")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Comparison of Coronary Heart Disease and Stroke in Association with Diabetic Retinopathy in Adults with Diabetes Using a National Survey
Received 21 November 2020
Accepted for publication 8 December 2020
Published 23 December 2020 Volume 2020:13 Pages 5079—5084
DOI https://doi.org/10.2147/DMSO.S292934
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Guang-Ran Yang,1 Dongmei Li,2 Lin Li3
1Department of Endocrinology, Beijing Tongren Hospital, Capital Medical University, Beijing 100730, People’s Republic of China; 2Clinical and Translational Science Institute, School of Medicine and Dentistry, University of Rochester Medical Center, Rochester, NY 14620, USA; 3Beijing Tongren Eye Center, Beijing Tongren Hospital, Beijing Ophthalmology and Visual Sciences Key Laboratory, Capital Medical University, Beijing 100730, People’s Republic of China
Correspondence: Guang-Ran Yang Email [email protected]
Objective: Diabetic retinopathy (DR) was reported to have higher prevalence of coronary heart disease (CHD) and stroke compared with people without DR. However, whether DR had similar effects on CHD and stroke in US adults with diabetes was not well known. This study was to compare the association between DR, CHD and stroke in US adults with diabetes using the 2015 Behavioral Risk Factor Surveillance System (BRFSS).
Methods: Respondents with diabetes aged over 18 years and undergone a fundus examination over the past 2 years were included in this study. DR, CHD and stroke were self-reported. A weighted hierarchical logistic regression was used to examine the association of DR with CHD and stroke.
Results: A total of 21,049 respondents with diabetes aged over 18 years having undergone a fundus examination over the past 2 years were included in the analysis. There were 4690 people reported having CHD, accounting for the weighted prevalence 22.1%. The weighted prevalence of stroke was 9.6%. There was 28.3% of CHD people who had DR which was higher than that in people without CHD. Differences in weighted frequency distributions of gender, age category (over 45 years or not), current smoking, hypercholesterolemia, hypertension and insulin treatment were significantly different between the CHD and without CHD groups (p< 0.001). Similar results were found in people with stroke. Logistic analysis showed that DR was related to CHD and stroke (crude OR =1.876, 2.263, respectively, p all < 0.001). After adjusting other variables, these associations persisted (Adjusted OR=1.632 (95% CI=1.625– 1.639), 1.846 (95% CI=1.836– 1.856), respectively, p all< 0.001).
Conclusion: The BRFSS 2015 data indicated that DR was not only associated with CHD but also associated with stroke in US adults with diabetes, independently of other risk factor. DR might be more strongly associated with stroke than with CHD.
Keywords: diabetes, diabetic retinopathy, coronary heart disease, stroke, risk factor
Introduction
According to the statistical reports of the American Heart Association in 2019 (based on the data of NHANES from 2013 to 2016), the prevalence of cardiovascular diseases (including coronary heart disease (CHD), heart failure, and stroke) in American adults older than 20 years of age is 9.0%.1 Cardiovascular diseases are the leading cause of death in adults. Diabetes mellitus (DM) is an important risk factor for cardiovascular diseases. Patients with DM are not only susceptible to cardiovascular diseases but also have microvascular complications unique to DM.
Diabetic retinopathy (DR) is one of the important diabetic microvascular complications. It was reported that about 4.1 million US adults aged over 40 years had DR.2 The mechanisms of DR are related with hyperglycemia, oxidative stress, hypertension, dyslipidemia, inflammation, etc.3 There are common mechanisms in DR and cardiovascular diseases, for example, hyperglycemia, hypertension, dyslipidemia and inflammation are all related with DR and cardiovascular diseases.4,5
Previous studies found that proliferative DR was related to the severity of calcification of the coronary artery.6 DR was also found to be related to an increased CHD event incidence in type 2 diabetes in a cohort study.7 There were several studies showing that DR was associated with stroke risk in US people with diabetes.8–10 However, whether DR had similar effects on the CHD and stroke in US adults with diabetes was not well known. There was a lack of studies to compare the effects of DR on CHD and stroke. The Behavioral Risk Factor Surveillance System database (BRFSS) was a large-scale investigation. The aim of this study was to analyze the 2015 BRFSS from adults with diabetes who had undergone a fundus examination in which the pupils were dilated over the past 2 years to ensure the reliability of self-reported DR diagnosis and to compare the association between DR, CHD and stroke in US adults with diabetes.
