")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Comparison of Psychological Difficulties in Patients with Migraine and Epilepsy Using PARADISE-24 Questionnaire
Authors Mirmosayyeb O, Shaygannejad V, Ghajarzadeh M
Received 5 May 2020
Accepted for publication 25 June 2020
Published 10 July 2020 Volume 2020:13 Pages 609—613
DOI https://doi.org/10.2147/JMDH.S260056
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Omid Mirmosayyeb, 1, 2,* Vahid Shaygannejad, 1, 3,* Mahsa Ghajarzadeh 2
1Isfahan Neurosciences Research Center, Isfahan University of Medical Sciences, Isfahan, Iran; 2Universal Council of Epidemiology (UCE), Universal Scientific Education and Research Network (USERN), Tehran University of Medical Sciences, Tehran, Iran; 3Department of Neurology, School of Medicine, Isfahan University of Medical Sciences, Isfahan, Iran
*These authors contributed equally to this work
Correspondence: Mahsa Ghajarzadeh
Universal Council of Epidemiology (UCE), Universal Scientific Education and Research Network (USERN), Tehran University of Medical Sciences, Tehran, Iran
Tel/ Fax +982166581560
Email [email protected]
Background: Patients with migraine or epilepsy suffer from a wide range of psychological difficulties, and various instruments are needed to separately assess each difficulty. However, the PARADISE-24 questionnaire is a comprehensive questionnaire for evaluating different psychological difficulties in cases with neurological disorders.
Objective: The aim of this study was to compare psychological difficulties in patients with migraine and those with epilepsy by using the PARADISE-24 questionnaire.
Methods: Overall, 240 migraineurs and 210 patients with epilepsy were enrolled. All the participants were asked to fill the Persian version of the PARADISE-24 questionnaire.
Results: In migraineurs, the mean age and mean headache severity (by means of visual analogue scale, VAS) were 38.6± 11.6 and 6.8± 2.8, respectively. In patients with epilepsy, the mean age and mean duration of the disease were 33.6± 13.4 and 12± 10.3 years, respectively. The mean PARADISE score was significantly higher in migraineurs than in epileptic cases (57.9± 12 vs 50.7± 15.1) (p< 0.001).
Conclusion: Patients with migraine suffer more from psychological difficulties than epileptic cases. This finding could help physicians to pay more attention to psychological well-being.
Keywords: migraine, epilepsy, psychological, Iran
A Letter to the Editor has been published for this article.
Introduction
Migraine is a devastating condition characterized by severe headache, and in some cases, accompanied by an aura.1 With the prevalence rate from 10% to 18%, it affects women more than men, yet the exact etiology is still unknown.2–4 It is the second cause of “years lost due to disability” (YLDs), imposing considerable costs to both patients and the health system.5
The other chronic condition is epilepsy that is characterized by unprovoked seizures, affecting all age groups (neonates to elderlies).6 Along with neurological disabilities, epilepsy causes psychological and psychiatric complications, affecting different aspects of life.7,8 People with epilepsy have a higher rate of mortality and a lower quality of life.9–11
Migraine and epilepsy are both among prevalent disabling conditions in all countries, including Iran. It is important to assess the impact of brain disorders on the patient’s life to help physicians better determine treatment outcomes and monitor the disease course, although there is no exact method to be used for this purpose. Some studies found a common pattern of psychosocial difficulties among patients with neurological disorders, so PARADISE-24 (Psychosocial fActors Relevant to BrAin DISorders in Europe) was developed by Cieza et al.12
We designed this study to compare psychological difficulties in patients with migraine and those with epilepsy, using PARADISE-24 questionnaire.
Methods
This cross-sectional study was conducted in Isfahan Neurosciences Research Center (INRC), Kashani hospital, between January and April 2020.
- Inclusion criteria for migraineurs were (a) headache history of more than two years, (b) diagnosis of migraine according to IHS ICHD-3 criteria, (c) patients under surveillance by a physician for headache treatment, (d) use of medications for3 16 weeks, and (e)
- 18 years of age and above.
Exclusion criteria for migraine group were:
- evidence of a secondary headache disorder attributed to
- head and/or neck trauma,
- cranial or cervical vascular disorder, or a n
- on-vascular cranial disorder,
- substance use or withdrawal,
- infection,
- hemostasis disorder,
- psychiatric disorder,
- current major medical illness such as malignancy,
- autoimmune or immune deficiency, diabetes mellitus, or u
- uncontrolled psychosis and pregnancy.
