")
Back to Journals » International Journal of General Medicine » Volume 15
Comparing the Efficacy of Articulating Spacers in Two-Stage Revision for Periprosthetic Joint Infection Following Total Knee Arthroplasty: All-Cement Spacers vs Sterilized Replanted Metal-Polyethylene Spacers
Authors Fei Z, Zhang Z, Wang Y, Zhang H, Xiang S
Received 31 December 2021
Accepted for publication 16 March 2022
Published 24 March 2022 Volume 2022:15 Pages 3293—3301
DOI https://doi.org/10.2147/IJGM.S354808
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Zhixuan Fei,1,2 Zian Zhang,1 Yingzhen Wang,1 Haining Zhang,1 Shuai Xiang1
1Department of Joint Surgery, The Affiliated Hospital of Qingdao University, Qingdao, People’s Republic of China; 2Qingdao University, Medical Department, Qingdao, People’s Republic of China
Correspondence: Shuai Xiang, Department of Joint Surgery, The Affiliated Hospital of Qingdao University, Qingdao, People’s Republic of China, Email [email protected]
Purpose: Two-stage revision is the most common treatment for periprosthetic joint infection (PJI) following total knee arthroplasty (TKA). Few studies have compared the clinical efficacy of different articulating spacers. This study compared the outcomes of all-cement articulating spacers and sterilized replanted metal-polyethylene articulating spacers for PJI following TKA.
Patients and Methods: In this retrospective observational study, 47 patients who received two-stage revision for PJI following TKA between 2006 and 2020 in our hospital were included. Patients were categorized as receiving an all-cement articulating spacer or a sterilized replanted metal-polyethylene articulating spacer in exclusion. Data on demographics, surgical information, and outcomes were collected in 2021.
Results: Forty-seven spacers were identified: all-cement spacer was noted in 23 patients and sterilized replanted spacer in 24. Patients in the all-cement spacer group had shorter operation time (155.87 ± 33.12 vs 189.79 ± 51.21 min; P = 0.0102) and less blood loss (845.22 ± 525.92 vs 1114.50 ± 547.81 mL; P = 0.0427) in exclusion. Patients in the sterilized replanted spacer group had superior interval range of motion (ROM; 61.00 ± 31.94° vs 31.75 ± 33.38°; P = 0.0072), postoperative ROM (85.00 ± 11.11° vs 77.37 ± 9.18°; P = 0.0329) as compared to all-cement spacers, but there was no difference in infection control between 2 groups.
Conclusion: The two types of spacers had no difference in the reinfection rate, indicating that both articulating spacers are safe and effective for 2-stage revision. Considering ROM of knee joint, bone loss and cost, sterilized replanted metal-polyethylene spacers are preferred in the treatment of PJI.
Keywords: total knee arthroplasty, periprosthetic joint infection, articulating spacer
Introduction
Periprosthetic joint infection (PJI) following total knee arthroplasty (TKA) has been one of the most serious and challenging complications.1 Dale et al2 reported that the incidence of PJI following TKA ranged from 0.5% to 2.0%. With the population aging, the incidence of TKA is growing rapidly and as a result, the number of PJI cases is also increasing.3 At present, total knee revision (TKR) due to PJI, which is the main reason for the treatment failure, accounts for 16–27% of all the TKR.4–6 It causes great suffering to patients, and also brings huge economic and social burdens.
A variety of methodologies have been developed to treat PJI, including irrigation and debridement, one-stage TKR, and two-stage TKR.7,8 In the two-stage TKR, the infected prosthesis is taken out, and an antibiotic-impregnated spacer is placed after debridement in exclusion (stage 1). When the infection is controlled, the spacer is taken out and new prosthesis was implanted in revision (stage 2). Compared with one-stage TKR, the patients with two-stage TKR undergo two major operations, which prolongs the hospital stay and increases the medical cost. However, the infection indicators can be monitored dynamically after exclusion, and the revision can be carried out when infection is controlled. Therefore, two-stage TKR is recognized as the gold standard for the treatment of PJI following TKA.7,8 At present, two-stage revision is used to treat PJI in most cases, with a success rate higher than 80%.9,10 However, complications such as recurrence of infection and poor joint function still exist after two-stage TKR. In addition, the bone loss caused by two operations increases the utilization rate of cushion block. It reduces the satisfaction of patients and increases the economic burden of patients.9
The type selection of spacer for two-stage TKR is still controversial. The ideal spacer needs to meet the following requirements: (1) the effectiveness and integrity should be ensured before revision; (2) the infection should be effectively controlled; (3) certain joint function should be maintained between exclusion and revision; (4) It is easy to remove and bone loss should be minimized; (5) It is easy to operate and the medical cost is low.
