")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 11
Comparison of zero-profile anchored spacer versus plate-cage construct in treatment of cervical spondylosis with regard to clinical outcomes and incidence of major complications: a meta-analysis
Authors Liu W, Hu L, Wang J, Liu M, Wang X
Received 16 July 2015
Accepted for publication 24 August 2015
Published 23 September 2015 Volume 2015:11 Pages 1437—1447
DOI https://doi.org/10.2147/TCRM.S92511
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Deyun Wang
Weijun Liu,1,* Ling Hu,2,* Junwen Wang,1 Ming Liu,1 Xiaomei Wang3
1Department of Orthopedics, Pu Ai Hospital, Affiliated to Tongji Medical College, Huazhong University of Science and Technology, 2Department of Anesthesiology, Tianyou Hospital, Affiliated to Wuhan University of Science and Technology, 3Department of Biological Science and Technology, Wuhan Bioengineering Institute, Wuhan, People’s Republic of China
*These authors contributed equally to this work
Purpose: Meta-analysis was conducted to evaluate whether zero-profile anchored spacer (Zero-P) could reduce complication rates, while maintaining similar clinical outcomes compared to plate-cage construct (PCC) in the treatment of cervical spondylosis.
Methods: All prospective and retrospective comparative studies published up to May 2015 that compared the clinical outcomes of Zero-P versus PCC in the treatment of cervical spondylosis were acquired by a comprehensive search in PubMed and EMBASE. Exclusion criteria were non-English studies, noncomparative studies, hybrid surgeries, revision surgeries, and surgeries with less than a 12-month follow-up period. The main end points including Japanese Orthopedic Association (JOA) and Neck Disability Index (NDI) scores, cervical lordosis, fusion rate, subsidence, and dysphagia were analyzed. All studies were analyzed with the RevMan 5.2.0 software. Publication biases of main results were examined using Stata 12.0.
Results: A total of 12 studies were included in the meta-analysis. No statistical difference was observed with regard to preoperative or postoperative JOA and NDI scores, cervical lordosis, and fusion rate. The Zero-P group had a higher subsidence rate than the PCC group (P<0.05, risk difference =0.13, 95% confidence interval [CI] 0.00–0.26). However, the Zero-P group had a significantly lower postoperative dysphagia rate than the PCC group within the first 2 weeks (P<0.05, odds ratio [OR] =0.64, 95% CI 0.45–0.91), at the 6th month [P<0.05, OR =0.20, 95% CI 0.04–0.90], and at the final follow-up time [P<0.05, OR =0.13, 95% CI 0.04–0.45].
Conclusion: Our meta-analysis suggested that surgical treatments of single or multiple levels of cervical spondylosis using Zero-P and PCC were similar in terms of JOA score, NDI score, cervical lordosis, and fusion rate. Although the Zero-P group had a higher subsidence rate than the PCC group, Zero-P had a lower postoperative dysphagia rate and might have a lower adjacent-level ossification rate.
Keywords: cervical spondylosis, anterior cervical decompression and fusion, integrated interbody device, dysphagia, meta-analysis, subsidence, adjacent-level ossification
Introduction
Age-related cervical degeneration is evident in over 50% of the middle-aged population and is the most common cause of neural dysfunction.1 Although the majority of cases are asymptomatic, changes such as disc herniation, osteophyte formation, and hypertrophied ligaments may compress the cervical neuraxis to result in neck pain, radiculopathy, or myelopathy.2 Conservative treatment is initially recommended for patients who do not have a significant neurological deficit; surgery is indicated for patients with moderate-to-severe myelopathy, or patients with unremitting and progressive symptoms that have failed nonoperative treatment.3
Since the first anterior cervical decompression and fusion (ACDF) was introduced in 1958,4 the procedure has become the gold-standard operation for single or multiple levels of degenerative cervical spondylosis.5,6 Traditionally, iliac bone graft was used; however, cervical cages were introduced to avoid donor-site complications such as hematoma, infection, and pain. Anterior plate is commonly added in order to reduce the incidence of pseudarthrosis and enhance construct stability. Although current anterior plates are thinner than earlier designs, there are still some potential plate-related complications such as dysphagia and adjacent-level ossification (ALO).7–11
To avoid these complications, stand-alone cages had been advocated by some surgeons. Nevertheless, cage dislocation, subsidence, nonunion, and sagittal malalignment of stand-alone cages are still of great concern.12,13 Zero-profile anchored spacer (Zero-P) is likely to provide immediate stability and prevent plate-related complications by virtue of the advantages of stand-alone cage and anchoring screws fixation. Nowadays, Zero-P devices are developed from different companies with different designs.
Some studies have tried to investigate the differences between Zero-P and plate-cage construct (PCC) on the clinical outcomes and complication rates in the treatment of cervical spondylosis. Most of these studies agreed that the Zero-P group had similar clinical outcomes and fusion rate compared to the PCC group, but no consensus on complication rates, especially dysphagia, has been reached.14–25 It is unknown whether the differences in the literature have been mostly due to the limitation of sample size or genuine heterogeneity. In this study, we sought to conduct a systematic review and meta-analysis from published studies to evaluate whether Zero-P could reduce the complication rates, while maintaining fusion rate and clinical outcomes similar to or even better than that of PCC.
Methods
Search strategy
The primary source of the reviewed studies was PubMed and EMBASE. The search included literature exclusively in English published up to May 27, 2015. The following search terms were used: 1) anchored cage OR anchored spacer; 2) zero-profile OR integrated plate OR self-locking stand-alone; 3) cervical; 2) and 3). Reference lists of all included studies were scanned to identify additional potentially relevant studies. Two reviewers independently screened the titles and abstracts of identified papers, and full text copies of all potentially relevant studies were obtained.
Inclusion criteria
Studies were included if they met the following criteria: 1) study design: prospective or retrospective comparative study; 2) patients with cervical spondylosis, including neck pain, radiculopathy, or myelopathy, who had one-to-four levels operation; excluding patients with tumor, trauma, infection, previous surgery, revision surgery, and hybrid surgery; 3) purpose of interventions: to compare clinical outcome differences between Zero-P and PCC; 4) outcome measurements: clinical evaluations including Japanese Orthopedic Association (JOA) and Neck Disability Index (NDI); radiological evaluations including cervical lordosis, fusion rate, and subsidence; complications including dysphagia; 5) more than 12-month mean follow-up term; 6) English studies. Studies that did not meet the above criteria were excluded from selection.
