")
Back to Journals » International Journal of General Medicine » Volume 16
Comparison of Clinical Outcomes of Endovascular Therapy and Hybrid Surgery in the Treatment of Trans-Atlantic Inter-Society Consensus II D Aortoiliac Occlusive Disease
Authors Gao Z, Yue Y, Zhang Y, Jiang W, Zhang Y, Ran F, Li X
Received 20 March 2023
Accepted for publication 23 May 2023
Published 31 May 2023 Volume 2023:16 Pages 2149—2156
DOI https://doi.org/10.2147/IJGM.S408609
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Zheng Gao,1,* Yanyu Yue,2,* Youjia Zhang,1 Wentao Jiang,1 Yepeng Zhang,1 Feng Ran,1 Xiaoqiang Li1
1Department of Vascular Surgery, Affiliated Drum Tower Hospital, Medical School of Nanjing University, Nanjing, 2100082, People’s Republic of China; 2Nanjing Drum Tower Hospital Clinical College of Traditional Chinese and Western Medicine, Nanjing University of Chinese Medicine, Nanjing, 210008, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Feng Ran; Xiaoqiang Li, Email [email protected]; [email protected]
Purpose: To study and compare the clinical outcomes of endovascular therapy with those of hybrid surgery in the treatment of Trans-Atlantic Inter-Society Consensus II (TASC II) D aortoiliac occlusive disease (AIOD).
Patients and Methods: Patients with TASC II D-type AIOD who underwent their first surgical treatment at our hospital between March 2018 and March 2021 were enrolled and followed up to evaluate the improvement in symptoms, complications, and primary patency. The Kaplan–Meier method was used to compare the differences in primary patency between the treatment groups.
Results: In total, 132 of 139 enrolled patients (94.96%) achieved technical success following treatment. The perioperative mortality rate was 1.44% (2/139), and postoperative complications occurred in two patients. Among the patients who successfully underwent surgery, 120 underwent endovascular treatment (110 patients with stenting and 10 patients with thrombolysis before stenting), 10 underwent hybrid surgery, and 2 underwent open surgery. The follow-up data were compared between the endovascular and hybrid groups. At the end of the follow-up period, the patency rates in the hybrid and endovascular groups were 100% and 89.17% (107/120), respectively. The endovascular group achieved primary patency rates of 94.12%, 92.44%, and 89.08% at 6, 12, and 24 months postoperatively, respectively, whereas the primary patency rate remained at 100% in the hybrid group, with no significant variation between the endovascular and hybrid groups (P = 0.289). The endovascular group was further divided into a stent subgroup (110 patients) and a thrombolysis/stent subgroup (10 patients), and no prominent variation was noted in the primary patency between the two subgroups (P = 0.276).
Conclusion: Although open surgery is the gold standard treatment for TASC II D-type AIOD, endovascular and hybrid treatments are feasible and effective. Both methods showed good technical success and early to midterm primary patency rates.
Keywords: aortoiliac occlusive disease, endovascular stenting, angioplasty, thrombolysis, hybrid surgery
Introduction
Aortoiliac occlusive disease (AIOD) also known as stenosis or occlusion, is primarily caused by atherosclerosis and occurs in the infrarenal abdominal aorta and iliac artery. Owing to a continuous increase in the ageing population, the incidence of peripheral artery diseases in China has increased in recent years. By 2019, approximately 41.13 million people had peripheral artery disease, and nearly one-third of them had the involvement of the main iliac artery.1 People with AIOD experience symptoms such as intermittent claudication, pain at rest, ulcers, and gangrene, which are difficult to treat. AIOD can eventually lead to amputation and other severe outcomes if left untreated, which can affect the patient’s quality of life. Recently, the use of endovascular therapy for AIOD has been increasing.2 Endovascular therapy is especially preferred for local lesions classified according to the Trans-Atlantic Inter-Society Consensus II (TASC II) guidelines.3 However, for extensive lesions (TASC II types C and D), reconstructive surgery is recommended because the current evidence does not provide proof regarding the effectiveness of endovascular therapy.3 As endovascular technology has developed rapidly in recent years, it can be used to treat complex TASC lesions with positive effects on patients. A meta-analysis showed that endovascular treatment and surgical revascularization have comparable secondary patencies when used to treat TASC II C and D lesions.4 However, the current studies evaluating the effectiveness of endovascular treatment for TASC II D lesions are mostly limited to relatively small sample sizes. Therefore, the clinical value of endovascular treatment has not yet been fully elucidated. Hence, in this study, we retrospectively analysed the efficacy, safety, and early patency of endovascular treatment and hybrid surgery to identify the best treatment for TASC II D-type AIOD.
