")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Comparison of serum B12, folate and homocysteine concentrations in children with autism spectrum disorder or attention deficit hyperactivity disorder and healthy controls
Authors Yektaş Ç , Alpay M, Tufan AE
Received 15 April 2019
Accepted for publication 10 June 2019
Published 6 August 2019 Volume 2019:15 Pages 2213—2219
DOI https://doi.org/10.2147/NDT.S212361
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Çiğdem Yektaş,1 Merve Alpay,2 Ali Evren Tufan3
1Department of Child and Adolescent Psychiatry, Düzce Üniversitesi, Düzce, Turkey; 2Department of Medical Biochemistry, Faculty of Medicine, Düzce Üniversitesi, Düzce, Turkey; 3Department of Child and Adolescent Psychiatry, Acıbadem Üniversitesi Tıp Fakültesi, Istanbul, Turkey
Objective: We aimed to investigate the serum concentrations of vitamin B12, folate and homocysteine in children diagnosed with attention deficit hyperactivity disorder (ADHD) or autism spectrum disorder (ASD) and healthy controls.
Materials and methods: Serum vitamin B12, folate and homocysteine concentrations were measured in 118 children (48 children diagnosed with ADHD, 35 children diagnosed with ASD and 35 healthy controls). Symptom severity in the ADHD and ASD groups was evaluated by the Childhood Autism Rating Scale and Turgay-DSM-IV-Based Screening and Assessment Scale for Disruptive Behavior Disorders. Multivariate analysis of covariance was used to evaluate the effects of diagnosis and gender on biochemical parameters.
Results: The ADHD and ASD groups and the healthy controls differed significantly regarding vitamin B12 and homocysteine concentrations, but not folate levels. Patients with ASD had the lowest vitamin B12 and the highest homocysteine levels. Vitamin B12 levels correlated negatively with hyperactivity and/orimpulsivity and oppositionality symptoms in children with ADHD. There were no relationships between psychometric evaluations and laboratory measurements in children with ASD. Gender did not affect vitamin concentrations.
Conclusion: Previous studies found that vitamin B12 was reduced while homocysteine was elevated among patients with ADHD and ASDs. Our results also support those reported previously. Oppositionality and hyperactivity and/orimpulsivity may be related to vitamin B12 and homocysteine levels in children with ADHD. Further studies are required to define the role of these parameters and effects on the etiology and clinical manifestations of ASD and ADHD.
Keywords: vitamin B12, folate, homocysteine, attention deficit hyperactivity disorder, autism spectrum disorder
Introduction
Although both autism spectrum disorder (ASD) and attention deficit hyperactivity disorder (ADHD) are highly heritable neurodevelopmental disorders, approximately 70.0–80.0% of the phenotypic variance of each disorder could be explained by genetic factors.1 An increase in the prevalence of ASD and ADHD has stimulated research on etiology of these neurodevelopmental disorders, including environmental factors such as vitamins which have important roles in central nervous system (CNS) functioning.2,3
Vitamin B12 and folate play important roles in the development, differentiation, and functioning of the CNS.4 They are involved in the methionine-homocysteine pathway, which is responsible for the methyl groups required for DNA and protein synthesis.4,5
In case of deficiencies, there is a decrease in re-methylation of homocysteine, which leads to an increase in homocysteine level.6 Reflecting their importance in CNS metabolism, previous studies reported that deficiencies in vitamin B12 and folate levels, as well as changes in homocysteine, might be related with depression, mood disorders, psychotic disorders, an obsessive-compulsive disorder.7–9 Recently, some studies have reported deficiencies in the levels of vitamins B12 and folate (vitamin B9) in patients diagnosed with ASD and ADHD as well as beneficial effects of those vitamins for some of the associated ASD and ADHD symptoms.10–12 Also in some other studies, altered levels of homocysteine were found to be associated with clinical symptoms of ASDs and ADHD-associated behavioral problems, respectively.13,14
As far as we are aware, no study from Turkey evaluated levels of vitamin B12, folate and homocysteine all together in children with ADHD and ASD. Therefore, in this study, we aimed to investigate the serum levels of vitamin B12, vitamin B9 (folate) and homocysteine in children diagnosed with ADHD and ASD and compare those findings to healthy controls. Also, we aimed to investigate if the serum levels of B12, folate and homocysteine correlate with ASD and ADHD symptom severity.
