")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Comparison of the Incidence of Cardiovascular Diseases in Weight Groups with Healthy and Unhealthy Metabolism
Authors Wang W, He J, Hu Y, Song Y, Zhang X, Guo H, Wang X, Keerman M, Ma J, Yan Y, Zhang J , Ma R, Guo S
Received 19 July 2021
Accepted for publication 9 September 2021
Published 1 October 2021 Volume 2021:14 Pages 4155—4163
DOI https://doi.org/10.2147/DMSO.S330212
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Wenqiang Wang,1,* Jia He,1,* Yunhua Hu,1 Yanpeng Song,2 Xianghui Zhang,1 Heng Guo,1 Xinping Wang,1 Mulatibieke Keerman,1 Jiaolong Ma,1 Yizhong Yan,1 Jingyu Zhang,1 Rulin Ma,1 Shuxia Guo1,3
1Department of Public Health, Shihezi University School of Medicine, Shihezi, Xinjiang, People’s Republic of China; 2Department of Social Work, The First Affiliated Hospital of Shihezi University Medical College, Shihezi, Xinjiang, People’s Republic of China; 3Department of NHC Key Laboratory of Prevention and Treatment of Central Asia High Incidence Diseases, The First Affiliated Hospital of Shihezi University Medical College, Shihezi, Xinjiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shuxia Guo
Department of Public Health, The Key Laboratory of Preventive Medicine, Building No. 1, Shihezi University School of Medicine, Suite 721, Beier Road, Shihezi, 832000, Xinjiang, People’s Republic of China
Tel +86-1800-9932-625
Fax +86-993-2057-153
Email [email protected]
Rulin Ma
Department of Public Health, The Key Laboratory of Preventive Medicine, Building No. 1, Shihezi University School of Medicine, Suite 816, Beier Road, Shihezi, 832000, Xinjiang, People’s Republic of China
Tel +86-1330-9930-561
Fax +86-993-2057-153
Email [email protected]
Background: We aimed to identify the relationship between metabolically healthy obesity (MHO), a special subtype of obesity, and the incidence of cardiovascular disease (CVD) in rural Xinjiang.
Methods: Body mass index (BMI) and the Joint Interim Statement criteria were utilized to define obesity and metabolic status, respectively. A baseline survey was conducted between 2010 and 2012. The cohort was followed-up until 2017, including 5059 participants (2953 Uyghurs and 2106 Kazakhs) in the analysis.
Results: During 6.78 years of follow-up, 471 individuals developed CVD, 10.8% (n=545) of whom were obese, and the prevalence of MHO and MHNW was 5.2% and 54.5%, respectively. Compared with metabolically healthy normal weight subjects, the subjects with MHO had an increased risk of CVD (hazard ratio [HR]=1.76, 95% confidence interval [CI]: 1.23− 2.51), while the metabolically unhealthy obesity (MUO) group had an even higher risk (HR=3.80, 95% CI: 2.87− 5.03). Additionally, there were sex differences in the relationship between BMI-metabolic status and incident CVD (Pinteraction =0.027). Compared with the subjects with MHO, those with MUO had an increased risk of CVD (HR=1.84, 95% CI: 1.26− 2.71).
Conclusion: MHO was associated with a high risk of CVD among adults in rural Xinjiang. In each BMI category, metabolically unhealthy subjects had a higher risk of developing CVD than did metabolically healthy subjects.
Keywords: metabolically healthy obesity, cardiovascular disease, rural areas, epidemiology
Introduction
Obesity is a major risk factor for diabetes, cardiovascular disease (CVD), and cancer, and is becoming a serious threat to global health.1 It is usually accompanied by a series of metabolic abnormalities, including impaired blood glucose level, elevated blood pressure, dyslipidemia, and inflammation.2 However, studies have reported that some obese individuals do not show any metabolic abnormalities, having a condition known as metabolically healthy obesity (MHO).3,4
Currently, there is no unified conclusion regarding the association between MHO and CVD. Several studies have indicated individuals with MHO have a higher risk for CVD than metabolically healthy normal weight (MHNW) subjects.5–7 Conversely, other studies have reported no difference in CVD risk between MHNW and MHO populations.8,9 The inconsistent results may be due to the differences in age, sex, race, and diagnostic criteria (metabolism and obesity) among the participants. Furthermore, a meta-analysis found that the follow-up duration (<10 or >10 years) can affect the relationship between MHO and CVD.10
Xinjiang, located in northwest China, is a multi-ethnic region. Different ethnic groups exhibit differences in genetic backgrounds, eating habits, and behaviors. The Uyghurs and Kazakhs are the main ethnic minorities in Xinjiang, comprising approximately 54% of Xinjiang’s total population. High morbidity from CVD in these populations is due to the high prevalence of obesity.11 Yang et al found that associated components of metabolic syndrome increased the risk of CVD in Kazakhs.12 However, there are limited reports on the association of MHO with CVD in Xinjiang. Therefore, this study included ethnic minorities in rural Xinjiang to explore the association between MHO and the risk of incident CVD based on Yang’s study.12 We aimed to provide supporting evidence to the preventive measures for CVD in the area.
