")
Back to Journals » OncoTargets and Therapy » Volume 14
Complete Response to Pembrolizumab in Advanced Colon Cancer Harboring Somatic POLE F367S Mutation with Microsatellite Stability Status: A Case Study
Received 7 January 2021
Accepted for publication 24 February 2021
Published 9 March 2021 Volume 2021:14 Pages 1791—1796
DOI https://doi.org/10.2147/OTT.S300987
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Gaetano Romano
Jianxin Chen,1 Haizhou Lou2
1Department of Medical Oncology, Quzhou People’s Hospital, Quzhou, 324000, Zhejiang, People’s Republic of China; 2Department of Oncology, Sir Run Run Shaw Hospital Zhejiang University School of Medicine, Hangzhou, 310016, Zhejiang, People’s Republic of China
Correspondence: Haizhou Lou
Department of Oncology, Sir Run Run Shaw Hospital Zhejiang University School of Medicine, Zhejiang, 310016, People’s Republic of China
Email [email protected]
Background: Polymerase epsilon (POLE) mutations are considered as one of the most potential and promising biomarkers for immune checkpoint inhibitors (ICIs) in patients with colorectal cancer. However, the treatment of ICIs sometimes also resulted in unsatisfactory results in patients with POLE mutations, which revealed that not all mutations on POLE contribute to tumor regression in colorectal cancer.
Case Presentation: We herein reported a case in which the patient with advanced colon cancer harboring somatic POLE F367S mutation, along with microsatellite stability status, has achieved efficacy of complete response to the programmed cell death 1 (PD-1) receptor inhibitor pembrolizumab, as well as a progression-free survival more than 49 months, and still in extension.
Conclusion: Somatic POLE F367S mutation might be presented as a sensitive predictor to pembrolizumab in patients with colon cancer.
Keywords: POLE mutation, colon cancer, pembrolizumab, complete response
Introduction
Colorectal cancer represents one of the most leading causes of cancer death worldwide.1 In recent decades, molecularly driven based treatment has been recommended as one of the standard strategies in patients with advanced or metastatic colorectal cancer. Specifically, monoclonal antibodies or small molecular agents, which target epidermal growth factor receptor (EGFR), vascular endothelial growth factor (VEGF), B-raf, and microsatellite instability-high (MSI-H)/deficient mismatch repair protein (dMMR), have been frequently prescribed in clinical practice for patients with metastatic disease.2 Targeted medicine, as well as new targets, has been considered as research hotspots, with much attention being paid to. As a novel target, polymerase epsilon (POLE) encodes the exonuclease subunit of polymerase epsilon with 2,286 amino acids, has been deemed as a potential biomarker responding to the treatment of immune checkpoint inhibitors (ICIs).3 However, the treatment of ICIs sometimes also resulted in unsatisfactory outcomes in patients with POLE mutations, which revealed that not all mutations on POLE sites contribute to tumor regression by ICIs in colorectal cancer.4 Herein, we presented a case in which the patient with advanced colon cancer harboring somatic POLE F367S mutation, along with microsatellite stability status, has achieved complete response to the programmed cell death 1 (PD-1) receptor inhibitor pembrolizumab. The patient has achieved a progression-free survival more than 49 months, and still in extension. We also systematically reviewed and summarized reported POLE mutation sites, as well as clinical response to ICIs with published literatures. We hope the presentation of the case and the summary of POLE mutations would provide some clinical thought for physicians.
