")
Back to Journals » Journal of Blood Medicine » Volume 13
Comorbidities, Health-Related Quality of Life, Health-care Utilization in Older Persons with Hemophilia—Hematology Utilization Group Study Part VII (HUGS VII)
Authors Curtis R , Manco-Johnson M, Konkle BA , Kulkarni R , Wu J , Baker JR , Ullman M , Tran DQ Jr , Nichol MB
Received 17 December 2021
Accepted for publication 11 April 2022
Published 9 May 2022 Volume 2022:13 Pages 229—241
DOI https://doi.org/10.2147/JBM.S354526
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Randall Curtis,1 Marilyn Manco-Johnson,2 Barbara A Konkle,3 Roshni Kulkarni,4 Joanne Wu,5 Judith R Baker,6 Megan Ullman,7 Duc Quang Tran Jr,8 Michael B Nichol5
1Factor VIII Computing, Berkeley, CA, USA; 2Hemophilia and Thrombosis Center, University of Colorado Anschutz Medical Campus, Aurora, CO, USA; 3Washington Center for Bleeding Disorders, BloodWorks Northwest and the University of Washington, Seattle, WA, USA; 4MSU Center of Bleeding and Clotting Disorders, Department Pediatrics and Human Development, Michigan State University, East Lansing, MI, USA; 5Sol Price School of Public Policy, University of Southern California, Los Angeles, CA, USA; 6Public Health Department, The Center for Comprehensive Care & Diagnosis of Inherited Blood Disorders, Orange, CA, USA; 7Department of Pediatrics, Gulf States Hemophilia & Thrombophilia Center, University of Texas Health Science Center at Houston, Houston, TX, USA; 8Department of Hematology and Medical Oncology, Hemophilia of Georgia Center for Bleeding & Clotting Disorders of Emory, Emory University School of Medicine, Atlanta, GA, USA
Correspondence: Michael B Nichol, Sol Price School of Public Policy University of Southern California, 650 Childs Way, RGL 212, Los Angeles, CA, 90089, USA, Tel +1 213 740 2355, Fax +1 213 740 3460, Email [email protected]
Purpose: We compare the impact of hemophilia on comorbidities, joint problems, health-related quality of life (HRQoL) and health-care utilization between two age groups: 40– 49 years and ≥ 50 years.
Patients and Methods: The HUGS VII study recruited persons with hemophilia A or B age ≥ 40 years. Participants completed surveys to collect data on sociodemographic and clinical characteristics, hemophilia treatment regimen, pain, joint problems, comorbidities, HRQoL, depression and anxiety, at baseline and 6-months later. Clinical chart reviews documented hemophilic severity and treatment.
Results: The sample includes 69 males, 65.2% aged ≥ 50 years, 75.4% with hemophilia A. Individuals ≥ 50 years were more likely to have mild or moderate hemophilia (68.9% vs 41.7%, P = 0.03) than those 40– 49 years old. Among persons with mild/moderate hemophilia, those ≥ 50 years old reported a higher rate of joint pain (83.9% vs 70.0%, P = 0.34 at baseline, 91.3% vs 57.1%, P = 0.06 at follow up) or range of motion limitation (73.3% vs 60.0%, P = 0.43 at baseline, 73.9% vs 28.6%, P = 0.04 at follow up) than the younger group. Compared to the younger group, the older group reported fewer emergency room visits (4.5% vs 21.7%, P = 0.03), and physical therapy visits (15.9% vs 43.5%, P = 0.01) at baseline. The sample depression rate was 85.7%, but the differences among the age groups were not significant. The mean covariate-adjusted EQ-5D index score was lower in older persons (0.77 vs 0.89, P = 0.02).
Conclusion: Older persons with hemophilia in this sample are over-represented by individuals with mild/moderate disease, potentially due to premature death among those with severe disease. Although this group included a larger proportion of individuals with mild disease than the younger group, they experienced lower quality of life, more comorbidities both of aging and of hemophilic arthropathy, and lower rates of health-care utilization.
Keywords: hemophilia A, hemophilia B, burden of hemophilia, aging in hemophilia
Introduction
Hemophilia is a rare genetic bleeding disorder, which affects one in 5000 male births, or approximately 20,000 males in the U.S.1 While there have been great advances in care and therapeutics over the past few decades, persons with hemophilia (PWH) still suffer from increased morbidity and mortality due to bleeding in joints, muscles, and other sites. Hemophilia treatment is extremely costly with the total annual cost of care per person estimated to be $139,102 (SD $304,033) in 1995 US dollars.2 The treatment of hemophilia is a lifetime commitment on the part of the providers, payers, affected persons and their families.
Major clinical manifestations of hemophilia involve bleeding episodes, most often in knee, ankle and elbow joints. In addition, individuals with hemophilia are at risk of bleeding into muscles and internal organs, including the central nervous system. Repeated bleeding and bleeding-related arthropathy are major causes of acute and chronic joint pain, hemophilic morbidity and reduced every day function.3 Inadequate management of bleeding events increases the risks of serious morbidities such as disability, as well as lower health-related quality of life (HRQoL). Clinical manifestations negatively impact not only the physical functioning of persons with hemophilia, but may also affect their every day functioning, mental health, and social health.4
With improved hemophilia care and prophylactic treatment, the life expectancy of PWH has increased, making age-related comorbidities more common. A study conducted by Khleif found that adults who were 40 years or older and were cared for by the Gulf States Hemophilia & Thrombophilia Treatment Center, had at least one comorbid condition other than hemophilia, and the majority had between 3 and 6 comorbidities.5 This study reported the most common conditions were chronic hepatitis C virus (HCV), hypertension, human immunodeficiency virus (HIV), chronic arthropathy, and overweight/obesity.5 HCV and HIV, both blood-borne viral infections, caused high mortality rate during the 1980s and 1990s.6,7 Another review on aging among PWH has identified the need to develop evidence to guide their treatment and their age-related comorbidities, as well as the need for additional prospective studies to guide proper delivery of care to this special population.8
Since 1995, the Hematology Utilization Group Studies (HUGS) have collected data from Hemophilia Treatment Centers (HTCs) to evaluate the costs of care and disease burden in PWH.2,9–11 However, these studies collected data from the general hemophilia population between 2 and 64 years old, with an inadequate sample of the elderly patient population. The HUGS VII study collected data focused on individuals aged 40 years and older (with the oldest being 79 years old). This article compares the impact of hemophilia on comorbidities, joint problems, HRQoL and health-care utilization between two age groups: 40–49 years and ≥50 years.
Materials and Methods
Design
HUGS VII is an observational cohort study that collected data from three US HTCs that provide care to PWH in three states (Colorado, Michigan, and Washington). Institutional review board approvals were obtained from the Data Coordinating Center at the University of Southern California and the three HTCs. The study complies with Declaration of Helsinki. Participants met the following inclusion criteria: 1) age 40 years or older; 2) factor VIII or factor IX activity level ≤30%; 3) male gender (since hemophilia is an X-linked disorder); 4) received the majority of their hemophilia care at the HTC to ensure the HTC can collect participant data through the study period; 5) provided care at the recruiting HTC in the year prior to enrollment in this study; 6) speaks English; and, 7) willing to provide written informed consent. Individuals judged by the clinician to be cognitively impaired or those with any additional blood disorder were excluded.