Data extraction
The following information was extracted from each study: 1) study ID; 2) study design; 3) study location; 4) etiology; 5) number of cases; 6) length of follow-up; 7) number of surgical levels; 8) preoperative and postoperative JOA scores; 9) preoperative and postoperative NDI scores; 10) fusion rate; 11) subsidence; 12) dysphagia; 13) other complications.
Data analysis
Statistical analysis was conducted using the Review Manager software (RevMan Version 5.2; The Nordic Cochrane Center, The Cochrane Collaboration, Copenhagen, Denmark). Heterogeneity was tested using the chi-square test and quantified by calculating the I2 statistic, in which P<0.05 and I2>50% was considered statistically significant. For the pooled effects, weighted mean difference (WMD) was calculated for continuous variables according to the consistency of measurement units, and odds ratio (OR) was calculated for dichotomous variables. Continuous variables are presented as mean differences and 95% confidence intervals (CIs), whereas dichotomous variables are presented as ORs and 95% CI. Random-effects or fixed-effects models were used depending on the heterogeneity of the studies included. Publication bias was tested using a funnel plot.
Results
Characteristics of studies
A total of 376 papers were identified by screening the titles and abstracts; 339 papers were excluded due to duplicates, irrelevant studies, case reports, revision surgeries, hybrid surgeries, non-English studies, and reviews. The remaining 37 papers underwent a detailed and comprehensive evaluation (Figure 1). Biomechanics studies, noncomparative studies, and studies with less than 12-month follow-up were excluded. Twelve studies were finally included in this meta-analysis.14–25 Information of all the studies was listed (Table 1).
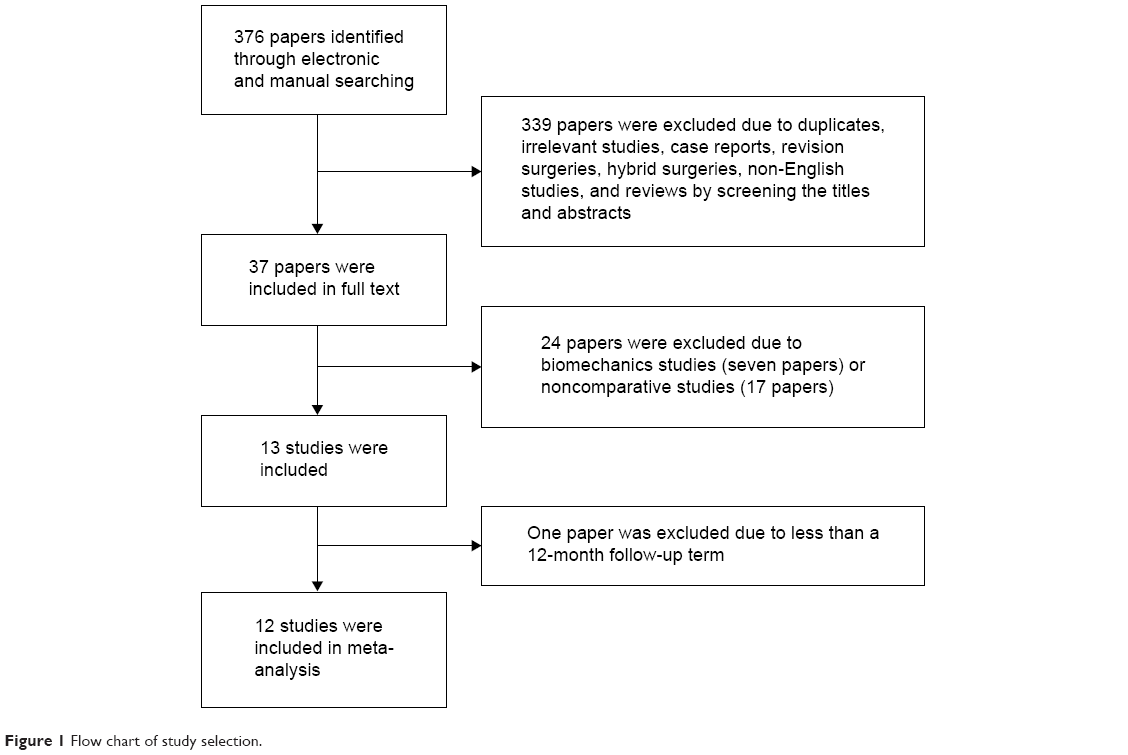 | Figure 1 Flow chart of study selection. |
