")
Back to Journals » Infection and Drug Resistance » Volume 15
Community Fecal Carriage and Molecular Epidemiology of Extended-Spectrum β-Lactamase- and Carbapenemase-Producing Escherichia coli from Healthy Children in the Central South China
Authors Liu X, Li X, Yang AW, Tang B , Jian ZJ, Zhong YM, Li HL, Li YM , Yan Q, Liang XH, Liu WE
Received 5 January 2022
Accepted for publication 26 March 2022
Published 6 April 2022 Volume 2022:15 Pages 1601—1611
DOI https://doi.org/10.2147/IDR.S357090
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Xuan Liu,1,* Xin Li,1,* A-wen Yang,1 Bin Tang,1 Zi-juan Jian,1 Yi-ming Zhong,1 Hong-ling Li,1 Yan-ming Li,1 Qun Yan,1 Xiang-hui Liang,1,2 Wen-en Liu1,2
1Department of Clinical Laboratory, Xiangya Hospital, Central South University, Changsha, Hunan Province, People’s Republic of China; 2National Clinical Research Center for Geriatric Disorders, Xiangya Hospital, Changsha, Hunan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wen-en Liu; Xiang-hui Liang, Department of Clinical Laboratory, Xiangya Hospital, Central South University, Changsha, 410008, Hunan Province, People’s Republic of China, Tel +86-731-84327437, Fax +86-731-84327332, Email [email protected]; [email protected]
Background: Fecal carriage of extended-spectrum β-lactamase-producing Escherichia coli (ESBL-EC) and carbapenemase-producing E. coli (CP-EC) is well reported among hospitalized adults and children. However, there are few studies on the carriage prevalence and ESBL-EC and CP-EC genotypes among healthy children in China.
Patients and Methods: Stool samples were collected from 330 students in 2021 from three randomly selected primary schools in Changsha, China. ESBL-EC and CP-EC were screened using CHROMagarTM chromogenic plates. ESBL and carbapenemase production was confirmed using the double-disc synergy test and a modified carbapenem inactivation method, respectively. Antimicrobial susceptibility was tested using the broth microdilution method. Resistance determinants, virulence factors, and phylogenetic groups were determined by PCR and sequencing. Multi-locus sequence typing (MLST) was performed (seven housekeeping genes were amplified and sequenced) on the phylogenic group B2 E. coli to detect high-risk clonal strains such as ST131 E. coli. Then, ST131 E. coli were characterized based on ST131 clades, O-type, and fimH alleles.
Results: In total, 118 (35.8%) ESBL-EC and 3 (0.9%) CP-EC were isolated. blaCTX-M was the most common genotype (27.1%), identified in all ESBL-EC, except one, which carried blaSHV-12. One isolate with mcr-1 was found amongst ESBL-EC, whereas all three CP-EC carried blaNDM-1. The predominant sequence type (ST) clones in group B2 were ST131 and ST1193. The prevalence of ST131 E. coli was 9.9%, displaying serotypes O16 and O25b, fimH alleles 30, 41, and 89, and ST131 clades A and C1-M27.
Conclusion: In this study, high carriage rate of ESBL-EC was found among healthy children, and the dominant ESBL was CTX-M-14. In addition, high-risk clones (ST131 and ST1193) were also detected. This emphasizes the importance of monitoring ESBL-EC in community settings.
Keywords: community children, ESBL, CPE, ST131, mcr-1
Introduction
The wide dissemination of extended-spectrum β-lactamase-producing Escherichia coli (ESBL-EC) throughout the world is a major problem that has resulted in increased global mortality, morbidity, and health-care expenses.1 The emergence of ESBL-EC is now no longer limited to the clinical setting, and the 15-year combined prevalence of ESBL-EC carriage has reached 16.5% globally.2 Although individuals carrying ESBL-EC in the intestine are usually asymptomatic, long-term colonization and high carrying rates of the microbe increase the risk of infection with multidrug-resistant (MDR) pathogenic bacteria.3 Studies have shown that fecal colonization with ESBL-EC is associated with infection in healthy individuals.4
Disconcertingly, there is a certain amount of ESBL-EC in the community. The distribution of sequence types (STs) and ESBL genes has been reported to be very similar between community fecal isolates and clinical isolates.5 In addition, with the increasing use of carbapenems and polymyxins, carbapenemase-producing E. coli (CP-EC) and colistin-resistant E. coli have also been isolated from feces samples procured from the community.6,7 This indicated that community may be a repository of ESBL-genes, carbapenemase-genes and colistin-resistant genes in the future.