Recruitment and Procedures
Eligible participants were identified by the site study coordinator during clinic visits or through retrospective clinical chart review. After obtaining informed consent, the study coordinator provided participants with written instructions for taking surveys at baseline (enrollment) and six months later. The coordinator administered the baseline survey. Six months after enrollment, the study coordinator sent a reminder to participants to complete the follow-up survey. Participants were given the option of completing the follow-up data via a Qualtrics online survey, or through a mailed survey or by a telephone interview conducted by the study coordinator. Most participants chose to complete the online survey, although some used the mailed or telephone surveys when more convenient, or they had no internet access. Participants received a $10 gift card for completing the initial survey and a $20 gift card for completing the follow-up survey. Recruitment began in April 2018 and was closed in December 2019; data collection was completed in October 2020.
At each HTC, the study coordinator abstracted clinical information from each participant’s medical chart for the period of six months prior to and after enrollment. Information collected included clinical characteristics of the participant, type of factor VIII or IX products prescribed (eg, recombinant derived, or plasma derived, bypassing agents, or other products), factor VIII or IX prescription information, inhibitor status and laboratory values, other anti-hemophilic medications, range of motion, outpatient doctor visits, hospitalizations, and emergency room visits. Clotting factor infusion records were acquired from pharmaceutical records supplied by the patient’s home health company or pharmaceutical benefit manager, or from HTC 340B pharmacy records. Where participants did not complete the follow-up survey, clinical chart review data was still collected.
Measures
The initial survey collected data on personal characteristics including hemophilia treatment, health-care utilization, bleeding information, pain, joint problems, health status, work productivity and activity impairment, medical conditions and comorbidities, access to care, and physical activity. Sociodemographic data was also collected, including marital status, employment, education, ethnicity, race, health insurance status and household income. The six-month follow-up survey collected similar data, with the exception of medical conditions, sociodemographics, and health insurance status.
Self-Reported Comorbidities and Complications
Self-reported comorbidities questionnaire was adapted from the National Health Nutrition Examination Survey (NHANES). Comorbidities were measured by asking “Has a doctor ever told you that you have certain conditions?” The questionnaire asked about 19 medical conditions, including high blood pressure/hypertension, osteo/rheumatoid arthritis, osteoporosis, heart attack/myocardial infarction, procedures to treat coronary artery disease, congestive heart failure, skin cancer, cancer (other than skin cancer), diabetes/high blood sugar, emphysema, asthma, chronic bronchitis, chronic obstructive pulmonary disease (COPD), stroke, hip fracture, Alzheimer’s disease, Parkinson’s disease, depression, anxiety, hepatitis C virus (HCV) infection, and HIV/AIDS status.
Self-Reported Joint Health and Pain
Self-reported joint pain and range of motion (ROM) limitation were obtained from two multiple choice questions.9 General and acute pain were measured by asking participants to specify the intensity of pain using a Visual Analogue Scale (VAS) ranging from 0 (no pain) to 10 (worst pain).12
Health-Related Quality of Life
HRQoL was measured by the EuroQoL EQ-5D-3L.13 The EQ-5D-3L consists of the EQ-5D descriptive system and the EQ visual analogue scale (EQ VAS). The EQ-5D-3L descriptive system comprises five dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. Each dimension has three levels: no problems, some problems, and extreme problems. The VAS records the respondent’s self-rated health on a vertical numeric scale ranging from 0 (the worst possible health status) to 100 (the best possible health status). The US-based valuation algorithm was used to generate a time trade-off (TTO) index score, which is anchored at 0 for death and 1 for perfect health.14
Work Productivity and Activity Impairment
The hemophilia-specific version of the Work Productivity and Activity Impairment (WPAI) questionnaire was used to measure the impact of the hemophilia on the participants’ productivity.15 The WPAI yields four types of scores based on the assessment in the previous 7 days: 1) absenteeism (work time missed), 2) presenteeism (impairment while working or reduced on-the-job effectiveness), 3) work productivity loss (overall work impairment or sum of absenteeism and presenteeism), 4) activity impairment. The scores are expressed in percentages.
Anxiety and Depression
Anxiety and depression were included as one of many self-reported comorbidities in the initial survey. The seven-item Generalized Anxiety Disorder (GAD-7) and the nine-question Patient Health Questionnaire (PHQ-9) were also included in the follow-up survey. GAD-7 was used to measure anxiety,16 and PHQ-9 was used to measure depression.17 If scores on either of these measures reach 10 or greater, it is considered as diagnostic for the respective mental health condition.16,17
Health-care Utilization
The patient surveys provided self-reported data on health-care utilization, including number of outpatient visits, physical therapy visits, medical procedures related to treating bleeding events, and emergency room visits, as well as overnight stays in a hospital. Participants were asked to consider the previous 30 days for the initial survey and the previous six months for the follow-up survey regarding health-care utilization. Health-care utilization data was also abstracted from participants’ clinical charts to document the utilization for a period of six-month prior and post enrollment.
Statistical Analysis
Descriptive statistics, such as frequencies and proportions (for categorical variables) and means, standard deviations, medians, and ranges (for continuous variables), describe the sample in terms of participant demographic and clinical characteristics, HRQoL, WPAI scores, and health-care utilization. Comparisons of individuals’ characteristics were made between two age groups, 40–49 vs ≥50 years old. To compare the variables between the two age groups, we defined the clinically meaningful difference as minimum 5% difference for the categorical variables, 0.5 points difference for scores that ranged from 0 to 10, or 5 points difference for scores that ranged from 10 to 100 for the continuous variables. Since all these cut points had at least 0.2 effect size, they fit Cohen’s definition for small effect size. A small effect size of this magnitude may be considered as clinically relevant.18
Generalized linear regression models were used to assess mean covariate-adjusted scores for pain and EQ-5D scores by age group. These scores were obtained from general linear regression models using least squares means, which computed for each age group appropriately adjusted for the covariate effect in the general linear models. Covariates included education, employment, marital status, prophylactic treatment use, hemophilic severity, and self-reported joint problems.
Results
Participants’ Characteristics
We recruited and collected baseline data from 70 males with hemophilia aged ≥40 years. One participant was lost to follow-up as he was no longer receiving care at the HTC during the six- month follow-up period. Fifty-seven participants (81%) completed the follow-up survey.
The analysis sample included 69 participants with a mean age of 56.8 years (standard deviation: 11.0; ranging from 40.0 to 79.0 years old), 65.2% were 50 years of age or older, and 75.4% were diagnosed with hemophilia A. The group of individuals ≥50 years of age had higher rates of: marriage or partnership (71.1% vs 54.2%, P = 0.16), high school or more education (100% vs 91.7%, P = 0.049), and were more likely to be retired or not employed (66.7% vs 25.0%, P = 0.001) than the group 40–49 years old. The older group had a significantly lower proportion of individuals with annual family income >$75,000, compared to those 40–49 years old (33.3% vs 65.2%, P = 0.02). The older group also had a significantly higher proportion with public health insurance (47.7% vs 18.2%, P = 0.0004) (Table 1).