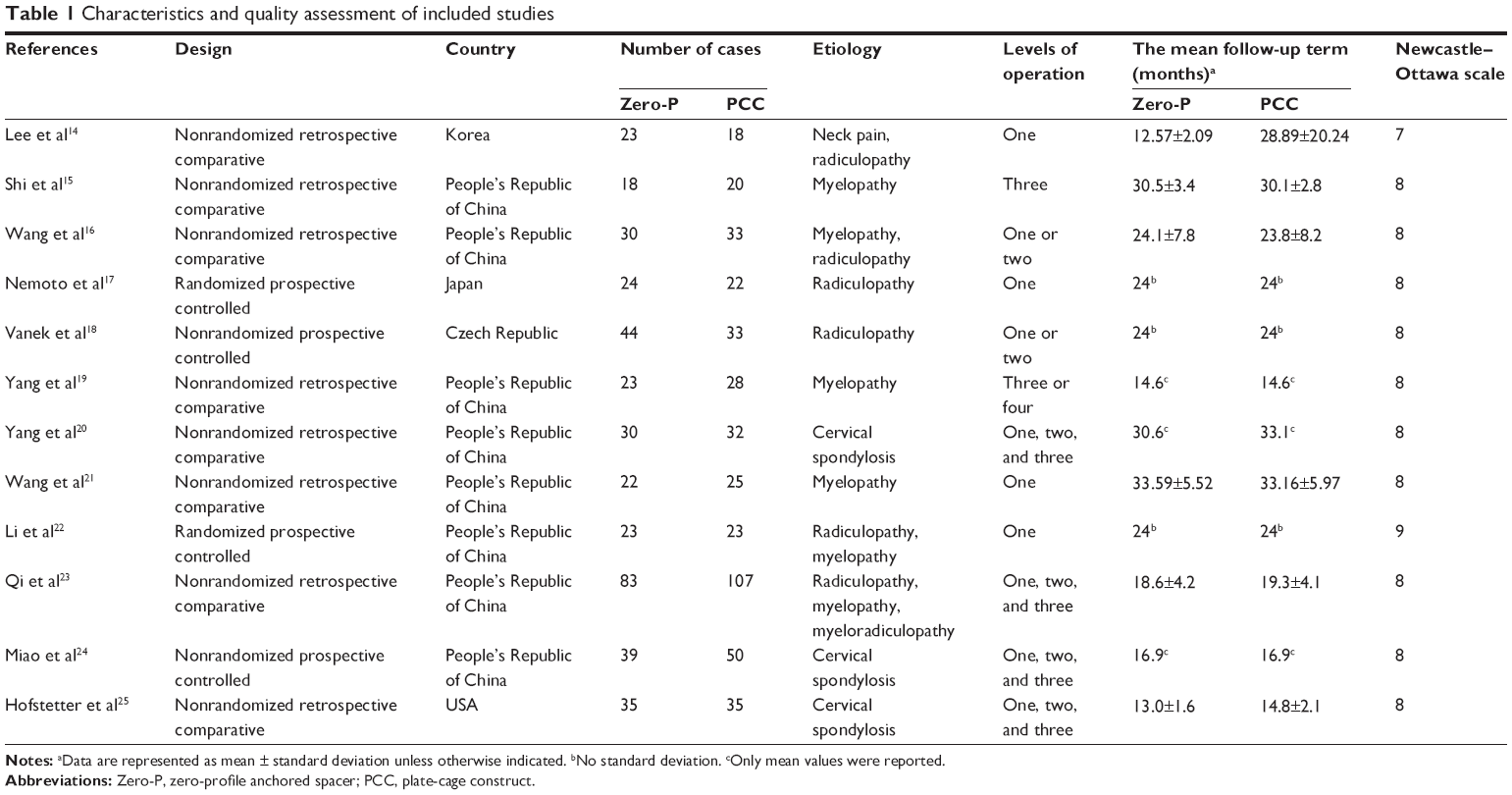 | Table 1 Characteristics and quality assessment of included studies |
Quality assessment
Two investigators evaluated each study and extracted data independently, and any controversies were resolved via discussion. The major baseline characteristics of participants in each study were similar. Newcastle–Ottawa scale was used to assess the quality of included studies. Of the studies, one scored 9 points, ten scored 8 points, and one scored 7 points; it indicated that all the studies were of a relatively high-quality (Table 1).
Preoperative JOA score
The preoperative JOA scores were analyzed in seven studies. Statistical data of one study were unavailable. Six studies and 350 cases were involved including 162 cases of Zero-P and 188 cases of PCC. There was no significant difference in the preoperative JOA score between Zero-P group and PCC groups (P>0.05, WMD −0.23 [−0.57, 0.11]; Figure 2). The χ2 test indicated no statistical evidence of heterogeneity (I2=0%, P=0.19).
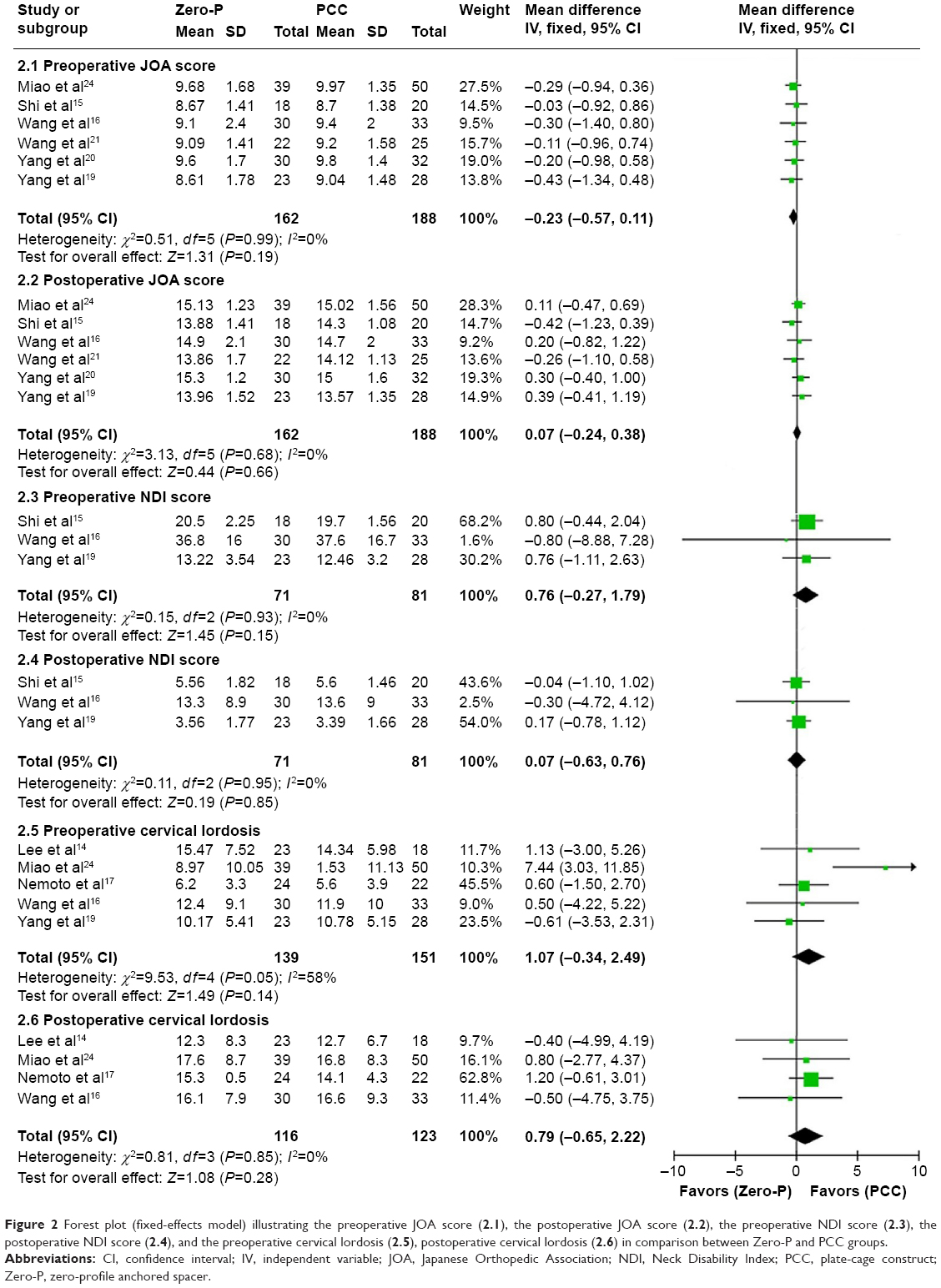 | Figure 2 Forest plot (fixed-effects model) illustrating the preoperative JOA score (2.1), the postoperative JOA score (2.2), the preoperative NDI score (2.3), the postoperative NDI score (2.4), and the preoperative cervical lordosis (2.5), postoperative cervical lordosis (2.6) in comparison between Zero-P and PCC groups. |
Postoperative JOA score
The postoperative JOA scores of the final follow-up time were analyzed in seven studies. Statistical data of one study were unavailable. Six studies and 350 cases were involved including 162 cases of Zero-P and 188 cases of PCC. There was no significant difference in the postoperative JOA score between Zero-P and PCC groups (P>0.05, WMD 0.07 [−0.24, 0.38]; Figure 2). The χ2 test indicated no statistical evidence of heterogeneity (I2=0%, P=0.66).
