")
Back to Journals » Drug Design, Development and Therapy » Volume 15
Comparison of Stimulated Cycles with Low Dose r-FSH versus Hormone Replacement Cycles for Endometrial Preparation Prior to Frozen-Thawed Embryo Transfer in Young Women with Polycystic Ovarian Syndrome: A Single-Center Retrospective Cohort Study from China
Authors Li L, Gao DD, Zhang Y, Song JY , Sun ZG
Received 26 April 2021
Accepted for publication 11 June 2021
Published 28 June 2021 Volume 2021:15 Pages 2805—2813
DOI https://doi.org/10.2147/DDDT.S317545
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Georgios Panos
Li Li,1 Dan-Dan Gao,2 Yi Zhang,2 Jing-Yan Song,1 Zhen-Gao Sun3
1The First Clinical College, Shandong University of Traditional Chinese Medicine, Jinan, 250014, People’s Republic of China; 2The College of Traditional Chinese Medicine, Shandong University of Traditional Chinese Medicine, Jinan, 250355, People’s Republic of China; 3Reproductive and Genetic Center of Integrated Medicine, The Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jinan, 250011, People’s Republic of China
Correspondence: Jing-Yan Song; Zhen-Gao Sun Tel +86 18765800113
; +86 13708938621
Email [email protected]; [email protected]
Objective: The principal purpose of this study was to compare reproductive outcomes for stimulated cycles (STC) and hormone replacement cycles (HRC) for endometrial preparation before frozen-thawed embryo transfer (FET) in young women with polycystic ovary syndrome (PCOS).
Methods: We conducted a retrospective study of 1434 FET cycles from January, 2017 to March, 2020 in our reproductive center, in which stimulated and hormone replacement cycles were used for endometrial preparation. Pregnancy outcomes of couples undergoing routine STC-FET or HRC-FET were analyzed by propensity score matching (PSM) and multivariable logistic regression analyses.
Results: Data on 1234 HRC protocols (86% of the total) and 200 STC protocols (14%) were collected. After PSM, 199 patients were included in both groups, respectively. There was no significant difference in positive pregnancy rate (52.7% vs 54.8%, p=0.763), clinical pregnancy rate (51.8% vs 52.8%, p=0.841), live birth rate (45.2% vs 43.7%, p=0.762), pregnancy loss rate (9.7% vs 16.2%, p=0.164) and ectopic pregnancy rate (1.5% vs 0.5%, p=0.615) between STC and HRC protocols. Subsequent multivariate logistic regression analysis also yielded similar results.
Conclusion: STC for endometrial preparation had similar pregnancy outcomes compared with HRC protocols. Evidence is available which shows that for young women with PCOS in preparation for FET, HRC could be a reasonable choice for patients who are unwilling to accept injections. However, STC may reduce unnecessary anxiety and operational costs and offer more flexibility for patients. Eventually, we must embrace the concepts of individualization, securitization, and optimization in the clinic.
Keywords: polycystic ovarian syndrome, stimulated cycle, hormone replacement cycle, frozen-thawed embryo transfer, endometrial preparation, propensity score matching
Introduction
The first successful frozen-thawed embryo transfer (FET) was reported in 1983 and the first live birth in 1984.1,2 Since then, elective embryo transfer and “freeze-all” strategy with segmentation of in vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI) treatment, aiming to cryopreserve all good quality embryos produced in a fresh cycle and to transfer these embryos in subsequent endometrial prepared cycles, has been widely used in assisted reproductive technology (ART) in recent years.3 FET can profoundly mitigate the risk of ovarian hyperstimulation syndrome (OHSS) and its use has now been extended to include those cycles of pre-implantation genetic diagnosis/screening, late-follicular progesterone elevation and embryo-endometrial asynchrony.4 Compared with fresh embryo transfer, FET increase maternal safety, improve pregnancy rates, decrease ectopic pregnancy rates.5 In addition, FET, avoiding the negative impact of controlled ovarian stimulation (COS) on endometrial receptivity, can provide a more physiologic uterine environment for embryo implantation with a fresh start and regrowth under alternative less intensive endometrial preparation regimens.6
PCOS is a heterogeneous endocrine disorder affecting reproductive aged women, with an estimated prevalence of between 8% and 13%.7 Patients with PCOS usually had menstrual dysfunction, infertility, hirsutism, acne, obesity, and metabolic syndrome. IVF had become an important therapeutic technique for infertility of PCOS.8 As known, PCOS patients refer to high responder group, hence, elective freeze-all strategy is recommended worldwide to prevent OHSS, and to alleviate the harmful effects of supra-physiologic steroid hormones on the endometrium before embryo implantation.9 Chen et al reported that FET increases live birth rates (LBRs) in their RCT of women with PCOS.10