Plasmid-mediated horizontal transfer of resistance genes and the emergence of dominant clones of E. coli can be among the reasons for the increased global incidence of MDR E. coli, such as plasmids carrying blaCTX-M and the E. coli ST131 clone.1 CTX-M is currently the most common ESBLs worldwide, and the spread of blaCTX-M is mainly driven by IncF plasmids, which enable resistance genes to spread widely in communities and hospitals.8–10 E. coli ST131, a high-risk clone, is a type of extraintestinal pathogenic E. coli (ExPEC) with a multidrug-resistant spectrum that often causes community- and hospital-acquired infections.11 E. coli ST131 largely belongs to phylogenetic group B2 and can be divided into clade A, clade B, and clade C based on its fimH allele and O-type.11 Furthermore, E. coli ST131 is usually related to the production of ESBLs, especially CTX-M-15, CTX-M-14, and CTX-M-27.12
Over the past decade, researches have reported the prevalence of ESBL-producing bacteria carried in the feces of healthy children.3,7 Among different geographic regions, the separation rate is significantly heterogeneous, ranging from 0.1% to 59%.7,13 Although there have been several reports in China regarding the prevalence of ESBL-carrying Enterobacteriaceae in healthy populations, most of these were restricted to examination of adults. Data regarding ESBL-EC and CP-EC carriage among community children in China are limited. Therefore, this study aimed to assess the current fecal carriage of ESBL-EC and CP-EC in healthy children in China and provide detailed molecular data.
Materials and Methods
Participants
A cross-sectional survey was conducted on healthy children in primary schools in Changsha, Hunan Province, China, in 2021. The resident population of Hunan province is 66,444,864, and Changsha, the capital city of Hunan province, has a resident population of 1,047,900 (Data updated to May 2021). Taking the geographical center of Changsha City as the center, the city was divided into four regions according to east, west, south and north directions. Large-scale primary schools (with more than 2000 students) were included in the selection range, and then schools that were relatively geographically scattered were considered. Three schools were finally selected in Kaifu District, Yuelu District, and Changsha County, and the geographic locations were shown in Figure S1. A total of 422 students from these schools participated in this study. After obtaining parental consent, fresh feces were collected from the children and immediately sent to the laboratory. In addition, a questionnaire was filled that requested information on the child’s gender, age, class, history of diarrhea, antibiotic treatments or hospitalization, whether they had pets, and whether they had been in contact with patients with diarrhea. Healthy children were defined as students who had no symptoms of diarrhea, no history of antibiotics use within one month, and who were younger than 14 years. Ultimately, 330 students were included in the study for subsequent analysis. This study was approved by the Ethics Committee of the Xiangya Hospital of Central South University (reference number 202110445).
Screening of Fecal ESBL-EC and CP-EC Isolates, Species Identification, and Antimicrobial Susceptibility
Within 4 h of feces sampling, an aliquot of fecal matter was smeared on two types of CHROMagarTM chromogenic plates (CHROMagar, Paris, France) for the selection of samples containing ESBL-producing and carbapenemase-producing Enterobacteriaceae isolates. Subsequently, E. coli were identified by MALDI-TOF MS (Bruker Daltonics GmbH, Bremen, German). The double-disc synergy test and a modified carbapenem inactivation method were used to confirm the production of ESBL and carbapenemase, respectively, according to Clinical and Laboratory Standards Institute (CLSI) guidelines.14 The antimicrobial susceptibility was then determined using the broth microdilution method, including cefazolin, cefuroxime, ceftriaxone, ceftazidime, cefepime, cefoxitin, amikacin, gentamicin, piperacillin/tazobactam, meropenem, tigecycline, aztreonam, levofloxacin, nitrofurantoin, cefoperazone/sulbactam, colistin, minocycline, ampicillin, ampicillin-sulbactam, and trimethoprim/sulfamethoxazole. The susceptibility of the strains to other antibiotics was determined according to the CLSI guidelines, while that to tigecycline and colistin was investigated by the Food and Drug Administration and EUCAST criteria, respectively. E. coli ATCC25922 was used as the quality control strain.