Materials and methods
Study design
This single center, case-control study was conducted at the Düzce University Medical Faculty, Department of Child and Adolescent Psychiatry. The study was conducted in accordance with the Declaration of Helsinki (International Committee of Medical Journal Editors, 1989) and IRB approval for this study was acquired from local ethics committee (Date: 03.05.2016, Number: 107).
Participants
Patients who were admitted to the Department of Child and Adolescent Psychiatry for the first time and who met inclusion criteria (diagnosis of ADHD or ASD) were enrolled in the study. The healthy control group was composed of children who applied to the Department of Pediatrics within the specified time frame with temporary health conditions (upper respiratory tract infection, etc.) and have neither chronic medical conditions nor psychiatric history. Patient and control groups consisted of medication-free children and also have no chronic disorders and vitamin supply intake before the study. Written Informed consent forms were procured from the families of both patients and control groups.
Procedures
Psychiatric evaluation and diagnosis
Diagnosis of ADHD (n=48) was based on the Schedule for Affective Disorders and Schizophrenia for School Age Children – Present and Lifetime Version (K-SADS-PL), which was developed based on DSM-IV diagnostic criteria.
Scales used in psychiatric evaluation
A semi-structured interview form developed by Kaufman et al was used to determine past and present psychopathologies of children and adolescents according to DSM-IV diagnostic criteria.15 Because the original version of K-SADS-PL does not include a module for the assessment of ASDs, the diagnosis of ASD was made based on the DSM-5 diagnostic criteria. KSADS-PL was applied to both children or adolescents and their primary caregiver.
CARS is a 15-point behavioral rating scale developed to separate non-autistic children with intellectual disabilitiesfrom children with autistic symptoms. It is especially effective on separating autistic children from children with moderate intellectual disability. It also enables us to determine the clinical severity of autism as mild-moderate and moderate-serious. Each item is graded with a half degree scoring between 1 and 4. The possible total score ranges from 15 at a minimum to 60 at maximum. According to the scoring, children with scores between 15 and 29.5 do not show autistic symptoms. Children with scores between 30 and 36.5 have a clinically mild-moderate autism and children between 37 and 60 have severe autism.16
T-DSM-IV-S was used for symptom severity in this study.17 The items in the scale are identical to the list of symptoms described in the DSM-IV criteria for ADHD (inattention: 9 items, hyperactivity-impulsivity: 9 items), oppositional defiant disorder (8 items) and conduct disorder (15 items). The T-DSM-IV-S was developed by Turgay (1994) and translated and adapted in Turkish by Ercan et al (2001).18 The symptoms are scored by assigning a severity estimate for each symptom on a 4-point Likert-type scale (namely, 0= not at all; 1= just a little; 2= much; and 3= very much). Ratings of “much” and “very much” for each item were considered positive, as done in previous studies.
Preparation of colorimetric analysis
After informed consent was procured, 3.0 mL of blood were taken from the antecubital veins of the non-dominant hand while sitting. Samples were centrifuged at 3000 rpm at +4.0 °C for 10 mins with EDTA tubes; then, the supernatant section was taken up with a separate Eppendorf tube and stored at – 80.0°C until assay time.
Measurement of vitamin B9 (folate) and vitamin B12 levels
Serum folate and vitamin B12 were analyzed on Epoch Analyzer TM spectrophotometric system (Biotek Diagnostics Inc.) according to manufacturer protocol. The measurements of parameters were made with the Human V B12 Elisa Kit (Cat: E-EL-0010) and Human VB9 Elisa Kit (Cat: E-EL-0009) (Elabscience, USA). Standardization of assay principles was diluted according to the stock standard solution contained in the kit and patient sample values were calculated according to standard concentration at the ending.