Essentially, the outcomes for the FET could be affected by female age, embryo quality, endometrium and embryo synchronization, as well as endometrial receptivity, etc. If it is assumed that those factors do not differ between protocols, that endometrial preparing cycles is critical for frozen-thawed embryo transfer.11,12 There are different ways for endometrial preparation, ranging from natural cycle (NC-FET) to stimulated cycle (STC-FET), or hormone replacement cycle (HRC-FET).13 However, elucidating which is the best option remains to be determined.14 The NC cycle is suitable for patients with regular menstrual periods. The endometrium is better developed and breakthrough bleeding is less likely when the NC regimen is used. However, it is reported that premature ovulation and follicular dysplasia lead to the cancellation of cycle, especially in women with PCOS.4,15 In addition, in the light of menstrual dysfunction, the natural cycle used in the preparation of endometrium is not applicable.16 The mild ovarian stimulation induces follicular development by generating endogenous hormones. That process of follicular development and ovulation is important to function of the corpus luteum. What calls for special attention is that the initial dosing of gonadotropins (Gn) should be low for preventing the risk of OHSS. Women also should be monitored closely.15 The most commonly used FET protocol for women with PCOS is the HRC. This cycle is easy to plan, thus improving patient convenience.17 The main reasons for canceling cycles in HRC group were related to an inadequate endometrial response.15,18
Currently, there are few data comparing stimulated cycles with hormone replacement cycles for FET, especially in PCOS patients. A recent meta-analysis indicated that, compared with the hormone replacement cycles (HRC), the letrozole stimulation cycle may have a lower miscarriage rate (MR). No significant difference had been found between the mild ovarian stimulation (OS) cycle and AC protocols in live birth rate (LBR), ongoing pregnancy rate (OPR), clinical pregnancy rate (CPR) and embryo implantation rate (IR),17 some researches were opposed to this meta in artificial and stimulated cycle for FET in PCOS.18,19 The main objective of this study was to compare reproductive outcomes for stimulated and hormone replacement endometrial preparation protocols in frozen embryo transfer (FET) cycles of PCOS. To minimize potential biases, we applied the PSM method to implement post-hoc randomization.20
Materials and Methods
Study Design and Participants
We performed a retrospective cohort study of 1434 FET cycles of PCOS from January 2017 to March 2020 in the fertility unit at a University Hospital. Patients in this present study had previously undergone treatment by IVF or intracytoplasmic sperm injection (ICSI) cycles. The study was approved by the Reproductive Ethics Committees of the Affiliated Hospital of Shandong University of TCM (ref approval no. SDTCM20201215). All participants provided written informed consent. Eligible patients included women with PCOS aged between 21 and 35 years, diagnosed by Rotterdam criteria:21 oligo-or anovulation, clinical or biochemical evidence of hyperandrogenism, and polycystic ovarian morphology on ultrasonography (defined as an ovary that either contains ≥12 antral follicles or that has a volume >10 cm3), with at least one embryo vitrified mainly at day 3, and for whom it was the first FET performed. The exclusion criteria were: (i) Body Mass Index (BMI) ≥30Kg/m2 at the time of embryo vitrification; (ii) Endometriosis; (iii) Preimplantation genetic diagnosis/screening cycle; (iv) History of recurrent pregnancy loss or recurrent implantation failure; (v) Uterine pathology; (vi) Cycles cancelled due to failure of embryo thawing and survival.
Controlled Ovarian Stimulation Protocol
All participants had undergone the IVF/ICSI treatment as clinically indicated. Furthermore, a flexible GnRH antagonist (GnRH-ant) (Cetrorelix; Merck Serono, Darmstadt, Germany) and long GnRH-a (Triptorelin, Decapeptyl, Ipsen, France) protocols were employed with 150–225 IU/day of recombinant FSH (Gonal-F, Merck-Serono, Lyon, France). Additionally, the doses of gonadotropin were determined based on the characteristics of individual patients. Thereafter, oocyte retrieval was conducted under ultrasound transvaginal guidance, 34–36 hours after triggering with 0.1mg GnRH-a or recombinant hCG (Ovitrelle®, 250μg, Merck), after which conventional IVF/ICSI were performed as previously described.22 The IVF/ICSI procedure had either been followed by a fresh embryo transfer and preservation of the redundant good embryos by vitrification or by a freeze-all strategy on clinical indication. Regular monitoring during controlled ovarian hyperstimulation (COS) treatment includes vaginal ultrasound (to assess endometrial thickness and follicle development) and blood hormone assays (including estradiol, progesterone and LH plasma levels).