Detection of Antibiotic Resistance Genes
ESBL-encoding genes blaCTX-M, blaTEM, and blaSHV were screened using multiplex polymerase chain reaction (PCR) as previously described.15 Specific primers were used to divide the blaCTX-M genes into five phylogenetic groups, CTX-M-1, CTX-M-2, CTX-M-8, CTX-M-9, and CTX-M-25.16 Except for blaCTX-M-15 that was detected by PCR,17 other blaCTX-M-positive isolates were determined by sequencing. The sequencing results were analyzed in BLAST (https://blast.ncbi.nlm.nih.gov/Blast.cgi) and ResFinder4.1 (https://cge.cbs.dtu.dk/services/ResFinder/). The presence of plasmid-mediated quinolone resistance determinants (qnrA, qnrB, qnrC, qnrS, aac (6ʹ)-Ib-cr, and qepA) and the colistin resistance gene (mcr-1) were detected in all the isolates by PCR.18,19 For three CP-EC, PCR was used to detect the carbapenemase genes (blaNDM-1, blaKPC-2, blaIMP, blaVIM, and blaOXA-48).20
Virulence Genotyping and Phylogenetic Group Detection
The presence of 26 virulence genes was assessed by multiplex PCR, and the virulence score was calculated as described previously.17 To investigate the phylogeny of ESBL-EC, multiplex PCR was performed according to the protocols provided by Clermont et al, in which E.coli was divided into seven groups (A, B1, B2, C, D, E, and F).21
Multi-Locus Sequence Typing (MLST)
MLST analysis was performed on the phylogenic group B2 E. coli to screen the high-risk clone ST131. The seven housekeeping genes (adk, fumC, gyrB, icd, mdh, purA, and recA) of B2 E. coli isolates were amplified and sequenced. The sequencing results were analyzed on PUBMLST (https://pubmlst.org/bigsdb?db=pubmlst_escherichia_seqdef), and the ST type of each strain was obtained. Furthermore, the carriage of resistance and virulence genes in ST131 and non-ST131 strains were compared.
Molecular Characterization of ST131
The ST131 clade of all 12 ST131 isolates was screened by multiplex PCR as described by Subramanya et al.17 O-type and fimH alleles were investigated according to a previous study.22
Statistical Analysis
Categorical data were generally analyzed using the chi-square test or Fisher’s exact test. P < 0.05 was considered statistically significant. All data analysis was performed using the SPSS software (version 23.0).
Results
Prevalence and Antimicrobial Susceptibility
A total of 330 students (173 males and 157 females) participated in the study belonging to the age group of 6 to 12 years (average 8.8 years). Of the 330 feces samples, 118 were positive for ESBL production and 3 for carbapenemase production. For the ESBL-EC isolates, 100% of the isolates were resistant to ampicillin, 99.2% to ceftriaxone, 95% to cefuroxime, 85.6% to cefazolin, 59.3% to trimethoprim/sulfamethoxazole, 40.7% to levofloxacin, 28.8% to aztreonam, 25.4% to ceftazidime, 17.8% to gentamicin, and 13.6% to ampicillin-sulbactam, while none were resistant to meropenem, tigecycline, nitrofurantoin, piperacillin-tazobactam, or cefoperazone/sulbactam. For CP-EC, all of the isolates were susceptible to amikacin, tigecycline, colistin, and minocycline (Table 1).