Case Presentation
A 29-year-old Chinese man was admitted to our hospital on April 5, 2016 with repeated diarrhea and bloody stools for 6 months. The patient denied smoking, alcohol, or any other medical or family history. His abdomen CT presented a mass (7.8x11.4x8.8 cm) surrounding the descending colon, along with stenosis. There were no lesions on the lungs or liver observed with CT scans. Based on that, he subsequently received radical resection of the descending colon tumor, as well as ileostomy in our hospital on April 11, 2016. Pathological findings suggested that the tumor was a moderately differentiated adenocarcinoma, without any metastasis to regional lymph nodes (pT3N0M0, stage IIA). One month after the surgery on May 10, 2016, his postoperative chemotherapy started with the regimen XELOX (oxaliplatin 130 mg/m2, on day 1, and oral capecitabine 1,000 mg/m2 twice a day, from day 1 to 14, every 21 days). From then on, he received a regular abdomen CT scan every two to three cycles at follow-up visits. However, after two cycles of chemotherapy on June 23, 2016, his abdomen CT scan revealed multiple emerging lesions on mesentery near anastomosis (largest one sized at 2.8x2.3 cm, Figure 1A). In consideration that the recurrence possibly had happened before adjuvant chemotherapy, we gave another two cycles of XELOX to identify the response of the emerging tumors. On September 20, 2016, his repeated abdomen CT suggested enlargement of the lesions on mesentery (largest one sized as 4.5x4.3 cm, Figure 1B), invaded to left psoas major and iliopsoas muscle. Based on the imaging findings, progression disease was considered according to the criteria of RECIST (Response Evaluation Criteria in Solid Tumors, RECIST) version 1.1. Based on that, the regimen of FOLFIRI (irinotecan 180 mg/m2 on day 1, leucovorin 200 mg/m2 on day 1, fluorouracil 2,600 mg/m2 continuous infusion over 24 hours on day 1, every 14 days) was administered as further line palliative treatment. In addition, whole exome sequencing (WES) with next generation sequencing (NGS) using tissue and plasma sample was conducted to search potentially available mutations. After two cycles′ exposure of regimen FOLFIRI, the patient complained of pain on his left waist. Local ultrasound findings revealed invasion on the left psoas major muscle. Although without any severe adverse events observed during the chemotherapy, he refused to receive