The choice of embryos for vitrification was expected to focus on the inclusion of no less than six blastomeres with ≤20% fragmentation. Embryos that presented a fragmentation rate between 20% and 50% were vitrified only when they had reached the 8-cell stage on Day 3. The applied vitrification procedure has been described in detail before.22
Endometrial Preparation Protocols
Women with PCOS were instructed to wait for spontaneous menses or prescribed with progestin to induce menses before endometrial preparation.23 The two endometrial preparation protocols used before the FET were the following:
Hormone Replacement Cycles
In hormone replacement cycles, 4 mg of oral estradiol valerate was administered starting on the second or third day of the menstrual cycle and continuing for five days. This was followed by 6 mg of oral estradiol for 6–8 days. When the endometrial thickness reached 7 mm and the serum progesterone level was below 1.5 ng/mL, we added vaginal supplementation with progesterone 90 mg daily (8% Crinone, Merck-Serono, Switzerland) prior to FET. The embryo was transferred according to its development stage at the time of freezing. The supplementation continued until a pregnancy test was performed. In case of a positive test, the patients were instructed to continue treatment until the 10th gestational week.24
Stimulated Cycles
In stimulated cycles, patients received a daily subcutaneous injection of Gonarfen (Merck Serono SA Aubonne Branch) (37.5–75 IU) from day 5 of the cycle onwards. The dose was adjusted according to the BMI, the ovarian reserve and any previous ovarian response to stimulation. A subcutaneous injection of hCG (5000 IU) or recombinant hCG (250 μg) was administered to induce oocyte ovulation, when the ovulation criteria were met (one dominant follicle ≥16 mm and peak plasma estradiol level >200 pg/mL). These patients had no intercourse on ovulation day. The adequacy of the luteal phase was evaluated by measuring blood progesterone levels three days after ovulation had been triggered. If the progesterone level 3 days after ovulation triggering exceeded 3 ng/mL, FET was implemented (depending on the embryo’s development stage at the time of freezing). STC protocols for endometrial preparation were not supplemented with progesterone.25
Study Endpoints and Definitions
Positive pregnancy was defined as a serum β-hCG level greater than 10 IU/L in the 14 days after cleavage embryo transfer.26,27 The patient underwent ultrasonographic monitoring to determine the number of gestational sacs and fetal viability at the 6th-7th week of gestation, ie, clinical pregnancy, if the β-hCG assay yielded a positive result. Pregnancy loss was defined as clinically recognized spontaneous loss of pregnancy before the completion of twenty gestational weeks. Ectopic pregnancy, defined as a pregnancy in which implantation takes place outside the uterine cavity, diagnosed by ultrasound, surgical visualization or histopathology. Live birth, defined as the birth of at least one child with breath and heartbeat, irrespective of the duration of gestation. A birth weight of 3500 g or more can be used if gestational age is unknown. Furthermore, this pathological state in which the death of a fetus prior to the complete expulsion from its mother after 20 completed weeks of gestational age was diagnosed as stillbirth. As opposed to live birth, the fetus does not breathe or show any other evidence of life.
Statistical Analysis
All data are evaluated using version 26.0 of SPSS program (SPSS Inc., Chicago, USA). Shapiro–Wilk test was used to assess data normality. Quantitative variables are expressed as means ± standard deviations (SD) or median (range) and were analyzed using Student’s t-test (normal distribution), Independent-Samples Mann–Whitney U-Test (when normal distribution was not obeyed). Qualitative variables are expressed as frequencies and percentages and were analyzed using the χ2-test. P< 0.05 was considered statistically significant for the two groups of data tested. Furthermore, a propensity score matching (PSM) model was established to balance differences in baseline characteristics between the two groups.20 The propensity scores were calculated using binary logistic regression analyses based on the following patients’ characteristics: female age, infertility duration, body mass index (BMI), infertility type (primary or secondary), AMH, protocol of COS (Long GnRH-a protocol or GnRH-ant protocol), initial treatment (IVF or ICSI), Gn usage time, Gn dosage, oocytes retrieved, total number of embryos, good quality embryos, transferred embryos.28 Patients undergoing STC were matched with the HRC group using the nearest-neighbor random matching algorithm in a ratio of 1:1. In our study, we also used binary logistic regression analysis to assess the association between endometrial preparation protocols and pregnancy outcomes. We calculated crude odds ratios (OR) and adjusted OR with 95% confidence interval (CI).
Results
Demographic and ART Characteristics of Patients
One thousand four hundred and thirty-four cycles undergoing IVF or ICSI who had been performed the first freeze-thaw embryo transfer were studied. In detail, A total of 200 (14%) patients received STC, and 1234 (86%) underwent HRC before FET. Simultaneously, the 199 cycles were matched after PSM. Patient characteristics before and after PSM for STC and HRC groups are presented in Table 1. There were significantly different between two groups in initial treatment, good quality embryos, transferred embryos of D3 before PSM. Furthermore, no significant differences were found regarding patient characteristics between two groups after PSM.
