")
Back to Journals » International Journal of Women's Health » Volume 14
Comparisons of Fertility Outcomes Following a Salpingectomy and a Salpingotomy with or Without Suturing for a Tubal Ectopic Pregnancy
Authors Zhang L, Zhao J, Bai Y, Liu X
Received 29 March 2022
Accepted for publication 19 July 2022
Published 4 August 2022 Volume 2022:14 Pages 1007—1013
DOI https://doi.org/10.2147/IJWH.S367948
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Elie Al-Chaer
Lei Zhang, Jun Zhao, Yun Bai, Xiuping Liu
Department of Obstetrics and Gynecology, the Third Hospital of Hebei Medical University, Shijiazhuang City, 050051, People’s Republic of China
Correspondence: Lei Zhang, Department of Obstetrics and Gynecology, the third hospital of Hebei Medical University, No. 139 of Ziqiang Road, Qiaoxi District, Shijiazhuang City, Hebei Province, 050051, People’s Republic of China, Tel +86-0311-88602058, Email [email protected]
Objective: This study aimed to compare fertility outcomes in patients who underwent different laparoscopic surgeries and to determine the most beneficial surgical treatment for tubal ectopic pregnancy (EP) patients who wished to become pregnant in the future.
Methods: In this retrospective study, patients aged 18– 36 years, who had been diagnosed with a tubal EP in our hospital, were enrolled. Based on the treatment methods, the patients were divided into three groups, ie a salpingectomy group, a salpingotomy with suturing group and a salpingotomy without suturing group. The follow-up time for the enrolled patients was more than three years. Serum beta (β)-human chorionic gonadotropin (β-HCG) levels were monitored after surgery. The intrauterine pregnancy (IUP) rate at 12, 24 and 36 months postoperatively, and recurrent EP rate were compared.
Results: The median time for β-HCG level returning to normal in the salpingectomy group was much shorter than in the salpingotomy with suturing or salpingotomy without suturing groups (P < 0.001). The 12, 24 and 36-month IUP rates among the three groups were not significantly different. A recurrent EP was found in only one patient in the salpingotomy with suturing group and two patients in the salpingotomy without suturing group.
Conclusion: In this study, we found that salpingectomy and salpingotomy with or without suturing methods reflected no significant differences in fertility outcomes for tubal EP patients.
Keywords: ectopic pregnancy, salpingectomy, salpingotomy, intrauterine pregnancy, fertility
Introduction
An ectopic pregnancy (EP) is defined as any pregnancy that does not implant into the uterine cavity; its rate of occurrence comprises 1%–2% of all pregnancies.1,2 The most common site for an EP is the fallopian tube (tubal EP).3,4 Reports indicate that more than 95% of EPs are detected in the ampulla, fimbrial and isthmic portions of the fallopian tube.5 The general symptoms of EP include amenorrhea, irregular and light vaginal bleeding and abdominal pain. It can acutely rupture and remains the primary cause of mortality in the first trimester of pregnancy.1,6
The treatments for tubal EP include medical (methotrexate, [MTX]) and surgical procedures. Surgical treatment is preferred for patients receiving ruptured tubal EP management or patients with a stable EP when medical therapy has failed.6 Compared with a laparotomy, a laparoscopic method has the advantages of decreased postoperative pain, hospital stay and a lower cost; accordingly, it has become the standard approach for the surgical management of EP.7 The main laparoscopic approaches for removing the EP from the fallopian tube include salpingectomy (excision of the affected tube) and salpingotomy (removal of only the products of gestation from the tube), with or without suturing.8 However, for patients who desire to become pregnant in the future, the best surgical approach for managing tubal EP has not yet been determined. Mol et al found that a salpingotomy did not significantly improve fertility outcomes compared with a salpingectomy in a randomised controlled trial including 446 patients.8 Chen et al retrospectively analysed the data of 95 patients diagnosed with a tubal EP.6 No significant differences in fertility outcomes were found between the salpingectomy and salpingotomy groups.6 However, Becker et al conducted a prospective follow-up study of 261 patients who underwent the laparoscopic management of an EP9 and found that a salpingotomy was of particular benefit for patients with additional fertility-reducing factors who desired to become pregnant in the future.9 A laparoscopic salpingotomy with suturing may also yield a different prognosis compared to a salpingotomy without suturing for a tubal EP. A study conducted by Fujishita found that a salpingotomy with suturing had no additional benefit for pregnancy outcomes compared with the non-suturing technique.10 However, Li et al found that suturing following a salpingotomy could decrease damage to the fallopian tube, thereby effectively reserving reproductive function for EP patients.11
The present study was conducted because existing studies have not provided a consensus regarding the best surgical treatment for tubal EP patients who desire to become pregnant in the future. The study aimed to compare fertility outcomes in patients who had undergone different laparoscopic surgeries to determine the most beneficial surgical treatment for tubal EP patients who desired to become pregnant in the future.
