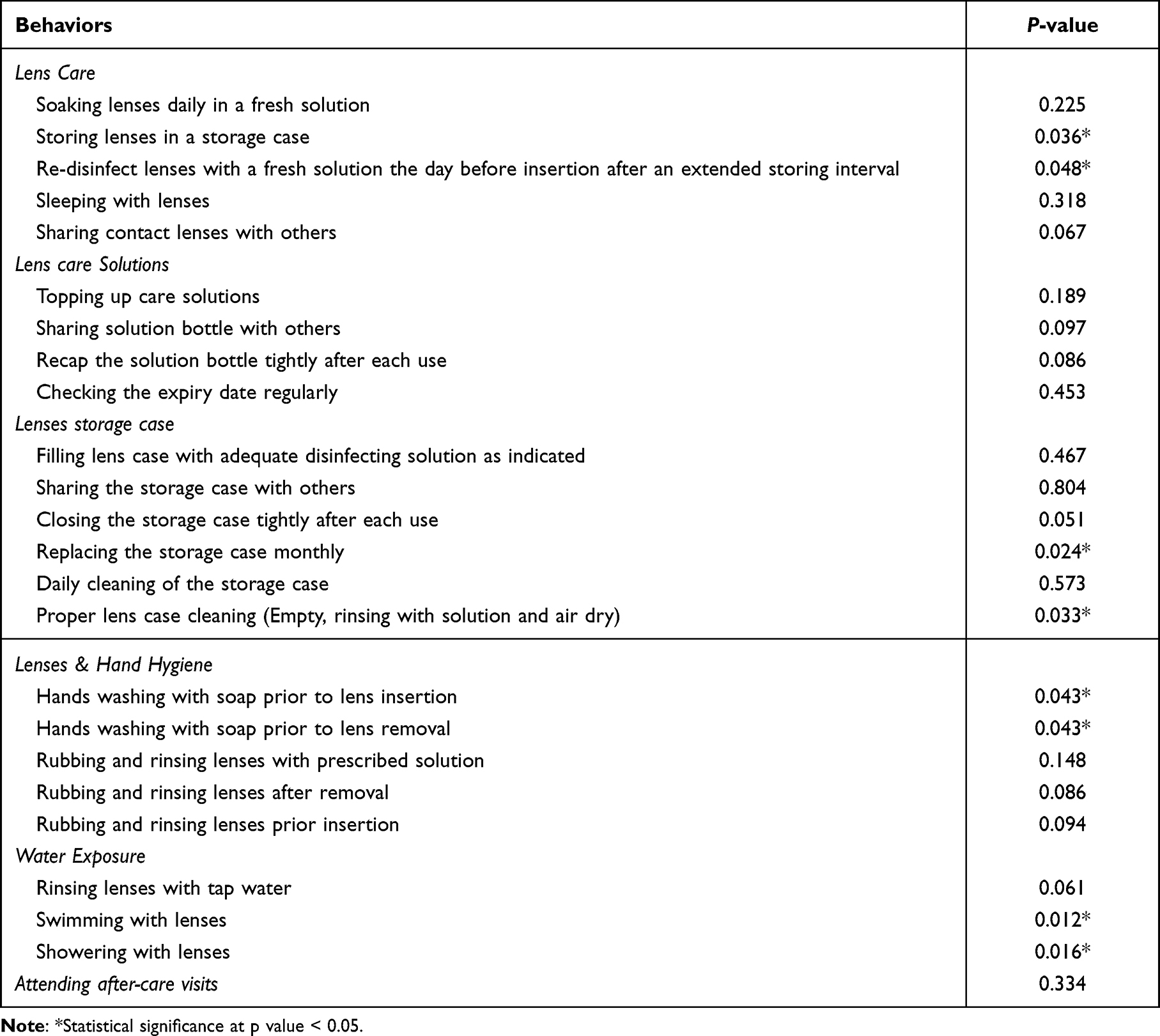 |
Table 7 Non-Compliance in Contact Lens Behaviors and Its Impact on Inducing Bacterial Contamination |
Discussion
This is the first study in Palestine which explores the CL’s care compliance among university students. This paper is unique in that it not only analyses the compliant and non-compliant CL care behaviors among university students in Palestine, but it also identifies the bacterial species found in the storage cases and the non-compliant behaviors that were associated with bacterial contamination. In addition, it analyses the reasons behind non-compliance from the CL wearer’s point of view. A full completion of the questionnaire, that was constructed based on previous research,1,2,4–9,26,27 was ensured through face-to-face interviews, which allowed gathering more detailed information from the participants.