Methods
BRFSS is a US national telephone survey, which is a health-related survey collecting health-related risk behaviours, chronic diseases and use of preventive services of US residents. BRFSS is conducted every year, and it is the largest health survey in the world. Data was collected by both landline and cellular telephone interviews.11 Questions used in this study in the 2015 BRFSS survey include age, race, ethnicity, education, overweight, smoking and chronic disease history.
The 2015 BRFSS data were de-identified data and available to the public. The data were available from the US Centers for Disease Control and Prevention website.
Age (<45 year or ≥45 year), race (White only, Black only, American Indian or Alaskan Native only, Asian only, Native Hawaiian or other Pacific Islander only, other race only, multiracial), ethnicity (Hispanic, Latino/a, or Spanish origin or no), education (did not graduate high school, graduated high school, attended college or technical school, graduated from college or technical school), overweight (body mass index (BMI)<25kg/m2 or BMI ≥25kg/m2), and current smoking were categorized according to the original variables in the questionnaire.
Chronic diseases were all self-reported. CHD was defined if the respondent answered yes to the question “has a doctor, nurse, or other health professional ever told you had angina or coronary heart disease?” or if the respondent answered yes to the question “ever told you had a heart attack, also called a myocardial infarction?” Stroke was defined if the respondent answered yes to the question “has a doctor, nurse, or other health professional ever told you had a stroke”. Diabetes was defined if the respondent answered yes to the question “ever told you have diabetes”. DR was defined if the respondent’s answer was yes to the question “has a doctor ever told you that diabetes has affected your eyes or that you had retinopathy”.
In the 2015 BRFSS survey, the response rate from cellular telephone and landline telephone is 46.4% and 47.7%, respectively.12 Unknown responses or non-responses were coded as missing in questions included in the study, and there were 21,049 subjects with diabetes who had undergone a fundus examination in which the pupils were dilated over the past 2 years included in the analysis after removing missing values.
Statistical Analysis
The records in the 2015 BRFSS survey data was weighted using raking weighting methodology.13 Each respondent was assigned final weight. SPSS 25.0 was used to analyse the BFRSS data. The weighted percentages were calculated. Categorical data between groups was analyzed using weighted Chi-square test. Weighted logistic regression analysis was utilized to analyse the association between DR, CHD and stroke. Odds ratios (OR) and corresponding 95% confidence intervals (CIs) were calculated. The significance level was set at p< 0.05, and all tests were two-sided.
Results
Clinical Characteristics in CHD Respondents
There were 21,049 respondents reporting having diabetes and having undergone a fundus examination over the past 2 years. There were 4690 people who reported having CHD, accounting for the weighted prevalence 22.1%. Among these respondents with diabetes, 3990 respondents reported having DR. The weighted prevalence of DR was 19.8%.
Compared with women, the weighted prevalence of men was higher (38.3% vs 61.7%, p<0.001) in CHD respondents. In the CHD group, 97.5% of respondents were aged over 45 years. Differences in the weighted percentages of smoking, education attainment, race, and ethnicity were statistically significant between the non-CHD and the CHD groups (p<0.001). More respondents were current smokers in the CHD group (14.8%) compared with that in the non-CHD group (12.8%, p<0.001). There was 21.6% of respondents in the CHD group who did not graduate high school, which was higher than the non-CHD group. More people were white in the CHD group (78.7%) compared with that in the non-CHD group (71.7%). However, less respondents were Latino in the CHD group (5.6%) than in the non-CHD group (7.9%, p<0.001, Table 1).
