")
Back to Journals » Research and Reports in Urology » Volume 11
Complete ureter avulsion causing a long defect as a complication of posterior spine fusion: a rare case treated with nonrobotic laparoscopic repair
Authors Lai CJ , Chang MY, Huang PC, Chu YC
Received 30 September 2018
Accepted for publication 12 December 2018
Published 17 January 2019 Volume 2019:11 Pages 15—19
DOI https://doi.org/10.2147/RRU.S189259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jan Colli

Chien-Jung Lai,1 Ming-Yuan Chang,2 Po-Chien Huang,1 Yuan-Chung Chu1
1Division of Urology, Department of Surgery, Min-Sheng General Hospital, Taoyuan, Taiwan; 2Division of Neurosurgery, Department of Surgery, Min-Sheng General Hospital, Taoyuan, Taiwan
Purpose: Ureter avulsion, a challenging urologic complication, has been rarely found in lumbar spine surgeries. Once ignored, the leaked urine usually leads to significant morbidity and also makes further repair more difficult. We present an unusual ureter injury causing a long defect which occurred in posterior spine fusion; immediate repair was performed with minimal invasion.
Case presentation: A 61-year-old female was receiving microscopic spine fusion (transforaminal lumbar interbody fusion) for her L3–L5 spondylosis. Ureter avulsion with one 3-cm defect occurred unexpectedly. We confirmed urine extravasation promptly, and performed end-to-end ureteroureterostomy with laparoscopy. Retrograde double-J stenting was indwelled. Her postoperative condition was uneventful.
Conclusion: This rare case with good outcome highlights the importance of early diagnosis and immediate repair for complete ureter avulsion. We prove that reanastomosis for ureter loss as much as 3 cm is feasible with laparoscopy in regional hospitals where a robot is not available. To deal with large gaps between stumps, adequate kidney mobilization is required before anastomosis.
Keywords: posterior spine fusion, iatrogenic ureter injury, realignment, end-to-end ureteroureterostomy, urine extravasation
Introduction
Iatrogenic ureter injury has been mostly found in gynecologic surgeries, and its extent could be varied. The damage ranges from ligation to compression, partial or complete transection, thermal injury, and ischemia from devascularization;1 different operations should be utilized to repair injury based on its grade and location. However, even with profound injury, ureter injury does not cause significant symptoms initially; thus, diagnosis is usually delayed. It has been verified that delayed diagnosis results in higher complications, including fistula, urinoma, infection, etc.2 Prolonged hospital stay and increased nephrectomy numbers are also proved.3
It was seldom reported previously that spine surgeries caused ureter injury. Since spine fusion has gained more popularity recently for spine interbody stability, some complications were encountered, such as vascular injury, ureteric injury, and nerve damage.4,5 Unlike great vessels, injured ureters usually cause obscure symptoms postoperatively. Endoscopic stenting (double-J) or percutaneous nephrostomy can be performed easily for most injured ureters; however, nephrectomy was also reported after ureteroureterostomy failure.3,6
Case report
A 61-year-old woman had suffered from worsening neurogenic claudication for 1 year and low back pain with radiation to the legs. L3–L4–L5 spondylolisthesis was diagnosed with magnetic resonance imaging, which revealed spinal stenosis between L4/5 making L5 bilateral nerve root compression, more severe on the left side (Figure 1). Microscopic transforaminal lumbar interbody fusion (TLIF) with cages had been discussed and planned. During the operation, L3/4/5 TLIF was performed through the left side under microscopy after paraspinal muscle dissection. A Kerrison rongeurs was then applied for L3/4 and L4/5 left-side laminectomy. However, one 3-cm ureter segment was clipped out unexpectedly (Figure 2). We confirmed urine extravasation with an intraoperative portal X-ray taken 5 min after contrast medium injection, which demonstrated that urine leaked from the right upper ureter (Figure 3).
