")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Complex effects of childhood abuse, affective temperament, and subjective social status on depressive symptoms of adult volunteers from the community
Authors Higashiyama M, Hayashida T, Sakuta K, Fujimura Y, Masuya J , Ichiki M, Tanabe H, Kusumi I , Inoue T
Received 18 March 2019
Accepted for publication 30 July 2019
Published 27 August 2019 Volume 2019:15 Pages 2477—2485
DOI https://doi.org/10.2147/NDT.S209100
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Taro Kishi
Motoki Higashiyama,1 Taito Hayashida,1 Keisuke Sakuta,1 Yota Fujimura,2 Jiro Masuya,3 Masahiko Ichiki,1 Hajime Tanabe,4 Ichiro Kusumi,5 Takeshi Inoue1
1Department of Psychiatry, Tokyo Medical University, Tokyo 160-0023, Japan; 2Department of Psychiatry, Tokyo Medical University Hachioji Medical Center, Tokyo 193-0998, Japan; 3Department of Psychiatry, Tokyo Medical University Ibaraki Medical Center, Ibaraki 300-0395, Japan; 4Department of Clinical Human Sciences, Graduate School of Humanities and Social Sciences, Shizuoka University, Shizuoka 422-8529, Japan; 5Department of Psychiatry, Hokkaido University Graduate School of Medicine, Sapporo 060-8638, Japan
Correspondence: Takeshi Inoue
Department of Psychiatry, Tokyo Medical University, 6-7-1 Nishishinjuku, Shinjuku-ku, Tokyo 160-0023, Japan
Tel +81 33 342 6111
Fax +81 33 340 4499
Email [email protected]
Background: How subjective social status is associated with childhood abuse and affective temperament in the mechanism of depressive symptom exacerbation remains unknown. In this study, we investigated how the complex effects of subjective social status, childhood abuse, and affective temperament influence depressive symptoms in adulthood.
Methods: Self-report questionnaires were distributed to 853 adult volunteers between January and August 2014. Of them, 404 people gave full consent and returned complete anonymous responses. The following five questionnaires were analyzed: demographic information, Patient Health Questionnaire-9, subjective social status, Child Abuse and Trauma Scale, and Temperament Evaluation of Memphis, Pisa, Paris and San Diego autoquestionnaire. The associations between the scores were analyzed by structural equation modeling. This study was conducted with approval from the ethics committees of Tokyo Medical University and Hokkaido University Hospital.
Results: Covariance structure analysis demonstrated that childhood abuse and subjective social status did not have a direct effect on adulthood depressive symptoms. Childhood abuse had direct effects on subjective social status and affective temperament and childhood abuse indirectly affected adulthood depressive symptoms through subjective social status and affective temperament. Subjective social status also affected depressive symptoms through an effect on affective temperament. This model explained 43% of the variability in depressive symptoms and the fitness of this model was good.
Conclusion: Regarding childhood abuse and adulthood depressive symptoms, subjective social status as well as affective temperament may be mediators. The results of this study are expected to contribute to the elucidation of the mechanism of depression.
Keywords: childhood abuse, subjective social status, affective temperament, depression, covariance structure analysis
Introduction
Various factors, such as the environment, personality, genetics, etc., have been reported as risk factors for the onset of depression.1–3 Several studies have shown that childhood experiences are a significant environmental factor. Various experiences in childhood, such as unhappy experiences, abuse, and low level of care, are major risk factors for the onset of depression.1,4,5 Experiencing childhood adversities (ie, domestic violence, divorce of parents, and child neglect) has been shown to increase the prevalence of depression.1,6–8 A comparison of personality traits between healthy subjects and patients with mood disorders showed that patients with mood disorders have higher affective temperament scores regarding depressive, cyclothymic, anxious, and irritable temperaments; these affective temperament scores were positively correlated with depressive symptoms in adult volunteers from the community and patients with depression.4,5,9–11
Depression constitutes a major public health concern because it is a substantial economic burden and has various negative consequences, such as suicidal behavior.12,13 To date, antidepressant medications, such as selective serotonin reuptake inhibitors, serotonin–noradrenaline reuptake inhibitors, and other new classes of antidepressants,14,15 have demonstrated their efficacy and potential to prevent negative outcomes associated with this debilitating illness.12 However, at least 5–10% of patients with depression meet the criteria for treatment-resistant depression.16 Therefore, the rapid diagnosis and treatment of people with depression is crucial for the welfare of the whole community. Childhood abuse, particular personality traits, and negative events during adult life are known to affect treatment responses to antidepressants.17 Therefore, the identification of predictors or risk factors that can assist in the diagnosis, classification of subtypes, and monitoring of disease progression is necessary from a therapeutic viewpoint.
Since the 1990’s, the association between health and social class has drawn attention and has been studied in various fields. Studies have demonstrated that not only objective socioeconomic status (OSS) but also subjective social status (SSS) affects health. SSS is a subjective measurement of people’s perception about where they are located in the social order structure,18,19 and subjects answer the following question “If society was divided into 10 social strata, which stratum do you think you would belong to?” Recently, a worldwide survey demonstrated that SSS is associated with several mental illnesses, including depression, bipolar disorder, anxiety disorder, drug dependence, etc.20 SSS was reported to be lower in depressed patients.20 The close association between SSS and mental health has been confirmed by many studies.21 In addition, as SSS is also associated with the severity of depressive symptoms in adult volunteers from the community, SSS may contribute to the onset of depression.22 However, there have been no prospective studies clarifying whether SSS is a predictive factor for the onset of depression. Furthermore, the mechanism by which SSS affects depression or depressive symptoms has remained unclear.