Before analysis, samples and kits were brought to room temperature. A quantity of 100 μ of working reagent, washing solution and standard curves were prepared from the stock buffer. A quantity of 90 μL of detection reagent was added to the whole standard, sample and blank wells for incubation. The plate was incubated 37°C for 4 hrs. Then, each well was washed for three times and substrate solution was added. A quantity of 50 μL of stopping solution was added at the appropriate incubation time. After 15 mins incubation in dark, the contents were removed and run through the microplate reader with measurements at 450 nm wavelength.
The ELISA was based on the competitive binding enzyme immunoassay technique. The concentrations of folate and vitamin B12 were measured by comparing the O.D. of the standard curve. The sample data were linearized by log concentrations 0–2000 ng/mL with the odd absorbance nm value determined by progression analysis. Coefficients of variation for folate and vitamin B12 levels were 5.0% for both.
Measurement of homocysteine
Homocysteine levels of experimental and control group samples were tested by Human ELISA kit (Elabscience, Cat: 201611). For quantification, 100 µL patient serum and 100 µL anti-homocysteine antibody are added to a plate coated with a homocysteine conjugate. Patient samples and kit conjugate were incubated 3 hrs at 37°C in the dark. This assay protocol differs from others (ie, folate and vitamin B12) because the sample and conjugate compete for antibody binding, which generates a reverse curve. Samples with high homocysteine levels will bind to most of the antibody, which gets washed away and results in a low O.D., while samples with low homocysteine levels will leave more antibody available to bind to the conjugate, producing a high signal. Binding plates were read in 570 nm. Evaluation of the results was carried out according to the kit protocol after completed stages. The coefficient of variation for homocysteine levels was 3.7%.
Statistical analyses
A priori power calculation was conducted using the results of previous studies as well as recent reviews.19–25 Overall effect sizes for changes in levels of vitamin B12, folate and homocysteine in ASD and ADHD were small to medium. We calculated that 144 participants would be required to conduct a MANCOVA at 90.0% power at a p level of 0.05 for three groups and three response variables and controlling for the effects of age and gender.26 However, we could enroll 118 children within the specified time frame leading to 85.0% power.
SPSS 22.0 software (IBM Inc.) was used in analyses. Descriptive statistics (means and standard deviations for normally distributed variables, medians and inter-quartile ranges for non-normal variables) were used to summarize data. Assumptions of normality were tested with Kolmogorov–Smirnov test. Nominal variables between groups were compared with chi-square test. Yates and Fisher’s corrections were used as needed. Due to outliers and non-normality, Pillai’s trace was used for MANCOVA. Bonferroni correction was used in post-hoc analyses. Bivariate correlations were analyzed with Spearman’s rho. P was set at 0.05 (two-tailed).
Results
Sociodemographic variables
One hundred and eighteen children (ADHD, n=48; ASD, n=35; controls, n=35) were enrolled. The majority of the sample (81.4%) were male. Rates of male children in control, ADHD and ASD groups were 100.0%, 68.8% and 80.0%; respectively. The groups differed significantly regarding gender (chi-square=46.4, dF=2, p=0.000) with the control group being significantly different from children with ADHD and ASD.
The ages of children were not distributed normally (p=0.000), and the median age of the whole sample was 8.0 (IQR=3.0) years. Median ages and inter-quartile ranges for controls, ADHD and ASD children were 9.0 (IQR=3.9), 8.6 (IQR=2.8) and 6.0 (IQR =3.0) years, respectively. The groups differed significantly regarding age (chi-square=45.7, dF=2, p=0.000). Post-hoc comparisons revealed that median ages of controls (Z= −5.6, p=0.000) and children with ADHD (Z=−6.2, p=0.000) were similar between themselves and significantly higher than those with ASDs (Bonferroni correction, Mann–Whitney U test).