Aspects of Contact Lens Care Compliance
In general, certain combinations of contact lens material and multipurpose solutions have been linked to corneal staining, ocular redness, and subjective symptoms30,31 including discomfort, which is the most common reason for CL patients to dropout.13 Noncompliance with CL and accessory care can exacerbate these symptoms and lead to more serious complications like corneal ulcers and microbial keratitis,11,32,33 so this should be given more public health attention because affected individuals may complain of pain, discomfort, and multiple visits to ophthalmic centers. In this study, the level of compliance was assessed in six areas: lens care, lens care solution, storage case, hygiene, water exposure, and aftercare visits.
Lens Care
The participants in this study were fully compliant with not sharing the CLs with others, which is consistent with previous research that found a high level of compliance in this behavior.5,27 Furthermore, there was a high level of compliance in storing the lenses daily in a fresh solution and in the designated storage case. However, a lower rate of compliance in this behavior (78.3%) was reported by Supiyaphun C and Jongkhajornpong P.7 Poor compliance in re-disinfecting the lenses before insertion after an extended storage interval was found in this study.
Sleeping with CLs was found to be a risk factor for inducing corneal ulcers,11,32 corneal infiltrative events,34 and microbial keratitis.33 In this study, high compliance was also found in not sleeping while wearing CLs. Similar findings were reported previously by Bakkar and Alzghoul5 and Sapkota et al,27 while Supiyaphun C and Jongkhajornpong P7 indicated that only 29.5% of their participants ever slept with CLs.
Lens Care Solution
In this study, there was a high level of compliance in not sharing the solution bottle with others and carefully closing the solution bottle after each usage. Noncompliance with these two behaviors could lead to ocular complications. There was moderate compliance (79.0%) in not topping up the lens solution. Lower rates ranging from 50 to 77% have been reported in the literature.1,10,35 ECPs need to pay more attention to this behavior as it could lead to Acanthamoeba keratitis.36 Checking the expiry date of the care solution on a regular basis was shown to have a low level of compliance. This would allow CL users to continue using the solution after it had expired and therefore weak or no preservatives.
Lens Storage Case
Inadequate cleaning and replacement of storage cases promotes the colonization of pathogenic organisms on the surface of the case and lens,8 which can then be conveyed to the eyes via fingers. Therefore, instructions in this regard must be thoroughly discussed during the CL dispensing consultation and emphasized during the follow-up visits.
The participants in this study were fully compliant with filling out the lens cases with adequate disinfecting solutions and not sharing the storage cases with others. High compliance was found in closing the storage case tightly after each use, which could prevent the transmission of germs into the case. In addition, this study found a high level of compliance in monthly storage case replacement, whereas prior research found a high,7 moderate5,26 and low6 level of compliance in replacing the cases once every one to three months. The most effective case cleaning procedure involves emptying the case of any leftover solution, rinsing it with MPS, and allowing it to air dry.37 Daily cleaning and rinsing of storage cases was found to be at a moderate level of compliance in this study, whereas lower levels have been reported in the literature.5,10,27
Lenses and Hands Hygiene
Contamination of CLs may occur if the lenses are handled with poor hygiene,38 which could lead to microbial keratitis.39 In this study, a high level of compliance was found in hand washing with soap and water prior to lens insertion, but a moderate level was found in hand washing prior to lens removal. This finding was expected as CL users clean their hands more frequently prior insertion than upon removal.40 Comparable rates of compliance in washing hands prior to CLs insertion have also been reported previously in a university-based population,5,7,27 and a higher level of compliance (83.3%) in hand washing prior to lens removal was reported by Supiyaphun C and Jongkhajornpong P.7 However, other studies indicated lower rates (>40%) in hand hygiene prior to lens insertion and removal in a population age similar to this study.6,41 This implies that age may not be a factor in poor or improved hand hygiene.
It is critical to rub and rinse CLs with the prescribed solution to prevent CL-related infection.1 Comparison of the findings with those of previous studies,1,5,7 this study found that rubbing and rinsing the lenses prior to insertion and after removal were found to have a moderate level of compliance, but with a lower rate of cleaning the lenses after removal (42.8%). An explanation of the rate variation could be an unclear recommendation of the necessity of CL cleaning prior to and after removal during the initial visit, in addition to the lack of reinforcement during the aftercare visits.
