")
Back to Journals » Clinical Interventions in Aging » Volume 12
Comparing the predictive accuracy of frailty, comorbidity, and disability for mortality: a 1-year follow-up in patients hospitalized in geriatric wards
Authors Ritt M, Ritt JI, Sieber CC, Gaßmann KG
Received 12 October 2016
Accepted for publication 17 November 2016
Published 8 February 2017 Volume 2017:12 Pages 293—304
DOI https://doi.org/10.2147/CIA.S124342
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Martin Ritt,1,2 Julia Isabel Ritt,2 Cornel Christian Sieber,1,3 Karl-Günter Gaßmann1,2
1Institute for Biomedicine of Ageing (IBA), Friedrich-Alexander Universität Erlangen-Nürnberg (FAU), Nürnberg, 2Department of Internal Medicine III (Medicine of Ageing), Geriatrics Centre Erlangen, Hospital of the Congregation of St Francis Sisters of Vierzehnheiligen, Erlangen, 3Department of Internal Medicine and Geriatrics, Hospital of the Order of St John of God, Regensburg, Germany
Background: Studies evaluating and comparing the power of frailty, comorbidity, and disability instruments, together and in parallel, for predicting mortality are limited.
Objective: This study aimed to evaluate and compare the measures of frailty, comorbidity, and disability in predicting 1-year mortality in geriatric inpatients.
Design: Prospective cohort study.
Patients and setting: A total of 307 inpatients aged ≥65 years in geriatric wards of a general hospital participated in the study.
Measurements: The patients were evaluated in relation to different frailty, comorbidity, and disability instruments during their hospital stays. These included three frailty (the seven-category Clinical Frailty Scale [CFS-7], a 41-item frailty index [FI], and the FRAIL scale), two comorbidity (the Cumulative Illness Rating Scale for Geriatrics [CIRS-G] and the comorbidity domain of the FI [Comorbidity-D-FI]), and two disability instruments (disability in basic activities of daily living [ADL-Katz] and the instrumental and basic activities of daily living domains of the FI [IADL/ADL-D-FI]). The patients were followed-up over 1 year.
Results: Using FI, CIRS-G, Comorbidity-D-FI, and ADL-Katz, this study identified a patient group with a high (≥50%) 1-year mortality rate in all of the patients and the two patient subgroups (ie, patients aged 65–82 years and ≥83 years). The CFS-7, FI, FRAIL scale, CIRS-G, Comorbidity-D-FI, and IADL/ADL-D-FI (analyzed as full scales) revealed useful discriminative accuracy for 1-year mortality (ie, an area under the curve >0.7) in all the patients and the two patient subgroups (all P<0.001). Thereby, CFS-7 (in all patients and the two patient subgroups) and FI (in the subgroup of patients aged ≥83 years) showed greater discriminative accuracy for 1-year mortality compared to other instruments (all P<0.05).
Conclusion: All the different instruments emerged as suitable tools for risk stratification in geriatric inpatients. Among them, CFS-7, and in those patients aged ≥83 years, also the FI, might most accurately predict 1-year mortality in the aforementioned group of individuals.
Keywords: frailty, comorbidity, disability, hospitalized geriatric patients, older people, health status, survival
Introduction
Older people are the fastest growing population in many Western societies.1,2 They represent a heterogeneous group with respect to their health status. Some old people reveal good physical and cognitive status and are active, whereas others are frail and/or suffer from multiple chronic diseases and/or disabilities.3 Frailty is a clinically recognizable state of increased vulnerability to stressors associated with an increased risk for adverse clinical outcomes.3–5 Comorbidity can be characterized as the concurrent presence of two or more medically diagnosed diseases.3 Disability is defined as difficulty or dependency in performing activities of daily living (ADLs).3 Measures of frailty, comorbidity, and/or disability can be used to estimate the biological age of older people.6,7 Such estimates of biological age were found to better predict mortality than chronological age in older people.8 Risk stratification, particularly estimating mortality risk, is important in terms of medical decision-making and optimal management of older patients.
Several different frailty, comorbidity, or disability instruments have been developed and evaluated. The Canadian Study on Health and Ageing Clinical Frailty Scale (CFS-7),5 and a Rockwood and Mitnitski frailty index (FI),5,9–12 for example, allow for the evaluation of older people in terms of the broader/larger construct of frailty.4 The FRAIL scale,13–15 among other instruments,16,17 can be used to evaluate people in terms of the construct of physical frailty.4 The Cumulative Illness Rating Scale for Geriatrics (CIRS-G)18,19 or an index or list based on several major diseases20 represents established comorbidity instruments. The Katz index21 or an index or list that comprises several major instrumental activities related to daily living (IADLs) and basic ADLs22,23 can be used to assess the ADL and IADL/ADL disability burden of older people.
Frailty, comorbidity, or disability instruments have been found to be successful in predicting mortality in different settings, including patients hospitalized in geriatric wards.24–30 However, data evaluation and comparison of the power of frailty, comorbidity, and disability instruments, together and in parallel, for predicting adverse clinical outcomes such as mortality are limited.31–33 It should be noted that the individual prognostic power of these measures of adverse clinical outcomes may vary between different age groups of older people.31,34 We had previously evaluated and compared the accuracy of different frailty instruments, together and in parallel, in predicting mortality in older patients hospitalized in geriatric wards.12,26,35 Until now, no study has adequately investigated and collated major different frailty, comorbidity, and disability instruments in terms of their ability to predict mortality in a cohort of older geriatric inpatients.
With this background, the present study aimed to analyze and contrast the ability of major frailty, comorbidity, and disability instruments in predicting 1-year mortality in older patients hospitalized in geriatric wards by considering different age ranges of the patients.