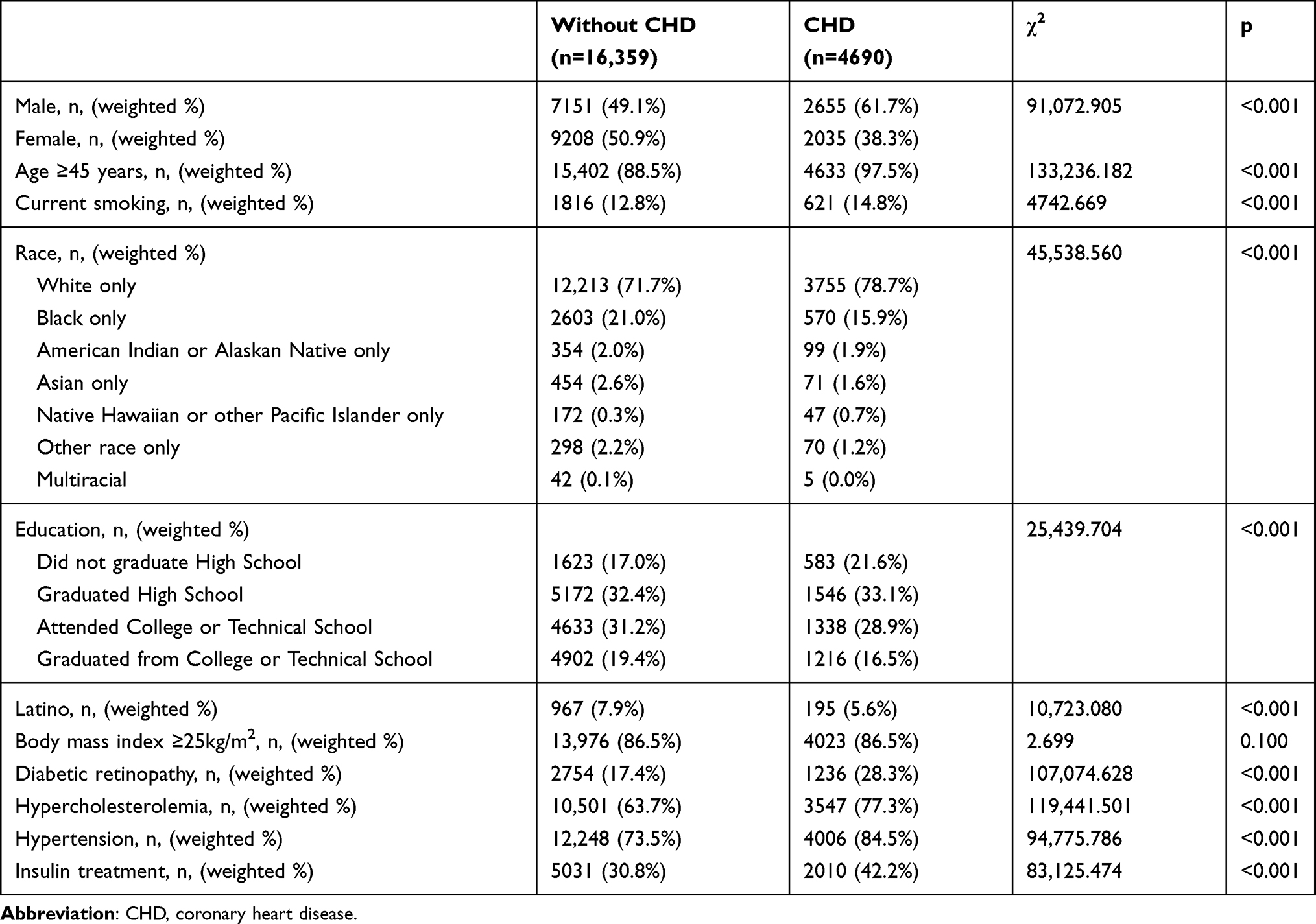 |
Table 1 Clinical Characteristics Between the Coronary Heart Disease Group and the Non-Coronary Heart Disease Group |
The weighted prevalence of hypercholesterolemia was higher in the CHD group than in the non-CHD group (77.3% vs 63.7%, p<0.001). Moreover, 84.5% of respondents in the CHD group had hypertension and the weighted percentage is much higher than that in the non-CHD group (73.5%, p<0.001). There was more respondents in the CHD group having DR (28.3%) compared with respondents without CHD (17.4%, p<0.001). However, there was no significant difference in the weighted prevalence of overweight (BMI ≥25kg/m2) between the CHD group and the group without CHD (p>0.05, Table 1).
