")
Back to Journals » Nutrition and Dietary Supplements » Volume 11
Community Pharmacists’ Knowledge, Attitude, and Professional Practice Behaviors Towards Dietary Supplements: Results from Multi-Center Survey in Ethiopia
Authors Emiru YK , Belay YB, Bizuneh GK , Tegegn HG
Received 5 July 2019
Accepted for publication 23 November 2019
Published 6 December 2019 Volume 2019:11 Pages 59—68
DOI https://doi.org/10.2147/NDS.S222114
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chandrika J Piyathilake
Yohannes Kelifa Emiru,1 Yared Belete Belay,2 Gizachew Kassahun Bizuneh,1 Henok Getachew Tegegn1
1School of Pharmacy, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia; 2School of Pharmacy, College of Health Sciences, Mekelle University, Mekelle, Ethiopia
Correspondence: Yohannes Kelifa Emiru
School of Pharmacy, College of Medicine and Health Science, University of Gondar, P.O. Box: 196, Gondar, Ethiopia
Email [email protected]
Background: The utilization of dietary supplement (DS) is dramatically increasing across the globe, but knowledge of the community pharmacists regarding these products has not been well studied. As to the best of the authors’ knowledge, there is no previous study explored community pharmacists knowledge, attitude, and practice (KAP) towards DS in Ethiopia context. Hence, this study was undertaken to assess KAP of the community pharmacist about DS.
Methods: A cross-sectional multi-center survey of community pharmacists in different cities of Ethiopia was conducted over a period of five months from January to May 2019. The survey evaluated demographic information and KAP of participants related to DS. A stratified random sample of registered pharmacy practitioners all over the country was chosen to respond to the survey. Descriptive and inferential statistics were performed. The result was considered significant if P < 0.05.
Results: Of the 672 surveys distributed, 608 pharmacists accepted to participate in the study with a response rate of 90.47% and only 600 met the inclusion criteria for further evaluation. Of pharmacists surveyed, 66.7% had adequate knowledge while 53.7% of the pharmacists were within a positive attitude range and lower proportion (41.2%) of pharmacists were found within the good practice range about DS. Age, education level, experience, and position in community pharmacies were significantly associated with KAP. Significant positive linear correlations between knowledge-attitude (r =0.471, p < 0.001), knowledge-practice (r = 0.546, p < 0.001), and attitude-practice (r = 0.741, p < 0.001) were also found.
Conclusion: The finding of this survey suggested that the majority of pharmacists had poor professional practice towards DS in spite of having adequate knowledge and a positive attitude regarding DS. Emphasis should be given to teaching/training community pharmacists how to critically evaluate the use, efficacy, and safety of common DS.
Keywords: beliefs, community pharmacists, dietary supplements, knowledge, practice, Ethiopia
Background
Due to the significant health care burden of chronic diseases, the World Health Organization (WHO) recommends dietary supplements (DS) may be useful to improve health in some situations.1,2 Complementary and alternative medicine (CAM) could be defined as a group of diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine.3 According to Dietary Supplement Health and Education (DSHEA), DS are defined as a wide array of non-food and non-drug substances intended to supplement the diet but are not proposed to treat human diseases. These agents might constitute one or more dietary ingredients, such as mineral, vitamin, herbal preparation, amino acid, or a mixture of these ingredients,4 which may provide a valuable health benefit for patients with chronic diseases. The consumption of calcium and vitamin D, for example, improves bone mineral density and prevents fracture in patients with osteoporosis,5 and the use of fish oil or other omega-3 fatty acid supplements prevents the rate of mortality in patients with cardiovascular disease.6
The American Society of nutrition reports the consumption of DS by a large proportion of the population in their day to day life.7 Both in Japan and the US, higher than 50% of the adult population have evidenced using DS.8,9 More than 80% of the physicians and nurses recommended a different DS product to their clients.10 Though the intake of these products suggested by the majority of health care providers, the frequent habit of consuming DS by a wide range of population may create the potential for misinformation, underestimation of side-effects, and drug-supplement/herbal interactions. A majority of consumers have less piece of information regarding the contents and properties of DS product. As a result of this, numerous studies highlighted health risks of using DS11–13 as well as development potential drug interaction between DS product and prescription drugs.14 Almost all customers get access to various DS products from the drug retail outlets (DRO) of community pharmacy. In Ethiopia, these DROs were established through an accreditation system to ensure the quality of their service, thereby protecting society.15 Pharmacists have an imperative role regarding appropriate use of DS in health care through an effective prescription cycle, and provision of correct information. Thus, knowledgeable pharmacists are highly warranted to counsel and educate patients regarding safe usage of this product.16–18
In most of the encounters, patients expect to be able to access an extensive range of information about DS products from community pharmacies.19 A recent survey in Australia showed about 87% of the consumers expected pharmacists to answer about the effectiveness of DS and 92% of them expected to receive safe information about these products.20 However, the majority of pharmacists′ have inadequate knowledge about DS and less self-confidence to answer patients’ questions.21 Similarly, one systematic review reported that the global knowledge of the community pharmacists regarding these products does not increase in parallel to growing sales of DS.16 Some of the speculated reasons that contribute to the inadequacy of information were inadequate training and non-corporation of counseling program about DS in a curriculum of pharmacy as well as unavailability of approved resources.21,22
Numerous published articles investigated the level of attitudes and knowledge of community pharmacist regarding CAM,23–27 but little has been explored to assess the knowledge, attitude, and practice (KAP) of community pharmacists towards DS alone.18,28 As to the best of the authors′ knowledge, there is no study considering pharmacists KAP towards DS in Ethiopia context. Therefore, the main objective of this study was to assess the KAP of community pharmacists in Ethiopia about DS.
