")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 14
Comparison between the long-axis/in-plane and short-axis/out-of-plane approaches for ultrasound-guided vascular catheterization: an updated meta-analysis and trial sequential analysis
Authors Liu C , Mao Z, Kang HJ, Hu X, Jiang S, Hu P , Hu J, Zhou F
Received 29 September 2017
Accepted for publication 19 December 2017
Published 20 February 2018 Volume 2018:14 Pages 331—340
DOI https://doi.org/10.2147/TCRM.S152908
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Deyun Wang
Chao Liu,* Zhi Mao,* Hongjun Kang, Xin Hu, Shengmao Jiang, Pan Hu, Jie Hu, Feihu Zhou
Department of Critical Care Medicine, Chinese People’s Liberation Army General Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Background: A long-axis in-plane (LA-IP) approach and a short-axis out-of-plane (SA-OOP) approach are the two main approaches used in ultrasound (US)-guided vascular catheterization. However, the efficacy and safety of these approaches remain controversial. Therefore, we performed this meta-analysis to compare the two techniques in vascular catheterization.
Materials and methods: Relevant studies were searched in PubMed, Embase, and the Cochrane Library databases from database inception until August 2017. Randomized controlled trials comparing a long-axis approach with a short-axis approach for US-guided vascular cannulation were selected. The RevMan software was used to analyze the results, and trial sequential analysis (TSA) was further applied to determine whether the currently available evidence was sufficient and conclusive.
Results: Eleven studies met the inclusion criteria. Overall, 1,210 patients were included. The total success rate was similar between the SA-OOP and LA-IP approaches for US-guided vascular catheterization (risk ratio [RR], 1.01; 95% CI, 0.99–1.04; P=0.35; I2=48%). In the radial artery (RA; RR, 1.00; 95% CI, 0.96–1.05; P=0.88; I2=49%) and internal jugular vein (IJV; RR, 1.00; 95% CI, 0.98–1.02; P=0.99; I2=0%) subgroups, the total success rate was also similar and was confirmed by the TSA. For populations with subclavian vein (SCV) and axillary vein catheterization, the SA-OOP approach showed a benefit for first-attempt success rate. No significant differences in first-attempt success rate, cannulation times, or complications were found between the two approaches.
Conclusion: Despite a similar total success rate between the SA-OOP approach and the LA-IP approach when used for RA and IJV catheterization (as confirmed by TSA), further robust well-designed trials are warranted to evaluate other outcomes. There is insufficient evidence to definitively state that the SA-OOP approach was superior to the LA-IP approach when used for SCV and axillary vein catheterization. High-quality trials are needed to confirm or refute this finding.
Keywords: ultrasound guidance, long-axis in-plane, short-axis out-of-plane, vascular catheterization, radial artery, internal jugular vein
Background
Ultrasound (US)-guided vascular cannulation has become more popular in recent years, and US is a proven tool to increase the success rate and decrease complications in a wide variety of vascular catheterization procedures.1 Numerous meta-analyses2–7 have demonstrated the advantage of US-guided vascular catheterization over a blind landmark approach. However, there is a controversy regarding which approach is preferable for the US probe, ie, the short-axis out-of-plane (SA-OOP) approach or the long-axis in-plane (LA-IP) approach. Each approach has distinct advantages and disadvantages that may either increase or decrease complications.8 In the SA-OOP approach, the relationships of the target vessel to the adjacent vessels are visualized, but the needle tip may not be continuously visualized during catheter placement. In the LA-IP approach, the needle path including the tip can be continuously visualized during catheterization; however, the relationship of the target vessel to adjacent vessels may be lost.9 A previous meta-analysis of five studies showed that there is insufficient evidence to definitively determine which approach is superior in patients undergoing US-guided vascular catheterization.10 Several randomized controlled trials (RCTs) on this topic have been published recently. Therefore, we performed this updated meta-analysis of RCTs to compare the efficacy and safety of these two techniques and further applied trial sequential analysis (TSA) to determine whether the currently available evidence was sufficient and conclusive. This in turn can provide more reliable evidence for clinical practice.
Materials and methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA statement) guidelines were used to perform this meta-analysis.11 Ethical approval was not required.
Search strategy and study selection
A search of the PubMed (US National Library of Medicine, Bethesda, MD, USA), Embase, and Cochrane Central Register of Controlled Trials databases was conducted from database inception to August 2017. Specific search strategies were developed for each database using exploded Medical Subject Headings and the appropriate corresponding keywords including “ultrasound,” “ultrasonography,” “ultrasonic” AND “catheterization,” “cannulation,” “catheter,” “catheters,” “insertion” AND “long axis,” “short axis,” “in plane,” “out of plane,” “longitudinal,” “transverse” AND “RCTs.” In addition, the reference lists of the screened full-text studies were searched to identify other potentially eligible trials. Searches were performed without language restrictions. A further search by manually reviewing conference proceedings and the references of review articles was performed.
The inclusion criteria were as follows: 1) population: adult patients requiring vascular catheterization; 2) comparison: the study compared LA-IP vs SA-OOP techniques for US-guided vascular catheterization; 3) outcome measure: the total success rate was reported; and 4) study design: RCTs.