Materials and Methods
Patients
The present research reflects a retrospective, observational study that was approved by the institutional review board of our hospital. All of the patients enrolled in this study signed an informed consent form that allowed for the publication of the research data. The data of patients aged 18–36 years old who had been diagnosed as having had a tubal EP (based on one or more modalities, eg ultrasound, serum beta-human chorionic gonadotropin [β-HCG] measurements) and who had undergone laparoscopic procedures in our hospital between July 2016 and January 2018 were retrospectively collected. An EP was diagnosed according to the positive visualisation of an adnexal mass via transvaginal ultrasound, combined with an abnormal rise (a <50% rise over two consecutive days) or plateau (a <15% decline within three days) in serum β-HCG and an abnormal serum progesterone level (<20 ng/mL). A salpingectomy or salpingotomy with or without suturing was offered as treatment options for these patients. The exclusion criteria were as follows: (1) patients had a prior EP history; (2) patients had no desire for future conception; (3) patients were pregnant after in vitro fertilisation; (4) patients had only one or contralateral fallopian tubal occlusions; (5) patients had a ruptured EP.
Based on the treatment selections, the patients were divided into three groups, ie salpingectomy, salpingotomy with suturing and salpingotomy without suturing groups.
Surgical Management
Before surgery, the patients had undergone routine cardiac activity check-ups such as cardiac ultrasound and electrocardiograph. Placed in the supine position, the patients received general anaesthesia. The salpingectomy involved an incision from the mesosalpinx to the tubal isthmus. The entirety of the fallopian tube (0.5–1 cm from the uterine horn) was excised.
Performing a salpingotomy involved making a 10–20 mm linear incision on the most prominent part of the fallopian tube, which correlated to the established location of the EP. The product of conception was removed entirely, and the placental bed was carefully examined. In the salpingotomy without suturing group, the salpingotomy wound was left open. In the salpingotomy with suturing group, the incision was closed in two layers using one or two interrupted sutures via 3–0 VicrylTM absorbable stitches (Johnson & Johnson Medical Co. Ltd, USA). We removed all clots and products of conception, and assessed the contralateral fallopian tube. If any bleeding from inside the lumen or tubal wall occurred, or the procedure was associated with complete tubal damage, such cases with salpingotomy were switched to salpingectomy. For some patients, MTX (1 mg/kg) was injected locally into the mesosalpinx near the EP site in order to prevent recurrent EP.
Assessment
The patient follow-up was more than three years. Serum β-HCG levels were monitored following surgery; the day on which the β-HCG level returned to normal (non-pregnant values, <3 mIU/mL) was recorded. The intrauterine pregnancy (IUP) rate at 12, 24 and 36 months postoperatively, as well as recurrent EP, was evaluated.
Statistical Analysis
The SPSS Statistics (v.22.0) software program was used to analyse the data in this study. Quantitative data were described as mean ± standard deviation. The significance of the differences among the groups was determined by a one-way analysis of variance followed by an LSD test. Categorical data were described as numbers and percentages and compared using a chi-squared test and Fisher’s exact test, followed by a post hoc test using the Bonferroni correction. For the data related to β-HCG changes, the normal β-HCG rate was calculated using the inverse curve analysis of the Kaplan–Meier method and the difference among the curves was evaluated by a Log rank test; P < 0.05 was considered to be statistically significant.
Results
A total of 98 patients diagnosed with a tubal EP and with a median age of 27 (range, 18–35 years) were retrospectively studied. All patients in our study had a desire to preserve their fertility. The median follow-up time was 40 months (range, 36–45 months). Among the enrolled patients, 36 (36.73%) were included in the salpingectomy group, 32 (32.65%) were included in the salpingotomy with suturing group and 30 (30.61%) were included in the salpingotomy without suturing group. None of the patients who underwent salpingotomy was converted to the salpingectomy group.
