")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Community Pharmacy Personnel Understanding of Antibiotic Dispensing in Eastern Nepal
Authors Goswami N, Dahal P , Shrestha S , KC B , Mallik SK
Received 23 May 2020
Accepted for publication 10 August 2020
Published 10 September 2020 Volume 2020:13 Pages 1513—1522
DOI https://doi.org/10.2147/RMHP.S264192
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Nikita Goswami,1,* Prasanna Dahal,1,* Shakti Shrestha,2 Bhuvan KC,3 Shyam Kumar Mallik1
1Purbanchal University College of Medical and Allied Sciences, Purbanchal University, Sundar Haraicha, Gothgaun, Morang, Nepal; 2School of Pharmacy, Pharmacy Australia Center of Excellence, The University of Queensland, Brisbane, QLD 4102, Australia; 3School of Pharmacy, Monash University Malaysia, Jalan Lagoon Selatan 47500, Bandar Sunway Selangor Darul Ehsan, Malaysia
*These authors contributed equally to this work.
Correspondence: Prasanna Dahal
Purbanchal University College of Medical and Allied Sciences, Purbanchal University, Sundar Haraicha, Gothgaun, Morang 56611, Nepal
Tel +9779852049828
Email [email protected]
Background: Community pharmacies are easily accessible outlets providing medicines to the general public in Nepal, but it is known that irrational dispensing of antibiotics from such outlets contributes to antimicrobial resistance.
Objective: To assess the understanding of community pharmacy personnel around antibiotic-dispensing in Eastern Nepal and the relationship between this understanding and their personal characteristics.
Methods: A cross-sectional survey was conducted on 312 pharmacy personnel working in community pharmacies of three districts within Eastern Nepal using a self-administered questionnaire. Descriptive statistics were used to analyze participants’ characteristics and their understanding of antibiotic dispensing. The relationships between their understanding of antibiotic dispensing and their characteristics were determined using Chi-square tests.
Results: Most of the pharmacy personnel considered that dispensing antibiotics without a valid prescription is a problem (76.9%), and that it would not be legal to do so (86.9%). In the survey, 34.9% of participants agreed that they had dispensed antibiotics without prescription, and 26.9% disagreed with the assertion that inappropriate dispensing of antibiotics could promote antimicrobial resistance. Most (94.5%) reported that they would advise patients to follow their antibiotic dosage regimen, but 34.3% reported that they believed antibiotics to reduce pain and inflammation. Bivariate analysis showed that the level of understanding about antibiotic indication was significantly associated with age (p< 0.001), work experience (p< 0.001) and qualifications (p=0.017) of the pharmacy personnel. Work experience and qualifications also had significant but independent relationships with the level of understanding that irrational dispensing of antibiotics promotes antimicrobial resistance (p=0.018 and p=0.004) and is on the need for patient follow-up after dispensing antibiotics (p< 0.001 and p=0.042).
Conclusion: The understanding of community pharmacy personnel about antibiotic dispensing in Eastern Nepal requires significant improvement. Degree of understanding of some aspects of antibiotic dispensing was influenced by age, work experience and qualifications.
Keywords: antibiotic dispensing practice, antibiotic resistance, community pharmacy, irrational drug dispensing, pharmacist, pharmacy personnel
Introduction
Antibiotics are the most commonly used group of medicines for the treatment of infection; however, appropriate antibiotic use has become a problem, especially in low-income counties (LICs).1,2 Healthcare systems of developing countries such as Nepal suffer from systemic inadequacies affecting quality, coverage, and delivery of healthcare services and medicines.3 Poor quality public healthcare services and medicines, high physician consultation charges in the private sector and lack of public awareness regarding proper antibiotic use encourage people to purchase these medicines without prescription, or self-refill previous prescriptions.4 Patients often share antibiotics with friends and family without professional consultation, follow inappropriate dosage regimens and stop taking antibiotics early without completing the regimen.4,5 These practices of consumers contribute to the misuse of medicines, including antibiotics, in LICs.
Dispensing antibiotics without prescription remains common practice, especially in LICs and can significantly contribute to antibiotic resistance.6 Misuse and abuse of antimicrobials not only increases antimicrobial resistance; but also causes therapeutic ineffectiveness, in turn increasing hospitalizations, durations of hospital stay, mortality rates and healthcare costs.7 The United Nations (UN) ad hoc Interagency Coordinating Group (IACG) on Antimicrobial Resistance has stated that drug-resistant diseases cause approximately 700,000 deaths every year, and this is predicted to rise to 10 million deaths each year by 2050 if no immediate action is taken to tackle the problem.8 This will also have serious economic consequences.
In Nepal, the Global Antibiotic Resistance Partnership Nepal is responsible for strategies to improve the utilization of antibiotics at a national level.9 The Government of Nepal formulated the 2014 National Antibiotic Treatment Guidelines.10 However, the implementation of these guidelines has been poor, likely due to inadequacies in the healthcare system and governance. Antibiotic resistance and irrational antibiotic use are therefore a serious problem in Nepal.11,12 Dispensing of antibiotics without a valid prescription is common in many countries.13–18 In 2015, a multi-country survey conducted by the World Health Organization (WHO) revealed that antibiotic consumption was comparatively higher in low-income countries, and estimated that 93% of patients obtained their antibiotics from pharmacies.19 Pharmacy personnel in community pharmacies can play a significant role in the promotion of rational medicine use through appropriate dispensing of antibiotics. It is, therefore, of utmost importance that pharmacy personnel are aware of the consequences of inappropriate dispensing of antibiotics and strive towards improving drug dispensing practice.20,21
In the Nepalese context, studies assessing the pharmacist’s contribution to the prescribing process and improving healthcare outcomes are scarce. A systematic review by Mikarni et al on the impact of clinical pharmacy services reports limited studies on pharmacist involvement in counselling and educating patients, detecting prescribing errors, reviewing prescriptions, giving training and monitoring policy implementation in Nepal.22 However, pharmacists have demonstrated potential impact in reducing direct healthcare costs, reducing prescription errors, increasing access to medicine and improving drug utilization patterns, patients’ knowledge about medicines and satisfaction.