Data extraction and outcome measurement
Two investigators (CL and ZM) independently performed the study selection. When data were missing or incomplete, the original authors were contacted by written correspondence for clarification. Disagreements between the two investigators were resolved by consensus or adjudicated by a third investigator (FZ). The dynamic needle tip positioning (DNTP) technique was classified as the SA-OOP approach. One standard form was used for data collection, which included the following information: first author, year of publication, patient population, the number of patients, age of patients, total success rate, first-attempt success rate, cannulation time, number of attempts, experience of the operators, puncture site, and type of US equipment. The primary outcome was the total success rate, and secondary outcomes included the first-attempt success rate, cannulation time, and the number of attempts.
Risk of bias assessment
We assessed the internal validity of included trials using the Cochrane Collaboration Risk of Bias tool.12 The criteria in the tool included a description of the random sequence generation, allocation concealment, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. Criteria were individually scored as high, low, or unclear risk of bias.
Statistical analysis
The statistical analysis was performed using RevMan software (version 5.3; Cochrane Collaboration, Copenhagen, Denmark) for outcome measurements. The results of the risk ratio (RR) for dichotomous outcomes or the mean difference (MD) for continuous data were expressed as means and 95% CIs. A random-effects model was used regardless of heterogeneity, which was estimated using the I2 statistic. A value of I2>50% indicated significant heterogeneity.13 Potential sources of heterogeneity were identified by sensitivity analyses. We further conducted subgroup analyses according to the puncture site. Publication bias was assessed using the Begg and Egger tests. P<0.05 was considered to indicate a statistically significant difference. The sample mean and SD were estimated according to the sample size, median, range, and/or interquartile range.14
TSA
An updated meta-analysis with new studies may result in false positive results; thus, to decrease the risk of type I errors, the TSA was used. This method can determine whether the present evidence is reliable and conclusive.15 When the cumulative Z-curve crosses the trial sequential monitoring boundary or enters the futility area, a sufficient level of evidence for the anticipated intervention effect may have been reached, and no further trials are needed. If the Z-curve does not cross any of the boundaries and the required information size (RIS) has not been reached, evidence to reach a conclusion is insufficient, and more trials are needed to confirm the results. For this TSA, we estimated the RIS using α=0.05 (two sided), β=0.10 (power 90%), the control event proportions calculated from the long-axis group, and a relative risk reduction of 10% in outcomes. TSA was conducted using TSA Version 0.9 Beta (www.ctu.dk/tsa).16
Results
Study enrolment and characteristics