Materials and Methods
Ethical Approval
This single-centre retrospective cohort study was conducted in compliance with the STROCSS guidelines and was approved by the Ethics Committee of the Affiliated Drum Tower Hospital, Medical School of Nanjing University (2018-015-05).
Patients and Data Collection
Patients with TASC II D-type AIOD who received their first surgical treatment in our department between March 2018 and March 2021 were enrolled. The study’s inclusion criteria were as follows: 1) patients with symptoms that met the diagnostic criteria for AIOD and were categorized as TASC II D-type lesions through digital subtraction angiography (DSA) and computed tomography angiography (CTA); 2) the presence of an outflow tract at the distal end of the limb; and 3) patients with intermittent claudication, pain at rest, lower limb ulcer, or gangrene. The exclusion criteria were as follows: 1) patients complicated by distal popliteal artery disease; 2) those with serious dysfunction or failure of the heart, liver, kidney, or other important organs; and 3) those with incomplete clinical data. All patients underwent imaging examinations, such as CTA (Figure 1A) or DSA of the lower limbs, or were evaluated using the ankle-brachial index (ABI) to assess the lesion location and the degree of stenosis. After comprehensively considering the patient’s condition as well as, the physiological and biochemical examination results and a discussion with the patient, a surgical plan for each patient was determined.
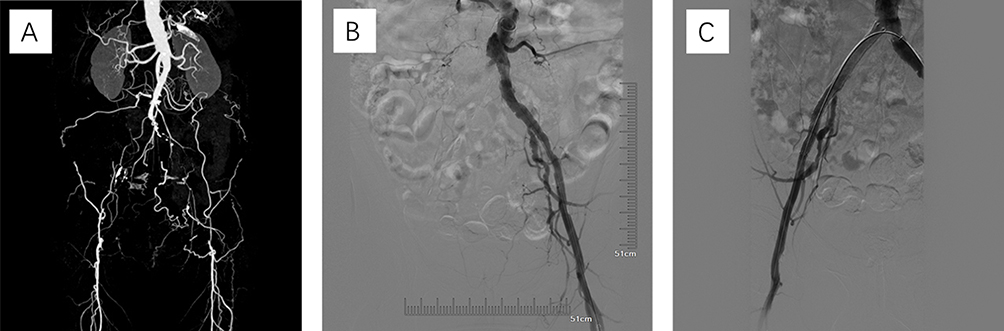 |
Figure 1 Imaging findings of a case with bilateral iliac artery occlusion. (A) Preoperative computed tomography angiography showed occlusion of bilateral iliac artery. (B) During the operation, the right iliac artery did not develop by angiography, and occlusion was confirmed. (C) The right iliac artery was recanalized after balloon angioplasty and stenting, and angiography confirmed that the vessel was in good condition without leakage. |
Endovascular Procedures
The vessel sheath was obtained from Cook Inc. (Bloomington, IN, USA). The guidewire, balloon dilatation catheter, and vascular closure device were obtained from Abbott Vascular (Abbott Park, IL, USA). The hydrophilic guidewire was obtained from Boston Scientific (Natick, MA, USA), and the percutaneous transluminal angioplasty (PTA) dilatation catheter and self-expanding biliary stent system were obtained from ev3 Incorporated (Plymouth, MN, USA). Drug-coated balloon catheters, iliac extension stent–graft systems, and bifurcated stent–graft systems were obtained from Medtronic (Santa Rosa, CA, USA). The abdominal aortic-covered stent–graft system was obtained from Lifetech Scientific (Shenzhen, China), and bare metal stents were obtained from Abbott Vascular (Abbott Park, IL, USA).