Water Exposure
Exposing the lenses to water by rinsing them directly with tap or bottled water, or when swimming or showering, is thought to increase the risk of vision-threatening corneal complications such as corneal ulcers, microbial keratitis,14,16,42 particularly Acanthamoeba keratitis43 and bacterial colonization on lenses.44 The current study demonstrates a high level of compliance in terms of not exposing the CLs to water by not rinsing the CL with tap water or swimming and showering with lenses. These findings are in line with previous studies that indicated high compliance with not cleaning the lenses with tab water,5,7,27,45 showering,27 and swimming27 with lenses. Other studies, however, found a moderate level of compliance with not swimming5,7 or showering5 with lenses and others showed a low level of compliance with not swimming42,45,46 or showering42 with lenses. The variable results could be due to differences in the participant’s demographics, clarity of CL care instructions, or different study designs.
After Care Visits
The participants of this study showed a low level of compliance in attending after care visits recommended by the ECPs. This finding accords with many reports on the low compliance rate in complying with the scheduled aftercare visits in university students5,6 or older adults,3 for example, Gyawali R et al (39.3%),3 Bakkar and Alzghoul (33.8%),5 and García-Ayuso D et al (19.2%).6 Failure to attend the CL’s after-care visits increases the risk of an undiagnosed complication, which could result in CL dropout.13 In addition, follow-up visits are critical for reinforcing the CL care instructions, which include recommendations for better lens use, solution, storage case, and behavior while wearing the lenses.1 As a result, ECPs must emphasize the need to attend follow-up consultations and discuss the potential complications that may arise for their patients during the initial visit.1
Factors Affecting Contact Lens Compliance
The study participants’ characteristics, as well as the features of their lenses, were investigated in regard to any contribution to a low level of contact lens compliance. Factors such as the faculty, CL power, the practitioner prescribing the lenses, and purchase place did not have an impact on the low level of compliance. This finding is supported by Supiyaphun C and Jongkhajornpong P’s study,7 but in contrast to earlier studies8,46 which found a positive impact of purchase place on low levels of CLs compliance. This could be explained by the fact that the majority of the participants in this study have similar educational levels and purchased the CLs from Optometry centers. A future study should include participants with different educational levels across the society.
Males were shown to have lower compliance in swimming and showering with lenses than females. Some studies observed an association between gender and low compliance,8,46 while others, such as those by Bakkar and Alzghoul5 and Supiyaphun C and Jongkhajornpong P,7 despite the fact that the latter found that males were more likely than females to have a history of CL problems.7 Additionally, the effect of age was found to have an effect on low compliance in a few behaviors, when the patient was between the ages of 18 and 25, such as swimming and showering with lenses, tightly closing the solution bottle after each use, and sharing the storage case with others. Previous research has indicated that younger adults are less compliant with CLs instruction than older adults in terms of hand hygiene,7,46 CL cleaning and using tab water with lenses,10,47 since young people are known to have risk-taking personalities.48
Smoking showed a positive impact on low compliance in rubbing and rinsing lenses prior insertion and after removal. Bakkar and Alzghoul5 also reported a similar correlation.
A lack of compliance in showering with lenses, rubbing and rinsing lenses with the prescribed solution, re-disinfecting lenses with a fresh solution the day before insertion after an extended storage interval, and attending after-care visits was found to be associated with a longer wearing experience of more than 6 months. This finding is consistent with previous research5,7 which found a significant impact of long CL experience duration on low compliance among university students. Therefore, reinforcement of care instructions needs to be carried out by the ECPs during the aftercare visits.