Vitamin B12, folate (folic acid) and homocysteine levels
None of the measurements were distributed normally in samples (p=0.000, 0.001 and 0.001 for vitamin B12, folate and homocysteine, respectively). Neither covariance matrices (Box’s M=71.9, p=0.000) nor error variances were equal (Levene’s test, p<0.05 for all). Laboratory values according to diagnostic groups are summarized in Table 1.
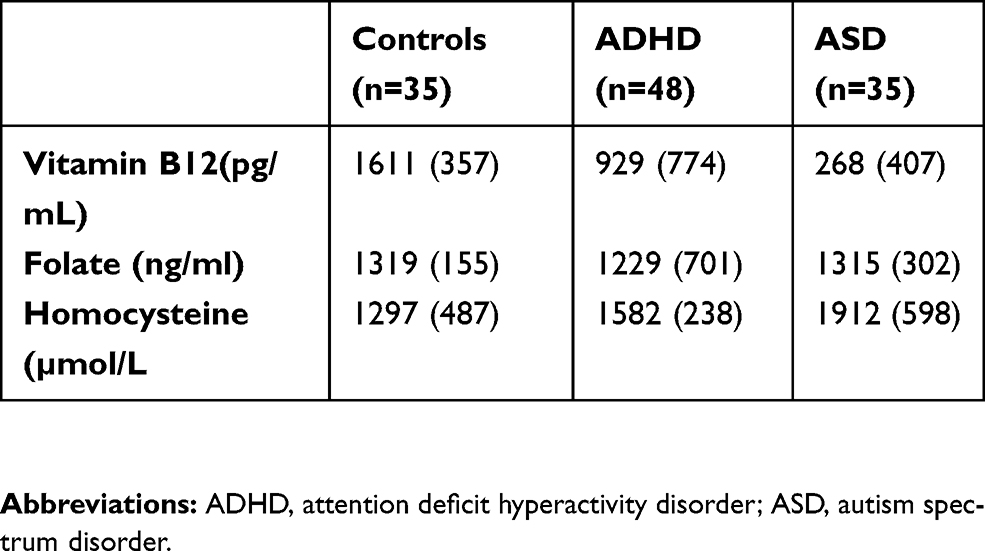 |
Table 1 Laboratory evaluations of subjects according to diagnostic groups |
The effects of age (F(3, 111)=0.6, p=0.614, partial η2=0.02) and gender (F(3, 111)=1.6, p=0.202, partial η2=0.04) were not significant. However, diagnosis affected the vitamin levels significantly (F(6, 224)=22.8, p=0.000, partial η2=0.379). Univariate analyses revealed that diagnostic status affected vitamin B12 (F=106.7, p=0.000, partial η2=0.654) and homocysteine levels (F=28.3, p=0.000, partial η2=0.333) but did not affect folate (F=1.3, p=0.288, partial η2=0.022). In pair-wise comparisons, controls had the highest vitamin B12 levels followed by children with ADHD (p=0.000, Bonferroni). Children with ASD had the lowest levels of vitamin B12. Lastly, children with ASD had the highest levels of homocysteine, followed by children with ADHD (p=0.000, Bonferroni). Controls had the lowest levels of homocysteine.
Psychometric evaluations
Symptoms of inattention, hyperactivity/impulsivity, oppositionality and conduct disorder were evaluated in children with ADHD using DSM-IV-Based Screening and Assessment Scale for Disruptive Behavior Disorders. Median scores and inter-quartile ranges for the corresponding subscales were 19.0 (IQR=7.0), 13.0 (IQR=9.0), 7.0 (IQR=9.8) and 2.0 (IQR=5.8), respectively.