The Seldinger technique was used in all the patients. Lidocaine hydrochloride was administered as local infiltration for inducing anaesthesia at the puncture site. The surgical approach was determined according to the lesion location and the degree of vascular stenosis. A retrograde approach via the bilateral femoral arteries was preferred. If occlusion occurred at the opening site of the iliac artery or if repeated puncture failed, an antegrade approach via the brachial artery was performed. After performing a successful puncture, a sheath was placed, followed by a guidewire and catheter. The length and boundary of the stenosis and the involvement of the abdominal aorta, bilateral iliac arteries, and femoral arteries were determined using angiography (Figure 1B). Surgical access was established by indwelling the puncture sheath or switching to a peel-away introducer sheath. An intravenous bolus of heparin (1 mg/kg) was administered, and a 0.035 guide wire or V-18 guidewire was introduced into the lesion. Subsequently, the sheath was withdrawn, and a balloon dilatation catheter was introduced through the guidewire. The stenotic segment was pre-dilated and changes in the blood flow were observed using angiography. An appropriate stent (bare or covered metal stent) was implanted (Figure 1C), and angioplasty was performed again to confirm that the stent was placed properly, the blood vessel was in good condition, and there was no leakage of the contrast agent. Balloon dilatation was performed again for managing any residual stenosis (Figure 1).
Urokinase thrombolysis was performed if the patient had a fresh thrombus or if there was difficulty passing the guidewire through the occluded segment. A thrombolytic catheter was placed in the distal abdominal aorta or bilateral common iliac arteries, and urokinase was injected. A total of 200,000 U of urokinase plus 50 mL of 0.9% sodium chloride injection was administered, ensuring that the injection was completed within 20–30 min. This dosage was later changed to a continuous pump of 100,000 U of urokinase plus 50 mL of 0.9% sodium chloride injection at a rate of 6–20 mL/h as part of thrombolytic therapy. After 2–7 days, the outcome of thrombolysis was determined using angiography, and endovascular treatment was performed.
Hybrid Surgery Procedures
The patients underwent hybrid surgery under general anaesthesia in a hybrid operating room where hybrid surgeries are performed. Arteriotomy of the femoral artery and embolectomy were performed in six patients, followed by transluminal angioplasty and stenting of the iliac artery. Two patients underwent arteriotomy of the femoral artery and embolectomy, followed by transluminal angioplasty and stenting of the abdominal aorta and bilateral iliac arteries. One patient underwent femoropopliteal artery bypass, followed by transluminal angioplasty and stenting of the iliac artery. One patient underwent plaque removal from the deep femoral artery and endarterectomy of the superficial femoral artery, followed by a transluminal angioplasty and stenting of the iliac artery.
Follow-Up and Outcomes
Anticoagulation and antiplatelet therapies were administered to all patients postoperatively. Statins were recommended for life. The patients were followed-up at 1, 3, 6, and 12 months postoperatively and annually thereafter and were assessed for clinical symptoms and postoperative complications as well as underwent physical examination, ABI measurement, and CTA when necessary. The improvement in clinical symptoms and physical condition was indicated by the following: no intermittent claudication or increased distance of intermittent claudication; no or reduced pain on rest; palpability of the femoral, popliteal, anterior tibial, posterior tibial, and dorsal pedis arteries of the affected limb; improved or healed ulcer or gangrene; and improved skin temperature and colour of the affected limb. The follow-up endpoint was June 2022.
Technical success was defined as the restoration of blood flow without stenosis or with <30% residual stenosis 24 h after surgery. Primary patency was defined as the absence of postoperative clinical symptoms and restenosis or occlusion on imaging. Loss of primary patency was defined as restenosis or occlusion of the target vessel and the need for reintervention to maintain arterial patency.