Various studies have shown that both childhood abuse and affective temperament are associated with the onset of major depressive disorder and with the development of depressive symptoms.1,4,5,9–11,17 Interactions among these factors may also affect depressive symptoms. For example, childhood abuse affects depressive symptoms through affecting affective temperament.5,10,17 Although there has been no research on the association of SSS with childhood abuse, OSS was shown to be associated with childhood abuse and to also affect the general health, mental health, and well-being of adults.23 We recently reported that the quality of parenting that a subject received as a child, which includes neglect, affects SSS.24 SSS is also associated with affective temperament (our unpublished data). In addition, SSS and OSS are associated with major depression/depressive symptoms to the same degree, but the effect of SSS is partly independent of OSS.20,22 Therefore, there is the possibility that SSS may affect any step of the pathways by which childhood abuse affects depressive symptoms through affective temperament. However, it has not been clarified as to whether SSS produces a complex effect together with childhood abuse or affective temperament in the mechanism of depressive symptom exacerbation.
In this study, using structural equation modeling, we aimed to clarify whether SSS, childhood abuse, and affective temperament interact with one another and affect depressive symptoms in adult volunteers from the community.
Subjects and methods
Subjects
Between January and August 2014, self-reported questionnaires were distributed to 853 nonclinical adult volunteers in Hokkaido University (Sapporo, Japan) through our acquaintances. The inclusion criteria were (a) being 20 years of age or older, (b) not having severe physical diseases, (c) not having organic brain diseases, and (d) having the ability to consent to this study. Of them, 404 people (220 men, 184 women; average age: 42.3 ± 11.9 years) gave full consent and returned complete anonymous responses. This study was part of a larger study,25 in which several questionnaires on demographic information, personality traits, and psychological symptoms were analyzed. No particular exclusion criteria were set. Written informed consent was obtained from all of the subjects after giving the following explanations: 1) their participation in this research is voluntary and not mandatory, 2) there is no disadvantage in not participating, and 3) the information from this research project will be kept completely confidential and managed anonymously. In accordance with the Helsinki Declaration, this study was conducted with approval from the ethics committees of Tokyo Medical University and Hokkaido University Hospital.
Questionnaires
The Patient Health Questionnaire-9 (PHQ-9) is a self-administered depression evaluation questionnaire composed of 9 items.26 The Japanese version of the PHQ-9 was developed by Muramatsu et al, and its reliability and validity have been verified.27 In this study, the total PHQ-9 score (0–27 points) was used for the analysis.
The Temperament Evaluation of Memphis, Pisa, Paris and San Diego-autoquestionnaire (TEMPS-A) is a self-rating questionnaire that quantitatively evaluates premorbid personality traits of mood disorders.28 TEMPS-A consists of 109 items in men and 110 items in women; depressive (21 items), cyclothymic (21 items), hyperthymic (21 items), irritable (20 items in men and 21 items in women), and anxious (26 items). The TEMPS-A is answered using a 2-point scale, and the average score of each subscale is used as the final score. In this study, the Japanese version of TEMPS-A developed by Akiyama et al was used.29
The Child Abuse and Trauma Scale (CATS) is a self-rating questionnaire to retrospectively evaluate the frequency and extent of various types of negative experiences in childhood and adolescence.30 The Japanese version translated by Tanabe et al31 was used in this study. The CATS consists of 38 items divided into the following subscales: sexual abuse (6 items), neglect/negative home atmosphere (14 items), punishment (6 items), and others (12 items). A 5-point Likert scale was used for each item (0–4; 0 =never; 4 =always). The average scores of each subscale or of all items were used for the analysis.
SSS measures people’s perceptions of which stratum they belong to among the 10 social strata. The questionnaire asks respondents the question “If Japanese society was divided into 10 social strata, which stratum do you think you would belong to?”.32 In this study, we defined 1 as the highest social status level and 10 as the lowest social status level.
Data analysis
To analyze the association among the demographic information and questionnaire data with depressive symptoms (PHQ-9), the Pearson correlation coefficient or Student's t-test was performed using SPSS Statistics 22.0 J (SPSS, Chicago, IL, USA). Furthermore, stepwise multiple regression analysis was performed, in which data from the demographic characteristics and questionnaires were independent variables and a summary score of the PHQ-9 was a dependent variable. Various demographic factors were added as independent variables because these may affect the association between CATS, SSS, and TEMPS-A with depressive symptoms.
The following structural equation model was designed, in which the depressive symptoms (PHQ-9 scores) were predicted by childhood abuse (CATS subscale scores), SSS, and affective temperament (TEMPS-A scores). Covariance structure analysis with the robust maximum likelihood estimation method was performed using Mplus version 7.3 software (Muthén & Muthén, Los Angeles, CA, USA), to analyze complex associations and mediation effects. Two latent variables were defined, namely, “childhood abuse” from the observed variables of neglect, punishment, and sexual abuse scores of the CATS, and “TEMPS-A” from the observed variables of depressive, cyclothymic, anxious, and irritable temperament scores. In this study, the comparative fit index (CFI) and root mean square error of approximation (RMSEA) were used for evaluating the goodness of fit of the model. A good fit was defined as a CFI > 0.97 and RMSEA < 0.05, and an acceptable fit was defined as CFI > 0.95 and RMSEA < 0.08.33 All coefficients of the covariance structure analysis were standardized (−1 to +1).
