")
Back to Journals » Drug Design, Development and Therapy » Volume 16
Comparison of Metaraminol, Phenylephrine, and Norepinephrine Infusion for Prevention of Hypotension During Combined Spinal-Epidural Anaesthesia for Elective Caesarean Section: A Three-Arm, Randomized, Double-Blind, Non-Inferiority Trial
Authors Zhou Y, Yu Y, Chu M, Zhang Y, Yu X, Chen G
Received 26 July 2021
Accepted for publication 15 December 2021
Published 7 January 2022 Volume 2022:16 Pages 117—127
DOI https://doi.org/10.2147/DDDT.S331177
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Manfred Ogris
Youfa Zhou,1,* Yunyun Yu,1,2,* Miaofei Chu,1,3 Yanting Zhang,1 Xin Yu,1 Gang Chen1
1Department of Anesthesiology, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Anesthesiology, Lishui Central Hospital, Lishui, Zhejiang, People’s Republic of China; 3Department of Anesthesiology, Zhejiang Greentown Cardiovascular Hospital, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Gang Chen Tel +8613757118681
Fax +8657186044817
Email [email protected]
Background: A direct comparison of phenylephrine, metaraminol, and norepinephrine in preventing hypotension during spinal anaesthesia for elective caesarean section has never been made.
Patients and Methods: Seventy-five parturients scheduled for elective caesarean section were randomly assigned into the three groups. After spinal anaesthesia induction, patients received a bonus dose of vasopressor (norepinephrine 4ug, phenylephrine 50ug, or metaraminol 250ug) combined with continuous infusion (norepinephrine 8ug/mL, phenylephrine 100ug/mL, or metaraminol 500ug/mL) at a rate of 30 mL/h to prevent hypotension. The primary outcome was umbilical arterial (UA) pH and other intraoperative data were also recorded.
Results: The UA pH was 7.32± 0.03 for metaraminol, 7.31± 0.03 for phenylephrine, and 7.31± 0.03 for norepinephrine. The 95% CI of MD was – 0.011 to 0.026 comparing metaraminol with norepinephrine and 0.0181 to 0.0182 comparing phenylephrine with norepinephrine. Both lower bounds of the 95% CI of MD were above the predetermined lower boundary of clinical non-inferiority of − 0.03, indicating both metaraminol and phenylephrine were non-inferior to norepinephrine. Moreover, the incidence of hypotension was lower in metaraminol compared with norepinephrine (P = 0.01). However, the incidence of hypertension was significantly lower in both phenylephrine and metaraminol compared with norepinephrine.
Conclusion: Both metaraminol and phenylephrine were non-inferior to norepinephrine with respect to neonatal UA pH when used as a bolus and continuous infusion to prevent hypotension during combined spinal-epidural anaesthesia for elective caesarean section.
Keywords: caesarean section, hypotension, metaraminol, phenylephrine, norepinephrine
Introduction
Caesarean section is one of the most commonly performed surgical procedures; spinal anaesthesia and combined spinal-epidural anaesthesia are the most commonly used methods of anaesthesia for caesarean section. However, their use is associated with a high incidence of hypotension, which can result in adverse maternal and fetal outcomes.1 A number of methods to prevent hypotension have been investigated and prophylactic infusion of vasopressors is commonly recommended.2,3
In the last decade, phenylephrine has been widely used as a vasopressor for maintaining blood pressure (BP) during spinal anaesthesia for caesarean delivery.4 However, as a pure the α-agonist, phenylephrine is often associated with baroreceptor-mediated bradycardia and thus leads to a subsequent decrease in cardiac output (CO).5 Although the decrease in CO is generally back to the pre-spinal anesthetic baseline in a short time,6 it may cause adverse effects in some high-risk situations such as maternal cardiac disease, placental insufficiency, and fetal distress.
Norepinephrine with α- agonist and slight β-agonist activity has been put forward as an alternative vasopressor during caesarean section due to its ability to treat hypotension while maintaining heart rate (HR).7 Moreover, recent studies have suggested that norepinephrine is non-inferior at maintaining BP while conferring a greater HR and CO compared with phenylephrine,6,8 which indicated that norepinephrine is the superior vasopressor for use in obstetric spinal anaesthesia.
Metaraminol, another vasopressor with α- and β-agonist activity, has also been suggested to be effective in the management of maternal hypotension during caesarean section.9–11 It was reported that metaraminol is at least non-inferior to phenylephrine in preventing hypotension of parturients concerning neonatal acid-base outcomes.12 However, there is still no study that directly compares metaraminol with norepinephrine in preventing hypotension of parturients with spinal anaesthesia.
The aim of this prospective, three-arm, randomized, double-blind trial was to directly compare the effect of prophylactic infusions of metaraminol, phenylephrine, and norepinephrine in women undergoing elective caesarean section under combined spinal-epidural (CSE) anaesthesia. We assumed that both metaraminol and phenylephrine infusions would be non-inferior to norepinephrine infusion to prevent maternal hypotension concerning neonatal acid-base status.
Patients and Methods
Ethics
This prospective, three-arm, randomized, double-blind non-inferiority trial (KY20191203-14) was conducted after obtaining approval from the Clinical Research Ethics Committee of Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University (Chairperson Prof Limin Liu) on December 03, 2019. The trial was registered before patient enrollment in the Chinese Clinical Trial Registry (registration No. ChiCTR1900028150; principal investigator, Chen Gang; date of registration, December 13, 2019) and conducted in accordance with the Declaration of Helsinki. All patients gave written informed consent before recruitment.