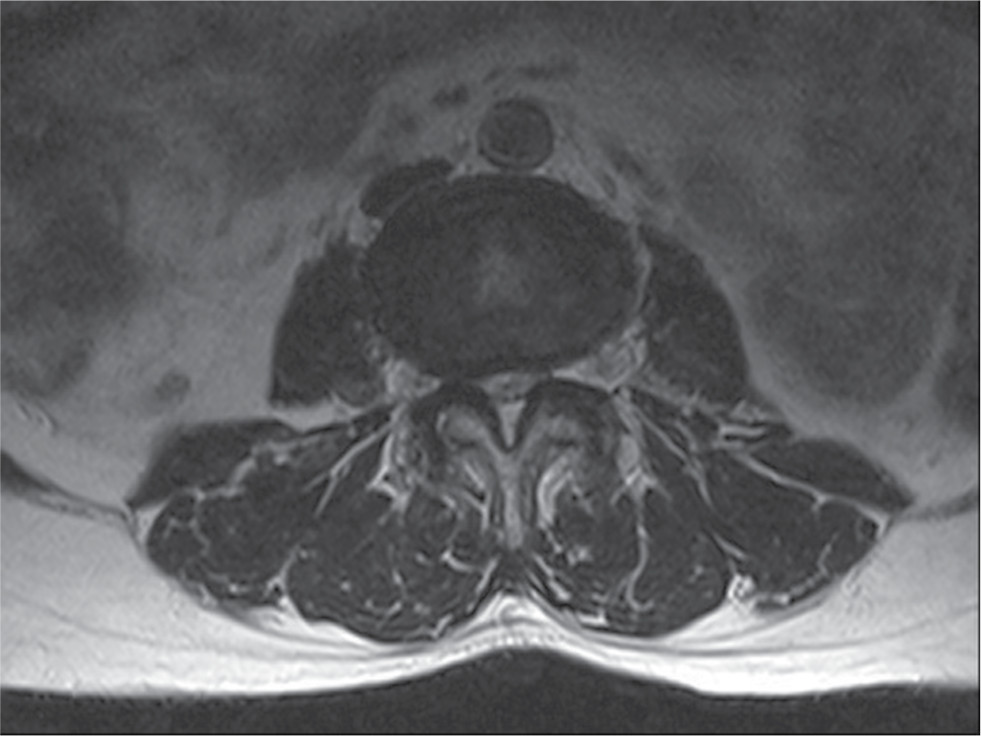 | Figure 1 Preoperative magnetic resonance image showing spinal stenosis between L4/5, making L5 bilateral nerve root compression, which was more severe on the left side. |
 | Figure 2 Clipped ureter segment, length 3 cm. |
 | Figure 3 Urine extravasation from the right upper ureter demonstrated on intraoperative portal X-ray image taken 5 min after contrast medium injection. |
Transperitoneal laparoscopic ureter realignment was attempted. Prior to repair, we indwelled a retrograde ureter catheter with ureteroscopy to make the distal ureter stump easier to recognize. One 10-mm periumbilical trocar was set up for the camera, followed by two working ports (10 and 5 mm) created along the right-side mid-clavicular line. With pneumoperitoneum and dissection, the avulsed two ureter stumps were found successfully. To reduce the gap between the stumps, we performed extensive mobilization of the right kidney, in which dissection was carried out along the kidney low pole, lateral side, hepatic flexure, and subhepatic area, with preservation of peri-renal fat tissue, and great care of hilar vessels. Both stumps were trimmed out of the devitalized ureter tissue and spatulated well. The end-to-end anastomosis was conducted with care to minimize handling of the ureter adventitia; interrupted sutures were performed meticulously with 3–0 Vicryl in four stitches (Figure 4). After this procedure, one retrograde double-J stent was placed under ureteroscopy, and a Jackson–Pratt drain was also left next to the anastomosis site.
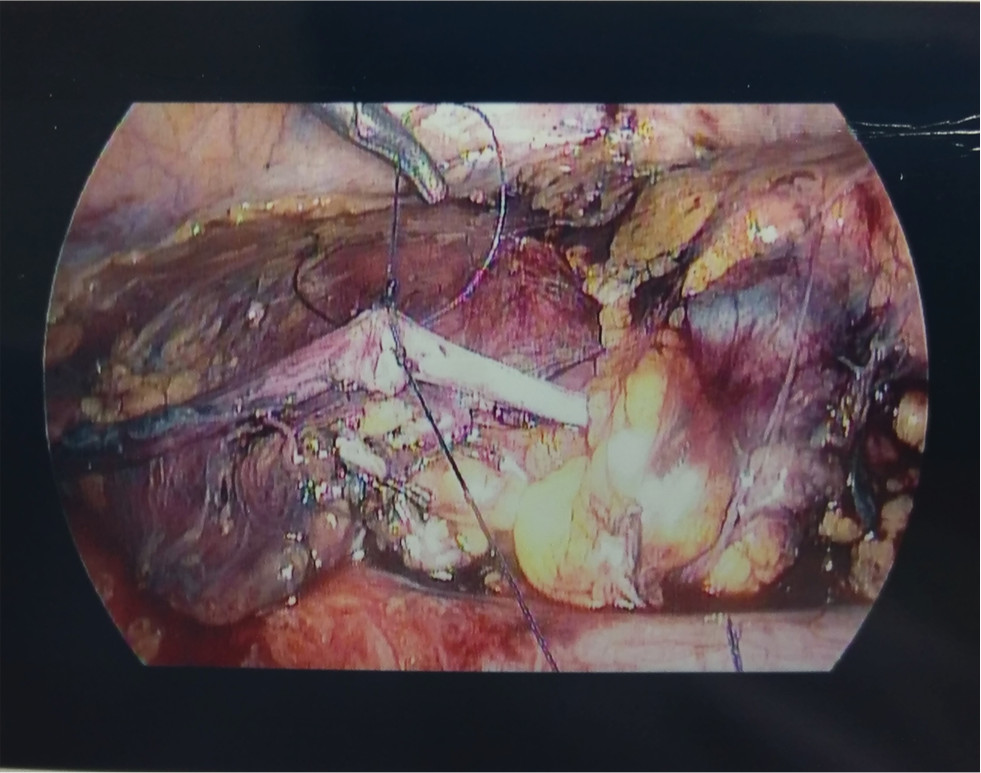 | Figure 4 The first stitch of end-to-end anamostosis was accomplished with laparoscopy. In total, four stitches of interrupted sutures were conducted. |
