")
Back to Journals » Journal of Inflammation Research » Volume 14
Comparison of Radiation Pneumonitis in Lung Cancer Patients Treated with HT versus IMRT and Circulating Lymphocyte Subsets as Predicting Risk Factors
Authors Zhang X, Yang D, Jiang Y, Huang L, Wang C, Tao D, Liu X, Lei Y, Wu Y, Zhou W
Received 12 July 2021
Accepted for publication 10 August 2021
Published 28 August 2021 Volume 2021:14 Pages 4205—4215
DOI https://doi.org/10.2147/JIR.S328955
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Xin Zhang,* Dingyi Yang,* Yong Jiang, Luo Huang, Can Wang, Dan Tao, Xianfeng Liu, Yongyang Lei, Yongzhong Wu, Wei Zhou
Chongqing Key Laboratory of Translational Research for Cancer Metastasis and Individualized Treatment, Chongqing University Cancer Hospital, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yongzhong Wu; Wei Zhou
Chongqing Key Laboratory of Translational Research for Cancer Metastasis and Individualized Treatment, Chongqing University Cancer Hospital, 181 Han Yu Road, Chongqing, 400030, People’s Republic of China
Tel +86 18323064006
Email [email protected]; [email protected]
Purpose: We sought to compare the symptomatic radiation pneumonitis (RP) in lung cancer patients treated with helical tomotherapy (HT) versus intensity-modulated radiotherapy (IMRT), and examine the predictive value of circulating lymphocyte subsets affecting the occurrence of RP.
Patients and Methods: Circulating lymphocyte subsets, clinical characteristics, dosimetric parameters and pulmonary function were collected from 130 lung cancer patients treated with HT (n = 53) or IMRT (n = 77) from 2016 through 2020. Symptomatic RP was compared between groups. Binary logistic regression was used to identify predictors of RP.
Results: The IMRT group had larger planning target volume (319.9 vs 240.8 cc, P = 0.041); more ECOG performance status 0– 1 (96.1% vs 79.2%, P = 0.002); more stage III–IV disease (94.8% vs 37.6%, P = 0.028); and more combined systemic therapy (85.7% vs 69.8%, P = 0.022). Grade ≥ 2 RP were comparable between IMRT and HT groups (16.9% vs 15.1%, P = 0.785). For stage III–IV disease, IMRT was associated with lower lung V10 (31.9% vs 35.8%, P = 0.047) and lower incidence of grade 5 RP (0% vs 9.1%, P = 0.018). All lymphocyte subsets reduced after radiotherapy. The decrease degree of total T cell count and CD4+ T cell count were larger after IMRT than HT (P = 0.043, P = 0.021). In univariate analysis, the smoking status, lower baseline FEV1, and higher total T cell count, higher CD8+ T cell count, lower total B cell count, lower CD4+/CD8+ ratio after radiotherapy were associated with the development of grade ≥ 2 RP. The higher CD8+T cell count after radiotherapy was the only risk factor associated with grade ≥ 2 RP in multivariable analysis (OR 1.003; 95% CI: 1.000– 1.005; P = 0.044).
Conclusion: IMRT was associated with lower lung V10 and less grade 5 RP than HT for stage III–IV lung cancer. Higher CD8+ T cell count after radiotherapy was associated with an increased risk of RP. HT may better preserve total T cell and CD4+ T cell than IMRT.
Keywords: radiation pneumonitis, lung cancer, helical tomotherapy, intensity-modulated radiotherapy, circulating lymphocyte
Introduction
Thoracic radiotherapy plays a critical role in the treatment of lung cancer. Nowadays, intensity-modulated radiotherapy (IMRT) has been the most widely used radiation technique for lung cancer. Helical tomotherapy (HT) is a form of IMRT with a helical beam delivery technique.1 Multiple dosimetric studies have shown the potential of HT to decrease radiation dose to lung, esophagus and heart, while maintaining radiation dose to the tumor compared with IMRT.2,3 On the other hand, a larger volume of lung tissues receives low radiation doses when HT is delivered, the so-called “low-dose bath”, which may increase toxicity.4
Regarding radiation-related toxicity, radiation pneumonitis (RP) is the most important dose-limiting toxic effect after thoracic irradiation. Symptomatic RP influences the quality of life and clinical course, even being fatal in some cases, with the incidence from 15% to 45%.5–7 Nevertheless, how these two radiation modalities, HT versus IMRT, contribute to the risk of RP in lung cancer is unclear yet.
Thoracic irradiation damages resident cells and initiates repair processes, leading to activation of the immune system. The recruitment of various immune cells and a perpetual cascade of cytokines were described in the process of RP.8 Some evidence from preclinical studies showed that T lymphocytes infiltrate the lung after irradiation.9 In addition, radiotherapy was often accompanied by lymphopenia because of the high radiosensitivity of circulating lymphocytes. Clinical study found that radiation-induced lymphocyte apoptosis was associated with late toxicity and survival outcome in cancer patients.10,11 Thus, we hypothesize that the changes of circulating lymphocyte subsets before and after radiotherapy, such as T cells, B cells and natural killer cells, may be associated with RP.
In the study, we aimed to compare the symptomatic RP in lung cancer patients treated with HT and IMRT. Moreover, we sought to examine the predictive value of circulating lymphocyte subsets, clinical characteristics, dosimetric parameters and pulmonary function affecting the occurrence of RP.
Methods
Patients
The medical records of lung cancer patients at the Chongqing University Cancer Hospital (CQUCH) between July 2016 and June 2020 were retrospectively reviewed. The eligibility criteria included: (1) stage I–IV lung cancer according to the 8th AJCC staging system, including locally advanced disease (stage III), inoperable stage I and II disease due to comorbidity or poor pulmonary function, limited extent of stage IV disease after effective systemic therapy; (2) thoracic radiotherapy was delivered with HT or IMRT; (3) radiation dose ≥40 Gy; (4) the availability of respiratory symptoms and corresponding radiographic images to evaluate the occurrence of RP.
This study was approved by the ethics committee of the CQUCH. Informed consent for all patients was obtained prior to therapy and performed in accordance with the Declaration of Helsinki and Good Clinical Practice Guidelines.