chemotherapeutics any more. The outcomes of WES suggested somatic POLE F367S mutation by frequency as 29% in tumor cells, and 4% in plasma (Figure 2). In addition, the WES also revealed microsatellite stability status (MSS), without any mutations on RAS, RAF, or Her-2. As salvage treatment, the patient received monotherapy with pembrolizumab (2 mg/kg) from November 1, 2016. Surprisingly, repeated abdomen CT scans on January 3, 2017 suggested dramatic regression of the lesions on the mesentery, which was evaluated as partial response according to the criteria of RECIST version 1.1 (Figure 1C). From then on, he had received mono-immunotherapy with pembrolizumab up to 24 months. On May 5, 2018, the efficacy was evaluated as complete response based on the absence of enhancement of striped lesion from abdomen CT scans (Figure 1G). He stopped the treatment in October, 2018 because of the completion of a 2 years course. There was no immune-related adverse event observed during the whole treatment. Tumor markers including CEA and CA19-9 varied in the normal range during the whole treatment. Abdomen CT scans during the whole treatment and follow-up are presented in Figure 1.
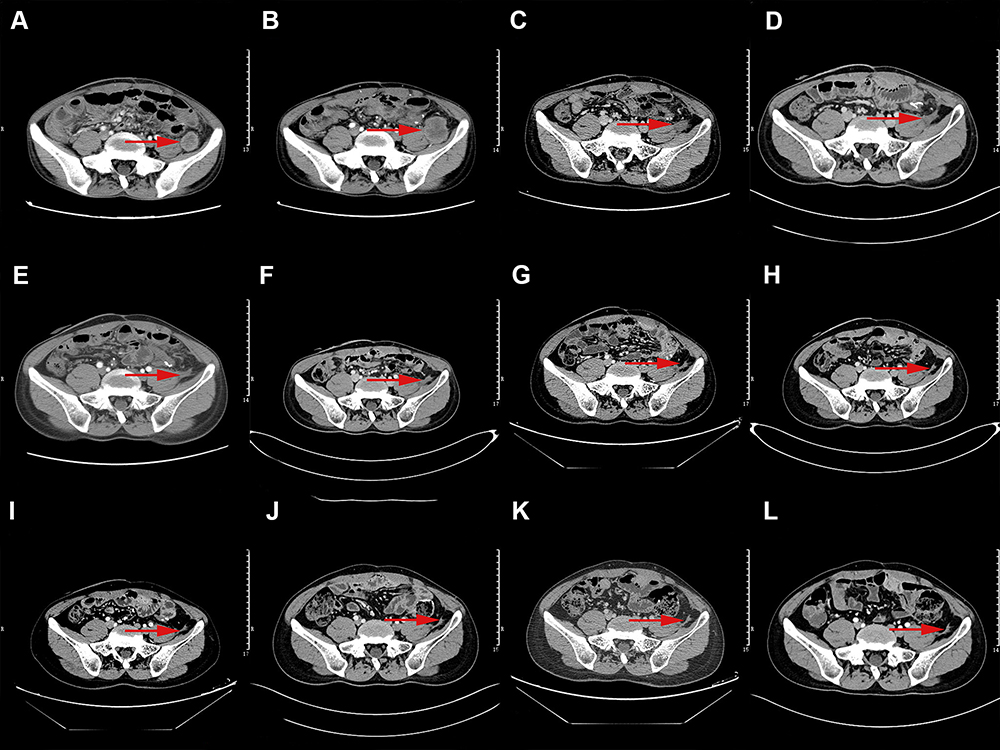 |
Figure 1 Abdomen CT scans showed the metastatic lesions on mesentery (red arrows for the target lesion). (A) June 23, 2016; (B) September 20, 2016; (C) January 3, 2017; (D) March 21, 2017; (E) June 27, 2017; (F) September 26, 2017; (G) May 5, 2018; (H) December 4, 2018; (I) April 1, 2019; (J) October 15, 2019; (K) March 30, 2020; (L) August 29, 2020. |
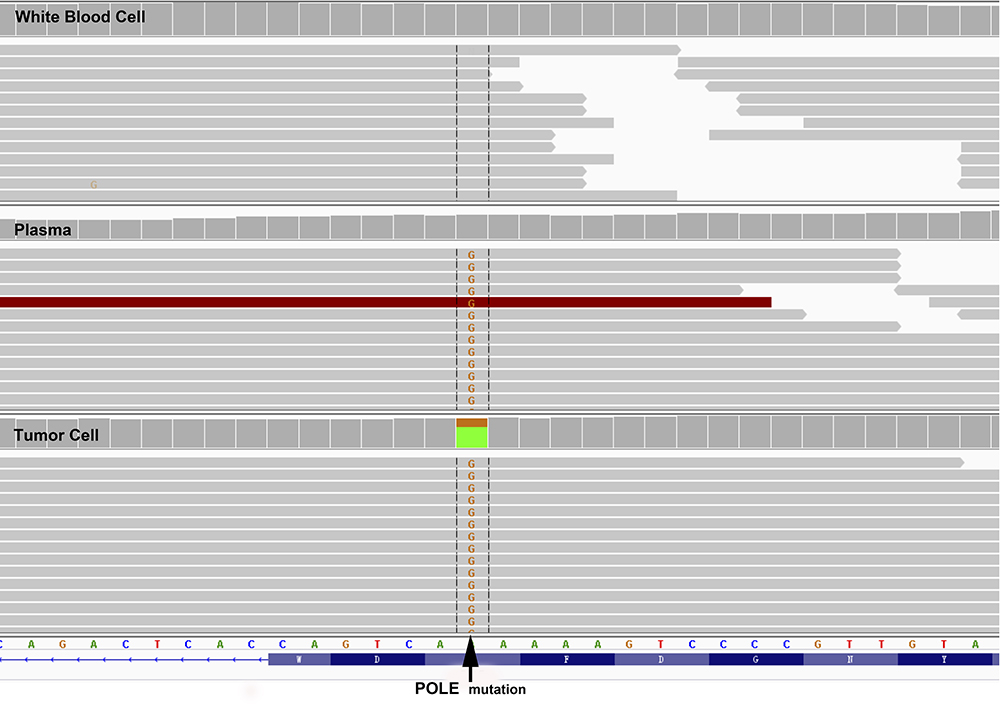 |
Figure 2 Integrative genomics viewer (IGV) screenshots displayed the chimeric reads from targeted sequencing, somatic POLE F367S mutation by frequency as 29% in tumor cells, 4% in plasma, and 0% in white blood cells. |
Discussion
We herein reported a case of a male patient with recurrent colon cancer localized on mesentery, invading to left psoas major and iliopsoas muscle. Based on the somatic POLE F367S mutation detected by WES, he received monotherapy of pembrolizumab as further line treatment. As a result, he achieved complete response of disease, with PFS as 49 months, and still in extension. To our knowledge, this is the first case reporting complete response to pembrolizumab in POLE F367S mutated advanced colon cancer, being the best responder to ICIs in advanced colorectal cancer.