Spearman’s correlation analyses were conducted to evaluate relationships between symptom severity and laboratory measurements in patients with ADHD. Vitamin B 12 levels and hyperactivity/impulsivity (Rho=−0.36, p=0.01) and oppositionality (Rho=−0.36, p=0.01) scores displayed low to medium negative correlations. No other relationships could be discerned. As a result, vitamin B12 levels could explain 13.0% of the variance in hyperactivity/impulsivity and oppositionality scores of patients with ADHD.
Symptoms of children with ASDs were evaluated with CARS. Median score of CARS in this group was 37.5 (IQR=12.5). In correlation analyses, no relationships between CARS total and item scores and laboratory evaluations could be discerned.
Discussion
In this single-center, cross-sectional, case-control study, we found that patients with ADHD and ASDs and healthy control children differed significantly regarding vitamin B12 and homocysteine. Patients with ASDs had the lowest vitamin B12 and the highest homocysteine levels. We did not find a significant difference in serum folate levels both in ASD and ADHD group compared to control group. Gender and age of children had no significant effect on vitamin levels.
Our study results support the studies showing low serum vitamin B12 and folate levels in ASD patients.27,28 A recent study conducted in Turkey found lower vitamin B12 serum levels in children diagnosed with ASD compared to controls.29 Similarly, another study from Oman reported lower serum folate and vitamin B12 levels in children diagnosed with ASD.28 As for ADHD, Unal et al. reported that Turkish children with ADHD had significantly lower vitamin B12 levels and that those levels negatively correlated with psychosomatic symptoms and learning problems as reported by teachers.23 This finding was supported and extended to folate in another study by Altun et al.30
Vitamin B12 status in the brain may play an important role in methylation-dependent processes and low serum vitamin B12 levels in ASD patients were interpreted to reflect increased levels of oxidative stress and impaired DNA methylation which can be an important factor in the pathophysiology of ASD.31,32 DNA methylation, an epigenetic regulatory system is known to be important in during pre- and post-natal brain development and alterations in DNA methylation have been shown in patients with ASDs.32,33 In line with these study results, DNA hypomethylation which affect the development of the CNS may be a possible explanation for the relation between vitamin B12 deficiency and autism.8 Lower levels of serum B12 were also found in ADHD group compared to control group. Vitamin B12 is required for a unique process known as dopamine-stimulated phospholipid methylation (PLM) performed by D4 receptor in CNS which is mostly associated with ADHD.34 PLM activity – differs by D4 gene variants – plays an important role in attention and neuronal synchronization and is known to be disturbed in children with both ASDs and ADHD.35 Although cross-sectional nature of our study precludes speculations on causality and may not reflect micro-nutrient levels in the fetal period, deficits in vitamin B12 and folate along with reduced methionine synthaseactivity might be posited to contribute to ADHD and ASD pathogenesis. Further, longitudinal studies exploring this issue are needed.
Patients with ASDs and ADHD in our sample were also found to have higher serum homocysteine levels compared to control group. Reduced vitamin B12 levels may increase the level of homocysteine. Homocysteine is also known to be a powerful excitotoxin, and its metabolic products may cause neuronal damage and disrupt the synthesis of proteins and neurotransmitters which are important for the structural integrity of the brain. As well as high levels of homocysteine were found to play a role in the etiology of various psychopathologies, recent clinical studies also reported higher serum and urine homocysteine levels in children with ASDs when compared to healthy controls.27,36,37 As for ADHD, some studies report elevated levels of homocysteine while others report reduced levels.13,25,30 The differing results may be due to enrollment of children with different comorbidities, diagnosed with separate ADHD subtypes and from variable age ranges. Our results support and extend those findings in showing reduced vitamin B12 and elevated homocysteine levels in patients with ADHD and ASDs.