Table 1 shows the data related to the clinical characteristics in each group. There was no difference among the three groups in terms of patient age, gravidity, history of tubal microsurgery, the distribution of the anatomic location of the EP, the mean dimensions of the ectopic mass or other general symptoms. Patients who underwent a salpingectomy did not use prophylactic MTX; 25.00% (8/32) of patients in the salpingotomy with suturing group and 16.67% (5/30) of patients in the salpingotomy without suturing group were locally injected with MTX in proximity to the EP site.
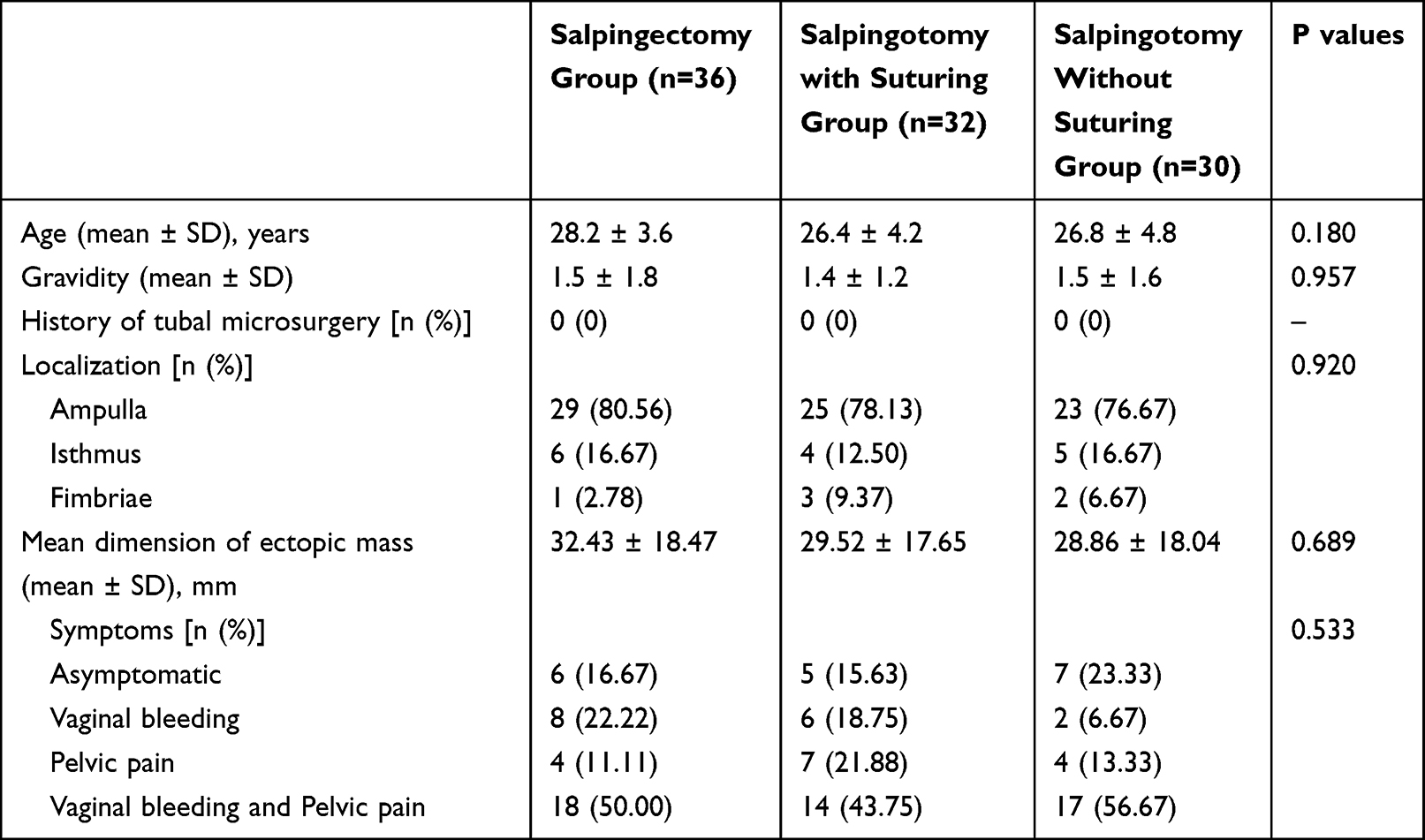 |
Table 1 The Clinical Characteristics of Each Group |
Figure 1 shows that the median time for the β-HCG levels to return to normal in the salpingectomy group was 21 days (range, 16–28 days), which was significantly shorter than in the salpingotomy without suturing group (26 days; range, 20–29 days) and the salpingotomy with suturing group (25.5 days; range, 20–30 days) (P < 0.001). The 12-month cumulative IUP rates were 27.78% (10/36), 43.75% (14/32) and 46.67% (14/30) in the salpingectomy, salpingotomy without suturing and salpingotomy with suturing groups, respectively. Differences in the 12-month IUP rates among the three groups were not significant (P = 0.228). For post hoc comparison, the 12-month IUP rate in the salpingectomy group was not significantly different from that in the salpingotomy without suturing and the salpingotomy with suturing groups, respectively (P > 0.05). As shown in Table 2, the 24 and 36-month IUP rates among the three groups were also not