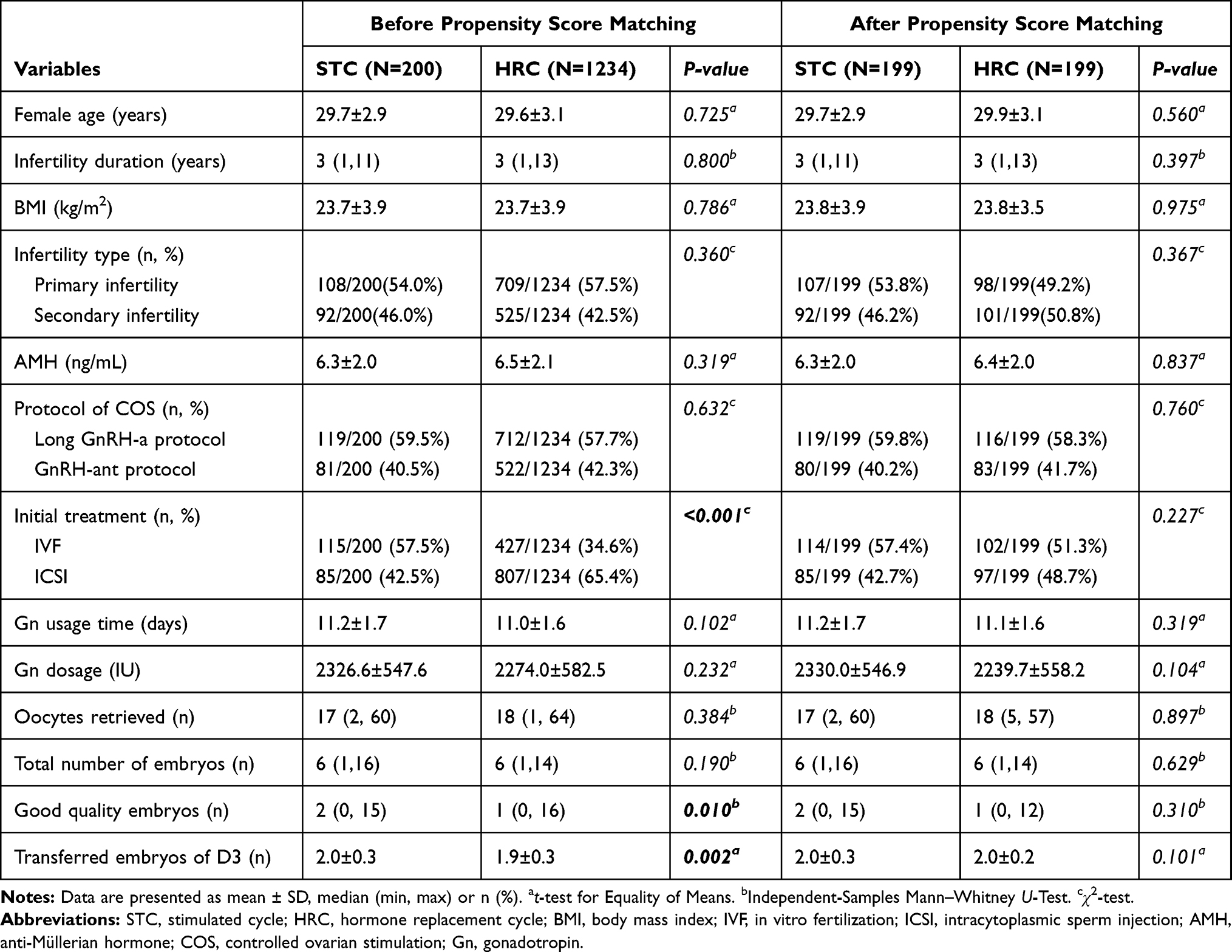 |
Table 1 Patient Characteristics for HRC and STC Groups |
Pregnancy Outcome Measures
Pregnancy outcomes reflected by matched FET method are shown in Table 2. However, no statistical significance was detected between STC and HRC groups in terms of positive pregnancy rate (PPR), clinical pregnancy rate (CPR), live birth rate (LBR), pregnancy loss rate (PLR) and ectopic pregnancy rate (EPR). (all P > 0.05)
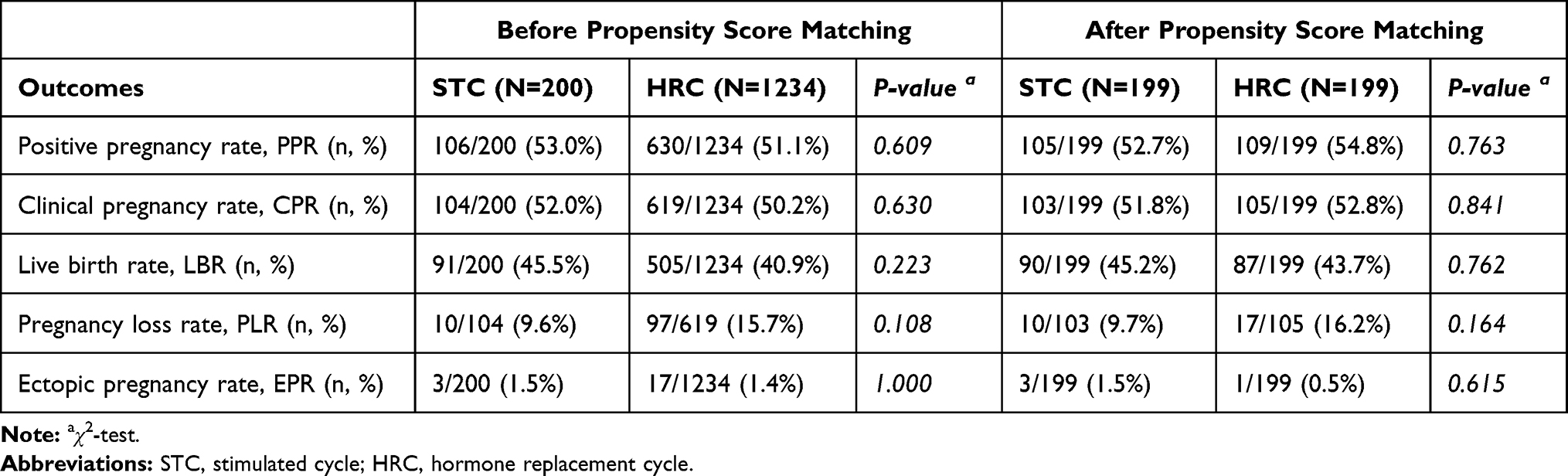 |
Table 2 Pregnancy Outcomes for HRC and STC Groups |
A binary logistic regression model was also used to assess the association between endometrial preparation protocols and pregnancy outcomes while adjusting for potential confounders (Table 3). In the crude and adjusted models, the STC group was comparable to the HRC group in terms of PPR, CPR, and LBR.