Inclusion criteria for epileptic cases were (a) diagnosis of epilepsy according to the International League Against Epilepsy (ILAE) Classification of the Epilepsies (2017) (b) 20 years of age or above; (c) two or more verified unprovoked epileptic seizures with at least 24-h time gap; and (d) at least one seizure within the previous 5 years.
Exclusion criteria for epileptic cases were:
- head and/or neck trauma
- migraine or other types of headache
- non-vascular cranial disorder
- substance use or withdrawal
- infection
- disorder of hemostasis
- psychiatric disorder
- current major medical illness such as malignancy, a
- autoimmune or immune deficiency, diabetes mellitus, or
- uncontrolled psychosis
- and pregnancy
All patients were asked to fill the informed consent forms before entering the study. The study was approved by the ethics committee of Isfahan university of medical sciences and that it was conducted in accordance with the Declaration of Helsinki.
The two patient groups were consecutively enrolled in the study, and the researcher was not blinded to the disease.
The PARADISE-24 is a self-report questionnaire, with questions answered on a 3-point scale (none =0, some =1, a lot = 2). The total score ranges from 0 to 100, while higher scores indicate psychosocial difficulties due to brain disorders.12
All participants were asked to fill a valid and reliable Persian version of the PARADISE-24 questionnaire.13