There are many types of spacers in use, which are generally divided into two categories: static spacers and articulating spacers. Static spacer is the first spacer type used. Freeman et al11 reported that static spacers could maintain joint stability and be conducive to the release of antibiotics. Romanò et al12 found that static spacers could brake joints, relief the pain, improve soft tissue healing, and control the infection effectively. On the other hand, immobilization for a long time is easy to cause soft tissue contracture and fibrosis, which leads to joint movement dysfunction, makes it difficult to expose in revision and adversely affects the postoperative function. Hao et al13 reported that static spacers increased the risk of spacer displacement and bone loss between exclusion and revision. In addition, the stress of bone cement on the bone contact surface will also accelerate osteolysis.9
Due to the disadvantages of the static spacers, increasing articulating spacers have been used in clinical practice.14 Articulating spacers are used to retain joint function, control infection effectively, and improve the quality of life and satisfaction in the interval from exclusion and revision. A study by Romanò et al12 found that preserving the effective range of motion (ROM) of the knee could reduce the contracture and fibrosis of the quadriceps femoris and bone loss. Voleti et al15 reported that there was no significant difference in the infection control between static spacers and articulating spacers.
The common type of articulating spacers includes all-cement spacers and sterilized replanted metal-polyethylene spacers.12,16,17 Spivey et al18 found that there was no significant difference in the infection control, postoperative complications and functional score after revision for different articulating spacers. Although all-cement spacers are easy to make, they are difficult to obtain an ideal joint matching, which will increase the friction in the knee joint, and have a high possibility of spacer breakage and displacement, and the debris produced due to the friction may accelerate the osteolysis.19
At present, few studies have compared the clinical efficacy of all-cement spacers and sterilized replanted metal-polyethylene spacers (sterilized replanted spacers). This study aimed to investigate the indexes in exclusion, in revision, and outcomes in patients receiving all-cement spacers or sterilized replanted metal-polyethylene spacers.
Materials and Methods
This was an retrospective study aiming to examine two types of articulating spacers placed for PJI in patients who received surgeon in our hospital between 2006 and 2020. The patients were divided into the all-cement spacer group (n=23) and the sterilized replanted spacer group (n=24) according to the type of spacer in exclusion. Patients were followed up for at least 1 year. This study has been approved by the Ethics Committee of the Affiliated Hospital of Qingdao University (No: QYFY WZLL 26744). Informed consent was obtained from each participant. This study was conducted following the Declaration of Helsinki. The inclusion and exclusion criteria were as follows:
Inclusion criteria: Patients suffered periprosthetic joint infection after TKA and underwent two-stage revision.
Exclusion criteria: Patients underwent irrigation and debridement, or one-stage TKR; patients who underwent two-stage revision for other reason, just like trauma.
Diagnostic Criteria for Infection
The diagnostic criteria of infection used in this study were as follows:20 There is a sinus communicating with the prosthesis; more than two groups of intra-articular tissues are subjected to bacterial culture and positive result is present; or a group of intra-articular tissues is subjected to bacterial culture and positive result is present, and there are following findings: 1) C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) increase; 2) white blood cell (WBC) count and neutrophil count increase; 3) a large amount of pus forms in the joint. The diagnostic criteria for infection control were as follows: the surrounding soft tissues heal well without pain, fever and other symptoms; the WBC count, ESR and CRP are normal in three consecutive laboratory tests. Failure of infection control was defined as follows: the need for further Surgery on the ipsilateral knee for septic reasons within 1 year of reimplantation.
Treatment Process and Spacer Production
In exclusion, knee joint was exposed along the original surgical incision, and 30-mL articular fluid was reserved. Six groups of soft tissues were randomly taken from the medial, lateral and suprapatellar capsule of the knee joint for bacterial culture and pathological examination. The femoral and tibial prosthesis was taken out.
Sterilized replanted spacer group: the femoral prosthesis and polyethylene gasket were clean thoroughly, and then soaked in 1% iodophor for 10 min. Then, they were put into a sterile package for high temperature and high pressure sterilization. The residual bone cement, abnormal synovium and necrotic tissues were removed completely. The knee joint was rinsed repeatedly with 200 mL of 2% hydrogen peroxide, 300 mL of 1% iodophor and 1000 mL of normal saline 3 times. According to the preoperative culture results, sensitive antibiotics (1 g of vancomycin or 1 g of meropenem or 200 mg of amphotericin B) with 40 g of bone cement were added on the back of the sterilized femoral prosthesis and the bone surface of the tibial plateau during the dough stage, and 1-cm bone cement column was retained in the tibia intramedullary cavity. The sterilized gasket and femoral prosthesis were placed on the bone surface of femur and tibia without compression when the bone cement was about to heat up. The bone defect was filled with bone cement. The articular cavity and subcutaneous tissues were washed with 2% hydrogen peroxide, 1% iodophor and normal saline after the bone cement was solidified. The drainage tube was placed and the wound was closed.
All-cement spacer group: the sterilized gasket and femoral prosthesis were replaced with all-cement spacer. Other surgical operations were the same to those in the sterilized replanted spacer group.
Postoperative Treatment
Sensitive antibiotics were applied intravenously for 6 weeks according to the culture results. The antibiotic treatment should be discontinued 2 weeks before revision. The WBC count, neutrophil count, ESR and CRP were monitored during this period. Revision can be carried out after 3 consecutive tests showed normal results.