Radiotherapy
Gross tumor volume (GTV) included the primary tumor and positive lymph nodes. Clinical tumor volume (CTV) encompassed GTV with an additional 0.6~0.8 cm margin. Involved-field node irradiation was done. The planning target volume (PTV) was defined as CTV plus 0.8~1.5 cm margin according to tumor location and extent of respiratory motion. Normal lung dose-volume histograms (DVH) were generated with inclusion of both lungs and exclusion of the GTV. The dose-volume constraints were as follows: median total lung dose (MLD) <18 Gy, relative volume of total lung that receives ≥20 Gy (V20) <30%, maximum spinal cord dose <45 Gy, heart V40 <30%, esophagus V50 <30%.
The choice of radiation modality was mainly influenced by institutional protocol and availability. HT plans were transferred to the tomotherapy treatment planning system (TomoTherapy Incorporated, Madison, WI). Scanned every day using megavoltage CT imaging before treatment. The IMRT plans with five to seven coplanar beams was generated. Patients in the IMRT group underwent kilovoltage cone beam CT during treatment once a week. All plans were delivered with 6-MV photon beams.
Evaluation of Radiation Pneumonitis
Patients were followed up 1 month after radiotherapy and then every 2–3 months thereafter. The follow-up time was shorter if pneumonitis was suspected when patients developed dry cough, dyspnea or fever. Interval history, physical examination, blood tests, and chest CT scans were performed. RP was diagnosed by clinical symptoms and the characteristic imaging findings by CT. Grading was conducted according to the Common Terminology Criteria for Adverse Events version 4.0 (CTCAE v4.0). The diagnosis and grading of RP were confirmed by two experienced radiation oncologists.
Date Collection
Circulating lymphocyte subsets, clinical information, pulmonary function, dosimetric parameters were recorded. Circulating lymphocytes were collected from peripheral blood samples within 1 month before and after radiotherapy, including total T cell count, CD4+T cell count, CD8+T cell count, total B cell count, natural killer cell count, total lymphocyte count, the CD4+ /CD8+ ratio. Multicolor flow cytometry was used to analyse circulating lymphocyte subtypes. The clinical information included age, sex, smoking status, drinking status, Eastern Cooperative Oncology Group (ECOG) performance status, histology, location of primary tumor, clinical stage, systemic treatment history. Baseline pulmonary