Data regarding age, sex, educational level, number of days per week with headache, frequency of headache per day, and severity of headache (using a visual analogue scale) were recorded for migraineurs cases. For epileptic cases, age, sex, educational level, duration of the disease, disease status (under control or not), and frequency of seizures per day were considered. Seizure-free was defined as having no attack for at least 1 year.
We used SPSS software version 22 (SPSS Inc., Chicago, IL, USA) to do data analysis. Data were presented as mean±SD for continuous and as frequencies for categorical variables. Independent sample t-test and Fisher exact test were used for comparison between quantitative and qualitative variables. A p-value of less than 0.05 was considered significant.
Results
The data were gathered from 240 migraineurs and 210 patients with epilepsy enrolled in this study. In migraineurs, mean age and mean headache severity were 38.6±11.6 and 6.8±2.8, respectively. The mean PARADISE score was 57.9±12 (Table 1).
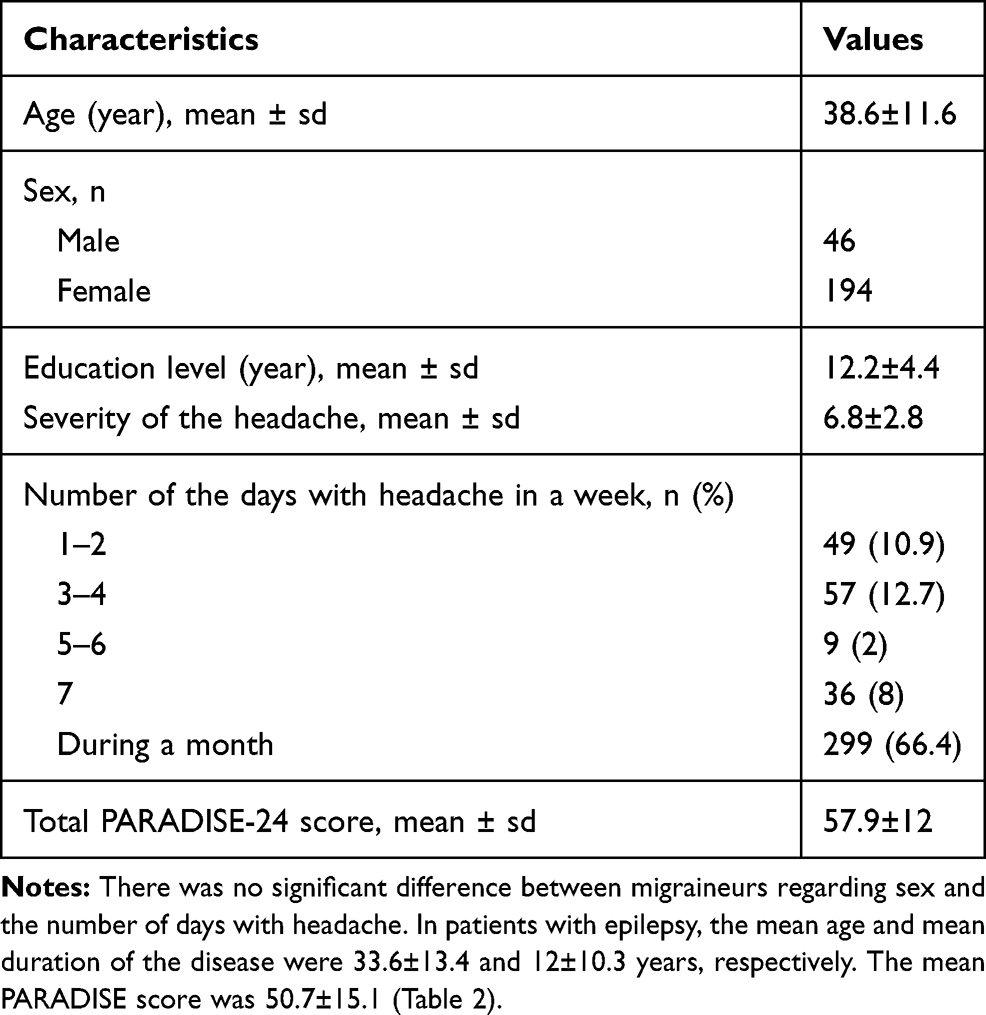 |
Table 1 Characteristics of Migraineurs |
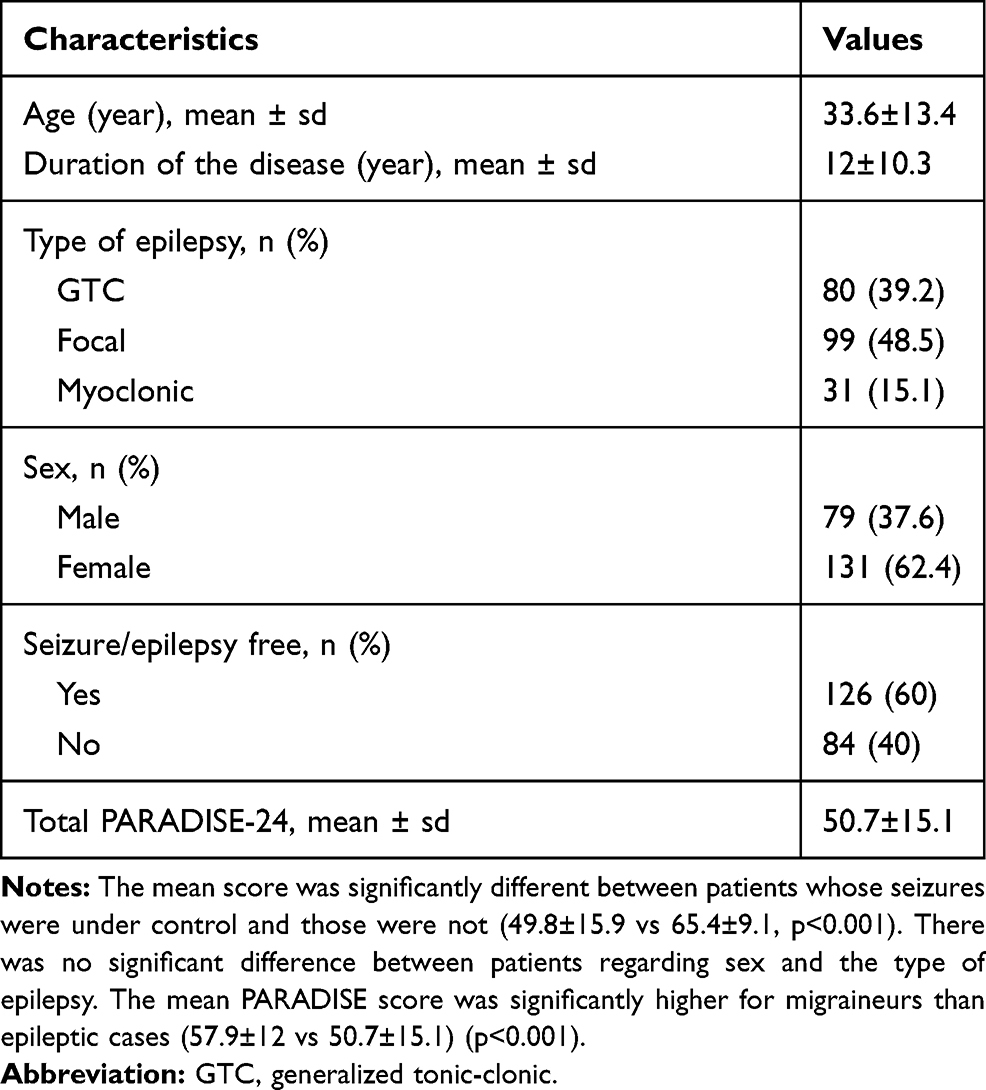 |
Table 2 Characteristics of the Patients with Epilepsy |
Discussion
The current study showed a significantly higher mean PARADISE score for migraineurs than patients with epilepsy, which indicates that patients with migraine suffer more from psychosocial difficulties than the other group.