Patients could take adequate exercise between exclusion and revision. Patients were asked to do straight leg lifting 50 times and passive ROM training on the first day after operation. Active ROM training was performed two weeks after operation.
The drainage tube was removed on the first or second day after operation according to volume of drainage. After the surgeon’s judgement, patients were asked to perform bedside activities, but weight-bearing exercise was not allowed.
Statistical Method
Blood loss was calculated as follow according to previously reported: blood loss = [(preoperative HCT - HCT on the second day after operation)/preoperative HCT] × weight × 7% × 1000 + intraoperative blood transfusion.21 Restricted flexion function is defined as the inability to reach 90° when the knee is flexed (a goniometer is used for measurement). In brief, the patient is asked to lay in a supine position; the fixed arm of the goniometer was parallel to the midline of the femur, the moving arm was parallel to the midline of the tibia, and the axis was located outside the center of the knee joint for measurement.
The categorical data between groups were analyzed by using Chi-square test or Fisher’s exact test, while the Student’s t-test and the Mann–Whitney U-test were used to analyze the quantitative data. GraphPad Prism 8 was employed for the statistical analysis. A value of P less than 0.05 was considered statistically significant. The data are expressed as mean ± standard deviation or (minimum, maximum).
Results
In the present study, a total of 47 patients who received exclusion at our center between 2006 and 2020. Of them, 23 patients (including 9 males and 14 females) were treated with all-cement spacers. Of note, 3 patients did not undergo revision (stage 2) by the time of follow-up, and remaining 20 patients underwent two-stage TKR at our center. During the follow-up, 1 patient was lost to follow up. 24 patients (including 10 males and 14 females) were treated with sterilized