function included forced expiratory volume in one second (FEV1), forced vital capacity (FVC), FEV1/FVC, carbon monoxide diffusion capacity (DLCO). The dosimetric parameters were extracted from the treatment planning system, including the radiation dose, PTV volume, MLD, and the percent volume of the total lung receiving more than 5, 10, 20, 30 and 40 Gy (named V5, V10, V20, V30, V40).
Statistical Analysis
Firstly, the incidence of RP was compared between IMRT and HT, also the patient characteristics, pulmonary function and dosimetric parameters. In order to find the factors associated with RP, all the patients were divided into two groups: grade ≥2 RP and grade <2 RP. Continuous data were presented as median and interquartile range (IQR) and compared using Mann–Whitney U-test. Categorical data were compared using χ2 test. P<0.05 (two-sided) was regarded as statistically significant. Variables with P <0.05 in univariable analysis were further analyzed by multivariable analysis using binary logistic regression. Statistical analysis was performed using SPSS 22.0 software (IBM, Armonk, New York, USA).
Results
Patient Characteristics and RP Between IMRT and HT
Patient and treatment characteristics of 130 eligible lung cancer patients were summarized and compared by radiotherapy technique (Table 1), including 77 with IMRT and 53 with HT. For the entire cohort, the median age was 63 years (range 39–92 y), and the median radiation dose of PTV was 60 Gy (range 40–68 Gy), with 66 (50.8%) patients receiving radiation doses ≥60 Gy. The median fractionation regimen was 2.0 Gy (range 1.5–2.5 Gy).
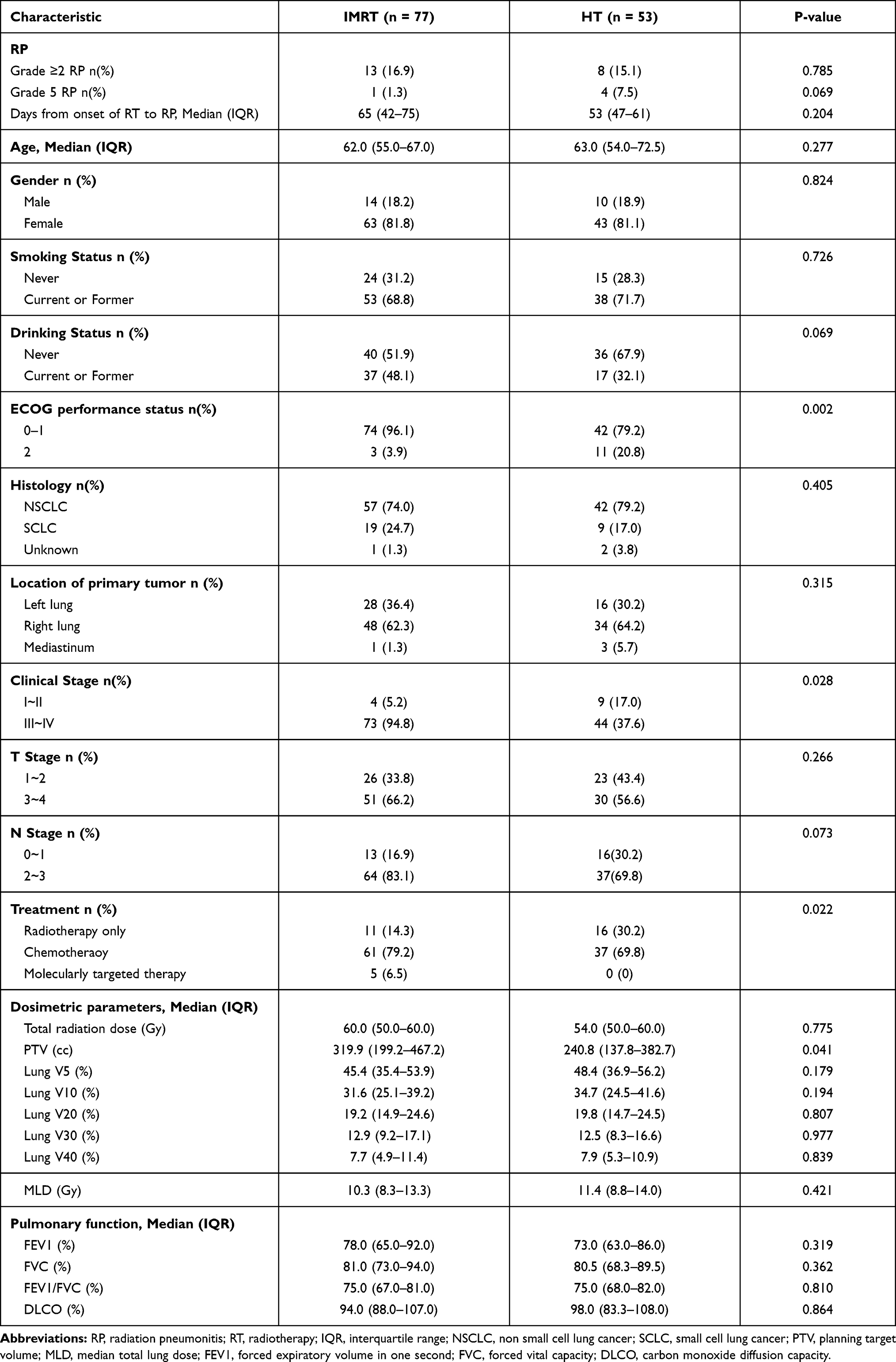 |
Table 1 Radiation Pneumonitis and Baseline Characteristics Between IMRT versus HT |
Compared with HT, IMRT group had more patients with ECOG performance status 0–1 (96.1% vs 79.2%, P = 0.002); more stage III–IV disease (94.8% vs 37.6%, P = 0.028); and more chemotherapy or molecularly targeted therapy combined with radiotherapy (85.7% vs 69.8%, P = 0.022). As for dosimetric parameters, the median PTV was greater in the IMRT group than in the HT group (319.9 vs 240.8 cc, P = 0.0041). No significant differences in lung V5-40 and MLD were observed between the two groups. For patients with stage III–IV disease (73 with IMRT vs 44 with HT), IMRT was associated with lower lung V10 than HT (31.9% vs 35.8%, P = 0.047) (Supplementary Table 1).