In a previous study conducted by Raggi et al the mean PARADISE score in patients with migraine was reported as 59.9±7.6, which is higher than our score. Yet congruent with our findings, they reported no significant difference between male and female patients.14
Patients with migraine suffer from a wide range of psychological difficulties such as depression, poor sleep, sexual dysfunction, anxiety, and impaired quality of life,15,16 each of which requires a specific questionnaire or instrument to be assessed. One of the advantages of the PARADISE questionnaire is assessing various psychological aspects such as anxiety and depression, pain, sensory disturbances, and sleep difficulties.14
Migraine is a chronic disabling neurological disease, causing near 45 million years lived with disability (YLDs), and is the second disabling condition after low back pain.17 It affects occupational, social, economic, and personal aspects of life, and its consecutive complications, including psychological problems, impair the quality of life.18 The quality of life in migraineurs is inversely correlated with days with headache and headache-associated disabilities.19 Furthermore, many health conditions are considered to be associated with migraine, such as cardiovascular disease, epilepsy, multiple sclerosis, restless legs syndrome, fibromyalgia, asthma, allergic rhinitis, and systemic lupus erythematosus.18 These physical disorders, along with psychological problems, make migraine as one of the most devastating conditions that should be carefully monitored by physicians.
Epilepsy is another neurological disorder associated with lower quality of life and psychological problems such as sexual dysfunction, depression, anxiety, memory dysfunction, and stigma.20,21 To evaluate these complications, different instruments should be used, while the PARADISE-24 questionnaire provides a comprehensive assessment tool.
The mean PARADISE score in our patients with epilepsy was 50.7±15.1. According to Quintas et al study on 80 cases with epilepsy, the mean PARADISE score was 50.9±8.9, and the quality of life score was negatively related to the PARADISE score.22
Different somatic disorders have been considered to be associated with epilepsy, such as tumors, diabetes mellitus, migraine, chronic obstructive pulmonary disease (COPD), peptic ulcers, cardiovascular diseases, and cataract.23
Among neurological disorders, epilepsy accounts for the highest age-standardized DALY (the disability-adjusted life year) in both sexes, which is 0.7% of total DALYs.24
Epilepsy affects education, occupation, familial relations, and childbearing, which affects health-related quality of life.25 So, monitoring and careful evaluation of the patients play an important role in somatic and psychological well-being.
This study showed that patients with migraine suffer more from psychological problems than epileptic cases. This finding could guide the physicians to consider psychological well-being in migraineurs (clinical meaningfulness). However, it had some limitations: First, it was conducted in a single center. Second, we did not apply the quality of life instruments. Multi-centric studies with an evaluation of other aspects of the disease are recommended.
Conclusion
Patients with migraine suffer more from psychological difficulties than epileptic cases. This finding could help physicians to pay more attention to psychological well-being.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jalilian R, Ghajarzadeh M, Fateh R, Togha M, Sahraian MA, Azimi A. Comparison of sleep quality in women with migraine moreover, multiple sclerosis. Acta Med Iran. 2014;690–693.