The “Drug Act 2035” was implemented in 1978 to prevent the misuse and abuse of drugs as well as to control the production, sale, distribution and international trade of drugs and pharmaceutical products.23 Section 17 of the Act promulgated the provision for drug classification into different categories, outlining the regulation in “Drugs category rules 2043”.24 The Act stated that antibiotics can only be dispensed by authorized pharmacy personnel, and only upon receipt of a valid prescription. The Nepalese drug act also mentions the Department of Drug Administration (DDA) as the national Regulatory Authority of Nepal for the licensure, regulation and quality assurance of antibiotics. The DDA, with support from the Global Antibiotic Resistance Partnership Nepal (GARP Nepal), has developed a community pharmacy training module that focused on drug prescription and distribution including a component on anti-microbial resistance (AMR) awareness. As such, the DDA has undertaken several activities to increase AMR awareness in the public and community pharmacy settings. However, there is no formal schedule or process for coordinating these activities, and the DDA also has limited capacity (in terms of human and economic resources) to expand these activities at the national or regional levels. There is understanding of the efforts needed to ensure access to good quality drugs, essential medicine lists, standard treatment guidelines, and efforts to combat antimicrobial resistance in hospitals (drug and therapeutic committees). However, there is much more to do in terms of practice.25 Studies have reported that dispensing antibiotics without prescription is common in the community pharmacies of central Nepal.26,27 Therefore, we aim to assess the understanding of dispensing antibiotics among community pharmacy personnel in Eastern Nepal, and the relationship between this understanding and their characteristics.
Methods
Study Design and Setting
A cross-sectional survey was conducted with pharmacy personnel working in community pharmacies of selected districts (Jhapa, Morang and Sunsari) of Eastern Nepal between March to August 2019. These three districts are some of the most densely populated districts of Eastern Nepal.
Study Population
Any pharmacy personnel involved in dispensing medicines, irrespective of their qualifications, practicing at community pharmacies during the time of visit were eligible to be included in the study. The Drug Act 2035 states that three levels of pharmacy personnel are authorized to run a pharmacy following registration with the DDA and dispense medicine. These include Pharmacist (four years’ undergraduate bachelor in pharmacy course); assistant pharmacist (three years’ diploma in pharmacy course) and “Professionalist” (“Byabasai” in Nepali language; 48–72 hours’ orientation training course, when the former two courses were not common in Nepal).23 Those who did not consent to participate in the study were excluded.
Sample Size and Sampling Techniques
According to the regional office of the Department of Drug Administration (DDA) in eastern Nepal, the total number of registered community pharmacies in the study districts was 1638 (Jhapa: 461, Morang: 682 and Sunsari: 495). Therefore, a sample size of 312 was estimated using Raosoft sample size calculator (Raosoft, Inc.), assuming a 95% confidence interval, 5% margin of error and 50% response rate. The community pharmacies were selected using cluster sampling. The number of community pharmacies from each district (cluster) was determined based on the proportion of registered pharmacies in that region, in order to obtain data from 312 pharmacies (Jhapa: 88, Morang: 130 and Sunsari: 94). One participant (member of pharmacy personnel) was selected from each pharmacy using simple random sampling. Any pharmacy that was closed during the visit or without pharmacy personnel was excluded from the study and the next pharmacy was selected. The same rule was also applied to the selection of pharmacy personnel if the selected individual did not agree to participate.
Data Collection
A self-administered questionnaire was used to assess the level of understanding around antibiotic dispensing among pharmacy personnel working in community pharmacies. The questionnaire had two sections. The first section included general information about the participants (age, gender, community pharmacy work experience, qualification, location). The second section included 16 structured questions to assess their understanding of regulatory requirements, antibiotic use, antibiotic dispensing habits, and issues regarding antibiotic dispensing practice. The questions in the second section were developed through a review of studies on antibiotic dispensing in community pharmacies.13,16,27–30 The questionnaire was piloted with 10 pharmacy personnel using face-to-face interviews. Following each interview, improvements were made to the wording of the questions until no further changes were deemed necessary. Face validity was determined by questionnaire piloting whereas validity of the contents was ensured through consultation with two senior Nepalese pharmacists.
Statistical Analysis
The data were analyzed using IBM-SPSS 25.0 (IBM Corporation, Armonk, NY, USA). Descriptive statistics were used to characterize participant information, and their understanding towards antibiotic dispensing. The relationship between participant characteristics and their understanding of antibiotic dispensing was determined using Chi-square tests. Results were considered statistically significant at a threshold of p<0.05.
Results
Participant Characteristics
The participant characteristics are shown in Table 1. This shows that out of the sample of 312 community pharmacy personnel, 79.5% were males, and 37.2% were aged between 26 and 35 years. 35.6% of the participants had more than 10 years’ experience, followed by 32.7% having between 1 and 5 years’ experience, and 16.3% having less than 1 year of experience. There were both pharmacy-related (62.9%) and non-pharmacy related (37.1%) personnel involved in dispensing of medicines in the pharmacies. Pharmacy-related personnel were pharmacy assistants (39.1%), professionalists (19.6%) and pharmacists (4.2%) while non-pharmacy related personnel were from a medical field other than pharmacy (32%) and also non-medical background (5.1%).