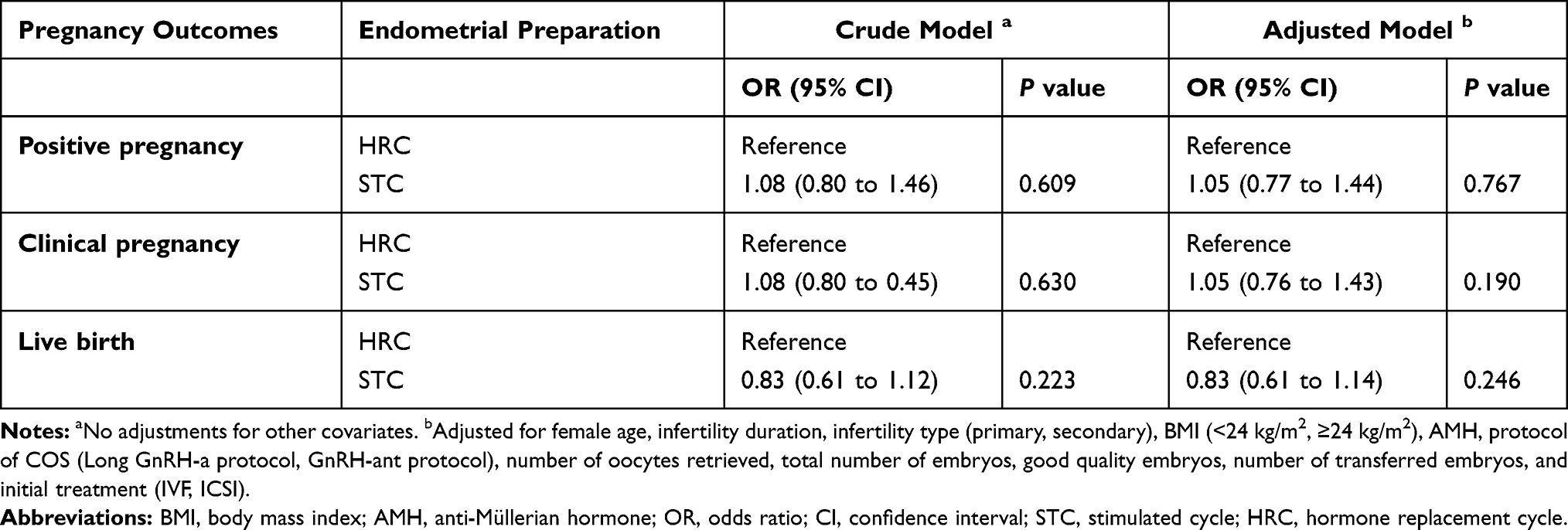 |
Table 3 Relationship Between Endometrial Preparation and Pregnancy Outcomes in Different Models |
Discussion
To our best knowledge, few studies have evaluated the different ways in which endometrium is prepared in young women with PCOS. In comparison to previous research, our practice can provide evidence-based guidance to select suitable endometrium preparation protocols for FET based on post-hoc randomization and large sample. In the current retrospective cohort analysis, we compared two different endometrial preparation protocols for FET with STC and HRC. Our findings showed that there was no statistical significance in the pregnancy outcomes between two groups.
PCOS resulted in infertility could have been attributed to anovulation as well as endometrial dysfunction which affect endometrial receptivity.16 In particular, hyperandrogenism and high level of LH during the follicular phase may decrease the rate of conception, the latter may lead to poor oocyte quality and embryo quality. Tomas et al noticed that the hormone replacement therapy (HRT) population has a higher pregnancy loss risk, which could be correlated with a higher prevalence of PCOS.29 Few studies have compared OS with HRT of PCOS patients in the reproductive outcomes. Most literature focuses on live birth rates and clinical pregnancy rates. In accordance with our outcomes, some literatures had the similar conclusion in HRT versus OS.17,30 In Yu et al retrospective study, the two protocols resulted in LPR (30.0% vs 31.7%), CPR (41.0% vs 41.6%), OPR (36.6% vs 34.7%), which were not statistically different. In addition, there is a relatively high cycle cancellation rate in stimulated cycle.18 A systematic review and meta-analysis in 2016 similarly found STC and HRC endometrial preparation protocols are equally effective, despite the low quality of evidence, for women with PCOS.19 A systematic review and meta-analysis including pooled results of only two studies of PCOS patients found letrozole produces similar CPR, LBR, and birth defect rates as NC and HRC; there were similar CPR and lower LBR in letrozole-stimulated cycle compared to HMG stimulation.32 Added to Chen et al conclusions, a recent meta-analysis comparing OS using letrozole or HMG with HRT for FET in patients with PCOS found no difference between mild OS cycles and HRT groups for OPR and embryo implantation rate (IR); the letrozole-stimulated cycle may lower the miscarriage rate more than the HRT cycle.17,32 Multiple retrospective cohort studies pointed out a different view, letrozole-stimulated cycle had significantly higher LBR and lower PLR compared with HRT after adjusting for possible confounding factors.33–35 Therefore, whether letrozole has an advantage in preparing FET requires more high-quality researches for confirmation. In contrast with our findings, in a recent historical cohort analysis on women with PCOS, OS protocol achieves a better pregnancy outcome than the HRT protocol. In detail, that LBR with HRT accompanied by the poorest endometrial thickness, is lower than OS with low doses of human menopausal gonadotropin.15 Peigne et al verified the same perspective, despite a similar CPR (24.4% vs 20.8%), LBR (17.1% vs 9.8%) was significantly higher with mild OS than with HRT preparation, even after adjusting for potential bias, such as patient age at freezing, PCOS, and so on.24 In Jouan et al’s retrospective study, he demonstrated the superiority of clomiphene citrate cycles over HRC not only in OPR but also CPR.36 Although Hatoum et al concluded that HRC were associated with more PLR and lower LPR than stimulated cycles, the parameters affecting the results of statistical analysis were not described and/or adjusted.25 We can find that there is no comparative study on OS with low dose r-FSH versus HRT in previous studies.