A total of 348 potentially relevant studies were collected, of which 334 studies were excluded based on titles, abstracts, and duplicate studies. Three articles were excluded because the article type was a letter or meta-analysis. Ultimately, 11 studies17–27 fulfilled the inclusion criteria for the meta-analysis (Figure 1). The study characteristics are summarized in Table 1. These studies were published between 2011 and 2017, and a total of 1,210 patients were included. The sample size of the studies ranged from 40 to 190 subjects. Baseline characteristics were similar between the two groups. All of the operators had experience in US-guided vascular catheterization. All studies reported the total success rate, and various complications were reported among these studies. The details for the risk of bias tool are shown in Figure 2. No study fulfilled all criteria for a low risk of bias. A randomized sequence was adequately generated in all studies. Due to the nature of the studies, it was impossible to perform the study blinded. No potential publication bias was observed for primary outcomes (data not shown).
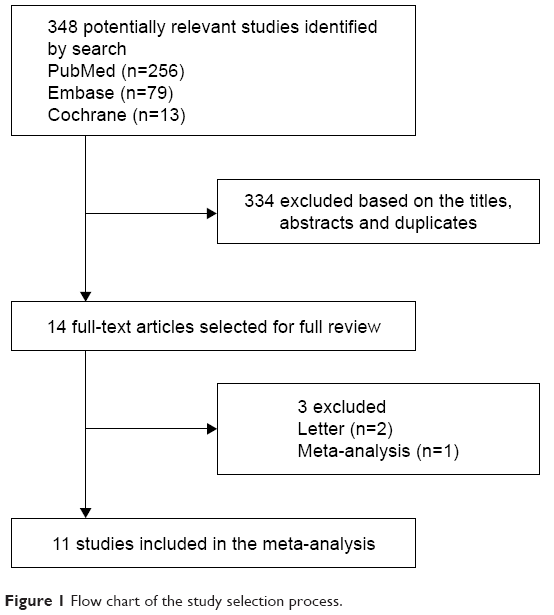 | Figure 1 Flow chart of the study selection process. |
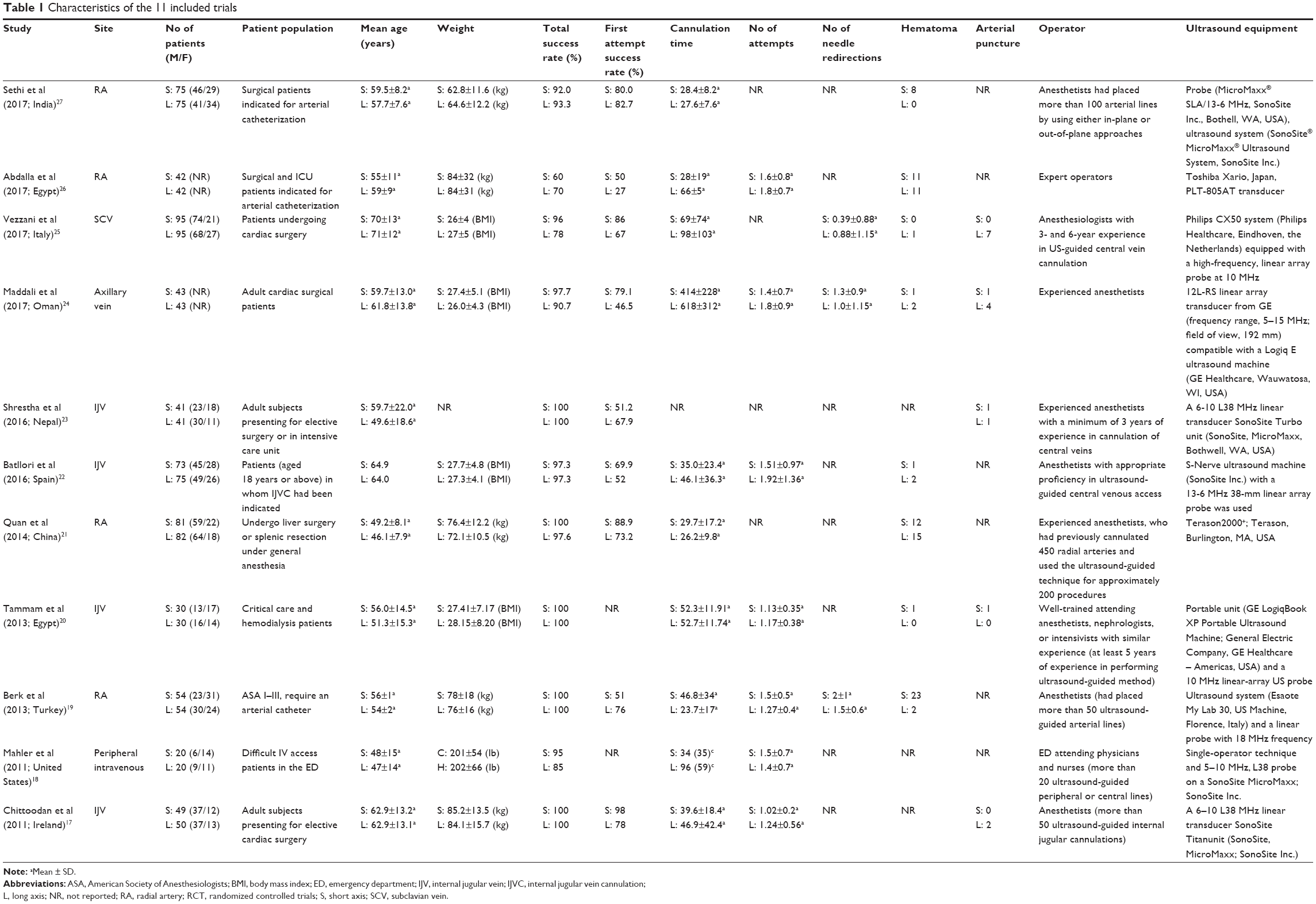 | Table 1 Characteristics of the 11 included trials33 |
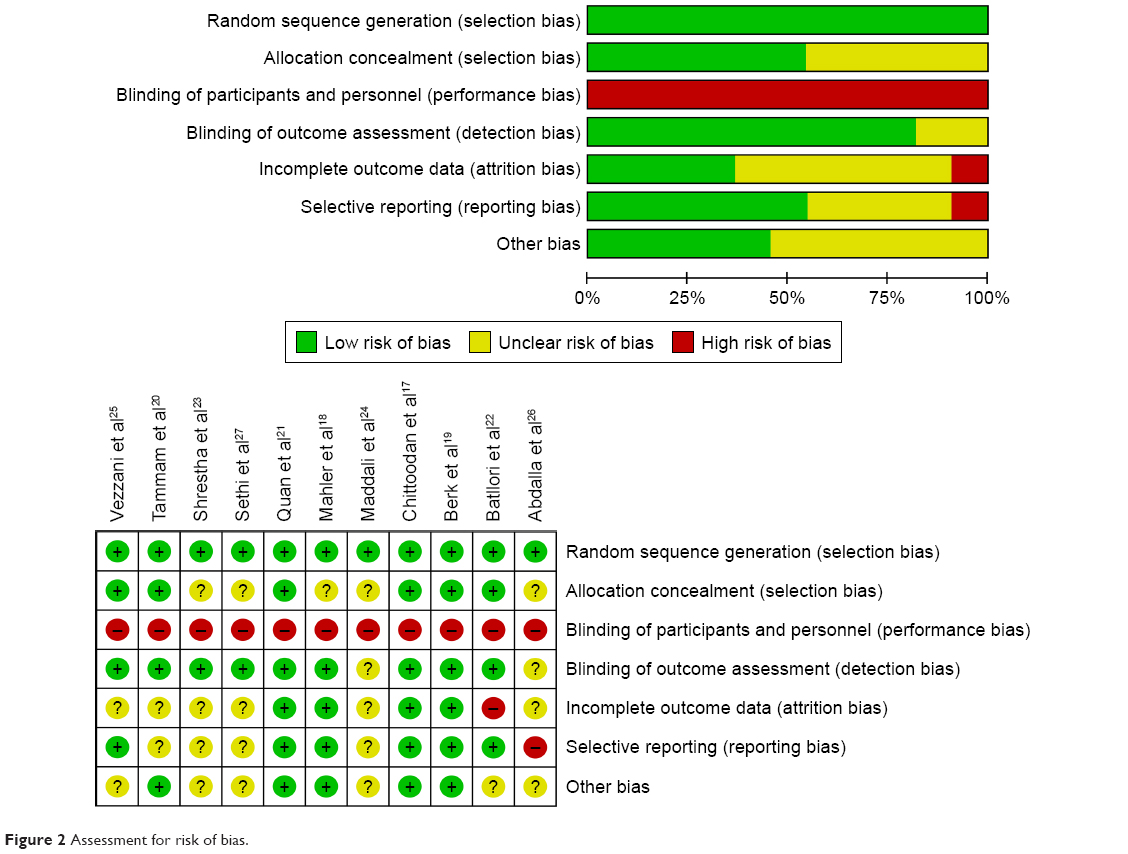 | Figure 2 Assessment for risk of bias. |
Primary outcome
Total success rate
All studies investigated the total success rate of both the SA-OOP and LA-IP approaches for US-guided vascular catheterization. No significant difference was observed between the two groups (RR, 1.01; 95% CI, 0.99–1.04; P=0.35; I2=48%; Figure 3). Subgroup analyses were performed to investigate the source of heterogeneity. In the radial artery (RA) subgroup,19,21,26,27 the total