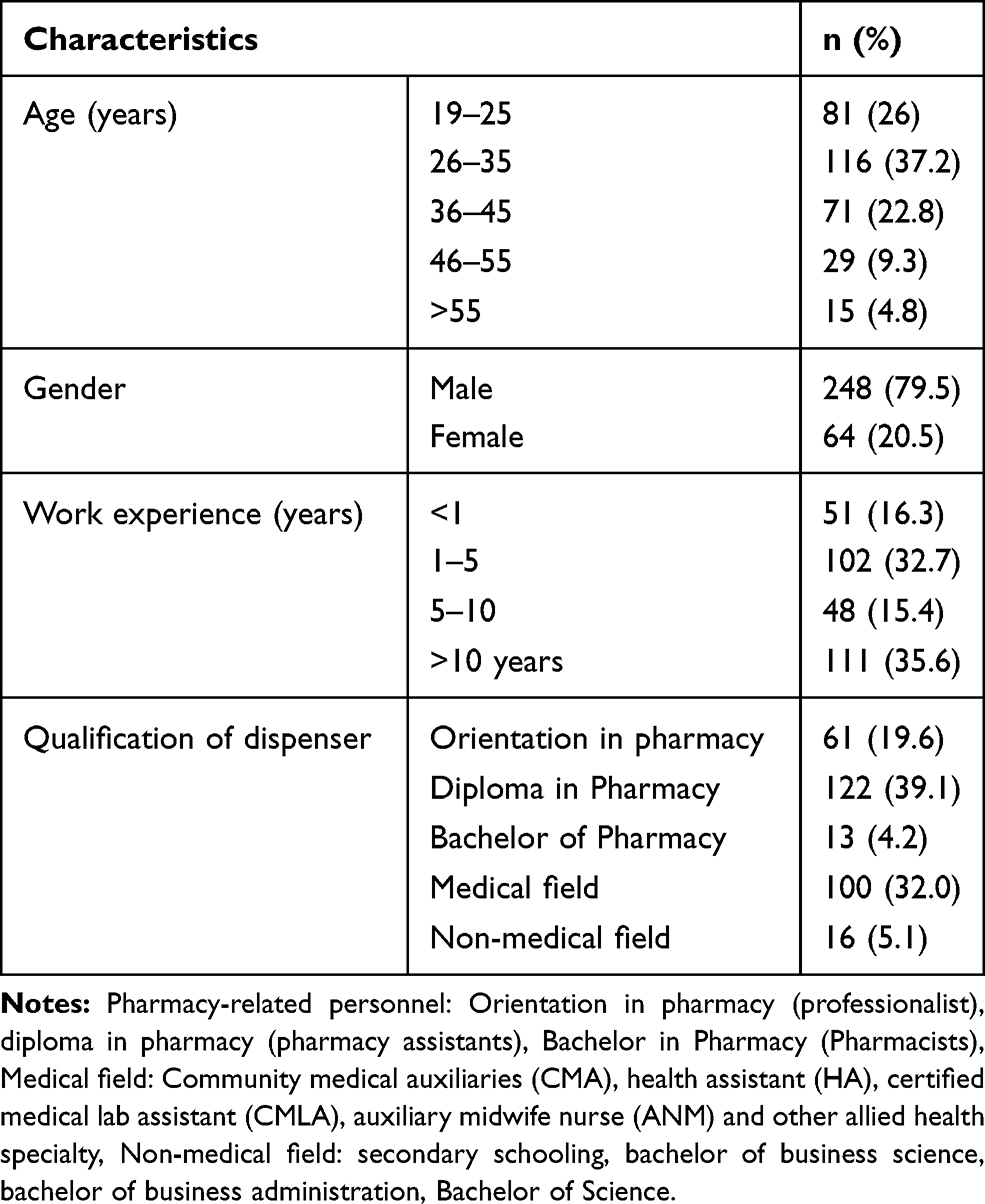 |
Table 1 Participant Characteristics (n=312) |
Understanding of Pharmacy Personnel Towards Antibiotic Dispensing
The level of understanding held by pharmacy personnel on the subject of antibiotic dispensing is presented in Table 2. 76.9% of the pharmacy personnel think that dispensing antibiotics without a valid prescription is a problem, 86.9% believe it is not legal practice. Most (86.5%) agree that pharmacy personnel should not dispense antibiotics without a valid prescription. Most respondents said they would ask the patients for a valid prescription (87.5%), about any history of drug allergies (73.1%) and about their use of any other medicines (89.7%) before dispensing antibiotics. 46.8% of participants said they would substitute for a different brand when the prescribed brand of antibiotic is not available in their pharmacy. However, 34.9% of respondents agreed that they dispense antibiotics without a prescription, 62.8% agreed that refusing to dispense antibiotics without prescription would negatively affect the sales and profits of the pharmacy, and 88.1% agreed that patients would try to obtain antibiotics from another pharmacy following refusal. In cases when a patient does not have sufficient money, a small proportion of the dispensers would replace the antibiotic with a cheaper brand (14.7%) but the majority would not dispense a full course (for complete duration) of antibiotic dosage regimen (85.3%). 94.5% of respondents said they would advise patients to adhere to their antibiotic dosage regimen to complete the course, while 65.4% would follow up with the patient after dispensing antibiotics. Only 26.9% of the participants disagreed with the statement that inappropriate dispensing of antibiotics could promote antimicrobial resistance and 34.3% agreed that antibiotics can reduce pain and inflammation.