Previous studies have shown that HRC protocol can easily lead to the lack of corpus luteum and the elevated incidence of hypertensive disorders of pregnancy and preeclampsia, which did not exist in natural or stimulated FET cycles.37,38 This may cause changes in the structure and/or function of the extracellular matrix in the decidual layer and was associated with underdevelopment decidual layer after pregnancies.39 Excessive estrogen may have adverse effects on the pregnancy outcome of anovulatory women, resulting in lower LBR.15,40 Embryo implantation is not only related to the serum progesterone level but also the inner membrane.25 When the progesterone value exceeded 20 ng/dl which is associated, overall pregnancy rate and live birth rate would become lower, spontaneous abortion rate and biochemical pregnancy rate become higher.41 Although thin endometrium is associated with lower success rate,42 implantation is related to the endometrial pattern, not to the thickness of the endometrium.43
According to the present research, it is unclear whether technique will result in a superior pregnancy outcome in FET.44,45 Once estradiol stimulation has resulted in an endometrial thickness more than 7 mm in HRC, progesterone may be introduced at any time that is convenient. The disadvantage is that in the event of pregnancy, a protracted dual hormonal therapy is necessary. STC, on the other hand, requires more transvaginal ultrasound examinations, urine LH measurement, precise hCG injection timing, and subsequent FET in order to prevent missing the implantation window. As a result, HRC might be a viable option for young PCOS patients undergoing IVF-ET and being unable to take injections. STC may reduce unnecessary anxiety and operational costs, and offer more flexibility for patients. Eventually, we must embrace the concepts of individualization, securitization, and optimization in the clinic.
Although this study has the advantage of using PSM to balance the variables that potentially affect the outcomes. Nevertheless, there are some drawbacks to this study. Every retrospective nature may not avoid completely introduced selection or information bias. First of all, we cannot investigate other confounding factors, including exercise, nutritional supplements and diet, which can add information bias. Second, since this is not an RCT, according to professional experience, patients are assigned to multiple groups, which can add selection bias.
Conclusion
In conclusion, STC for endometrial preparation had similar PPR, CPR, LBR, PLR, EPR compared with HRC by excluding heterogeneous factors after PSM. For young women with PCOS who were undergoing in-vitro fertilization-embryo transfer (IVF-ET), HRC could be a reasonable choice for patients who are unwilling to accept injections. Additionally, STC may reduce unnecessary anxiety and operational costs, and offer more flexibility for patients and IVF centres. We should follow the principles of individualization, securitization and optimization. To validate the obtained results, broader analyses, as well as an economic assessment of the costs involved, are required.
Data Sharing Statement
The data generated and analyzed from the current study will be availed by the corresponding author upon request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki. The study was approved by the Reproductive Ethics Committees of the Affiliated Hospital of Shandong University of TCM (ref approval no. SDTCM20201215). All participants provided written informed consent.
Consent for Publication
Written informed consent for publication was obtained from all participants.
Acknowledgments
We would like to thank all the participants in this study and, in particular, professor Zhen-Gao Sun for his assistance in the statistical analysis.
Author Contributions
Zhen-Gao Sun and Jing-Yan Song conceived and designed the study. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
None of the authors have a conflict of interest to declare with regard to this study.
References
1. Trounson A, Mohr L. Human pregnancy following cryopreservation, thawing and transfer of an eight-cell embryo. Nature. 1983;305(5936):707–709. doi:10.1038/305707a0
2. Zeilmaker GH, Alberda AT, van Gent I, Rijkmans CMPM, Drogendijk AC. Two pregnancies following transfer of intact frozen-thawed embryos. Fertil Steril. 1984;42(2):293–296. doi:10.1016/S0015-0282(16)48029-5
3. Bosch E, De Vos M, Humaidan P. The future of cryopreservation in assisted reproductive technologies. Front Endocrinol (Lausanne). 2020;11:11. doi:10.3389/fendo.2020.00067
4. Mackens S, Santos-Ribeiro S, van de Vijver A, et al. Frozen embryo transfer: a review on the optimal endometrial preparation and timing. Hum Reprod. 2017;32(11):2234–2242. doi:10.1093/humrep/dex285
5. Boynukalin FK, Turgut NE, Gultomruk M, et al. Impact of elective frozen vs. fresh embryo transfer strategies on cumulative live birth: do deleterious effects still exist in normal & hyper responders? PLoS One. 2020;15(6):e0234481. doi:10.1371/journal.pone.0234481
6. Wei D, Liu J-Y, Sun Y, et al. Frozen versus fresh single blastocyst transfer in ovulatory women: a multicentre, randomised controlled trial. Lancet. 2019;393.