Statistical Analysis
GraphPad Prism version 7.0 (GraphPad Software, San Diego, CA, USA) was used for statistical analyses. Discrete variables are expressed as percentages or frequencies and were compared using Fisher’s exact test. Continuous variables are expressed as mean ± standard deviation or median with interquartile ranges and were compared using the t-test or nonparametric Mann‒Whitney test. The Kaplan‒Meier method was used to generate the primary patency curve, and the Log rank test was used to compare the curves. A P value of < 0.05 was considered statistically significant.
Results
A total of 139 patients with TASC II D-type AIOD underwent their first surgical treatment at our hospital between March 2018 and March 2021. The endovascular operation failed in three patients because the guidewire could not pass through the arterial occlusion, one patient underwent open vessel repair owing to vascular injury during the operation, and one patient did not cooperate during endovascular treatment. Two patients died postoperatively, with a perioperative mortality rate of 1.44%. Technical success was achieved in 132 patients (94.96%). Among the patients who successfully underwent surgery, 120 underwent endovascular therapy, 10 underwent hybrid surgery, and 2 underwent open surgery. Because the sample size of patients who underwent open surgery was too small, only the data of those who underwent endovascular therapy and hybrid surgery were analysed in this study. Ultimately, the data of 130 patients with 171 limbs were analysed. Baseline demographic and clinical variables are presented in Table 1.
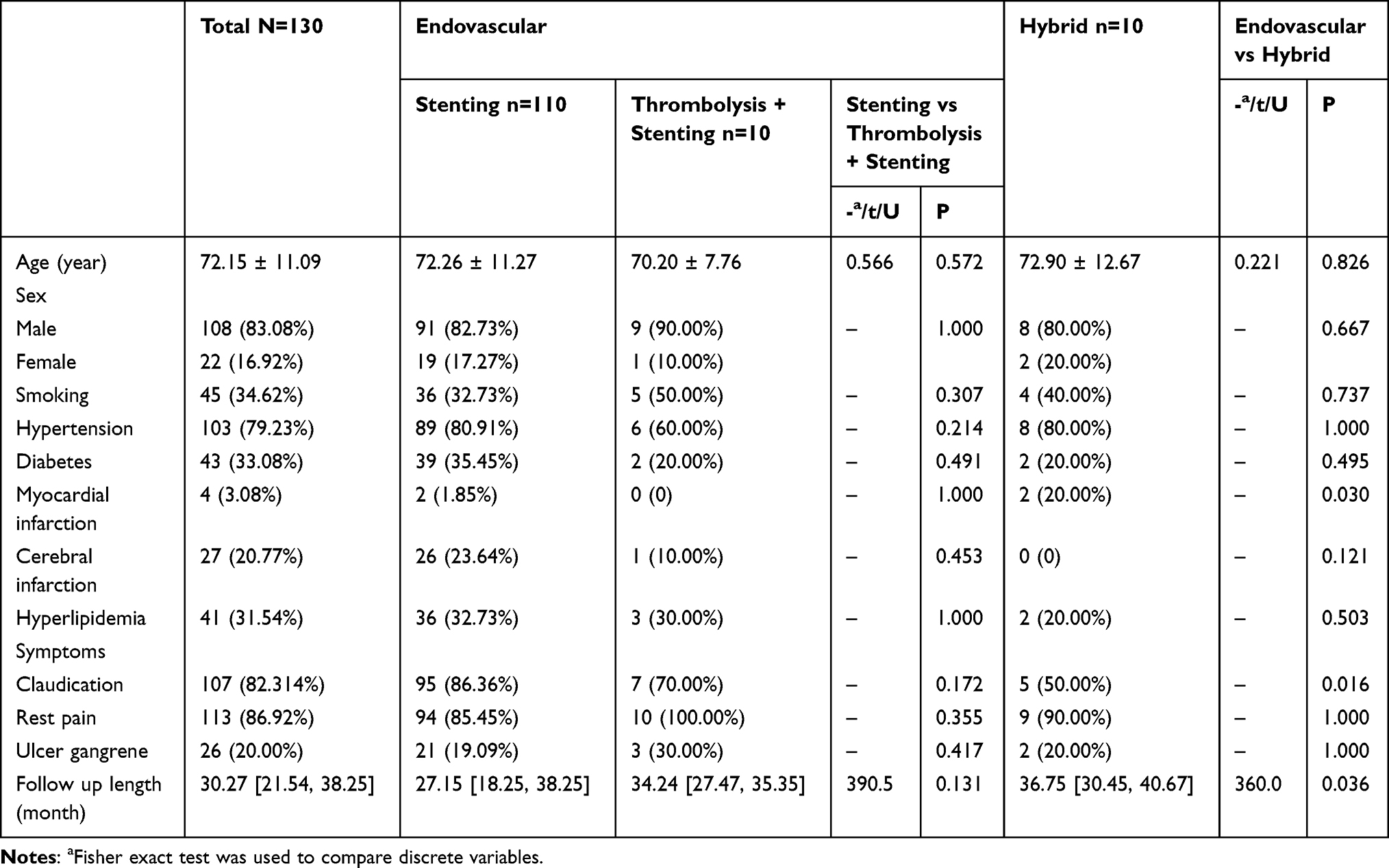 |
Table 1 Baseline Demographic and Clinical Characteristics of All Patients |
