")
Back to Journals » Medical Devices: Evidence and Research » Volume 15
Comparison of Clinical Outcomes of Gripping Surface Technology Staple Reloads versus Standard Staple Reloads Used with Manual Linear Surgical Staplers
Authors Fortin SP, Petraiuolo W, Cafri G, Scapini G, Agarwal P, Chakke D, Johnston S, Johnson BH , Coplan PM , Zhang S
Received 28 October 2022
Accepted for publication 7 December 2022
Published 15 December 2022 Volume 2022:15 Pages 385—399
DOI https://doi.org/10.2147/MDER.S393881
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Stephen P Fortin,1 William Petraiuolo,2 Guy Cafri,1 Gustavo Scapini,3 Pratyush Agarwal,4 Divya Chakke,4 Stephen Johnston,1 Barbara H Johnson,1 Paul M Coplan,1,5 Shumin Zhang1
1MedTech Epidemiology and Real-World Data Science, Office of the Chief Medical Officer, Johnson & Johnson, New Brunswick, NJ, USA; 2Medical Affairs, Ethicon, Cincinnati, OH, USA; 3Regional Medical Affairs, Johnson & Johnson, São Paulo, Brazil; 4Mu Sigma, Bengaluru, Karnataka, India; 5University of Pennsylvania Perelman School of Medicine, Philadelphia, PA, USA
Correspondence: Stephen P Fortin, MedTech Epidemiology and Real-World Data Science, Office of the Chief Medical Officer, Johnson & Johnson, 410 George St, New Brunswick, NJ, USA, Tel +1 908 927 4844, Email [email protected]
Purpose: Linear surgical staplers reduce rates of surgical adverse events (bleeding, leaks, infections) compared to manual sutures thereby reducing patient risks, surgeon workflow disruption, and healthcare costs. However, further improvements are needed. Ethicon Gripping Surface Technology (GST) reloads, tested and approved by regulatory authorities in combination with powered staplers, may reduce surgical risks through improved tissue grip. While manual staplers are used in some regions due to affordability, clinical data on GST reloads used with manual staplers are unavailable. This study compared surgical adverse event rates of manual staplers with GST vs standard reloads. These data may be used for label changes in China and Latin America.
Patients and Methods: Patients undergoing general or thoracic surgery between October 1, 2015 and August 31, 2021 using ECHELON FLEX™ manual staplers with GST or standard reloads were identified from the Premier Healthcare Database. GST reloads were compared to standard reloads for non-inferiority in bleeding and anastomotic leak for general surgery. Secondary outcomes included sepsis for general surgery, and bleeding and prolonged air leak for thoracic surgery. Covariate balancing was performed using stable balancing weights.
Results: The general and thoracic surgery cohorts contained 4571 (GST: 2780; standard: 1791) and 814 (GST: 514; standard: 300) patients, respectively. GST reloads were non-inferior to standard reloads for bleeding and anastomotic leak (adjusted cumulative incidence ratio: 1.02 [90% CI: 0.71, 1.45] and 1.03 [90% CI: 0.72, 1.46], respectively) for general surgery. Compared with standard reloads, GST reloads had a similar incidence of sepsis (2.2% vs 2.1%) for general surgery and lower incidences of bleeding (9.5% vs 16.0%) and prolonged air leak (12.6% vs 14.0%,) for thoracic surgery.
Conclusion: GST reloads, compared to standard reloads, used with ECHELON FLEX™ manual staplers had comparable perioperative bleeding and anastomotic leak for general surgery, and lower incidences of safety events for thoracic surgery.
Keywords: real-world evidence, safety, ECHELON, general surgery, thoracic surgery
Introduction
Linear surgical staplers are routinely used for applications in general and thoracic surgical procedures for tissue transection, resection, and creation of anastomoses. However, tissue movement or slippage in response to the applied pressure during the actuation of linear surgical staplers may compromise the integrity of the staple line and necessitate intervention. As such, tissue movement and slippage may be associated with increased surgical complications and untoward clinical outcomes, including surgical bleeding, leaks, and infection, associated with significant healthcare costs.1
ECHELON FLEX™ manual staplers possess enhanced system-wide compression, which gently exudes fluid from the targeted tissue during device actuation leading to reliable performance across a diverse set of tissue types and thicknesses. In 2014, Ethicon launched the ECHELON FLEX™ GST system, a powered stapler system incorporating staple reloads with gripping surface technology (GST). Featuring proprietary pocket extensions, GST reloads hold tissue in place and guide staple legs towards anvil pockets during firing thereby promoting the creation of uniform, secure staple lines. Delivering four times less tissue slippage during firing compared to other powered staplers, the GST system allows for more targeted tissue transection potentially eliminating one staple reload per procedure thereby providing enhanced economic value.2
Prior literature has associated the GST system with a reduction in intraoperative staple line interventions, including endoclip placement, oversewing, or targeted cautery, as compared with Ethicon’s powered staplers using standard reloads among patients undergoing laparoscopic sleeve gastrectomy (LSG).3 A subsequent retrospective study of patients who underwent LSG found that the GST system was associated with a lower rate of hemostasis-related complications as compared to the Medtronic’s powered Signia™ Stapling System, which uses Tri-Staple™ technology.4 Additionally, in a study of video-assisted thoracoscopic surgery (VATS) lobectomy patients in Korea, fewer hemostasis-related complications and reduced hospital costs were associated with the GST system as compared with manual staplers with standard reloads.5
Nevertheless, to our knowledge, no prior literature exists assessing clinical outcomes of GST reloads as compared to standard reloads with ECHELON FLEX™ manual staplers. As such, the purpose of this retrospective study was to compare clinical outcomes associated with the use of GST vs standard reloads among patients undergoing general or thoracic surgery using ECHELON FLEX™ manual staplers in the course of routine clinical practice.
Materials and Methods
Study Design and Data Source
We conducted a retrospective, comparative, observational study in the Premier Healthcare Database (PHD), which contains hospital administrative and billing discharge data from approximately 1164 hospitals, including 1 in 4 annual inpatient hospital stays, in the United States. The PHD includes discharge-level information on all International Classification of Diseases, Tenth Revision, Clinical Modification and Procedure Code System (ICD-10-CM and ICD-10-PCS, respectively) diagnoses and procedures recorded during each admission, and patient, hospital, and provider information. Detailed service-level information for each hospital day is recorded, including details on devices received. Although the PHD excludes federally funded hospitals (eg, Veterans Affairs), the hospitals included are nationally representative based on bed size, geographic region, location (urban/rural), and teaching hospital status.
The PHD consists of de-identified healthcare records. In the United States, retrospective analyses performed in the PHD are considered exempt from informed consent and institutional review board approval as dictated by Title 45 Code of Federal Regulations (45 CFR 46, 101(b)(4)).