replanted spacers. Of note, 4 patients did not undergo revision (stage 2) by the time of follow-up, and remaining 20 patients underwent two-stage TKR at our center. During the follow-up, 4 were lost to follow up. In addition, there were no significant differences in the age, gender and duration of follow-up between two groups (Table 1).
 |
Table 1 Basic Information |
In the all-cement spacer group, the bacterial culture during exclusion showed Staphylococcus infection in 12 cases (including Staphylococcus epidermidis in 7, Staphylococcus aureus in 4, and Pseudointermediate Staphylococcus in 1), Escherichia coli infection in 2, Streptococcus infection in 1, Nontuberculous Mycobacterium in 1, Acinetobacter baumannii in 1, Pseudomonas aeruginosa in 1, Corynebacterium pseudodiphtheria in 1, and Candida glabrata in 1. In addition, bacterial culture showed negative in 3 cases. In the sterilized replanted spacer group, the bacterial culture during exclusion showed Staphylococcus in 14 patients, (including Staphylococcus epidermidis in 8, Staphylococcus aureus in 3, Coagulase-negative-Staphylococcus in 2 and hemolytic Staphylococcus in 1), Aeromonas hydrophila in 1, Corynebacterium in 1, Pseudomonas aeruginosa in 1, Streptococcus in 1, and Candida glabrata in 1. In addition, bacterial culture showed negative in 5 cases (Table 2).
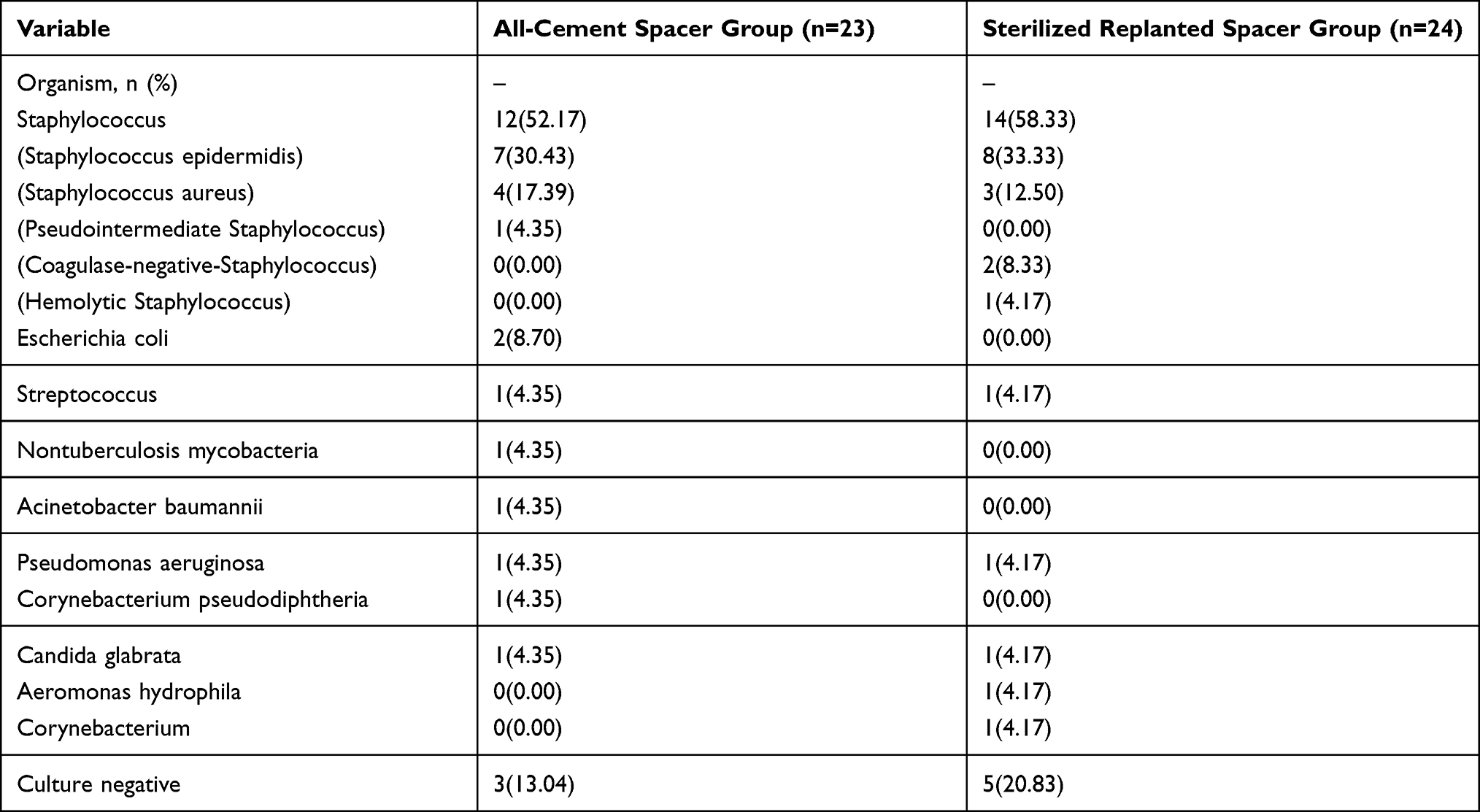 |
Table 2 Bacterial Culture in Exclusion |
Before exclusion, the ROM of knee joint and results from blood examinations were comparable between two groups. Patients in the sterilized replanted spacer group had higher hemoglobin (Hb; 108.57±14.60 g/L vs 122.71±10.17 g/L, P = 0.0004). The operation time in the sterilized replanted spacer group was longer (155.87±33.12 min vs 189.79±51.21 min, P = 0.0102), and patients in the sterilized replanted spacer group had more blood loss (845.22±525.92 mL vs 1114.50±547.81 mL, P = 0.0427). In addition, 3 patients in the all-cement spacer group and 4 patients in the sterilized replanted spacer group received blood transfusion in exclusion or after exclusion, and there was no significant difference in the blood loss within two days after exclusion between two groups (Table 3).