Methods
Study design and study population
This study was a prospective longitudinal analysis with a 1-year follow-up of hospitalized patients who were admitted to the geriatric wards of the Geriatrics Centre of the Hospital of the Congregation of St Francis Sisters of Vierzehnheiligen, Erlangen, Germany. The inclusion criterion was that age should be ≥65 years; the exclusion criteria were inability to give written informed consent and nonavailability of a legal guardian to give written informed consent on behalf of the study participant. The objective of this study was to evaluate and compare the ability of major different frailty (Rockwood et al’s5 seven-category Canadian Study on Health and Aging CFS-7, a Rockwood et al and Mitnitski et al’s5,9–12 41-item FI, and the Abellan van Kan et al’s13,14 FRAIL scale), comorbidity (the Miller et al’s19 CIRS-G and the comorbidity domain of FI [Comorbidity-D-FI]), and disability instruments (ADL disability based on the ADLs of the Katz et al’s21 Katz Index [ADL-Katz] and the IADL/ADL domain of the aforementioned FI [IADL/ADL-D-FI]) in predicting 1-year mortality in older patients hospitalized in geriatric wards. To this end, we performed the analyses on all the study participants and the two subgroups, that is, patients aged less than the median age and patients aged greater than or equal to the median age of the total study cohort, as well. The patients were evaluated in terms of different degrees of frailty, comorbidity, or disability according to the aforementioned instruments (baseline examination) at the same time before discharge of patients who were hospitalized in geriatric wards after treatment for an acute disease or the exacerbation of a chronic disease leading to hospital admission. Follow-up data were obtained 12 months after the baseline examination. These data included, among others, information about the death of the study participants during the follow-up period. Follow-up data were collected through telephonic interviews with patients, their physicians, specialists, relatives, or legal guardians. The study followed the principles of the Declaration of Helsinki and Good Clinical Practice. The study protocol was approved by the local ethics committee, that is, the Ethics Committee of the University of Erlangen-Nürnberg. Written informed consent was obtained from each study participant or from his or her legal guardian.
Instruments used for the evaluation of patients in terms of frailty, comorbidity, and disability
The seven-category Canadian Study on Health and Aging CFS-7
The CFS-7 allows grading of the frailty status of a patient by seven categories, as has previously been described in detail by Rockwood et al.5 In this way, the CFS-7 takes a persons’ fitness level, motivation, disease symptoms, fatique, performance in IADLs and ADLs as well as his/her clinical state of being terminally ill into account.5 The seven categories of the CFS-7 are: category 1 (very fit), category 2 (well), category 3 (well, with treated comorbid disease), category 4 (apparently vulnerable), category 5 (mildly frail), category 6 (moderately frail), and category 7 (severely frail/terminally ill).5
The 41-item FI
The FI consisted of 41 items (Table 1). The criteria reported by Searle et al11 and Rockwood et al36 were considered in order to operationalize FI. Thus, it can be regarded as a classical Rockwood and Mitnitski et al5,9–12 FI. The FI was based on data from a standardized comprehensive geriatric assessment (CGA).37 Table 1 summarizes the 41 items of the FI. The FI was calculated according to the sum of the scores for each item divided by the total number of items considered, resulting in a score ranging in magnitude from 0 to 1.
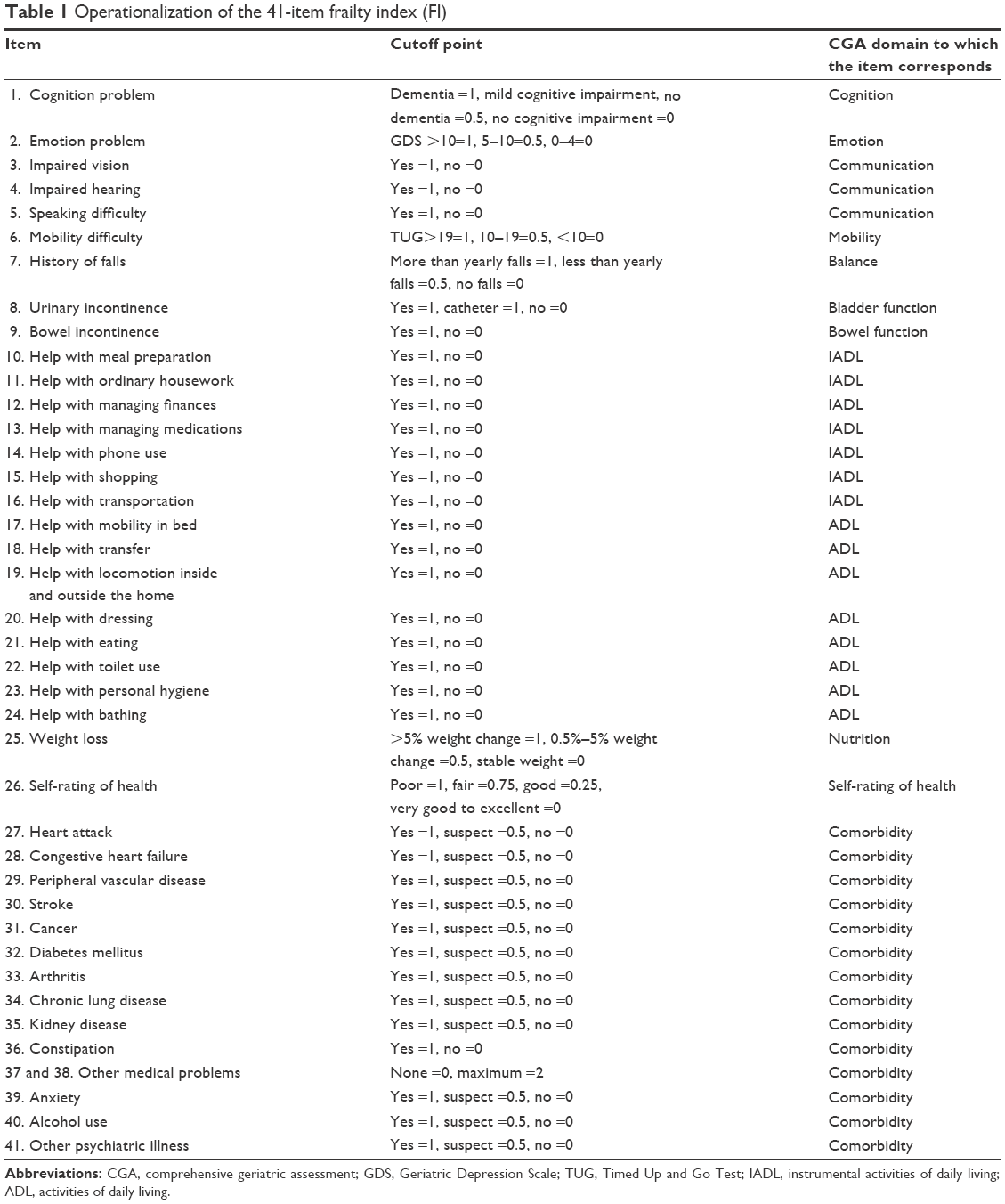 | Table 1 Operationalization of the 41-item frailty index (FI) |
The FRAIL scale
The FRAIL scale is based on five components: fatigue, resistance, ambulation, illness, and loss of weight.13–15 For this study, fatigue was operationalized as self-report of “feeling tired all the time,” resistance was operationalized as “inability to climb a flight of stairs,” ambulation was operationalized as “needing assistance with walking or he/she being unable to walk,” illness was operationalized as
five or more of the following 11 illnesses: heart attack, congestive heart failure, peripheral vascular disease, stroke, cancer, diabetes mellitus, arthritis, chronic lung disease, kidney disease, dementia, and depression,
and weight loss was operationalized as “weight loss of 5% or more within the last 12 months.” Patients with none of these components were considered to be robust; those with one or two to be pre-frail, and those with three or more to be frail.