The median duration of follow-up was 27.50 months (range, 1–51.67 months) in the endovascular group and 36.75 months (range, 27.23–44.40 months) in the hybrid group. At the end of the follow-up period, all patients who underwent hybrid surgery retained vascular patency. In the endovascular group, the patency rate at the end of the follow-up period was 89.17% (107/120), with 12 cases of reintervention and one death (unrelated to surgery). Two complications occurred within 30 days postoperatively (one hematoma at the puncture site and one femoral artery pseudoaneurysm) in the endovascular group. Patients with complications were treated appropriately after hospitalization. The short-term primary patency rates were 100%, 98.32%, 94.12%, and 92.44% in the endovascular group and 100% in the hybrid group at 1, 3, 6, and 12 months postoperatively, respectively. The midterm primary patency rate at 24 and 36 months postoperatively was 89.08% in the endovascular and 100% in the hybrid group, with no significant difference between the two groups (χ2 = 1.125; P = 0.289; Figure 2).
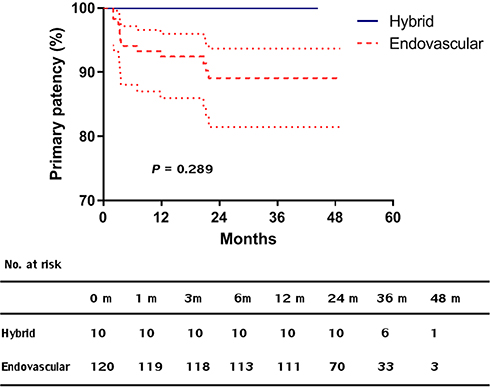 |
Figure 2 Kaplan‒Meier plots showing the vascular patency of the endovascular and hybrid groups. |
We further evaluated the role of thrombolysis in endovascular therapy in patients with TASC D-type AIOD. In the endovascular group, 10 patients received thrombolytic therapy before endovascular treatment. The differences in the baseline and clinical characteristics between the two groups were not significant (Table 1). As shown in the Log rank test, no prominent variation was noted in the primary patency duration between the stent subgroup and thrombolysis/stent subgroup (χ2 = 1.187; P = 0.276; Figure 3). The short-term primary patency rates at 1, 3, 6, and 12 months postoperatively were 100%, 99.08%, 94.41%, and 93.58%, respectively, in the stent group and 100%, 90.00%, 80.00%, and 80.00%, respectively, in the thrombolysis/stent group. The midterm primary patency rate at 24 and 36 months was 89.82% in the stent subgroup and 80.00% in the thrombolysis/stent subgroup.