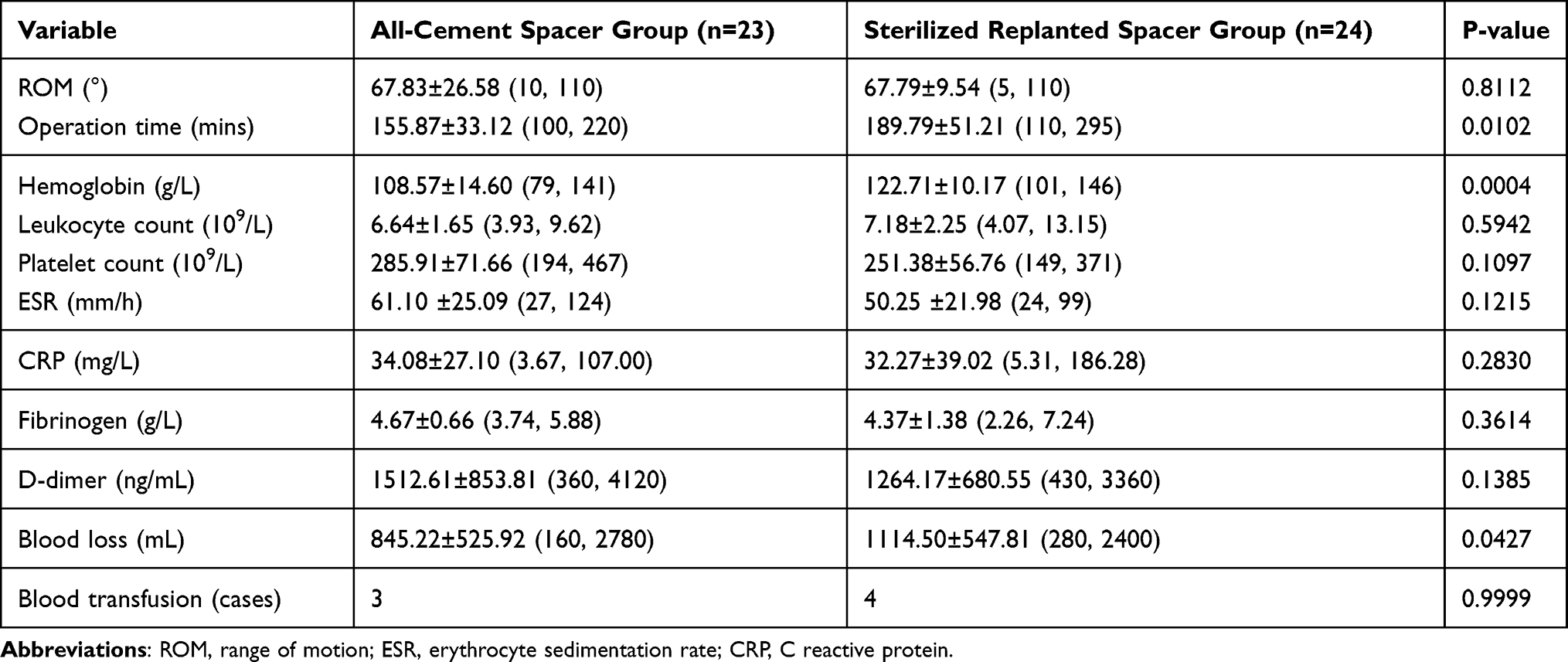 |
Table 3 Exclusion Information |
Before revision, patients in the sterilized replanted spacer group had better ROM of knee joint (31.75±33.38° vs 61.00±31.94°, P = 0.0072), and had longer operation interval (3.61±2.03 months vs 6.41±4.56 months, P =0.0069). Patients in the all-cement spacer group had higher D-dimer (1536.50±658.09 ng/mL vs 719.00±355.20 ng/mL, P = 0.0001), but there were no marked differences in the remaining findings from blood examinations.
In revision, the operation time and dose of bone cement were comparable between two groups. Due to bone loss, augments were used in 14 patients in the all-cement spacer group, and hinged knee prosthesis for revision was used in 1 patient. The rate of use of augments and high restrictive prosthesis was 75.00%. The augments were applied in only 6 patients in the sterilized replanted spacer group in revision. The rate of use of augments was 30.00%. Moreover, 7 patients in the all-cement spacer group and 6 patients in the sterilized replanted spacer group received blood transfusion in revision or after revision, and the blood loss within two days after revision was similar between two groups.
In the all-cement spacer group, intraoperative bacterial culture still showed positive in 1 patient. The pathogenic microorganism was Candida albicans, which was inconsistent with that found in exclusion (non tuberculous Mycobacterium). One patient was admitted again for knee swelling and pain after revision, which were relieved after conservative treatment.