Methods
Subjects
This study was conducted in rural Xinjiang. The population sampling method has been described previously.13 A baseline survey was performed from April 2010 to December 2012, during which we investigated 6736 participants aged ≥18 years who had been local residents for at least six months. Participants were followed-up until December 2017, with an average follow-up time of >5 years. We excluded 1677 participants due to reasons as follows: body mass index (BMI) <18.5 kg/m2 (n=316), incomplete anthropometric or laboratory data (n=178), preexisting CVD (n=895), and loss to follow-up (n=288). Consequently, 5059 eligible subjects were included in the final analysis.
Data Collection
Data were collected using questionnaires, as well as from physical and laboratory examinations. Standardized questionnaires, which include general demographic information, behavior and lifestyle, dietary habits, and disease history, were administered in the form of face-to-face interviews. Smoking was defined as consuming >100 cigarettes or consistently smoking for 6 months.14 Drinking was defined as drinking alcoholic beverages (beer, red wine, and white wine) ≥2 times per month.15 A previous study reported the methods for measuring height, weight, blood pressure and collecting blood samples.16 BMI was calculated as weight (kg)/height (m)2. Fasting plasma glucose (FPG), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), and other biochemical indicators were evaluated using an automatic biochemical analyzer (Olympus AU 2700; Olympus Diagnostics, Hamburg, Germany) at the Laboratory Department of the First Affiliated Hospital of Shihezi University School of Medicine.
Definitions
The subjects were classified as normal weight (BMI 18.5–23.9 kg/m2), overweight (BMI 24.0–27.9 kg/m2), and obese (BMI≥28.0 kg/m2) based on the recommendation of the Working Group on Obesity in China.17 The metabolic syndrome (MS) components in the Joint Interim Statement (JIS)18 were used to define metabolic status. Metabolically healthy was defined as having ≤ 2 of the following five components: (1) waist circumference (WC) of ≥85 cm for men or ≥80 cm for women, (2) TG ≥1.7 mmol/L, (3) systolic blood pressure (SBP) ≥130 mmHg or diastolic blood pressure (DBP) ≥85 mmHg, (4) FPG ≥5.6 mmol/L, and (5) HDL-C of <1.0 mmol/L for men or <1.3 mmol/L for women. According to the above definition of metabolic status and BMI, the participants were divided into six phenotypes: MHNW, metabolically healthy overweight, MHO, metabolically unhealthy normal weight (MUNW),metabolically unhealthy overweight, and metabolically unhealthy obesity (MUO).
Outcome Ascertainment
According to the WHO-MONICA protocol standard,19 the diagnosis of CVD was made during follow-up for those who had coronary heart disease, unstable angina (or nitroglycerin use), myocardial infarction, congestive heart failure, stroke, transient cerebral ischemia, peripheral vascular disease, or coronary intervention. CVD events were obtained from self-reported questionnaire responses and hospitalization medical records. If the same type of CVD event occurred more than once, the first CVD event was considered as the outcome event, and its onset was recorded. Self-reporting patients were required to provide clinical diagnosis certificates.
Statistical Analysis
Continuous variables were presented as the mean ± standard deviation and analyzed using analysis of variance. Categorical variables were described as numbers and percentages and were analyzed using the Chi-square test. The Cox regression model was used to evaluate the association of BMI-metabolic status and CVD incidence after adjusting for potential confounding factors. Subgroup analysis was used to observe whether the association varied by sex. Interaction was assessed using a multiplicative interaction term in the adjusted model. Data were analyzed using SPSS 20.0 (SPSS Inc., Chicago, IL, USA). All tests were two-sided, and statistical significance was set at P <0.05.
Results
Baseline Characteristics
We included 5059 individuals in this study, of whom 471 developed CVD during a median follow-up of 6.78 years. The overall CVD incidence was 9.3% (17.0% and 31.4% in MHO subjects and in MUO subjects, respectively). Of the participants, 10.8% (n=545) were obese and 76.8% (n=3886) were metabolically healthy (Table 1). The prevalence of MHO and MHNW was 5.2% and 54.5%, respectively. Compared with the MUO phenotype, MHO subjects were younger, included a higher proportion of women, and had a healthier metabolic state. The levels of TG, FPG, SBP, DBP, and low-density lipoprotein cholesterol in MHO individuals were lower than those in MUO individuals, while the HDL-C level was higher than in MUO individuals.