As another finding in our study, oppositionality and hyperactivity/impulsivity symptoms in ADHD group were related to vitamin B12 and homocysteine levels which partially supported Saha et al's results.13 Some preliminary studies suggest that vitamin and micronutrient supplements may reduce emotional lability, aggression and oppositional behaviors in children with ADHD and ASDs.38–40
Our results should be evaluated within the context of their limitations. Due to the cross-sectional nature of our study direction of causality could not be ascertained. Children with ASDs often display avoidance/restriction of certain foods due to sensory reactivity and resistance to novelty. This may also cause deficiencies of vitamins in children with ASDs. To control for this possibility, we also evaluated correlations with CARS sensory reactivity item scores but did not apply checklists to parents (ie, ABC, etc.). Also, in the planning stage of our study, we aimed to conduct separate univariate analyses of variance controlling for type I errors as per the Garipardic study but chose to conduct a multivariate analysis of covariance to control for effects of gender and age.19 Our data violated some of the assumptions of MANCOVA but we tried to control for this by using robust measures (ie, Pillai’s trace). Also, our findings may be affected by timing of measurements and may not reflect CNS levels of micronutrients in earlier development. Regardless of those limitations, our study is among the first ones to evaluate vitamin B12, vitamin B9 (folate) and homocysteine levels in children with ASDs and ADHD and compare the results with controls.
Our study results show low B12 and high homocysteine levels are detected in children diagnosed with ASD and ADHD compared to healthy controls. Children with ADHD or ASD often show emotional and behavioral problems. Deficiencies in micronutrients like B12 may play a role in the etiopathogenesis and clinical symptoms of these neurodevelopmental disorders. However, these parameters should be analyzed in a wider population to clarify the effect on the etiology of ADHD and ASD.
Acknowledgments
This study was supported by the Duzce University coordinatorship of scientific research projects. This study was presented as an oral presentation at the Child and Adolescent Mental Health Congress, Istanbul, 2018 This study was conducted at the Duzce University Biochemistry Laboratory. We thank the laboratory staff, and all the patients and their families for participating in the study.
Disclosure
The authors alone are responsible for the content and writing of the paper and they report no conflicts of interest in this work.
References
1. Lichtenstein P, Carlstrom E, Rastam M, Gillberg C, Anckarsater H. The genetics of autism spectrum disorders and related neuropsychiatric disorders in childhood. Am J Psychiatry. 2010;167:1357–1363. doi:10.1176/appi.ajp.2010.10020223
2. Raghavan R, Riley AW, Volk H, et al. Maternal multivitamin intake, plasma folate and vitamin B12 levels and autism spectrum disorder risk in offspring. Paediatr Perinat Epidemiol. 2018;32:100–111. doi:10.1111/ppe.12414
3. Zhang Z, Yu L, Li S, Liu J. Association study of polymorphisms in genes relevant to vitamin B12 and folate metabolism with childhood autism spectrum disorder in a Han Chinese population. Med Sci Monit. 2018;24:370–376. doi:10.12659/msm.905567
4. Stanger O, Fowler B, Piertzik K, et al. Homocysteine, folate, and vitamin B12 in neuropsychiatric diseases: review and treatment recommendations. Expert Rev Neurother. 2009;9:1393–1412. doi:10.1586/ern.09.75
5. Basoglu C, Ates MA, Algul A, et al. Adjuvant folate with escitalopram treatment and homocysteine, folate, vitamin B12 levels in patients with the major depressive disorder. Bull Clin Psychopharmacol. 2009;19:135–142.