The mutation of POLE exonuclease domain, detected in 6–12% of endometrial cancers,5,6 1–2% of colorectal cancers,7,8 and less than 1% in gastric, breast, and brain cancer,9,10 has emerged as one of the most promising candidate biomarkers. POLE encodes the catalytic subunit of DNA polymerase epsilon, which replicates the leading DNA strand before cell division. The pathogenic mutation of POLE leads to tumor ultra-mutation, with a significantly high burden of tumor mutations, which has been identified as one of the efficacy predictors to ICIs.11,12
POLE mutations in patients with colorectal cancer present distinct clinical characteristics, including younger age, a greater proportion of males than females, diagnosis at an earlier stage, as well as significant increasing tumor mutation burden (TMB).8,13 However, owing to its low frequency, there were limited prospective, controlled, clinical trials designed to evaluate the efficacy of ICIs in colorectal cancer patients harboring POLE mutations. Instead of that, several retrospective researches and case studies have reported the efficacy of ICIs in colorectal patients with POLE mutations.4,7,14–16 However, there still remain inconsistently clinical outcomes on response to ICIs among different POLE mutations in colorectal disease.4,17 In the present study, the sensitive mutation was somatic POLE F367S mutation, which has been reported in basic research.9,10,17 It was reported that, phenylalanine residues of the sequence alteration in POLE, F367S, is highly conserved in organisms including human, mouse, S. cerevisiae, and S. pombe,17 which suggested that F367S is dysfunctional and pathogenic.18 In other words, the F367S mutation found in the POLE gene encodes the POL epsilon catalytic subunit, which includes the proofreading domain. However, there was no clinical evidence to support the efficacy to ICIs treatment for POLE F367S mutation. Hence, the presentation of the present study may be considered as a clinical supplement for basic research, though need further confirmation in a larger population. In addition, we systematically reviewed published literature, and summarized POLE mutations, associated with efficacy to ICIs in patients with colorectal cancer (Table 1). We hope the summary of the mutations would provide suggestions in clinical practice.
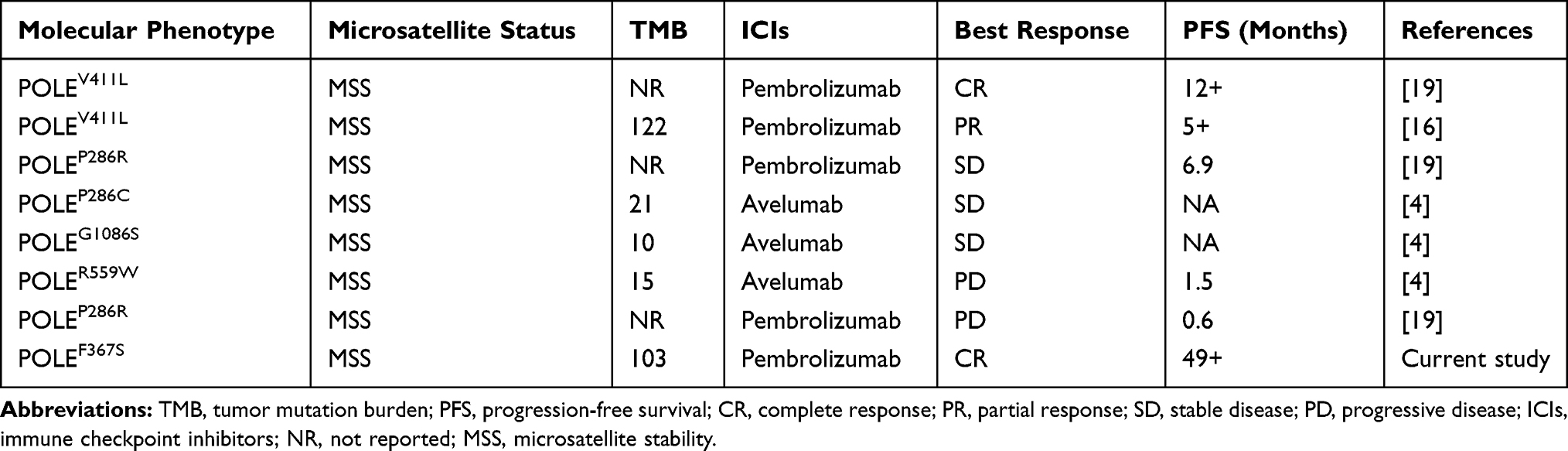 |
Table 1 Molecular Phenotypes of POLE Mutations and Response to ICIs in Literatures of Patients with Colorectal Cancer |
As presented in Table 1, there was a difference on response status in patients with POLE mutations. Although without certain conclusions, there might be several possible reasons addressed for that. Firstly, different mutations might result in different outcomes. POLEV411L mutation was more common in responders according to published literature, which was considered as a hotspot for POLE mutations.4,16,19,20 Moreover, in the present case, POLEF367S mutation might also come to be another alternative hotspot. Pathogenic POLE mutations on exonuclease domain might be more likely to achieve remission status of