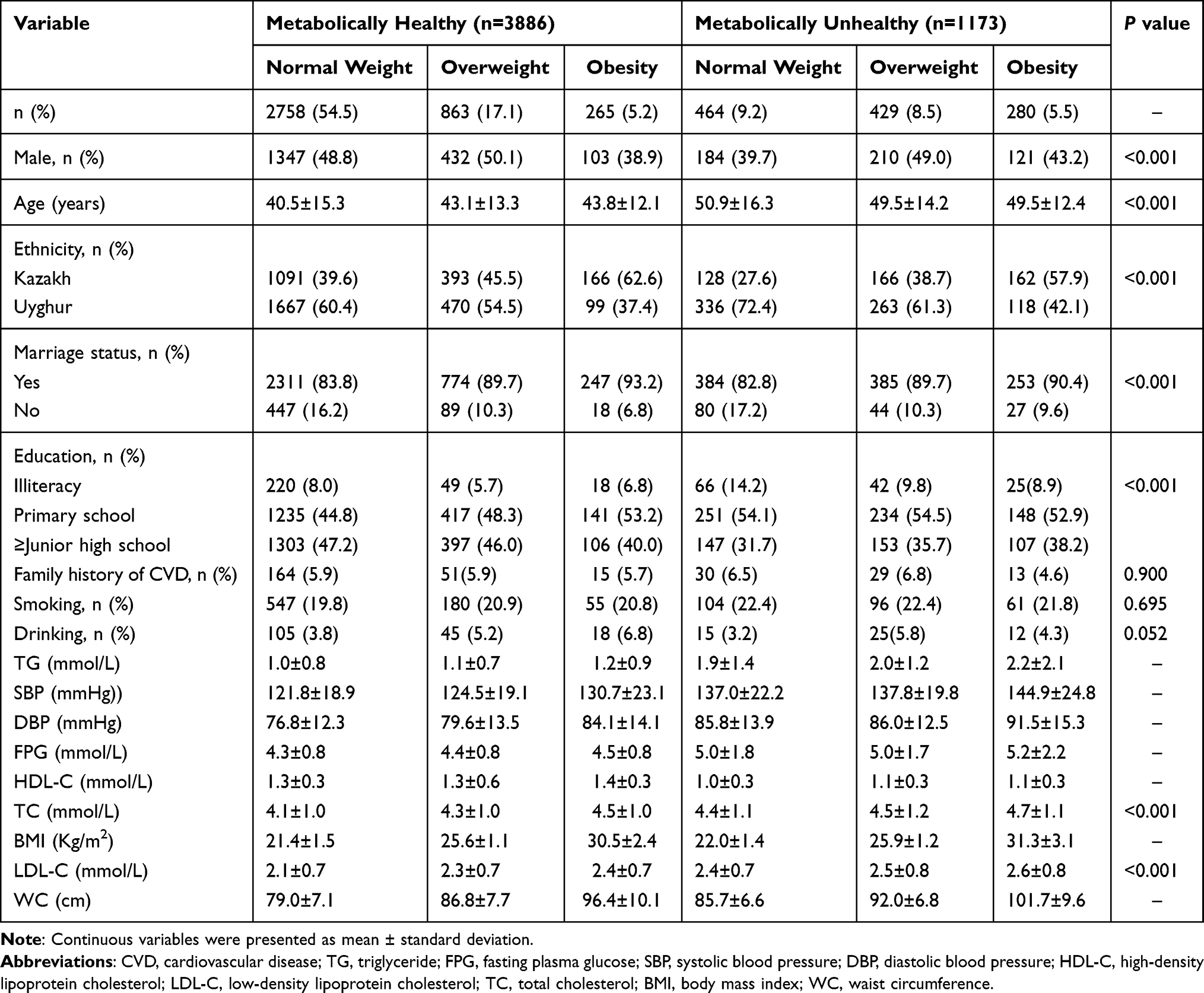 |
Table 1 Baseline Characteristics of Study Population Based on Metabolic Health Status and BMI |
Association Between BMI Categories, JIS Components, Metabolic Status, and Incident CVD
Compared with the normal weight group, the overweight group had an increased risk of CVD (hazard ratio [HR]=1.57, 95% confidence interval [CI]: 1.26–1.95), and the obese group had a higher CVD risk (HR=2.27, 95% CI: 1.80–2.88) after adjusting for potential confounding factors (Table 2). All components of the JIS definition had an increased incidence of CVD, and WC was strongly associated with CVD (HR=2.37, 95% CI: 1.86–3.02). The risk of CVD increased with the number of metabolically abnormal components. The metabolically unhealthy group was associated with a higher risk of CVD (HR=2.34, 95% CI: 1.94–2.82) than the metabolically healthy group.