In spite of the patient’s uneventful postoperative course, she received 14 days of parenteral ciprofloxacin to prevent adjacent spine infection. The Foley catheter was removed on the seventh postoperative day; she was discharged on the 15th day. The Jackson–Pratt drain was removed at the outpatient clinic 3 weeks after ureter repair, and the double-J was also removed 2 months after the anastomosis. However, excruciating back pain and vomiting developed, and hydronephrosis and an elevated creatinine level (increased from 0.67 to 1.87 mg/dL) were noted. Ureteroscopy revealed a short segment (<1 cm) of ureter stricture at the suture site (Figure 5); therefore, this patient received long-term double-J stenting for ureter stricture. The associated flank pain and vomiting subsided once she received restenting in the repaired ureter.
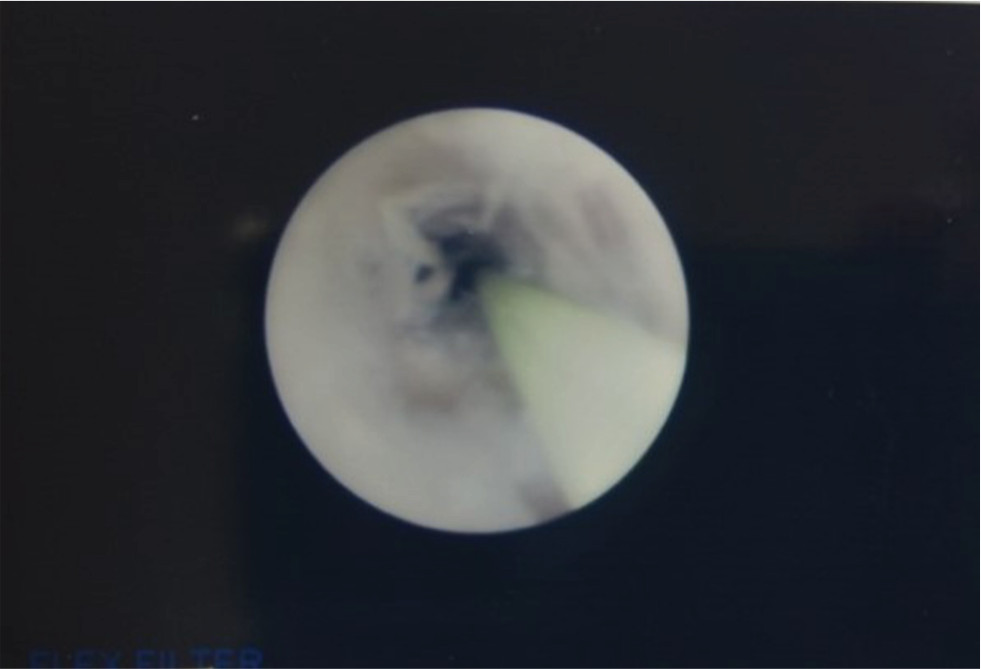 | Figure 5 Two months after anamostosis, ureter stricture (<1 cm) was revealed under ureteroscopy at the repair site. |
Discussion
Other than gynecologic and colorectal surgeries, ureter transection or avulsion also occurs in other cases, such as ureteroscopy and other retroperitoneal surgeries, where minimally invasive surgery is widely used. Ureter injury associated with a lumbar spine procedure has only been published in sporadic case reports; various approach methods were reported, including anterior exposure and oblique or posterior spine interbody fusion.6–10Among them, anterior lumbar interbody fusion and TLIF procedures combined with posterior instrumentation both improve the construct stability of intact spinal motion segments significantly, and do not yield to statistical difference.11 We chose TLIF for the fewer complications of vascular injury and damage on the spine musculature and neural structure.5 In addition, it is assumed that revision procedures are more susceptible to ureter injury because of worse adhesion. In a review of 25 revision case, two ureter injuries (8%) were found; this incidence is much greater than the 0.3%–0.5% in other anterior lumbar spine surgeries.6 Most of the cases received adequate ureter repair immediately or a couple of days later once ureter injury was confirmed. However, kidney loss was also reported.