Patients and Randomization
Full-term pregnant women aged over 18 years old scheduled for elective caesarean section were recruited. Exclusion criteria were American Society of Anesthesiologists physical status ≥ 3, weight <50 kg or >100kg, height <140 cm or >180 cm, preexisting or pregnancy-induced hypertension, known fetal abnormality or intrauterine growth restriction, known cardiovascular or cerebrovascular disease, thrombocytopenia, coagulopathy, any medical contraindication to combined spinal-epidural anaesthesia, known allergy to phenylephrine, norepinephrine or metaraminol, inability or refusal to give informed consent. Patients were excluded from subsequent analysis if combined spinal-epidural (CSE) anaesthesia was not established successfully, epidural drugs were required before delivery of the fetus, or severe shivering made non-invasive blood pressure monitoring unreliable.
Patients were randomly assigned in 1:1:1 ratios using computer-generated random number sequence in blocks of six to metaraminol group (M group), phenylephrine group (P group), or norepinephrine group (N group). The randomization codes were concealed in consecutively numbered, sealed opaque envelopes by a secretarial staff who was not involved with the following study. The envelope was opened just before the enrolled patients entered the operation room.
A researcher who had no role in patient management or data collection and analysis opened the envelope and prepared two syringes, one 5-mL syringe labeled “bolus” the other 50-mL syringe labeled “infusion” for each patient. In group M, the bolus syringe contained 1.25mg metaraminol (250 µg/mL) and the infusion syringe contained 25mg metaraminol (500 µg/mL). In group P, the bolus syringe contained 250µg phenylephrine (50 µg/mL) and the infusion syringe contained 5000 µg phenylephrine (100µg/mL). In group N, the bolus syringe contained 20µg norepinephrine (4 µg/mL) and the infusion syringe contained 400µg norepinephrine (8 µg/mL). The study drugs were administered by the Anesthesiologist who was blinded to the group assignment. The infusion syringe was placed in a syringe pump (Graseby 3500 Anaesthesia Pump; Graseby Medical Ltd, Watford, UK) that was connected to a 3-way stopcock attached directly to the patient’s IV cannula.
Procedures
All participants were fasted for at least 8 hours before surgery and no premedication was given. An 18-G IV catheter was inserted and no prehydration was given in the holding area. Upon entering the operating room, the patient was positioned supine with left uterine displacement by tilting the operating table to the left, and standard monitoring including noninvasive BP, pulse oximetry, and 5-lead electrocardiography was applied. We allowed patients to rest for several minutes before baseline values for systolic BP (SBP) and maternal HR were recorded as the means of three consecutive readings with a difference of no more than 10% at 3 min intervals. Blood pressure was measured at 1-min intervals after induction of spinal anaesthesia and 5-min intervals after delivery of the fetus.
Combined spinal-epidural anaesthesia was performed with patients in the right lateral position at the L2–3 or L3–4 vertebral interspace. After confirming cerebrospinal fluid (CSF), 2.5 mL hyperbaric bupivacaine 0.5% was injected into the subarachnoid space over 30 seconds. Gentle aspiration was applied to verify the successful administration of the spinal solution during the injection of local anesthetics.
Immediately after the injection of the spinal anesthetic, a 1-mL bolus of the solution from the bolus syringe was administered and the continued infusion was started at a rate of 30 mL/h. Simultaneously, 10 mL/kg of lactated Ringer’s solution was infused over 20–30 minutes. After that, the rate of Ringer’s solution was then reduced to 1 mL/kg/h to keep the vein open until delivery of the fetus.
An 18-gauge epidural catheter was inserted and secured. The catheter was gently aspirated and observed for the presence of blood or CSF and was then flushed with 3 mL saline. No epidural test dose was given. Patients were positioned supine with left uterine displacement, and 5 L/min oxygen was delivered via a face mask. The sensory block level was defined as any loss of cold sensation to ice. Surgery was not permitted until the sensory block to the T5 dermatome was confirmed.
Measurements
Blood pressure and heart rate were measured at 1-minute intervals. If the systolic arterial pressure decreased to <90% baseline at any time, the study drug infusion rate was increased by 5 mL/h. If the systolic arterial pressure fell to <80% baseline, a bolus of 1 mL study drug was given. If at any time, the SBP rose>110% baseline, the infusion rate was reduced by 5 mL/h. If a reading >120% baseline occurred, the infusion was stopped until pressure returned to <120% baseline. Bradycardia was defined as HR < 50 beats/min. If bradycardia was accompanied by hypotension, it was treated with an IV bolus of 0.5 mg atropine; if not accompanied by hypotension, the infusion was stopped and then restarted when HR exceeded 50 beats/min. The study ended at the delivery of the fetus. Arterial and venous blood samples were taken from a double-clamped segment of the umbilical cord by the obstetrician at birth and immediately analyzed through a blood gas analyzer in the operative room by an investigator who was blinded to the patient allocation.
Demographic characteristics of participants including age, height, and weight were recorded, as well as the duration of surgery, induction-to-delivery interval, uterine incision-to-delivery interval, and the number of physician interventions (such as stopping or restarting infusion, administering rescue bolus). Episodes of hypotension (defined as SBP below the 80% of baseline value), hypertension (defined as SBP above the 120% of baseline value), bradycardia, nausea, vomiting, dizziness, and chest distress were recorded. Neonatal Apgar scores were assessed by the neonatology team at 1 min and 5 min after birth. The anesthesiologist who recorded the above data was also blinded to the group assignment.