6. Carmel R, Green R, Rosenblatt DS, Watkins D. Update on cobalamin, folate, and homocysteine. Hematology Am Soc Hematol Educ Program. 2003;1:62–81. doi:10.1182/asheducation-2003.1.62
7. Güzelcan Y, van Loon P. Vitamin B12 status in patients of Turkish and Dutch descent with depression: a comparative cross-sectional study. Ann Gen Psychiatry. 2009;8:18. https://doi.org/10.1186/1744-859x-8-18
8. Zhang Y, Hodgson NW, Trivedi MS, et al. Decreased brain levels of vitamin B12 in aging, autism, and schizophrenia. PLoS One. 2016;11:e0146797. doi:10.1371/journal.pone.0146797
9. Türksoy N, Bilici R, Yalçıner A, et al. Vitamin B12, folate, and homocysteine levels in patients with obsessive-compulsive disorder. Neuropsych Dis Treat. 2014;10:1671–1675. doi:10.2147/ndt.s67668
10. Bala KA, Doğan M, Kaba S, Mutluer T, Aslan O, Doğan SK. Hormone disorder and vitamin deficiency in attention deficit hyperactivity disorder (ADHD) and autism spectrum disorders (ASDs). J Pediatr Endocrinol Metab. 2016;29:1077–1082. doi:10.1515/jpem-2015-0473
11. Üskül H, Kılıçaslan Ö, Yıldırmak ZY, Özsan H. Evaluation of blood parameters in attention deficit hyperactivity disorder. Konuralp Med J. 2017;9:207–212. doi:10.18521/ktd.329860
12. Fuentes-Albero M, Cauli O. Homocysteine levels in autism spectrum disorder: a clinical update. Endocr Metab Immune Disord Drug Targets. 2018;18:289–296. doi:10.2174/1871530318666180213110815
13. Saha T, Chatterjee M, Verma D, et al. Genetic variants of the folate metabolic system and mild hyperhomocysteinemia may affect ADHD associated behavioral problems. Prog Neuropsychopharmacol Biol Psychiatry. 2018;84:1–10. doi:10.1016/j.pnpbp.2018.01.016
14. Gordon HA, Rucklidge JJ, Blampied NM, Johnstone JM. Clinically significant symptom reduction in children with attention-deficit/hyperactivity disorder treated with micronutrients: an open-label reversal design study. J Child Adolesc Psychopharmacol. 2015;25:783–798. doi:10.1089/cap.2015.0105
15. Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P. Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry. 1997;36:980–988. doi:10.1097/00004583-199707000-00021
16. Mesibov G, Schopler E, Schaffer B, Michal N. Use of childhood autism rating scale with autistic adolescents and adults. J Am Acad Child Adolesc Psychiatry. 1989;28:538–541. doi:10.1097/00004583-198907000-00012
17. Turgay A. Disruptive Behavior Disorders: Child and Adolescent Screening and Rating Scales for Children, Adolescents, Parents and Teachers. West Bloomfield (MI): Integrative Therapy Institute Publication; 1994.
18. Ercan ES, Amado S, Somer O. Development of a test battery for the assessment of attention deficit hyperactivity disorder [in Turkish]. J Child Adolesc Ment Health. 2001;8:132–144.
19. Garipardic M, Doğan M, Bala KA, et al. Association of attention deficit hyperactivity disorder and autism spectrum disorders with mean platelet volume and vitamin D. Med Sci Monit. 2017;23:1378–1384. doi:10.12659/msm.899976
20. Li Y-J, Ou -J-J, Li Y-M, Xiang D-X. Dietary supplement for core symptoms of autism spectrum disorder: where are we now and where should we go? Front Psychiatry. 2017;8:155. doi:10.3389/fpsyt.2017.00297
21. Frye RE, Slattery JC, Quadros EV. Folate metabolism abnormalities in autism: potential biomarkers. Biomark Med. 2017; 11(8):687–699.
22. Modabbernia A, Velhorst E, Reichenberg A. Environmental risk factors for autism: an evidence- based review of systematic reviews and meta-analyses. Mol Autism. 2017;8:13. doi:10.1186/s13229-017-0121-4
23. Unal D, Celebi F, Bildik HN, Koyuncu A, Karahan S. Vitamin B12 and haemoglobin levels may be related with ADHD symptoms: a study in Turkish children with ADHD. Psychiatry Clin Psychopharmacol. In Press 2019.