Preoperative NDI score
The preoperative NDI scores were analyzed in four studies. Statistical data of one study were unavailable. Three studies and 152 cases were involved including 71 cases of Zero-P and 81 cases of PCC. There was no significant difference in the preoperative NDI score between Zero-P and PCC groups (P>0.05, WMD 0.76 [−0.27, 1.79]; Figure 2). The χ2 test indicated no statistical evidence of heterogeneity (I2=0%, P=0.15).
Postoperative NDI score
The postoperative NDI scores at the 3rd month were analyzed in four studies. Statistical data of one study were unavailable. Three studies and 152 cases were involved including 71 cases of Zero-P and 81 cases of PCC. There was no significant difference in the postoperative NDI score between Zero-P and PCC group (P>0.05, WMD 0.07 [−0.63, 0.76]; Figure 2). The χ2 test indicated no statistical evidence of heterogeneity (I2=0%, P=0.85).
Preoperative cervical lordosis
Preoperative cervical lordosis was analyzed in seven studies. Statistical data of two studies were unavailable. Five studies and 290 cases were involved including 139 cases of Zero-P and 151 cases of PCC. There was no significant difference in preoperative cervical lordosis between Zero-P and PCC groups (P>0.05, WMD 1.07 [−0.34, 2.49]; Figure 2). Moderate heterogeneity existed between these studies (I2=58%, P=0.14).
Postoperative cervical lordosis
Postoperative cervical lordosis at the 12th month was analyzed in four studies, in which 239 cases were involved including 116 cases of Zero-P and 123 cases of PCC. There was no significant difference in postoperative cervical lordosis between Zero-P and PCC group (P>0.05, WMD 0.79 [−0.65, 2.22]; Figure 2). The χ2 test indicated no statistical evidence of heterogeneity (I2=0%, P=0.28).
Fusion rate
Five studies provided a postoperative (final follow-up) fusion rate. Here, 412 cases were involved including 189 cases of Zero-P and 223 cases of PCC. Fusion rates in Zero-P group were 100% in Shi et al,15 100% in Wang et al,16 100% in Yang et al,19 100% in Qi et al23 and 95.2% in Hofstetter et al.25 In comparison, fusion rates in the PCC group were 100% in Shi et al,15 100% in Wang et al,16 100% in Yang et al,19 100% in Qi et al23 and 96% in Hofstetter et al.25 A cross-study analysis was calculated to measure the homogeneity of outcomes. P-values of each study with the other four studies were analyzed in Zero-P and PCC group, and P-values were all >0.05 except for the study of Hofstetter et al.25 However, the sample number of this study was small and fusion rates of all five studies were similar. All data for five studies were involved in the final statistical analysis, where no significant difference was found in fusion rate between Zero-P and PCC groups (P=0.468).
Subsidence
Subsidence was analyzed in three studies. Here, 125 cases were involved including 65 cases of Zero-P and 60 cases of PCC. The Zero-P group had a significantly higher subsidence rate than the PCC group (P<0.05, risk difference =0.13, 95% CI 0.00–0.26; Figure 3). Mild heterogeneity existed between these studies (I2=28%, P=0.04).
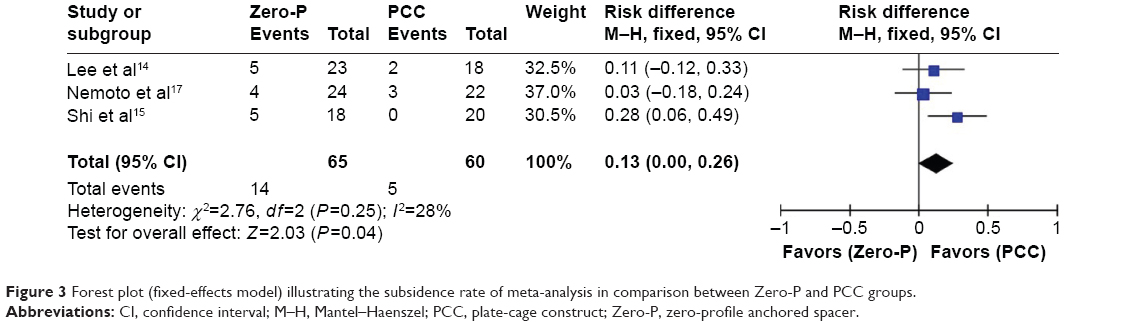 | Figure 3 Forest plot (fixed-effects model) illustrating the subsidence rate of meta-analysis in comparison between Zero-P and PCC groups. |
Postoperative dysphagia rate within the first 2 weeks
Postoperative dysphagia rates within the first 2 weeks were analyzed in nine studies. Statistical data of one study were unavailable. Eight studies and 582 cases were involved including 279 cases of Zero-P and 303 cases of PCC. The Zero-P group had a significantly lower dysphagia rate than the PCC group (P<0.05, OR=0.64, 95% CI 0.45–0.91; Figure 4). The χ2 test indicated no statistical evidence of heterogeneity (I2=0%, P=0.01).