The primary outcome was umbilical artery (UA) pH and other intra-operative outcomes were secondary outcomes in the current study.
Sample Size Calculation
The sample size for this three-arm trial was determined according to the primary outcome of UA pH. Based on the data from our clinical practice, the primary endpoint standard deviation (SD) was assumed to be 0.03. A non-inferiority margin of 0.03 was adopted in our study in accordance with the previous studies.4,12 One-tailed power analysis for the outcome of UA pH indicated that a sample size of 21 patients per group would provide at least 90% power with an alpha of 0.025 to demonstrate the non-inferiority of both metaraminol and phenylephrine to norepinephrine (PASS 2008; NCSS, Kaysville, Utah, USA). Therefore, we planned to recruit 25 patients in each group to compensate for dropouts.
Statistical Analysis
All of our analyses were performed using a per-protocol approach. The Shapiro–Wilk test was used to confirm the normality of data distribution. We presented continuous data as mean ± SD and a one-way ANOVA combined with the Tukey’s test for post hoc testing was used in analyzing the normally distributed data; Nonparametric data were reported as median (25th, 75th percentiles) and were analyzed using the Kruskal–Wallis test with the Dunn’s test for post hoc testing. The categorical data were presented as numbers or percentages and the chi-square test was used in analyzing the categorical data. P<0.05 was considered significant. If the significant effect was indicated among three groups in chi-square, pairwise chi-square comparisons were followed with a more conservative alpha level of 0.017. Non-inferiority testing was done by comparing the 95% CI of the difference between groups to the predetermined non-inferiority margin of −0.03. Since the interval till delivery varied among patients, intergroup trends of SBP and heart rate for 15 minutes from vasopressor administration were compared. Serial changes in SBP and HR were analyzed using a 2-factor (treatment and time) repeated measures analysis of variance model. The outliers were detected by judging whether the studentized residuals exceed ±3 times the SD. The normality of data distribution was tested through the analysis of studentized residuals and the Shapiro–Wilk test. The sphericity was estimated by the Mauchly test. If the Mauchly test was significant, Greenhouse-Geisser epsilon adjustment was adopted. If there was a significant difference between groups, we performed simple comparisons between groups for all time levels with Bonferroni adjustments. The above statistical analyses were performed by GraphPad Prism version 5.0 (GraphPad Software Inc., San Diego, CA, USA) and IBM SPSS Statistics for Windows version 22.0 (IBM Corp, Armonk, NY, USA).
Results