The CIRS-G
The Cumulative Illness Rating Scale (CIRS) was initially developed and introduced by Linn et al18 in 1968. Miller et al19 later revised the CIRS, aiming to reflect the common problems of older people and renamed the index (CIRS-G). The CIRS-G is based on 14 items representing individual body systems: 1) heart, 2) vascular, 3) hematopoietic, 4) respiratory, 5) eyes, ears, nose, throat, and larynx, 6) upper gastrointestinal, 7) lower gastrointestinal, 8) liver, 9) renal, 10) genitourinary, 11) musculoskeletal/integument, 12) neurological, 13) endocrine/metabolic and breast, and 14) psychiatric illness.19 In this way, the severity of chronic diseases in each aforementioned 14 individual body systems is rated along a five grade system with a minimum score of 0 (no problem affecting that system) up to a maximum score of 4 (extremely severe problem) according to the criteria described previously in detail by Miller et al.19 Theoretically, the total score of the CIRS-G varies from 0 to 56.19
The Comorbidity-D-FI and the IADL/ADL domain of the FI (IADL/ADL-D-FI)
Individual items from the aforementioned FI can be referred to different domains of a CGA37 (Table 1). The score for the Comorbidity-D-FI was calculated as the sum of the scores for items 27–41 of the FI divided by 15. The score for the IADL/ADL-D-FI was calculated as the sum of the scores for items 10–24 of the FI divided by 15. Theoretically, the scores of the Comorbidity-D-FI and the IADL/ADL-D-FI can consequently range from 0 to 1.
The disability burden based on the six ADLs of the Katz index (ADL-Katz)
The ADL-Katz considers the six ADLs of the Katz Index,21 namely 1) bathing, 2) dressing, 3) toileting, 4) transferring, 5) continence (bowel and bladder), and 6) feeding.21 For this study, performance in functioning each of the ADLs was scored as follows: needing help with =1 and independence =0. Thus, the score for the ADL-Katz can vary from 0 (independence in all the six ADLs of the Katz index) to 6 (needing help in all the six ADLs of the Katz index).
Statistical analysis
All the statistical analyses were performed using SPSS software (SPSS Statistics 23; IBM Corporation, Armonk, NY, USA). The results are expressed as mean ± standard deviation, median (interquartile range), or percentage. Cox proportional hazard models were performed to analyze the hazard ratios for 1-year mortality risk of each increment in category or score of 0.1 of the different frailty, comorbidity, or disability instruments unadjusted and adjusted for age and gender. Receiver operating characteristic (ROC) curves were calculated to estimate the areas under the curve (AUCs) for the different instruments, analyzed as continuous variables, in relation to 1-year mortality. AUC values >0.7 indicate at least “useful” predictive accuracy of the model.38 Comparisons among the AUCs were performed using the method of Hanley and McNeil.39 The level of statistical significance was set a priori at P<0.050.
Results
A total of 307 (208 female and 99 male) patients were included in the study. One-year follow-up data were obtained from 305 patients (99.3%). The two patients who withdrew from the study during the 1-year follow-up period were 89.0±4.2 years old, one female and one male, and had a CFS-7 category of 5.00±0.0, FI score of 0.24±0.1, number of FRAIL scale components of 2.50±0.7, CIRS-G score of 10±2.8 points, Comorbidity-D-FI score of 0.18±0.0, ADL-Katz score of 1.00±0.0, and IADL/ADL-D-FI score of 0.30±0.4.
The clinical characteristics of the 305 patients from whom follow-up data were obtained and stratified into all patients, a subgroup of 139 patients aged between 65 and 82 years (ie, patients with an age less than the median age of the total study cohort), and a subgroup of 166 patients aged ≥83 years (ie, patients with an age greater than or equal to the median age of the total study cohort), are summarized in Table 2. Patients aged between 65 and 82 years were younger and taller, had a greater body weight, had a greater body mass index, and except for lung disease had lower percentage of history of individual diseases or adverse medical conditions (congestive heart failure, kidney disease, and bowel incontinence), lower percentage of patients who were institutionalized, lower CFS-7 category, FI, CIRS-G, ADL-Katz, IADL/ADL-D-FI score, and lower 1-year mortality rate compared to the patients aged ≥83 years (Table 2). Patients aged between 65 and 82 years did not differ from the patients aged ≥83 years with respect to the percentage of female patients, Mini Mental State Examination, Geriatric Depression Scale score, percentage of patients with history of heart attack, stroke, diabetes mellitus, percentage of patients with urinary incontinence or those being catheterized, percentage of patients with >5 medications, FRAIL scale components, and Comorbidity-D-FI score.