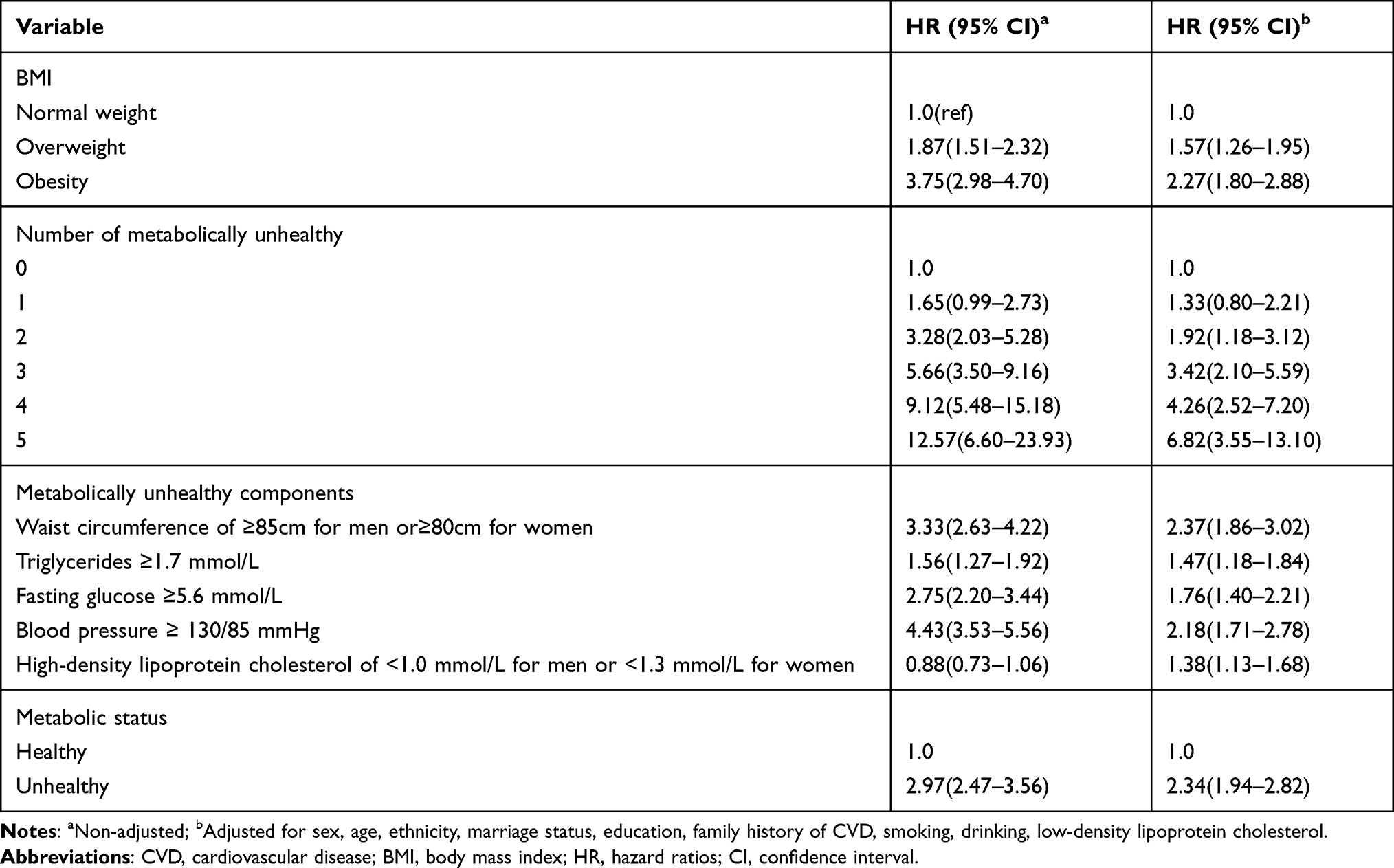 |
Table 2 The Association of BMI, Number of Metabolically Unhealthy, Metabolically Unhealthy Component and Metabolic Status with CVD |
Association of BMI-Metabolic Status with Incident CVD
After adjusting for potential confounding factors, compared with the MHNW group, the five other groups had an increased risk of CVD (Figure 1). The risk of CVD in the MHO group was 1.76-fold higher than that in the MHNW group (HR=1.76, 95% CI: 1.23–2.51), and the MUO group had the highest risk of CVD (HR=3.80, 95% CI: 2.87–5.03).
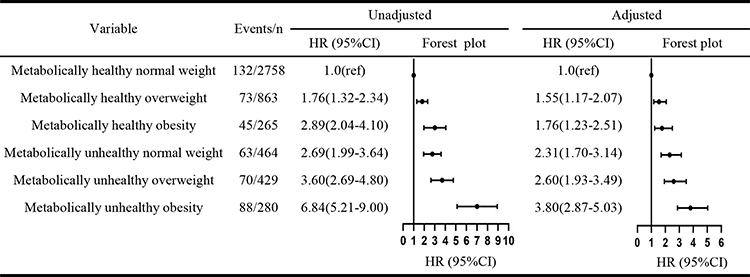 |
Figure 1 Relationship between BMI-metabolic status and incident CVD. Abbreviations: BMI, body mass index; CVD, cardiovascular disease; HR, hazard ratios; CI, confidence interval. Notes: Left, non-adjusted; Right, adjusted for sex, age, ethnicity, marriage status, education, family history of CVD, smoking, drinking, low-density lipoprotein cholesterol. |
Association of Metabolic Status Stratified by BMI Category with Incident CVD
Study participants were stratified according to BMI. In normal weight, overweight, and obese subjects, metabolically unhealthy subjects had a higher risk of CVD than metabolically healthy subjects. The HR values (95% CI) of the three groups were 2.23 (1.63–3.05), 1.94 (1.37–2.76), and 1.84 (1.26–2.71), respectively (Table 3).