A total of 253 patients were screened for eligibility from December 13, 2019, to March 11, 2020. Among them, 178 were excluded (95 did not meet exclusion criteria, 78 refused to participate in the trial, 5 had their surgery canceled). A total of 75 patients were randomized, allocated, completed the study protocol, and had their data analyzed (25 patients in each group). The CONSORT flow diagram showing the research progress is presented in Figure 1. There were no statistically significant differences in maternal characteristics, baseline SBP and surgical time from incision to delivery among the three groups (Table 1).
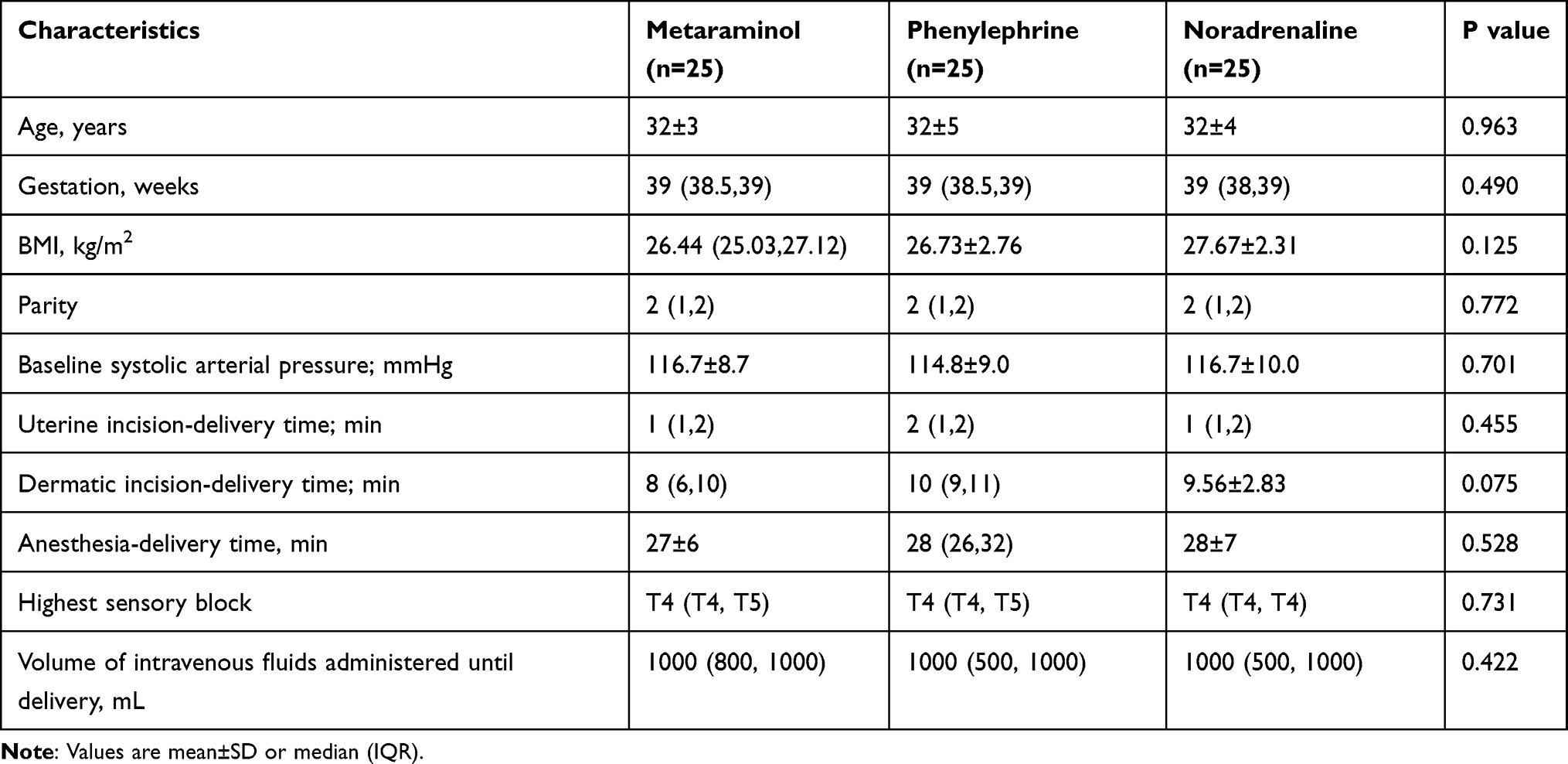 |
Table 1 Patient and Procedural Characteristics |
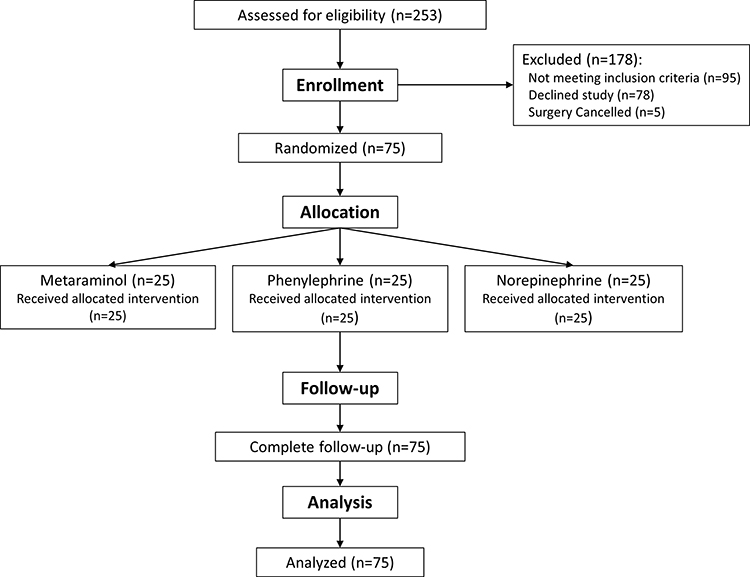 |
Figure 1 CONSORT diagram. |
Non-inferior was showed for both metaraminol and phenylephrine compared with norepinephrine with a non-inferiority margin of 0.03 units. In the comparison of metaraminol and norepinephrine, the umbilical arterial pH was 7.32±0.03 for metaraminol and 7.31±0.03 for norepinephrine (n=25; difference 0.008; 95% CI 0.011–to 0.026). Comparing phenylephrine with norepinephrine, the umbilical arterial pH was 7.31±0.03 in both groups. The estimated mean difference was nearly 0 and the 95% CI of the estimated difference was −0.0181 to 0.0182. Both lower bounds of the 95% CI of the estimated difference in the above two comparisons were above the predetermined lower boundary of clinical non-inferiority of −0.03, indicating that both metaraminol and phenylephrine were non-inferior to norepinephrine (Figure 2). Other neonatal outcomes were not different across the three groups except for the umbilical arterial pO2, which was significantly higher in the M group compared with the N group (Table 2).
 |
Table 2 Umbilical Vessel Biochemical Values and Apgar Scores in Neonates |
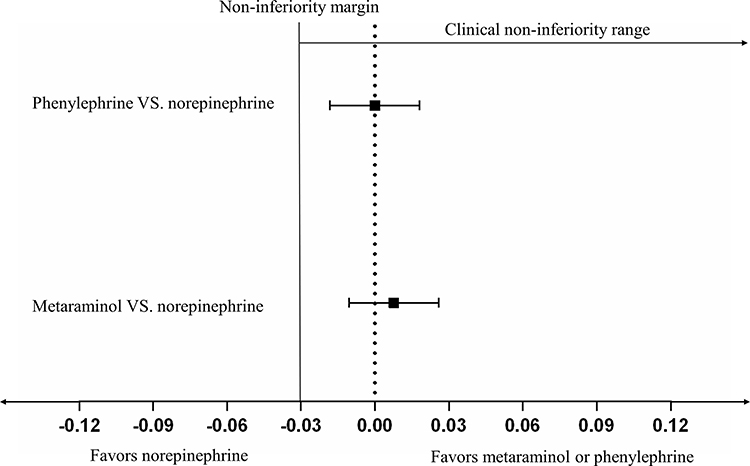 |
Figure 2 Differences in umbilical arterial pH compared both metaraminol group and phenylephrine group with norepinephrine group. The confidence intervals of both comparisons do not cross the non-inferiority margin, which was set at −0.03 pH units, indicating that both phenylephrine and metaraminol are non-inferior to norepinephrine. |
For the intra-operative outcomes of the participants, there was no significant difference among the three groups with respect to the incidence of bradycardia, dizziness, chest distress, nausea, and vomiting. Significant differences in the incidence of hypotension, hypertension, the number of rescue bolus doses, and pump adjustments among the three groups were indicated by the chi-square test. Moreover, the pairwise chi-square comparisons with a more conservative alpha level of 0.017 suggested that the incidence of hypotension was significantly lower in the M group compared with the N group. However, the number of pump adjustments and the incidence of hypertension were significantly higher in the P group and M group compared with the N group (Table 3).