Study Population
We used hospital charge master data to identify all inpatient admissions and outpatient visits occurring between October 1, 2015 and August 31, 2021, where the use of an ECHELON FLEX™ manual stapler and either a GST reload or standard reload was recorded. The study included patients aged 18 years or older with an ICD-10-PCS primary procedure code associated with general or thoracic surgery recorded between the admission and discharge date. For each patient, the index event was defined as the first inpatient admission or outpatient visit meeting these criteria.
To prevent potential confounding due to the concurrent use of alternative surgical stapling devices, we excluded patients with both a GST reload and standard reload, either an Ethicon or Medtronic powered linear stapler, or a secondary ICD-10-PCS procedure code associated with robotic surgery recorded during the index event. Furthermore, analyses were limited to patients in hospitals contributing data for at least 30 days from the index procedure date and with an elective, emergency, or urgent admission type. Finally, we required staple reload size to be inferable based on hospital charge master data for staple reloads and/or ECHELON FLEX™ manual staplers used during the index event; patients with insufficient or discordant staple reload size information were excluded.
Patient, Hospital, Provider, and Procedure Characteristics
We measured patient demographics, including age, sex, race, marital status, and payor type. Patient clinical characteristics were measured at index using the weighted Elixhauser comorbidity system, a risk-adjustment score comprised 30 comorbid conditions derived from ICD-10-CM diagnosis codes.6,7 Hospital and provider characteristics included hospital bed size, annual surgical volume for each respective procedure type, geographic location, urban vs rural setting, and teaching status. Procedural characteristics included year of surgery, surgical approach (ie, open or minimally invasive surgery), admission type, anatomical site of procedure, and staple reload size (ie, 45 mm or 60 mm). Surgical approach (ie, open surgery and minimally invasive surgery) and anatomical site of procedure were classified from ICD-10-CM diagnosis codes (see Supplemental Appendix A Table 1). Anatomical sites of procedure were categorized by procedure type as follows: colorectal, stomach, appendix, gallbladder, spleen, or other (ie, abdominal wall, hernia, liver, or pancreas) for general surgery; and lung or other (ie, heart, thymus/adrenal glands, or diaphragm) for thoracic surgery.
Study Outcomes
We examined short-term safety and utilization outcomes. The following clinical outcomes, which differed between the general and thoracic surgery cohorts, were identified using ICD-10-CM diagnosis codes (see Supplemental Appendix A Table 1): perioperative bleeding, anastomotic leak within 30 days of the index procedure and sepsis for the general surgery cohort; and perioperative bleeding and prolonged air leak for the thoracic surgery cohort. Prolonged air leak was defined as an ICD-10-CM diagnosis code associated with air leak observed during the index event and patient discharge occurring at least 7 days after the index procedure. Utilization outcomes included hospital length of stay (LOS) and operating room time (ORT).
Statistical Analyses
As complications of interest varied for the general and thoracic surgery cohorts, all analyses were stratified by procedure type. Due to limitations in sample size for the thoracic surgery cohort, primary non-inferiority analyses were performed only in the general surgery cohort. Specifically, the primary objectives evaluated the non-inferiority of GST reloads to standard reloads on both perioperative bleeding and anastomotic leak within 30 days from the index procedure.
Secondary objectives estimated the adjusted cumulative incidence ratio of the following perioperative clinical outcomes between staple reload groups: sepsis for the general surgery cohort and prolonged air leak and bleeding for the thoracic surgery cohort. Exploratory objectives estimated the difference in the average LOS and ORT between staple reload groups. Analyses for LOS and ORT were restricted to patients with an inpatient admission and a valid ORT, respectively. A valid ORT was defined as an ORT ranging between 15 minutes and 24 hours.
Stable Balancing Weights
In the absence of randomization, differences in baseline characteristics may exist between study comparison groups, which may lead to potential confounding. For instance, improvements in surgical technique over time may be associated with improved surgical outcomes. It follows that systematic bias may exist in favor of devices used more frequently in recent years relative to comparator devices thereby warranting the use of statistical methods to adjust for differences in baseline characteristics.
To address potential confounding and systematic bias due to differences in baseline characteristics between study comparison groups, we performed covariate balancing using stable balancing weights, an optimization algorithm that finds the optimal set of weights meeting a set of prespecified balance criteria.8 Specifically, the standard reload group was weighed to mimic the GST reload group on the basis of all aforementioned baseline patient, hospital, provider, and procedural characteristics. Weights were derived such that the standardized mean difference (SMD) of covariate categories between study comparison groups did not exceed 0.10, a common threshold for balance after weighting and matching procedures.9
Descriptive Analyses
Descriptive statistics were used to describe patient, hospital, provider, and procedure characteristics stratified by procedure type. SMDs, defined according to the definition of target absolute SMDs described by Chattopadhyay et al, were used to assess imbalance in characteristics prior to and after covariate balancing.10 An absolute SMD ≤0.20 was considered to denote adequate balance between study comparison groups.9 To ensure objectivity, covariate balancing and descriptive analyses were performed by an independent statistician blinded to the study outcomes.
Analyses of Outcomes
Weighted generalized linear models with log link functions and binomial distributions were used to estimate the adjusted cumulative incidence ratio of binary outcomes after covariate balancing. For all outcomes, we estimated the variance of the effect estimates based on a non-parametric bootstrap.11
For the primary objectives, the non-inferiority of GST reloads vs standard reloads was based on the adjusted cumulative incidence ratio after covariate balancing. The non-inferiority margin for the adjusted cumulative incidence ratio was set such that if the upper bound of a two-sided 90% Wald confidence interval (CI) of the adjusted cumulative incidence ratio, corresponding to a one-sided 5% significance level, was ≤2.0, then there was evidence supporting a conclusion of non-inferiority.12 The choice of 2.0 for the non-inferiority margin was based on the anticipated event percentages for the clinical outcomes of interest, which was anticipated to be low. As such, the method identified findings with very small population effects. Two-sided 95% confidence intervals were estimated for outcomes of interest without hypothesis testing for all secondary and exploratory objectives.
Results
Descriptive Analyses for General Surgery Cohort
A total of 4571 (GST reload: 2780; standard reload: 1791) patients undergoing general surgery met the study criteria. The characteristics of patients undergoing general surgery at baseline and after covariate balancing are summarized in Tables 1 and 2.