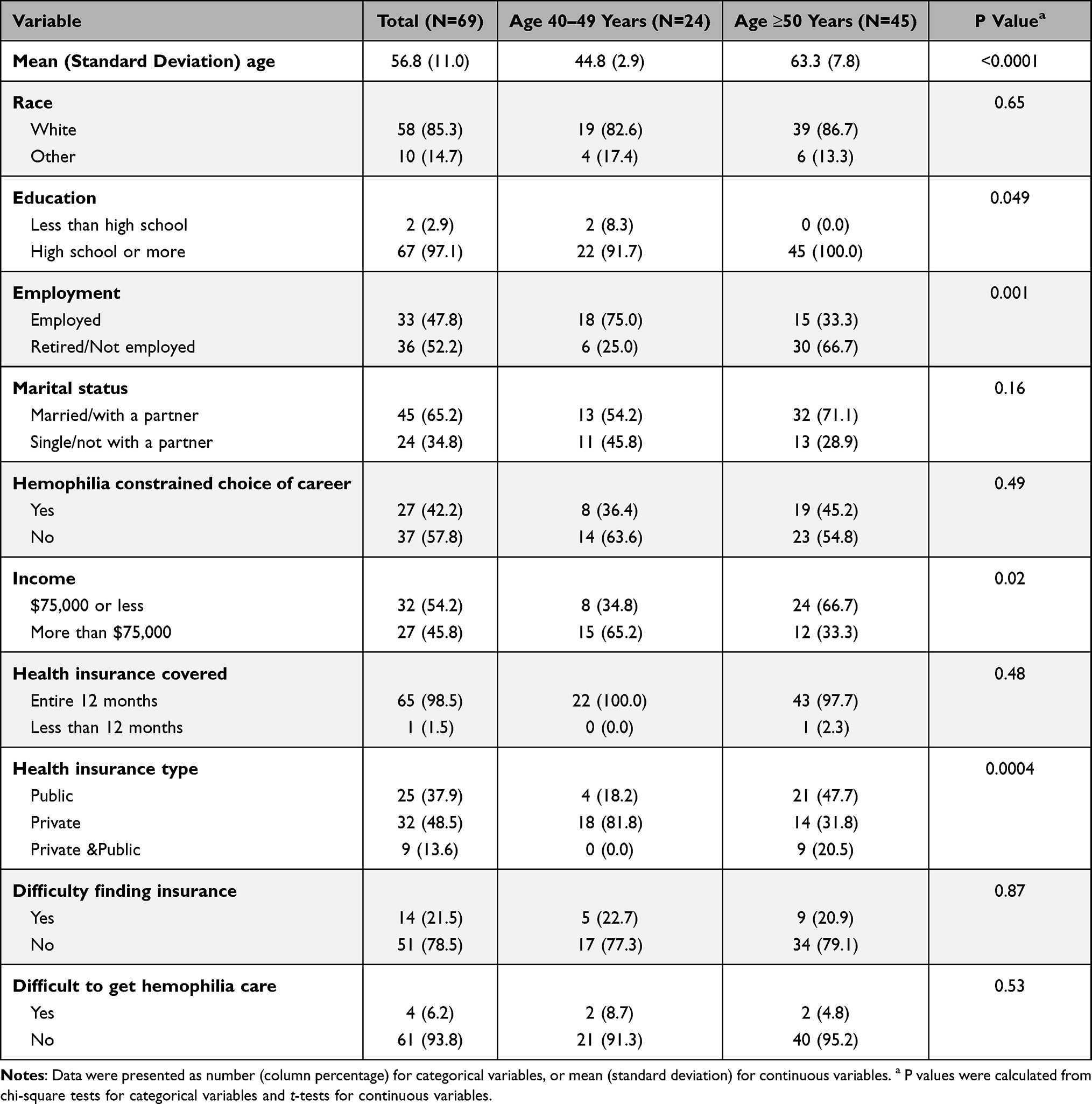 |
Table 1 Participants’ Social Demographic Characteristics and Health Insurance from Initial Survey |
Self-Reported Clinical Characteristics
Persons ≥50 years were more likely to have mild or moderate hemophilia (68.9% vs 41.7%, P = 0.03) than persons in the 40–49 age group (Table 2). Use of prophylaxis among those with severe hemophilia did not differ by age group.
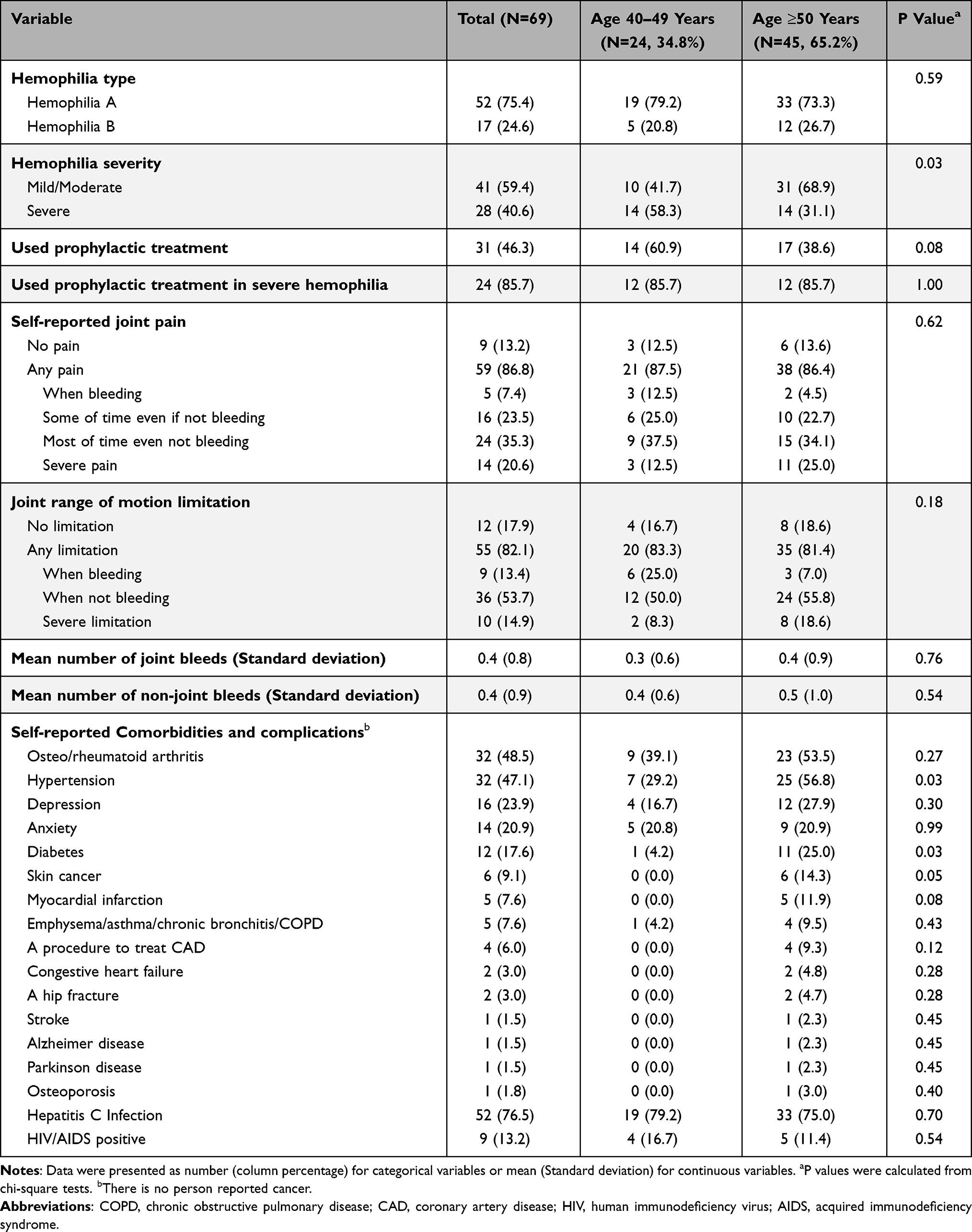 |
Table 2 Self-Reported Clinical Characteristics from Initial Survey |
Self-Reported Comorbidities and Complications
The most frequently reported comorbidities were HCV infection (76.5%), hypertension (47.1%), depression (23.9%), anxiety (20.9%), and diabetes (17.6%). Of those with HCV infection, 78.9% had been treated, and 82.4% of those treated had cleared the virus (Table 2). When depression and anxiety were measured by the PHQ-9 and GAD-7, 85.7% of the sample met the clinical diagnosis threshold for depression and 35.7% for anxiety, but the differences among the age groups were not statistically significant (Table 3). The older age group had higher rates of self-reported myocardial infarction (11.9% vs 0%, P = 0.08) and diabetes (25.0% vs 4.2%, P = 0.03) than those 40–49 years of age (Table 2).