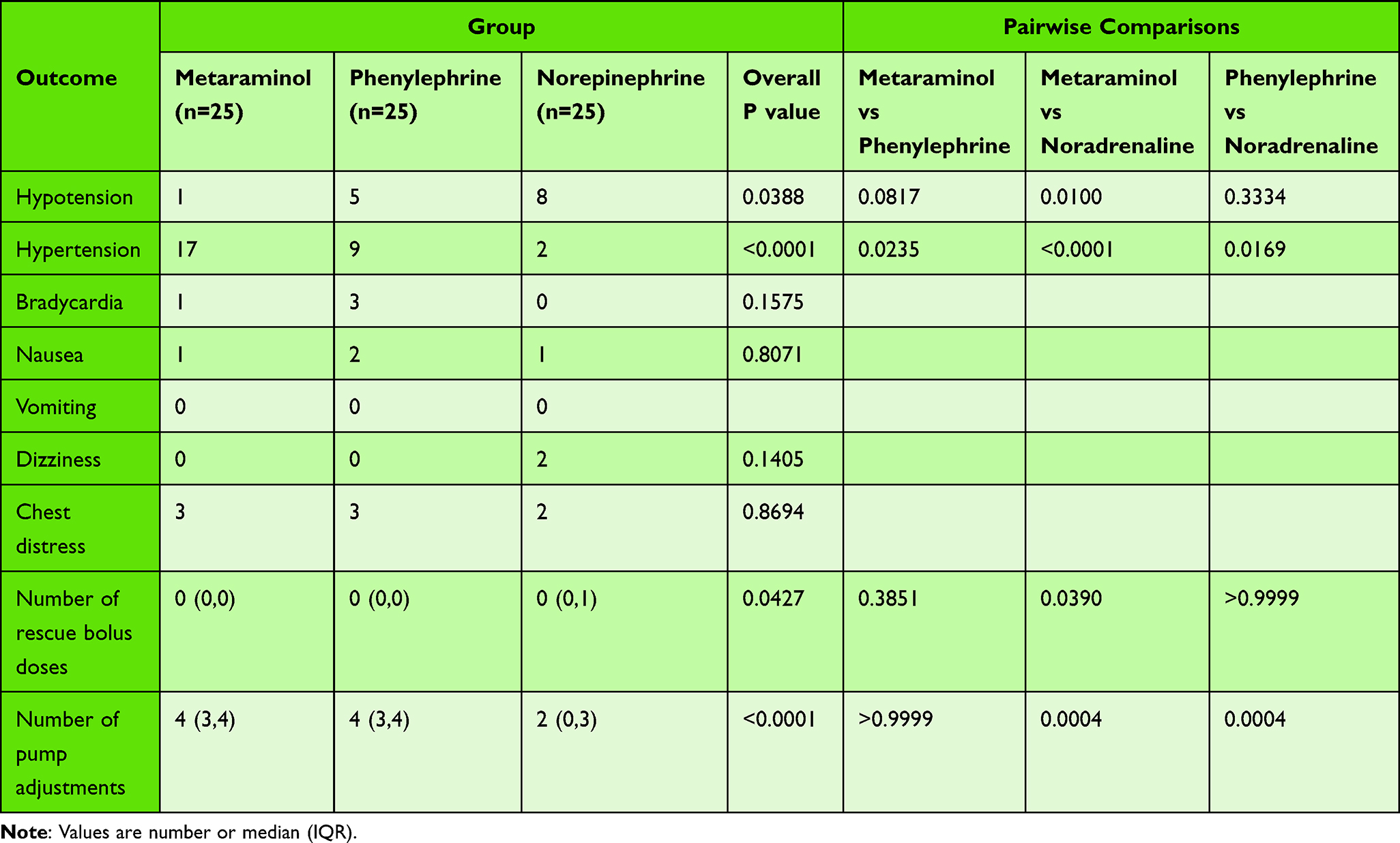 |
Table 3 Intraoperative Data of Different Groups |
Serial changes of SBP and HR were respectively presented in Figures 3 and 4. In general, the M group had higher SBP compared with the N group and the P group (Figure 3); the N group had higher HR compared with the M group and the P group in most readings (Figure 4).