The median follow-up periods for all but 5 patients, who died of RP less than 3 months from the start of radiotherapy, were 22.5 months (range 8–48 months). The median time from the start of IMRT and HT to grade ≥2 RP (symptomatic RP) occurrence was 65 days and 53 days, respectively. Of the 130 patients, 15 experienced grade 2 RP (11.5%), 1 experienced grade 3 RP (0.8%) and 5 experienced grade 5 RP (3.8%). The accumulative incidence of grade ≥2 RP was 16.2%. Patients treated with HT tended to have more grade 5 RP than those treated with IMRT (7.5% vs 1.3%, P = 0.069). In addition, grade ≥2 RP were comparable between IMRT and HT group (16.9% vs 15.1%, P = 0.785). For patients with stage III–IV disease, HT was associated with higher incidence of grade 5 RP (0% vs 9.1%, P = 0.018) (Supplementary Table 1). But grade ≥2 RP were still comparable (15.1% vs 15.9%, P = 0.903).
The details of the 5 patients who developed fatal RP are shown in Table 2. None of the 5 patients received concurrent chemoradiotherapy, and 3 received chemotherapy before radiotherapy. Four patients developed cough and dyspnea and 1 patient developed low-grade fever during the course of disease. All 5 patients then succumbed to respiratory failure and 2 patients suffered tumor progression simultaneously. During the RP treatment with glucocorticoid, 2 patients developed pneumocystis carinii and fungus, respectively. Figure 1 depicts the CT images of patient No. 1 during the course of fatal RP.
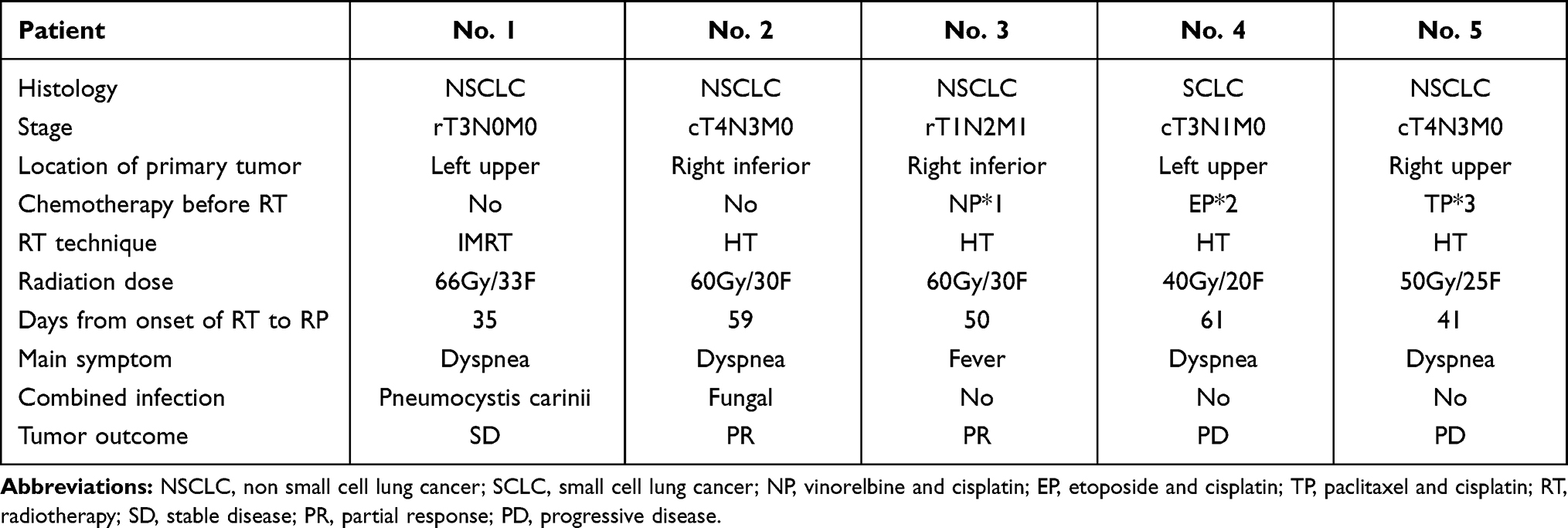 |
Table 2 The Details of the 5 Patients with Grade 5 Radiation Pneumonitis |
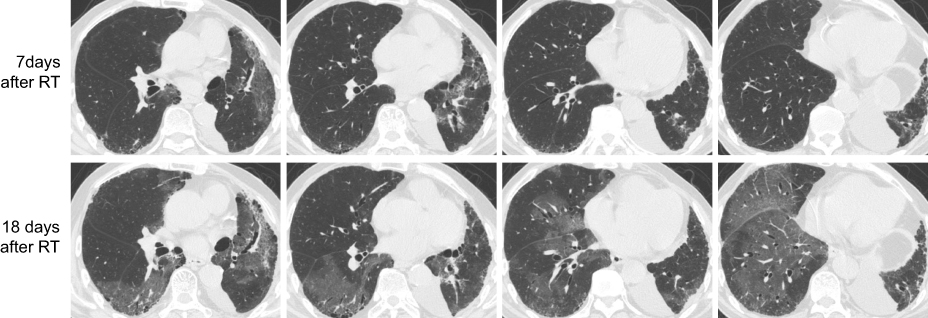 |
Figure 1 The CT images of patient No. 1 during the course of fatal RP. |
Univariate Analysis of Factors Associated with Grade ≥2 RP
Patient and tumor characteristics associated with cases of grade < 2 RP and grade ≥ 2 RP are listed in Table 3. In univariate analyses, current or former smoking was found to contribute to the occurrence of grade ≥2 RP (P = 0.025). However, the other factors (age, sex, ECOG status, histology, location of primary tumor, stage and systemic treatment) were comparable between the two groups.
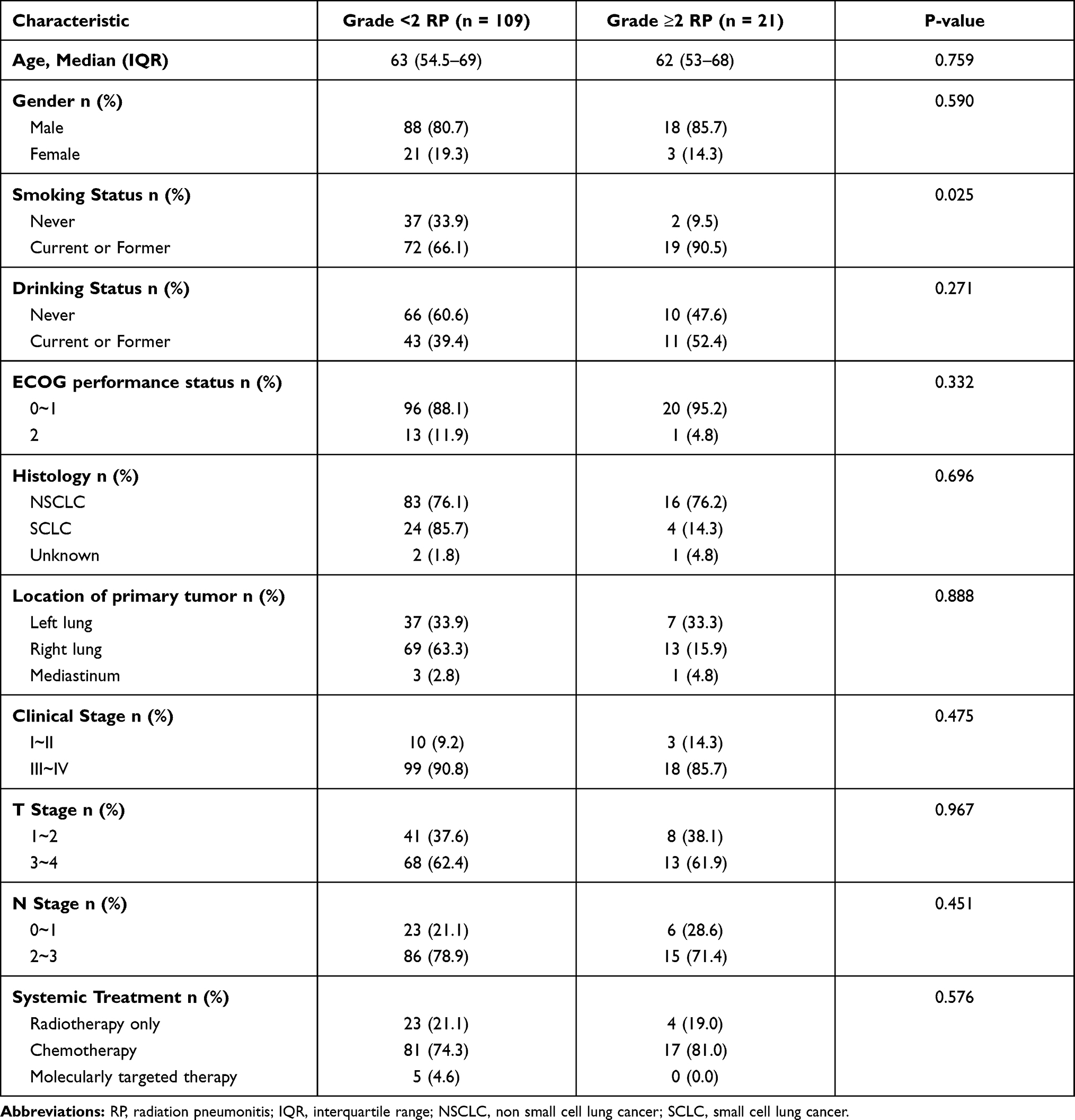 |
Table 3 Univariate Analysis of Patients Characteristics Associated with the Development of Grade ≥2 RP |
The results of the univariate analysis for pulmonary function and dosimetric parameters are shown in Table 4. The lower FEV1 was associated with development of grade ≥2 RP (P = 0.035). None of the dosimetric parameters could predict grade ≥2 RP at univariate analysis.