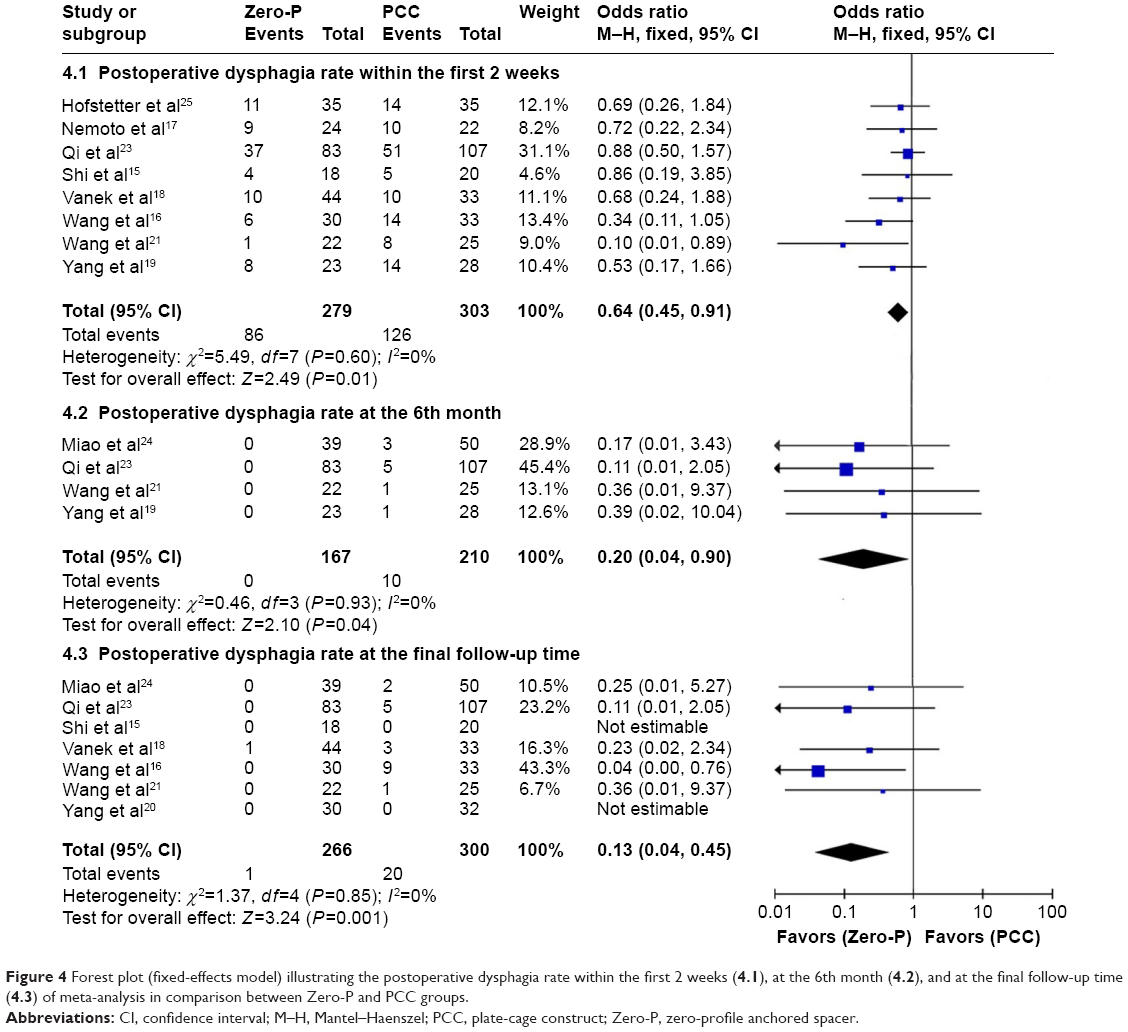 | Figure 4 Forest plot (fixed-effects model) illustrating the postoperative dysphagia rate within the first 2 weeks (4.1), at the 6th month (4.2), and at the final follow-up time (4.3) of meta-analysis in comparison between Zero-P and PCC groups. |
Postoperative dysphagia rate at the 6th month
Four studies reported postoperative dysphagia rates at the 6th month. Here, 377 cases were involved including 167 cases of Zero-P and 210 cases of PCC. The dysphagia rate was significantly lower in the Zero-P group compared to the PCC group (P<0.05, OR =0.20, 95% CI 0.04–0.90; Figure 4). The χ2 test indicated no statistical evidence of heterogeneity (I2=0%, P=0.04).
Postoperative dysphagia rate at the final follow-up time
Postoperative dysphagia rates at the final follow-up time were analyzed in seven studies, 566 cases were involved including 266 cases of Zero-P and 300 cases of PCC. The Zero-P group had a significantly lower dysphagia rate than the PCC group (P<0.05, OR =0.13, 95% CI 0.04–0.45; Figure 4). The χ2 test indicated no statistical evidence of heterogeneity (I2=0%, P=0.001).
Publication bias
The Stata 12.0 software (StataCorp LP, College Station, TX, USA) was used to examine the publication bias of the main results. All funnel plots were largely symmetric including preoperative and postoperative JOA and NDI, cervical lordosis, subsidence, and postoperative dysphagia rate within the first 2 weeks (Figure 5). These results indicated that publication bias might not play a vital role in the observed effects and the conclusions were reliable.