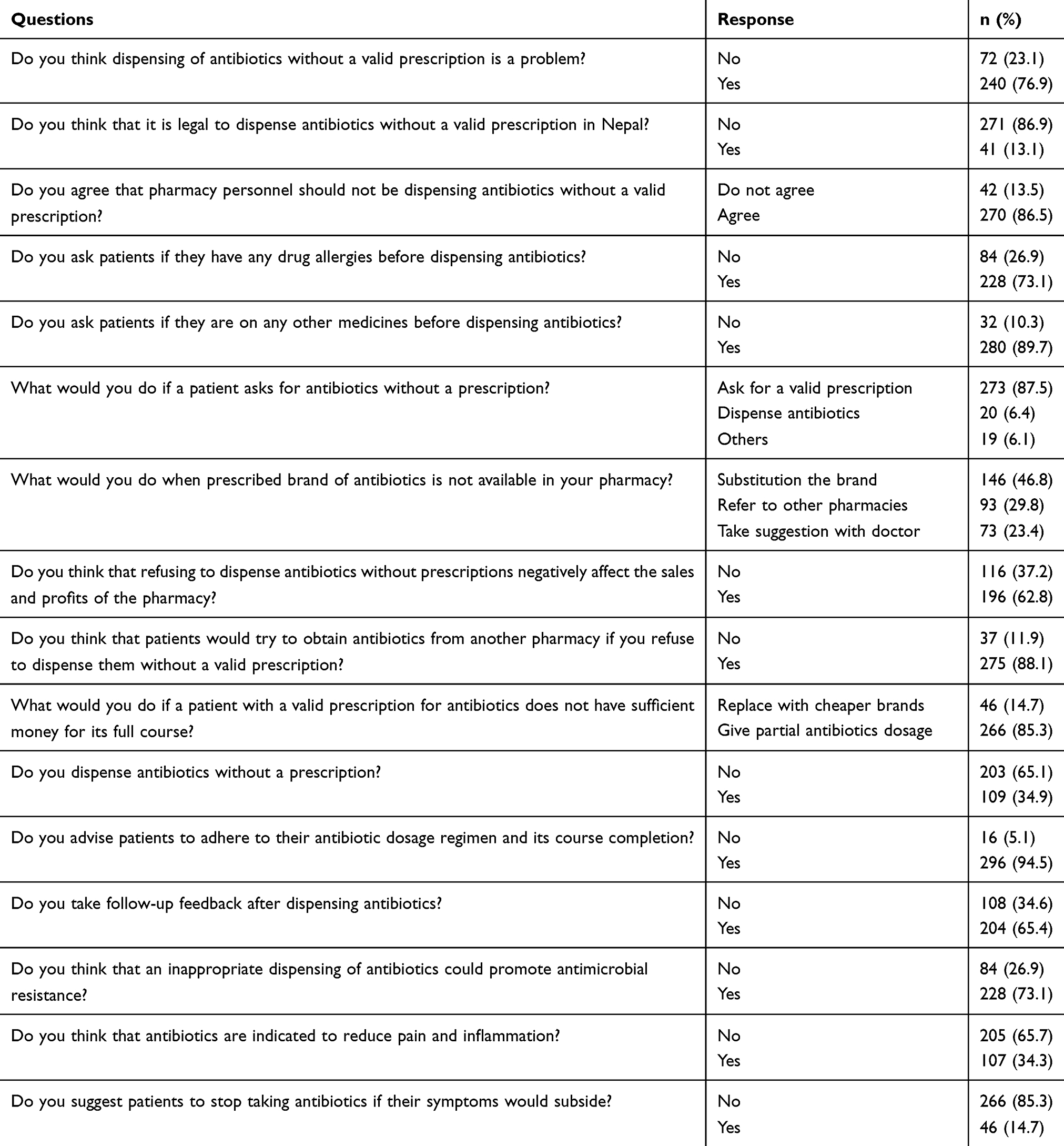 |
Table 2 Understanding of Pharmacy Personnel Towards Antibiotic Dispensing |
Relationship Between Participants’ Understanding of Antibiotic Dispensing and Participant Characteristics
Table 3 demonstrates that age, work experience and qualifications had independent and significant positive relationships with the understanding that antibiotics are not indicated to reduce pain and inflammation (p<0.001, P<0.001 and p=0.017, respectively). Work experience and qualifications were both associated with following up on patients after dispensing antibiotics (p<0.001 and p=0.042, respectively), and the understanding that inappropriate dispensing of antibiotics could promote antimicrobial resistance (p=0.018 and p=0.004, respectively). Age was independently associated with the practice of switching to a cheaper brand in cases where patients had insufficient money to purchase the full course of antibiotics (p=0.041). The level of qualifications held by participants was independently related to the practice of not dispensing antibiotics without a prescription (p=0.025) and work experience was related to the understanding of the legality of dispensing antibiotics without a valid prescription (p=0.016). Work experience was also associated with the practice of suggesting that patients should not stop taking antibiotics if their symptoms subside (p=0.003). Further detail about the relationships between gender, age group, work experience and qualifications are provided in Tables S1, S2, S3 and S4, respectively (Supplementary file 1).