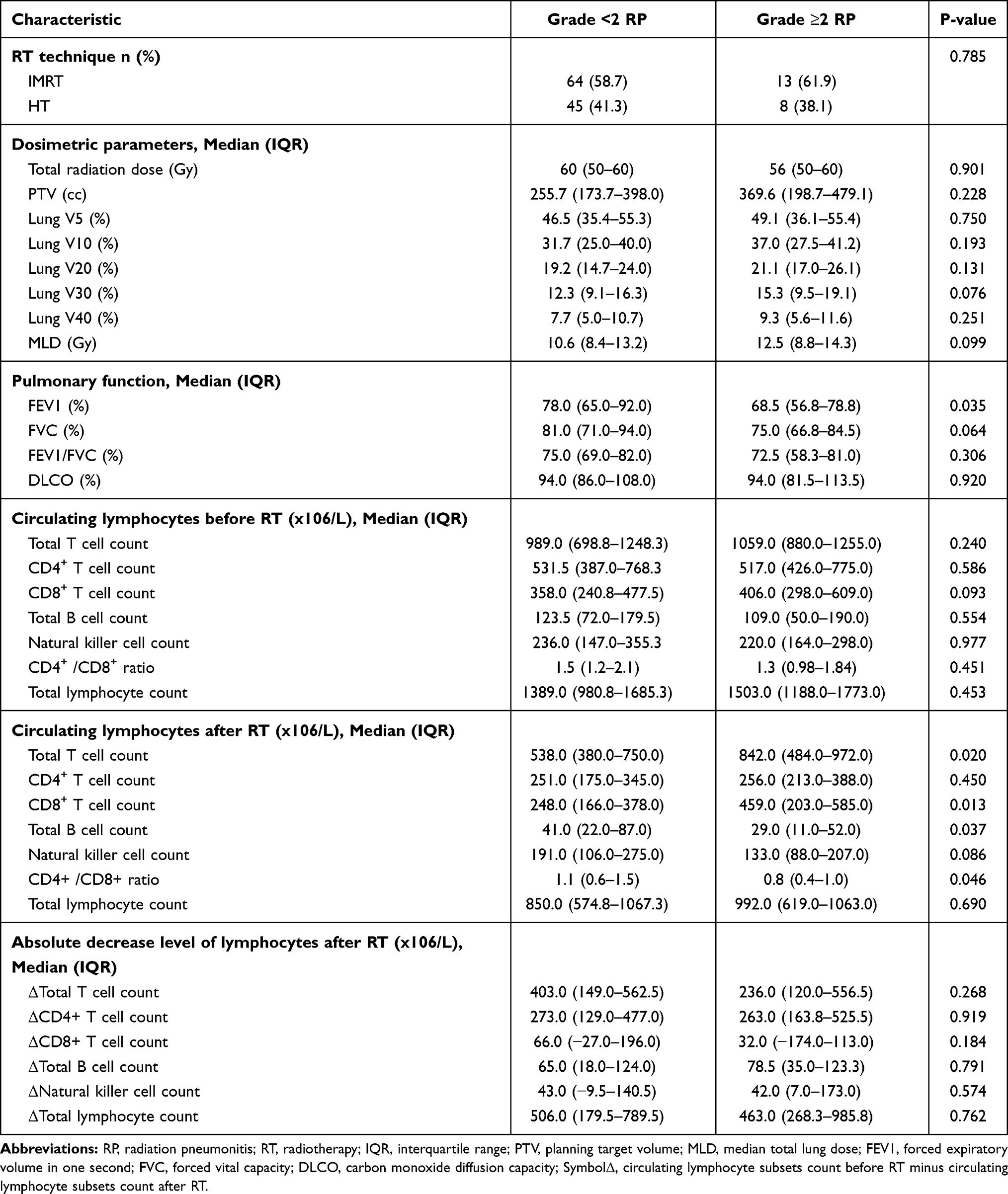 |
Table 4 Univariate Analysis of Risk Factors Associated with the Development of Grade ≥2 RP |
All lymphocyte subsets reduced after radiotherapy. Absolute decrease levels of lymphocyte subsets after IMRT versus HT are shown in Figure 2. The decrease degree of total T cell count and CD4+ T cell count were larger after IMRT than HT (P = 0.043, P = 0.021) (Supplementary Table 2). When adjustment was made for stage III–IV disease, the statistical significance remained (P = 0.036, P = 0.038). Grade ≥2 RP group had higher total T and CD8+ T cell count after radiotherapy (P = 0.020, P = 0.013) (Table 4). In addition, grade ≥2 RP group had lower total B and CD4+/CD8+ ratio after radiotherapy (P = 0.037, P = 0.046). However, absolute decrease levels of lymphocyte subsets after radiotherapy were comparable between the two groups.
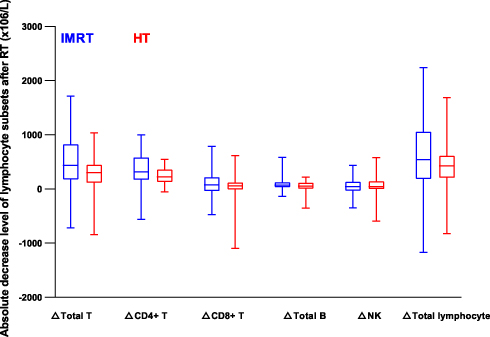 |
Figure 2 Absolute decrease level of lymphocyte subsets after IMRT versus HT. |
Multivariate Analysis of Factors Associated with Grade ≥2 RP
Finally, the smoking status, baseline FEV1, total T cell count, CD8+ T cell count, total B cell count and CD4+/CD8+ ratio after radiotherapy were selected as covariates for multivariable analysis. The result of the multivariate analysis by forward-LR binary logistic regression is shown in Table 5. The higher CD8+ T cell count after radiotherapy was a risk factor associated with grade ≥2 RP (OR 1.003; 95% CI: 1.000–1.005; P = 0.044). Then a linear regression model was conducted to identify whether lung irradiation contributes to decrease of lymphocytes. Neither PTV nor lung DVH had statistical significance (data not shown).