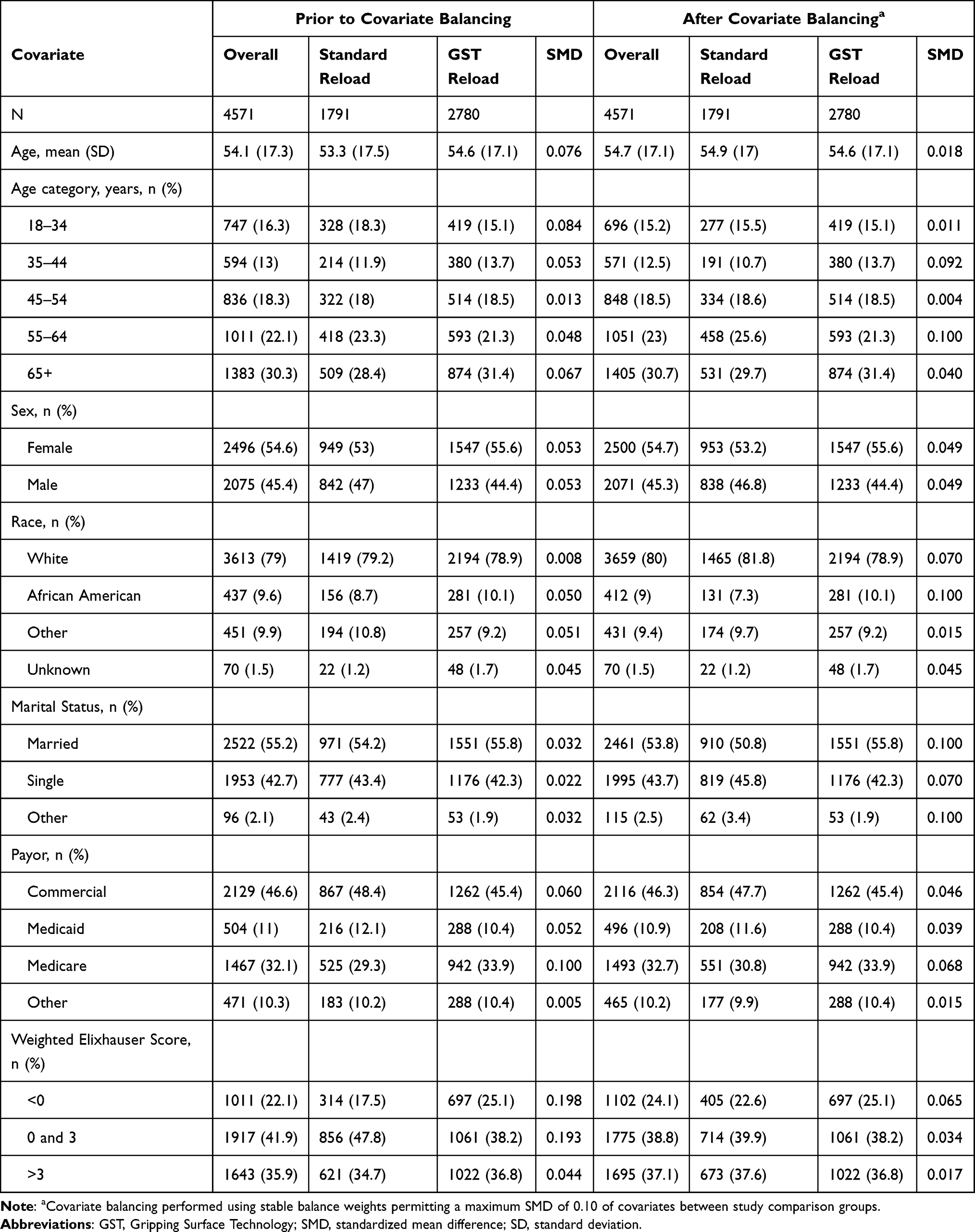 |
Table 1 Patient Characteristics of the General Surgery Cohort |
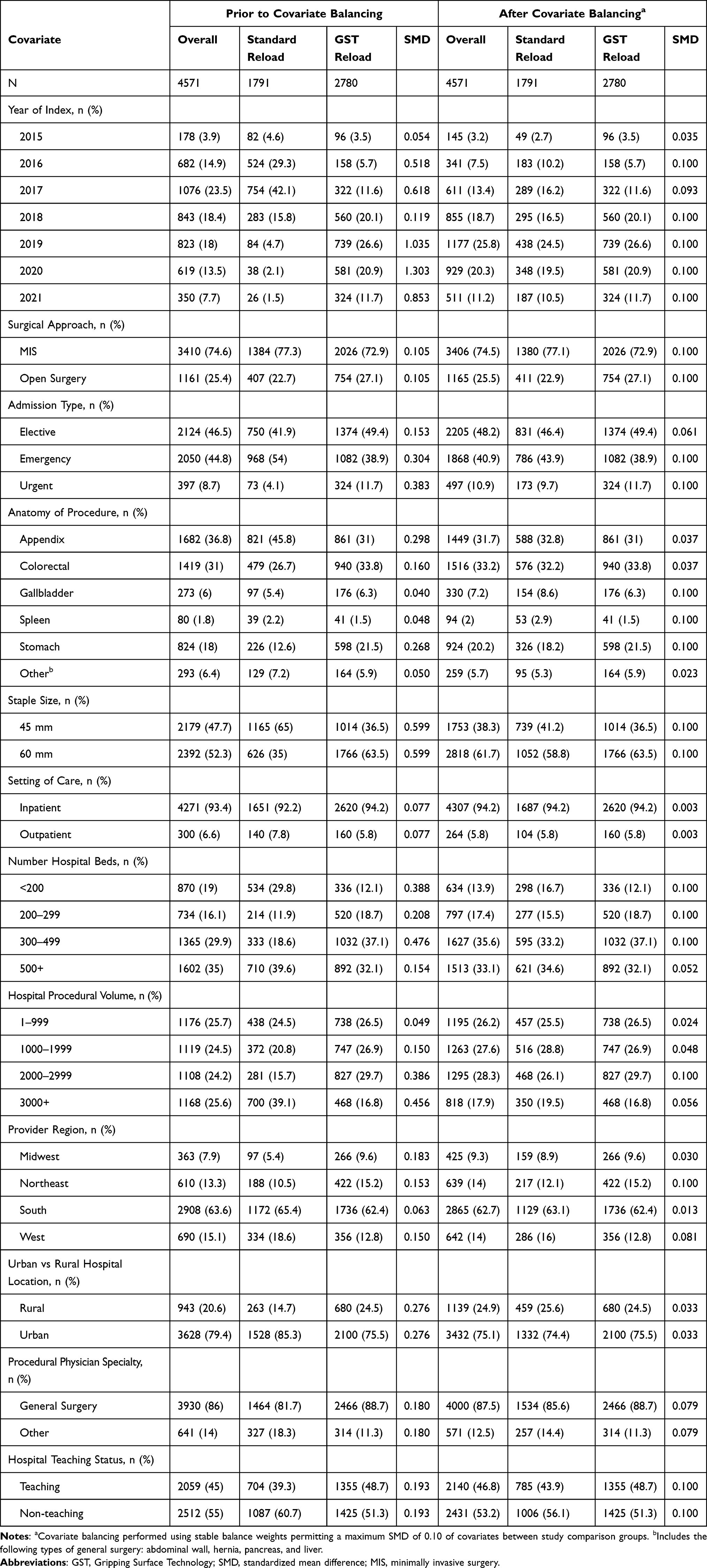 |
Table 2 Hospital, Provider, and Procedure Characteristics of the General Surgery Cohort |
Prior to covariate balancing, overall, the mean age was 54.1 (SD = 17.3) years, and approximately 54.6% of patients were female, and 79.0% were white. As evidenced by a SMD >0.20, a total of 18 covariate categories were not adequately balanced. As compared to the standard reload group, the GST reload group had a higher proportion of patients with a weighted Elixhauser score less than 0 (25.1% vs 17.5%) and a year of index between 2018 and 2021 (79.3% vs 24.1%). Overall, after covariate balancing, the mean age was 54.7 (SD = 17.1) years, and approximately 54.7% of patients were female, 80.0% were white, 24.1% had a weighted Elixhauser score less than 0, and 76.0% had a year of index between 2018 and 2021. As indicated by a SMD ≤0.20, adequate balance was achieved across all covariate categories between study comparison groups.