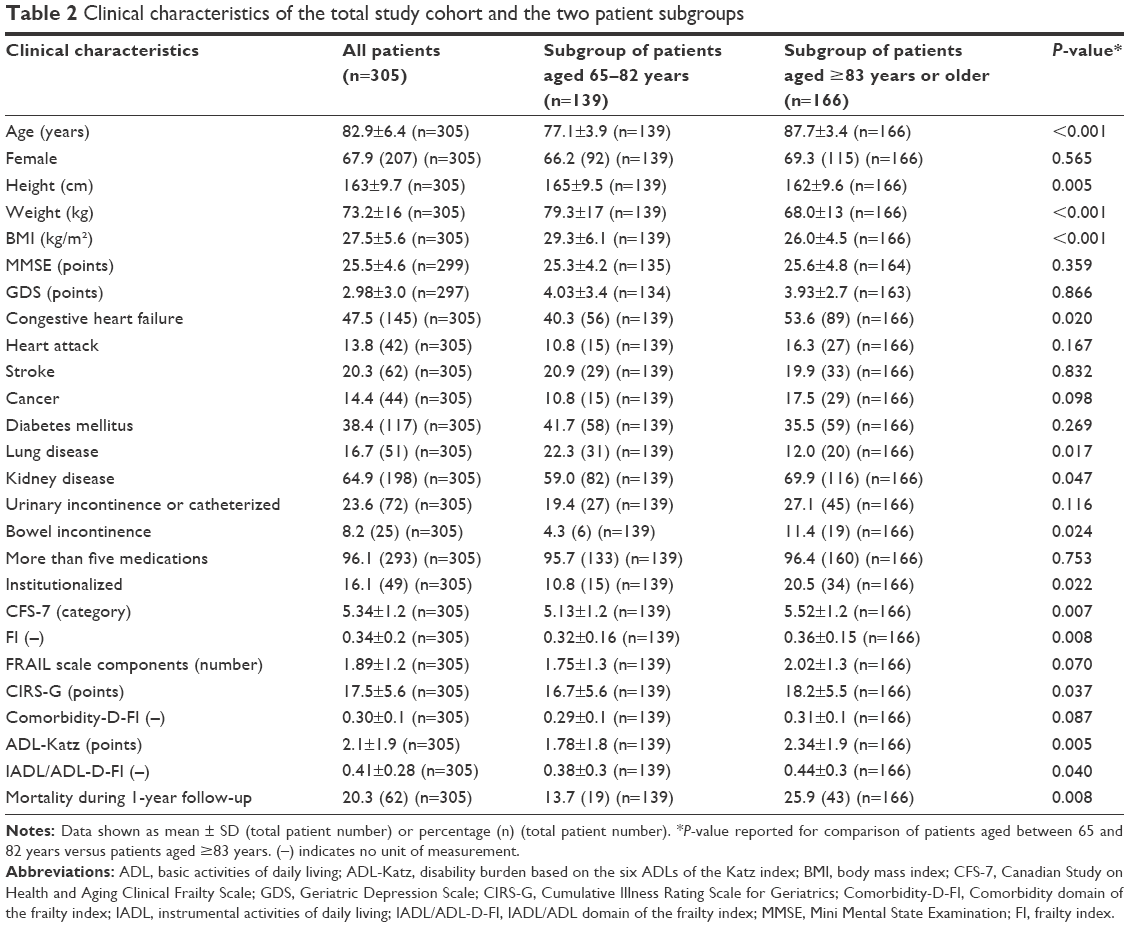 | Table 2 Clinical characteristics of the total study cohort and the two patient subgroups |
The mortality rates of the patients stratified into different categories or groups in terms of different frailty, comorbidity, or disability instruments, in all the patients and the two patient subgroups are summarized in Table 3. Table 3 implied that the FI, CIRS-G, Comorbidity-D-FI, and ADL-Katz were able to identify a group of patients with a 1-year mortality rate of 50% or higher, in all the patients and the two patient subgroups. Each increment in category or score of 0.1 of the different instruments with respect to frailty, comorbidity, or disability was associated with higher 1-year mortality risk independent of age and gender, in all the patients and the two patient subgroups (Table 4).
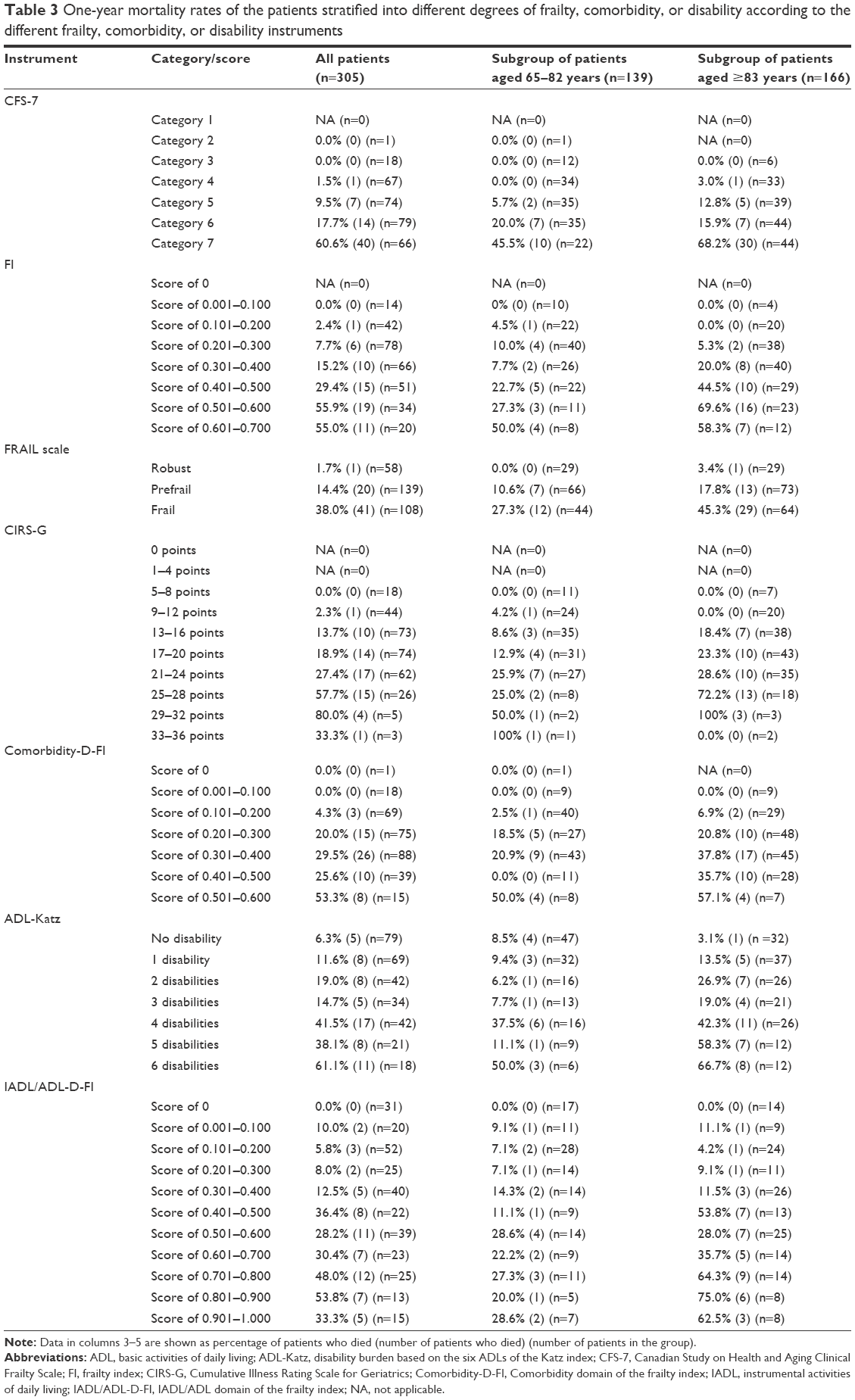 | Table 3 One-year mortality rates of the patients stratified into different degrees of frailty, comorbidity, or disability according to the different frailty, comorbidity, or disability instruments |
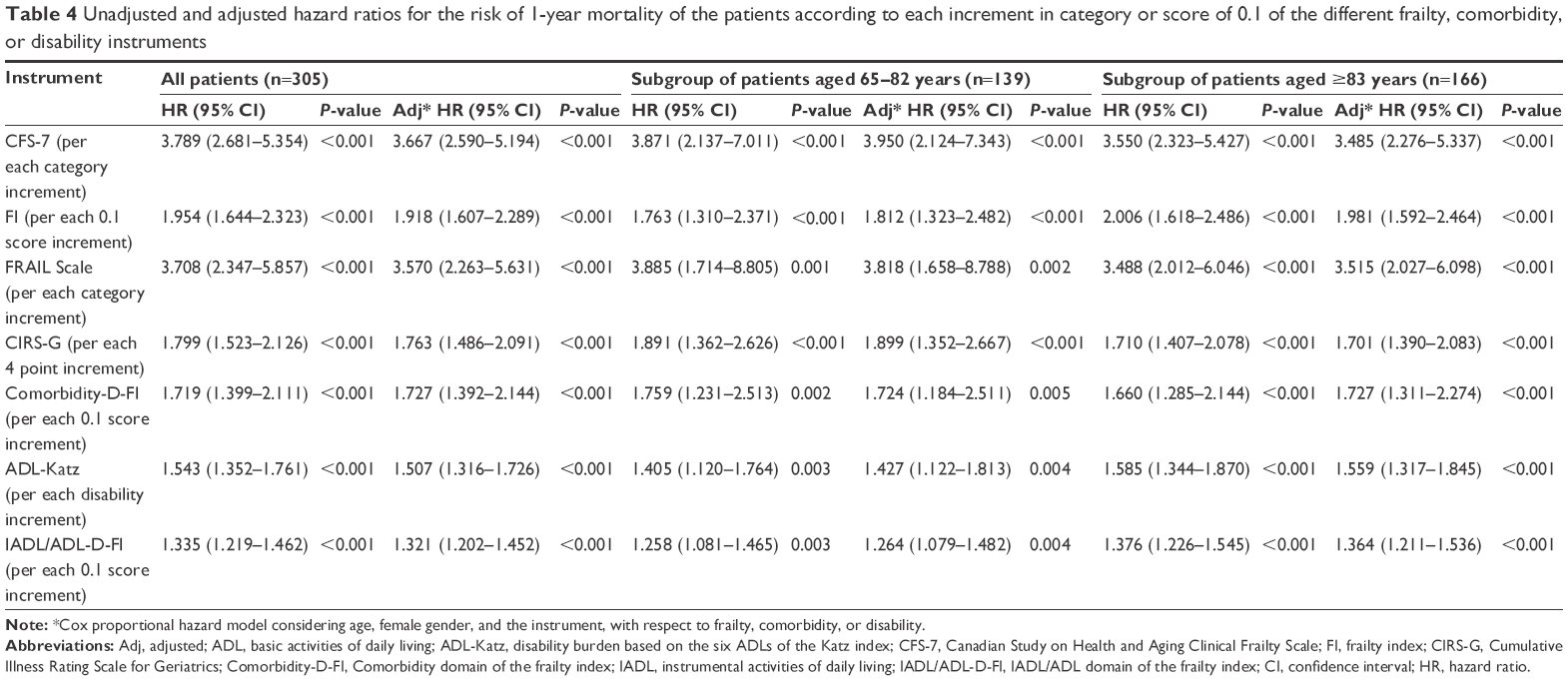 | Table 4 Unadjusted and adjusted hazard ratios for the risk of 1-year mortality of the patients according to each increment in category or score of 0.1 of the different frailty, comorbidity, or disability instruments |
Except for the ADL-Katz in patients aged between 65 and 82 years, all the frailty, comorbidity, or disability instruments revealed a useful discriminative accuracy for 1-year mortality, as indicated by an AUC >0.7 for 1-year mortality, in all the patients and the two patient subgroups (Table 5). The CFS-7 and, in the subgroup of patients aged ≥83 years, also the FI showed superior discriminative accuracy for 1-year mortality compared to the FRAIL scale, CIRS-G, Comorbidity-D-FI, ADL-Katz, and IADL/ADL-D-FI (Table 5). In all the patients, but not in the subgroup of patients aged ≥83 years, the CFS-7 revealed better discriminative accuracy for 1-year mortality compared to the FI (Table 5).
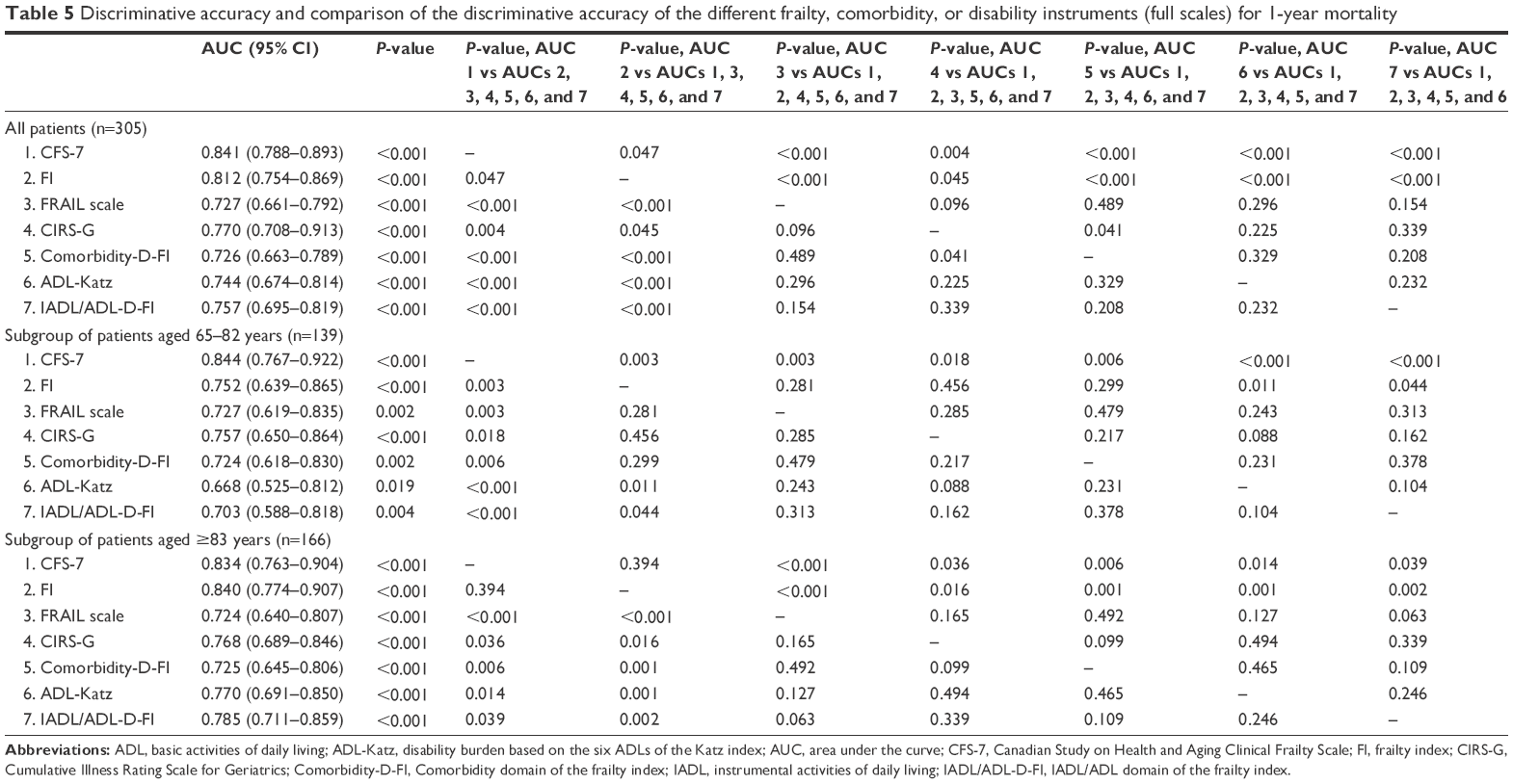 | Table 5 Discriminative accuracy and comparison of the discriminative accuracy of the different frailty, comorbidity, or disability instruments (full scales) for 1-year mortality |