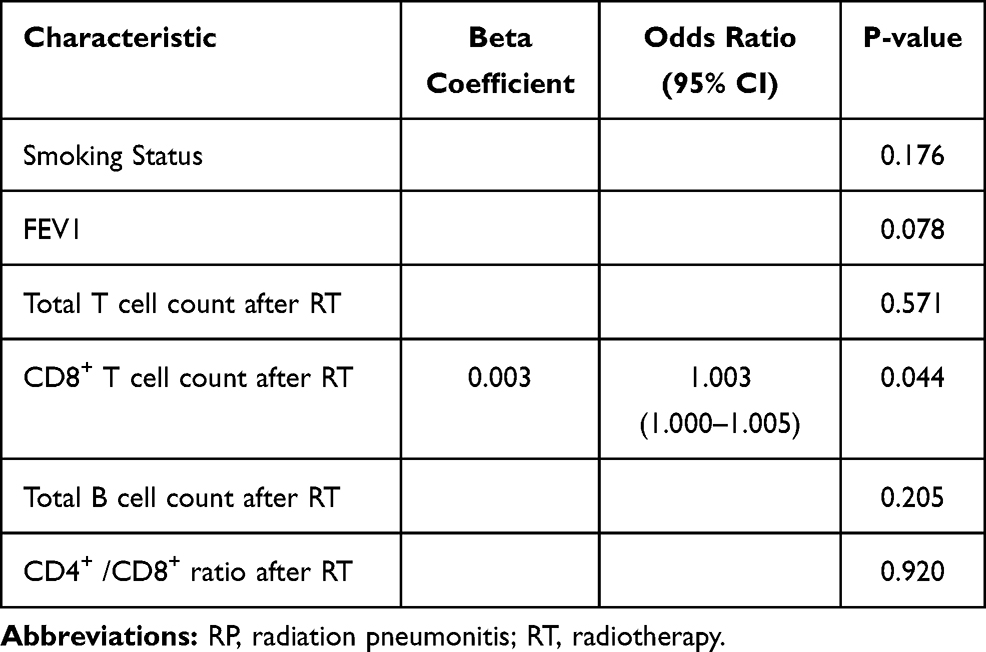 |
Table 5 Multivariate Analysis of Risk Factors Predicting Grade ≥2 RP |
Discussion
This study compared the symptomatic RP in lung cancer patients treated with either HT or IMRT, and examined the predictive value of circulating lymphocyte subsets, clinical and dosimetric parameters affecting the occurrence of RP.
So far, only a few studies have reported the RP incidence in lung cancer patients treated with HT, and no studies compared the symptomatic RP between HT and IMRT. The incidence of grade 5 RP after HT was 3.2~11%, and the incidence of grade ≥2 RP was 53.2~70%.12–14 In our study, 8 patients treated with HT experienced grade ≥2 RP (15.1%) and 4 experienced grade 5 RP (7.5%), which seems to be lower than other studies. We speculate that the worse ECOG performance status and earlier stage in HT group contributed to the decreasing number of patients receiving chemotherapy. Less intense chemotherapy regimens may result in lower incidence of RP in our study. Despite larger PTV and more frequent systemic treatment in IMRT group than HT group, the incidence of grade ≥2 RP and grade 5 RP were comparable. However, for patients with stage III–IV disease, IMRT group had less grade 5 RP than HT. Collectively, considering cost-effectiveness, IMRT should be a preferential radiotherapy option at present, especially for patients with stage III–IV lung cancer. However, HT was reported as a safe and effective technique for hypofractionated stereotactic body radiotherapy (SBRT) with lower incidence of RP. Of 28 patients with early stage inoperable NSCLC treated with HT-SBRT, 3.5% experienced grade 3 RP, and 14% experienced grade 2 RP.15 Moreover, of 22 patients with early stage NSCLC and 17 with oligometastasis, only one (2.6%) experienced grade 2 RP.16
HT continuously delivers radiation to the target and rotates 360° around the patient, thereby spreading a low dose over a larger area.17 For patients with stage III–IV lung cancer, HT group achieved higher lung V10 than IMRT in our study, which was consistent with the “low-dose bath” theory. Current studies have reported that various dosimetric parameters contribute to the risk of development of RP, but the results were still inconsistent. The lung V20 was the most frequently described dosimetric parameter to predict probability of lung injury.18,19 However, some retrospective studies demonstrated the correlation of RP and low-dose baths, such as the V5-15, especially for patients treated with HT.13,14,20 However, in our study, none of the dosimetric parameters was independent predictors of grade ≥2 RP. One possible reason is that our study had lower MLD, V5, V20 and V30 than dose-volume constraints and other studies, which was not enough to reveal such a significant difference.
Abnormal pulmonary function may increase the risk of RP. A number of studies found that the DLCO was a strong predictor of RP,21–23 and FEV1, the exhaled fraction of nitric oxide also had correlation.24 However, some studies did not show any correlation between pulmonary function and radiation-induced lung toxicity.25,26 In our study, FEV1 was the only predictive factor for grade ≥2 RP in univariate analysis, but not in multivariate analysis.
The radiation can damage lungs by breaking DNA and activating oxygen radicals during the development of RP. Inflammatory mediators released from damaged or dying cells result in lymphocytes activating and infiltrating into lung tissue. Lymphocyte fractions in bronchi alveolar lavage fluid increased significantly at 1 month after radiotherapy of the lung cancer patients with RP.27 While the hypersensitivity reaction mediated by radiotherapy was elucidated, the immunosuppressive effects are becoming better explored. Radiotherapy was often accompanied by lymphopenia because of the high radiosensitivity of circulating lymphocytes. Thus, we hypothesize that the change of circulating lymphocyte subsets after radiotherapy may provide potentially important information of RP. In our study, the higher CD8+T cell count after radiotherapy were the unique risk factor associated with grade ≥2 RP by multivariable analysis. Zheng et al. found that circulating lymphocytes were not predictive for symptomatic RP in stage I NSCLC patients treated with SBRT.28 Zhou et al. showed that decrease of circulating lymphocyte count reflected the severity of RP and lower CD4+ T lymphocytes were associated with higher incidence of RP.29 The study did not include dosimetric parameters or pulmonary function in RP risk assessment, which may result in the different conclusion from our study. The mechanism behind the relationship between the higher CD8+ T cell count after radiotherapy and increased RP is still unclear.