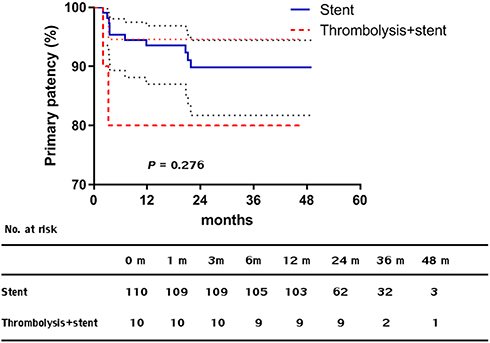 |
Figure 3 Kaplan‒Meier plots showing the vascular patency of stent and thrombolysis/stent subgroups in the endovascular group. |
Discussion
Owing to the insufficient understanding of AIOD in grassroots hospitals and the limited level of diagnosis, most patients with AIOD develop extensive and complex D-type lesions when they visit the department of vascular surgery. Open surgical options, such as aortobifemoral bypass grafting, aortoiliac endarterectomy, and extra-anatomic bypass, are considered the gold standard treatment for such complex lesions. The overall 5-year primary patency rate of these open surgeries is >85.0%, with systemic morbidity of >10%.5 Open surgery is more traumatic, which puts forward higher requirements for the basic condition of patients, resulting in an increasing interest in less invasive approaches with similar therapeutic outcomes. The Chinese expert consensus suggests that endovascular treatment is recommended for extensive D-type lesions and that hybrid surgery can be performed when patients with AIOD have common femoral artery bifurcation disease.6 Our experience suggests that both endovascular and hybrid treatments demonstrate satisfactory midterm outcomes and low perioperative mortality in patients with TASC II D-type lesions and are worthy of further clinical application.
In this study, 94.96% of patients achieved technical success. A meta-analysis of 19 studies with 1711 patients showed that the technical success of endovascular treatment for C- and D-type lesions ranged between 86% and 100%,4 consistent with that reported in recent studies.7–9 As only D-type lesions were included in the present study, the treatment difficulty was relatively high. We believe that a technical success rate of 94.96% is satisfactory.
In the current study, the 1-, 2-, and 3-year primary patency rates were 92.44%, 89.08%, and 89.08%, respectively, for the endovascular treatment and 100% for the hybrid treatment. Although the patency rate of hybrid surgery appears to be higher than those of endovascular treatment, the difference is not significant, and the small sample size of the hybrid group may be associated with this result. Similarly, a study reported that patency in patients who underwent hybrid surgery (femoral endarterectomy and stenting) tended to improve compared with that in patients who underwent stenting only.10 In comparison, in another study with a mean follow-up duration of 23 months, the primary patency rate was 85.4% for the hybrid approach of femoral endarterectomy and stenting in patients with C- and D-type lesions.11 Previous studies have reported that the 1- and 3-year primary patency rates of endovascular treatment ranged from 70% to 97% and 66% to 91%, respectively, in patients with C- and D-type lesions.9,10,12–17 Several studies reported that the patency rates of endovascular treatment in patients with D-type lesions ranged from 85% to 93% at 1 year and 80% to 93.75% at 2 years.7,8,18–22 Although only D-type lesions were included in the present study, the difference in the long-term patency rates between patients with A/B lesions and those with C/D lesions who received endovascular treatment was not significant, similar to that reported in previous studies.9,15 Several endovascular techniques have been developed in recent years, among which the commonly used techniques include kissing stents, covered endovascular reconstruction of aortic bifurcations, and unibody-branched stent grafts. Although the patency rates of various techniques in patients with C- and D-type lesions vary at different centres, a comprehensive meta-analysis suggested that the primary and secondary patency rates are similar; compared with those who underwent open surgery, patients who underwent endovascular treatment demonstrated lower 30-day mortality and comparable secondary patency.23 Furthermore, endovascular treatment is associated with lower hospital expenses and is more cost-effective than open surgery.24
The merit of this study is that the total sample size is relatively large. However, this study has some limitations. First, the sample sizes of some individual subgroups were too small. Therefore, we could not compare the effectiveness of endovascular treatment with that of open surgery. Second, the follow-up period was insufficient to analyse the long-term primary and secondary patency rates. Third, the research results were inevitably affected by the decision-making process and technical level of different surgeons. For example, experienced vascular surgeons have higher success rates in performing endovascular surgeries. Further multicentre controlled clinical studies are needed to provide more evidence on the long-term outcomes of TASC II type D lesions. Nonetheless, our study provides useful information regarding the safety and efficacy of endovascular treatment for extensive AIOD.