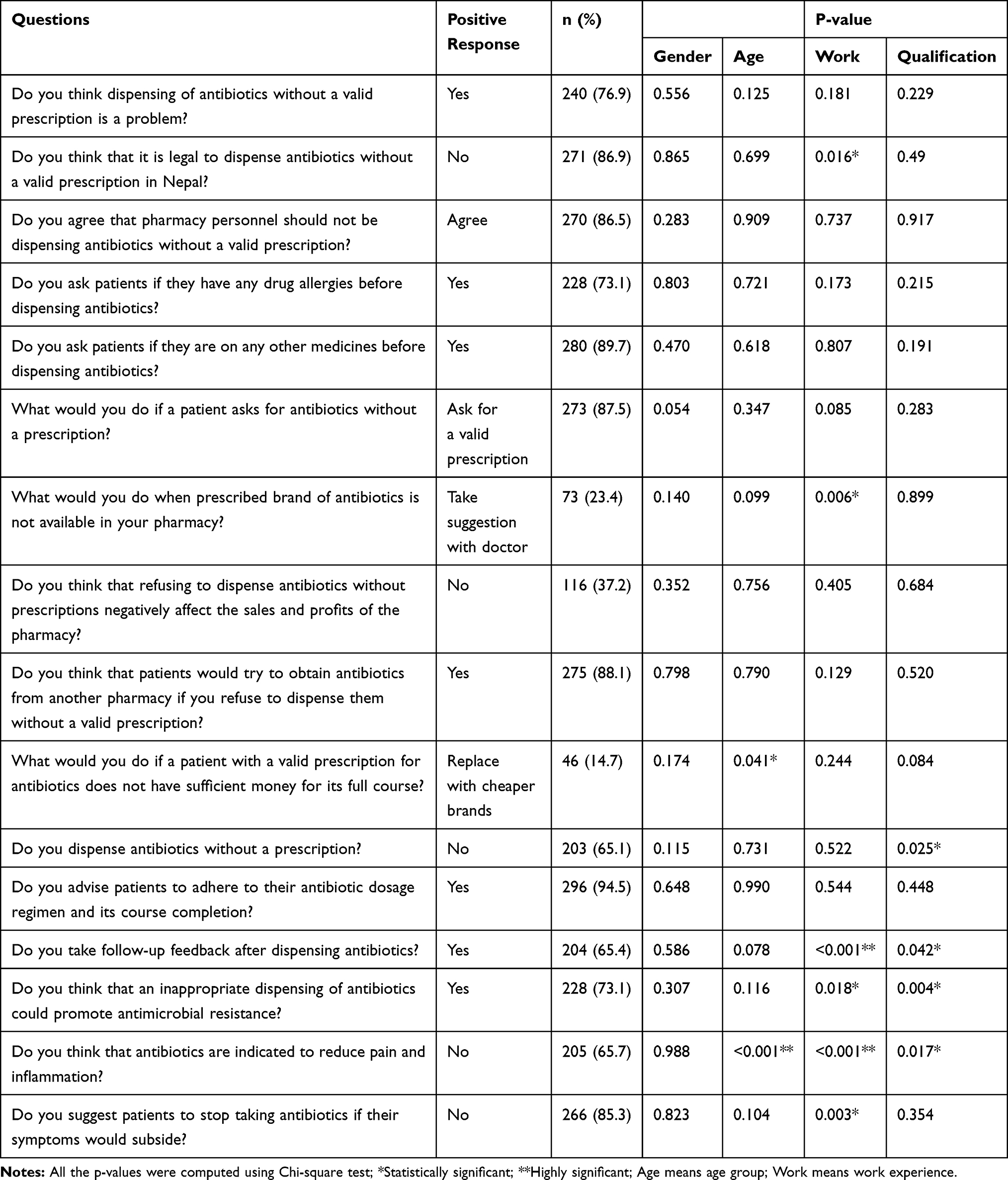 |
Table 3 Relationship Between Participants Understanding of Antibiotic Dispensing and Participant Characteristics |
Discussion
This study evaluated the understanding of pharmacy personnel in the field of antibiotic dispensing in three selected districts of Eastern Nepal. The findings suggested that the majority of pharmacy personnel were aware that non-authorized and non-prescription dispensing of antibiotics were legislatively restricted in Nepal, and that this was significantly related to the level of work experience (p=0.016) but not qualifications (p=0.49) of the personnel, as many respondents were paramedics and from non-medical fields. Paramedics such as community medicine auxiliaries (CMA) and health assistants (HA) undergo 18–36 months of medical training and have the authority to treat common illnesses, and to prescribe selected medicines, but do not have the legal authority to dispense medicines independently. In Nepal, the professional registration of pharmacists and assistant pharmacists (excluding professionalists) is provided by Nepal Pharmacy Council.31 The Drug Act 2035,23 formulated in 1978 still authorizes professionalists to run a community pharmacy,24,32 and as such, they are also legitimate pharmacy personnel in Nepal. Of our sample, 19.6% of participants were professionalists. Though the intention of our study was to characterize the range of qualifications held by pharmacy personnel, our finding shows that many non-pharmacy personnel have been providing community pharmacy services which distinctly reflects that the current regulations and monitoring by Nepalese legal authorities are extremely weak.