Clinical Characteristics in Stroke Respondents
Among the 21,049 respondents with diabetes, 2055 people reported having stroke and the weighted prevalence of stroke was 9.6%. In the stroke group, the weighted prevalence of men was higher compared with women (52.4% vs 47.6%, p<0.001). There were 96.3% of respondents aged over 45 years in the stroke group. Differences in the weighted percentages of smoking, education attainment, race, and ethnicity were statistically significant between the without and with stroke groups (p<0.001). More respondents were current smokers in the stroke group (17.9%) compared with that in the group without stroke (12.8%, p<0.001). There was 26.7% of respondents in the stroke group who did not graduate high school, which was higher than in the group without stroke. However, less respondents were Latino in the stroke group (6.8%) than that in the non-stroke group (7.4%, p<0.001, Table 2).
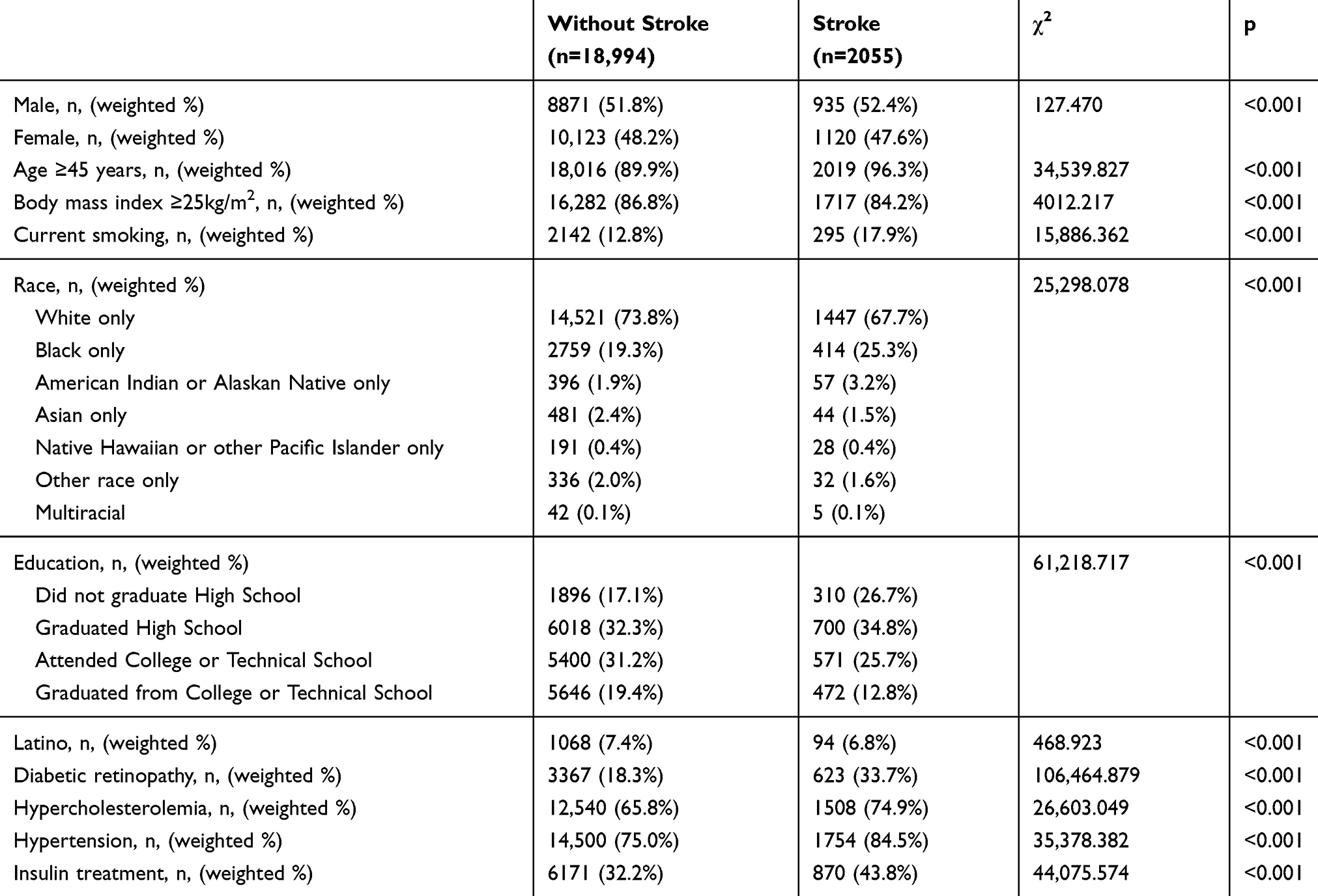 |
Table 2 Clinical Characteristics Between the Without and with Stroke Group |
The weighted prevalence of hypercholesterolemia and hypertension were higher than those in the group without stroke (74.9% vs 65.8%, 84.5% vs 75.0%, p all <0.001). Moreover, 43.8% of respondents in the stroke group took insulin treatment (p<0.001). More respondents in the stroke group had DR (33.7%) compared with respondents without stroke (18.3%, p<0.001). However, people whose BMI was below 25kg/m2 had higher weighted prevalence of stoke compared to those whose BMI was above 25kg/m2 (p<0.001, Table 2).