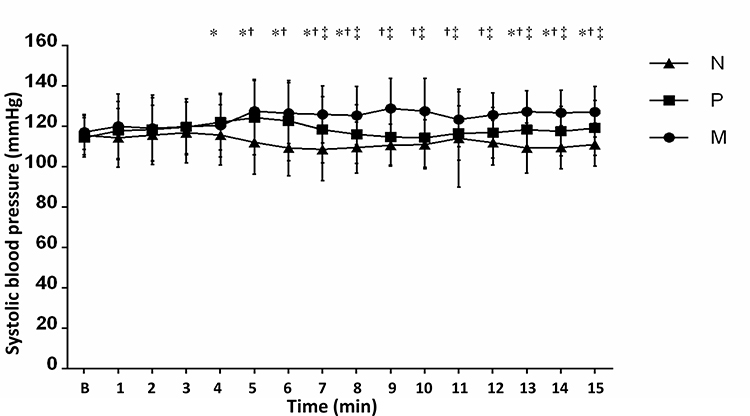 |
Figure 3 Serial changes in SBP in the first 15 min after induction of spinal anaesthesia for different groups. Data are shown as mean (standard deviation, SD). *Statistical significance between the P group and the N group. †Statistical significance between the M group and the N group. ‡Statistical significance between the M group and the P group. |
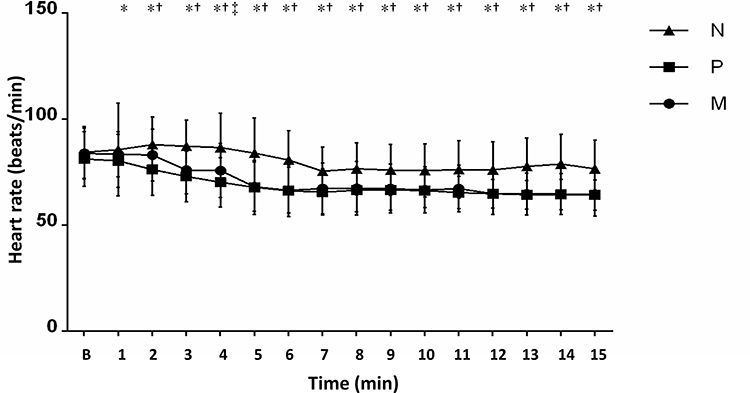 |
Figure 4 Serial changes in HR in the first 15 min after induction of spinal anaesthesia for different groups. Data are shown as mean (standard deviation, SD). *Statistical significance between the P group and the N group. †Statistical significance between the M group and the N group; ‡Statistical significance between the M group and the P group. |
Discussion
In the current study, we found that prophylactic use of both metaraminol and phenylephrine infusions to prevent maternal hypotension in caesarean section were non-inferior to norepinephrine infusion concerning neonatal umbilical arterial pH. However, the umbilical arterial pO2 was significantly higher in the M group compared with the N group. Moreover, the incidence of hypotension was significantly lower in the M group compared with the N group and the number of pump adjustments and the incidence of hypertension were significantly higher in the P group and M group compared with the N group. In addition, significant differences were indicated in SBP and HR at each time interval among the three groups except during the first 1 to 5 minutes.
UA pH is a well-established measure of neonatal condition at birth that reflects both the metabolic and the respiratory parts of fetal acidaemia. The respiratory fetal acidaemia is mainly caused by carbon dioxide accumulation due to acute insufficient perfusion of the placenta. Both spinal anaesthesia and intraoperative vasopressors administration are risk factors of the acute insufficient perfusion of the placenta. BE is also an appropriate indicator of outcome since it reflects the metabolic fetal acidaemia. However, a previous study suggested that the metabolic component does not predict those at risk of adverse outcomes once pH is taken into account.13 Therefore, we took the UA pH as the primary outcome. Nonetheless, we compared UA BE among groups as a secondary outcome.
In consideration of the reflex decrease in HR and an associated decrease in CO induced by a pure vasoconstrictor, alternative agents such as dilute norepinephrine and metaraminol combine α- and β-adrenergic receptor agonist activity and may be a more ideal agent for the management of spinal-induced hypotension. Several studies comparing norepinephrine and phenylephrine for preventing hypotension during spinal anaesthesia for caesarean section have been conducted in recent years.6,8,14–17 However, most of the previous studies focused on hemodynamic differences between norepinephrine and phenylephrine with fetal outcomes included as secondary outcomes. In the current study, we took UA pH as the primary outcome and found that phenylephrine was non-inferior to norepinephrine concerning the fetal outcome which was consistent with a newly published study.18 Unlike the newly published study, we also compared norepinephrine with metaraminol which is another alternative agent with combined α- and β-adrenergic receptor agonist activity in the current study. There is still no published study that compared norepinephrine with metaraminol in preventing hypotension during caesarean section. The current study for the first time demonstrated that metaraminol was also non-inferior to norepinephrine regarding UA pH. Moreover, the other outcomes of UA and UV blood gases were also comparable among the three groups including BE. However, there is an exception that the umbilical arterial pO2 was significantly higher in the M group compared with the N group. The difference in maternal hemodynamics between the two groups may account for this phenomenon. As showed in the current study, the SBP and HR were relatively stable in the three groups and sufficient perfusion of the placenta was indicated by normal UA pH. However, the SBP in the M group was the highest one among the three groups at most time intervals with SBP in the N group being the lowest one. Therefore, the fetuses in group M will have a more adequate supply of oxygen manifested as higher umbilical arterial pO2.