Our study suggests that around one-third of respondents dispense antibiotics without a prescription. This finding is in agreement with a study in Bara and Parsa districts of Nepal, where two-thirds of the pharmacy personnel did this.27 An earlier study in the capital city of Nepal also found that unauthorized dispensing by pharmacy staff is a foremost problem in community pharmacies.26 Dispensing of medicines by non-pharmacy professionals is often a consequence of a lack of adequate pharmacy resources, weak regulatory monitoring and unfounded practices, and has been observed in countries such as Ethiopia and China.16,33 Dispensing antibiotics without a prescription is another challenging problem and has been reported in several low and middle-income countries.5,6,28,29,34 The community pharmacy sector needs proper monitoring and supervision from enforcement agencies as well as the pharmacy council to stop untrained professionals from dispensing medicines and to curb the issue on inappropriate medicine use and increasing antimicrobial resistance at the community level. The majority of the pharmacy personnel in this study were aware that inappropriate dispensing of antibiotics could lead to antimicrobial resistance, and this awareness was significantly associated with both qualifications and work experience. We also found that most respondents thought that patients would try to obtain the antibiotics from another pharmacy if they were refused sale. This concurs with a study from Saudi Arabia.30 The practice of obtaining antibiotics without a prescription may be the consequence of unethical business practices in some pharmacies, or due to self-medication by some patients and/or their lack of awareness about the links between antibiotic use and resistance.35,36 Such practices will further promote the inappropriate use of medicines in society, cause adverse drug reactions, and contribute to antibiotic resistance.
Almost half of the pharmacy personnel would switch to a different brand of the same drug in the case of non-availability, and only 23.4% of pharmacy personnel would consult the prescribing doctor, which was significantly associated with work experience (p=0.006). This was similar to findings obtained in India where 56% of pharmacists would substitute brands in case of non-availability of medicines.28 Brand substitution should not alter the active pharmaceutical ingredients, dosage or strength, and should not compromise the safety, quality and performance characteristics of the medicine being dispensed. Although brand switching (proprietary to generic) may represent an appropriate alternative in many cases, there may be an associated risk that must be considered.37 The Pharmaceutical Society of Australia has brand substitution guidelines for pharmacists.38 These guidelines state that the health and safety of the patient should be the foremost concern if substitution has to occur, and that whenever possible, the same product should be supplied to patients on chronic therapy. Nepal may benefit from forming policy on the issue of brand substitution. The majority of pharmacy personnel would give a partial dose of the medicines if the patient had insufficient money for the full course. In low-income countries like Nepal, an out-of-pocket payment is the principal means of obtaining healthcare.3 Though the government has been working towards providing health and social security schemes since 2015, the implementation of such schemes is still a major challenge.39 Therefore, the perception by pharmacy personnel that an incomplete course of antibiotics can be given is more likely to affect patient compliance, and thus the overall outcome of the therapy. Furthermore, patients may stop taking antibiotics when the symptoms subside, also contributing to antibiotic resistance.9 Dispensing an incomplete course of antibiotics (or any medicine) is a problem unique to developing countries, where there is both financial hardship and a broad lack of awareness regarding rational antibiotic use.28 Addressing this problem requires comprehensive measures promoting both access to and quality of healthcare services and medicines.
In our study, 26.9% of the participants were unaware that inappropriately dispensing antibiotics could promote antimicrobial resistance. Likewise, one-third thought antibiotics can reduce pain and inflammation. This finding was in agreement with a study from Pakistan, where 31.5% of respondents disagreed that antibiotics misuse reduces antibiotic sensitivity towards specific pathogens, and 19.1% of these participants agreed that antibiotics were given for pain reduction and inflammation.29 Studies in Egypt have found that community pharmacists believed that antibiotics could be given for viral conditions such as colds and influenza.20,40 In our study, age, work experience and qualifications had a significant association with the positive perception about antibiotic indication (p<0.001 and p=0.017, respectively). However, above one third of respondents (34.3%) believed that antibiotics can be used to reduce pain and inflammation. This may reflect the low competency level of most pharmacy personnel in the community pharmacy setting. It is also possible that the non-pharmacy dispensing work force in the community pharmacy might have contributed to this incompetence. Nevertheless, it highlights the need for interventions such as education and awareness programs on the proper use of antibiotics, and for regulatory bodies to urgently improve their monitoring and supervision of pharmacies to prevent further increase of antimicrobial resistance.
We also noted some good practice compared with a previous study in two districts of Nepal, such as the intention to instruct that patients adhere to, and complete, the dosage regimen (94.5% vs 20%), and conducting follow-up on patients who have received antibiotics (65.4% vs 44%).27 This response was significantly related to both work experience and qualifications (p<0.001 and p=0.042, respectively). Patient follow-up after dispensing is an important task of community pharmacy personnel as it improves patient education, reduces medication errors, and improves safety.41 In addition, we found that pharmacy personnel were aware of the importance of completing a full course of antibiotics, as most respondents would not suggest that patients stop taking their medication when their symptoms subside, and that was found to be significantly associated with work experience (p=0.003). This shows that most community pharmacy personnel were invested in the health of their patients.
Conclusion
In a study involving 312 community pharmacy personnel in Eastern Nepal, the understanding of a significant number of respondents on the subject of antibiotic dispensing was poor, and needs improvement. The level of understanding about antibiotic indication was significantly associated with age, work experience and qualifications. Work experience and qualifications were also significantly related to respondents’ understanding about obtaining a follow-up feedback after dispensing antibiotics, and understanding the link between irrational antibiotic use and antimicrobial resistance.
Strengths and Limitations
One of the limitations is that we used a self-administered questionnaire to collect data, which relied on the recall and cognitive abilities of respondents. This could introduce recall bias and/or response bias. Another limitation is that as we conducted this study in just three districts of Eastern Nepal, the findings may not be generalizable. We also could not assess the impact of AMS training on responses due to unavailability of AMS training records at the community level. We did not conduct a predictive analysis, and as such, cannot adjust for the co-dependence of variables. Despite these limitations, to the best of our knowledge, this is probably the first study to assess the understanding surrounding antibiotic dispensing practice of community pharmacy personnel in Eastern, Nepal.