Logistic Analysis
Logistic analysis showed that DR was related to CHD (crude OR =1.876, 95% CI=1.869–1.883, p<0.001). After adjusting age ≥45 years, race, low education, insulin treatment, current smoking, gender, overweight, hypercholesterolemia, Latino and hypertension variables, this association persisted (Adjusted OR=1.632, 95% CI=1.625–1.639, p<0.001). Age ≥45 years, race, low education, insulin treatment, current smoking, overweight, hypercholesterolemia, male, Latino and hypertension were also associated with CHD (p<0.001).
When stroke was the dependent variable, logistic analysis showed that DR was related to stroke (crude OR =2.263, 95% CI=2.251-2.274, p<0.001). After adjusting age ≥45 years, race, low education, insulin treatment, current smoking, gender, overweight, hypercholesterolemia, Latino and hypertension variables, this association persisted (Adjusted OR=1.846, 95% CI=1.836–1.856, p<0.001). Age ≥45 years, race, low education, insulin treatment, current smoking, overweight, hypercholesterolemia, male, Latino and hypertension were also associated with stroke (p<0.001).
Discussion
The analysis of BRFSS 2015 data indicated that 19.8% of respondents with diabetes self-reported having DR. Moreover, 22.1% of respondents reported having CHD and 9.6% of respondents reported having stroke. Respondents with CHD or stroke had a higher prevalence of DR. Besides, DR was associated with CHD in adult DM respondents and those with stroke. Our data also suggested that DR may increase the risk of CHD by about 60% and the risk of stroke by 85% in adult DM respondents.
DR is one of the main microvascular complications in DM patients. Different studies on the prevalence of DR have reported different results. In this study, the weighted prevalence of DR was 19.8%, which was similar to the results of DM patients in the American Indians and Alaskan Natives and Cardiovascular Health Study,14,15 but higher than that in a study on US people over 40 years old,16,17 which was consistent with reports of other countries18 and may be related to the difference of the selected population.
CHD and stroke are crucial macrovascular complications in DM patients and the main causes of death in type 2 DM patients.19 DR, CHD and stroke have common risk factors, such as hyperglycemia, hyperlipidemia, and hypertension.20–22 In clinical practice, DM patients tend to present with DR and macrovascular complications at the same time.
There have been some reports on DR and CHD in patients with diabetes. In the US atherosclerosis risk in communities (ARIC) study that enrolled 1524 middle-aged type 2 DM patients without CHD or stroke, after an average follow-up of 7.8 years, it was found that DR was associated with an increased risk of CHD events and was independent of known risk factors.7 Additionally, cohort studies on adult Asian populations found that DR increased the risk of all-cause and cardiovascular death in DM patients.23 Moreover, a meta-analysis involving eight prospective studies revealed that vision-threatening DR increased the risk of fatal CHD events.24 There were several studies reporting the association between DR and stroke in US diabetes. In a population-based cohort study conducted in Wisconsin, DR was related to stroke mortality in elder-onset DM people.8 In a nested case-control study enrolled 2124 persons with diabetes in California, DR was found to be an independent risk factor for nonembolic stroke.9 In another population-based cohort study of 1617 US middle-aged people with diabetes, it was shown that DR predicted the incidence of ischemic stroke in people with diabetes.10 However, there was lack of studies to compare the effects of DR on CHD and stroke in US diabetes population.