A p-value of less than 0.05 was considered to indicate a statistically significant difference between 2 groups. In the structural equation model (see Figure 1), childhood abuse is assumed to affect SSS and affective temperament (TEMPS-A) and have an indirect effect on depressive symptoms through its effects on SSS and affective temperament (TEMPS-A). SSS is assumed to have an indirect effect on depressive symptoms through its effects on TEMPS-A.
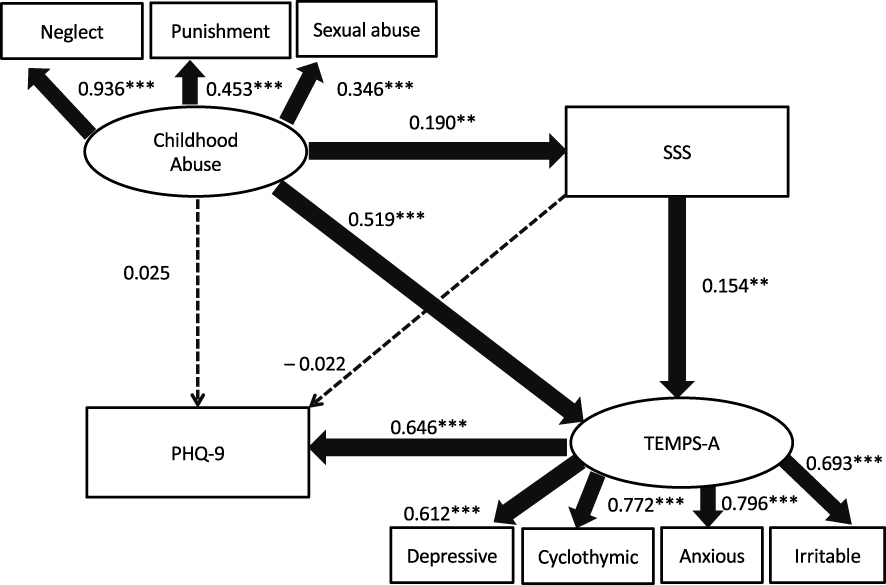 |
Figure 1 Results of covariance structure analysis of the structural equation model with the childhood abuse subscale on child abuse and trauma (childhood abuse), subjective social status score (SSS), and the score of the Temperament Evaluation of Memphis, Pisa, Paris and San Diego autoquestionnaire (TEMPS-A), as well as depressive symptoms (PHQ-9) in 404 adult volunteers from the community. Rectangles indicate the observed variables, some of which are associated with the latent variable, which is shown as an oval. The arrows with solid lines represent the statistically significant paths, and the broken lines show the nonsignificant paths. The numbers beside the arrows show the direct standardized path coefficients (minimum: –1; maximum: +1), but indirect effects through variables are shown in the Results section. **p < 0.01, ***p < 0.001. |
Results
Demographic information, questionnaire data, and PHQ-9 summary scores of the subjects
Table 1 shows the results of the demographic and questionnaire data in 404 adult volunteers from the community and their association with depressive symptoms (PHQ-9 summary scores). Age, sex, and marital status were significantly associated with PHQ-9 summary scores, but no other demographic factor was associated with PHQ-9 summary scores.
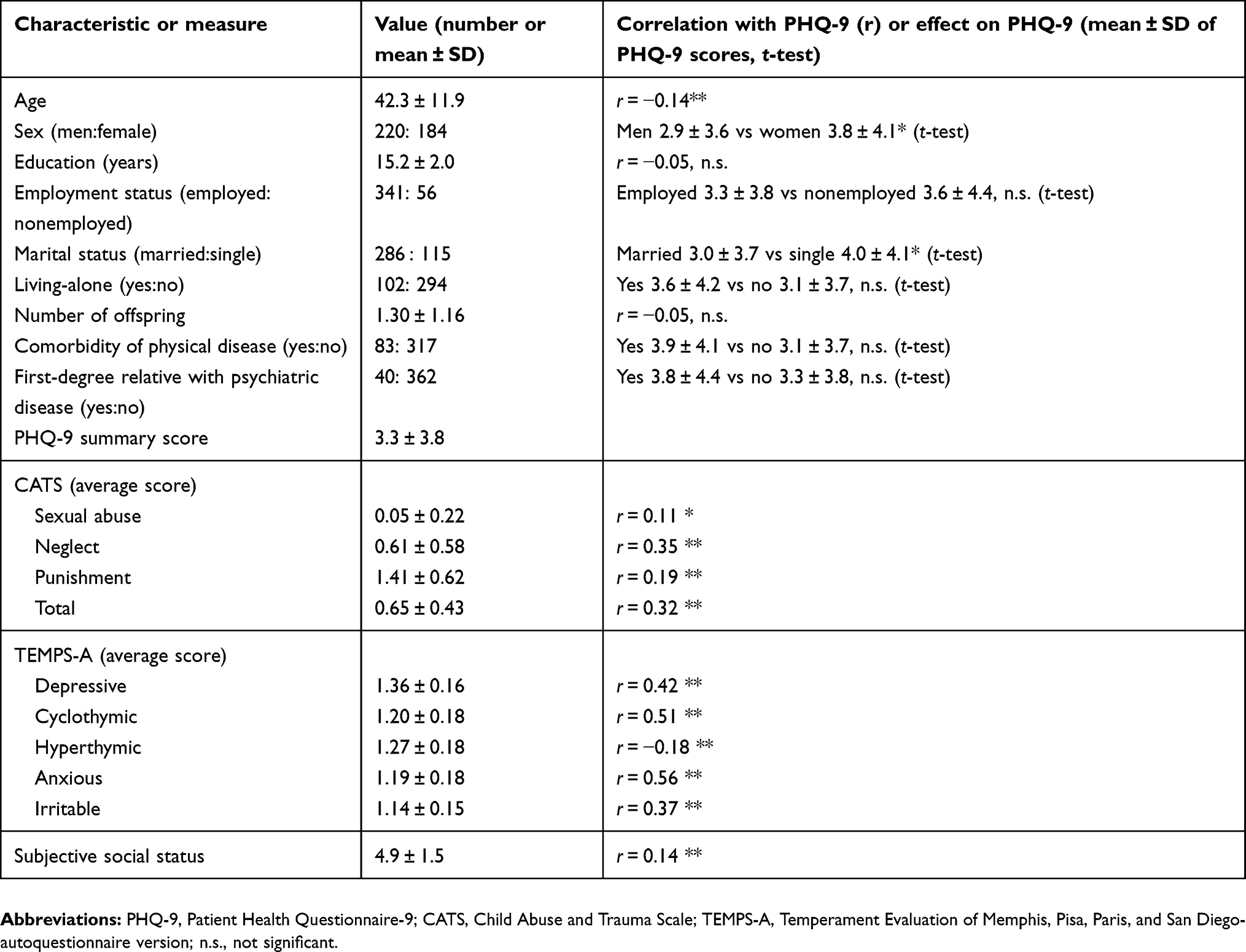 |
Table 1 Characteristics of the study subjects and correlation with or effects on PHQ-9 |