The characteristics of patients undergoing general surgery with an inpatient admission and valid operating room time prior to and after covariate balancing are available in Supplemental Appendix B Tables 1 and 2.
Descriptive Analyses for Thoracic Surgery Cohort
Among patients undergoing thoracic surgery meeting the study criteria, approximately 63.1% (n = 514) and 36.9% (n = 300) used GST reloads and standard reloads, respectively. Tables 3 and 4 list the characteristics of patients undergoing thoracic surgery at baseline and after covariate balancing.
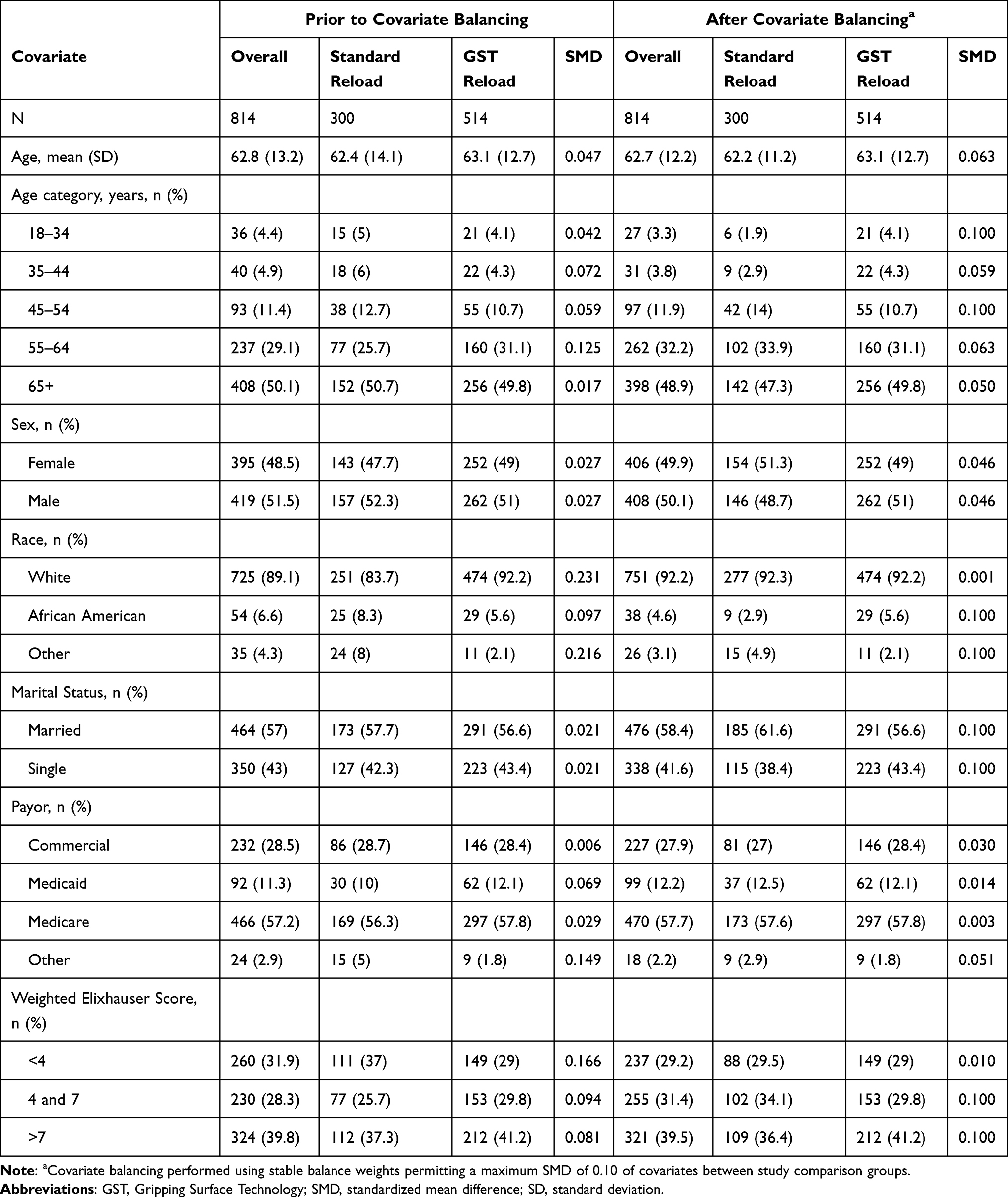 |
Table 3 Patient Characteristics of the Thoracic Surgery Cohort |
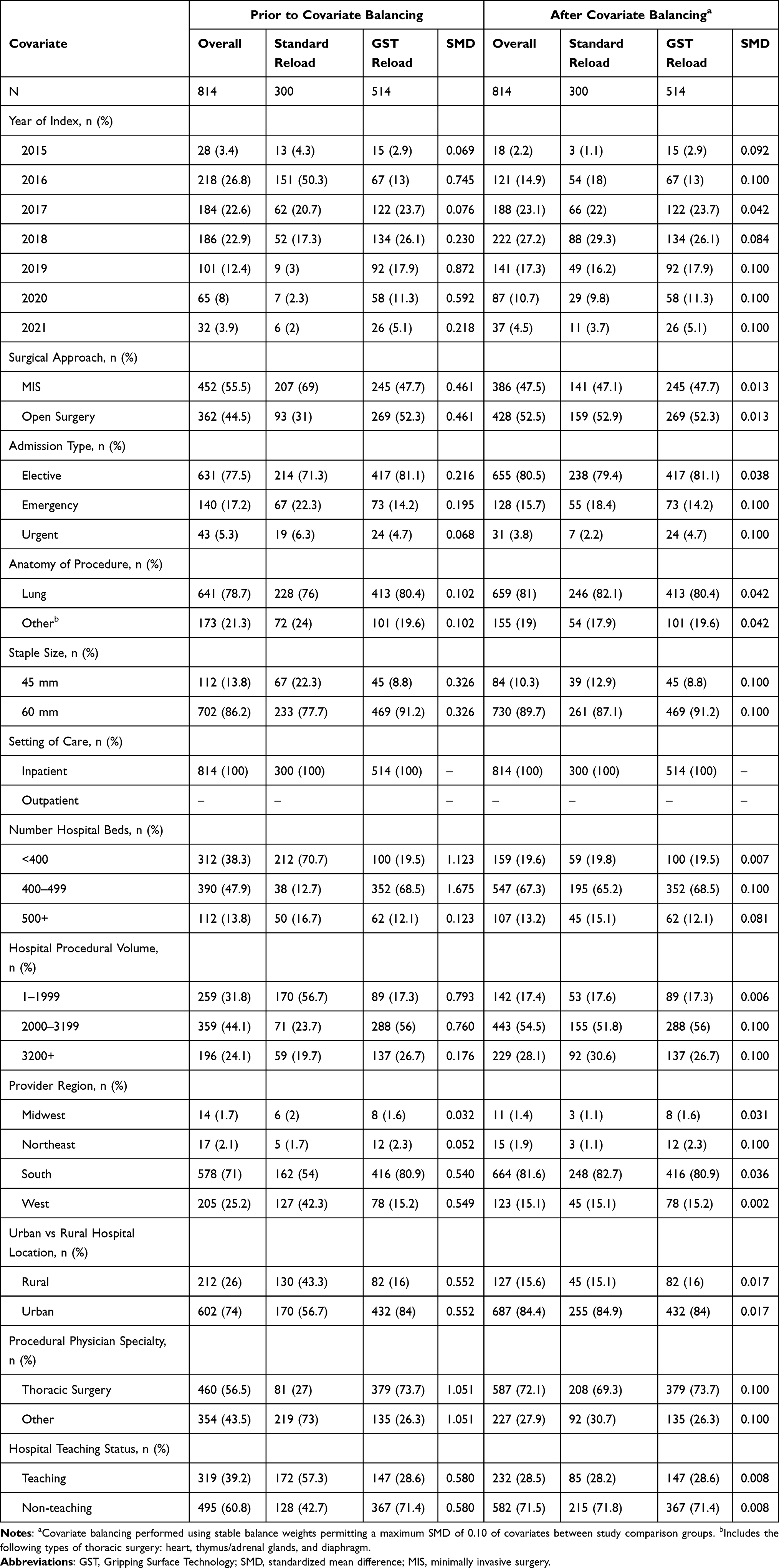 |
Table 4 Hospital, Provider, and Procedure Characteristics of the Thoracic Surgery Cohort |
At baseline, overall, the mean age was 62.8 (SD = 13.2) years, and approximately 48.5% of patients were female, 39.8% had a weighted Elixhauser score >7, and all procedures were performed on an inpatient basis. As indicated by a SMD >0.20, a total of 26 covariate categories were not adequately balanced. The GST reload group had a higher proportion of patients who were white (92.2% vs 83.7%) and had a year of index between 2018 and 2021 (60.3% vs 24.7%) as compared to the standard reload group. After covariate balancing, the overall mean age was 62.7 (SD = 12.2) years, and approximately 49.9% of patients were female, 92.2% were white, 59.7% had a year of index between 2018 and 2021, and 39.5% had a weighted Elixhauser score >7. Adequate balance was achieved across all covariate categories between study comparison groups as denoted by a SMD ≤0.20.