Discussion
We evaluated and compared the ability of major frailty (CFS-7, FI, and FRAIL scale), comorbidity (CIRS-G and Comorbidity-D-FI), or disability instruments (ADL-Katz and IADL/ADL-D-FI) in predicting 1-year mortality in 305 patients hospitalized in geriatric wards. Thereby, we considered different patient age ranges (ie, all the patients, a subgroup of patients aged between 65 and 82 years, and a subgroup of patients aged ≥83 years). Except for the ADL-Katz in the subgroup of patients aged between 65 and 82 years, all the different frailty, comorbidity, or disability instruments revealed at least useful discriminative accuracy for 1-year mortality, as indicated by an AUC >0.7 for 1-year mortality, in all patients and the two patient subgroups. Nevertheless, the ADL-Katz among other aforementioned instruments was able to identify a group of patients with a high 1-year mortality rate, that is, a 1-year mortality rate of 50% or higher, in all patients and the two patient subgroups, as well. Thus, all the aforementioned different frailty, comorbidity, or disability instruments were found to be powerful tools for estimating the 1-year mortality risk.
In addition, we found a dose–response relationship of all the aforementioned frailty, comorbidity, or disability instruments with 1-year mortality that was independent of age and gender. Such a dose-dependent relationship of frailty, comorbidity, or disability instruments with mortality was also found in other studies in older hospitalized patients40,41 and/or older patients who were hospitalized in geriatric wards.25–27,35
Among the different frailty, comorbidity, or disability instruments, the CFS-7 and, in the subgroup of patients aged ≥83 years, also the FI showed superior discriminatory accuracy for 1-year mortality. Both CFS-7 and FI are the tools that allow for the evaluation of patients in relation to the larger construct of frailty.4,5 They consider disability and comorbidity directly or indirectly. Data from previous studies in hospitalized patients and people living in the community indicate that comorbidity and disability impact mortality additively or synergistically in older people.7,42,43 A synergistic interaction between