7. Teede HJ, Misso ML, Costello MF, et al. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum Reprod. 2018;33(9):1602–1618. doi:10.1093/humrep/dey256
8. Nandi A, Chen Z, Patel R, Poretsky L. Polycystic ovary syndrome. Endocrinol Metab Clin North Am. 2014;43(1):123–147. doi:10.1016/j.ecl.2013.10.003
9. Bushaqer NJ, Alkhudhairy NN, Alturaigi ZM, et al. The effect of fresh IVF cycle characteristics on frozen embryo transfer (FET) outcomes. JBRA Assist Reprod. 2020;24(2):135–142. doi:10.5935/1518-0557.20190074
10. Chen ZJ, Shi Y, Sun Y, et al. Fresh versus frozen embryos for infertility in the polycystic ovary syndrome. N Engl J Med. 2016;375(6):523–533. doi:10.1056/NEJMoa1513873
11. Veleva Z, Orava M, Nuojua-Huttunen S, Tapanainen JS, Martikainen H. Factors affecting the outcome of frozen-thawed embryo transfer. Hum Reprod. 2013;28(9):2425–2431. doi:10.1093/humrep/det251
12. Pan Y, Hao G, Wang Q, et al. Major factors affecting the live birth rate after frozen embryo transfer among young women. Front Med (Lausanne). 2020;7:94. doi:10.3389/fmed.2020.00094
13. Wang B, Zhu Q, Wang Y. Pregnancy outcomes after different cycle regimens for frozen-thawed embryo transfer: a retrospective study using propensity score matching. Front Med (Lausanne). 2020;7:327. doi:10.3389/fmed.2020.00327
14. Ghobara T, Gelbaya TA, Ayeleke RO. Cycle regimens for frozen-thawed embryo transfer. Cochrane Database Syst Rev. 2017;7:CD003414. doi:10.1002/14651858.CD003414.pub3
15. Man Y, Bian Y, Zhao S, et al. The effect of different endometrial preparations on women with polycystic ovary syndrome undergoing initial frozen embryo transfer: a historical cohort analysis. Acta Obstet Gynecol Scand. 2021;100(6):1116–1123. doi:10.1111/aogs.14058
16. Wageh A, Fawzy M. PCOS patients; how the endometrium can be ready for frozen embryo transfer? A retrospective study. Middle East Fertil Soc J. 2018;23(4):409–412. doi:10.1016/j.mefs.2018.06.004
17. Zeng MF, Zhou X, Duan JL. Stimulated cycle versus artificial cycle for frozen embryo transfer in patients with polycystic ovary syndrome: a meta-analysis. Gynecol Endocrinol. 2021;1–6.
18. Yu J, Ma Y, Wu Z, et al. Endometrial preparation protocol of the frozen-thawed embryo transfer in patients with polycystic ovary syndrome. Arch Gynecol Obstet. 2015;291(1):201–211. doi:10.1007/s00404-014-3396-0
19. Kollmann M, Martins WP, Lima ML, et al. Strategies for improving outcome of assisted reproduction in women with polycystic ovary syndrome: systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2016;48(6):709–718. doi:10.1002/uog.15898
20. Garrido MM, Kelley AS, Paris J, et al. Methods for constructing and assessing propensity scores. Health Serv Res. 2014;49(5):1701–1720. doi:10.1111/1475-6773.12182
21. Rotterdam EA-SPCWG. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril. 2004;81(1):19–25. doi:10.1016/j.fertnstert.2003.10.004
22. Song J, Xiang S, Sun Z. Frozen embryo transfer at the cleavage stage can be performed within the first menstrual cycle following the freeze-all strategy without adversely affecting the live birth rate: a STROBE-Compliant Retrospective Study. Medicine (Baltimore). 2019;98(38):e17329. doi:10.1097/MD.0000000000017329
23. Wei D, Shi Y, Li J, et al. Effect of pretreatment with oral contraceptives and progestins on IVF outcomes in women with polycystic ovary syndrome. Hum Reprod. 2017;32(2):354–361. doi:10.1093/humrep/dew325
24. Peigne M, Devouche E, Ferraretto X, et al. Higher live birth rate with stimulated rather than artificial cycle for frozen-thawed embryo transfer. Eur J Obstet Gynecol Reprod Biol. 2019;243:144–149. doi:10.1016/j.ejogrb.2019.10.040
25. Hatoum I, Bellon L, Swierkowski N, et al. Disparities in reproductive outcomes according to the endometrial preparation protocol in frozen embryo transfer: the risk of early pregnancy loss in frozen embryo transfer cycles. J Assist Reprod Genet. 2018;35(3):425–429. doi:10.1007/s10815-017-1078-0
26. Duffy JMN, Bhattacharya S, Bhattacharya S, et al. Standardizing definitions and reporting guidelines for the infertility core outcome set: an international consensus development studydagger double dagger. Hum Reprod. 2020;35(12):2735–2745. doi:10.1093/humrep/deaa243