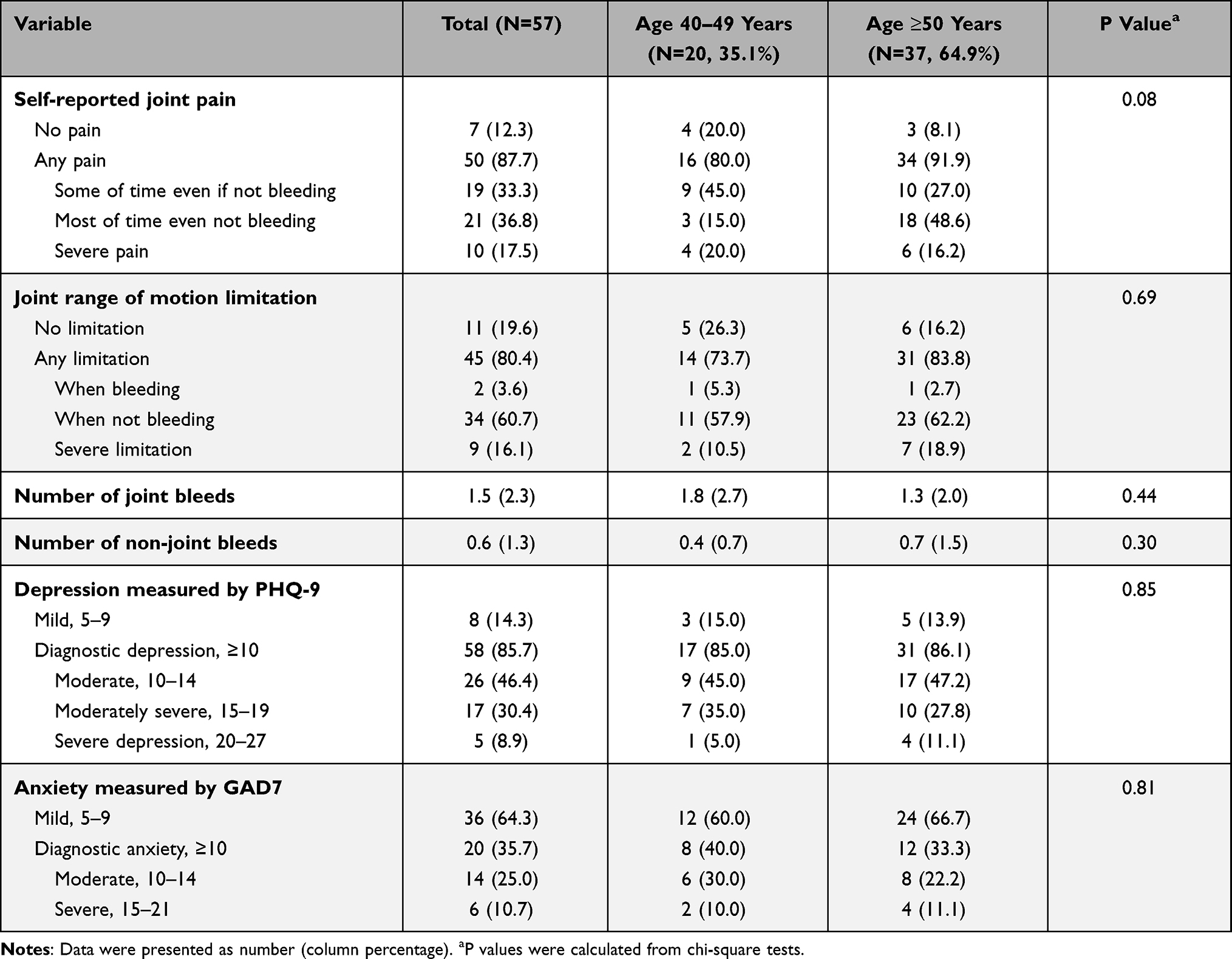 |
Table 3 Self-Reported Clinical Characteristics from Follow-Up Survey |
Self-Reported Joint Health and Pain
Among participants with mild/moderate hemophilia, the older age group reported a higher rate of joint pain (83.9% vs 70.0%, P = 0.34 at baseline, 91.3% vs 57.1%, P = 0.06 at follow up) than the younger group. Similarly, a greater proportion of the older group reported having range of motion limitations (73.3% vs 60.0%, P = 0.43 at baseline, 73.9% vs 28.6%, P = 0.04 at follow up). Among the study sample, rates of self-reported joint pain (91.9% vs 80.0%, P = 0.08) or of joint range of motion limitation (83.8% vs 73.7%, P = 0.69) in the follow-up survey were higher among the older group than in the younger age group in the follow-up survey (Table 3). Mean number of joint bleeds and non-joint bleeds were not significantly different between age groups, either at initial survey or at follow-up (Tables 2 and 3). Mean daily pain level in general was greater in the older age group than that in the younger age group (3.8 vs 3.0, P = 0.19 at initial survey, 4.1 vs 3.2, P = 0.23 in follow-up survey, respectively) (Table 4). Mean pain rating related to acute bleeding was similar between age groups at initial survey (2.5 vs 2.3, P = 0.73), but not significantly different among the age groups (3.1 vs 2.2, P = 0.30) at follow up.