comorbidity and disability on mortality during a median follow-up period of 10.9 years was previously found in a cohort of 12,804 acutely disabled patients with a mean age of 73±12 years who were admitted for inpatient rehabilitation in Singapore rehabilitation community hospitals.7 An additive prognostic effect of comorbidity and ADL disability according to the Katz index on mortality over a follow-up period of 2.8 years was detected in 1,099 older people aged 77–100 years who were living in the community and institutions.42 A combined effect of multi-morbidity and disability on 4-year mortality was found in 364 patients aged ≥80 years who were living in the community in the Aging and Longevity Study in the Sirente geographic area.43 The findings of the present study indicate that such an additive or synergistic effect of comorbidity and disability also holds true in patients hospitalized in geriatric wards. In addition, both CFS-7 and FI, in contrast to the FRAIL scale and other instruments that allow for the evaluation of patients in relation to physical frailty, such as the Fried and Walston frailty phenotype16,44 or the Study of Osteoporotic Fractures Frailty index,17 allow for a fine grading of frailty. This more differentiated grading of frailty severity might explain the superiority of the CFS-7 and, in the subgroup of patients aged ≥83 years, also the FI compared to the FRAIL scale in predicting 1-year mortality in the cohort of this study.
When applying a tool for risk stratification in a hospital setting, aspects such as time and/or skills needed for the application of the instrument and health care costs may be of relevance. In light of the findings of this study, we think that it is important to mention that with respect to the CFS-7, in particular, adequate judgment with respect to the state of a patient being terminally ill, that is, the probability that a patient might die within the next 6 months, needs experience and skills. In addition, with respect to the FI, the evaluation of patients in relation to a large list of potential health deficits may be time consuming. Similarly, the evaluation of patients in relation to the CIRS-G is complex, which needs some training and is also time consuming.