A 3–6 month CL replacement schedule was found to be associated with a low level of compliance in showering and swimming with lenses, as well as rubbing and rinsing lenses with the recommended solution. Furthermore, low compliance in hand washing with soap prior to lens insertion, showering and swimming with lenses, tightly closing the solution bottle after each use, and rubbing and rinsing lenses after removal was found to be5,7 related to CL wearing time of 5–12 hours per day. Previous investigations reported similar findings.5,7 Longer wearing time may result in laziness in adhering to compliance-related behaviors such as hygienic practices.5
Reasons for CL Non-Compliance
In the current studies, a few factors were reported by the participants as possible reasons for non-compliance after they had been given the appropriate instructions. The reported reasons include complexity of procedures recommended, poor understanding of instructions, poor patient-practitioner relationship, time needed to perform the prescribed tasks correctly, costs, insufficient instructions given, forgetfulness, laziness, and intermittent use of CL. Previous studies also reported similar reasons for non-compliance, such as costs,10 forgetfulness,40 complexity of procedures recommended7 and poor understanding of instructions.7
Poor comprehension of instructions was linked to a lack of compliance in proper lens case cleaning and re-disinfecting lenses with a new solution the day before insertion after an extended storage interval. These findings suggest that CL care and maintenance instructions may not be adequately explained to CL wearers. It is essential, therefore, for optometrists and eye care professionals to clearly illustrate the best practices of CL and accessory care and maintenance in the initial visit, provide them with illustrated handouts or videos,39 and provide an effective educational reinforcement strategy in order to enhance compliance and prevent low compliance-related complications.
Bacterial Contamination
Another aim of this study was to check for bacterial contamination among the participants. This can be accomplished through the culture of a sample from the lenses, solution, or storage case. In this study, a sample from the CL storage case was used because it has previously been reported that the highest contamination occurs in the storage case49 due to the formation of a thicker bacterial biofilm on the cases’ walls17,19 when compared to lenses, and its hygiene plays an important role in reducing CL-related complications, in addition to the fact that cross contamination could occur between the lenses, lens case, and the solution if any is present.50
In this study, positive bacterial contamination was found to be 19.55% (26/107 cases). This is consistent with previous research, which found a case contamination rate ranging between 18 to 85%.50 The variations in results between the different studies are due to differences in sample size, study site, lens types, microorganisms tested for, and methods used.50 The low contamination rate found in this study may be due to only checking for bacterial contamination and to the majority of the participants (61 participants, 45.8%) belonging to the Faculty of Medicine and Health Sciences (37 participants, 27.8%) and the Faculty of Science (24 participants, 18.0%), who may have higher hygiene standards and better understanding of contamination transmission. In this study, the most common bacteria recovered from the participants’ cases were Staphylococcus Aureus, Pseudomonas Aeruginosa, Serratia Marcescens, Pseudomonas Pneumonia, and with a lower percentage of Streptococcus Pneumonia, Klebsiella Oxytoca, Klebsiella Pneumonia and Shigella Boydii. These bacteria species have been reported in previous studies that looked for microbial contamination in CL user cases, and they are known to cause infection and inflammation of the cornea and other parts of the eye.11,12,20,21,50
In the current study, the CL care behaviors that were associated with CL case contamination were poor hand, lens, and case hygiene, as well as water exposure while wearing the lenses Poor personal hygiene was the most frequently reported risk factor for microorganism contamination in the literature. Proper cleaning of the storage cases is required to remove all microorganisms attached to the cases, but it is insufficient alone,17,19 due to its ability to form a biofilm that can be resistant to disinfecting solutions.17–19 As a result, CL users should be encouraged to change their lens cases at least once a month.1 Poor hand hygiene prior to CL insertion and removal, which is typical among young adults who use CL,46 also contributes to contamination development and is responsible for transferring bacteria to the eyes or CL cases via fingers. Swimming, showering, or cleaning the lenses with bottled water has also been linked to the contamination of the lenses by microorganisms such as Pseudomonas Aeruginosa or Acanthamoeba, which can lead to devastating complications such as CL-related microbial keratitis keratitis.43,44,50 Recommendations against using water with lenses should be taught during the initial visit and reinforced during follow-up visits.