Methods
Study Area, Design, Period, and Population
A cross-sectional multi-center survey of community pharmacists in different cities of Ethiopia was conducted over a period of five months from January to May 2019. Ethiopia is a Federal Democratic Republic composed of nine National Regional states: namely Tigray, Afar, Amhara, Oromia, Somali, Benishangul-Gumuz, Southern Nations Nationalities and People Region (SNNPR), Gambella, and Harari, and Two Administrative states (Addis Ababa city administration and Dire Dawa city council). The current population of Ethiopia is 109,097,936 as of Friday, February 9, 2019 based on the latest United Nations estimates. The research mainly focussed on the capital of the city of the country and cities with the highest population.
Sample Size and Sampling Procedure
A stratified random sampling with stratification based on geographic location was used for the selection of participants from six main cities in the country: Addis Ababa, Mekelle, Gondar, Bahir Dar, Hawassa, and Mizan-Teppi. The target population was pharmacy professionals who have been working in community pharmacies and drug stores of these cities. Eligible respondents were those who were Ethiopian nationals, willing to participate and provided verbal consent, filled and answered all questions. A stratified random sample of 672 registered pharmacy practitioners all over the country was chosen to respond to the survey. A proportional number of community pharmacies in Ethiopia were randomly selected for this survey according to their geographical distribution (ie, north, south, east, and west). The selection of facilities was done at random with a clear intention to include different areas of the country. Non-respondents were visited to return their questionnaire. All returned working questionnaires were completed anonymously. Details of the number of participants recruited from each city are presented in Figure 1.
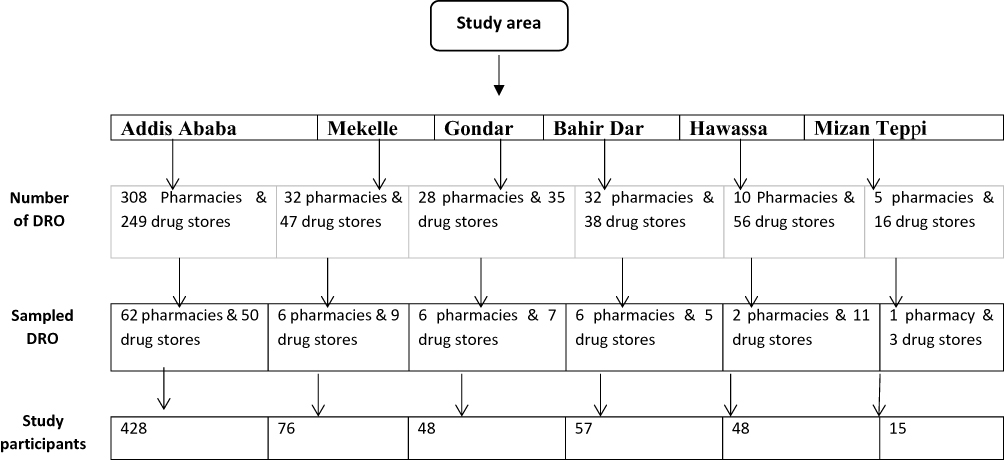 |
Figure 1 Sampling procedures and the number of individuals selected from each city. Abbreviation: DRO, drug retail outlets. |
Data Collection Tool
The questionnaire was designed and developed from a review of the literature and previous study relating to pharmacists KAP regarding DS.28 The survey questions were pre-tested by a pharmacist with an extensive experience in DS. The questionnaire was piloted on a convenient sample of 20 practicing pharmacists to check for understandability, time consumed by each question, and consistency among related variables. Grounded on the result of this pilot study, the questionnaire was used with little modifications and the final questionnaire was sent to the participants through handling by face to face.
The survey consisted of two parts: Part I: five questions related to a sociodemographic characteristic of the pharmacists’. This section comprised demographic information on age, gender, education level, experience, and position of practicing pharmacists in community pharmacy. Part II: KAP questionnaire related to DS which is presented in Table 3. The questions consisted of close-ended dichotomized (Yes/No) response. Knowledge section consists seven items and measured with a score of “1” for yes response and “0” for no response. Knowledge scores for individuals were calculated and summed up to give the total knowledge score. The total knowledge score ranged from 0 to 7; a score of ≥4 was considered to reflect adequate knowledge. Questions assessing attitudes towards DS were also close-ended (Yes/No) items which consisted of eight questions. A score of “1” awarded for yes response and “0” for no response. The value ranged from 0 to 8; a score of >4 was considered to reflect a positive attitude. The practice was assessed by asking ten questions towards DS and the responses were dichotomized (Yes/No). A score of “1” is given for yes responses and “0” for no responses. The cut off value of >5 was considered to reflect a good practice towards DS.