Sexual abuse, neglect, punishment subscores, and total scores of the CATS and depressive, cyclothymic, anxious, and irritable temperament scores of the TEMPS-A were positively associated with PHQ-9 summary scores. PHQ-9 summary scores were negatively associated with hyperthymic temperament scores of the TEMPS-A. SSS scores were positively correlated with PHQ-9 summary scores; in other words, the lower the SSS (high SSS scores indicate low SSS in this study), the stronger the severity of depressive symptoms.
Multiple regression analysis of PHQ-9 summary scores by the stepwise method
Table 2 shows the results of multiple regression analysis of PHQ-9 summary scores by the stepwise method. Eighteen independent variables, including those from the CATS, TEMPS-A, and SSS were added to the analysis, but the stepwise method demonstrated that significant independent variables predicting PHQ-9 summary scores were 6 variables of age, employed or nonemployed, cyclothymic temperament, hyperthymic temperament, anxious temperament, and CATS neglect subscores. Other variables were excluded from the model (adjusted R2=0.401, F = 41.187, p < 0.001). Multicollinearity was denied.
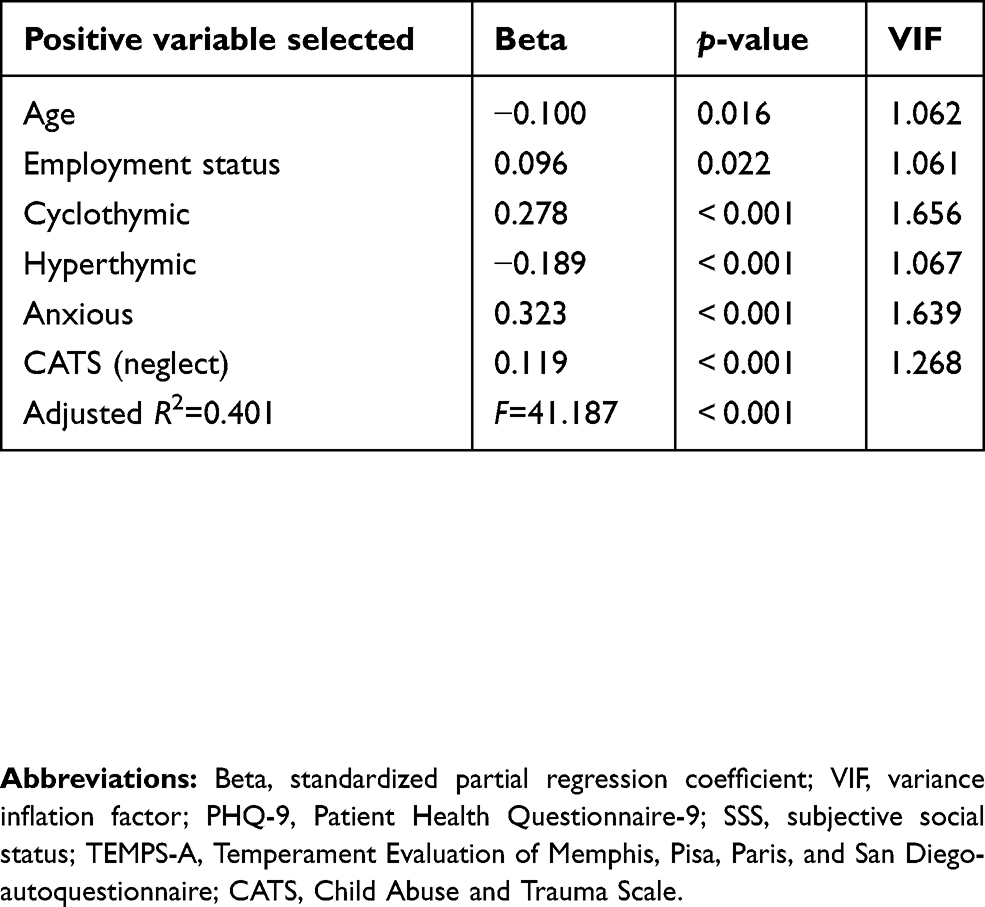 |
Table 2 Results of stepwise multiple regression analysis of PHQ-9 |
Analysis of the structural equation model
In the model, “neglect”, “punishment”, and “sexual abuse” were observed variables, and “childhood abuse” was taken as a latent variable, as shown in Figure 1. Furthermore, PHQ-9, SSS, and the latent variable “TEMPS-A” were included in this path model analyzed by a structural equation model based on maximum likelihood estimation with robust standard errors (Figure 1). The fitness of the model was CFI = 0.961 and RMSEA = 0.057, which indicate an acceptable fit. From the latent variable of childhood abuse to the observed variables, the standardized coefficient of neglect was the maximum value. In the structural equation model of the association between variables, childhood abuse increased SSS scores and had a positive effect on “TEMPS-A”, but had no direct effect on PHQ-9 scores. Although the SSS score had no direct effect on PHQ-9 scores, the SSS score increased “TEMPS-A”.