Many studies have investigated the potency ratio for norepinephrine/phenylephrine. At first, Ngan et al suggested that the potency ratio for norepinephrine/phenylephrine was 17:1 (norepinephrine 6 μg equivalent to phenylephrine 100 μg).6 However, the subsequent works suggested that the real potency ratio may be smaller with a potency ratio of 13:1 (norepinephrine 7.6 μg equivalent to phenylephrine 100μg)19 and 11:1 (norepinephrine 8.8 μg equivalent to phenylephrine 100μg).20 Therefore, we chose to study norepinephrine at a concentration of 8μg/mL and phenylephrine at 100μg/mL. Since the potency ratio for metaraminol/ phenylephrine has been widely demonstrated to be 5:1, we studied metaraminol at 500μg /mL. Moreover, some studies have suggested that a bolus of vasoconstrictor before starting continuous infusion may reduce the rates of maternal hypotension and nausea.21,22 Therefore, we gave the participants a bolus of norepinephrine 4 μg, phenylephrine 50 μg, or metaraminol 250 μg before starting the continuous infusion. A rate of 25–50 μg/min was reported to provide the best balance in maintaining maternal blood pressure without reactive hypertension or bradycardia23,24 for phenylephrine. Therefore, the initial infusion rate was set to 30 mL/h (50 ug/min for phenylephrine) in all groups to ensure the anesthesiologists were blinded to the patients’ allocation.
In the current study, we found that most intra-operative data including the incidence of bradycardia, dizziness, chest distress, nausea, and vomiting were comparable among the three groups. However, the incidence of hypotension was significantly lower in the M group compared with the N group and the number of pump adjustments and the incidence of hypertension was significantly higher in the P group and M group compared with the N group. In addition, the M group had higher SBP compared with the N group and P group at most time points. Regardless of the potential differences in pharmacodynamics, metaraminol may have an advantage over phenylephrine or norepinephrine due to the potential bias induced by drug preparation for infusion. A very small part of the solution will inevitably remain in the ampoules, which will cause the deviation between the actual concentration and the target concentration. The concentration deviation caused by the dilution process is most obvious in the N group among the three groups due to its highest potency. Therefore, the incidence of hypotension could be significantly higher in the N group compared with the M group due to concentration deviation related to the huge difference in their potencies. The above reason could also account for the differences in the incidence of hypertension, the number of pump adjustments, and serial SBP among the three groups.
There are some limitations in our study. Firstly, the subjects were all healthy women and fetuses. The results might not be applicable for women with cardiovascular disease or fetuses with uteroplacental insufficiency. Secondly, not all cases were the first cases of the day, therefore, women who have longer fasting periods may be more likely to suffer from intraoperative hypotension due to fasting. In addition, there may be potential bias in the process of drug preparation for infusion which may affect the authenticity of the results.
Conclusion
Both metaraminol and phenylephrine were non-inferior to norepinephrine in preventing maternal hypotension during caesarean section concerning neonatal UA pH. Future studies should be performed to further compare the potential differences among phenylephrine, metaraminol, and norepinephrine on side effects or obstetric outcomes.
Data Sharing Statement
The de-identified data for individual participants underlying our results can be accessed with approval from the corresponding author 6 months after publication. The study protocol, statistical analyses, and clinical study report will also be available.
Acknowledgments
Assistance with the study: all the staff at the department of anesthesiology, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University for their help in this study.
Financial support and sponsorship: This work was supported by the Natural Science Foundation of Zhejiang Province (grant number: LZ19H090003) and the Health Commission of Zhejiang Province (grant number: 2021KY176).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Reynolds F, Seed PT. Anaesthesia for Caesarean section and neonatal acid-base status: a meta-analysis. Anaesthesia. 2005;60(7):636–653. doi:10.1111/j.1365-2044.2005.04223.x
2. Chooi C, Cox JJ, Lumb RS, et al. Techniques for preventing hypotension during spinal anaesthesia for caesarean section. Cochrane Database Syst Rev. 2020;7:CD002251. doi:10.1002/14651858.CD002251.pub4
3. Kinsella SM, Carvalho B, Dyer RA, et al. International consensus statement on the management of hypotension with vasopressors during caesarean section under spinal anaesthesia. Anaesthesia. 2018;73(1):71–92. doi:10.1111/anae.14080
4. Lee A, Ngan Kee WD, Gin T. A quantitative, systematic review of randomized controlled trials of ephedrine versus phenylephrine for the management of hypotension during spinal anaesthesia for caesarean delivery. Anesth Analg. 2002;94(4):920–6, table of contents. doi:10.1097/00000539-200204000-00028
5. Doherty A, Ohashi Y, Downey K, Carvalho JC. Phenylephrine infusion versus bolus regimens during caesarean delivery under spinal anaesthesia: a double-blind randomized clinical trial to assess hemodynamic changes. Anesth Analg. 2012;115(6):1343–1350. doi:10.1213/ANE.0b013e31826ac3db
6. Ngan Kee WD, Lee SW, Ng FF, Tan PE, Khaw KS. Randomized double-blinded comparison of norepinephrine and phenylephrine for maintenance of blood pressure during spinal anaesthesia for caesarean delivery. Anesthesiology. 2015;122(4):736–745. doi:10.1097/ALN.0000000000000601
7. Chen Y, Zou L, Li Z, et al. Prophylactic norepinephrine infusion for postspinal anaesthesia hypotension in patients undergoing caesarean section: a randomized, controlled, dose-finding trial. Pharmacotherapy. 2021;41(4):370–378.