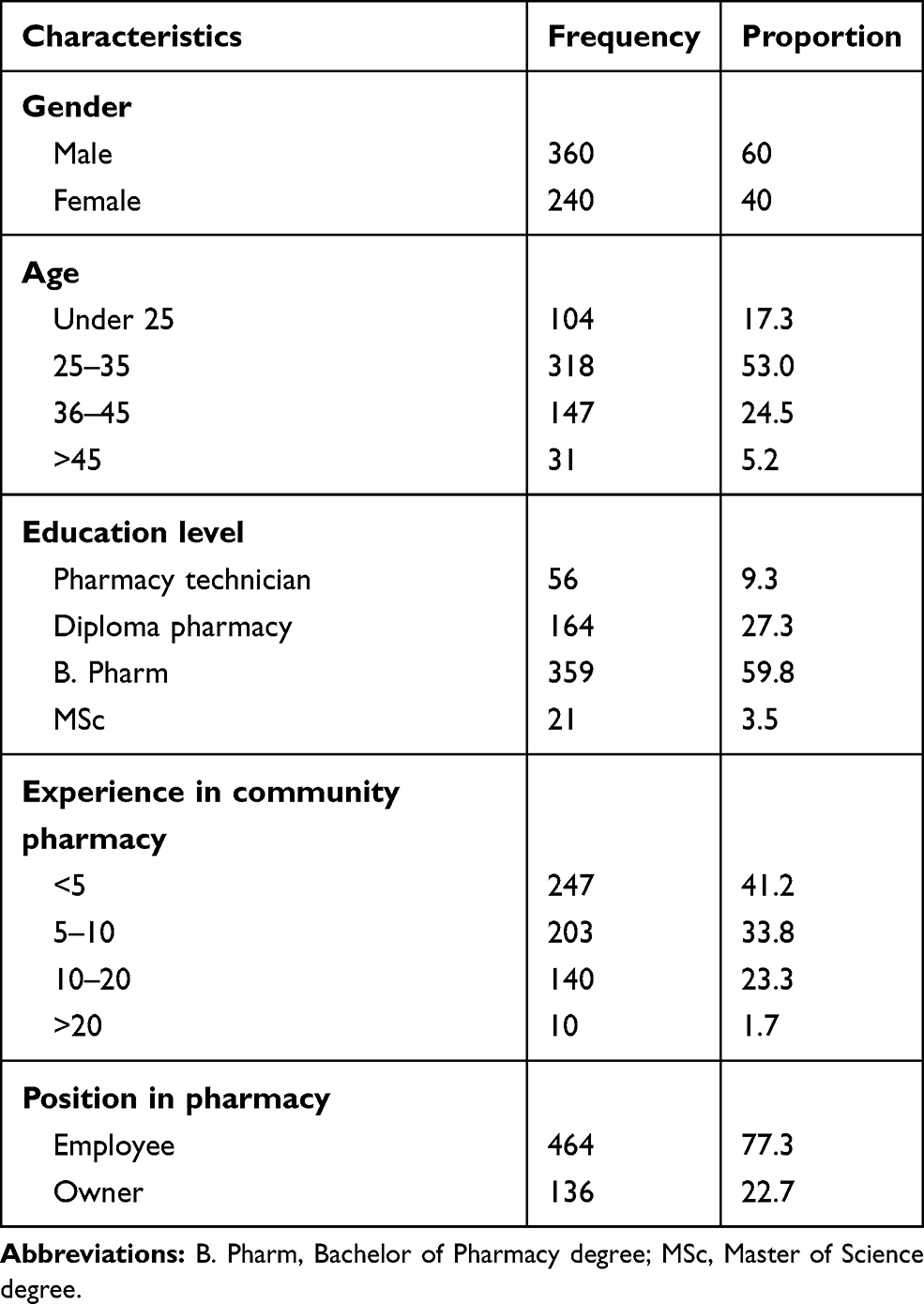 |
Table 1 Demographic Characteristics of the Study Respondents (N = 600) |
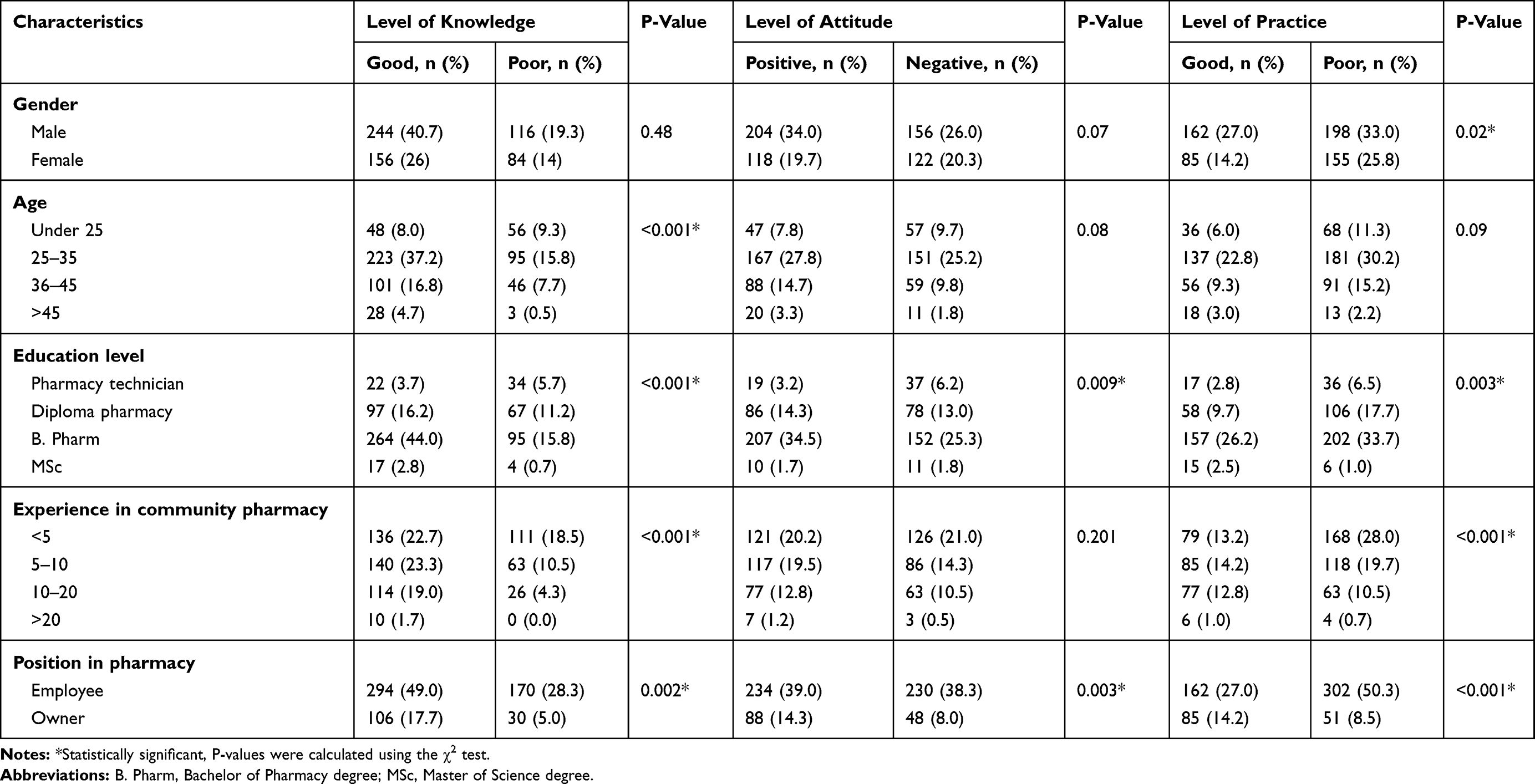 |
Table 2 Distribution of the Level of Knowledge, Attitude and Practices Towards Dietary Supplements Across Demographic Characteristics (N = 600) |
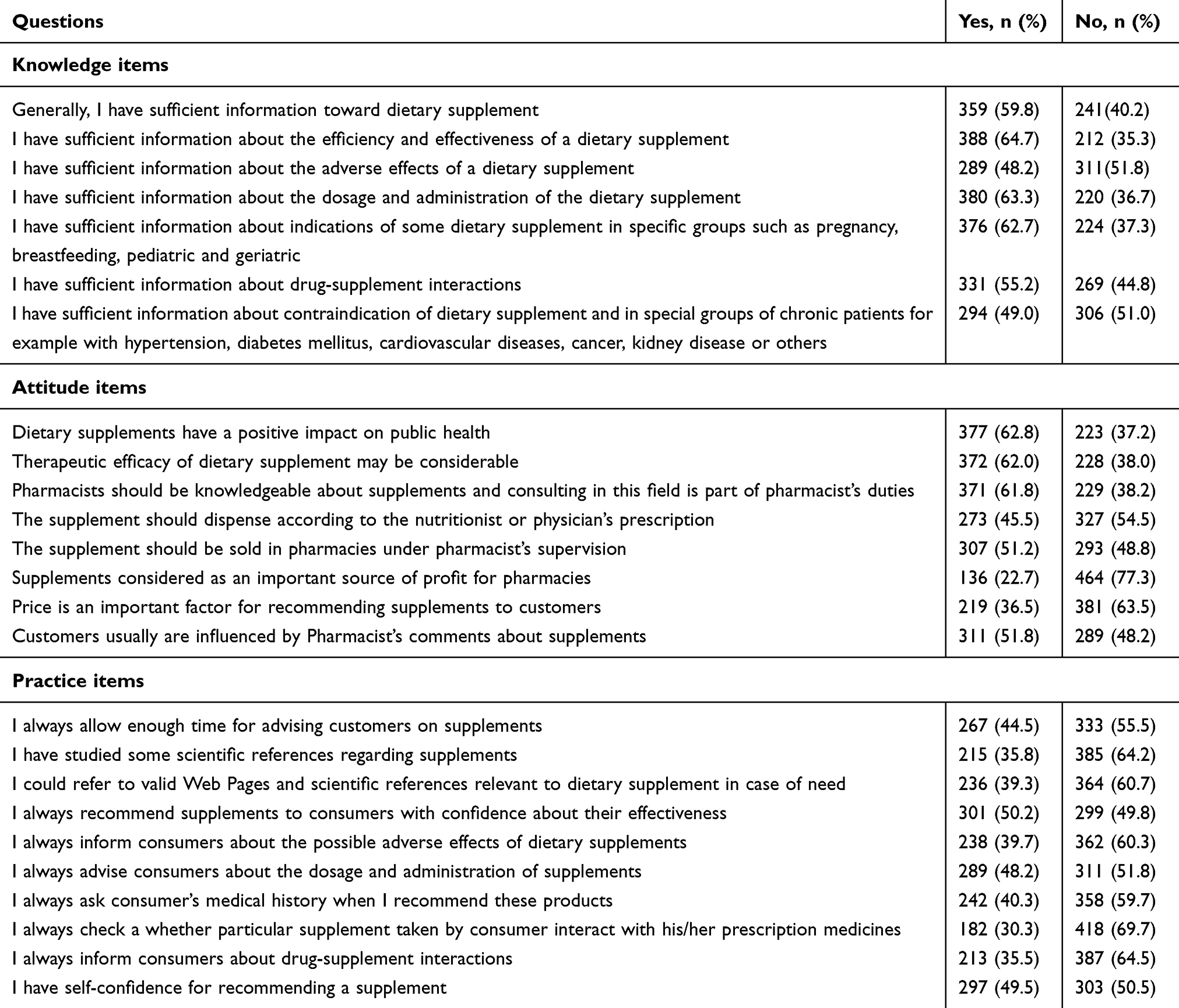 |
Table 3 Descriptive Analysis of Knowledge, Attitude, and Practice Questionnaire |
Ethical Approval
The study protocol was reviewed and approved by University of Gondar, School of Pharmacy, Ethical Review Board. Furthermore, verbal informed consent from the participants was approved by the University of Gondar, School of Pharmacy, Ethical Review Board to keep the decision-making autonomy of the participants. No identifier was mentioned in the data abstraction tool, and the raw data were not used for other purposes or shared for the third party.
Data Processing and Analysis
Data were checked every day for its completeness, edited, cleaned, and analyzed using the Statistical Package for Social Sciences (SPSS) version 21 for Windows (SPSS Inc., Chicago, IL) to run all statistical analysis with a P-value < 0.05 indicating significant differences. Descriptive analysis summarizing respondents’ demographic information with frequencies and proportions were reported using tables and text. Inferential statistics (Mann–Whitney U-test and Kruskal–Wallis tests) were performed to identify the main socio-demographic factors associated with pharmacists’ KAP towards DS. The strength and direction of the relationship among respondents’ KAP related to DS were examined by Spearman Rank Correlation Coefficient.29
Results
Demographic Characteristics of the Respondent Pharmacists
Table 1 summarizes the demographic characteristic of the pharmacists. Of a total of 672 community pharmacists approached, 608 pharmacists accepted to participate in the study with a response rate of 90.47%. About 600 pharmacists met the inclusion criteria and were included in the analysis. More than half of the respondents were male (n = 360, 60.0%). Majority of them belong to the age group of 25–35 years (53.0%), while a slightly smaller number (n = 31, 5.2%) were in the age group of greater than 45. Concerning the years of experience, 247 (41.2%) participants had less than five years, and 203 (33.8%) had between 5–10 years of experience while a few of them (n = 10, 1.7%) had 20 or more years of experience.