Supplemental Appendix C Table 1 describes the characteristics of patients undergoing thoracic surgery with a valid operating room time prior to and after covariate balancing.
Outcome Analyses for Primary Objectives
Outcome analyses for primary objectives were conducted among patients who underwent general surgery. In the covariate balanced sample, as shown in Table 5, the incidence of perioperative bleeding (GST reload: 6.4% [n = 177]; standard reload: 6.3% [n = 112]) and 30-day anastomotic leak (GST reload: 6.9% [n = 193]; standard reload: 6.8% [n = 121]) were similar. As compared to the standard reload group, the adjusted cumulative incidence ratios of perioperative bleeding and 30-day anastomotic leak in the GST reload group were 1.02 (90% CI: [0.71, 1.45]; p-value compared to the non-inferiority margin of 2.0 = 0.0009) and 1.03 (90% CI: [0.72, 1.46]; p-value compared to the non-inferiority margin of 2.0 = 0.0009), respectively. Therefore, the GST staple group was considered non-inferior to the standard staple groups on the primary study outcomes of perioperative bleeding and 30-day anastomotic leak.
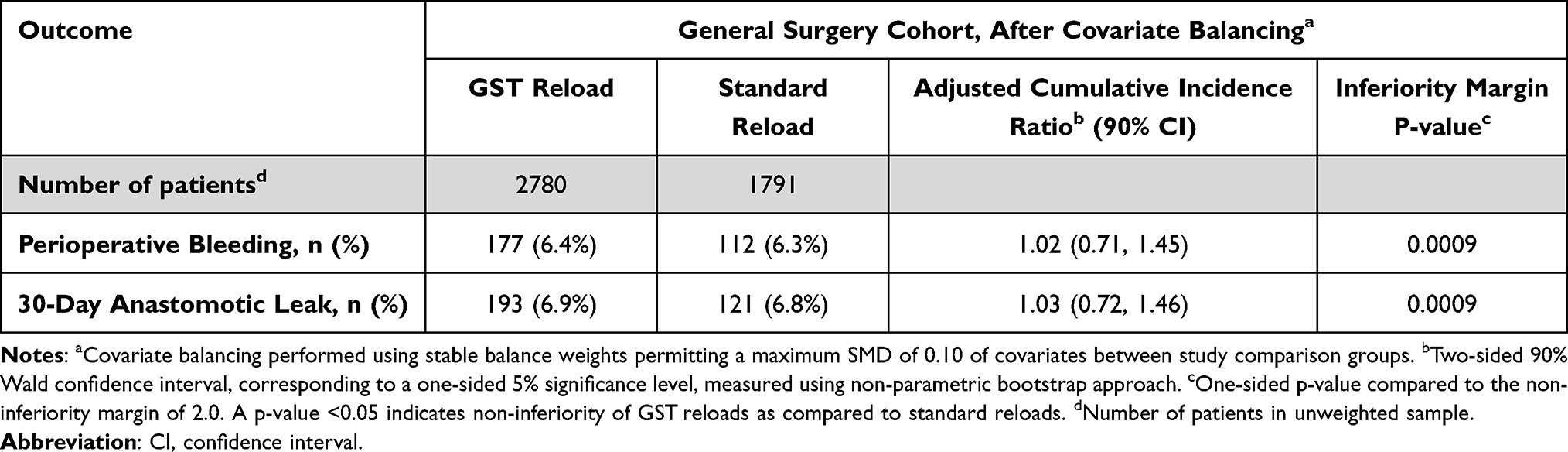 |
Table 5 Outcome Analyses for Primary Objectives in General Surgery Cohort |
Outcome Analyses for Secondary and Exploratory Objectives
The results of outcome analyses for secondary and exploratory objectives among patients who underwent general and thoracic surgery in the weighted sample are summarized in Tables 6 and 7, respectively.