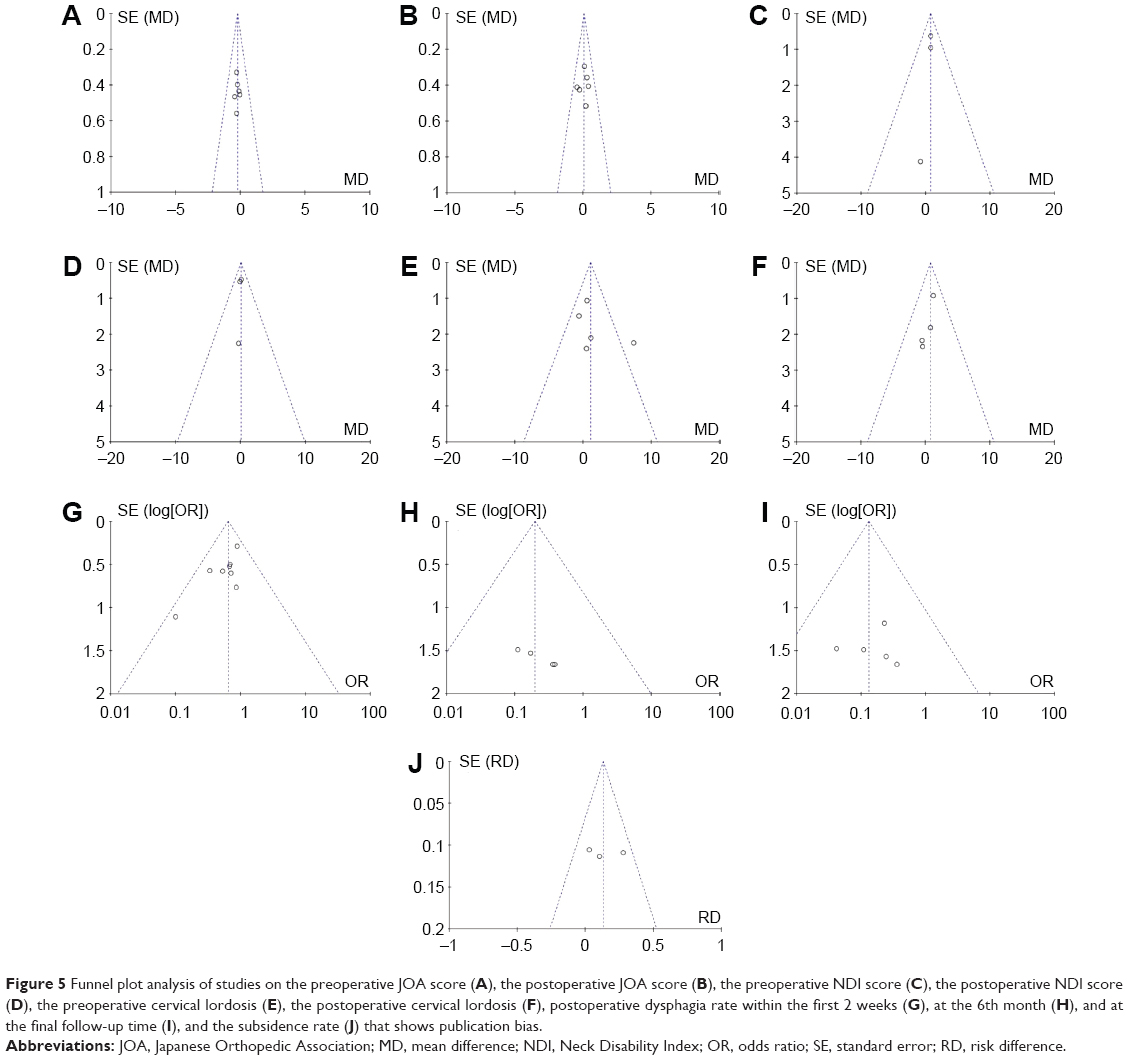 | Figure 5 Funnel plot analysis of studies on the preoperative JOA score (A), the postoperative JOA score (B), the preoperative NDI score (C), the postoperative NDI score (D), the preoperative cervical lordosis (E), the postoperative cervical lordosis (F), postoperative dysphagia rate within the first 2 weeks (G), at the 6th month (H), and at the final follow-up time (I), and the subsidence rate (J) that shows publication bias. |
Discussion
ACDF is considered the standard operation for cervical spondylosis when nonoperative treatment fails. The outcomes of ACDF depend on direct decompression, stability of fused segment, restoration of cervical lordosis, and avoidance of complications. To achieve these objectives, a series of cages and plates were designed. Zero-P was approved by the US Food and Drug Administration in 2008. It utilizes an integrated, anchor design to avoid protrusion in front of the vertebral body, which is likely to provide immediate stability and prevent plate-related complications. Biomechanical studies reported that Zero-P provided a similar stability to PCC in one-level ACDF,26 although it might not provide adequate segmental stability in multilevel ACDF,27,28 the encouraging clinical outcomes were reported in one or multiple levels ACDF surgery.14–25 However, conflicting results existed in different studies with regard to complications, especially dysphagia. To verify the conclusion of clinical outcomes based on the latest high-quality studies for strong evidence, we systematically compared Zero-P with PCC in terms of clinical outcomes and incidence of major complications in the treatment of one- or multiple-level cervical spondylosis.
In our meta-analysis, there were no statistically significant differences in preoperative or postoperative JOA and NDI scores between Zero-P and PCC groups. Visual Analog Scale (VAS) scores were also reported in four studies, but only one study provided the detailed data of arm or neck VAS score. No statistically significant differences were reported in preoperative or postoperative VAS scores between Zero-P and PCC groups in these studies. All these available evidence indicated that the clinic evaluations of both Zero-P and PCC groups were similar.
Fusion is a basic goal of ACDF. The nonunion rate after ACDF can vary based on the number of levels fused, the type of allograft used, and the surgical technique. Fraser and Hartl reported an increased rate of nonunion for stand-alone cage surgery in comparison with PCC surgery in a meta-analysis.29 The nonunion rate increased from 7.9% for one-level, 21.1% for two-level, to 35% for three-level stand-alone cage surgery. In comparison, a significantly lower nonunion rate (2.9% one-level, 4.1% two-level, and 17.5% three-level) was detected when an additional plate was used. Symptomatic pseudarthrosis needs a revision surgery. Although it might not provide adequate segmental stability like PCC in multilevel ACDF, Zero-P was more stable than stand-alone cage not only in one but also in two or three levels.27,28 In this meta-analysis, we found a relatively high-fusion rate in both Zero-P and PCC groups and no statistically significant difference was observed between them. These results indicated that the Zero-P held the equivalent capability for solid fusion to that of PCC.