This study has some major strengths. This is the first study that has evaluated and compared different frailty, comorbidity, and disability instruments, together and in parallel, as predictors of mortality in a cohort of hospitalized patients from geriatric wards. Moreover, we considered different age ranges of patients being hospitalized in the geriatric wards. In addition, this study considered different major measures of frailty capturing two (ie, the CFS-7 and the FI) in terms of the larger construct of frailty,4,5 and one (ie, the FRAIL scale) in terms of the construct of physical frailty,4 and major measures of comorbidity and disability. The CFS-7,5,45,46 FI,5,9,10 and FRAIL scale15,47,48 have been repeatedly and very well validated as powerful predictors of mortality in older people. However, so far, no study has considered a comparative analysis of the accuracy of these three aforementioned frailty instruments, together and in parallel, in predicting mortality in older hospitalized patients. Among comorbidity instruments, the CIRS-G and, with respect to disability instruments, disability in ADLs that construct the Katz index have been found to be powerful predictors of mortality in previous comparative studies in older people.49–51 The CIRS-G and the Geriatric Index of Comorbidity revealed the largest coefficient of determination for 1-year mortality among six comorbidity indexes including the CIRS-G, the Charlson Comorbidity Index, Index of Coexistent Diseases, Kaplan, Geriatric Index of Comorbidity, and Chronic Disease Score in 444 older patients (mean age of 85 years) discharged from an acute geriatric hospital in Switzerland.49 The CIRS-G and the Charlson Comorbidity Index revealed a good and comparable ability to predict 3-month mortality in a cohort of older individuals.50 ADL disability in the items of the Katz index was at least as powerful in predicting 360-day mortality as ADL disability based on the Barthel index in 86 centenarians (102±1 years old).51 ADL disability according to the Katz index had the highest impact on mortality during a mean follow-up period of 2.8 years, among other parameters, in 1,099 older Swedish persons with an age of 77–100 years from the Kungsholmen Project.42
This study has some limitations. The study cohort included only hospitalized patients from geriatric wards. As was the case in other studies of hospitalized patients in geriatric wards,12,25,26,52 in the present study, a large proportion of patients were frail and suffered from multiple diseases and disabilities. Consequently, extrapolation of the findings of the current study to other patient groups or settings may be misleading. This analysis was a single-center study. The clinical profile of the patients treated and cared for at geriatric wards might be unequal among individual hospitals due to different characteristics and focuses on single hospitals. In this study, we did not use any special inclusion or exclusion criteria (except for patients aged ≥65 years [as an inclusion criterion] and the inability to give written, informed consent or non-availability of a legal guardian to give written informed consent on behalf of the study participant [as exclusion criteria]). Thus, the cohort of this study includes all inpatients admitted to geriatric wards of a general hospital. Several different instruments for evaluating frailty, comorbidity, or disability have been developed.4,5,20,22,23,49–51,53 It might be misleading to compare our findings with those obtained using other instruments than were applied in the study presented here for assessing frailty, comorbidity, or disability.
Conclusion
All frailty, comorbidity, or disability instruments evaluated in this study emerged as powerful tools for risk stratification of hospitalized patients on geriatric wards in relation to 1-year mortality risk across different patient age ranges. Thereby, among the different instruments, the CFS-7 and, in the subgroup of patients aged ≥83 years, also the FI were found to reveal superior discriminative accuracy for 1-year mortality.
Acknowledgments
This study was supported by grants (financial support enabling the performance of the study) from the Robert Bosch Foundation (a scholarship based on the Research and Study Program on Geriatrics) and the Austrian Society of Geriatrics and Gerontology (Walter Doberauer Scholarship) to MR.
Disclosure
The authors report no conflicts of interest in this work.
References
Arai H, Ouchi Y, Toba K, et al. Japan as the front-runner of super-aged societies: Perspectives from medicine and medical care in Japan. Geriatr Gerontol Int. 2015;15(6):673–687. | ||
Pallin DJ, Espinola JA, Camargo CAJ. US population aging and demand for inpatient services. J Hosp Med. 2014;9(3):193–196. | ||
Fried LP, Ferrucci L, Darer J, Williamson JD, Anderson G. Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci. 2004;59(3):255–263. | ||
Morley JE, Vellas B, van Kan GA, et al. Frailty consensus: a call to action. J Am Med Dir Assoc. 2013;14(6):392–397. | ||
Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;5(173):489–495. | ||
Mitnitski A, Song X, Rockwood K. Assessing biological age: the origin of deficit accumulation. Biogerontology. 2013;14(6):709–717. | ||
Chen C, Sia I, Ma H-M, et al. The synergistic effect of functinoal status and comorbidity burden on mortality: a 16-year survivial analysis. PLoS One. 2014;9(8):e106248. | ||
Mitnitski A, Graham AB, Mogilner AJ, Rockwood K. Frailty, fitness and late-life mortality in relation to chronological and biological age. BMC Geriatr. 2002;27(2):1. | ||
Mitnitski A, Mogilner AJ, Rockwood K. Accumulation of deficits as a proxy measure of ageing. ScientificWorldJournal. 2001;1:323–336. | ||
Rockwood K, Rockwood MRH, Mitnitski A. Physiological redundancy in older adults in relation to the change with age in the slope of a frailty index. J Am Geriatr Soc. 2010;58:318–323. | ||
Searle S, Mitnitski A, Gahbauer EA, Gill TM, Rockwood K. A standard procedure for creating a frailty index. BMC Geriatr. 2008;8:24. | ||
Ritt M, Radi KH, Schwarz C, Bollheimer LC, Sieber CC, Gaβmann KG. A comparison of frailty indexes based on a comprehensive geriatric assessment for the prediction of adverse outcomes. J Nutr Health Aging. 2016;20(7):760–767. | ||
Abellan van Kan G, Rolland Y, Bergman H, Morley JE, Kritchevsky SB, Vellas B. The I.A.N.A. Task Force on frailty assessment of older people in clinical practice. J Nutr Health Aging. 2008;12:29–37. | ||
Abellan van Kan G, Rolland YM, Morley JE, Vellas B. Frailty: toward a clinical definition. J Am Med Dir Assoc. 2008;9:71–72. | ||
Morley JE, Malmstrom TK, Miller DK. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged african americans. J Nutr Health Aging. 2012;16(7):601–608. | ||
Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: Evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56A:M146–M156. | ||
Ensrud KE, Ewing SK, Taylor BC, et al. Comparison of 2 frailty indexes for prediction of falls, disability, fractures, and death in older women. Arch Intern Med. 2008;168(4):382–389. | ||
Linn BS, Linn MW, Gurel L. Cumulative illness rating scale. J Am Geriat Soc. 1968;16:622–626. | ||