In this analysis of BRFSS database, the associations between DR, CHD and stroke in US adult respondents with diabetes was compared. We found that 28.3% of CHD people had DR and 33.7% of stroke people had DR, which was higher than that in people without CHD or stroke, respectively. In addition, this study also found that DR was not only associated with CHD but also with stroke. We found that education, gender, BMI, and smoking were all associated with DR. Still, CHD and stroke were associated with DR after adjusting for these factors, suggesting that DR was associated with CHD and stroke. Moreover, when comparing the association between DR, CHD and stroke, DR was found to be more strongly associated with stroke than with CHD in diabetes respondents. DR might increase the risk of stroke in US adults with diabetes by 85%.
This study has a few limitations. Firstly, this is an investigative study. All data were self-reported by respondents, which may result in underestimation of the prevalence of chronic diseases compared with clinical studies based on laboratory tests. Secondly, although the risk factors of CHD and stroke, such as age and overweight, were included in the study, laboratory test results of other risk factors, such as glycosylated hemoglobin, were missing.18 Thirdly, the DM type of the respondents in the study was not clear, and type 1 or type 2 DM could not be determined. DM and DR were self-reported, without specific fundus examination results. However, in order to improve the accuracy of the DR self-report, only patients who had undergone a fundus examination in which the pupils were dilated over the past two years were included in this study for analysis. Therefore, the diagnosis of DR was reliable. Besides, fatal CHD and stroke patients were not included in this study, so the prevalence of CHD and stroke in adult DM patients reported in this study may be lower than the actual prevalence.
Cross-sectional analysis of BRFSS showed that 22.1% of diabetes respondents had CHD and 9.6% of diabetes respondents had stroke. After adjusting for age, overweight, smoking, and other factors, DR was still associated with CHD and stroke. Moreover, DR might be more strongly associated with stroke than with CHD.
Funding
This research was funded by Beijing Municipal Training Foundation for Highly-qualified and Technological Talents of Health System [2014-3-013] and Capital’s Funds for Health Improvement and Research [2016-2-2054, 2020-1-1181].
Disclosure
The authors report no conflicts of interest for this work.
References
1. Benjamin EJ, Muntner P, Alonso A, et al. Heart disease and stroke statistics-2019 update: a report from the american heart association. Circulation. 2019;139(10):e56–e528.
2. Kempen JH, O’Colmain BJ, Leske MC, et al. Eye Diseases Prevalence Research G: the prevalence of diabetic retinopathy among adults in the United States. Arch Ophthalmol. 2004;122(4):552–563.
3. Kohner EM. Microvascular disease: what does the UKPDS tell us about diabetic retinopathy? Diabet Med. 2008;25(Suppl 2):20–24. doi:10.1111/j.1464-5491.2008.02505.x
4. Luscher TF, Creager MA, Beckman JA, Cosentino F. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part II. Circulation. 2003;108(13):1655–1661. doi:10.1161/01.CIR.0000089189.70578.E2
5. Duh EJ, Sun JK, Stitt AW. Diabetic retinopathy: current understanding, mechanisms, and treatment strategies. JCI Insight. 2017;2:14. doi:10.1172/jci.insight.93751
6. Reaven PD, Emanuele N, Moritz T, et al. Veterans Affairs Diabetes T: proliferative diabetic retinopathy in type 2 diabetes is related to coronary artery calcium in the Veterans Affairs Diabetes Trial (VADT). Diabetes Care. 2008;31(5):952–957. doi:10.2337/dc07-1926
7. Cheung N, Wang JJ, Klein R, Couper DJ, Sharrett AR, Wong TY. Diabetic retinopathy and the risk of coronary heart disease: the Atherosclerosis Risk in Communities Study. Diabetes Care. 2007;30(7):1742–1746. doi:10.2337/dc07-0264
8. Klein R, Klein BE, Moss SE, Cruickshanks KJ. Association of ocular disease and mortality in a diabetic population. Arch Ophthalmol. 1999;117(11):1487–1495. doi:10.1001/archopht.117.11.1487
9. Petitti DB, Bhatt H. Retinopathy as a risk factor for nonembolic stroke in diabetic subjects. Stroke. 1995;26(4):593–596. doi:10.1161/01.STR.26.4.593
10. Cheung N, Rogers S, Couper DJ, Klein R, Sharrett AR, Wong TY. Is diabetic retinopathy an independent risk factor for ischemic stroke? Stroke. 2007;38(2):398–401. doi:10.1161/01.STR.0000254547.91276.50
11. Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System (BRFSS). About BRFSS. Available from: https://www.cdc.gov/brfss/about/index.htm.