significantly different (P = 0.542 and P = 0.615, respectively). For the post hoc comparison, the 24 and 36-month IUP rates in the salpingectomy group were not significantly different from those in the salpingotomy without suturing or salpingotomy with suturing groups (P > 0.05). A recurrent EP was only found in one patient in the salpingotomy with suturing group and for two patients in the salpingotomy without suturing group. During the follow-up time, the salpingectomy group did not experience a recurring EP (Table 2). The live birth rates were 44.44% (16/36) in the salpingectomy group, 56.25% (18/32) in the salpingotomy with suturing group and 50.00% (15/30) in the salpingotomy without suturing group (Table 2). No significant differences were found in the fertility outcomes among the three groups (P = 0.624, Table 2).
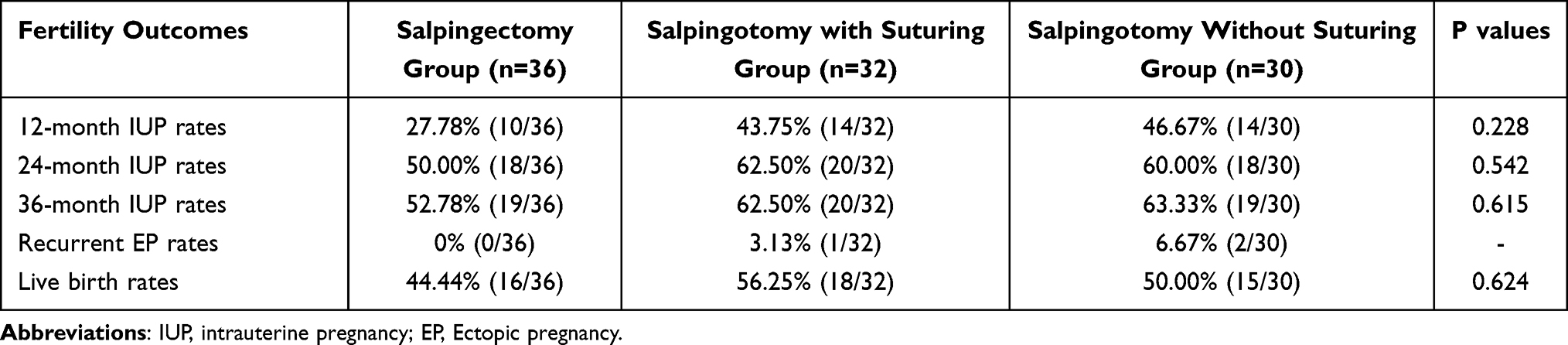 |
Table 2 Comparisons of Fertility Outcomes |
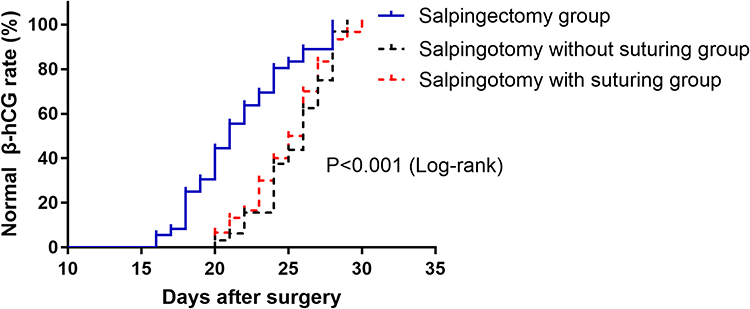 |
Figure 1 Inverse curve analysis of the Kaplan-Meier methods for time of β-HCG returning to normal. |
Discussion
The present study retrospectively analysed data from 98 EP patients who underwent laparoscopic treatment; 36 underwent a salpingectomy, 32 underwent a salpingotomy with incision suturing and 30 patients underwent a salpingotomy without incision suturing. After a follow-up period of at least three years, the current study found that patients who had undergone a salpingectomy experienced a shorter time for β-HCG levels to return to normal. No significant differences were found in the fertility outcomes among the three patient groups.