27. Cai H, Mol BW, Gordts S, et al. Early and late pregnancy loss in women with polycystic ovary syndrome undergoing IVF/ICSI treatment: a retrospective cohort analysis of 21 820 pregnancies. BJOG. 2020;128(7):1160–1169. doi:10.1111/1471-0528.16590
28. Williamson EJ, Forbes A. Introduction to propensity scores. Respirology. 2014;19(5):625–635. doi:10.1111/resp.12312
29. Tomas C, Alsbjerg B, Martikainen H, Humaidan P. Pregnancy loss after frozen-embryo transfer--a comparison of three protocols. Fertil Steril. 2012;98(5):1165–1169. doi:10.1016/j.fertnstert.2012.07.1058
30. Wright KP, Guibert J, Weitzen S, Davy C, Fauque P, Olivennes F. Artificial versus stimulated cycles for endometrial preparation prior to frozen–thawed embryo transfer. Reprod Biomed Online. 2006;13(3):321–325. doi:10.1016/S1472-6483(10)61434-4
31. Konc J, Kanyo K, Varga E, Kriston R, Cseh S. The effect of cycle regimen used for endometrium preparation on the outcome of day 3 frozen embryo transfer cycle. Fertil Steril. 2010;94(2):767–768. doi:10.1016/j.fertnstert.2009.09.053
32. Chen D, Shen X, Fu Y, Ding C, Zhong Y, Zhou C. Pregnancy outcomes following letrozole use in frozen-thawed embryo transfer cycles: a systematic review and meta-analysis. Geburtshilfe Frauenheilkd. 2020;80(8):820–833. doi:10.1055/a-1202-2059
33. Tatsumi T, Jwa SC, Kuwahara A, Irahara M, Kubota T, Saito H. Pregnancy and neonatal outcomes following letrozole use in frozen-thawed single embryo transfer cycles. Hum Reprod. 2017;32(6):1244–1248. doi:10.1093/humrep/dex066
34. Zhang J, Liu H, Wang Y, et al. Letrozole use during frozen embryo transfer cycles in women with polycystic ovary syndrome. Fertil Steril. 2019;112(2):371–377. doi:10.1016/j.fertnstert.2019.04.014
35. Yarali H, Polat M, Mumusoglu S, Yarali I, Bozdag G. Preparation of endometrium for frozen embryo replacement cycles: a systematic review and meta-analysis. J Assist Reprod Genet. 2016;33(10):1287–1304. doi:10.1007/s10815-016-0787-0
36. Jouan C, Emonard V, Ruggeri P, et al. Pregnancy outcome following frozen embryo transfer after artificial cycle or treatment by clomiphene citrate. Gynecol Endocrinol. 2016;32(10):807–810. doi:10.1080/09513590.2016.1177012
37. von Versen-hoynck F, Schaub AM, Chi YY, et al. Increased preeclampsia risk and reduced aortic compliance with in vitro fertilization cycles in the absence of a corpus luteum. Hypertension. 2019;73(3):640–649. doi:10.1161/HYPERTENSIONAHA.118.12043
38. Ginstrom Ernstad E, Wennerholm UB, Khatibi A, Petzold M, Bergh C. Neonatal and maternal outcome after frozen embryo transfer: increased risks in programmed cycles. Am J Obstet Gynecol. 2019;221(2):126 e121–126 e118. doi:10.1016/j.ajog.2019.03.010
39. Nakamura Y, Yaguchi C, Itoh H, et al. Morphologic characteristics of the placental basal plate in in vitro fertilization pregnancies: a possible association with the amount of bleeding in delivery. Hum Pathol. 2015;46(8):1171–1179. doi:10.1016/j.humpath.2015.04.007
40. Wei D, Yu Y, Sun M, et al. The effect of supraphysiological estradiol on pregnancy outcomes differs between women with PCOS and ovulatory women. J Clin Endocrinol Metab. 2018;103(7):2735–2742. doi:10.1210/jc.2018-00613
41. Kofinas JD, Blakemore J, McCulloh DH, Grifo J. Serum progesterone levels greater than 20 ng/dl on day of embryo transfer are associated with lower live birth and higher pregnancy loss rates. J Assist Reprod Genet. 2015;32(9):1395–1399. doi:10.1007/s10815-015-0546-7
42. Liu KE, Hartman M, Hartman A, Luo ZC, Mahutte N. The impact of a thin endometrial lining on fresh and frozen-thaw IVF outcomes: an analysis of over 40 000 embryo transfers. Hum Reprod. 2018;33(10):1883–1888. doi:10.1093/humrep/dey281
43. Gingold JA, Lee JA, Rodriguez-Purata J, et al. Endometrial pattern, but not endometrial thickness, affects implantation rates in euploid embryo transfers. Fertil Steril. 2015;104(3):620–628e625. doi:10.1016/j.fertnstert.2015.05.036
44. von Versen-hoynck F, Conrad KP, Baker VL. Which protocol for frozen-thawed embryo transfer is associated with the best outcomes for the mother and baby? Fertil Steril. 2021;115(4):886–887. doi:10.1016/j.fertnstert.2021.01.042
45. Dal Prato L, Borini A. Best protocol for frozen-thawed embryo transfer-cost benefit analysis needed. Fertil Steril. 2006;86(5):1554–1555;author reply 1555–1556. doi:10.1016/j.fertnstert.2006.05.013
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.