Distribution of KAP Level Towards DS Across Demographic Variables
The majority of the community pharmacists (400 (66.7%)) showed adequate knowledge whereas 200 (33.3%) had poor knowledge level. In the present study, 322 (53.7%) of pharmacists were within a positive attitude range, whereas 278 (46.3%) showed a negative attitude about DS. Regarding practice assessment towards DS, a lower proportion (247, 41.2%) of pharmacists were found within the good practice range. However, the majority (353, 58.8%) of the respondents showed poor practice towards DS. Table 2 clearly shows the distribution of KAP regarding DS according to gender, age, education level, and experience in community pharmacy and position in pharmacy. Furthermore, Table 3 illustrates descriptive parameters including frequency and percentage corresponding to each KAP question. As can be seen from the data in Table 2, men and women did not differ in knowledge and attitudes, but men were more likely to have good practice compared to women. Pharmacists aged between 25 and 35 were more likely to have a good knowledge than under 25 and older pharmacists. However, there is no significant difference in attitude and practice between age groups.
Association of Demographic Characteristics and Mean KAP Scores
The association of demographic characteristics and mean KAP scores is summarized in Table 4. Mann–Whitney test was employed to compared pharmacists′ KAP mean score about DS between male and female and employee and owner pharmacist. No significant differences were observed between male and female KAP responses, with p values being greater than 0.05, but a significant difference was observed between employee and owner pharmacist (p = <0.001). Besides, a significant difference in mean KAP scores value was found between pharmacists according to age group, educational level, and experience in the community pharmacy (Kruskal–Wallis test; p-value < 0.05). Pharmacists aged >45 had a higher mean score of KAP than younger pharmacists. Furthermore, pharmacists with a master degree scored a higher mean score of knowledge and practice that pharmacists with a bachelor degree, diploma pharmacist, and pharmacy technician. The study revealed that the mean score of KAP increased as the pharmacists’ experience increased.
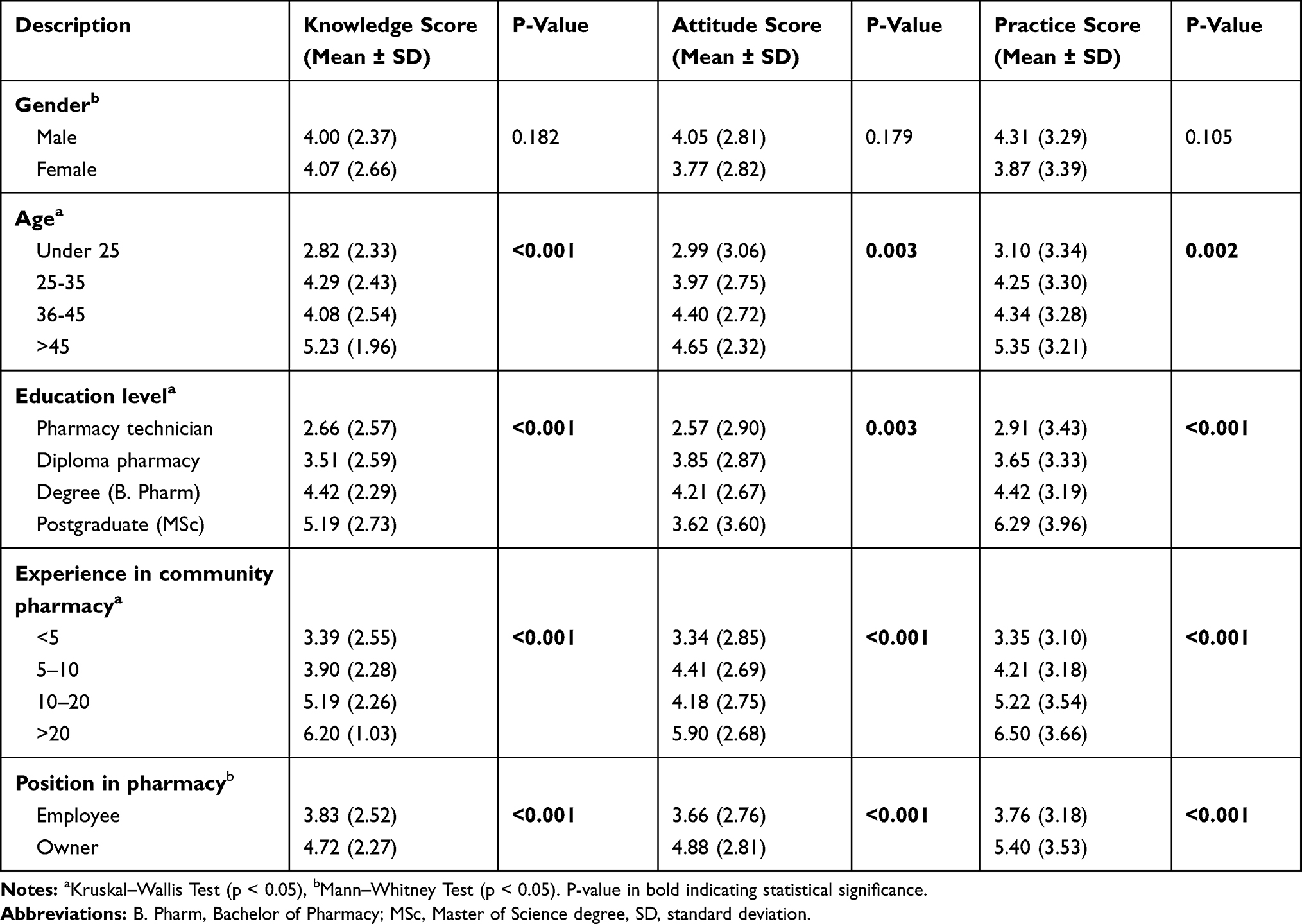 |
Table 4 Mean Scores of Knowledge, Attitude, and Practice |
Correlation Between KAP
Spearman rank correlation revealed significant positive linear correlations between knowledge-attitude (r =0.471, p < 0.001), knowledge-practice (r = 0.546, p < 0.001), and attitude-practice (r = 0.741, p < 0.001). As shown in Table 5, there were significant correlations between knowledge and attitude, between knowledge and practice, and between attitude and practice.