Ectopic pregnancy is a serious health condition for women of reproductive age.12 The risk factors for EP include a history of pelvic inflammatory disease, a previous EP, cigarette smoking and fallopian tube surgery.12,13 Compared with a laparotomy, in recent years, laparoscopy procedures have become preferable methods for managing tubal EP.13 Salpingectomy and salpingotomy procedures with or without suturing are the main laparoscopic approaches. Regarding the selection of laparoscopic management, patient age, fallopian tube condition, β-HCG levels and the desire for becoming pregnant in the future were the main factors that were considered.6 An increasing number of young patients are required to retain the affected fallopian tubes.14 It has been reported that patients with large ectopic masses (ie a mean mass size of >4 cm) or those with ruptured tubal EPs had been advised to remove the affected tube by salpingectomy.6 In the present study, 98 patients without ruptured tubal EPs were enrolled, all of whom desired preserving the option for future conception. Accordingly, these patients could receive either salpingectomy or a salpingotomy treatment. There was no difference among the three treatment groups in terms of patient age, gravidity, history of tubal microsurgery, the distribution of the anatomic location of the EP or the mean dimension of the ectopic mass.
Syncytiotrophoblasts secrete β-HCG, of which an increase in levels in serum often indicates the presence of a uterine pregnancy.15 As a marker of trophoblastic viability, the β-HCG level is also used for diagnosis and follow-up in patients with an EP.16 It has been found that postoperative HCG regression patterns were similar in women undergoing fallopian tube-conserving surgery compared with women undergoing a salpingectomy for an EP.17 However, the present study found that the median time for β-HCG levels returning to normal in the salpingectomy group was much shorter than that in the salpingotomy with suturing or the salpingotomy without suturing groups. The current study’s small sample size may have contributed to this difference. Therefore, similar research to the present study should be conducted with a larger sample size to confirm its findings.
For tubal EP patients who wished to become pregnant in the future, the specific surgical approach that would obtain better fertility outcomes has not yet been determined. In some studies, a salpingotomy was suggested to EP patients who wished to become pregnant in the future. For example, Becker et al found that a salpingotomy was of particular benefit for such patients who also evidenced additional fertility-reducing factors.9 The data from a study conducted by Kostrzewa supported higher IUP rates after a salpingotomy for the surgical treatment of EP compared to salpingectomy.18 However, studies conducted by Chen et al6 and Turan et al19 presented different outcomes; in these cases, neither salpingotomy nor salpingectomy methods had a significant difference in fertility outcomes for EP patients.6,19 A meta-analysis conducted by Cheng et al confirmed this conclusion.20 The study concluded that the subsequent fertility for EP patients after a salpingectomy/salpingotomy were similar in the long term.20 A randomised controlled trial comprising 446 patients also found that a salpingotomy did not significantly improve fertility prospects compared with a salpingectomy.8 Some studies also posited that a salpingotomy with or without suturing may affect the reproductive function of EP patients. Li et al found that suturing after a salpingotomy could decrease damage to the fallopian tube, effectively reserving reproductive function for EP patients.11 However, Fujishita et al found that a salpingotomy with suturing had no additional benefit for pregnancy outcome compared with the non-suturing technique.10
The present study compared three surgical treatments for fertility outcomes for EP patients. The results supported that a salpingectomy and salpingotomy, with or without suturing, showed no significant differences in fertility outcomes for tubal EP patients. The 12, 24 and 36-month IUP rates among the three groups were not significantly different. Although a salpingotomy preserved the fallopian tube’s structure and function, it increased the probability of an EP recurring in the future, as was reported in existing research.20 In the current study, we observed that a repeated EP occurred in one patient in the salpingotomy with suturing group and two patients in the salpingotomy without suturing group. The salpingectomy procedure did not include any recurrent EPs. Thus, the salpingotomy procedure may cause higher recurrent cases of EP compared to a salpingectomy. However, this study had too low a rate of recurrent EPs to conduct statistical analysis. Further studies are thus needed to confirm its results.