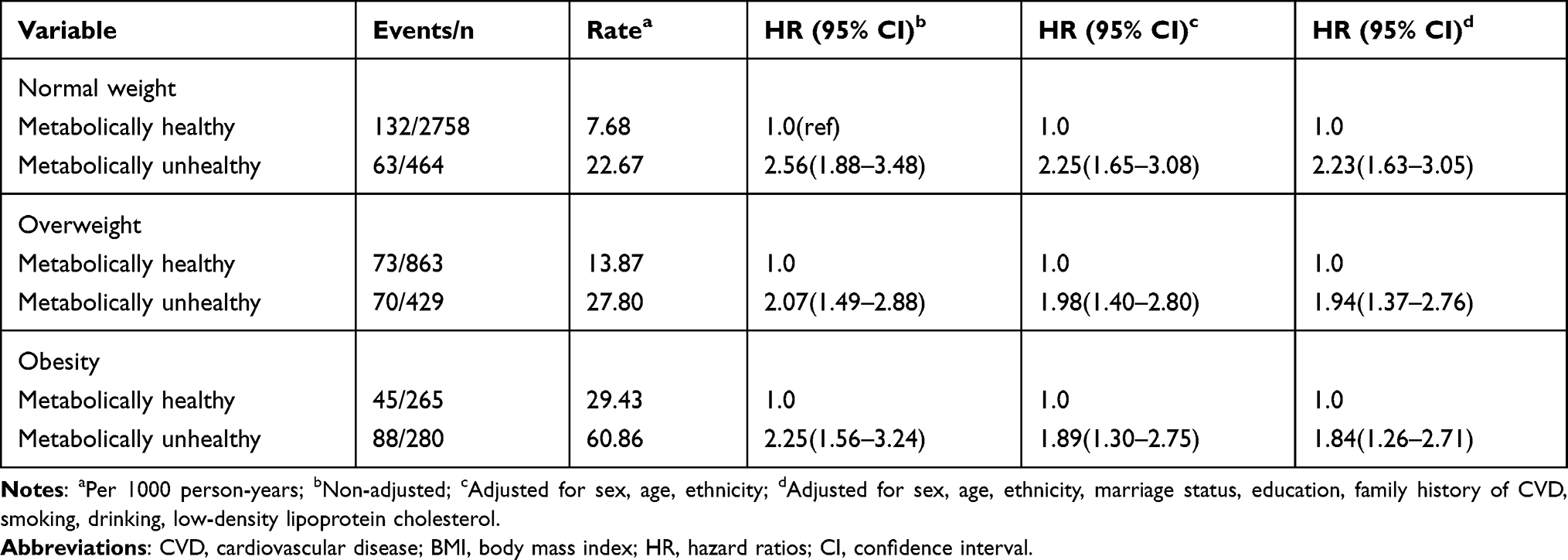 |
Table 3 The Association of Metabolic Health Status with CVD Based on BMI Category |
Subgroup Analysis According to Sex
Figure 2 shows the association of BMI-metabolic status with incident CVD by sex. The HRs were different across strata by sex (males or females) (Pinteraction =0.027). Male subjects in the MHO group were found to have a higher risk of CVD (HR=2.26, 95% CI: 1.36–3.78) than male MHNW subjects.
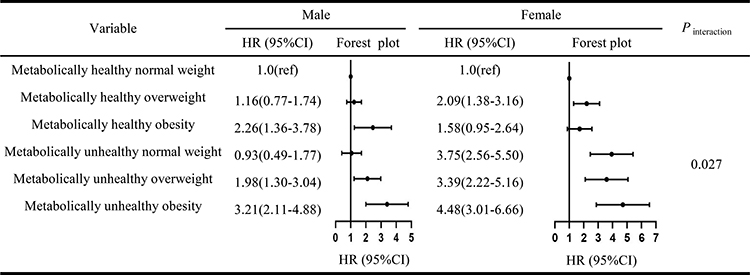 |
Figure 2 Subgroup analysis according to sex. Abbreviations: HR, hazard ratios; CI, confidence interval. Notes: Left, male; Right, female; Model was adjusted for age, ethnicity, marriage status, education, family history of CVD, smoking, drinking, low-density lipoprotein cholesterol. |
Discussion
This study found that nearly 80% of adults in rural Xinjiang were metabolically healthy, while 10.8% were obese. The prevalence of MHO and MHNW were 5.2% and 54.5%, respectively. MHO subjects had a lower age, higher proportion of women, and healthier metabolic state than MUO subjects. Compared with MHNW subjects, MHO subjects were at an increased risk of CVD, and MUO subjects had a higher risk of CVD. Subgroup analysis revealed sex differences in the relationship between BMI-metabolic status and incident CVD. Among the normal weight, overweight, and obese subjects, the metabolically unhealthy group had a higher risk of CVD than the metabolically healthy group.