24. Saha T, Chatterjee M, Sinha S, Rajamma U, Mukhopadhyay K. Components of the folate metabolic pathway and ADHD core traits: an exploration in eastern Indian probands. J Hum Genet. 2017;62(7):687–695. doi:10.1038/jhg.2017.23
25. Greenblatt JM, Delane DD. Micronutrient deficiencies in ADHD: A global research consensus. J Orthomol Med. 2017;32:6.
26. Faul F, Erdfelder E, Lang AG, Buchner A. G Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39:175–191. https://doi.org/10.3758/bf03193146
27. Ali A, Waly MI, Al-Farsi YM, Essa MM, Al-Sharbati MM, Deth RC. Hyperhomocysteinemia among Omani autistic children: a case-control study. Acta Biochim Pol. 2011;58:547–551. doi:10.18388/abp.2011_2223
28. Al-Farsi YM, Waly MI, Deth RC, et al. Low folate and vitamin B12 nourishment is common among Omani children newly diagnosed with autism. Nutrition. 2013;29:537–541. doi:10.1016/j.nut.2012.09.014
29. Altun H, Kurutaş EB, Şahin N, Güngör O, Fındıklı E. The levels of vitamin D, vitamin D receptor, homocysteine and complex B vitamin in children with autism spectrum disorders. Clin Psychopharmacol Neurosci. 2018;16:383–390. doi:10.9758/cpn.2018.16.4.383
30. Altun H, Sahin N, Belge Kurutas E, Gungor O. Homocysteine, pyridoxine, folate and vitamin B12 levels in children with attention deficit/hyperactivity disorder. Psychiatr Danub. 2018;30(3):310–316. doi:10.24869/psyd.2018.310
31. Guy J, Cheval H, Selfridge J, Bird A. The role of MeCP2 in the brain. Annu Rev Cell Dev Biol. 2011;27:631–652. doi:10.1146/annurev-cellbio-092910-154121
32. Ladd-Acosta C, Hansen KD, Briem E, Fallin MD, Kaufmann WE, Feinberg AP. Common DNA methylation alterations in multiple brain regions in autism. Mol Psychiatry. 2014;19:862–871. doi:10.1038/mp.2013.114
33. Rose S, Melnyk S, Pavliv O, et al. Evidence of oxidative damage and inflammation associated with low glutathione redox status in the autism brain. Transl Psychiatry. 2012;2:e134. doi:10.1038/tp.2012.61
34. Kuznetsova AY, Deth RC. A model for modulation of neuronal synchronization by D4 dopamine receptor-mediated phospholipid methylation. J Comput Neurosci. 2008;24:314–329. doi:10.1007/s10827-007-0057-3
35. Deth R, Muratore C, Benzecry J, Power-Charnitsky VA, Waly M. How environmental and genetic factors combine to cause autism: a redox/methylation hypothesis. Neurotoxicology. 2008;29:190–201. doi:10.1016/j.neuro.2007.09.010
36. Pasca SP, Nemes B, Vlase L, et al. High levels of homocysteine and low serum paraoxonase 1 arylesterase activity in children with autism. Life Sci. 2006;78:2244–2248. doi:10.1016/j.lfs.2005.09.040
37. Kałuzna-Czaplinska J, Michalska M, Rynkowski J. Homocysteine level in urine of autistic and healthy children. Acta Biochim Pol. 2011;58:31–34. doi:10.18388/abp.2011_2281
38. Rucklidge J, Kaplan B. Broad-spectrum micronutrient treatment for attention-deficit/hyperactivity disorder: rationale and evidence to date. CNS Drugs. 2014;28:1–11. https://doi.org/10.1007/s40263-014-0190-2
39. Adams JB, Audhya T, McDonough-Means S, et al. Effect of a vitamin/mineral supplement on children and adults with autism. BMC Pediatr. 2011;11:111.
40. Kaplan BJ, Hilbert P, Tsatsko E. Micronutrient treatment for children with emotional and behavioral dysregulation: case series. J Med Case Rep. 2015;9:240. https://doi.org/10.1186/s13256-015-0735-0
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.