8. Sharkey AM, Siddiqui N, Downey K, Ye XY, Guevara J, Carvalho JCA. Comparison of intermittent intravenous boluses of phenylephrine and norepinephrine to prevent and treat spinal-induced hypotension in caesarean deliveries: randomized controlled trial. Anesth Analg. 2019;129(5):1312–1318. doi:10.1213/ANE.0000000000003704
9. Ngan Kee WD, Lau TK, Khaw KS, Lee BB. Comparison of metaraminol and ephedrine infusions for maintaining arterial pressure during spinal anaesthesia for elective caesarean section. Anesthesiology. 2001;95(2):307–313. doi:10.1097/00000542-200108000-00009
10. Ngan Kee WD, Khaw KS, Lee BB, Wong MM, Ng FF. Metaraminol infusion for maintenance of arterial blood pressure during spinal anaesthesia for caesarean delivery: the effect of a crystalloid bolus. Anesth Analg. 2001;93(3):703–708. doi:10.1097/00000539-200109000-00033
11. Yuen MK, Key LK. Prophylactic i.v. metaraminol during spinal anaesthesia for elective Caesarean delivery. Can J Anaesth. 2003;50(8):858–859. doi:10.1007/BF03019392
12. McDonnell NJ, Paech MJ, Muchatuta NA, Hillyard S, Nathan EA. A randomised double-blind trial of phenylephrine and metaraminol infusions for prevention of hypotension during spinal and combined spinal-epidural anaesthesia for elective caesarean section. Anaesthesia. 2017;72(5):609–617. doi:10.1111/anae.13836
13. Knutzen L, Svirko E, Impey L. The significance of base deficit in acidemic term neonates. Am J Obstet Gynecol. 2015;213(3):373 e1–7. doi:10.1016/j.ajog.2015.03.051
14. Xu T, Zheng J, An XH, Xu ZF, Wang F. Norepinephrine intravenous prophylactic bolus versus rescue bolus to prevent and treat maternal hypotension after combined spinal and epidural anaesthesia during caesarean delivery: a sequential dose-finding study. Ann Transl Med. 2019;7(18):451. doi:10.21037/atm.2019.08.50
15. Vallejo MC, Attaallah AF, Elzamzamy OM, et al. An open-label randomized controlled clinical trial for comparison of continuous phenylephrine versus norepinephrine infusion in prevention of spinal hypotension during caesarean delivery. Int J Obstet Anesth. 2017;29:18–25. doi:10.1016/j.ijoa.2016.08.005
16. Wang X, Mao M, Zhang SS, Wang ZH, Xu SQ, Shen XF. Bolus norepinephrine and phenylephrine for maternal hypotension during elective caesarean section with spinal anaesthesia: a randomized, double-blinded study. Chin Med J. 2020;133(5):509–516. doi:10.1097/CM9.0000000000000621
17. Theodoraki K, Hadzilia S, Valsamidis D, Stamatakis E. Prevention of hypotension during elective caesarean section with a fixed-rate norepinephrine infusion versus a fixed-rate phenylephrine infusion. Alpha double-blinded randomized controlled trial. Int J Surg. 2020;84:41–49. doi:10.1016/j.ijsu.2020.10.006
18. Ngan Kee WD, Lee SWY, Ng FF, Lee A. Norepinephrine or phenylephrine during spinal anaesthesia for Caesarean delivery: a randomised double-blind pragmatic non-inferiority study of neonatal outcome. Br J Anaesth. 2020;125(4):588–595. doi:10.1016/j.bja.2020.05.057
19. Ngan Kee WD. A random-allocation graded dose-response study of norepinephrine and phenylephrine for treating hypotension during spinal anaesthesia for caesarean delivery. Anesthesiology. 2017;127(6):934–941. doi:10.1097/ALN.0000000000001880
20. Mohta M, Dubey M, Malhotra RK, Tyagi A. Comparison of the potency of phenylephrine and norepinephrine bolus doses used to treat post-spinal hypotension during elective caesarean section. Int J Obstet Anesth. 2019;38:25–31. doi:10.1016/j.ijoa.2018.12.002
21. Bhardwaj N, Jain K, Arora S, Bharti N. A comparison of three vasopressors for tight control of maternal blood pressure during caesarean section under spinal anaesthesia: effect on maternal and fetal outcome. J Anaesthesiol Clin Pharmacol. 2013;29(1):26–31. doi:10.4103/0970-9185.105789
22. Aragao FF, Aragao PW, Martins CA, Salgado Filho N, Barroqueiro Ede S. [Comparison of metaraminol, phenylephrine and ephedrine in prophylaxis and treatment of hypotension in caesarean section under spinal anaesthesia]. Rev Bras Anestesiol. 2014;64(5):299–306. Portuguese. doi:10.1016/j.bjan.2013.07.014
23. Stewart A, Fernando R, McDonald S, Hignett R, Jones T, Columb M. The dose-dependent effects of phenylephrine for elective caesarean delivery under spinal anaesthesia. Anesth Analg. 2010;111:1230–1237.
24. Allen TK, George RB, White WD, Muir HA, Habib AS. A double-blind, placebo-controlled trial of four fixed rate infusion regimens of phenylephrine for hemodynamic support during spinal anaesthesia for caesarean delivery. Anesth Analg. 2010;111(5):1221–1229. doi:10.1213/ANE.0b013e3181e1db21
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.