2. Stovner LJ, Zwart JA, Hagen K, Terwindt G, Pascual J. Epidemiology of headache in Europe. Eur J Neurol. 2006;13(4):333–345. doi:10.1111/j.1468-1331.2006.01184.x
3. Woldeamanuel YW, Cowan RP. Migraine affects 1 in 10 people worldwide featuring recent rise: a systematic review and meta-analysis of community-based studies involving 6 million participants. J Neurol Sci. 2017;372:307–315. doi:10.1016/j.jns.2016.11.071
4. Buse DC, Rains JC, Pavlovic JM, et al. Sleep disorders among people with migraine: results from the chronic migraine epidemiology and outcomes (CaMEO) study. Headache. 2019;59(1):32–45. doi:10.1111/head.13435
5. Vos T, Abajobir AA, Abate KH. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet (London, England). 2017;390(10100):1211–1259. doi:10.1016/S0140-6736(17)32154-2
6. Song P, Liu Y, Yu X, et al. Prevalence of epilepsy in China between 1990 and 2015: a systematic review and meta-analysis. J Glob Health. 2017;7(2):020706. doi:10.7189/jogh.07.020706
7. Tellez‐Zenteno JF, Patten SB, Jetté N, Williams J, Wiebe S. Psychiatric comorbidity in epilepsy: a population‐based analysis. Epilepsia. 2007;48(12):2336–2344. doi:10.1111/j.1528-1167.2007.01222.x
8. Hermann B, Seidenberg M, Jones J. The neurobehavioural comorbidities of epilepsy: can a natural history be developed? Lancet Neurol. 2008;7(2):151–160. doi:10.1016/S1474-4422(08)70018-8
9. Thurman DJ, Beghi E, Begley CE, et al. Standards for epidemiologic studies and surveillance of epilepsy. Epilepsia. 2011;52:2–26. doi:10.1111/j.1528-1167.2011.03121.x
10. Ngugi AK, Bottomley C, Kleinschmidt I, Sander JW, Newton CR. Estimation of the burden of active and life‐time epilepsy: a meta‐analytic approach. Epilepsia. 2010;51(5):883–890. doi:10.1111/j.1528-1167.2009.02481.x
11. Baker GA, Jacoby A, Buck D, Stalgis C, Monnet D. Quality of life of people with epilepsy: a European study. Epilepsia. 1997;38(3):353–362. doi:10.1111/j.1528-1157.1997.tb01128.x
12. Cieza A, Sabariego C, Anczewska M, et al. PARADISE 24: a measure to assess the impact of brain disorders on people’s lives. PLoS One. 2015;10(7):7. doi:10.1371/journal.pone.0132410
13. Azimi ADR, Mohammad Vali Samani S, Roostaei B, Hamtaei Gashti S, Navardi S, Ghajarzadeh M.Psychometric properties of the Persian version of the PARADISE-24 questionnaire, Running title: Persian version of the PARADISE-24 questionnaire. IJPM.2020 IP.
14. Raggi A, Covelli V, Schiavolin S, et al. Psychosocial difficulties in patients with episodic migraine: a cross-sectional study. Neurol Sci. 2016;37(12):1979–1986. doi:10.1007/s10072-016-2705-8
15. Lantéri-Minet M, Radat F, Chautard M-H, Lucas C. Anxiety and depression associated with migraine: influence on migraine subjects’ disability and quality of life, and acute migraine management. Pain. 2005;118(3):319–326. doi:10.1016/j.pain.2005.09.010
16. Ghajarzadeh M, Jalilian R, Togha M, Azimi A, Hosseini P, Babaei N. Depression, poor sleep, and sexual dysfunction in migraineurs women. Int J Prev Med. 2014;5(9):1113.
17. Stovner LJ, Nichols E, Steiner TJ, et al. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018;17(11):954–976. doi:10.1016/S1474-4422(18)30322-3
18. Burch RC, Buse DC, Lipton RB. Migraine: epidemiology, Burden, and Comorbidity. Neurol Clin. 2019;37(4):631–649. doi:10.1016/j.ncl.2019.06.001
19. Abu Bakar N, Tanprawate S, Lambru G, Torkamani M, Jahanshahi M, Matharu M. Quality of life in primary headache disorders: a review. Cephalalgia. 2016;36(1):67–91. doi:10.1177/0333102415580099
20. Quintas R, Raggi A, Giovannetti AM, et al. Psychosocial difficulties in people with epilepsy: a systematic review of literature from 2005 until 2010. Epilepsy Behav. 2012;25(1):60–67. doi:10.1016/j.yebeh.2012.05.016
21. Morrell MJ. Sexual dysfunction in epilepsy. Epilepsia. 1991;32(s6):S38–S45. doi:10.1111/j.1528-1157.1991.tb05891.x
22. Quintas R, Cerniauskaite M, Giovannetti AM, et al. PARADISE 24 instrument: an observational study on psychosocial difficulties, quality of life, and disability levels in patients with epilepsy. Epilepsy Behav. 2016;64:160–165. doi:10.1016/j.yebeh.2016.08.019
23. Beghi E. Addressing the burden of epilepsy: many unmet needs. Pharmacol Res. 2016;107:79–84. doi:10.1016/j.phrs.2016.03.003
24. Whiteford HA, Ferrari AJ, Degenhardt L, Feigin V, Vos T. Global burden of mental, neurological, and substance use disorders: an analysis from the Global Burden of Disease Study 2010. Mental Neurol Subst Use Disord. 2015;29.
25. Cianchetti C, Messina P, Pupillo E, et al. The perceived burden of epilepsy: impact on the quality of life of children and adolescents and their families. Seizure. 2015;24:93–101. doi:10.1016/j.seizure.2014.09.003
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.