Miller MD, Paradis CF, Houck PR, et al. Rating chronic medical illness burden in geropsychiatric practice and research: application of the Cumulative Illness Rating Scale. Psychiatry Res. 1992;41(3):237–248. | ||
Ferraro KF, Wilmoth JM. Measuring morbidity: disease counts, binary variables, and statistical power. J Gerontol B Psychol Sci Soc Sci. 2000;55(3):S173–S189. | ||
Katz S, Down TD, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged: the index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185(12):914–919. | ||
Freedman VA, Aykan H, Wolf DA, Marcotte JE. Disability and home care dynamics among older unmarried Americans. J Gerontol B Psychol Sci Soc Sci. 2004;59(1):S25–S33. | ||
Noel-Miller C. Longitudinal changes in disabled husbands’ and wives’ receipt of care. Gerontologist. 2010;50(5):681–693. | ||
Belga S, Majumdar SR, Kahlon S, et al. Comparing three different measures of frailty in medical inpatients: Multicenter prospective cohor study examining 30-day risk of readmission or death. J Hosp Med. 2016;11(8):556–562. | ||
Pilotto A, Rengo F, Marchionni N, et al. Comparing the prognostic accuracy for all-cause mortality of frailty instruments: a multicentre 1-year follow-up in hospitalized older patients. PLoS One. 2011;7(1):e29090. | ||
Ritt M, Schwarz C, Kronawitter V, et al. Analysis of Rockwood et al‘s Clinical Frailty Scale and Fried et al’s frailty phenotype as predictors of mortality and other clinical outcomes in older patients who were admitted to a geriatric ward. J Nutr Health Aging. 2015;19(10):1043–1048. | ||
Martinez-Velilla N, Cambra-Contin K, Ibanez-Beroiz B. Comorbidity and prognostic indices do not improve the 5-year mortality prediction of components of comprehenisve geriatric assessment in hospitalized older paitents. BMC Geriatr. 2014;14:64. | ||
Formiga F, Ferrer A, Padros G, Montero A, Gimenez-Argente C, Corbella X. Evidence of functinal declining and global comorbidity measured at baseline proved to be the strongest predictors for long-term death in elderly community residents aged 85 years: a 5-year follow-up evaluation, to OCTABAIX study. Clin Interv Aging. 2016;18(11):437–444. | ||
Nakajima H, Yoshioka J, Totsuka N, et al. Activities of daily living as an additional predictor of complications and outcomes in elderly patients with acure myocardial infarction. Clin Interv Aging. 2016;11:1141–1147. | ||
Romero-Ortuno R, Wallis SJ, Biram RW, Keevil V. Clinical frailty adds to acute illness severity in predicting mortality in hospitalized older adults: an observational study. Eur J Intern Med. 2016;35:24–34. | ||
Abizanda P, Romero L, Sanchez-Jurado PM, Martinez-Reig M, Alfonso-Silguero SA, Rodriguez-Manas L. Age, frailty, disability, institutionalization, multimorbidity or comorbidity. Which are the main targets in older adults? J Nutr Health Aging. 2014;18(6):622–627. | ||
Sanchis J, Bonanad C, Ruiz V, et al. Frailty and other geriatric conditions for risk stratification of older patients with acute coronary syndrome. Am Heart J. 2014;168(5):784–791. | ||
Theou O, Rockwood K, Mitnitski A, Rockwood K. Disability and co-morbidity in relation to frailty: how much do they overlap? Arch Gerontol Geriatr. 2012;55(2):e1–e8. | ||
Gu D, Feng Q. Frailty still matters to health and survival in centenarians: the case of China. BMC Geriatr. 2015;15:159. | ||
Ritt M, Bollheimer LC, Sieber CC, Gaβmann KG. Prediction of one-year mortality by five different frailty instruments: a comparative study in hospitalized geriatric patients. Arch Gerontol Geriatr. 2016;66:66–72. | ||
Rockwood K, Mitnitski A. How might deficit accumulation give rise to frailty. J Frailty Aging. 2012;1(1):8–12. | ||
Rockwood K, Silvius JL, Fox RA. Comprehensive geriatric assessment. Helping your elderly patients maintain functional well-being. Postgrad Med. 1998;103(3):247–264. | ||
Swets K. Measuring the accuracy of diagnostic systems. Science. 1988;240:1285–1293. | ||
Hanley JA, McNeil BJ. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology. 1983;148:839–843. | ||
Evans SJ, Sayers M, Mitnitski A, Rockwood K. The risk of adverse outcomes in hospitalized older patients in relation to a frailty index based on a comprehensive geriatric assessment. Age Ageing. 2014;43(1):127–132. | ||
Khandelwal D, Goel A, Kumar U, Gulatj V, Narang R, Dey AB. Frailty is associated with longer hospital stay and increased mortality in hospitalized older patients. J Nutr Health Aging. 2012;16(8):732–735. | ||
Marengoni A, von Strauss E, Rizzuto D, Winblad B, Fratiglioni L. The impact of chronic multimorbidity and disability on functional decline and survival in elderly persons. A community-based, longitudinal study. J Intern Med. 2009;265(2):288–295. | ||
Landi F, Liperoti R, Russo A, et al. Disability, more than multimorbidity, was predictive of mortality among older persons aged 80 years and older. J Clin Epidemiol. 2010;63(7):752–759. | ||
Bieniek J, Wilcznski K, Szewieczek J. Fried frailty phenotype assessment components as applied to geriatric inpatients. Clin Interv Aging. 2016;11:453–459. | ||
Ekerstad N, Swahn E, Janzon M, et al. Frailty is independently assoicated with short-term outcomes for elderly patients with non-ST-segment elevation myocardial infarction. Circulation. 2011;124:2397–2404. | ||
Alfaadhel TA, Soroka SD, Kiberd BA, Landry D, Moorhouse P, Tennankore KK. Frailty and mortality in dialysis: evaluation of a clinical frailty scale. Clin J Am Soc Nephrol. 2015;2015(10):832–840. | ||
Ravindrarajah R, Lee DM, Pye SR, et al. The ability of three different models of frailty to predict all-cause mortality: results from the European Male Aging Study (EMAS). Arch Gerontol Geriatr. 2013;57(3):360–368. | ||
Woo J, Leung J, Morley JE. Comparison of frailty indicators based on clinical phenotype and the multiple deficit approach in predicting mortality and physical limitation. J Am Geriatr Soc. 2012;60:1478–1486. | ||
Zekry D, Loures Valle BH, Graf C, et al. Prospective comparison of 6 comorbidity indices as predictors of 1-year post-hospital discharge institutionalization, readmission, and mortality in elderly individuals. J Am Med Dir Assoc. 2012;13(3):272–278. | ||
Beloosesky Y, Weiss A, Mansur N. Validity of the Medication-based Disease Burden Index compared with the Charlson Comorbidity Index and the Cumulative Illness Rating Scale for Geriatrics: a cohort study. Drugs Aging. 2011;28(12):1007–1014. | ||
Szewieczek J, Francuz T, Dulawa J, et al. Functional measures, inflammatory markers and endothelin-1 as predictors of 360-day survival in centenarians. Age (Dordr). 2015;37(5):85. | ||
Ritt M, Schülein S, Lubrich H, Bollheimer LC, Sieber CC, Gaβmann KG. High-technology based gait assessment in frail people: association between spatio-temporal and three-dimensional gait characteristics with frailty status across four different frailty measures. J Nutr Health Aging. Epub June 2016; doi:10.1007/s12603-016-0764-4. | ||
Verloo H, Goulet C, Morin D, von Gunten A. Association between frialty and delirium in older adult patients discharged from hospital. Clin Interv Aging. 2016;11:55–63. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.