success rate was no different between the SA-OOP and LA-IP groups (RR, 1.00; 95% CI, 0.96–1.05; P=0.88; I2=49%; Figure 3), and the TSA confirmed this result (the cumulative Z-curve crossed the futility boundary and entered the futility area; Figure 4A). In the internal jugular vein (IJV) subgroup,17,20,22,23 the total success rate was also no different between the SA-OOP and LA-IP groups (RR, 1.00; 95% CI, 0.98–1.02; P=0.99; I2=0%; Figure 3) and the TSA also confirmed the result (the cumulative Z-curve crossed the futility boundary and entered the futility area; Figure 4B). Only one study25 was included in the subclavian vein (SCV) subgroup, and the results show that the SA-OOP approach was more efficacious than the LA-IP approach in increasing the total success rate (RR, 1.23; 95% CI, 1.10–1.38; P<0.01; Figure 3).
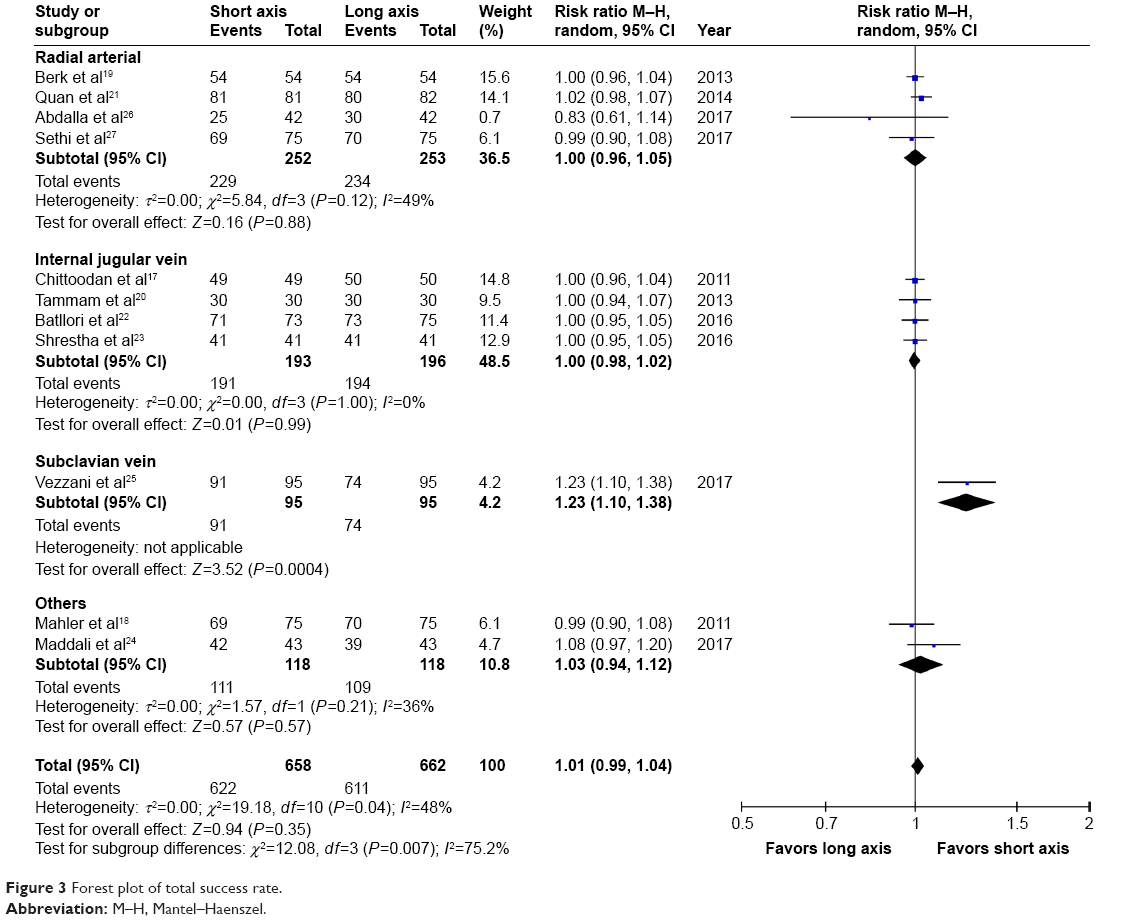 | Figure 3 Forest plot of total success rate. |
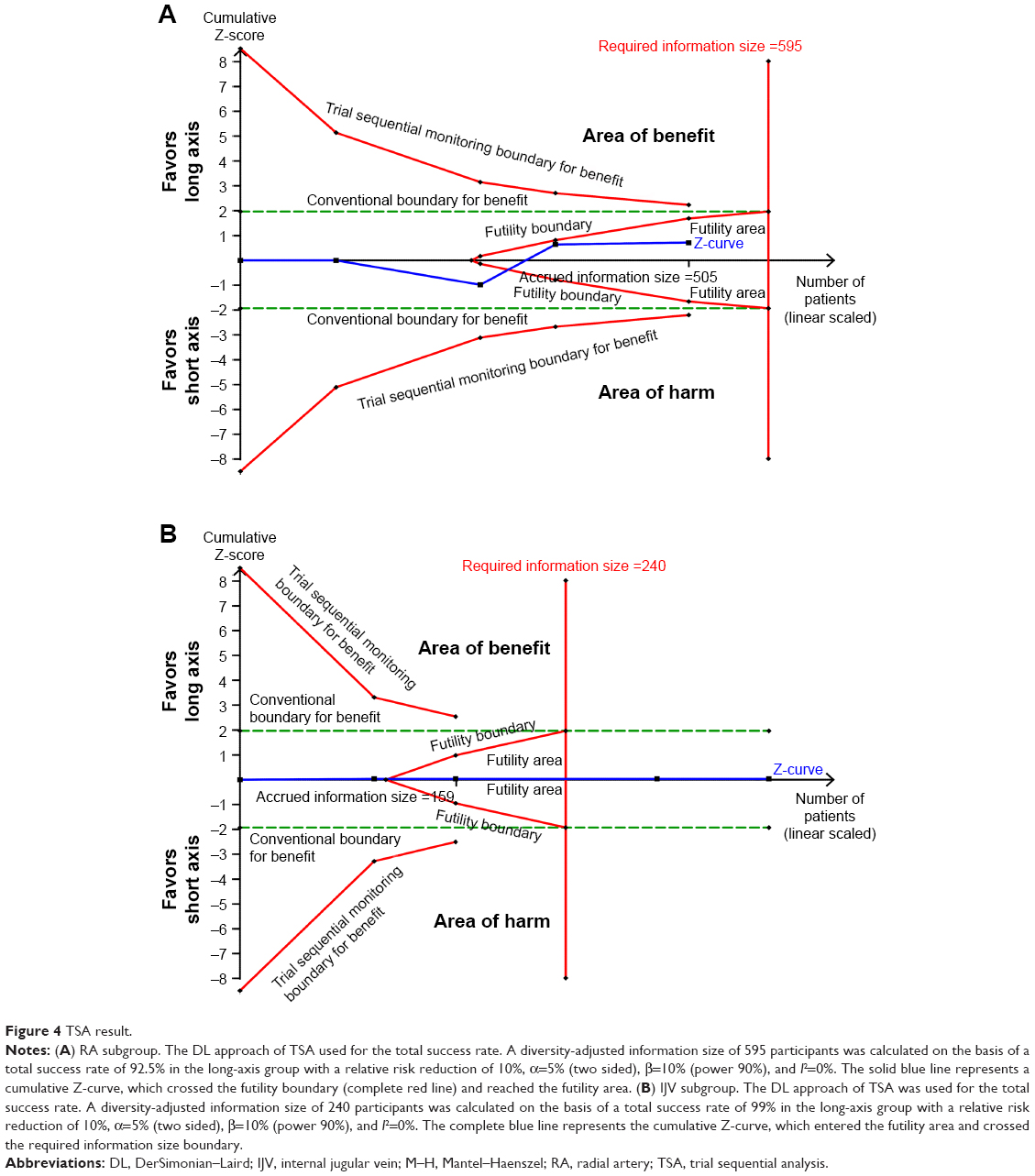 | Figure 4 TSA result. |
Secondary outcomes
First-attempt success rate
Nine studies17,19,21–27 reported the first-attempt success rate. There was no significant difference between the LA-IP approach group and the SA-OOP approach group (RR, 1.14; 95% CI, 0.96–1.35, P=0.14, I2=80%; Figure 5). Due to remarkable heterogeneity, preset subgroup analyses were performed for the populations with RA catheterization (RR, 1.03; 95% CI, 0.77–1.38; P=0.85, I2=84%; Figure 5) and IJV catheterization (RR, 1.12; 95% CI, 0.84–1.49; P=0.33; I2=74%; Figure 5). No significant differences were observed. For populations with SCV catheterization25 and axillary vein catheterization,24 the SA-OOP approach showed a benefit.