Regarding indirect effects, childhood abuse showed a significant indirect effect (0.029, p = 0.03) on “TEMPS-A” via SSS, but had no significant indirect effect on PHQ-9 scores via SSS scores (–0.004, p = 0.583). The indirect effect of childhood abuse on PHQ-9 scores via “TEMPS-A” was significant (0.335, p < 0.001). In addition, the indirect effect of “childhood abuse” on PHQ-9 scores via both SSS and “TEMPS-A” was also significantly positive (0.019, p = 0.044). Finally, the SSS had a significant indirect effect on PHQ-9 scores via “TEMPS-A” (0.100, p = 0.011).
In other words, SSS mediates the effects of childhood abuse on affective temperament. Affective temperament mediates the effects of SSS on depressive symptoms. The combination of SSS and affective temperament significantly mediated the effects of childhood abuse on depressive symptoms.
The coefficient of determination (R2) of PHQ-9 scores was 0.429, ie, this model explains 42.9% of the variability in PHQ-9 scores.
Discussion
In this study, we first showed by covariance structure analysis that childhood abuse has an indirect effect on depressive symptoms in adulthood, through its effects on SSS and affective temperament. Previous studies have reported the association between childhood abuse and depressive symptoms in adulthood,1,6,10,17,34 between affective temperament and depressive symptoms in adulthood,4,9–11,17 and between SSS and depressive symptoms in adulthood.20,22 However, no study has analyzed how SSS influences the effects of childhood abuse and affective temperament on adulthood depressive symptoms. It should be noted that our results suggest that SSS may be a mediator of the effects of childhood abuse on affective temperament and depressive symptoms in adulthood. To our knowledge, there have been no studies to date showing the direct association between childhood abuse and SSS in adult volunteers from the community. On the other hand, a previous study reported that OSS is associated with psychological and physical abuse in childhood and affects mental health, general health, and the well-being of adults.23 OSS is moderately associated with SSS, and its effects on depressive symptoms of adults is partially mediated by SSS.22 Therefore, the findings of the effects of OSS, which is closely associated with SSS, on childhood abuse and adult health support the results of this study.22 There is a possibility that the experience of childhood abuse reduces SSS. A recent study reported that developmental trajectories in SSS exist and that SSS changes greatly from adolescence to adulthood in a subset of subjects.35
To the best of our knowledge, no studies have analyzed the association between affective temperament evaluated by TEMPS-A and SSS in adult volunteers from the community. This study is the first to demonstrate that SSS affects affective temperament. SSS is weakly associated with neuroticism,36,37 and neuroticism is moderately associated with depressive, cyclothymic, irritable, and anxious temperaments on the TEMPS-A.38 Therefore, an association between SSS and affective temperament was presumed from these past research results. Affective temperaments are the fundamental states of mood disorders, which are namely subclinical states in the premorbid stages or remission periods between mood episodes.28 We previously reported that affective temperament can be affected by childhood abuse.10,11 In other words, affective temperament is a personality trait that can change during development. Therefore, it is possible that subjects in a low social level receive more stress, and in turn this stress influences affective temperament.
Our earlier studies on nonclinical adult volunteers have demonstrated that childhood abuse has adverse effects on depressive symptoms, which are mediated by affective temperament.10,17 In these previous studies, the effect of neglect was the strongest among the various types of childhood abuse.10,17 Furthermore, in a structural equation model mediated by a latent variable composed of 4 affective temperaments (depressive, cyclothymic, irritable, and anxious), the effect of childhood abuse on adult depressive symptoms was not a direct effect but was completely mediated by affective temperaments.10 The above results were also observed reproducibly in this present study, which analyzed another subject sample. Because the experience of childhood abuse is an event that occurred decades previously, it is unlikely that such an event from the past directly affects a person’s current mood, and this mediation model is considered to be valid. We have also reported similar mediating effects of affective temperament in patients with major depressive disorder and bipolar disorder,4,5,39 indicating that this mediating effect is clinically relevant. However, there is a limitation that the mediation effects by these affective temperaments have not been confirmed in long-term prospective studies. Therefore, it is necessary to verify the hypothesis of this research by future prospective studies.