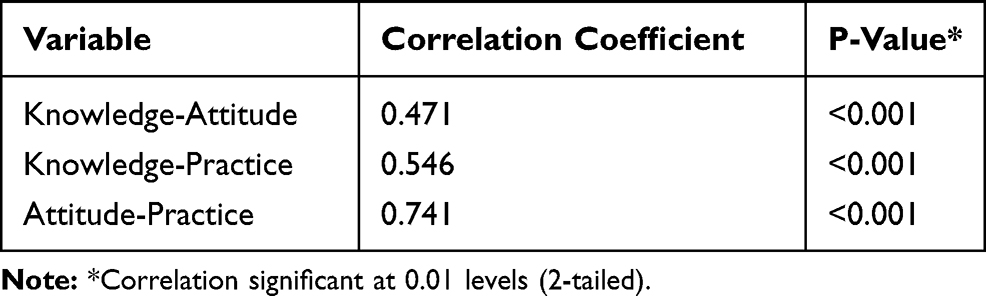 |
Table 5 Correlation Between Knowledge, Attitude, and Practice Scores |
Discussion
Globally, the use of DS has been rapidly growing.30 The high use of herbal remedies has been reported in Ethiopia.31 The increasing demands for DS highly needed a great insight of pharmacists on DS.32 Therefore, this study sought to examine the level of KAP of community pharmacist regarding DS in Ethiopia.
A recent systematic review showed that community pharmacist knowledge of DS is generally poor despite having a professional responsibility to provide consultation about DS to clients.16 Similarly, this study found 33.3% of the participants described their knowledge about DS as poor which is consistent with another study done in Ethiopia (27.7%)26 and a study done elsewhere by Kheir et al (30%).33 However, a higher proportion of poor knowledge was obtained in other studies ranging from 40% to 62%.17,28,34 Poor knowledge among community pharmacists might be owing to different factors. The pharmacy curriculum in Ethiopia does not embrace specific DS courses thus far. Moreover, a systematic review done in US and Canada revealed that there had been a lack of quality information on DS,19 and such lack of evidence in the efficacy of some of the DS6 may also play its part for the poor DS knowledge among community pharmacists.
The current study also examined community pharmacists′ perceived knowledge on adverse effects, indications, drug–supplement interactions, and contraindication of DS. About 48.2% of the participants responded that they have adequate information about the adverse effects of DS. The comparable finding was found in other studies.26,35 However, this study has a higher proportion of participants who knew about the general safety of traditional medicine products and side effects with respect to those reported by Shraim et al study (24.2%)27 but lower than the finding reported by Chen et al study (64.9%).34 The results of Mehralian et al28 showed that the average knowledge score had a significant difference in terms of gender. In other words, men participants were more knowledgeable than women participants towards DS. In contrast, this study failed to reveal a significant knowledge difference among men and women but age, education level, experience, and position in pharmacy had a positive relationship with knowledge. According to Shraim et al,27 pharmacists aged between 20 and 29 had a higher knowledge score than older pharmacists. Furthermore, pharmacists with a master degree reported to have a higher knowledge score than pharmacists with a bachelor degree.27 Also, good knowledge is positively linked with pharmacist’s years of experience.33
In the present study, more than half of the participants (53.7%) had a positive attitude towards DS which is comparable with other studies.18,36,37 About 62.8% of the participants deem that DS has a positive impact on public health. However, a higher proportion of participants (93.7%) had agreed that herbal medicines have beneficial effects in another study done in Ethiopia.33 Therapeutic efficacy of DS was taken into account by most participants (62.0%), and another study suggested scientific testing is vital before the use of DS.27 Selling of DS in pharmacies was recommended by nearly half of the participants which is reasonably higher than a study done in China (39%).35 In Ethiopia, it is not common to sell herbal medicines, including DS, in a pharmacy setting as this practice has not been well promoted.26 It is highly recommended to sell DS in pharmacies because clients may have trust in pharmacists who have an ethical responsibility to provide relevant and up to date information.32 Bastani et al18 found that the average attitude score was significantly different between male and female pharmacists and the female pharmacists’ attitude toward DS was more positive than male. Besides the gender factor, this study also found a significant difference in average attitude score between sociodemographic variables like age, education level, experience, and ownership of community pharmacy. Mehralian et al28 also concluded that there is a significant relationship between attitude and other demographic data like age, experience, education level, and ownership.
More than half of pharmacists described their practice about DS was poor. This finding is also supported by another study done in Ethiopia as counseling about DS is seldom practiced, and few inquiries are also received from consumers.26 On the contrary, other studies reported that recommending DS is widespread among pharmacists.25,27,34 One of the factors affecting pharmacy practice on recommending DS might be due to a lack of evidence on the safe use of DS.34,35 Evidence using Web pages and scientific references was searched among a few participants (39%) about DS while the majority (61%) could not refer to any of the references in the current study. Howard et al study also described that the internet was used as a critical source for recommendations of DS; review articles, case reports in clinical journals, and professional association meeting abstracts were also used in making clinical decisions about DS (70%).38 As a result, pharmacists tend to not decide on DS use if no references are available.22 The practice has a significant and positive relationship with age, experience, education, and ownership situation. The score for practice towards DS seems to increase up to the age of 45 and 20 years of experience and then decline28 but in the present study, practice scores increase with age.