Methotrexate is a folic acid antagonist that inactivates deoxyribonucleic acid synthesis, particularly in fast-growing tissue.21 Existing research has revealed the reduction rate of persistent trophoblastic disease using prophylactic MTX, which can be administered either during or following surgery.5,22,23 In the present study, 25.00% (8/32) of patients in the salpingotomy with suturing group and 16.67% (5/30) of patients in the salpingotomy without suturing group were injected with MTX locally in proximity to the EP site. A longer follow-up is needed to confirm the efficacy of this treatment.
The present study includes several limitations. First, this research was a retrospective study with results that should be validated by future randomised clinical trials. Second, the sample size of this study was small; Third, all of the enrolled patients were sourced from a single centre. This may have given rise to a selection bias. Furthermore, in this study, we did not collect enough data about postoperative complications such as hemoperitoneum, peritubal adhesions, endometriosis and pelvic inflammatory disease due to the retrospective nature. Finally, the follow-up time of this study was not long enough.
Conclusions
The results of the present study found that salpingectomy and salpingotomy procedures with or without suturing showed no significant difference regarding fertility outcomes for tubal EP patients. Thus, the choice of surgical treatment for EP patients desiring to become pregnant in the future should be comprehensively evaluated in clinical settings.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Statement of Ethics
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of The third hospital of Hebei Medical University. Written informed consent was obtained from all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Consent for Publication
The manuscript is not submitted for publication or consideration elsewhere.
Funding
This work was supported by Key research project plan of medical science of Hebei Health Commission [No.: 20190667].
Disclosure
The authors declare that they have no competing interests.
References
1. Sahin C, Uygun ZO, Hortu I, et al. Using dynein heavy chain 5 and creatine kinase levels in cervical fluid and blood for early diagnosing of ectopic pregnancy. J Obstet Gynaecol Res. 2021;47(3):921–927. doi:10.1111/jog.14616
2. Sun F, Yang S, Yang Y, Liu X, Xu H. Laparoscopic Management of 42 Cases of Tubal Stump Pregnancy and Postoperative Reproductive Outcomes. J Minim Invasive Gynecol. 2020;27(3):618–624. doi:10.1016/j.jmig.2019.04.030
3. Acet F, Goker ENT, Hortu I, Sahin G, Tavmergen E, Rare A. Case of Bilateral Tubal Ectopic Pregnancy Following Intracytoplasmic Sperm Injection-Embryo Transfer (ICSI-ET). Rev Bras Ginecol Obstet. 2020;42(3):165–168. doi:10.1055/s-0040-1708093
4. Hortu I, Akman L, Akdemir A. Management of Ectopic Pregnancy in Unusual Locations: five-Year Experience in a Single Center. J Clin Exp Invest. 2017;8(3):90–95. doi:10.5799/jcei.343197
5. Ghafouri-Fard S, Shoorei H, Taheri M. The role of microRNAs in ectopic pregnancy: a concise review. Noncoding RNA Res. 2020;5(2):67–70. doi:10.1016/j.ncrna.2020.04.002
6. Chen L, Zhu D, Wu Q, Yu Y. Fertility outcomes after laparoscopic salpingectomy or salpingotomy for tubal ectopic pregnancy: a retrospective cohort study of 95 patients. Int J Surg. 2017;48:59–63. doi:10.1016/j.ijsu.2017.09.058
7. Ehrenberg-Buchner S, Sandadi S, Moawad NS, Pinkerton JS, Hurd WW. Ectopic pregnancy: role of laparoscopic treatment. Clin Obstet Gynecol. 2009;52(3):372–379. doi:10.1097/GRF.0b013e3181b0be24
8. Mol F, van Mello NM, Strandell A, et al. Salpingotomy versus salpingectomy in women with tubal pregnancy (ESEP study): an open-label, multicentre, randomised controlled trial. Lancet. 2014;383(9927):1483–1489. doi:10.1016/S0140-6736(14)60123-9
9. Becker S, Solomayer E, Hornung R, et al. Optimal treatment for patients with ectopic pregnancies and a history of fertility-reducing factors. Arch Gynecol Obstet. 2011;283(1):41–45. doi:10.1007/s00404-009-1270-2
10. Fujishita A, Masuzaki H, Khan KN, Kitajima M, Hiraki K, Ishimaru T. Laparoscopic salpingotomy for tubal pregnancy: comparison of linear salpingotomy with and without suturing. Arch Gynecol Obstet. 2011;283(1):41–45. doi:10.1007/s00404-009-1270-2
11. Li L, Wang JJ, Cheng JM. Laparoscopic salpingotomy for tubal pregnancy: comparison of linear salpingotomy with and without suturing. National Med J China. 2016;96(30):2424–2426.