Conclusion
In conclusion, the results of this single-centre retrospective study suggest that both endovascular and hybrid treatment methods have good technical success and early- to midterm primary patency rates. Although open surgery is still the primary recommendation for TASC II type D lesions, we need to combine different measures according to specific circumstances to implement the most beneficial treatment for lower-risk patients.
Abbreviations
AIOD, Aortoiliac occlusive disease; TASC, Trans-Atlantic Inter-Society Consensus; DSA, Digital subtraction angiography; CTA, Computed tomography angiography; ABI, Ankle–brachial index.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author (Feng Ran) upon reasonable request, and the data was after obtaining informed consent from the patients.
Ethics Statement
The study was reviewed and approved by the Medical School of Nanjing University and was conducted according to the guidelines of the Declaration of Helsinki. All the patients provided written informed consent to participate in this study and were assured of the confidentiality and anonymity of the information related to the survey.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Song P, Rudan D, Wang M, Chang X, Rudan I. National and subnational estimation of the prevalence of peripheral artery disease (PAD) in China: a systematic review and meta-analysis. J Glob Health. 2019;9(1):010601. doi:10.7189/jogh.09.010601
2. Upchurch Jr. GR, Dimick JB, Wainess RM, et al. Diffusion of new technology in health care: the case of aorto-iliac occlusive disease. Surgery. 2004;136(4):812–818. doi:10.1016/j.surg.2004.06.019
3. Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FGR; TASC II Working Group. Inter-society consensus for the management of peripheral arterial disease (TASC II). Eur J Vasc Endovasc Surg. 2007;33(1 Supplement):S1–S75.
4. Jongkind V, Akkersdijk GJM, Yeung KK, Wisselink W. A systematic review of endovascular treatment of extensive aortoiliac occlusive disease. J Vasc Surg. 2010;52(5):1376–1383. doi:10.1016/j.jvs.2010.04.080
5. Chiu KWH, Davies RSM, Nightingale PG, Bradbury AW, Adam DJ. Review of direct anatomical open surgical management of atherosclerotic aorto-iliac occlusive disease. Eur J Vasc Endovasc Surg. 2010;39(4):460–471. doi:10.1016/j.ejvs.2009.12.014
6. Expert consensus writing group of lower extremity arterial disease Group, Vascular Surgery Committee, National Expert Committee on Cardiovascular Diseases. Vascular Surgery Committee, Chinese Medical Education Association. Association, Chinese expert consensus on diagnosis and treatment of aortoiliac occlusive disease. Chin Circ J. 2020;35(10):948–954.