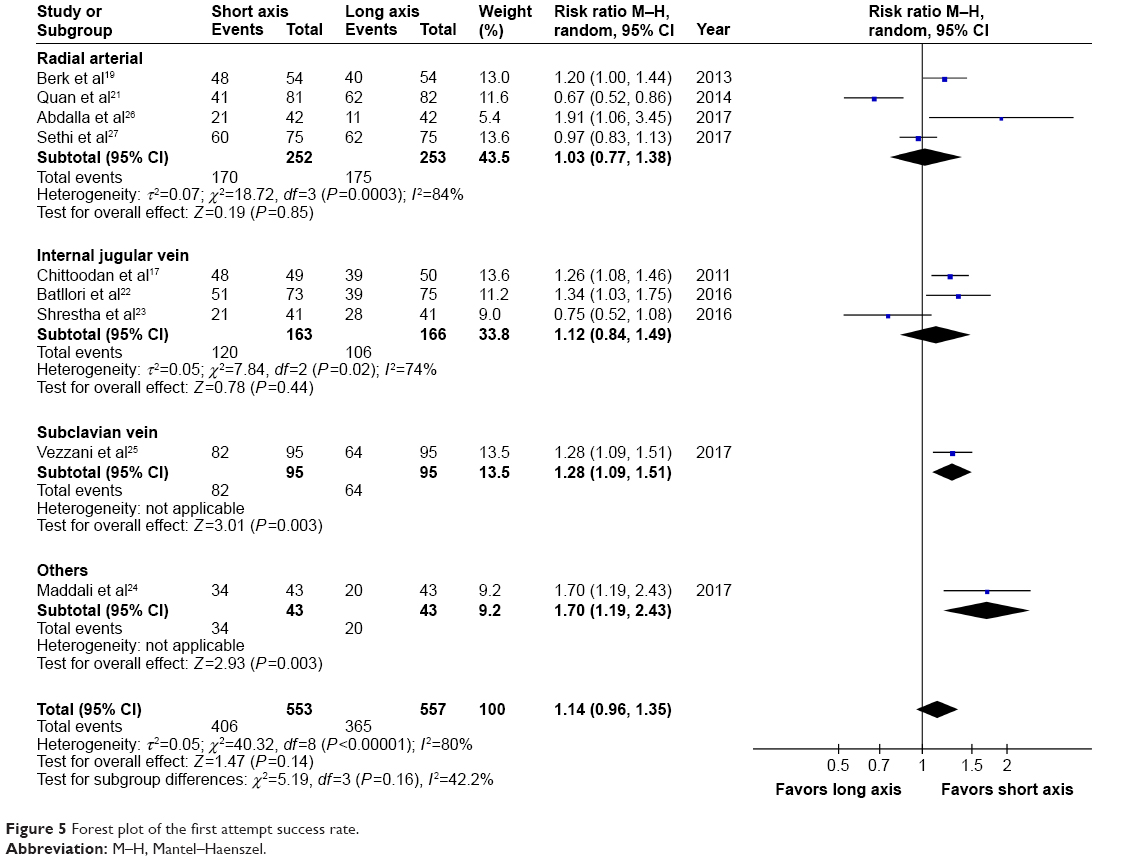 | Figure 5 Forest plot of the first attempt success rate. |
Other secondary outcomes are summarized in Table 2, including cannulation times, the number of attempts, complications of hematoma, and arterial puncture. The cannulation times of the two approaches used in the US-guided RA and IJV catheterization were similar. The number of attempts may be reduced when the SA-OOP approach is used in US-guided IJV catheterization and the LA-IP approach is used in US-guided RA catheterization. No significant differences were observed when comparing the complications of hematoma and arterial puncture between the two approaches.
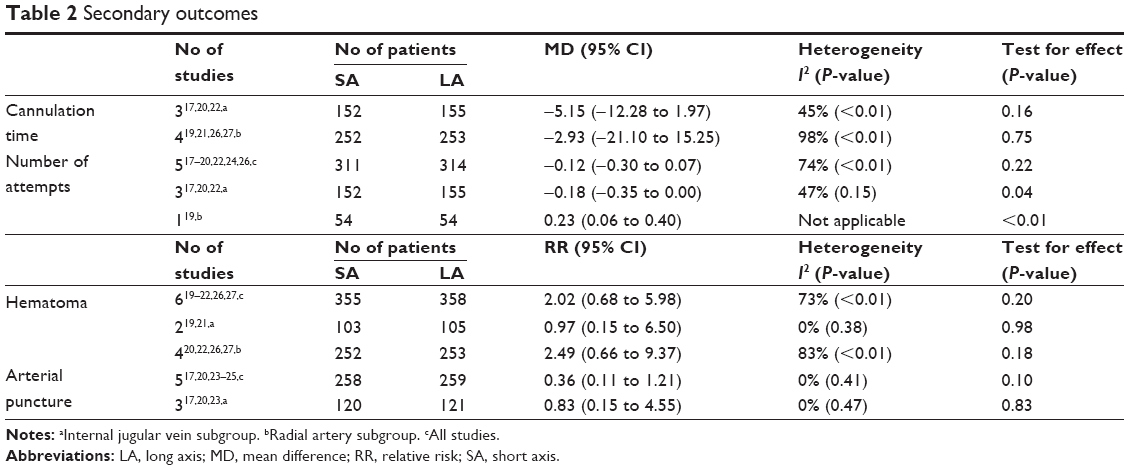 | Table 2 Secondary outcomes |
Discussion
The key findings of this updated meta-analysis are as follows. 1) The total success rate was similar between the SA-OOP approach and LA-IP approach when used for RA and IJV catheterization, as confirmed by TSA. The SA-OOP approach showed a benefit when used for SCV catheterization; however, further RCTs are needed to confirm this. 2) The first-attempt success rate was also similar between the two approaches when used for US-guided RA or IJV catheterization. Whether the SA-OOP approach has an advantage in increasing the first-attempt success rate when used for SCV and axillary vein catheterization also requires further studies to confirm or refute this finding. 3) The number of attempts may be reduced when the SA-OOP approach is used in US-guided IJV catheterization and when the LA-IP approach is used in US-guided RA catheterization. 4) No significant differences in cannulation times or complications were found between the two approaches.