In the structural equation model of this study, the 4 indirect effects, namely mediation effects, on affective temperament and depressive symptoms were shown: SSS mediated the association between childhood abuse and affective temperament, affective temperament mediated the association between SSS, and depressive symptoms and affective temperament mediated the association between childhood abuse and depressive symptoms. Finally, the association between childhood abuse and depressive symptoms was significantly mediated by the combination of SSS and affective temperament. Among these factors, SSS has never been reported as a mediator. However, a previous study reported that the effect of SSS on subjective health is mediated by self-esteem and neuroticism,37 consistent with some of the results regarding the 4 significant indirect effects in this study. Furthermore, our recent study reported the similar findings that SSS is a mediator in the effects of the quality of parenting in childhood on adulthood depressive symptoms and self-esteem, and that self-esteem further mediates the effects of SSS.24 The results demonstrating that childhood abuse significantly reduces SSS, and lower SSS worsens affective temperament and depressive symptoms, are important points for considering the psychopathology of childhood abuse and depression. Therefore, attention should be paid to the SSS of patients in psychiatric practice.
Next, regarding the significance of our results from the point of view of preventive medicine, the crucial role of psychological resources linking SSS and health has been pointed out.21 Psychological resources are psychological traits that help an individual to endure stress and difficulties, and become the force to have a positive view on life.21 Specifically, self-esteem, optimism, sense of coherence, sense of control, etc., correspond to this, and those with higher OSS or SSS are thought to have a higher level of psychological resources.21 Factors that increase adult SSS include occupational position, satisfaction with their standard of living, education level, household income, and feeling of financial security.40 Factors that cause SSS to decline in children are race/ethnicity, lower household income, and low parent education.35 In childhood, people are protected by their families at home as they grow and develop. Families and other social environments affect children in a variety of ways, and hence the foundation of health throughout life can be considered to be established in childhood. In summary, it is important to increase SSS by working on various social and psychological factors to prevent adulthood depressive symptoms.41 Moreover, SSS is not inherent35 but is formed over time, and is affected by various environmental factors. Improving the childhood environment and preventing childhood abuse are effective towards promoting mental health, such as decreasing depressive symptoms.
There are some limitations to this study. In this research, we investigated data from a self-reported questionnaire, which might be subject to recall bias. As this research was a cross-sectional study and not a prospective survey, a prospective study to follow up subjects who experienced childhood abuse is necessary to confirm our results. Furthermore, as the subjects of this study are adult volunteers from the community, including many healthy subjects, the results may not be generalized to patients with depression.
Conclusions
In this study, childhood abuse showed indirect effects on adulthood depressive symptoms through SSS and affective temperament. To our knowledge, this study is the first to show the mediating role of SSS on adulthood depressive symptoms. SSS scores should receive more attention in psychiatric practice and when considering mental health. In the future, a large-scale prospective study should be performed to confirm that SSS mediates the effects of childhood abuse on the onset of depression.
Acknowledgment
This work was partly supported by a Grant-in-Aid for Scientific Research (No. 16K10194, T. Inoue) from the Japanese Ministry of Education, Culture, Sports, Science and Technology, the Research and Development Grants for Comprehensive Research for Persons with Disabilities from Japan Agency for Medical Research and Development, AMED, and SENSHIN Medical Research Foundation.
Author contributions
MH and TI designed the study and wrote the protocol. MH collected data. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
JM has received personal compensation from Otsuka Pharmaceutical, Eli Lilly, Astellas, and Meiji Yasuda Mental Health Foundation and grants from Pfizer. MI has received personal compensation from Otsuka Pharmaceutical, Pfizer, Eli Lilly, Mitsubishi Tanabe Pharma, Mochida Pharmaceutical, Meiji Seika Pharma, Janssen Pharmaceutical, Takeda Pharmaceutical, MSD, Dainippon Sumitomo Pharma, and Eisai; grants from Otsuka Pharmaceutical, Eli Lilly, Eisai, Shionogi, Takeda Pharmaceutical, MSD, and Pfizer; and is a member of the advisory board of Meiji Seika Pharma. IK has received honoraria from Astellas, Chugai Pharmaceutical, Daiichi Sankyo, Dainippon Sumitomo Pharma, Eisai, Eli Lilly, Janssen Pharmaceutical, Kyowa Hakko Kirin, Meiji Seika Pharma, MSD, Nippon Chemiphar, Novartis Pharma, Ono Pharmaceutical, Otsuka Pharmaceutical, Pfizer, Tanabe Mitsubishi Pharma, Shionogi and Yoshitomiyakuhin, and has received research/grant support from AbbVie GK, Asahi Kasei Pharma, Astellas, Boehringer Ingelheim, Chugai Pharmaceutical, Daiichi Sankyo, Dainippon Sumitomo Pharma, Eisai, Eli Lilly, GlaxoSmithKline, Kyowa Hakko Kirin, Meiji Seika Pharma, MSD, Novartis Pharma, Ono Pharmaceutical, Otsuka Pharmaceutical, Pfizer, Takeda Pharmaceutical, Tanabe Mitsubishi Pharma, Shionogi and Yoshitomiyakuhin, and is a member of the advisory board of Dainippon Sumitomo Pharma and Tanabe Mitsubishi Pharma. TI has received personal fees from Mochida Pharmaceutical, Takeda Pharmaceutical, Eli Lilly, Janssen Pharmaceutical, MSD, and Taisho Toyama Pharmaceutical, Yoshitomiyakuhin, and Daiichi Sankyo; grants from Shionogi, Astellas, Tsumura, and Eisai; and grants and personal fees from Otsuka Pharmaceutical, Dainippon Sumitomo Pharma, Mitsubishi Tanabe Pharma, Kyowa Pharmaceutical Industry, Pfizer, Novartis Pharma, and Meiji Seika Pharma; and is a member of the advisory boards of Pfizer, Novartis Pharma, and Mitsubishi Tanabe Pharma. The authors report no other conflicts of interest in this work.