The occurrence of cage subsidence might be related to various factors including size, position, and contact surface ratio of a cage as well as bone density and applied distraction during surgery.17 Hida et al reported a 7% of subsidence rate in the stand-alone cage.30 Although clinical outcomes of the patients affected by the cage subsidence were controversial, the secondary kyphosis of subsidence may be regarded as a risk factor contributing to the progression of degenerative changes in adjacent segments.17 Subsidence rate after ACDF varied from 5.4% to 55.6% depending on the surgical method.31–35 The reported subsidence rates of Zero-P were not accordant, one study reported that it was higher than that of PCC,15 while another study reported that it was similar.17 In this meta-analysis, we found that the Zero-P group had a higher subsidence rate than the PCC group, however, no statistically significant difference was found in cervical lordosis.
Dysphagia is a common complication of ACDF. The incidence of dysphagia was between 2% and 67%.7–10 In the majority of cases, dysphagia resolves within the first 3 months; however, in 12.5%–35.1% of patients, dysphagia persists for more than 3 months.8 Postoperative soft tissue swelling, hematoma at the operative site, esophageal injury, and adhesion formation around implanted cervical plates may be possible reasons for dysphagia.7 Dysphagia was also related to the thickness of the anterior plate at the fusion level.36 In this meta-analysis, we analyzed postoperative dysphagia rates at three different time points including within the first 2 weeks, at the 6th month and at the final follow-up time. The Zero-P group had statistically significant lower postoperative dysphagia rate than the PCC group at all three time points.
ALO was considered as another plate-related complication. Park et al reported a positive association between the plate-to-disc distance and ALO following anterior cervical plate procedures.11 The incidence of ALO was significantly increased when the distance was below 5 mm. Two included studies reported that Zero-P surgery could reduce the incidence of ALO than PCC surgery.17,20 However, an obvious limitation was that the follow-up terms of both studies were not sufficient. Mean follow-up terms of both studies were <33 months, and no other studies reported ALO. Longer follow-up term and more related studies are needed for stronger evidence in future.
Temporary postoperative hoarseness was reported in both Zero-P and PCC groups. All other complications including hematoma, dual tear, screw loosening, dislocation, and infection had been seldom or not reported in all these studies. It might indicate that both Zero-P and PCC surgeries are relatively safe.
However, there are some limitations to this meta-analysis. First, all the included publications are English language, thus a potential language bias maybe exist in this meta-analysis. Second, the sample size is not large enough to find the possible existing evidence, more included studies are needed. Third, there was a variable length of follow-up between the studies, which is important for evaluating good surgery results. Lastly, clinical heterogeneity might be caused by the various indications for surgery and the surgical technologies used at the different treatment centers. In summary, our meta-analysis suggested that, in the treatment of cervical spondylosis, the Zero-P group had a higher subsidence rate and lower postoperative dysphagia rate when it maintained the similar clinical outcomes compared to the PCC group. We believe that Zero-P implant is a viable alternative to ACDF in patients with cervical spondylosis, especially when it is applied in one-level ACDF surgery. However, longer follow-up term and more randomized prospective studies especially on multilevel Zero-P surgery are needed.
Conclusion
In this meta-analysis, we systematically compared Zero-P with PCC with regard to clinical outcomes and incidence of major complications in the treatment of one or multiple levels of cervical spondylosis. No statistical difference was observed in JOA score, NDI score, cervical lordosis, and fusion rate between Zero-P and PCC groups. Although the Zero-P group had a higher subsidence rate than the PCC group, Zero-P had a lower postoperative dysphagia rate and might have a lower ALO rate. However, the evaluation criteria of fusion in the studies were not accordant, which might result in a deviated outcome. Larger-scale and higher-quality studies with longer follow-up terms are needed to provide more reliable evidence for future evaluation.
Disclosure
The authors report no conflicts of interest in this work.
References
Irvine DH, Foster JB, Newell DJ, Klukvin BN. Prevalence of cervical spondylosis in general practice. Lancet. 1965;1(7395):1089–1092. | ||
Chau AM, Mobbs RJ. Bone graft substitutes in anterior cervical discectomy and fusion. Eur Spine J. 2009;18(4):449–464. | ||
Hirpara KM, Butler JS, Dolan RT, O’Byrne JM, Poynton AR. Nonoperative modalities to treat symptomatic cervical spondylosis. Adv Orthop. 2012;2012:294857. | ||
Cloward RB. The anterior approach for removal of ruptured cervical disks. J Neurosurg. 1958;15(6):602–617. | ||
Korinth MC. Treatment of cervical degenerative disc disease – current status and trends. Zentralbl Neurochir. 2008;69(3):113–124. | ||
Mummaneni PV, Kaiser MG, Matz PG, et al. Cervical surgical techniques for the treatment of cervical spondylotic myelopathy. J Neurosurg Spine. 2009;11(2):130–141. | ||
Fountas KN, Kapsalaki EZ, Nikolakakos LG, et al. Anterior cervical discectomy and fusion associated complications. Spine (Phila Pa 1976). 2007;32(21):2310–2317. | ||
Bazaz R, Lee MJ, Yoo JU. Incidence of dysphagia after anterior cervical spine surgery: a prospective study. Spine (Phila Pa 1976). 2002;27(22):2453–2458. | ||
Smith-Hammond CA, New KC, Pietrobon R, Curtis DJ, Scharver CH, Turner DA. Prospective analysis of incidence and risk factors of dysphagia in spinesurgery patients: comparison of anterior cervical, posterior cervical, and lumbar procedures. Spine (Phila Pa 1976). 2004;29(13):1441–1446. | ||