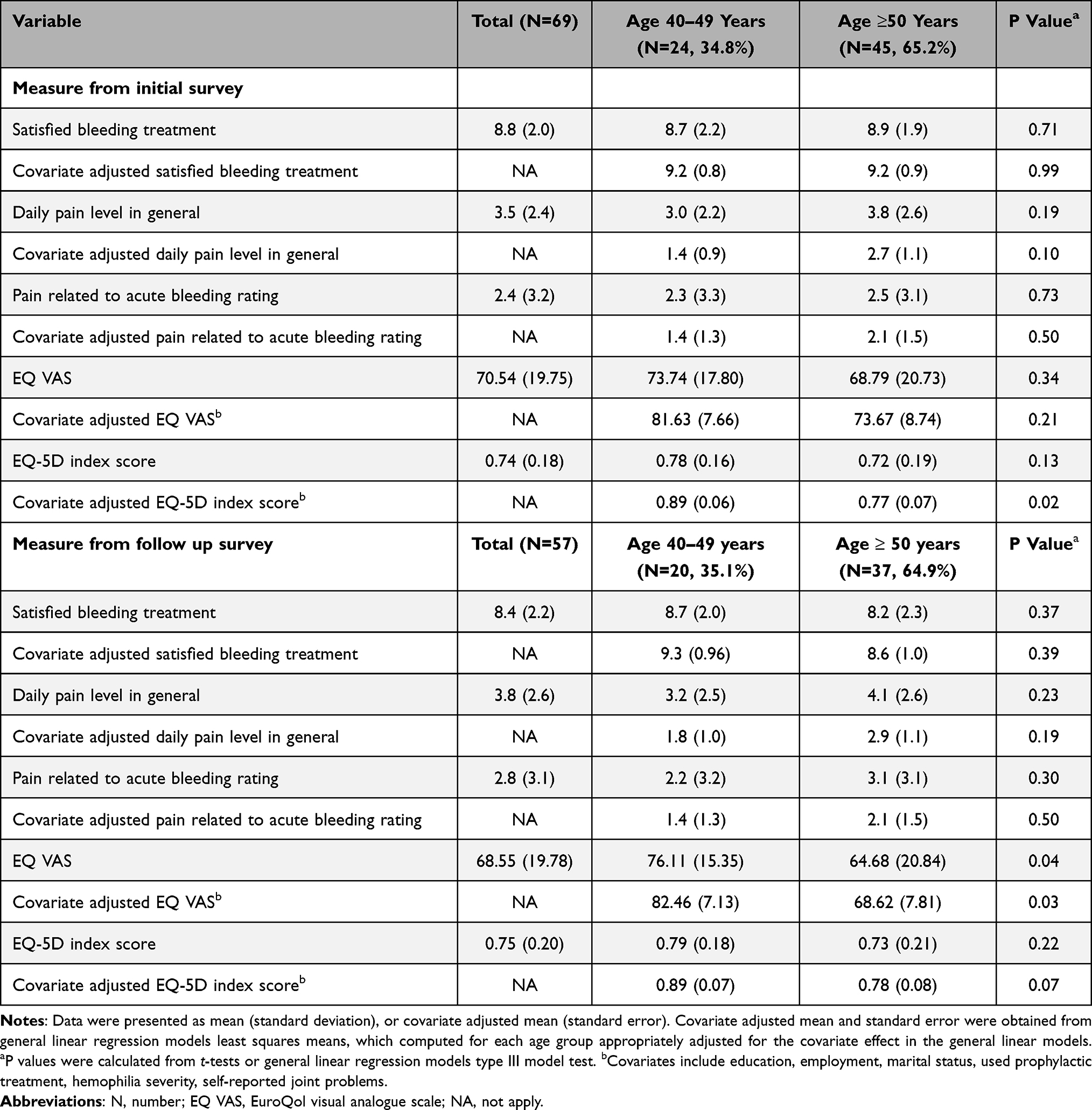 |
Table 4 Pain and Health-Related Quality of Life Measurement |
Health-Related Quality of Life
Table 4 shows the mean EQ-5D scores for the overall sample and stratified by age group. The mean covariate-adjusted EQ-5D VAS and index scores were lower among older persons (68.79 vs 73.74, P = 0.34 for VAS, 0.77 vs 0.89, P = 0.02 for EQ-5D index score) at the initial survey (Table 4). At follow up, the mean covariate-adjusted EQ-5D VAS was significantly lower in older persons than in younger individuals (68.62 vs 82.46, P = 0.03) and mean covariate-adjusted EQ-5D index score was lower in older persons (0.78 vs 0.89, P = 0.07) (Table 4).
Work Productivity and Activity Impairment
The results of WPAI were reported for 33 participants who were employed at the time of enrollment. Although none of the results were significant, those in the older age group had lower absenteeism scores (0% vs 11.1%, P = 0.16), or activity impairment (16.7% vs 22.2%, P = 0.52), but had a higher presenteeism score or work productivity loss (both were 12.1% vs 6.3%, P = 0.32). None of the 25 persons employed at the time of the follow-up survey had missed work. Those ≥50 years old reported higher presenteeism score or work productivity loss (both were 10.0% vs 3.8% P = 0.32), and activity impairment (14% vs 7.7%, P = 0.35) from the follow-up survey.
Health-care Utilization
As compared to those 40–49 years old, fewer proportion of participants ≥50 years old reported emergency room visits (4.5% vs 21.7%, P = 0.03), or physical therapy visits (15.9% vs 43.5%, P = 0.01) at baseline, but a higher proportion of individuals in this group reported doctor visits (69.4% vs 50.0%, P = 0.15) and emergency room visits (27.8% vs 15.0%, P = 0.28) at follow up (Table 5). Among those who visited the emergency room, older persons had a greater mean number of visits (1.4 vs 1.0, P < 0.0001) based on 12 months of medical chart reviews (Table 6).