References
1. Caspi A, Sugden K, Moffitt TE, et al. Influence of life stress on depression: moderation by a polymorphism in the 5-HTT gene. Science. 2003;301:386–389. doi:10.1126/science.1083968
2. Kendler KS, Kuhn J, Prescott CA. The interrelationship of neuroticism, sex, and stressful life events in the prediction of episodes of major depression. Am J Psychiatry. 2004;161:631–636. doi:10.1176/appi.ajp.161.4.631
3. Alloy LB, Abramson LY, Walshaw PD, Keyser J, Gerstein RK. A cognitive vulnerability-stress perspective on bipolar spectrum disorders in a normative adolescent brain, cognitive, and emotional development context. Dev Psychopathol. 2006;18:1055–1103. doi:10.1017/S0954579406060524
4. Toda H, Inoue T, Tsunoda T, et al. The structural equation analysis of childhood abuse, adult stressful life events, and temperaments in major depressive disorders and their influence on refractoriness. Neuropsychiatr Dis Treat. 2015;11:2079–2090. doi:10.2147/NDT.S82236
5. Toda H, Inoue T, Tsunoda T, et al. Affective temperaments play an important role in the relationship between childhood abuse and depressive symptoms in major depressive disorder. Psychiatry Res. 2016;236:142–147. doi:10.1016/j.psychres.2015.12.016
6. Kessler RC, Magee WJ. Childhood adversities and adult depression: basic patterns of association in a US national survey. Psychol Med. 1993;23:679–690. doi:10.1017/S0033291700025460
7. Wise LA, Zierler S, Krieger N, Harlow BL. Adult onset of major depressive disorder in relation to early life violent victimisation: a case-control study. Lancet. 2001;358:881–887.
8. Weich S, Patterson J, Shaw R, Stewart-Brown S. Family relationships in childhood and common psychiatric disorders in later life: systematic review of prospective studies. Br J Psychiatry. 2009;194:392–398. doi:10.1192/bjp.bp.107.049007
9. Matsumoto S, Akiyama T, Tsuda H, et al. Reliability and validity of TEMPS-A in a Japanese non-clinical population: application to unipolar and bipolar depressives. J Affect Disord. 2005;85:85–92. doi:10.1016/j.jad.2003.10.001
10. Nakai Y, Inoue T, Toda H, et al. The influence of childhood abuse, adult stressful life events and temperaments on depressive symptoms in the nonclinical general adult population. J Affect Disord. 2014;158:101–107. doi:10.1016/j.jad.2014.02.004
11. Nakai Y, Inoue T, Chen C, et al. The moderator effects of affective temperaments, childhood abuse and adult stressful life events on depressive symptoms in the nonclinical general adult population. J Affect Disord. 2015;187:203–210. doi:10.1016/j.jad.2015.08.011
12. Pompili M, Venturini P, Lamis DA, et al. Suicide in stroke survivors: epidemiology and prevention. Drugs Aging. 2015;32(1):21–29. doi:10.1007/s40266-014-0233-x
13. Okumura Y, Higuchi T. Cost of depression among adults in Japan. Prim Care Companion CNS Disord. 2011;13:10m01082. doi:10.4088/PCC.10m01072
14. Girardi P, Pompili M, Innamorati M, et al. Duloxetine in acute major depression: review of comparisons to placebo and standard antidepressants using dissimilar methods. Hum Psychopharmacol. 2009;24(3):177–190. doi:10.1002/hup.1005
15. Pompili M, Serafini G, Innamorati M, et al. Agomelatine, a novel intriguing antidepressant option enhancing neuroplasticity: a critical review. World J Biol Psychiatry. 2013;14(6):412–431. doi:10.3109/15622975.2013.765593
16. Inoue T, Izumi T, Koyama T. Strategy of augmentation therapy for refractory depression. In: Okuma T, Inoue Y, Kanba S, editors. Recent Advances in the Research of Affective Disorders in Japan. Amsterdam: Elsevier Science; 2002:147–151.
17. Otsuka A, Takaesu Y, Sato M, et al. Interpersonal sensitivity mediates the effects of child abuse and affective temperaments on depressive symptoms in the general adult population. Neuropsychiatr Dis Treat. 2017;13:2559–2568. doi:10.2147/NDT.S144788
18. Adler NE, Epel ES, Castellazzo G, Ickovics JR. Relationship of subjective and objective social status with psychological and physiological functioning: preliminary data in healthy white women. Health Psychol. 2000;19:586–592. doi:10.1037/0278-6133.19.6.586
19. Ostrove JM, Adler NE, Kuppermann M, Washington AE. Objective and subjective assessments of socioeconomic status and their relationship to self-rated health in an ethnically diverse sample of pregnant women. Health Psychol. 2000;19:613–618.