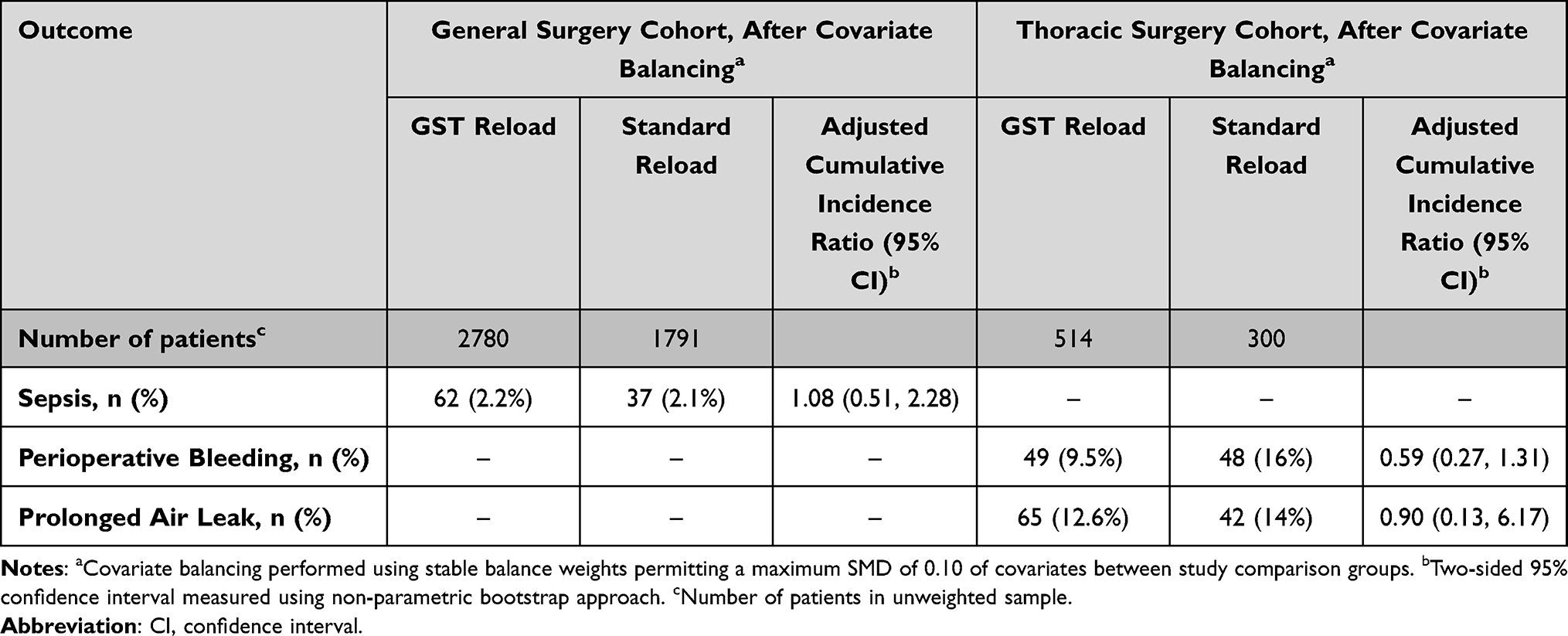 |
Table 6 Outcome Analyses for Secondary Objectives in General and Thoracic Surgery Cohorts |
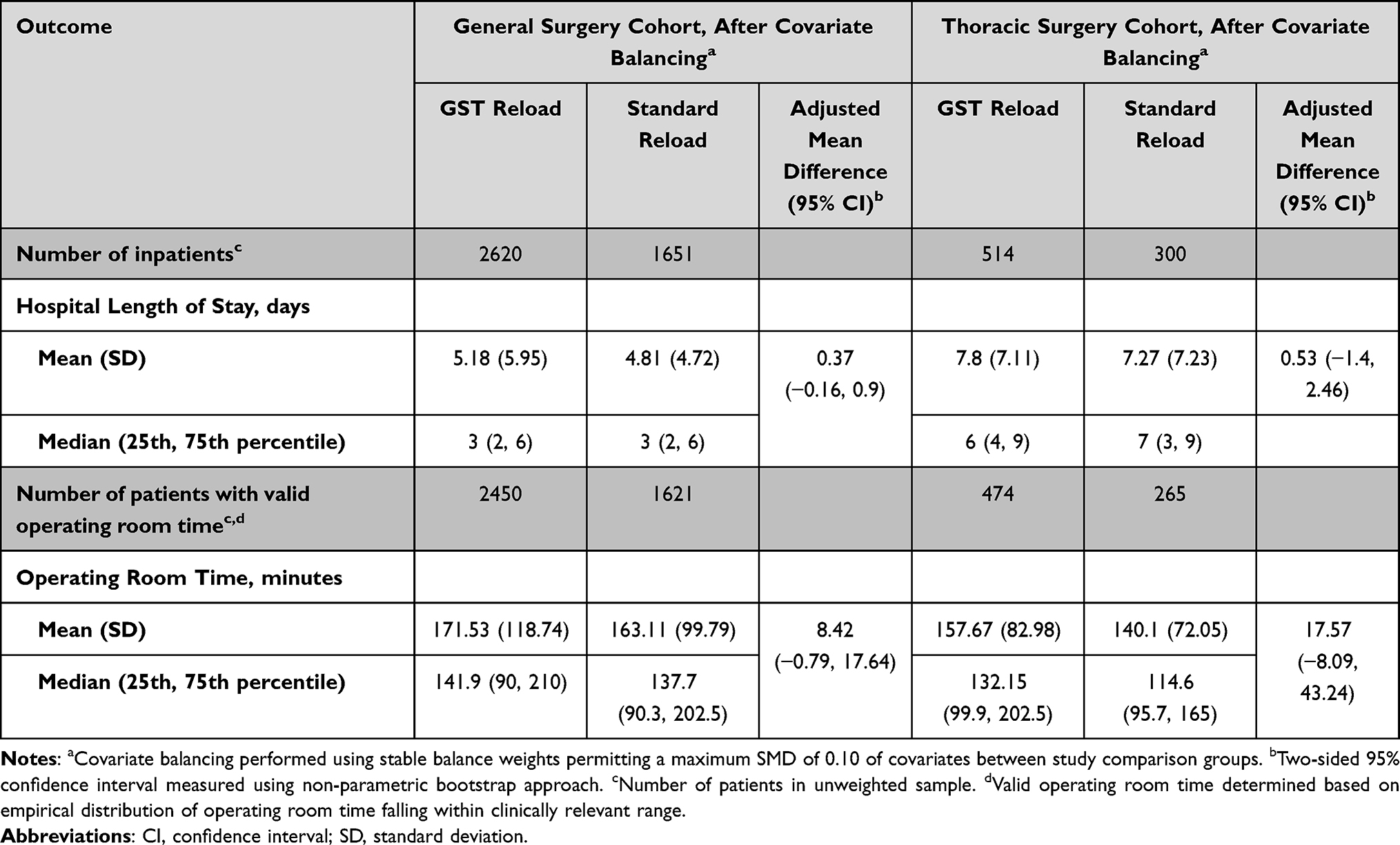 |
Table 7 Outcome Analyses for Exploratory Objectives in General and Thoracic Surgery Cohorts |
In the general surgery cohort, the adjusted cumulative incidence of sepsis was similar (2.2% [n = 62] and 2.1% [n = 37] in the GST reload and standard reload groups, respectively, corresponding to an adjusted cumulative incidence ratio of sepsis of 1.08 [95% CI: 0.51, 2.28]). Among inpatient admissions (n = 4271; 93.4%), the adjusted mean difference in LOS was 0.37 (95% CI: −0.16, 0.90) with a similar average LOS of 5.18 (SD = 5.95) in the GST reload group and 4.81 (SD = 4.72) in the standard reload group. Meanwhile, among patients with valid ORT (n = 4071; 89.1%), the adjusted mean difference in ORT was 8.42 (95% CI: −0.79, 17.64) minutes with a comparable average ORT of 171.53 (SD = 118.74) and 163.11 (SD = 99.79) minutes in the GST reload and standard reload groups, respectively.