Since ureters are found at higher risk of minimally invasive lumbar spine surgeries, a dual-phase computed tomography (CT) scan was examined to assess ureters preoperatively.12 In their preoperative CT images, 90.4% of ureters were classified as anatomically close to the surgical corridor for oblique lateral interbody fusion, and 16% are at risk of injury during extreme lateral interbody fusion. In addition, ureters could be damaged inadvertently with violent use of thread pins or pedicle screws, even if being wrapped in fat and peritoneum.9,12 Systemic disease, like rheumatoid arthritis, can alter ureter locations unpredictably. To prevent ureter injury, ureter stenting prior to operations has been largely acknowledged as the most effective method.1,2,6 However, this could be only feasible for selected cases who have higher possibility of ureter injury as a result of intractable disease. Since ureter injury was hardly predictable in our case, we did not indwell the ureter stent beforehand.
Both American Urological Association and European Association of Urology guidelines recommend complete intravenous urography as the best imaging method to confirm the suspicion of ureter damage.1,2 There are insufficient data to recommend a CT scan, but it appears to be accurate for delayed diagnosis of ureteric injury with signs of contrast medium extravasation, ascites, hydronephrosis, and urinoma.2 In our case, an intraoperative X-ray image taken with the use of contrast medium was utilized as an alternative for excretory urography, followed by retrograde ureteroscopy. We proposed that this instant imaging taken intraoperatively can be used commonly if there is any suspicion of ureter avulsion which needs urgent realignment.
To repair injured ureters, different operations should be adopted according to injury grade and location. EAU and AUA guidelines recommended that grade 2 or grade 3 ureter injury (partial injury or laceration only) can be repaired by primary closure over stents. Most minor injuries such as perforations could be treated well with only endoscopic stenting.12 For complete avulsion (grade 4 and 5) above iliac vessels, ureteroureterostomy should be performed over a stent,2,13,14 whereas ureter reimplantation should more often be applied for distal ureter injury happening during gynecologic surgeries.2 It has been recommended that immediate recognition and repair of ureter convulsion allow for better results and fewer complications.2 In most cases of late diagnosis, the treatment usually started with percutaneous drainage.15 Patients usually suffered from flank pain or vomiting; a longer hospital stay would be required.3 Besides, ureter tissue becomes more fragile in urinoma following urine leak, which also increases the challenge to further repair. Therefore, nephrectomy was chosen in some cases after reanastomosis failed.
To optimize the anastomosis, general principles must be taken: 1) careful ureter mobilization; 2) debridement of devitalized tissue; 3) mucosa to mucosa, spatulated, tension-free, and watertight anastomosis; 4) ureter drainage (usually with an internal double-J); and 5) isolation of the anastomosis from associated injury.1 Given the large ureter loss in our case, extensive kidney mobilization is the most determining step to approximate the two ureter stumps and best reduce the tension. This end-to-end anastomosis took 3 h, only causing minimal blood loss (<50 mL). Our case emphasizes the importance of awareness and early diagnosis when ureter injury occurs. However, ureter stricture develops when ischemic ureters heal from scar tissue, often from extensive adventitial dissection, radiation, or blast injury.2 In our case, the high tension of the repaired ureter and devascularization associated with ureter dissection aggravated the scar formation despite our best efforts to reduce the tension. Fortunately, like most of the cases which are short and diagnosed early, our case’s ureter stricture was managed successfully with an endourological procedure. Open excision and repair can be preserved for endoscopic failure, late stricture discovery, overly dense or long cases, or radiation-induced cases.2 Laparoscopic ureter repair has been proven feasible, safe, and effective for damage occurring during gynecologic surgeries.16 Moreover, robotic surgery was also applied for difficult repair in complete ureter avulsion. An evidence-based review on this technique by Tracey et al17 proved the high success rate and faster recovery. However, ureter repair for a large defect with laparoscopy has never been reported. We presented the first case of intraoperative laparoscopic ureter reanastomosis for a complete avulsion causing ureter loss of 3 cm. This certifies that primary realignment is feasible for intractable cases with minimal invasiveness in regional hospitals where robots are not available.