20. Scott KM, Al-Hamzawi AO, Andrade LH, et al. Associations between subjective social status and DSM-IV mental disorders: results from the World Mental Health surveys. JAMA Psychiatry. 2014;71:1400–1408. doi:10.1001/jamapsychiatry.2014.1337
21. Kanbayashi H. Subjective social status and health: A review from a perspective of status identification study. J Hum Hypertens. 2016;21:59–82. Japan.
22. Hoebel J, Maske UE, Zeeb H, Lampert T. Social inequalities and depressive symptoms in adults: the role of objective and subjective socioeconomic status. PLoS One. 2017;12:e0169764. doi:10.1371/journal.pone.0169764
23. Sheikh MA, Abelsen B, Olsen JA. Differential recall bias, intermediate confounding, and mediation analysis in life course epidemiology: an analytic framework with empirical example. Front Psychol. 2016;7:1828. doi:10.3389/fpsyg.2016.01828
24. Hayashida T, Higashiyama M, Sakuta K, et al. Subjective social status via mediation of childhood parenting is associated with adulthood depression in non-clinical adult volunteers. Psychiatry Res. 2019;274:352–357. doi:10.1016/j.psychres.2019.02.061
25. Kanai Y, Takaesu Y, Nakai Y, et al. The influence of childhood abuse, adult life events, and affective temperaments on the well-being if the general, nonclinical adult population. Neuropsychiatr Dis Treat. 2016;12:823–832.
26. Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of prime-md the PHQ primary care study. JAMA. 1999;282:1737–1744. doi:10.1001/jama.282.18.1737
27. Muramatsu K, Miyaoka H, Kamijima K, et al. The patient health questionnaire, Japanese version: validity according to the mini-international neuropsychiatric interview-plus. Psychol Rep. 2007;101:952–960. doi:10.2466/pr0.101.3.952-960
28. Akiskal HS, Akiskal KK, Haykal RF, Manning JS, Connor PD. TEMPS-A: progress towards validation of a self-rated clinical version of the Temperament Evaluation of the Memphis, Pisa, Paris, and San Diego autoquestionnaire. J Affect Disord. 2005;85:3–16. doi:10.1016/j.jad.2004.12.001
29. Akiyama T, Tsuda H, Matsumoto S, et al. Cyclothymia and typus melancholicus: empirical study on personality character of mood disorder. Seishin Shinkeigaku Zasshi. 2003;105:533–543. Japan.
30. Sanders B, Becker-Lausen E. The measurement of psychological maltreatment: early data on the Child Abuse and Trauma Scale. Child Abuse Negl. 1995;19:315–323. doi:10.1016/S0145-2134(94)00131-6
31. Tanabe H, Ozawa S, Goto K. Psychometric properties of the Japanese version of the Child Abuse and Trauma Scale (CATS).
32. Tsuno K, Kawakami N, Tsutsumi A, et al. Socioeconomic determinants of bullying in the workplace: a national representative sample in japan. PLoS One. 2015;10:e0119435. doi:10.1371/journal.pone.0119435
33. Schermelleh-Engel K, Moosbrugger H, Müller H. Evaluating the fit of structural equation models: tests of significance and descriptive goodness-of-fit measures. MPR Online. 2003;8:23–74.
34. Hayashi Y, Okamoto Y, Takagaki K, et al. Direct and indirect influences of childhood abuse on depression symptoms in patients with major depressive disorder. BMC Psychiatry. 2015;15:244. doi:10.1186/s12888-015-0636-1
35. Goodman E, Maxwell S, Malspeis S, Adler N. Developmental trajectories of subjective social status. Pediatrics. 2015;136:e633–640. doi:10.1542/peds.2015-0573
36. Alfonsi G, Conway M, Pushkar D. The lower subjective social status of neurotic individuals: multiple pathways through occupational prestige, income, and illness. J Pers. 2011;79:619–642. doi:10.1111/j.1467-6494.2011.00684.x
37. Kan C, Kawakami N, Karasawa M, et al. Psychological resources as mediators of the association between social class and health: comparative findings from Japan and the USA. Int J Behav Med. 2014;21:53–65. doi:10.1007/s12529-012-9249-y
38. Gonda X, Fountoulakis KN, Juhasz G, et al. Association of the s allele of the 5-HTTLPR with neuroticism-related traits and temperaments in a psychiatrically healthy population. Eur Arch Psychiatry Clin Neurosci. 2009;259:106–113. doi:10.1007/s00406-008-0842-7
39. Toda H, Inoue T, Tanichi M, et al. Affective temperaments play an important role in the relationship between child abuse and the diagnosis of bipolar disorder. Psychiatry Res. 2018;262:13–19. doi:10.1016/j.psychres.2018.01.040
40. Singh-Manoux A, Adler NE, Marmot MG. Subjective social status: its determinants and its association with measures of ill-health in the Whitehall II study. Soc Sci Med. 2003;56:1321–1333. doi:10.1016/S0277-9536(02)00131-4
41. Zvolensky MJ, Paulus DJ, Bakhshaie J, et al. Anxiety sensitivity and age: roles in understanding subjective social status among low income adult latinos in primary care. J Immigr Minor Health. 2018;20:632–640. doi:10.1007/s10903-017-0623-3
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.