There are several differences between our meta-analysis and a previous meta-analysis.10 First, this meta-analysis included an additional six studies.22–27 Thus, this updated meta-analysis represents the latest and most comprehensive study. Second, TSA was further applied to better establish sufficient and conclusive evidence. Third, we also analyzed the difference between the two approaches when used in different vessels.
In this meta-analysis, the total success rate was similar when the two approaches were used for US-guided RA and IJV catheterization and was confirmed by TSA. Moreover, more studies are needed to further evaluate whether the complications, first-attempt success rate, and cannulation times are different between the two approaches. A study25 included in this meta-analysis showed that the SA-OOP approach may increase the total success rate when used for SCV catheterization; however, this led to controversy.28 High-quality studies are needed to confirm or refute this finding.
One study26 included in this meta-analysis reported that the oblique approach for US-guided RA catheterization may replace the two classic approaches due to its superior success rate, higher first-attempt success, and shorter time consumed for catheterization with higher operator satisfaction after the procedure. Confirmation of this requires further research. Another study22 in this meta-analysis compared three transducer orientation approaches for US-guided IJV catheterization and found that the oblique-axis (OAX) approach showed a higher first-needle pass success rate than LA-IP approach and a lower mechanical complications rate than the SA-OOP approach. Although more clinical studies are needed, this new approach may be superior in reducing complications related to IJV catheterization.
US-guidance for vascular catheterization is a user-dependent technology, and it is necessary to use medical simulators to train novice US users before they practice on patients. However, there are some discrepancies between the medical simulator result and the patient result. For example, one study29 evaluated the two approaches used in SCV catheterization in a human torso mannequin and found that the LA-IP view for SCV catheterization was more efficient with a decreased time to cannulation and fewer redirections. The simulators could not reflect the actual circumstances of the patients, and they lacked the nerves and arteries from soft tissue that commonly complicate US-guided vascular catheterization.30 Hence, whether the benefit obtained from the medical simulators can be proven in live patients is unknown. Therefore, to provide more reliable evidence for clinical practice, more high-quality, anatomically accurate, vascular phantoms and standardized performance procedures are needed for US training.31 Furthermore, when using the medical simulator to train novice US users, we should carefully consider the discrepancy between the medical simulator and the patient to improve clinical practice.
This meta-analysis has several potential limitations. First, considerable heterogeneity was observed between the included studies with respect to blood vessel type, operator experience, US equipment, and outcome definition, which could have influenced the results; second, due to the limited data, it is difficult to perform more subgroup or sensitivity analyses. Third, double blinding was not performed due to the features of the trials, which may result in performance and detection bias.
Conclusion
A similar total success rate between the SA-OOP approach and the LA-IP approach for RA and IJV catheterization was confirmed by TSA. However, further robust and well-designed trials are warranted to evaluate other outcomes. There is insufficient evidence to definitively state that the SA-OOP approach was better than the LA-IP approach when used for SCV and axillary vein catheterization. High-quality trials are needed to confirm or refute this finding.
Data sharing statement
The authors confirm that all data underlying the findings are fully available without restriction. All relevant data are within the paper.
Acknowledgments
This work was not supported by any funding.
Disclosure
The authors report no conflicts of interest in this work.