Conclusion
Despite the low incidence rate, ureter injury possibly happens during posterior spine fusion. Neurosurgeons and urologists both need to keep aware of this complication. An intraoperative X-ray scan with contrast medium injected is a quick tool to ensure urine extravasation. To deal with ureter avulsion, immediate recognition and adequate kidney mobilization are both determining steps to achieve laparoscopic reanastomosis.
Ethic approval
Ethical approval was given by Min-Sheng General Hospital ethics committee for reporting this case.
Consent
We have obtained a written informed consent from this patient for all of the anonymized information to be published.
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Bryk DJ, Zhao LC. Guideline of guidelines: a review of urological trauma guidelines. BJU Int. 2016;117(2):226–234. | ||
Brandes S, Coburn M, Armenakas N, McAninch J. Diagnosis and management of ureteric injury: an evidence-based analysis. BJU Int. 2004;94(3):277–289. | ||
Kunkle DA, Kansas BT, Pathak A, Goldberg AJ, Mydlo JH. Delayed diagnosis of traumatic ureteral injuries. J Urol. 2006;176(6 Pt 1):2503–2507. | ||
Quillo-Olvera J, Lin GX, Jo HJ, Kim JS. Complications on minimally invasive oblique lumbar interbody fusion at L2-L5 levels: a review of the literature and surgical strategies. Ann Transl Med. 2018;6(6):101. | ||
Mobbs RJ, Phan K, Daly D, Rao PJ, Lennox A. Approach-related complications of anterior lumbar interbody fusion: results of a combined spine and vascular surgical team. Global Spine J. 2016;6(2):147–154. | ||
Flouzat-Lachaniette CH, Delblond W, Poignard A, Allain J. Analysis of intraoperative difficulties and management of operative complications in revision anterior exposure of the lumbar spine: a report of 25 consecutive cases. Eur Spine J. 2013;22(4):213:766–774. | ||
De Quintana-Schmidt C, Clavel-Laria P, Bartumeus-Jené F. Ureteral injury after posterior lumbar surgery. Case report. Neurocirugia. 2011;22(2):162–166. | ||
Lee HJ, Kim JS, Ryu KS, Park CK. Ureter injury as a complication of oblique lumbar interbody fusion. World Neurosurg. 2017;102:693.e7–693.e14. | ||
Kubota G, Orita S, Umimura T, Takahashi K, Ohtori S. Insidious intraoperative ureteral injury as a complication in oblique lumbar interbody fusion surgery: a case report. BMC Res Note. 2017;10(1):193. | ||
Anand N, Baron EM. Urological injury as a complication of the transpsoas approach for discectomy and interbody fusion. J Neurosurg Spine. 2013;152(1):18–23. | ||
Ploumis A, Wu C, Fischer G, et al. Biomechanical comparison of anterior lumbar interbody fusion and transforaminal lumbar interbody fusion. J Spinal Disord Tech. 2008;21(2):120–125. | ||
Fujibayashi S, Otsuki B, Kimura H, Tanida S, Masamoto K, Matsuda S. Preoperative assessment of the ureter with dual-phase contrast-enhanced computed tomography for lateral lumbar interbody fusion procedures. J Orthop Sci. 2017;22(3):420–424. | ||
Morey AF, Brandes S, Dugi DD, et al. Urotrauma: AUA guideline. J Urol. 2014;192(2):327–335. | ||
Summerton DJ, Kitrey ND, Lumen N, Serafetinidis E, Djakovic N, European Association of Urology. EAU guidelines on iatrogenic trauma. Eur Urol. 2012;62(4):628–639. | ||
Fomekong E, Pierrard J, Danse E, Tombal B, Raftopoulos C. An unusual case of ureteral perforation in minimally invasive pedicle screw instrumentation: case report and review of the literature. World Neurosurg. 2018;111:28–35. | ||
De Cicco C, Schonman R, Craessaerts M, van Cleynenbreugel B, Ussia A, Koninckx PR. Laparoscopic management of ureteral lesions in gynecology. Fertil Steril. 2009;92(4):1424–1427. | ||
Tracey AT, Eun DD, Stifelman MD, et al. Robotic-assisted laparoscopic repair of ureteral injury: an evidence-based review of techniques and outcomes. Minerva Urol Nefrol. 2018;70:231–241. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.