At present, the association between MHO and CVD incidence remains controversial. Several studies conducted in European, American, and Korean populations (follow-up period >10 years) observed that the MHO group had a higher risk of CVD than the MHNW group,20–23 which was consistent with our results. However, other studies (follow-up period <10 years) found that the CVD risk in MHO and MHNW individuals was similar.24,25 The inconsistency may be related to the length of the follow-up period. One study indicated that the possibility of a time lag of 10−15 years before the effect of metabolic status becomes evident.26 Although the follow-up duration of this study was <10 years, it still showed that individuals with MHO have a higher risk of developing CVD than individuals with MHNW. This may be related to the high prevalence of obesity in rural Xinjiang.16 A large cohort study from Finland showed that the risk of heart failure in obese men and women was 1.99-fold and 2.06-fold higher than that in normal weight individuals, respectively.27 Another meta-analysis comprising 31 cohort studies found that the risk of coronary heart disease increased by 29% for every five-unit increase in BMI and remained elevated by 16%, even after adjusting for blood pressure and lipids.28 This indicates that MHO is not a benign state and suggests that individuals with MHO need to improve their lifestyle (exercise and healthy diet) to reduce weight, thereby decreasing the risk of CVD. In present study, we observed a significantly positive association for MHO and risk of CVD in men but not in women. This may be explained by the different hormone levels between sexes.
Studies demonstrated that MUO individuals were associated with a higher risk of CVD than MHO subjects,9,29 which is consistent with the present study findings. Eckel et al followed 90,257 subjects for 24 years and reported that up to 93.9% of MHO subjects at baseline converted to MUO individuals at the end of the follow-up.22 This emphasizes the need for MHO subjects to regularly assess their related metabolic indicators to delay the conversion from MHO to MUO. However, other studies reported similar risks of incident CVD between MHO and MUO subjects.21,30 The reason for the difference may be attributable to differences in race, age, and sex in studies. Our results indicated that in normal weight subjects, the risk of incident CVD in metabolically unhealthy individuals was also higher than in metabolically healthy individuals. Similarly, one study found that the risk of CVD in MUNW subjects was 2.04-fold higher than that in MHNW subjects.21 A study by Lee also showed that compared with MHNW subjects, the risk of CVD in MUNW subjects increased by 68%.9 One possible mechanism is that MUNW individuals present higher levels of inflammation markers, which further lead to a higher risk of CVD.31 This suggests that it is necessary to strengthen the health monitoring of the normal weight population in the future and to avoid ignoring the screening requirements for MUNW people due to normal weight, which can still be associated with an increased risk of disease.
At present, due to the lack of uniform diagnostic criteria for metabolic health, the prevalence of MHO varies,32 which may also be the main reason for the inconsistency in the relationship between MHO and CVD risk. One study revealed that even in the same population, using different diagnostic criteria for MHO can result in different findings.5 Metabolic health has been defined based on the number of metabolically abnormal components (eg, 0–1, ≤ 2, or ≤ 3). The JIS definition, built on the Adult Treatment Panel III (ATP‐III) criteria, was used to define the metabolic state in this study. A series of studies have shown that it is more reasonable to use the ATP-III standard because its defined metabolic risk threshold has been validated in several situations.32–34 With the widespread prevalence of the MHO phenotype in obese people, studies have been increasingly conducted to elucidate its metabolic health characteristics and underlying mechanisms. Wildman’s study suggested that hormones can keep certain obese people metabolically healthy. Additionally, the location, metabolic activity, and histological characteristics, rather than quantity of adipose tissue, may be important factors affecting metabolic health among obese subjects.35 Another study indicated that an interconnection among genetic, environmental, and behavioral factors played a key role in the pathogenesis of the MHO phenotype.36
One strength of our study is that the data related to CVD events were retrieved from hospital medical records and health insurance claims, ensuring the accuracy of the data. Moreover, survey data were collected by trained health professionals. Nevertheless, this study has certain limitations. First, the participants were the Uyghur and Kazakh populations, thus limiting the generalization of study findings to other populations. Moreover, this study lacked diet and physical exercise indicators, which were not adjusted for in the analysis, and the impact of these indicators on the association between MHO and CVD risk was not evaluated. Finally, we only used BMI to define obesity, which may have led to some controversial results.37
Conclusions
Among adults in rural Xinjiang, the MHO population has a higher risk of incident CVD than the MHNW population, whereas there is an even higher risk in the MUO population. Among normal weight, overweight, and obese participants, compared with metabolically healthy subjects, metabolically unhealthy subjects are at an increased risk of incident CVD. MHO is not a benign phenotype, and obese individuals should strengthen their weight management and reduce weight reasonably.
Abbreviations
MHO, metabolically healthy obesity; CVD, cardiovascular disease; MHNW, metabolically healthy normal weight; BMI, body mass index; FPG, fasting plasma glucose; TG, triglyceride; HDL-C, high-density lipoprotein cholesterol; MS, metabolic syndrome; JIS, Joint Interim Statement; SBP, systolic blood pressure; DBP, diastolic blood pressure; WC, waist circumference; MUNW, metabolically unhealthy normal weight; MUO, metabolically unhealthy obesity; HR, hazard ratio; CI, confidence interval; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; ATP‐III, Adult Treatment Panel III.
Data Sharing Statement
The data used in this study can be obtained from the corresponding author according to reasonable requirements.
Ethics Approval and Informed Consent
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of name of the First Affiliated Hospital of Shihezi University School of Medicine (IERB No. SHZ2010LL01). All participants provided written informed consent to participate in the study. Participation was strictly voluntary, and anonymity was guaranteed.