7. Tewksbury R, Taumoepeau L, Cartmill A, Butcher A, Cohen T. Outcomes of covered expandable stents for the treatment of TASC D aorto-iliac occlusive lesions. Vascular. 2015;23(6):630–636. doi:10.1177/1708538114568479
8. Mayor J, Branco BC, Chung J, et al. Outcome comparison between open and endovascular management of TASC II D aortoiliac occlusive disease. Ann Vasc Surg. 2019;61:65–71.e3. doi:10.1016/j.avsg.2019.06.005
9. Yang M, Zhang B, Niu G, Yan Z, Tong X, Zou Y. Long-term results of endovascular reconstruction for aortoiliac occlusive disease. Quant Imaging Med Surg. 2021;11(4):1303–1312. doi:10.21037/qims-20-599
10. Rzucidlo EM, Powell RJ, Zwolak RM, et al. Early results of stent-grafting to treat diffuse aortoiliac occlusive disease. J Vasc Surg. 2003;37(6):1175–1180. doi:10.1016/S0741-5214(03)00326-4
11. Ray JJ, Eidelson SA, Karcutskie CA, et al. Hybrid revascularization combining iliofemoral endarterectomy and iliac stent grafting for transatlantic inter-society consensus C and D aortoiliac occlusive disease. Ann Vasc Surg. 2018;50:73–79. doi:10.1016/j.avsg.2017.11.061
12. Nyman U, Uher P, Lindh M, Lindblad B, Ivancev K. Primary stenting in infrarenal aortic occlusive disease. Cardiovasc Intervent Radiol. 2000;23(2):97–108. doi:10.1007/s002709910021
13. Björses K, Ivancev K, Riva L, Manjer J, Uher P, Resch T. Kissing stents in the aortic bifurcation – a valid reconstruction for aorto-iliac occlusive disease. Eur J Vasc Endovasc Surg. 2008;36(4):424–431. doi:10.1016/j.ejvs.2008.06.027
14. Kashyap VS, Pavkov ML, Bena JF, et al. The management of severe aortoiliac occlusive disease: endovascular therapy rivals open reconstruction. J Vasc Surg. 2008;48(6):1451–1457.e3. doi:10.1016/j.jvs.2008.07.004
15. Ichihashi S, Higashiura W, Itoh H, Sakaguchi S, Nishimine K, Kichikawa K. Long-term outcomes for systematic primary stent placement in complex iliac artery occlusive disease classified according to Trans-Atlantic Inter-Society Consensus (TASC)-II. J Vasc Surg. 2011;53(4):992–999. doi:10.1016/j.jvs.2010.10.069
16. Taeymans K, Groot Jebbink E, Holewijn S, et al. Three-year outcome of the covered endovascular reconstruction of the aortic bifurcation technique for aortoiliac occlusive disease. J Vasc Surg. 2018;67(5):1438–1447. doi:10.1016/j.jvs.2017.09.015
17. Shen C, Zhang Y, Qu C, Fang J, Liu X, Teng L. Outcomes of Total Aortoiliac Revascularization for TASC-II C&D lesion with kissing self-expanding covered stents. Ann Vasc Surg. 2020;68:434–441. doi:10.1016/j.avsg.2020.04.055
18. Park KB, Do YS, Kim DI, et al. The TransAtlantic InterSociety Consensus (TASC) classification system in iliac arterial stent placement: long-term patency and clinical limitations. J Vasc Interv Radiol. 2007;18(2):193–201. doi:10.1016/j.jvir.2006.12.726
19. Sixt S, Alawied AK, Rastan A, et al. Acute and long-term outcome of endovascular therapy for aortoiliac occlusive lesions stratified according to the TASC classification: a single-center experience. J Endovasc Ther. 2008;15(4):408–416. doi:10.1583/08-2359.1
20. Psacharopulo D, Ferrero E, Ferri M, et al. Increasing efficacy of endovascular recanalization with covered stent graft for TransAtlantic Inter-Society Consensus II D aortoiliac complex occlusion. J Vasc Surg. 2015;62(5):1219–1226. doi:10.1016/j.jvs.2015.06.218
21. Ahn S, Park KM, Kim YK, et al. Outcomes of endovascular treatment for TASC C and D aorto-iliac lesions. Asian J Surg. 2017;40(3):215–220. doi:10.1016/j.asjsur.2015.11.006
22. Bracale UM, Giribono AM, Spinelli D, et al. Long-term results of endovascular treatment of TASC C and D aortoiliac occlusive disease with expanded polytetrafluoroethylene stent graft. Ann Vasc Surg. 2019;56:254–260. doi:10.1016/j.avsg.2018.07.060
23. Salem M, Hosny MS, Francia F, et al. Management of extensive aorto-iliac disease: a systematic review and meta-analysis of 9319 patients. Cardiovasc Intervent Radiol. 2021;44(10):1518–1535. doi:10.1007/s00270-021-02785-6
24. Rocha-Neves J, Ferreira A, Sousa J, et al. Endovascular approach versus aortobifemoral bypass grafting: outcomes in extensive aortoiliac occlusive disease. Vasc Endovascular Surg. 2020;54(2):102–110.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.