Frempong-Boadu A, Houten JK, Osborn B, et al. Swallowing and speech dysfunction in patients undergoing anterior cervical discectomy and fusion: a prospective, objective preoperative and postoperative assessment. J Spinal Disord Tech. 2002;15(5):362–368. | ||
Park JB, Cho YS, Riew KD. Development of adjacent-level ossification in patients with an anterior cervical plate. J Bone Joint Surg Am. 2005;87(3):558–563. | ||
Kulkarni AG, Hee HT, Wong HK. Solis cage (PEEK) for anterior cervical fusion: preliminary radiological results with emphasis on fusion and subsidence. Spine J. 2007;7(2):205–209. | ||
Schmieder K, Wolzik-Grossmann M, Pechlivanis I, Engelhardt M, Scholz M, Harders A. Subsidence of the wing titanium cage after anterior cervical interbody fusion: 2-year follow-up study. J Neurosurg Spine. 2006;4(6):447–453. | ||
Lee YS, Kim YB, Park SW. Does a zero-profile anchored cage offer additional stabilization as anterior cervical plate? Spine (Phila Pa 1976). 2015;40(10):E563–E570. | ||
Shi S, Liu Z, Li XF, Qian L, Zhong GB, Chen FJ. Comparison of plate-cage construct and stand-alone anchored spacer in the surgical treatment of three-level cervical spondylotic myelopathy: a preliminary clinical study. Spine J. 2015;15(9):1973–1980. | ||
Wang Z, Jiang W, Li X, et al. The application of zero-profile anchored spacer in anterior cervical discectomy and fusion. Eur Spine J. 2015;24(1):148–154. | ||
Nemoto O, Kitada A, Naitou S, Tachibana A, Ito Y, Fujikawa A. Stand-alone anchored cage versus cage with plating for single-level anterior cervical discectomy and fusion: a prospective, randomized, controlled study with a 2-year follow-up. Eur J Orthop Surg Traumatol. 2015;25(Suppl 1):127–134. | ||
Vanek P, Bradac O, Delacy P, Lacman J, Benes V. Anterior interbody fusion of the cervical spine with Zero-P spacer: prospective comparative study-clinical and radiological results at a minimum 2 years after surgery. Spine (Phila Pa 1976). 2013;38(13):E792–E797. | ||
Yang L, Gu Y, Liang L, et al. Stand-alone anchored spacer versus anterior plate for multilevel anterior cervical diskectomy and fusion. Orthopedics. 2012;35(10):e1503–e1510. | ||
Yang H, Chen D, Wang X, Yang L, He H, Yuan W. Zero-profile integrated plate and spacer device reduces rate of adjacent-level ossification development and dysphagia compared to ACDF with plating and cage system. Arch Orthop Trauma Surg. 2015;135(6):781–787. | ||
Wang ZD, Zhu RF, Yang HL, et al. The application of a zero-profile implant in anterior cervical discectomy and fusion. J Clin Neurosci. 2014;21(3):462–466. | ||
Li Y, Hao D, He B, Wang X, Yan L. The efficiency of zero-profile implant in anterior cervical discectomy fusion: a prospective controlled long-term follow-up study. J Spinal Disord Tech. Epub 2013 Oct 16. | ||
Qi M, Chen H, Liu Y, Zhang Y, Liang L, Yuan W. The use of a zero-profile device compared with an anterior plate and cage in the treatment of patients with symptomatic cervical spondylosis: A preliminary clinical investigation. Bone Joint J. 2013;95-B(4):543–547. | ||
Miao J, Shen Y, Kuang Y, et al. Early follow-up outcomes of a new zero-profile implant used in anterior cervical discectomy and fusion. J Spinal Disord Tech. 2013;26(5):E193–E197. | ||
Hofstetter CP, Kesavabhotla K, Boockvar JA. Zero-profile anchored spacer reduces rate of dysphagia compared with ACDF with anterior plating. J Spinal Disord Tech. 2015;28(5):E284–E290. | ||
Scholz M, Reyes PM, Schleicher P, et al. A new stand-alone cervical anterior interbody fusion device: biomechanical comparison with established anterior cervical fixation devices. Spine (Phila Pa 1976). 2009;34(2):156–160. | ||
Nayak AN, Stein MI, James CR, et al. Biomechanical analysis of an interbody cage with three integrated cancellous lag screws in a two-level cervical spine fusion construct: an in vitro study. Spine J. 2014;14(12):3002–3010. | ||
Paik H, Kang DG, Lehman RA Jr, et al. Do stand-alone interbody spacers with integrated screws provide adequate segmental stability for multilevel cervical arthrodesis? Spine J. 2014;14(8):1740–1747. | ||
Fraser JF, Hartl R. Anterior approaches to fusion of the cervical spine: a meta analysis of fusion rates. J Neurosurg Spine. 2007;6(4):298–303. | ||
Hida K, Iwasaki Y, Yano S, Akino M, Seki T. Long-term follow-up results in patients with cervical disk disease treated by cervical anterior fusion using titanium cage implants. Neurol Med Chir (Tokyo). 2008;48(10):440–446. | ||
Njoku I Jr, Alimi M, Leng LZ, et al. Anterior cervical discectomy and fusion with a zero-profile integrated plate and spacer device: a clinical and radiological study: clinical article. J Neurosurg Spine. 2014;21(4):529–537. | ||
Chen Y, Wang X, Lu X, et al. Comparison of titanium and polyetheretherketone (PEEK) cages in the surgical treatment of multilevel cervical spondylotic myelopathy: a prospective, randomized, control study with over 7-year follow-up. Eur Spine J. 2013;22(7):1539–1546. | ||
Wu WJ, Jiang LS, Liang Y, Dai LY. Cage subsidence does not, but cervical lordosis improvement does affect the long-term results of anterior cervical fusion with stand-alone cage for degenerative cervical disc disease: a retrospective study. Eur Spine J. 2012;21(7):1374–1382. | ||
Gercek E, Arlet V, Delisle J, Marchesi D. Subsidence of stand-alone cervical cages in anterior interbody fusion: warning. Eur Spine. 2003;12(5):513–516. | ||
Lee YS, Kim YB, Park SW. Risk factors for postoperative subsidence of single-level anterior cervical discectomy and fusion: the significance of the preoperative cervical alignment. Spine (Phila Pa 1976). 2014; 39(16):1280–1287. | ||
Lee MJ, Bazaz R, Furey CG, Yoo J. Influence of anterior cervical plate design on Dysphagia: a 2-year prospective longitudinal follow-up study. J Spinal Disord Tech. 2005;18(5):406–409. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.