Acknowledgments
We sincerely thank these rural multi-ethnic residents for their willingness to participate in the study. We are grateful to Nalati Township Hospital and Jiangbazi Township Hospital for providing study facilities and other assistance. Shuxia Guo and Rulin Ma are co-correspondence authors for this study. Wenqiang Wang and Jia He are co-first authors for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the National Natural Science Foundation of China (No. 81560551), the Shihezi University Innovation Outstanding Young Talents Program (Natural Science) (No. CXPY202004) and the Non-profit Central Research Institute Fund of Chinese Academy of Medical Sciences (2020-PT330-003).
Disclosure
The authors declare no conflict of interests.
References
1. Romieu I, Dossus L, Barquera S, et al. Energy balance and obesity: what are the main drivers? Cancer Causes Control. 2017;28(3):247–258. doi:10.1007/s10552-017-0869-z
2. Hamer M, Stamatakis E. Metabolically healthy obesity and risk of all-cause and cardiovascular disease mortality. J Clin Endocrinol Metab. 2012;97(7):2482–2488. doi:10.1210/jc.2011-3475
3. Byun AR, Kwon S, Lee SW, Shim KW, Lee HS. Metabolic health is more closely associated with prevalence of cardiovascular diseases or stroke than obesity: a cross-sectional study in Korean populations. Medicine. 2016;95(24):e3902. doi:10.1097/MD.0000000000003902
4. Roberson LL, Aneni EC, Maziak W, et al. Beyond BMI: the “Metabolically healthy obese” phenotype & its association with clinical/subclinical cardiovascular disease and all-cause mortality – a systematic review. BMC Public Health. 2014;14:1–12. doi:10.1186/1471-2458-14-14
5. Ogorodnikova AD, Kim M, McGinn AP, Muntner P, Khan U, Wildman RP. Incident cardiovascular disease events in metabolically benign obese individuals. Obesity. 2012;20(3):651–659. doi:10.1038/oby.2011.243
6. Li H, He D, Zheng D, et al. Metabolically healthy obese phenotype and risk of cardiovascular disease: results from the China Health and Retirement Longitudinal Study. Arch Gerontol Geriatr. 2019;82:1–7. doi:10.1016/j.archger.2019.01.004
7. Hansen L, Netterstrøm MK, Johansen NB, et al. Metabolically healthy obesity and ischemic heart disease: a 10-year follow-up of the Inter99 study. J Clin Endocrinol Metab. 2017;102(6):1934–1942. doi:10.1210/jc.2016-3346
8. Mongraw-Chaffin M, Foster MC, Anderson CAM, et al. Metabolically healthy obesity, transition to metabolic syndrome, and cardiovascular risk. J Am Coll Cardiol. 2018;71(17):1857–1865. doi:10.1016/j.jacc.2018.02.055
9. Lee HJ, Choi EK, Lee SH, Kim YJ, Han KD, Oh S. Risk of ischemic stroke in metabolically healthy obesity: a nationwide population-based study. PLoS One. 2018;13(3):e0195210. doi:10.1371/journal.pone.0195210
10. Zheng R, Zhou D, Zhu Y. The long-term prognosis of cardiovascular disease and all-cause mortality for metabolically healthy obesity: a systematic review and meta-analysis. J Epidemiol Community Health. 2016;70(10):1024–1031. doi:10.1136/jech-2015-206948
11. He J. Investigation and research on the epidemiological characteristics of obesity among rural residents of Kazakh and Uyghur Nationalities in Xinjiang. Shihezi University; 2014.
12. Yang W, Guo S, Wang H, et al. The Association of Metabolic Syndrome with the development of cardiovascular disease among Kazakhs in remote rural areas of Xinjiang, China: a cohort study. BMC Public Health. 2021;21(1):216. doi:10.1186/s12889-021-10241-w
13. Jiang Y, Ma R, Guo H, et al. External validation of three atherosclerotic cardiovascular disease risk equations in rural areas of Xinjiang, China. BMC Public Health. 2020;20(1):1471. doi:10.1186/s12889-020-09579-4
14. Centers for Disease Control and Prevention. Cigarette smoking among adults–United States, 1992, and changes in definition of smoking. Morb Mortal Wkly Rep. 1994;43(19):342–346.
15. Sun K, Ren M, Liu D, Wang C, Yang C, Yan L. Alcohol consumption and risk of metabolic syndrome: a meta-analysis of prospective studies. Clin Nutr. 2014;33(4):596–602. doi:10.1016/j.clnu.2013.10.003
16. He J, Guo S, Liu J, et al. Ethnic differences in prevalence of general obesity and abdominal obesity among low-income rural Kazakh and Uyghur adults in far western China and implications in preventive public health. PLoS One. 2014;9(9):e106723. doi:10.1371/journal.pone.0106723
17. Zhou BF. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults–study on optimal cut-off points of body mass index and waist circumference in Chinese adults. Biomed Environ Sci. 2002;15(1):83–96.