Recommendations for Practice and Policy
Our study revealed that a significant proportion of pharmacy personnel were from non-pharmacy backgrounds. This highlights that community pharmacies are violating the legal obligation that these pharmacies must be managed by authorized pharmacy personnel. The regulatory bodies need to urgently address this issue as this may contribute to irrational antibiotic use. The Nepalese government needs to initiate policy for antimicrobial stewardship and instigate programs for the improvement of rational antimicrobial use, in order to minimize harm to patients and reduce the risks of antimicrobial resistance.
Data Sharing Statement
Raw and analyzed study data are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
Ethical approval was obtained from the Ethical Review Board of Nepal Health Research Council (Reg No 82/2019 Ref: 2500), Kathmandu, Nepal. Each participant provided a verbal consent followed by a written consent prior to the data collection.
Acknowledgments
The authors are grateful to Dr. Rebeca Dewey (University of Nottingham, Nottingham, United Kingdom), Dr. Roger Watson (University of Hall, Hull, United Kingdom) and Dr. P Ravi Sankhar (Oceania University of Medicine, Florida, United States) for their English editing. We would like to kindly thank all the faculty members of Purbanchal University College of Medical and Allied sciences (Gothgaun, Morang, Nepal), especially, Dr. Sailesh Mani Pokhrel (Dean, Faculty of Medicine), Dr. Kajiram Adhikari (Program Head, Department of Pharmacy), Mrs. Kabita Adhikari (Campus chief) for their motivation and support in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Abdulah R. Antibiotic abuse in developing countries. Pharmaceut Reg Affairs. 2012;1:2. doi:10.4172/2167-7689.1000e106
2. Hart CA, Kariuki S. Antimicrobial resistance in developing countries. BMJ. 1998;317(7159):647–650. doi:10.1136/bmj.317.7159.647.
3. Mills A. Health care systems in low- and middle-income countries. N Engl J Med. 2014;370(6):552–557. doi:10.1056/NEJMra1110897
4. Atif M, Asghar S, Mushtaq I, et al. What drives inappropriate use of antibiotics? A mixed methods study from Bahawalpur, Pakistan. Infect Drug Resist. 2019;12:687–699. doi:10.2147/IDR.S189114
5. Mboya EA, Sanga LA, Ngocho JS. Irrational use of antibiotics in the moshi municipality Northern Tanzania: a cross sectional study. Pan Afr Med J. 2018;31:165. doi:10.11604/pamj.2018.31.165.15991.
6. Morgan DJ, Okeke IN, Laxminarayan R, Perencevich EN, Weisenberg S. Non-prescription antimicrobial use worldwide: a systematic review. Lancet Infect Dis. 2011;11(9):
7. Llor C, Bjerrum L. Antimicrobial resistance: risk associated with antibiotic overuse and initiatives to reduce the problem. TherAdv Drug Saf. 2014;5(6):229–241. doi:10.1177/2042098614554919.
8. AdHoc Interagency Coordination Group on Antimicrobial Resistance, No time to wait: securing the future from drug resistant infection. Summary report to secretary general general of united nation; APRIL 2019. Available from https://www.who.int/antimicrobial-resistance/interagency-coordination-group/final-report/en/.
9. Basnyat B, Pokharel P, Dixit S, Giri S. Antibiotic use, its resistance in Nepal and recommendations for action: a situation analysis. J Nepal Health Res Counc. 2015;13(30):102–111.
10. National antibiotic treatment guidelines. Ministry of health and population. Kathmandu, Nepal: Government of Nepal; 2014. Available from https://www.publichealthupdate.com/national-antibiotic-treatment-guideline-2014/.
11. Acharya KP, Wilson RT. Antimicrobial resistance in Nepal. Front Med. 2019;6:105. doi:10.3389/fmed.2019.00105
12. Dahal RH, Chaudhary DK. Microbial infections and antimicrobial resistance in Nepal: current trends and recommendation. Open Microbiol J. 2018;12:230–242. doi:10.2174/1874285801812010230
13. Okuyanv B, Savan MA, Izzettin FV, Sancar M. Evaluation of rational antibiotic dispensing in the community pharmacy setting: a simulated patient study. Acta Pharm Sci. 2017;55(2):7–15.
14. Bin Abdulhak AA, Altannir MA, Almansor MA, et al. Non prescribed sale of antibiotics in Riyadh, Saudi Arabia: a cross sectional study. BMC Public Health. 2011;11:538. doi:10.1186/1471-2458-11-538
15. Fakhir TA, Attiah AK, Mesfer SA, Hassan AA. Community pharmacists’ knowledge, attitude and practices towards dispensing antibiotics without prescription. Egypt J Hosp. 2018;70(7):1234–1237. doi:10.12816/0044556
16. Chang J, Ye D, Lv B, et al. Sale of antibiotics without a prescription at community pharmacies in urban China: a multicentre cross-sectional survey. J Antimicrob Chemother. 2017;72(4):
17. Nepal A, Hendrie D, Robinson S, et al. Survey of the pattern of antibiotic dispensing in private pharmacies in Nepal. BMJ Open. 2019;9:e032422. doi:10.1136/bmjopen-2019-032422
18. Vazquez-Lago J, Gonzalez-Gonzalez C, Zapata-Cachafeiro M, et al. Knowledge, attitudes, perceptions and habits towards antibiotics dispensed without medical prescription: a qualitative study of Spanish pharmacists. BMJ Open. 2017;7(10):e015674. doi:10.1136/bmjopen-2016-015674
19. WHO. Antibiotic resistance: multi-country public awareness survey. Available from: https://apps.who.int/medicinedocs/documents/s23688en/s23688en.pdf.