12. Hendriks E, Rosenberg R, Prine L. Ectopic Pregnancy: diagnosis and Management. Am Fam Physician. 2020;101(10):599–606.
13. Taran FA, Kagan KO, Hübner M, Hoopmann M, Wallwiener D, Brucker S. The Diagnosis and Treatment of Ectopic Pregnancy. Dtsch Arztebl Int. 2015;112(41):693–703. doi:10.3238/arztebl.2015.0693
14. Li X, Zhang C, Li Y, Yuan J, Lu Q, Wang Y. Predictive values of the ratio of beta-human chorionic gonadotropin for failure of salpingostomy in ectopic pregnancy. Int J Clin Exp Pathol. 2019;12(3):901–908.
15. Faraji Darkhaneh R, Asgharnia M, Farahmand Porkar N, Alipoor AA. Predictive value of maternal serum β-hCG concentration in the ruptured tubal ectopic pregnancy. Iran J Reprod Med. 2015;13(2):101–106.
16. Cartwright J, Duncan WC, Critchley HO, Horne AW. Serum biomarkers of tubal ectopic pregnancy: current candidates and future possibilities. Reproduction. 2009;138(1):9–22. doi:10.1530/REP-09-0060
17. Hellemans P, Gerris J, Joostens M, van der Meer S, Verdonk P, Francx M. Serum hCG decline following salpingotomy or salpingectomy for extrauterine pregnancy. Eur J Obstet Gynecol Reprod Biol. 1994;53(1):59–64. doi:10.1016/0028-2243(94)90139-2
18. Kostrzewa M, Zyła M, Litwińska E, et al. Salpingotomy vs salpingectomy–a comparison of women’s fertility after surgical treatment of tubal ectopic pregnancy during a 24-month follow-up study. Ginekol Pol. 2013;84(12):1030–1035. doi:10.17772/gp/1675
19. Turan V. Fertility outcomes subsequent to treatment of tubal ectopic pregnancy in younger Turkish women. J Pediatr Adolesc Gynecol. 2011;24(5):251–255. doi:10.1016/j.jpag.2010.12.007
20. Cheng X, Tian X, Yan Z, et al. Comparison of the Fertility Outcome of Salpingotomy and Salpingectomy in Women with Tubal Pregnancy: a Systematic Review and Meta-Analysis. PLoS One. 2016;11(3):e0152343. doi:10.1371/journal.pone.0152343
21. Ozyuncu O, Tanacan A, Duru SA, Beksac MS. Methotrexate Therapy for Ectopic Pregnancies: a Tertiary Center Experience. Rev Bras Ginecol Obstet. 2018;40(11):680–685. doi:10.1055/s-0038-1675807
22. Kaya H, Babar Y, Ozmen S, et al. Intratubal methotrexate for prevention of persistent ectopic pregnancy after salpingotomy. J Am Assoc Gynecol Laparosc. 2002;9(4):464–467. doi:10.1016/s1074-3804(05)60520-8
23. Lund CO, Nilas L, Bangsgaard N, Ottesen B. Persistent ectopic pregnancy after linear salpingotomy: a non-predictable complication to conservative surgery for tubal gestation. Acta Obstet Gynecol Scand. 2002;81(11):1053–1059. doi:10.1034/j.1600-0412.2002.811110.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.