In the thoracic surgery cohort, the incidences of perioperative bleeding and prolonged air leak in the GST reload group were lower than those in the standard reload group (9.5% vs 16.0% and 12.6% vs 14.0%, respectively, corresponding to adjusted cumulative incidence ratios of 0.59 [95% CI: 0.27, 1.31] and 0.90 [95% CI: 0.13, 6.17], respectively). All thoracic surgery patients underwent surgery on an inpatient basis, and the adjusted mean difference in LOS was 0.53 (95% CI: −1.40, 2.46) with a similar average LOS of 7.80 (SD = 7.11) in the GST reload group and 7.27 (SD = 7.23) in the standard reload group. Among patients with valid ORT (n = 739; 90.8%), the adjusted mean difference in ORT was 17.57 (95% CI: −8.09, 43.24) minutes with a comparable average ORT of 157.67 (SD = 82.98) and 140.1 (SD = 72.05) minutes in the GST reload and standard reload groups, respectively.
Discussion
This was the first study to assess clinical outcomes of GST reloads in ECHELON FLEX™ manual linear staplers. As compared to standard reloads, GST reloads had comparable risks of safety outcomes for perioperative bleeding and 30-day anastomotic leak among patients undergoing general surgery and met the prespecified non-inferiority criteria.
In a prior study, Fegelman et al found the GST system to be associated with improved clinical outcomes among patients undergoing LSG as compared to Ethicon-powered staplers with standard reloads.3 These findings highlight the benefits of the proprietary pocket extensions featured in GST reloads, which have been associated with a four-fold decrease in tissue slippage and seven-fold increase in the likelihood to fully capture mucosa at the staple line.13 Further supporting the potential benefits of GST reloads, Rawlins et al and Park et al found the GST system to be associated with fewer hemostasis-related complications and reduced hospital costs as compared to the Signia™ Stapling System among patients undergoing LSG and manual staplers with standard reloads among patients undergoing thoracoscopic lobectomy, respectively.4,5 The prior evidence, therefore, suggests GST reloads are associated with improved clinical and economic outcomes when used with Ethicon-powered staplers. Manual staplers are also commonly used in routine surgical care; however, no published data exists describing clinical and economic outcomes of GST reloads in comparison to standard reloads when used with manual staplers.
As such, the current study evaluated the safety of GST reloads among patients undergoing general or thoracic surgery using ECHELON FLEX™ manual staplers as compared to standard reloads. The relative frequencies of clinical outcomes for the primary objectives in the GST reload vs standard reload groups among patients undergoing general surgery were comparable; specifically, perioperative bleeding, 6.4% vs 6.3%, respectively; and 30-day anastomotic leak, 6.9% vs 6.8%, respectively. There was evidence that GST reloads were non-inferior and had comparable safety to standard reloads for both perioperative bleeding and 30-day anastomotic leak based on a non-inferiority margin of the adjusted cumulative incidence ratio of 2.0 (p values compared to the non-inferiority margin of 2.0: 0.0009) among patients undergoing general surgery using ECHELON FLEX™ manual staplers. These findings demonstrate the backward compatibility of GST reloads in ECHELON FLEX™ manual staplers for general surgery.
Among patients undergoing thoracic surgery using ECHELON FLEX™ manual staplers, GST reloads were associated with lower relative frequencies of perioperative bleeding (9.5% vs 16.0%) and prolonged air leak (12.6% vs 14.0%) as compared to standard reloads. These findings suggest that GST reloads may be backward compatible in ECHELON FLEX™ manual staplers across various procedure types. Indeed, it may be reasonable to assume that the backward compatibility of GST reloads, which possess more advanced stapling technology, in ECHELON FLEX™ manual staplers may be applicable to surgeries of various tissue types and anatomical sites. However, the non-inferiority of clinical outcomes was not assessed among patients undergoing thoracic surgery due to sample size limitations.
GST reloads and standard reloads were also comparable in terms of healthcare utilization outcomes among patients undergoing general or thoracic surgery using ECHELON FLEX™ manual staplers. For instance, the average hospital length of stay was similar between the GST reload and standard reload groups for both the general surgery (5.18 vs 4.81 days; difference = 0.37 [95% CI: −0.16, 0.9]) and thoracic surgery (7.80 vs 7.27 days; difference = 0.53 [95% CI: −1.40, 2.46]) cohorts. Likewise, operating room time was comparable between study comparison groups in the general surgery (GST: 171.53; standard: 163.11 minutes; difference = 8.42 [95% CI: −0.79, 17.64]) and thoracic surgery (GST: 157.67; standard: 140.10 minutes; difference = 17.57 [95% CI: −8.09, 43.24]) cohorts.
These findings further reinforce the backward compatibility of GST reloads in ECHELON FLEX™ manual staplers. Although the current study assessed the non-inferiority of GST reloads as compared to standard reloads by design, the advantages of GST reloads are well documented in prior literature. Notably, Fegelman et al found a decrease in intraoperative staple line interventions associated with the use of a powered stapler system with GST reloads as compared to standard reloads.3 Given manual staplers are commonly used in surgical care, especially in locations with less access to powered staplers, the demonstration of the backward compatibility of GST reloads in ECHELON FLEX™ manual staplers is of great significance in supporting the use of the newer staple reload technology to improve surgical care. Nevertheless, opportunity exists to further improve surgical outcomes through technological innovation in regions with less access to powered staplers.