In the sterilized replanted spacer group, intraoperative bacterial culture still showed positive in 2 patients. The pathogenic microorganism of one patient was Trichophyton rubrum, which was inconsistent with that found in exclusion (Staphylococcus epidermidis). And the pathogenic microorganism of the other patient was Hemolytic Staphylococcus, which was consistent with that found in exclusion. One patient was admitted again due to the dislocation of cushion block, which was resolved after reoperation (Table 4).
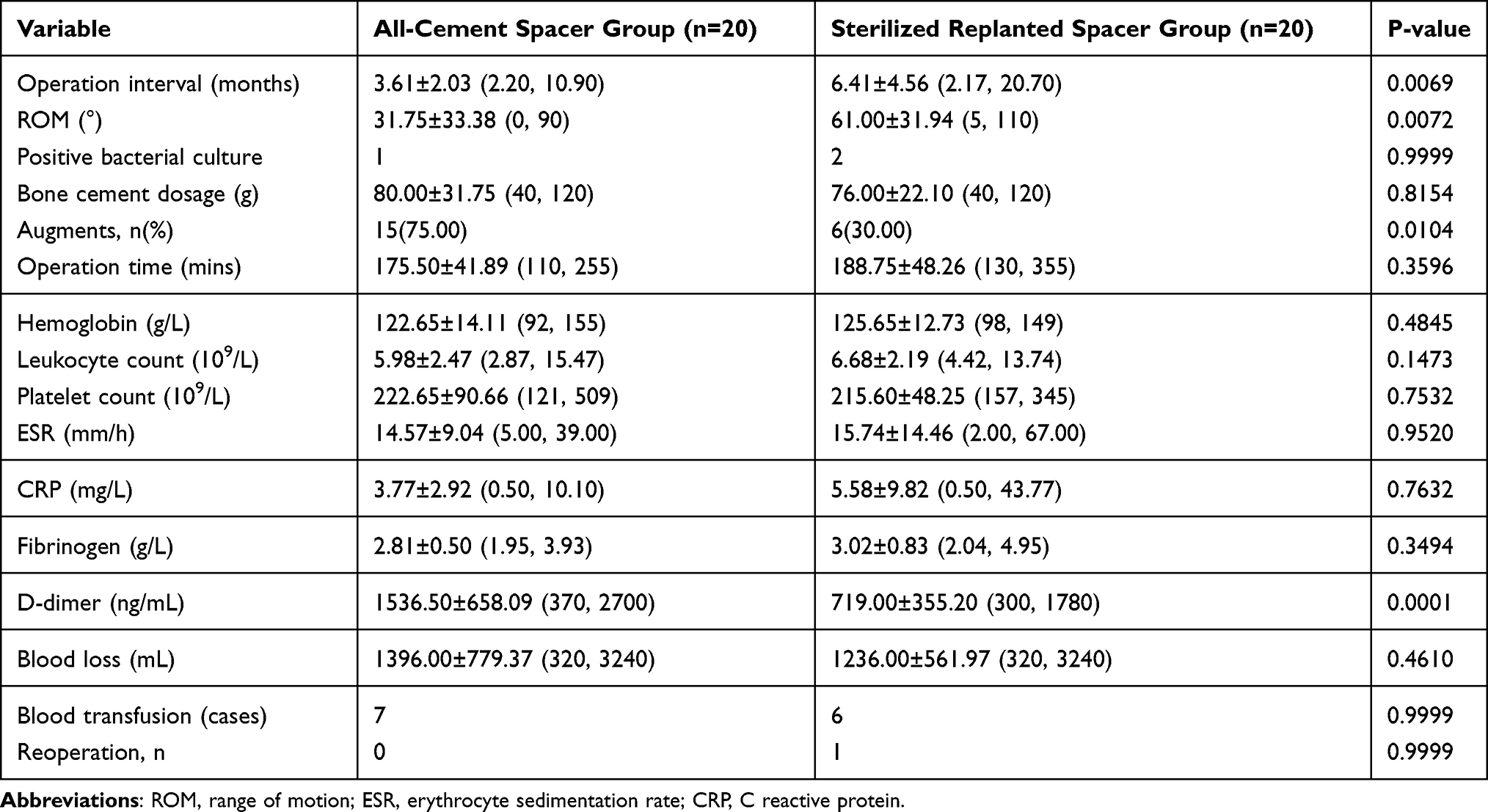 |
Table 4 Revision Information |
During the follow-up, patients in the sterilized replanted spacer group had better ROM of knee joint (77.37±9.18° vs 85.00±11.11°, P = 0.0329). The flexion contracture, Knee Society Score (KSS), Knee Society Functional Score (KSFS) and postoperative satisfaction were comparable between two groups. In addition, 4 of 19 patients in the all-cement spacer group reported evident pain when walking, and 3 of 16 patients in the sterilized replanted spacer group reported evidence pain when walking (Table 5).
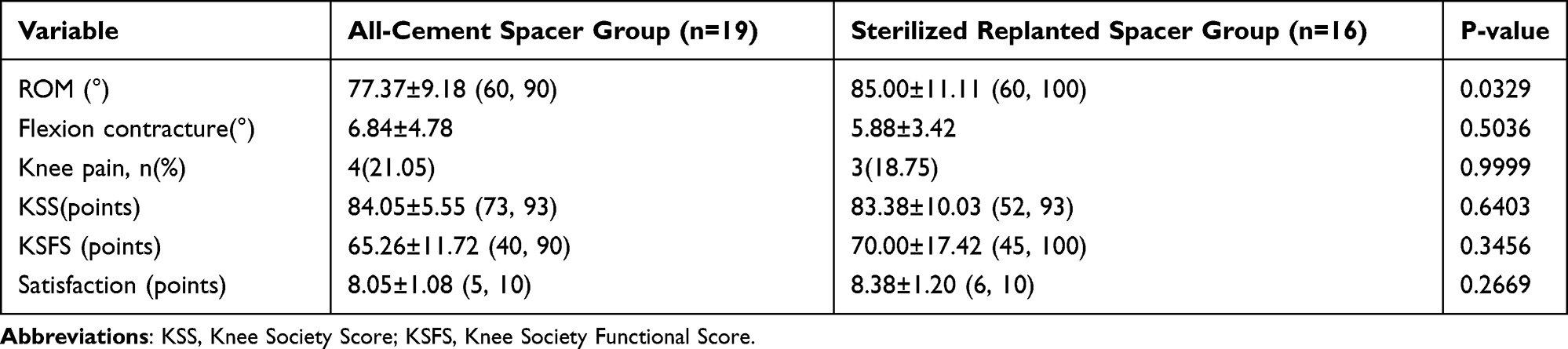 |
Table 5 Follow-Up Information |
Discussion
In the present retrospective observational analysis, the outcomes of patients receiving sterilized replanted spacer were compared with those receiving all-cement spacer for the treatment of knee PJI following TKA. Our results showed that patients who received sterilized replanted spacers had superior interval ROM and postoperative ROM as compared to those undergoing all-cement spacers, but there was no difference in the infection control between 2 groups.
It has been reported that PJI is the main cause of treatment failure and accounts for 16–27% of all the TKR.4–6 In our study, 52.17% and 58.33% of patients in two groups were infected with Staphylococcus, which was consistent with the findings reported by Flurin et al.22 The Staphylococcus infection might be ascribed to the incision surface contamination and low resistance. The bacterial culture showed negative in 3 patients of the all-cement spacer group, and 5 of the sterilized replanted spacer group, which might be related to factors such as preoperative antibiotics and specimen sampling error.