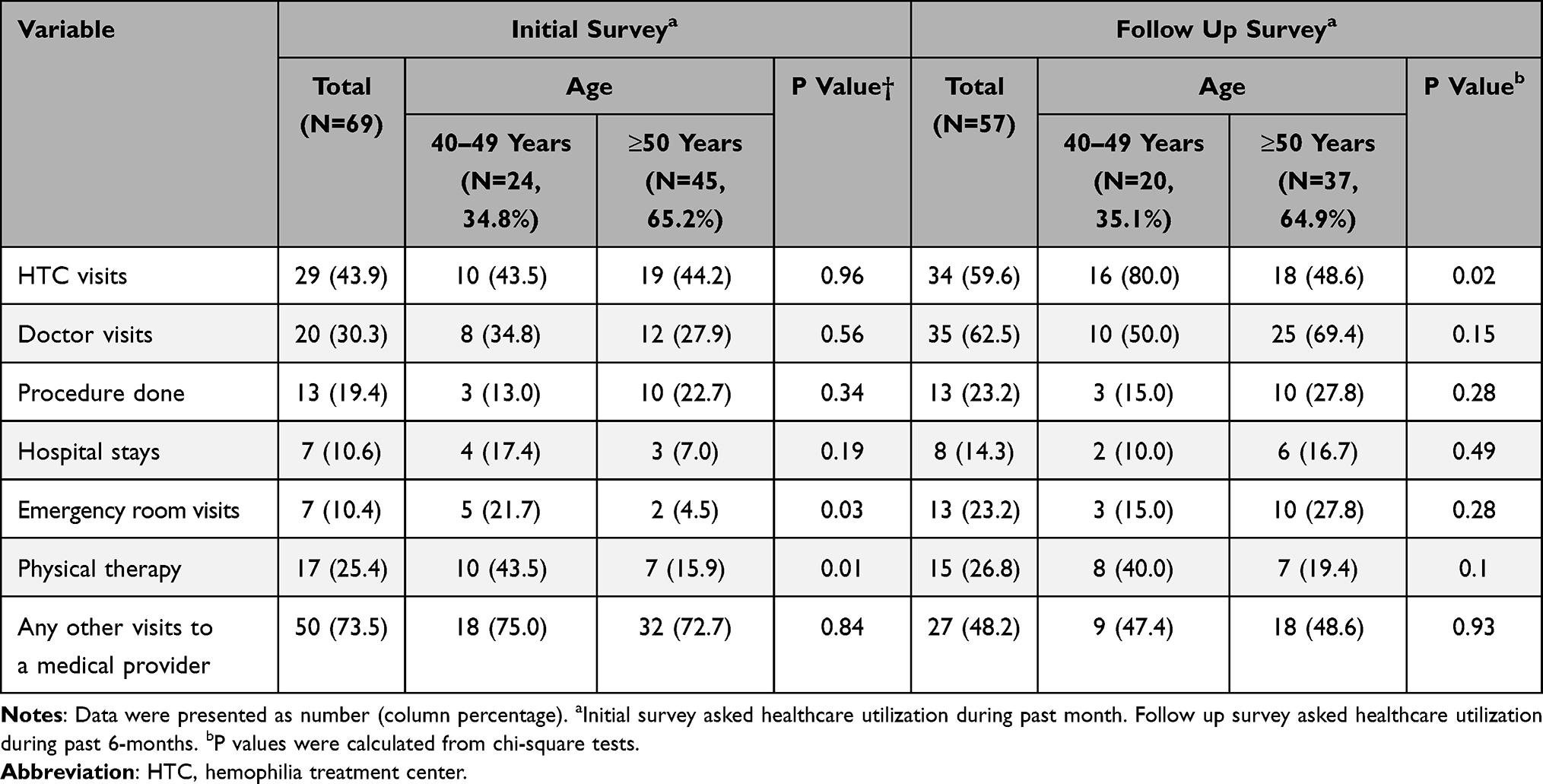 |
Table 5 Self-Reported Health-care Utilization |
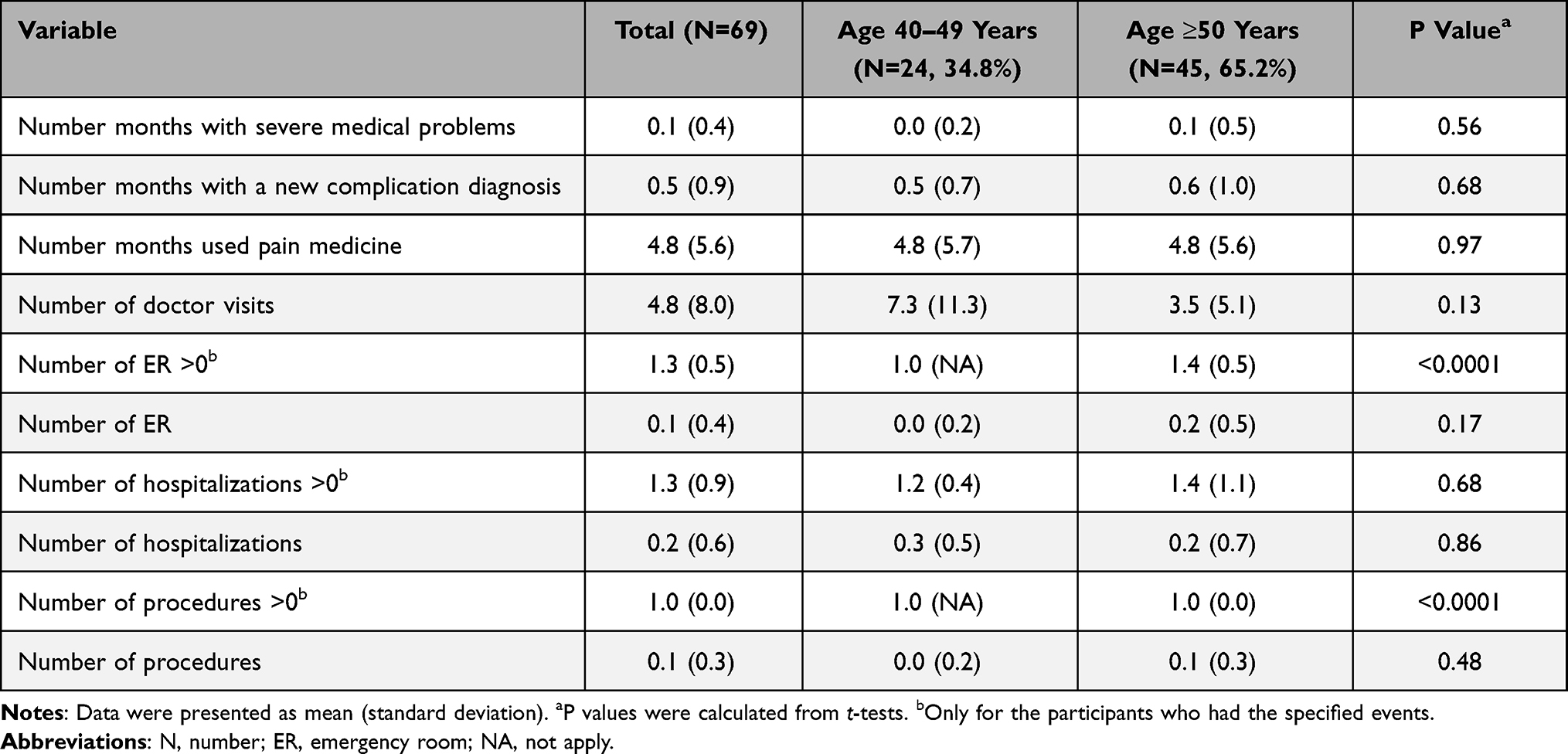 |
Table 6 Mean of Health-care Utilization from Clinical Chart Review for 12 Months Period |
Discussion
This observational study compared a sample of US men with hemophilia of all severities in their 40ʹs (beginning middle age) to counterparts 50 years of age or older (middle and older age adulthood) who obtained care at three HTCs. This study’s aim was to describe their health status, in terms of hemophilia and aging-related comorbidities, and to examine the impact of hemophilia on joint health, quality of life, and health-care services utilization.
The study sample included more participants in the older age group, and they were more likely to have a diagnosis of mild/moderate rather than severe hemophilia. The predominance of non-severe hemophilia among the older group may be due to premature death among those with severe disease. Especially since the older cohort was born about two decades before both viral inactivation manufacturing processes eliminated both HIV and HCV from hemophilia medications in the US, and before the regional networks of HTCs nationwide were established, which enhanced widespread access to expert team-based care.19 This is also noted in an analysis of life expectancy and cause of death in individuals with hemophilia A and B in Norway from 1986-2018, which showed that the persons with severe hemophilia died at a mean age of 53.4±21.7 compared to 71.5±19.6 for mild and moderate hemophilia.20
Not surprisingly, the older age group included a higher proportion of people retired or not employed, and these individuals were more likely to use public health insurance. There was no statistically significant difference among age groups regarding difficulty obtaining health insurance or hemophilia care. Both age groups with severe hemophilia had similar proportions using clotting factor treatment prophylactically.