Clients are always informed about the possible adverse effects of DS by 39.7% of the participants. Although this finding looks to be a bit higher than a study done in Japan39 (19.6% of the pharmacists), it is still not sufficient. This is because pharmacists may inform DS side effects whenever requested by the consumers or whenever considered necessary. This result ties well with the previous study by Chen et al., wherein half of the respondents would further engage in counseling on the adverse effects whenever deemed appropriate.34 The absence of counseling may also be related to self-confidence while recommending DS as half of the respondents in this study reported they lacked self-confidence while recommending DS. Other studies also reported a consistent finding that a lack of confidence among pharmacists in discussing on the safety issue of DS is pervasive owing to poor knowledge.19,21,22,35,40,41 There has been a positive and significant association between KAP of DS which is consistent with the finding of other studies.18,28
Study Limitations
The following limitations were acknowledged from the present study. (1) This study did not evaluate KAP on the specific DS such as calcium or vitamin D. (2) The knowledge regarding DS was asked generally not with specific DS product side effect, indication, interaction, or contraindication. (3) Surveys of pharmacists knowledge primarily included measures for ‘perceived’, as opposed to “actual” knowledge. Further research exploring pharmacists’ knowledge, beliefs, and practice regarding specific DS will be warranted to enhance understanding of clinical trends and issues surrounding pharmacy care relating to DS.
Conclusions
The current findings have highlighted the need for additional training regarding DS. The Ethiopian Food, Medicine and Health Care Administration and Control Authority (FMHACA) should emphasize on teaching/training community pharmacists how to critically evaluate the use, efficacy, and safety of common DS as well as how to interact with patients to address these and other issues associated with common DS. Furthermore, pharmacy educators in Ethiopia should incorporate the standard professional practice in the area of DS in their curriculum. Future surveys should focus on assessing the opinions and behaviors of pharmacists for specific types of DS in order to facilitate comparisons and generalizations better.
Abbreviations
CAM, complementary and alternative medicine; DRO, drug retail outlets; DS, dietary supplement; DSHEA, Dietary Supplement Health and Education; FMHACA, Food, Medicine and Health Care Administration and Control Authority; KAP, Knowledge, Attitude, and Practice; WHO, World Health Organization.
Ethics Approval and Consent to Participate
The study protocol was approved by an ethical review committee of the School of pharmacy, University of Gondar. Furthermore, verbal informed consent from the participants was approved by the University of Gondar, School of Pharmacy, Ethical Review Board.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors would like to appreciate the community pharmacists who contributed and participated in this study. The authors also gratefully acknowledge the contribution of data collectors. The abstract of this paper was presented at ISPOR 2019 has held May 18-22, 2019 at the Ernest N. Morial Convention Center in New Orleans, USA as a poster presentation. The poster’s abstract was published in “Poster Abstracts” in Value in Health Journal with DOI (https://doi.org/10.1016/j.jval.2019.04.078).
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Glynna L, Valderasb J, Healya P, et al. The prevalence of multimorbidity in primary care and its effect on health care utilization and cost. Fam Pract. 2011;28(5):523–526.
2. World Health Organization. Diet, Nutrition and the Prevention of Chronic Diseases. Geneva; 2003. Contract No.: 797. ISBN:
3. NCCAM: what is complementary and alternative medicine? Available from: http://nccam.nih.gov/health/whatiscam/.
4. National Institutes of Health (NIH). Dietary Supplement Health and Education Act. Public Law No. 1994:103–417. 108 Stat 4325 (codified at 21 USC § 301 [1994]).
5. Tang BM, Eslick GD, Nowson C, Smith C, Bensoussan A. Use of calcium or calcium in combination with vitamin D supplementation to prevent fractures and bone loss in people aged 50 years and older: a meta-analysis. Lancet. 2007;370(9588):657–666. doi:10.1016/S0140-6736(07)61342-7
6. Cao Y, Lu L, Liang J, et al. Omega-3 fatty acids and primary and secondary prevention of cardiovascular disease. Cell Biochem Biophys. 2015;72(1):77–81. doi:10.1007/s12013-014-0407-5
7. Bailey RL, Gahche JJ, Lentino CV, et al. Dietary supplement uses in the United States 2003–2006. J Nutr. 2011;141(2):261–266.
8. Imai T, Nakamura M, Ando F, Shimokata H. Dietary supplement use by community-living population in Japan: data from the National Institute for Longevity Sciences Longitudinal Study of Aging (NILS-LSA). J Epidemiol. 2006;16(6):249–260. doi:10.2188/jea.16.249
9. Garcia-Cazarin ML, Wambogo EA, Regan KS, Davis CD. Dietary supplement research portfolio at the NIH, 2009–2011. J Nutr. 2014;144(4):414–418. doi:10.3945/jn.113.189803
10. Dickinson A, Boyon N, Shao A. Physicians and nurses use and recommend dietary supplements: report of a survey. Nutr J. 2009;8:29. doi:10.1186/1475-2891-8-29
11. The HOPE and HOPE-TOO Trial Investigators. Effects of long term vitamin E supplementation on cardiovascular events and cancer. J Am Med Assoc. 2005;293(11):1338–1347. doi:10.1001/jama.293.11.1338
12. Saremi A, Arora R. Vitamin E and cardiovascular disease. Am J Ther. 2010;17(3):e56–65. doi:10.1097/MJT.0b013e31819cdc9a
13. García-Cortés M, Robles-Díaz M, Ortega-Alonso A, Medina-Caliz I, Andrade RJ. Hepatotoxicity by dietary supplements: a tabular listing and clinical characteristics. In J Mol Sci. 2016;17(4):537. doi:10.3390/ijms17040537
14. Shalansky S, Lynd L, Richardson K, Ingaszewski A, Kerr C. Risk of warfarin related bleeding events and supratherapeutic international normalized ratios associated with complementary and alternative medicine: a longitudinal analysis. Pharmacother. 2007;27(9):1237–1247. doi:10.1592/phco.27.9.1237
15. Food, Medicine and Health Care Administration and Control the Proclamation of the Federal Democratic Republic of Ethiopia No. 661/2009. Addis Ababa: Federal Negarit Gazeta; January 2010.
16. Waddington F, Naunton M, Kyle G, Thomas J, Cooper G, Waddington A. A systematic review of community pharmacist therapeutic knowledge of dietary supplements. Int J Clin Pharm. 2015;37:439–446. doi:10.1007/s11096-015-0092-5
17. World Health Organization Media Centre. Traditional medicine fact sheet no. 134. 2008. Available form: http://www.who.int/mediacentre/fact sheets/fs134/en/index.html.