20. Zakaa El-Din M, Samy F, Mohamed A, Hamdy F, Yasser S, Ehab M. Egyptian community pharmacists’ attitudes and practices towards antibiotic dispensing and antibiotic resistance; a cross-sectional survey in Greater Cairo. Curr Med Res Opin. 2019;35(6):
21. Roque F, Soares S, Breitenfeld L, López-Durán A, Figueiras A, Herdeiro MT. Attitudes of community pharmacists to antibiotic dispensing and microbial resistance: a qualitative study in Portugal. Int J Clin Pharm. 2013;35(3):
22. Mikrani R, Naveed M, Mikrani A, et al. The impact of clinical pharmacy services in Nepal in the context of current health policy: a systematic review. J Public Health. 2020;28;:245–255. doi:10.1007/s10389-019-01042-y
23. Government of Nepal, Department of drug administration. Drug act; 2035. Available from: http://dda.gov.np/content/drugs-act-2035.
24. Government of Nepal, Department of drug administration. Drug standard regulation; 2043. Available from: http://dda.gov.np/content/drug-standard-regulation-2043.
25. Getting AMR into plans and budgets of government and development partners Nepal country report. Available from: https://www.who.int/antimicrobial-resistance/national-action-plans/Nepal-AMR-integration-Report-WHO-Sept-2018.pdf. Accessed july 2020
26. Wachter DA, Joshi MP, Rimal B. Antibiotic dispensing by drug retailers in Kathmandu, Nepal. Trop Med Int Health. 1999;4(11):
27. Ansari M. Evaluation of community pharmacies regarding dispensing practices of antibiotics in two districts of central Nepal. PLoS One. 2017;12(9):e0183907. doi:10.1371/journal.pone.0183907
28. Soumya R, Devarashetty V, Jayanthi CR, Sushma M. Drug dispensing practices at pharmacies in Bengaluru: a cross-sectional study. Indian J Pharmacol. 2016;48(4):
29. Sarwar MR, Saqib A, Iftikhar S, Sadiq T. Knowledge of community pharmacists about antibiotics, and their perceptions and practices regarding antimicrobial stewardship: a cross-sectional study in Punjab, Pakistan. Infect Drug Resist. 2018;11:
30. Hadi MA, Karami NA, Al-Muwalid AS, et al. Community pharmacists’ knowledge, attitude, and practices towards dispensing antibiotics without prescription (DAwP): a cross-sectional survey in Makkah Province, Saudi Arabia. Int J Infect Dis. 2016;47:95–100. doi:10.1016/j.ijid.2016.06.003
31. https://nepalpharmacycouncil.org.np/.
32. https://ncda.org.np/organizational-profile/.
33. Lenjisa JL, Mosisa B, Woldu MA, Negassa DE. Analysis of dispensing practices at community pharmacy settings in Ambo Town, West Shewa, Ethiopia. J Community Med Health Educ. 2015;5:329. doi:10.4172/2376-0214.1000329
34. Erku DA, Aberra SY. Non-prescribed sale of antibiotics for acute childhood diarrhea and upper respiratory tract infection in community pharmacies: a 2 phase mixed-methods study [published correction appears in antimicrob resist infect control. 2019 Jan 11;8:10]. Antimicrob Resist Infect Control. 2018;(7):92. doi:10.1186/s13756-018-0389-y
35. Topor G, Grosu IA, Ghiciuc CM, Strat AL, Lupuşoru CE. Awareness about antibiotic resistance in a self-medication user group from Eastern Romania: a pilot study. Peer J. 2017;5:e3803. doi:10.7717/peerj.3803.
36. Darwish DA, Abdelmalek S, Abu Dayyih W, Hamadi S. Awareness of antibiotic use and antimicrobial resistance in the Iraqi community in Jordan. J Infect Dev Ctries. 2014;8(5):616–623. doi:10.3855/jidc.4086.
37. Straka RJ, Keohane DJ, Liu LZ. Potential clinical and economic impact of switching branded medications to generics. Am J Ther. 2017;24(3):e278–e289. doi:10.1097/MJT.0000000000000282.
38. Pharmaceutical Society of Australia. Guidelines for pharmacists on PBS brand substitution. Australian Pharmacist. 2004;23(9):668.
39. Mishra SR, Khanal P, Karki DK, Kallestrup P, Enemark U. National health insurance policy in Nepal: challenges for implementation. Glob Health Action. 2015;8:28763. doi:10.3402/gha.v8.28763.
40. Abdelaziz AI, Tawfik AG, Rabie KA, et al. Quality of community pharmacy practice in antibiotic self-medication encounters: a simulated patient study in upper Egypt. Antibiotics. 2019;8(2):35. doi:10.3390/antibiotics8020035.
41. WHO. The role of pharmacist in encouraging prudent use of antibiotic medicines and averting antimicrobial resistance: a review of current policies and experiences in Europe. Available from: http://www.euro.who.int/__data/assets/pdf_file/0006/262815/The-role-of-pharmacist-in-encouraging-prudent-use-of-antibiotics-and-averting-antimicrobial-resistance-a-review-of-policy-and-experience-Eng.pdf.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.