tumor. Besides, higher TMB from POLE mutations may also contribute to response to ICIs, which has been reached as consensus. As presented in Table 1, higher TMB usually resulted in satisfactory outcomes. In addition, in patients with POLE mutations, responders to ICIs had significantly higher densities of PD-1-expressing CD8+ TILs, compared to non-responders according to a retrospective study (P=0.0007),19 which was not detected in the present case. However, with the limited sample (n=5), the speculative conclusion should be approached modestly.
In conclusion, we reported a case in which the patient with advanced colon cancer harboring somatic POLE F367S mutation has achieved efficacy of complete response to pembrolizumab, as well as a PFS more than 49 months, and still in extension. We considered that somatic POLE F367S mutation might be presented as a sensitive predictor to pembrolizumab in patients with colon cancer.
Data Sharing Statement
All data generated or analyzed during this study are included in this article.
Ethics Statements
The publication of the present case details was approved by Ethical Committee of People′s Hospital of Quzhou.
Consent for Publication
Written informed consent was obtained from the patient himself for publication of this case report and any accompanying images.
Acknowledgments
The authors thank the patient for his participation and agreement to publication of the report.
Funding
No source of funding to declare.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Goding Sauer A, et al. Colorectal cancer statistics, 2020. CA Cancer J Clin. 2020;70(3):145–164. doi:10.3322/caac.21601
2. Gong J, Cho M, Fakih M. RAS and BRAF in metastatic colorectal cancer management. J Gastrointest Oncol. 2016;7(5):687–704. doi:10.21037/jgo.2016.06.12
3. Mo S, Ma X, Li Y, et al. Somatic POLE exonuclease domain mutations elicit enhanced intratumoral immune responses in stage II colorectal cancer. J Immunother Cancer. 2020;8(2):e000881. doi:10.1136/jitc-2020-000881
4. Kim JH, Kim SY, Baek JY, et al. A Phase II study of avelumab monotherapy in patients with mismatch repair-deficient/microsatellite instability-high or POLE-mutated metastatic or unresectable colorectal cancer. Cancer Res Treat. 2020;52(4):1135–1144. doi:10.4143/crt.2020.218
5. Stasenko M, Tunnage I, Ashley CW, et al. Clinical outcomes of patients with POLE mutated endometrioid endometrial cancer. Gynecol Oncol. 2020;156(1):194–202. doi:10.1016/j.ygyno.2019.10.028
6. van Gool IC, Eggink FA, Freeman-Mills L, et al. POLE proofreading mutations elicit an antitumor immune response in endometrial cancer. Clin Cancer Res. 2015;21(14):3347–3355. doi:10.1158/1078-0432.CCR-15-0057
7. Domingo E, Freeman-Mills L, Rayner E, et al. Somatic POLE proofreading domain mutation, immune response, and prognosis in colorectal cancer: a retrospective, pooled biomarker study. Lancet Gastroenterol Hepatol. 2016;1(3):207–216. doi:10.1016/S2468-1253(16)30014-0
8. Hu H, Cai W, Wu D, et al. Ultra-mutated colorectal cancer patients with POLE driver mutations exhibit distinct clinical patterns. Cancer Med. 2020.