Conclusion
This study investigated, for the first time, the SCL compliance and non-compliance behaviors of university students in Palestine. A moderate to high compliance level was found. Total compliance was found in filling the lens case with adequate disinfecting solution as indicated and not sharing the lenses or storage case with others, while the poorest compliance was found in attending after-care visits, checking the expiry date of the lens solution regularly, and re-disinfecting the lenses with a fresh solution the day before insertion after an extended storage interval. Poor understanding of the instructions contributed significantly to a low level of non-compliance. One important finding of this study is that non-compliance with lens storage cases in terms of cleaning, and replacement, in addition to poor hand hygiene and un-allowed water activities, had a higher risk of developing bacterial contamination in their storage cases. This study has a few limitations, including the use of a small sample of university students and the exclusion of individuals from the general public. This study was also unable to determine the accuracy of the instructions and advice offered to participants throughout the fitting process by eye care practitioners. Therefore, a more diversified and larger sample size study is needed in addition to including CL users who were given appropriate care instructions. Furthermore, while this study only looked into bacterial contamination, other microorganisms need to be included as well. However, despite these limitations, it added valuable data on the CL compliance status in Palestine and highlighted the importance of proper patient education on safer lens wear modalities, proper wearing schedules, and hygiene regimens, previously, in order to reduce the risks of developing contact lens complications.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Morgan PB, Efron N, Toshida H, Nichols JJ. An international analysis of contact lens compliance. Cont Lens Anterior Eye. 2011;34(5):223–228. doi:10.1016/j.clae.2011.08.001
2. Rueff EM, Wolfe J, Bailey MD. A study of contact lens compliance in a non-clinical setting. Cont Lens Anterior Eye. 2019;42(5):557–561. doi:10.1016/j.clae.2019.03.001
3. Gyawali R, Nestha Mohamed F, Bist J, Kandel H, Marasini S, Khadka J. Compliance and hygiene behavior among soft contact lens wearers in the Maldives. Clin Exp Optom. 2014;97(1):43–47. doi:10.1111/cxo.12069
4. Hickson-Curran S, Chalmers RL, Riley C. Patient attitudes and behavior regarding hygiene and replacement of soft contact lenses and storage cases. Cont Lens Anterior Eye. 2011;34(5):207–215. doi:10.1016/j.clae.2010.12.005
5. Bakkar MM, Alzghoul EA. Assessment of compliance with contact lens wear and care among university-based population in Jordan. Cont Lens Anterior Eye. 2020;43(4):395–401. doi:10.1016/j.clae.2020.02.020
6. García-Ayuso D, Moya-Rodríguez E, Valiente-Soriano FJ, Galindo-Romero C, Sobrado-Calvo P, Di Pierdomenico J. University students fail to comply with contact lens care. Cont Lens Anterior Eye. 2021;45:101411. doi:10.1016/j.clae.2021.01.006
7. Supiyaphun C, Jongkhajornpong P. Contact lens use patterns, behavior and knowledge among university students in Thailand. Clin Ophthalmol. 2021;15:1249–1258. doi:10.2147/OPTH.S304735
8. Bui TH, Cavanagh HD, Robertson DM. Patient compliance during contact lens wear: perceptions, awareness, and behavior. Eye Contact Lens. 2010;36(6):334–339. doi:10.1097/ICL.0b013e3181f579f7
9. Giri PA, Chavan WM, Phalke DB, Bangal SV. Knowledge and practice of contact lens wear and care among contact lens users medical students of rural medical college, Loni, Maharashtra, India. Int J Biol Med Res. 2012;3(1):1385–1387.
10. Dumbleton KA, Richter D, Woods CA, et al. A multi-country assessment of compliance with daily disposable contact lens wear. Cont Lens Anterior Eye. 2013;36(6):304–312. doi:10.1016/j.clae.2013.05.004