18. Alberti KG, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation. 2009;120(16):1640–1645.
19. WHO MONICA Project Principal Investigators. The World Health Organization MONICA Project (monitoring trends and determinants in cardiovascular disease): a major international collaboration. J Clin Epidemiol. 1988;41(2):105–114. doi:10.1016/0895-4356(88)90084-4
20. Thomsen M, Nordestgaard BG. Myocardial infarction and ischemic heart disease in overweight and obesity with and without metabolic syndrome. JAMA Intern Med. 2014;174(1):15–22. doi:10.1001/jamainternmed.2013.10522
21. Hinnouho GM, Czernichow S, Dugravot A, et al. Metabolically healthy obesity and the risk of cardiovascular disease and type 2 diabetes: the Whitehall II cohort study. Eur Heart J. 2015;36(9):551–559. doi:10.1093/eurheartj/ehu123
22. Eckel N, Li Y, Kuxhaus O, Stefan N, Hu FB, Schulze MB. Transition from metabolic healthy to unhealthy phenotypes and association with cardiovascular disease risk across BMI categories in 90 257 women (the Nurses’ Health Study): 30 year follow-up from a prospective cohort study. Lancet Diabetes Endocrinol. 2018;6(9):714–724. doi:10.1016/S2213-8587(18)30137-2
23. Lee H, Choi EK, Lee SH, et al. Atrial fibrillation risk in metabolically healthy obesity: a nationwide population-based study. Int J Cardiol. 2017;240:221–227. doi:10.1016/j.ijcard.2017.03.103
24. Itoh H, Kaneko H, Kiriyama H, et al. Metabolically healthy obesity and the risk of cardiovascular disease in the general population- analysis of a nationwide epidemiological database. Circ J. 2021;85(6):914–920. doi:10.1253/circj.CJ-20-1040
25. Appleton SL, Seaborn CJ, Visvanathan R, et al. Diabetes and cardiovascular disease outcomes in the metabolically healthy obese phenotype: a cohort study. Diabetes Care. 2013;36(8):2388–2394. doi:10.2337/dc12-1971
26. Sundström J, Risérus U, Byberg L, Zethelius B, Lithell H, Lind L. Clinical value of the metabolic syndrome for long term prediction of total and cardiovascular mortality: prospective, population based cohort study. BMJ. 2006;332(7546):878–882. doi:10.1136/bmj.38766.624097.1F
27. Hu G, Jousilahti P, Antikainen R, Katzmarzyk PT, Tuomilehto J. Joint effects of physical activity, body mass index, waist circumference, and waist-to-hip ratio on the risk of heart failure. Circulation. 2010;121(2):237–244. doi:10.1161/CIRCULATIONAHA.109.887893
28. Bogers RP, Bemelmans WJ, Hoogenveen RT, et al. Association of overweight with increased risk of coronary heart disease partly independent of blood pressure and cholesterol levels: a meta-analysis of 21 cohort studies including more than 300 000 persons. Arch Intern Med. 2007;167(16):1720–1728. doi:10.1001/archinte.167.16.1720
29. Voulgari C, Tentolouris N, Dilaveris P, Tousoulis D, Katsilambros N, Stefanadis C. Increased heart failure risk in normal-weight people with metabolic syndrome compared with metabolically healthy obese individuals. J Am Coll Cardiol. 2011;58(13):1343–1350. doi:10.1016/j.jacc.2011.04.047
30. Li L, Chen K, Wang AP, et al. Cardiovascular disease outcomes in metabolically healthy obesity in communities of Beijing cohort study. Int J Clin Pract. 2018;73:e13279.
31. Edgley AJ, Krum H, Kelly DJ. Targeting fibrosis for the treatment of heart failure: a role for transforming growth factor-β. Cardiovasc Ther. 2012;30(1):e30–e40. doi:10.1111/j.1755-5922.2010.00228.x
32. Hinnouho GM, Czernichow S, Dugravot A, Batty GD, Kivimaki M, Singh-Manoux A. Metabolically healthy obesity and risk of mortality: does the definition of metabolic health matter? Diabetes Care. 2013;36(8):2294–2300. doi:10.2337/dc12-1654
33. Stefan N, Fritsche A, Schick F, Häring HU. Phenotypes of prediabetes and stratification of cardiometabolic risk. Lancet Diabetes Endocrinol. 2016;4(9):789–798. doi:10.1016/S2213-8587(16)00082-6
34. Musso G, Gambino R, Bo S, et al. Should nonalcoholic fatty liver disease be included in the definition of metabolic syndrome? A cross-sectional comparison with Adult Treatment Panel III criteria in nonobese nondiabetic subjects. Diabetes Care. 2008;31(5):562–568. doi:10.2337/dc07-1526
35. Wildman RP. Healthy obesity. Curr Opin Clin Nutr Metab Care. 2009;12:438–443. doi:10.1097/MCO.0b013e32832c6db7
36. Blüher M. The distinction of metabolically ‘healthy’ from ‘unhealthy’ obese individuals. Curr Opin Lipidol. 2010;21(1):38–43. doi:10.1097/MOL.0b013e3283346ccc
37. Chrysant SG, Chrysant GS. The single use of body mass index for the obesity paradox is misleading and should be used in conjunction with other obesity indices. Postgrad Med. 2019;131(2):96–102. doi:10.1080/00325481.2019.1568019
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.