9. Shinbrot E, Henninger EE, Weinhold N, et al. Exonuclease mutations in DNA polymerase epsilon reveal replication strand specific mutation patterns and human origins of replication. Genome Res. 2014;24(11):1740–1750. doi:10.1101/gr.174789.114
10. Rayner E, van Gool IC, Palles C, et al. A panoply of errors: polymerase proofreading domain mutations in cancer. Nat Rev Cancer. 2016;16(2):71–81. doi:10.1038/nrc.2015.12
11. Pursell ZF, Isoz I, Lundstrom EB, Johansson E, Kunkel TA. Yeast DNA polymerase epsilon participates in leading-strand DNA replication. Science. 2007;317(5834):127–130. doi:10.1126/science.1144067
12. Alexandrov LB, Nik-Zainal S, Wedge DC, et al. Signatures of mutational processes in human cancer. Nature. 2013;500(7463):415–421. doi:10.1038/nature12477
13. Siraj AK, Bu R, Iqbal K, et al. POLE and POLD1 germline exonuclease domain pathogenic variants, a rare event in colorectal cancer from the Middle East. Mol Genet Genomic Med. 2020;8(8):e1368. doi:10.1002/mgg3.1368
14. Ahn SM, Ansari AA, Kim J, et al. The somatic POLE P286R mutation defines a unique subclass of colorectal cancer featuring hypermutation, representing a potential genomic biomarker for immunotherapy. Oncotarget. 2016;7(42):68638–68649. doi:10.18632/oncotarget.11862
15. Bellido F, Pineda M, Aiza G, et al. POLE and POLD1 mutations in 529 kindred with familial colorectal cancer and/or polyposis: review of reported cases and recommendations for genetic testing and surveillance. Genet Med. 2016;18(4):325–332. doi:10.1038/gim.2015.75
16. Gong J, Wang C, Lee PP, Chu P, Fakih M. Response to PD-1 blockade in microsatellite stable metastatic colorectal cancer harboring a POLE mutation. J Natl Compr Canc Netw. 2017;15(2):142–147. doi:10.6004/jnccn.2017.0016
17. Yoshida R, Miyashita K, Inoue M, et al. Concurrent genetic alterations in DNA polymerase proofreading and mismatch repair in human colorectal cancer. Eur J Hum Genet. 2011;19(3):320–325. doi:10.1038/ejhg.2010.216
18. Huang D, Knuuti R, Palosaari H, Pospiech H, Syvaoja JE. cDNA and structural organization of the gene Pole1 for the mouse DNA polymerase epsilon catalytic subunit. Biochim Biophys Acta. 1999;1445(3):363–371. doi:10.1016/S0167-4781(99)00058-5
19. Wang C, Gong J, Tu TY, Lee PP, Fakih M. Immune profiling of microsatellite instability-high and polymerase epsilon (POLE)-mutated metastatic colorectal tumors identifies predictors of response to anti-PD-1 therapy. J Gastrointest Oncol. 2018;9(3):404–415. doi:10.21037/jgo.2018.01.09
20. Palles C, Cazier JB, Howarth KM, et al. Germline mutations affecting the proofreading domains of POLE and POLD1 predispose to colorectal adenomas and carcinomas. Nat Genet. 2013;45(2):136–144. doi:10.1038/ng.2503
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.