Strengths and Limitations
This study has several strengths. First, analyses of primary outcomes were performed in a large, nationally representative sample of 4571 patients undergoing general surgery using ECHELON FLEX™ manual staplers. Second, the study used appropriate statistical methods including covariate balancing using stable balancing weights to adjust for potential confounders. In addition, the objectivity of study findings was further strengthened by separating the processes of covariate balancing, which was conducted by a first statistician blinded to study outcomes, with subsequent outcome analyses and non-inferiority hypothesis testing by a second statistician.
The current study was subject to limitations. First, the identification of ECHELON FLEX™ manual staplers, GST reloads, and standard reloads was based upon hospital charge master data, which may be subject to misclassification. To overcome this limitation, device search strategies were tailored to be highly specific to the devices of interest. Furthermore, we excluded patients with evidence of powered linear stapler use or robotic surgery during the index event. Second, as with any observational study, there is a possibility of residual confounding due to unobserved or otherwise unadjusted covariates due to limitations of the data. For instance, clinical outcomes may be impacted by surgeon experience, technique, or use of concomitant devices. As such, it is assumed that the distribution of potential confounders is similar between study comparison groups. Third, the study results may not necessarily be generalizable to all hospitals in the United States. However, the PHD contains a nationally representative sample of hospitals capturing 1 in 4 annual inpatient admissions. Furthermore, as the clinical presentation of patients receiving these devices should not differ across the populations, the study is generalizable to all patients meeting the study inclusion and exclusion criteria.
Conclusion
GST reloads represent an important innovation in surgical stapling technology. The current study compared clinical outcomes associated with the use of GST vs standard reloads among patients undergoing general or thoracic surgery using ECHELON FLEX™ manual staplers. As compared to standard reloads, GST reloads had comparable safety in terms of perioperative bleeding and 30-day anastomotic leak and met the prespecified non-inferiority criteria among patients undergoing general surgery using ECHELON FLEX™ manual staplers. Furthermore, GST reloads had a numerically lower incidence of safety events as compared to standard reloads for thoracic surgery using ECHELON FLEX™ manual staplers. It is hoped the findings of the current study will guide the direction of future technology development, especially in regions with less access to powered staplers.
Abbreviations
GST, gripping surface technology; LSG, laparoscopic sleeve gastrectomy; VATS, video-assisted thoracoscopic surgery; PHD, Premier Healthcare Database; ICD-10-CM, International Classification of Diseases, Tenth Revision, Clinical Modification; ICD-10-PCS, International Classification of Diseases, Tenth Revision, Procedure Coding System; LOS, length of stay; ORT, operating room time; SMD, standardized mean difference; CI, confidence interval; SD, standard deviation.
Data Sharing Statement
The data that support the findings of this study are available from Premier Applied Sciences®.but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are, however, available from the authors upon reasonable request and with permission of Premier Applied Sciences®. Please, contact Stephen P Fortin with any data-related requests.
Ethics Approval and Informed Consent
Pursuant to Title 45 Code of Federal Regulations, Part 46 of the United States, specifically 45 CFR 46.104 (d)(4), retrospective analyses conducted in the DOD and MDCD are considered exempt from informed consent and institutional review board (IRB) approval in the United States. All methods were carried out in accordance with relevant guidelines and regulations.
Acknowledgments
There are no further acknowledgements to disclose.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding was provided by Johnson & Johnson.
Disclosure
Stephen P Fortin, William Petraiuolo, Guy Cafri, Gustavo Scapini, Stephen Johnston, Barbara H Johnson, Paul M Coplan, and Shumin Zhang are employees of Johnson & Johnson or subsidiary companies of Johnson & Johnson and own stock of Johnson & Johnson. Pratyush Agarwal and Divya Chakke are paid consultants for Johnson & Johnson. Pratyush Agarwal and Divya Chakke are employees of Mu Sigma Inc. which received funds to provide data analytic support for the study. The authors report no other conflicts of interest in this work.
References
1. Highet A, Johnson EH, Bonham AJ, et al. Cost effectiveness of staple line reinforcement in laparoscopic sleeve gastrectomy. Ann Surg. 2021. doi:10.1097/SLA.0000000000004950
2. Ethicon website. Available from: https://www.jnj.com/media-center/press-releases/ethicon-launches-echelon-flex-gst-system-with-advanced-gripping-surface-technology.
3. Fegelman E, Knippenberg S, Schwiers M, et al. Evaluation of a powered stapler system with gripping surface technology on surgical interventions required during laparoscopic sleeve gastrectomy. J Laparoendosc Adv Surg Tech A. 2017;27(5):489–494. doi:10.1089/lap.2016.0513
4. Rawlins L, Johnson BH, Johnston SS, et al. Comparative effectiveness assessment of two powered surgical stapling platforms in laparoscopic sleeve gastrectomy: a retrospective matched study. Med Devices. 2020;13:195–204. doi:10.2147/MDER.S256237
5. Park SY, Kim DJ, Mo Nam C, et al. Clinical and economic benefits associated with the use of powered and tissue-specific endoscopic staplers among the patients undergoing thoracoscopic lobectomy for lung cancer. J Med Econ. 2019;22(12):1274–1280. doi:10.1080/13696998.2019.1634081
6. Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36(1):8–27. doi:10.1097/00005650-199801000-00004
7. van Walraven C, Austin PC, Jennings A, Quan H, Forster AJ. A modification of the Elixhauser comorbidity measures into a point system for hospital death using administrative data. Med Care. 2009;47(6):626–633. doi:10.1097/MLR.0b013e31819432e5
8. Zubizarreta JR. Stable weights that balance covariates for estimation with incomplete outcome data. J Am Stat Assoc. 2015;110:910–922. doi:10.1080/01621459.2015.1023805
9. Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009;28:3083–3107. doi:10.1002/sim.3697
10. Chattopadhyay A, Hase CH, Zubizarreta JR. Balancing vs modeling approaches to weighting in practice. Stat Med. 2020;39(24):3227–3254. doi:10.1002/sim.8659
11. Efron B, Tibshirani RJ. An Introduction to the Bootstrap. New York: Chapman and Hall/CRC; 1994.
12. Cafri G, Wood J, Gagne J, Sirois C. Partition testing for real-world evidence studies. Pharmacoepidemiol Drug Saf. 2022;31:1–7. doi:10.1002/pds.5540
13. Ethicon website. Available from: https://www.jnjmedicaldevices.com/sites/default/files/user_uploaded_assets/pdf_assets/2019-08/ECHELON-FLEX-GST-System-Brochure-066368-170821_0.pdf.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.