Although the older age group included a lower proportion of individuals with severe hemophilia, the proportion with self-reported joint pain and joint range of motion limitations were similar among the two age groups at the initial survey. However, a higher proportion of the older age group reported severe joint pain at baseline (25.0% vs 12.5%) and at the follow-up survey (20.0% vs 16.2%). This may reflect participants’ more severe joint pain when aging, even if they had less severe hemophilia. The mean number of self-reported joint bleeds and non-joint bleeds at the initial survey were not significantly different among the two age groups. At follow-up, we observed that the mean number of joint bleeds was lower in the older age group (1.3 vs 1.8), although it was not statistically significant. This result may indicate that patients with severe disease experienced more bleeding episodes. These results parallel the findings of Mazepa et al,21 although the HUGS VII sample extended to moderately severe populations.
The aging hemophilia population, like the general US aging population, faces age-related cardiovascular disease and malignancy. The most frequently reported comorbidity was osteo/rheumatoid arthritis (48.5%). The older age group in our study had a frequency of 53.5% for osteo/rheumatoid arthritis, which is lower than the rate reported from the literature.22 Hemophilia has been associated with low bone mineral density, with 66.6% of persons with moderate or severe hemophilia ≥50 years having osteoporosis.22 A higher proportion of the older age group in HUGS VII reported age-related comorbidities, including hypertension, depression, diabetes, skin cancer, and myocardial infarction than the younger group.
Although self-reported rates of depression and anxiety at baseline were 23.9% and 20.1%, the results of the self-reported depression scale (PHQ-9) administered at the six-month follow-up survey deserve attention. While there was no statistically significant difference among the age groups, 85.7% of the overall sample (N = 57) had a score ≥10, indicating a classification of moderate/severe depression and 35.7% of the overall sample had a score of ≥10 on the anxiety scale.17 The baseline survey obtained depression and anxiety measures through self-report based on whether a physician had ever mentioned that the respondent had the condition. The higher rates of possible diagnosed depression and anxiety in the follow-up may be due to persons who had mental health symptoms but had not sought care. The depression rate in our sample was much higher than that among adult men in the general US population in 2019, who reported moderate/severe symptoms of depression (score PHQ-8≥10) at a rate of 5.5%.23 The same was true for anxiety: males in the general US population reported moderate/severe symptoms of anxiety (score GAD-7≥10) at a rate of 4.3%.24
The mean daily pain level in general, and pain related to acute bleeding were both higher in the older age group than the younger group, although they were not statistically significant at either time point. However, the magnitude of differences among age groups may be clinically meaningful, as a 0.9 difference was demonstrated in the follow-up survey. The older age group reported higher pain scores and lower HRQoL. Both the mean EQ VAS and index scores at the time of the follow-up survey were similar to the scores obtained at baseline. The mean EQ VAS scores (70.54, and 68.55 at initial and follow-up, respectively) were lower than the US population norm of 80.0. The mean EQ index scores (0.74, and 0.75 for initial and follow-up, respectively) were also lower than the US population norm. Even when stratified by age group, both EQ VAS and index scores were lower than US age-specific norm scores. Reduced HRQoL scores in older persons may be related to age, but may also be associated with increased pain.25,26 Moreover, older PWH often experience anxiety due to chronic pain, impaired quality of life, and reduced ability to maintain an independent lifestyle.27,28
Our results demonstrated that the older age group had more physician visits and fewer emergency department visits at baseline, providing some evidence that regular care may result in lower acute care use, but this was not supported by the six-month follow-up use. However, when the analysis excluded those participants lost to follow-up, the lower emergency department utilization persisted six months later. The changes between baseline and six months later may relate to one or more bleeding events or poorer outcomes due to other comorbidities, and further analyses could be helpful.
Limitations
The study sample included 69 total participants. This small sample size limits statistical power to detect between-group differences for many study variables. As hemophilia is a rare congenital condition, it is challenging to recruit a large study sample. Focusing on clinically meaningful differences rather than statistically significant differences may be helpful for interpreting this observational sample. As the study sample includes more individuals with mild/moderate hemophilia in the older age group, it is important to adjust for severity in these analyses. Further caution should be taken related to individuals in the sample who did not complete the six-month follow-up survey.
Conclusion
The 50 years or older age group was over-represented by individuals with mild/moderate disease, likely due to premature death among those with severe disease. Although those ≥50 years included a larger proportion of individuals with mild hemophilia than the 40–49 year group, they experienced statistically and clinically significant lower HRQoL scores, more comorbidities related to aging and hemophilic arthropathy, and lower health-care utilization. These results, coupled with the important finding of a high rate of depression and anxiety in both age groups, highlight the need for special attention be paid to PWH. The increasing survival rates among PWH reveal a growing array of physical, social, and mental health vulnerabilities requiring the attention of clinicians, caregivers, advocates and health-care policymakers.
Acknowledgments
The study was supported by Pfizer through an Investigator-Initiated Research agreement between Pfizer and the University of Southern California (USC).
The members of the study group: University of Southern California: Michael B. Nichol, PhD, Principal Investigator (PI), Joanne Wu, MS, Steven Carrasco, MPH; University of Colorado Denver Hemophilia and Thrombosis Center: Marilyn Manco-Johnson, MD, Site PI, Hana Durkee, Lindsey Furton; BloodWorks Northwest, Seattle, WA: Barbara Konkle, MD, Site PI, Sarah Galdzicka, Sarah Ruuska, Rachel Hervey; Michigan State University Center for Bleeding and Clotting Disorders, East Lansing, MI: Roshni Kulkarni, MD, Site PI, Anna Robinson, Kathleen Anderson.
Disclosure
Randall Curtis received a consultant fee from USC through the project funding provided by Pfizer. He also received consultant fee from Bayer, Patient Outcomes Research Group and Novo Nordisk. Marilyn Manco-Johnson reports grants from HRSA/MCHB. Barbara A. Konkle, MD, has received grant funding from Pfizer, Regeneron, Spark, Sangamo, Sanofi, Sigilon, Takeda and Uniqure and has received consulting fees from BioMarin, CSL Behring, Pfizer and Sigilon. Roshni Kulkarni, 1) Advisory boards: Bioverativ/Sanofi, BPL, Genentech, Kedrion, Novo Nordisk, Octapharma, Pfizer, Takeda, Catalyst Bioscience Bayer; 2) Clinical Trials: Sanofi/Bioverativ, Bayer, Biomarin, Shire/Takeda, Novo Nordisk, Freeline; 3) Speakers bureau, stocks or shares: none. Joanne Wu received financial support through the project funding provided by Pfizer. Judith Baker, Megan Ullman have no significant conflicts of interest to declare. Duc Quang Tran Jr received consultant fees from Bayer, Bioverativ, HEMA Biologics, UniQure, Novo Nordisk, and Takeda. Michael B. Nichol is the principal investigator for the HUGS research group and has received grant funding from multiple sources including Pfizer, Genentech Inc., Shire (formerly Takeda/Baxter), Octapharma, CSL Behring, and Global Blood Therapeutics. The authors report no other conflicts of interest in this work.