In the exclusion, no significant differences were observed in the preoperative ROM, WBC, ESR and other parameter between 2 groups. Patients in the all-cement spacers group had significantly shorter operation time and less blood loss, which was related to the time for prosthesis disinfection during exclusion in sterilized replanted spacer group. However, patients in the sterilized replanted spacer group had higher Hb, which was ascribed to the limitation of retrospective study.
In addition, patients in the sterilized replanted spacers had superior ROM and longer operation interval in revision, which may be related to that the sterilized replanted prosthesis and gasket can obtain a good joint matching degree, allowing the knee joint to achieve greater ROM. A wide ROM for joint activities can also reduce soft tissue contracture around the knee joint and improve the quality of life during the operation interval. In the all-cement spacers group, the rate of use of augments was significantly higher. The artificially all-cement spacer might cause friction and adversely affect the knee joint during movement, resulting in osteolysis and serious bone defects in revision, and thus filling with augments is needed. In addition, the D-dimer was higher in the all-cement spacers group, which might be related to limitations of retrospective study and sample size. There was no difference in other parameters between two groups in revision.
In the follow-up period, although the ROM was better in the sterilized replanted spacers group, there was no marked difference in the flexion contracture, incidence of complications, KSS, KSFS, and satisfaction between 2 groups. Taken together, our results showed the sterilized femoral prosthesis and gasket could preserve ROM during the operation interval, and improve the quality of life. Moreover, this method reduced the incidence of soft tissue contractures and bone loss, decreased the use of augments and high-restriction prostheses, and reduced the medical cost.
However, the use of sterilized replanted spacers is also controversial. At present, the most common concern is whether there is bacterial biofilms on the prosthesis after autoclaving, which may cause recurrence of infection and treatment failure. Steven et al6 observed the autoclaved femoral prosthesis under an electron microscope and found that autoclaving effectively removed the bacteria on the surface of cobalt-chromium alloy, and the alloy could be used safely as a spacer. Choi et al17 used sterilized replanted spacers to treat PJI, and they found that there was no significant difference from other types of spacers in terms of infection control rate and postoperative functional scores. In the present study, the spacer was composed of femoral prosthesis and gasket, and the rates of infection control, satisfaction and functional score were similar to previously reported.18
In addition, postoperative complications are also an important concern for articulating spacers. Struelens et al23 reported that the complication rate of articulating spacers was as high as 57%, mainly including prosthesis tilt and displacement. Arian et al24 speculated that, if the articulating prosthesis appeared subluxation, the use of restrictive prosthesis would increase in revision. Lanting et al25 reported that the complications of spacers in operation interval would significantly affect the joint function. In our study, none had prosthetic tilt or displacement in operation interval in both groups, and the main complications were restricted flexion function and knee pain. In order to reduce the complications, the selection of spacer types is important. Currently, there is no consensus on the indications for the spacer selection.
There were still limitations in the present study. This was a retrospective study, which had low evidence level of and was prone to selection bias. Although there was no significant differences in the functional improvement and infection control in patients infected by different strains, there was no etiological basis to prove that such methods were equally effective in patients infected by different bacterial strains. In addition, there is no etiological research on the interval between exclusion and revision. In addition, although the infection control rate in the sterilized replanted spacers group of our study was similar to previously reported, infection control was related to many factors, such as debridement, antibiotic use, and others. We could not attribute the infection control to the use of spacers alone. Moreover, the results might be biased due to the individualized treatment. In the further, more randomized, controlled studies with large sample size and long term follow up are needed to confirm our findings.
Conclusions
Our study show patients receiving sterilized replanted spacers have superior interval ROM, postoperative ROM and less restricted flexion function as compared to those treated with all-cement spacers, which may be ascribed to the improved quality of life in operation interval. Moreover, the use of sterilized replanted spacers can effectively reduce bone loss, leading to low use rate of augments, which reduces the medical cost. In addition, there is no difference in the infection control between 2 groups. Thus, the sterilized replanted Metal-Polyethylene spacers are preferred in the treatment of PJI.
Abbreviations
PJI, periprosthetic joint infection; TKA, total knee arthroplasty; TKR, total knee revision; CRP, C reactive protein; ESR, erythrocyte sedimentation rate; WBC, white blood cell; HCT, red blood cell specific volume; ROM, range of motion; KSS, Knee Society Score; KSFS, Knee Society Functional Score.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Klinder A, Zaatreh S, Ellenrieder M, et al. Antibiotics release from cement spacers used for two‐stage treatment of implant‐associated infections after total joint arthroplasty. J Biomed Mater Res B Appl Biomater. 2019;107(5):1587–1597. doi:10.1002/jbm.b.34251
2. Dale H, Fenstad AM, Hallan G, et al.Increasing risk of prosthetic joint infection after total hip arthroplasty. Acta Orthopaedica. 2012;83(5):449–458.
3. Hanssen AD. Evaluation and treatment of infection at the site of a total hip or knee arthroplasty. Instr Course Lect. 1999;48:111–112.
4. Sharkey PF, Lichstein PM, Shen C, Tokarski AT, Parvizi J. Why are total knee arthroplasties failing today–has anything changed after 10 years? J Arthroplasty. 2014;29(9):1774–1748.