11. Lim CHL, Stapleton F, Mehta JS. Review of contact lens–related complications. Eye Contact Lens. 2018;44:S1–S10. doi:10.1097/ICL.0000000000000481
12. Stellwagen A, Macgregor C, Kung R, Konstantopoulos A, Hossain P. Personal hygiene risk factors for contact lens-related microbial keratitis. BMJ Open Ophthalmol. 2020;5(1):e000476. doi:10.1136/bmjophth-2020-000476
13. Pucker AD, Tichenor AA. A review of contact lens dropout. Clin Optom. 2020;12:85–94. doi:10.2147/OPTO.S198637
14. Becmeur PH, Abry F, Bourcier T, Meyer N, Sauer A. Risk factors for contact lens-related microbial keratitis: a multicenter case-control study. J Fr Ophtalmol. 2017;40(3):224–231. doi:10.1016/j.jfo.2016.10.008
15. Sauer A, Meyer N, Bourcier T, et al. Risk factors for contact lens-related microbial keratitis: a case-control multicenter study. Eye Contact Lens. 2016;42(3):158–162. doi:10.1097/ICL.0000000000000180
16. Green M, Apel A, Stapleton F. Risk factors and causative organisms in microbial keratitis. Cornea. 2008;27(1):22–27. doi:10.1097/ICO.0b013e318156caf2
17. McLaughlin-Borlace L, Stapleton F, Matheson M, Dart JKG. Bacterial biofilm on contact lenses and lens storage cases in wearers with microbial keratitis. J Appl Microbiol. 1998;84(5):827–838. doi:10.1046/j.1365-2672.1998.00418.x
18. Russell AD. Bacterial resistance to disinfectants: present knowledge and future problems. J Hosp Infect. 1999;43(SUPPL 1):S57–S68. doi:10.1016/S0195-6701(99)90066-X
19. Szczotka-Flynn LB, Imamura Y, Chandra J, et al. Increased resistance of contact lens-related bacterial biofilms to antimicrobial activity of soft contact lens care solutions. Cornea. 2009;28(8):918–926. doi:10.1097/ICO.0b013e3181a81835
20. Szczotka-Flynn LB, Pearlman E, Ghannoum M. Microbial contamination of contact lenses, lens care solutions, and their accessories: a literature review. Eye Contact Lens. 2010;36(2):116–129. doi:10.1097/ICL.0b013e3181d20cae
21. Holden B, La Hood D, Grant T, et al. Gram-negative bacteria can induce contact lens related acute red eye (CLARE) responses. CLAO J. 1996;22(1):47–52.
22. Morgan PB, Efron N, Helland M, et al. Demographics of international contact lens prescribing. Cont Lens Anterior Eye. 2010;33(1):27–29. doi:10.1016/J.CLAE.2009.09.006
23. Haddad MF, Bakkar M, Gammoh Y, Morgan P. Trends of contact lens prescribing in Jordan. Cont Lens Anterior Eye. 2016;39(5):385–388. doi:10.1016/J.CLAE.2016.06.004
24. Bakkar MM, Alzghoul EA. Assessment of contact lens wearers’ attitude toward contact lens wear and care during Coronavirus Disease 2019 (COVID-19) pandemic: a cross-sectional online survey. Cont Lens Anterior Eye. 2021;44(6):101410. doi:10.1016/j.clae.2021.01.005
25. Vianya-Estopa M, Garcia-Porta N, Piñero D, et al. Contact lens wear and care in Spain during the COVID-19 pandemic. Cont Lens Anterior Eye. 2021;44(5):101381. doi:10.1016/j.clae.2020.11.001
26. Yung AMS, Boost MV, Cho P, Yap M. The effect of a compliance enhancement strategy (self-review) on the level of lens care compliance and contamination of contact lenses and lens care accessories. Clin Exp Optom. 2007;90(3):190–202. doi:10.1111/j.1444-0938.2007.00147.x
27. Sapkota K. Level of compliance in contact lens wearing medical doctors in Nepal. Cont Lens Anterior Eye. 2015;38(6):456–460. doi:10.1016/j.clae.2015.05.010
28. Yung MS, Boost M, Cho P, Yap M. Microbial contamination of contact lenses and lens care accessories of soft contact lens wearers (university students) in Hong Kong. Ophthalmic Physiol Opt. 2007;27(1):11–21. doi:10.1111/j.1475-1313.2006.00427.x
29. Murray PR, Baron EJ, Jorgensen JH, Pfaller MA, Yolken RH, Hanna BA. Manual of clinical microbiology, 8th edition:manual of clinical microbiology. Clini Infect Dis. 2004;38(8):1199–1200. doi:10.1086/383067
30. Beshtawi IM, Qaddomi J, Khuffash H, El-Titi S, Ghannam M, Otaibi R. Ocular surface response and subjective symptoms associated to lens care solutions in Palestine. J Optom. 2019;12(4):248–255. doi:10.1016/j.optom.2019.03.001