18. Bastani P, Jooybar M, Zadeh MA, Samadbeik M. Community pharmacy-based survey on pharmacists’ knowledge, attitude, and performance regarding dietary supplements: evidence from South of Iran. Natl J Physiol Pharm Pharmacol. 2017;7(4):396–402. doi:10.5455/njppp.
19. Kwan D, Hirschkorn K, Boon H. US and Canadian pharmacists’ attitudes, knowledge, and professional practice behaviour towards dietary supplements: a systematic review. Bio Med Cent Complement Altern Med. 2006;6:31. doi:10.1186/1472-6882-6-31
20. Braun LA, Tiralongo E, Wilkinson JM, et al. Perceptions, use and attitudes of pharmacy customers on complementary medicines and pharmacy practice. BMC Complement Altern Med. 2010;10:38. doi:10.1186/1472-6882-10-38
21. Naidu S, Wilkinson JM, Simpson MD. Attitudes of Australian pharmacists toward complementary and alternative medicines. Ann Pharmacother. 2005;39(9):1456–1461. doi:10.1345/aph.1G089
22. Brown CM, Barner JC, Shah S. Community pharmacist’s actions when patients use complementary and alternative therapies with medications. J Amer Pharmaci Assoc. 2005;45(1):41–47. doi:10.1331/1544345052843011
23. Robinson N, Lorenc A. Responding to patient demand: community pharmacists and herbal and nutritional products for children. Phytother Res. 2011;25:892–896. doi:10.1002/ptr.v25.6
24. Maher JH, Lowe J, Hughes R. Community pharmacy as a setting for public health nutrition action: Australian nutritionists’ perspectives. Pub Health Nutr. 2014;18(10):1864–1872. doi:10.1017/S1368980014002201
25. Ogbogu U, Necyk C. Community pharmacists’ views and practices regarding natural health products sold in community pharmacies. PLoS One. 2016;11(9):1–19. doi:10.1371/journal.pone.0163450
26. Gelayee DA, Mekonnen GB, Atnafe SA, Birarra MK, Asrie AB. Herbal medicines: personal use, knowledge, attitude, dispensing practice, and the barriers among community pharmacists in Gondar, Northwest Ethiopia. Hindawi Evidence-Based Complement Altern Med. 2017;2017:1–6.
27. Shraim NY, Shawahna R, Sorady MA, et al. Community pharmacists’ knowledge, practices and beliefs about complementary and alternative medicine in Palestine: a cross-sectional study. BMC Complement Altern Med. 2017;17:429. doi:10.1186/s12906-017-1940-8
28. Mehralian G, Yousefia N, Hashemian F, Maleksabet H. Knowledge, attitude and practice of pharmacists regarding dietary supplements: a community pharmacy- based survey in Tehran. Iranian J Pharm Res. 2014;13(4):1457–1465.
29. Haq NU, Hassali MA, Shafie AA, et al. A cross-sectional assessment of knowledge, attitude and practice among Hepatitis-B patients in Quetta, Pakistan. BMC Pub Health. 2013;13:448. doi:10.1186/1471-2458-13-448
30. Xue CC, Zhang AL, Lin V, Da Costa C, Story DF. Complementary and alternative medicine use in Australia: a national population-based survey. J Altern Complement Med. 2007;13(6):643–650. doi:10.1089/acm.2006.6355
31. Kassaye KD, Amberbir A, Getachew B, Mussema Y. A historical overview of traditional medicine practices and policy in Ethiopia. Ethiop J Health Develop. 2006;20(2):127–134.
32. Boon H, Hirschkorn K, Griener G, Cali M. The ethics of dietary supplements and natural health products in pharmacy practice: a systematic documentary analysis. Int J Pharm Pra. 2009;17(1):31–38. doi:10.1211/ijpp.17.1.0005
33. Kheir N, Gad HY, Abu-Yousef SE. Pharmacists’ knowledge and attitudes about natural health products: a mixed-methods study. Drug Healthcare Patient Saf. 2014;6:7. doi:10.2147/DHPS.S57756
34. Chen X, Ung CO, Hu H, Liu X, Zhao J, Hu Y, Li P, Yang Q. Community pharmacists’ perceptions about pharmaceutical care of traditional medicine products: A questionnaire-based cross-sectional study in Guangzhou, China. Evidence-Based Complement Altern Med. 2016;2016:7801637.
35. Bushett NJ, Dickson-Swift VA, Willis JA, Wood P. Rural Australian community pharmacists’ views on complementary and alternative medicine: A pilot study. BMC Complement Altern Med. 2011;11(1):103. doi:10.1186/1472-6882-11-103
36. Portyansky E. Alternative medicine-how bountiful is the harvest. Drug Topics. 1998;142(7):44–45.
37. Montbriand MJ. Alternative therapies: health professionals’ attitudes. Canadian Nurse. 2000;96(3):22.
38. Howard N, Tsourounis C, Kapusnik-Uner J. Dietary supplement survey of pharmacists: personal and professional practices. J Altern Complement Med. 2001;7(6):667–680. doi:10.1089/10755530152755225
39. Chiba T, Sato Y, Kobayashi E, Ide K, Yamada H, Umegaki K. Behaviors of consumers, physicians and pharmacists in response to adverse events associated with dietary supplement use. Nutr J. 2017;16:18. doi:10.1186/s12937-017-0239-4
40. Dolder C, Lacro J, Dolder N, Gregory P. Pharmacists’ use of and attitudes and beliefs about alternative medications. Am J Health Syst Pharm. 2003;60(13):1352–1357. doi:10.1093/ajhp/60.13.1352
41. Asahina Y, Hori S, Sawada Y. Community pharmacists’ attitudes relating to patients’ use of health products in Japan. Int J Clinic Pharm. 2012;34(4):529–537. doi:10.1007/s11096-012-9640-4
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.