5. Schroer WC, Berend KR, Lombardi AV, et al. Why are total knees failing today? Etiology of total knee revision in 2010 and 2011. J Arthroplasty. 2013;28(8):116–119. doi:10.1016/j.arth.2013.04.056
6. Kurtz SM, Lau E, Watson H, et al. Economic burden of periprosthetic joint infection in the United States. J Arthroplasty. 2012;27(8):61–65.e1. doi:10.1016/j.arth.2012.02.022
7. Zimmerli W, Trampuz A, Ochsner PE. Prosthetic-joint infections. N Engl J Med. 2004;351(16):1645–1654. doi:10.1056/NEJMra040181
8. Kunutsor SK, Whitehouse MR, Lenguerrand E, Blom AW, Beswick AD; INFORM Team. Re-infection outcomes following one- and two-stage surgical revision of infected knee prosthesis: a systematic review and meta-analysis. PLoS One. 2016;11(3):e0151537.
9. Warth LC, Hadley CJ, Grossman EL. Two-stage treatment for total knee arthroplasty infection utilizing an articulating prefabricated antibiotic spacer. J Arthroplasty. 2020;35(3S):S57–S62.
10. Andrzej K, Mustafa C, Armin ST, et al. Success rates for initial eradication of peri-prosthetic knee infection treated with a two-stage procedure. Ortop Traumatol Rehabil. 2014;16(1):11–16.
11. Freeman MG, Fehring TK, Odum SM, et al. Functional advantage of articulating versus static spacers in 2-stage revision for total knee arthroplasty infection. J Arthroplasty. 2007;22(8):1116–1121. doi:10.1016/j.arth.2007.04.009
12. Romanò CL, Gala L, Logoluso N, et al. Two-stage revision of septic knee prosthesis with articulating knee spacers yields better infection eradication rate than one-stage or two-stage revision with static spacers. Knee Surg Sports Traumatol Arthroscopy. 2012;20(12):2445–2453. doi:10.1007/s00167-012-1885-x
13. Hao S, Xianlong Z, Yao J, et al. Intraoperatively-made cement-on-cement antibiotic-loaded articulating spacer for infected total knee arthroplasty. Knee. 2010;17(6):407–411.
14. Pivec R, Naziri Q, Issa K, Banerjee S, Mont MA. Systematic review comparing static and articulating spacers used for revision of infected total knee arthroplasty. J Arthroplasty. 2014;29(3):553–7.e1. doi:10.1016/j.arth.2013.07.041
15. Voleti PB, Baldwin KD, Lee GC. Use of static or articulating spacers for infection following total knee arthroplasty: a systematic literature review. J Bone Joint Surg Am. 2013;95(17):1594–1599. doi:10.2106/JBJS.L.01461
16. Hofmann AA, Kane KR, Tkach TK, Plaster RL, Camargo MP. Treatment of infected total knee arthroplasty using an articulating spacer. Clin Orthop Relat Res. 1995;430(321):45–54.
17. Choi H-R, Malchau H, Bedair H. Are prosthetic spacers safe to use in 2-stage treatment for infected total knee arthroplasty? J Arthroplasty. 2012;27(8):1474–1479.e1. doi:10.1016/j.arth.2012.02.023
18. Spivey JC, Guild GN, Scuderi GR. Use of articulating spacer technique in revision total knee arthroplasty complicated by sepsis: a systematic meta-analysis. Orthopedics. 2017;40(4):212–220. doi:10.3928/01477447-20170208-06
19. Duncan CP, Beauchamp C. A temporary antibiotic-loaded joint replacement system for management of complex infections involving the hip. Orthop Clin North Am. 1993;24(4):751–759.
20. Javad P, Thorsten G. Definition of periprosthetic joint infection. J Arthroplasty. 2014;29(7):1331.
21. Ke C, Tian N, Zhang X, Chen M. Changes in perioperative hemoglobin and hematocrit in patients undergoing total knee arthroplasty: a prospective observational study of optimal timing of measurement. J Int Med Res. 2020;48(11):0300060520969303.
22. Flurin L, Greenwood-Quaintance KE, Patel R. Microbiology of polymicrobial prosthetic joint infection. Diagn Microbiol Infect Dis. 2019;94(3):255–259.
23. Bernard S, Steven C, Johan B. Spacer-related problems in two-stage revision knee arthroplasty. Acta Orthop Belg. 2013;79(4):422–426.
24. Lau AC, Howard JL, Macdonald SJ, Teeter MG, Lanting BA. The effect of subluxation of articulating antibiotic spacers on bone defects and degree of constraint in revision knee arthroplasty. J Arthroplasty. 2016;31(1):199–203.
25. Lanting BA, Lau A, Teeter MG, Howard JL. Outcome following subluxation of mobile articulating spacers in two-stage revision total knee arthroplasty. Arch Orthop Trauma Surg. 2017;137(3):375–380. doi:10.1007/s00402-017-2630-1
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.