31. Garofalo RJ, Dassanayake N, Carey C, Stein J, Stone R, David R. Corneal staining and subjective symptoms with multipurpose solutions as a function of time. Eye Contact Lens. 2005;31(4):166–174. doi:10.1097/01.ICL.0000152489.99455.DB
32. Stapleton F, Keay L, Edwards K, et al. The incidence of contact lens-related microbial keratitis in Australia. Ophthalmology. 2008;115(10):1655–1662. doi:10.1016/j.ophtha.2008.04.002
33. Dart J, Radford C, Minassian D, Verma S, Stapleton F. Risk factors for microbial keratitis with contemporary contact lenses: a case-control study. Ophthalmology. 2008;115:10. doi:10.1016/J.OPHTHA.2008.05.003
34. Chalmers R, Keay L, McNally J, Kern J. Multicenter case-control study of the role of lens materials and care products on the development of corneal infiltrates. Optom Vis Sci. 2012;89(3):316–325. doi:10.1097/OPX.0B013E318240C7FF
35. Vianya-Estopa M, Wolffsohn J, Beukes E, Trott M, Smith L, Allen P. Soft contact lens wearers’ compliance during the COVID-19 pandemic. Cont Lens Anterior Eye. 2021;44(4). doi:10.1016/J.CLAE.2020.08.003
36. Verani J, Lorick S, Yoder J, et al. National outbreak of Acanthamoeba keratitis associated with use of a contact lens solution, United States. Emerg Infect Dis. 2009;15(8):1236–1242. doi:10.3201/EID1508.090225
37. Wu Y, Zhu H, Willcox M, Stapleton F. Removal of biofilm from contact lens storage cases. Invest Ophthalmol Vis Sci. 2010;51(12):6329–6333. doi:10.1167/IOVS.10-5796
38. Fonn D, Jones L. Hand hygiene is linked to microbial keratitis and corneal inflammatory events. Cont Lens Anterior Eye. 2019;42(2):132–135. doi:10.1016/J.CLAE.2018.10.022
39. Lim CHL, Carnt NA, Farook M, et al. Risk factors for contact lens-related microbial keratitis in Singapore. Eye. 2016;30(3):447–455. doi:10.1038/eye.2015.250
40. Dumbleton K, Richter D, Bergenske P, Jones L. Compliance with lens replacement and the interval between eye examinations. Optom Vis Sci. 2013;90(4):351–358. doi:10.1097/OPX.0B013E318288AFCB
41. Wu Y, Carnt N, Stapleton F. Contact lens user profile, attitudes and level of compliance to lens care. Cont Lens Anterior Eye. 2010;33(4):183–188. doi:10.1016/j.clae.2010.02.002
42. Zimmerman A, Richdale K, Mitchell G, et al. Water exposure is a common risk behavior among soft and gas-permeable contact lens wearers. Cornea. 2017;36(8):995–1001. doi:10.1097/ICO.0000000000001204
43. Carnt N, Hoffman J, Verma S, et al. Acanthamoeba keratitis: confirmation of the UK outbreak and a prospective case-control study identifying contributing risk factors. Br J Ophthalmol. 2018;102(12):1621–1628. doi:10.1136/BJOPHTHALMOL-2018-312544
44. Choo J, Vuu K, Bergenske P, Burnham K, Smythe J, Caroline P. Bacterial populations on silicone hydrogel and hydrogel contact lenses after swimming in a chlorinated pool. Optom Vis Sci. 2005;82(2):134–137. doi:10.1097/01.OPX.0000153168.54495.DA
45. Robertson DM, Cavanagh HD. Non-compliance with contact lens wear and care practices: a comparative analysis. Optom Vis Sci. 2011;88(12):1402–1408. doi:10.1097/OPX.0B013E3182333CF9
46. Wagner H, Richdale K, Mitchell G, et al. Age, behavior, environment, and health factors in the soft contact lens risk survey. Optom Vis Sci. 2014;91(3):252–261. doi:10.1097/OPX.0000000000000164
47. Cope J, Collier S, Nethercut H, Jones J, Yates K, Yoder J. Risk behaviors for contact lens-related eye infections among adults and adolescents - United States, 2016. MMWR Morb Mortal Wkly Rep. 2017;66(32):841–845. doi:10.15585/MMWR.MM6632A2
48. Cook P, Bellis M. Knowing the risk: relationships between risk behavior and health knowledge. Public Health. 2001;115(1):54–61. doi:10.1038/SJ/PH/1900728
49. Thakur D, Gaikwad U. Microbial contamination of soft contact lenses & accessories in asymptomatic contact lens users. Indian J Med Res. 2014;140(2):307–309.
50. Wu YTY, Willcox M, Zhu H, Stapleton F. Contact lens hygiene compliance and lens case contamination: a review. Cont Lens Anterior Eye. 2015;38(5):307–316. doi:10.1016/j.clae.2015.04.007
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.