Regarding radiotherapy technique, our study indicated that absolute decrease levels of total T cell count and CD4+ T cell count were larger after IMRT than HT. When adjustment was made for stage III–IV disease, the statistical significance remained. Our study is the first to compare the absolute decline of circulating lymphocyte subsets between HT and IMRT. Contrary to our study, Chen et al. found that SBRT group had less absolute lymphocyte count decline than traditional radiotherapy in lung cancer patients receiving combined immunotherapy and radiotherapy.30 A larger volume of lung tissues received low radiation doses during HT, resulting in a hypersensitivity immune reaction. We suspected that the decreased level of circulating lymphocyte subsets after HT was counteracted by the increased level due to the low dose radiation area. And a hypersensitivity immune reaction might be the reason for much more grade 5 RP in HT group by adjusted analyses. Furthermore, several studies indicated that lower lymphocyte values during definitive radiotherapy were associated with larger GTV and larger lung V5 in lung cancer patients.30,31 Similarly, Abravan et al. showed that mean lung dose, mean heart dose and vertebrae V20 had negative correlations with grade ≥ 3 lymphopenia in lung cancer cohort and was further tested in esophageal cancer cohort.11 However, neither PTV nor lung DVH had statistical significance for lymphocyte decrease in our study.
Besides the inherent bias of retrospective studies, some other limitations should be noted. Firstly, the patient and tumor characteristics had some heterogeneity, such as different stages from I to IV. To investigate this further, we conducted subgroup analyses for stage III–IV disease. Secondly, the sample size was small and the incidence of grade 2 RP was low, which may be insufficient to distinguish difference. Thirdly, survival outcome and other radiation-related adverse events were not analyzed between HT and IMRT.
Conclusion
In summary, for all lung cancer patients, despite larger PTV and more frequent systemic treatment in IMRT group than HT group, the incidence of grade ≥2 RP and grade 5 RP were comparable. When administering in stage III–IV disease, IMRT was associated with lower lung V10 and lower grade 5 RP than HT. Higher CD8+ T cell count after radiotherapy was the only risk factor associated with grade ≥2 RP. HT may better preserve total T cell and CD4+ T cell than IMRT. However, the mechanism behind the relationship between the circulating lymphocyte subsets and RP need further investigation.
Data Sharing Statement
All data included in this study are available upon request by contact with the corresponding author Wei Zhou.
Ethical Approval and Informed Consent
This study was approved by the ethics committee of the CQUCH. Informed consent for all patients was obtained prior to therapy and performed in accordance with the Declaration of Helsinki and Good Clinical Practice Guidelines.
Funding
Xin Zhang is supported by Science and Technology Research Project of Chongqing Education Commission (KJQN201900104). Xianfeng Liu is supported by the Performance Incentive Guide Special Project of Chongqing Scientific Research Institute [No. cstc2019jxjl130031]. Yongzhong Wu is supported by Integrated innovation and application of key technologies for precision prevention and treatment of primary lung cancer (2019ZX002).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mackie TR, Holmes T, Swerdloff S, et al. Tomotherapy: a new concept for the delivery of dynamic conformal radiotherapy. Med Phys. 1993;20(6):1709–1719. doi:10.1118/1.596958
2. Cattaneo GM, Dell’oca I, Broggi S, et al. Treatment planning comparison between conformal radiotherapy and helical tomotherapy in the case of locally advanced-stage NSCLC. Radiother Oncol. 2008;88(3):310–318. doi:10.1016/j.radonc.2008.06.006
3. Meng LL, Feng LC, Wang YL, Dai XK, Xie CB. Dosimetric comparison between helical tomotherapy and intensity-modulated radiation therapy plans for non-small cell lung cancer. Chin Med J. 2011;124(11):1667–1671.
4. Khalil AA, Hoffmann L, Moeller DS, Farr KP, Knap MM. New dose constraint reduces radiation-induced fatal pneumonitis in locally advanced non-small cell lung cancer patients treated with intensity-modulated radiotherapy. Acta Oncol. 2015;54(9):1343–1349. doi:10.3109/0284186X.2015.1061216
5. Kim K, Lee J, Cho Y, et al. Predictive factors of symptomatic radiation pneumonitis in primary and metastatic lung tumors treated with stereotactic ablative body radiotherapy. Radiat Oncol J. 2017;35(2):163–171. doi:10.3857/roj.2017.00066
6. Kong M, Lim YJ, Kim Y, et al. Diabetes mellitus is a predictive factor for radiation pneumonitis after thoracic radiotherapy in patients with lung cancer. Cancer Manag Res. 2019;11:7103–7110. doi:10.2147/CMAR.S210095
7. Wu K, Xu X, Li X, et al. Radiation pneumonitis in lung cancer treated with volumetric modulated arc therapy. J Thorac Dis. 2018;10(12):6531–6539. doi:10.21037/jtd.2018.11.132
8. Wirsdorfer F, Jendrossek V. The role of lymphocytes in radiotherapy-induced adverse late effects in the lung. Front Immunol. 2016;7:591.