References
Moore CL. Ultrasound first, second, and last for vascular access. J Ultrasound Med. 2014;33(7):1135–1142. | ||
Randolph AG, Cook DJ, Gonzales CA, Pribble CG. Ultrasound guidance for placement of central venous catheters: a meta-analysis of the literature. Crit Care Med. 1996;24(12):2053–2058. | ||
Hind D, Calvert N, McWilliams R, et al. Ultrasonic locating devices for central venous cannulation: meta-analysis. BMJ. 2003;327(7411):361. | ||
Gu WJ, Tie HT, Liu JC, Zeng XT. Efficacy of ultrasound-guided radial artery catheterization: a systematic review and meta-analysis of randomized controlled trials. Crit Care. 2014;18(3):R93. | ||
Gao YB, Yan JH, Gao FQ, Pan L, Wang XZ, Lv CJ. Effects of ultrasound-guided radial artery catheterization: an updated meta-analysis. Am J Emerg Med. 2015;33(1):50–55. | ||
Lalu MM, Fayad A, Ahmed O, et al. Ultrasound-guided subclavian vein catheterization: a systematic review and meta-analysis. Crit Care Med. 2015;43(7):1498–1507. | ||
Stolz LA, Stolz U, Howe C, Farrell IJ, Adhikari S. Ultrasound-guided peripheral venous access: a meta-analysis and systematic review. J Vasc Access. 2015;16(4):321–326. | ||
Erickson CS, Liao MM, Haukoos JS, et al. Ultrasound-guided small vessel cannulation: long-axis approach is equivalent to short-axis in novice sonographers experienced with landmark-based cannulation. West J Emerg Med. 2014;15(7):824–830. | ||
Dilisio R, Mittnacht AJ. The “medial-oblique” approach to ultrasound-guided central venous cannulation – maximize the view, minimize the risk. J Cardiothorac Vasc Anesth. 2012;26(6):982–984. | ||
Gao YB, Yan JH, Ma JM, et al. Effects of long axis in-plane vs short axis out-of-plane techniques during ultrasound-guided vascular access. Am J Emerg Med. 2016;34(5):778–783. | ||
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010;8(5):336–341. | ||
Higgins JP, Altman DG, Gotzsche PC, et al. The Cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. | ||
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560. | ||
Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14:135. | ||
Liu C, Mao Z, Kang H, Hu J, Zhou F. Regional citrate versus heparin anticoagulation for continuous renal replacement therapy in critically ill patients: a meta-analysis with trial sequential analysis of randomized controlled trials. Crit Care. 2016;20(1):144. | ||
Thorlund K, Engstrøm J, Wetterslev J, Brok J, Imberger G, Gluud C [webpage on the Internet]. User Manual for Trial Sequential Analysis (TSA). Copenhagen, Denmark: Copenhagen Trial Unit, Centre for Clinical Intervention Research; 2011:1–115. Available from: www.ctu.dk/tsa. Accessed May 3, 2017. | ||
Chittoodan S, Breen D, O’Donnell BD, Iohom G. Long versus short axis ultrasound guided approach for internal jugular vein cannulation: a prospective randomised controlled trial. Med Ultrason. 2011;13(1):21–25. | ||
Mahler SA, Wang H, Lester C, Skinner J, Arnold TC, Conrad SA. Short- vs long-axis approach to ultrasound-guided peripheral intravenous access: a prospective randomized study. Am J Emerg Med. 2011;29(9):1194–1197. | ||
Berk D, Gurkan Y, Kus A, Ulugol H, Solak M, Toker K. Ultrasound-guided radial arterial cannulation: long axis/in-plane versus short axis/out-of-plane approaches? J Clin Monit Comput. 2013;27(3):319–324. | ||
Tammam TF, El-Shafey EM, Tammam HF. Ultrasound-guided internal jugular vein access: comparison between short axis and long axis techniques. Saudi J Kidney Dis Transpl. 2013;24(4):707–713. | ||
Quan Z, Tian M, Chi P, Cao Y, Li X, Peng K. Modified short-axis out-of-plane ultrasound versus conventional long-axis in-plane ultrasound to guide radial artery cannulation: a randomized controlled trial. Anesth Analg. 2014;119(1):163–169. | ||
Batllori M, Urra M, Uriarte E, et al. Randomized comparison of three transducer orientation approaches for ultrasound guided internal jugular venous cannulation. Br J Anaesth. 2016;116(3):370–376. | ||
Shrestha GS, Gurung A, Koirala S. Comparison between long- and short-axis techniques for ultrasound-guided cannulation of internal jugular vein. Ann Card Anaesth. 2016;19(2):288–292. | ||
Maddali MM, Arora NR, Chatterjee N. Ultrasound guided out-of-plane versus in-plane transpectoral left axillary vein cannulation. J Cardiothorac Vasc Anesth. 2017;31(5):1707–1712. | ||
Vezzani A, Manca T, Brusasco C, et al. A randomized clinical trial of ultrasound-guided infra-clavicular cannulation of the subclavian vein in cardiac surgical patients: short-axis versus long-axis approach. Intensive Care Med. 2017;43(11):1594–1601. | ||
Abdalla UE, Elmaadawey A, Kandeel A. Oblique approach for ultrasound-guided radial artery catheterization vs transverse and longitudinal approaches, a randomized trial. J Clin Anesth. 2017;36:98–101. | ||
Sethi S, Maitra S, Saini V, Samra T, Malhotra SK. Comparison of short-axis out-of-plane versus long-axis in-plane ultrasound-guided radial arterial cannulation in adult patients: a randomized controlled trial. J Anesth. 2017;31(1):89–94. | ||
Preda G, Bige N, Bonsey M, et al. Discussion on “a randomized clinical trial of ultrasound-guided infra-clavicular cannulation of the subclavian vein in cardiac surgical patients: short-axis versus long-axis approach”. Intensive Care Med. 2017;43(8):1169–1170. | ||
Vogel JA, Haukoos JS, Erickson CL, et al. Is long-axis view superior to short-axis view in ultrasound-guided central venous catheterization? Crit Care Med. 2015;43(4):832–839. | ||
Resnick JR, Cydulka R, Jones R. Comparison of two transducers for ultrasound-guided vascular access in long axis. J Emerg Med. 2007;33(3):273–276. | ||
AIUM practice guideline for the use of ultrasound to guide vascular access procedures. J Ultrasound Med. 2013;32(1):191–215. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.