References
1. Soucie JM, Evatt B, Jackson D. Occurrence of hemophilia in the United States. The hemophilia surveillance system project investigators. Am J Hematol. 1998;59(4):288–294. PMID: 9840909. doi:10.1002/(sici)1096-8652(199812)59:4<288::aid-ajh4>3.0.co;2-i
2. Globe DR, Curtis RG, Koerper MA; HUGS Steering Committee. Utilization of care in haemophilia: a resource-based method for cost analysis from the Haemophilia Utilization Group Study (HUGS). Haemophilia. 2004;10(Suppl 1):63–70. PMID: 14987251. doi:10.1111/j.1355-0691.2004.00881.x
3. Choinière M, Melzack R. Acute and chronic pain in hemophilia. Pain. 1987;31(3):317–331. doi:10.1016/0304-3959(87
4. Poon JL, Zhou ZY, Doctor JN, et al. Quality of life in haemophilia A: hemophilia Utilization Group Study Va (HUGS-Va). Haemophilia. 2012;18(5):699–707; PMID: 22507546. doi: 10.1111/j.1365-2516.2012.02791.x
5. Khleif AA, Rodriguez N, Brown D, Escobar MA. Multiple comorbid conditions among middle-aged and elderly hemophilia patients: prevalence estimates and implications for future care. J Aging Res. 2011;2011:985703. doi:10.4061/2011/985703
6. Miesbach W, Alesci S, Krekeler S, Seifried E. Comorbidities and bleeding pattern in elderly haemophilia A patients. Haemophilia. 2009;15(4):894–899. PMID: 19473414. doi:10.1111/j.1365-2516.2009.02030.x
7. Arnold DM, Julian JA, Walker IR. Association of hemophilia clinic directors of Canada. Mortality rates and causes of death among all HIV-positive individuals with hemophilia in Canada over 21 years of follow-up. Blood. 2006;108(2):460–464. PMID: 16551974. doi:10.1182/blood-2005-11-4407
8. Angelini D, Konkle BA, Sood SL. Aging among persons with hemophilia: contemporary concerns. Semin Hematol. 2016;53(1):35–39. doi:10.1053/j.seminhematol.2015.10.004
9. Zhou ZY, Wu J, Baker J, et al. Haemophilia utilization group study - Part Va (HUGS Va): design, methods and baseline data. Haemophilia. 2011;17(5):729–736; PMID: 21689212. doi: 10.1111/j.1365-2516.2011.02595.x
10. Zhou ZY, Koerper MA, Johnson KA, et al. Burden of illness: direct and indirect costs among persons with hemophilia A in the United States. J Med Econ. 2015;18(6):457–465. doi:10.3111/13696998.2015.1016228.
11. Chen CX, Baker JR, Nichol MB. Economic burden of illness among persons with hemophilia B from HUGS Vb: examining the association of severity and treatment regimens with costs and annual bleed rates. Value Health. 2017;20(8):1074–1082. PMID: 28964439. doi:10.1016/j.jval.2017.04.017
12. Siboni SM, Mannucci PM, Gringeri A, et al. Health status and quality of life of elderly persons with severe hemophilia born before the advent of modern replacement therapy. J Thromb Haemost. 2009;7(5):780–786; PMID: 19220727. doi: 10.1111/j.1538-7836.2009.03318.x
13. Brooks R. EuroQol: the current state of play. Health Policy. 1996 ;37(1):53-72. doi:10.1016/0168-8510(96)00822-6
14. Shaw JW, Johnson JA, Coons SJ. US valuation of the EQ-5D health states: development and testing of the D1 valuation model. Med Care. 2005;43(3):203–220. PMID: 15725977. doi:10.1097/00005650-200503000-00003
15. Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics. 1993;4(5):353–365. PMID: 10146874. doi:10.2165/00019053-199304050-00006
16. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. PMID: 16717171. doi:10.1001/archinte.166.10.1092
17. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. PMID: 11556941; PMCID: PMC1495268. doi:10.1046/j.1525-1497.2001.016009606.x
18. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
19. Baker JR, Crudder SO, Riske B, Bias V, Forsberg A. A model for a regional system of care to promote the health and well-being of people with rare chronic genetic disorders. Am J Public Health. 2005;95(11):1910–1916. PMID: 16195525; PMCID: PMC1449458. doi:10.2105/AJPH.2004.051318
20. Skjefstad K, Solberg O, Glosli H, von der Lippe C, Feragen KB. Life expectancy and cause of death in individuals with haemophilia A and B in Norway, 1986-2018. Eur J Haematol. 2020;105(5):608–615. PMID: 32710483. doi:10.1111/ejh.13494
21. Mazepa MA, Monahan PE, Baker JR, Riske BK, Soucie JM; US Hemophilia Treatment Center Network. Men with severe hemophilia in the United States: birth cohort analysis of a large national database. Blood. 2016;127(24):3073–3081. PMID: 26983851; PMCID: PMC4911863. doi:10.1182/blood-2015-10-675140
22. Kiper Unal HD, Comert Ozkan M, Atilla FD, et al. Evaluation of bone mineral density and related parameters in patients with haemophilia: a single center cross-sectional study. Am J Blood Res. 2017;7(5):59–66. PMID: 29181264; PMCID: PMC5698560.
23. Villarroel MA, Terlizzi EP Symptoms of depression among adults: United States, 2019. NCHS Data Brief, no 379. Hyattsville, MD: National Center for Health Statistics.; 2020.
24. Terlizzi EP, Villarroel MA Symptoms of generalized anxiety disorder among adults: United States, 2019. NCHS Data Brief, no 378. Hyattsville, MD: National Center for Health Statistics.; 2020.
25. Langley P, Müller-Schwefe G, Nicolaou A, Liedgens H, Pergolizzi J, Varrassi G. The societal impact of pain in the European Union: health-related quality of life and healthcare resource utilization. J Med Econ. 2010;13(3):571–581. PMID: 20815688. doi:10.3111/13696998.2010.516709
26. Gureje O, Von Korff M, Simon GE, Gater R. Persistent pain and well-being: a World Health Organization Study in Primary Care. JAMA. 1998;280(2):147–151. doi:10.1001/jama.280.2.147
27. Evans DL, Charney DS, Lewis L, et al. Mood disorders in the medically ill: scientific review and recommendations. Biol Psychiatry. 2005;58(3):175–189. PMID: 16084838. doi:10.1016/j.biopsych.2005.05.001
28. Vun E, Turner S, Sareen J, Mota N, Afifi TO, El-Gabalawy R. Prevalence of comorbid chronic pain and mental health conditions in Canadian armed forces active personnel: analysis of a cross-sectional survey. CMAJ Open. 2018;6(4):E528–E536. PMID: 30389752; PMCID: PMC6221807. doi:10.9778/cmajo.20180093
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.