9. Cho O, Oh YT, Chun M, Noh OK, Lee HW. Radiation-related lymphopenia as a new prognostic factor in limited-stage small cell lung cancer. Tumour Biol. 2016;37(1):971–978. doi:10.1007/s13277-015-3888-y
10. Ozsahin M, Crompton NE, Gourgou S, et al. CD4 and CD8 T-lymphocyte apoptosis can predict radiation-induced late toxicity: a prospective study in 399 patients. Clin Cancer Res. 2005;11(20):7426–7433. doi:10.1158/1078-0432.CCR-04-2634
11. Abravan A, Faivre-Finn C, Kennedy J, McWilliam A, van Herk M. Radiotherapy-related lymphopenia affects overall survival in patients with lung cancer. J Thorac Oncol. 2020;15(10):1624–1635. doi:10.1016/j.jtho.2020.06.008
12. Song CH, Pyo H, Moon SH, Kim TH, Kim DW, Cho KH. Treatment-related pneumonitis and acute esophagitis in non-small-cell lung cancer patients treated with chemotherapy and helical tomotherapy. Int J Radiat Oncol Biol Phys. 2010;78(3):651–658. doi:10.1016/j.ijrobp.2009.08.068
13. Kim Y, Hong SE, Kong M, Choi J. Predictive factors for radiation pneumonitis in lung cancer treated with helical tomotherapy. Cancer Res Treat. 2013;45(4):295–302. doi:10.4143/crt.2013.45.4.295
14. Yao B, Wang YD, Liu QZ. Radiation pneumonitis in non-small-cell lung cancer patients treated with helical tomotherapy. Niger J Clin Pract. 2016;19(1):25–29. doi:10.4103/1119-3077.173709
15. Arcangeli S, Agolli L, Portalone L, et al. Patterns of CT lung injury and toxicity after stereotactic radiotherapy delivered with helical tomotherapy in early stage medically inoperable NSCLC. Br J Radiol. 2015;88(1048):20140728. doi:10.1259/bjr.20140728
16. Figlia V, Mazzola R, Cuccia F, et al. Hypo-fractionated stereotactic radiation therapy for lung malignancies by means of helical tomotherapy: report of feasibility by a single-center experience. Radiol Med. 2018;123(6):406–414. doi:10.1007/s11547-018-0858-7
17. Mackie TR, Balog J, Ruchala K, et al. Tomotherapy. Semin Radiat Oncol. 1999;9(1):108–117. doi:10.1016/S1053-4296(99)80058-7
18. Chun SG, Hu C, Choy H, et al. Impact of intensity-modulated radiation therapy technique for locally advanced non-small-cell lung cancer: a secondary analysis of the NRG oncology RTOG 0617 randomized clinical trial. J Clin Oncol. 2017;35(1):56–62. doi:10.1200/JCO.2016.69.1378
19. Marks LB, Yorke ED, Jackson A, et al. Use of normal tissue complication probability models in the clinic. Int J Radiat Oncol Biol Phys. 2010;76(3 Suppl):S10–S19. doi:10.1016/j.ijrobp.2009.07.1754
20. Jo IY, Kay CS, Kim JY, et al. Significance of low-dose radiation distribution in development of radiation pneumonitis after helical-tomotherapy-based hypofractionated radiotherapy for pulmonary metastases. J Radiat Res. 2014;55(1):105–112. doi:10.1093/jrr/rrt080
21. Zhou Y, Yan T, Zhou X, et al. Acute severe radiation pneumonitis among non-small cell lung cancer (NSCLC) patients with moderate pulmonary dysfunction receiving definitive concurrent chemoradiotherapy: impact of pre-treatment pulmonary function parameters. Strahlenther Onkol. 2020;196(6):505–514. doi:10.1007/s00066-019-01552-4
22. Videtic GM, Stitt LW, Ash RB, et al. Impaired diffusion capacity predicts for decreased treatment tolerance and survival in limited stage small cell lung cancer patients treated with concurrent chemoradiation. Lung Cancer. 2004;43(2):159–166. doi:10.1016/j.lungcan.2003.08.026
23. Lopez Guerra JL, Gomez D, Zhuang Y, et al. Change in diffusing capacity after radiation as an objective measure for grading radiation pneumonitis in patients treated for non-small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2012;83(5):1573–1579. doi:10.1016/j.ijrobp.2011.10.065
24. Torre-Bouscoulet L, Munoz-Montano WR, Martinez-Briseno D, et al. Abnormal pulmonary function tests predict the development of radiation-induced pneumonitis in advanced non-small cell lung cancer. Respir Res. 2018;19(1):72. doi:10.1186/s12931-018-0775-2
25. Dehing-Oberije C, De Ruysscher D, van Baardwijk A, Yu S, Rao B, Lambin P. The importance of patient characteristics for the prediction of radiation-induced lung toxicity. Radiother Oncol. 2009;91(3):421–426. doi:10.1016/j.radonc.2008.12.002
26. Wang J, Cao J, Yuan S, et al. Poor baseline pulmonary function may not increase the risk of radiation-induced lung toxicity. Int J Radiat Oncol Biol Phys. 2013;85(3):798–804. doi:10.1016/j.ijrobp.2012.06.040
27. Yamagishi T, Kodaka N, Kurose Y, et al. Analysis of predictive parameters for the development of radiation-induced pneumonitis. Ann Thorac Med. 2017;12(4):252–258. doi:10.4103/atm.ATM_355_16
28. Zheng Y, Shi A, Wang W, et al. Posttreatment immune parameters predict cancer control and pneumonitis in stage I non-small-cell lung cancer patients treated with stereotactic ablative radiotherapy. Clin Lung Cancer. 2018;19(4):e399–e404. doi:10.1016/j.cllc.2017.12.012
29. Zhou P, Chen L, Yan D, et al. Early variations in lymphocytes and T lymphocyte subsets are associated with radiation pneumonitis in lung cancer patients and experimental mice received thoracic irradiation. Cancer Med. 2020;9(10):3437–3444. doi:10.1002/cam4.2987
30. Chen D, Patel RR, Verma V, et al. Interaction between lymphopenia, radiotherapy technique, dosimetry, and survival outcomes in lung cancer patients receiving combined immunotherapy and radiotherapy. Radiother Oncol. 2020;150:114–120. doi:10.1016/j.radonc.2020.05.051
31. Tang C, Liao Z, Gomez D, et al. Lymphopenia association with gross tumor volume and lung V5 and its effects on non-small cell lung cancer patient outcomes. Int J Radiat Oncol Biol Phys. 2014;89(5):1084–1091. doi:10.1016/j.ijrobp.2014.04.025
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.