12. Centers for Disease Control and Prevention. Behavioral risk factor surveillance system 2015 Summary Data Quality Report with Response Rates. Available from: https://www.cdc.gov/brfss/annual_data/2015/pdf/2015-sdqrpdf.
13. Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System. Weighting BRFSS data BRFSS 2015. Available from: https://www.cdc.gov/brfss/annual_data/2015/pdf/weighting_the-data_webpage_contentpdf.
14. Bursell SE, Fonda SJ, Lewis DG, Horton MB. Prevalence of diabetic retinopathy and diabetic macular edema in a primary care-based teleophthalmology program for American Indians and Alaskan Natives. PLoS One. 2018;13(6):e0198551. doi:10.1371/journal.pone.0198551
15. Klein R, Marino EK, Kuller LH, et al. The relation of atherosclerotic cardiovascular disease to retinopathy in people with diabetes in the Cardiovascular Health Study. Br J Ophthalmol. 2002;86(1):84–90. doi:10.1136/bjo.86.1.84
16. Zhang X, Saaddine JB, Chou CF, et al. Prevalence of diabetic retinopathy in the United States, 2005-2008. JAMA. 2010;304(6):649–656. doi:10.1001/jama.2010.1111
17. Wong TY, Klein R, Islam FM, et al. Diabetic retinopathy in a multi-ethnic cohort in the United States. Am J Ophthalmol. 2006;141(3):446–455. doi:10.1016/j.ajo.2005.08.063
18. Song P, Yu J, Chan KY, Theodoratou E, Rudan I. Prevalence, risk factors and burden of diabetic retinopathy in China: a systematic review and meta-analysis. J Glob Health. 2018;8(1):010803. doi:10.7189/jogh.08.010803
19. Lyu Y, Luo Y, Li C, et al. Regional differences in the prevalence of coronary heart disease and stroke in patients with Type 2 Diabetes in China. J Clin Endocrinol Metab. 2018;103(9):3319–3330. doi:10.1210/jc.2018-00422
20. Liu L, Quang ND, Banu R, et al. Hypertension, blood pressure control and diabetic retinopathy in a large population-based study. PLoS One. 2020;15(3):e0229665. doi:10.1371/journal.pone.0229665
21. Shi R, Zhao L, Wang F, et al. Effects of lipid-lowering agents on diabetic retinopathy: a meta-analysis and systematic review. Int J Ophthalmol. 2018;11(2):287–295.
22. Wu WX, Ren M, Cheng H, et al. prevention of macrovascular disease in patients with short-duration type 2 diabetes by multifactorial target control: an 8-year prospective study. Endocrine. 2014;47(2):485–492. doi:10.1007/s12020-013-0158-x
23. Sabanayagam C, Chee ML, Banu R, et al. Association of diabetic retinopathy and diabetic kidney disease with all-cause and cardiovascular mortality in a multiethnic asian population. JAMA Netw Open. 2019;2(3):e191540. doi:10.1001/jamanetworkopen.2019.1540
24. Xie J, Ikram MK, Cotch MF, et al. Association of diabetic macular edema and proliferative diabetic retinopathy with cardiovascular disease: a systematic review and meta-analysis. JAMA Ophthalmol. 2017;135(6):586–593. doi:10.1001/jamaophthalmol.2017.0988
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.