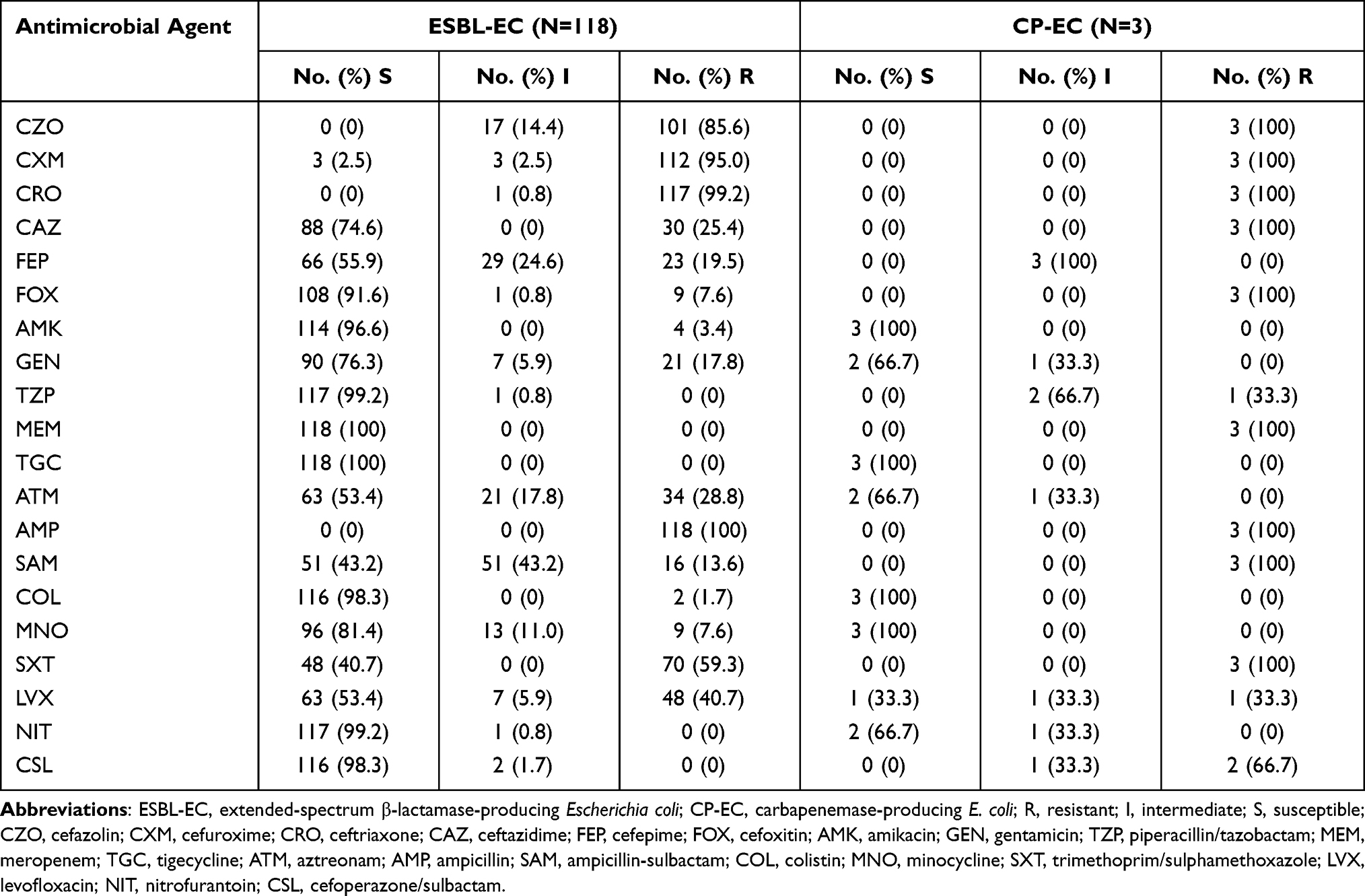 |
Table 1 Prevalence of Antimicrobial Susceptibility of ESBL-EC Vs CP-EC from Healthy Children |
Molecular Analysis of the Antibiotic Resistance Genes
The blaCTX-M gene was found in all of the ESBL-EC strains except for one isolate carrying blaSHV-12, while blaTEM was found in 45.8% of the strains. The PCR and sequencing analysis revealed that the most common blaCTX-M subtype was blaCTX-M-14 (27.1%), followed by blaCTX-M-15 (24.6%), blaCTX-M-27 (24.6%), blaCTX-M-65 (8.5%), blaCTX-M-213 (4.2%), blaCTX-M-55 (4.2%), blaCTX-M-110 (1.7%), and blaCTX-M-24 (0.8%). Additionally, four strains co-harboring multiple blaCTX-M genes were found, two of which carried blaCTX-M-15 and blaCTX-M-27, one carried blaCTX-M-14 and blaCTX-M-15, and one carried blaCTX-M-15 and blaCTX-M-213. Three types of the plasmid-mediated quinolone resistance (PMQR) genes were found: qnrS (22.0%), aac (6’)-Ib (3.4%), and qnrB (1.7%). Notably, one ESBL-EC isolate carried mcr-1 and all the three CP-EC isolates carried blaNDM-1. The detailed results are shown in Table 2.
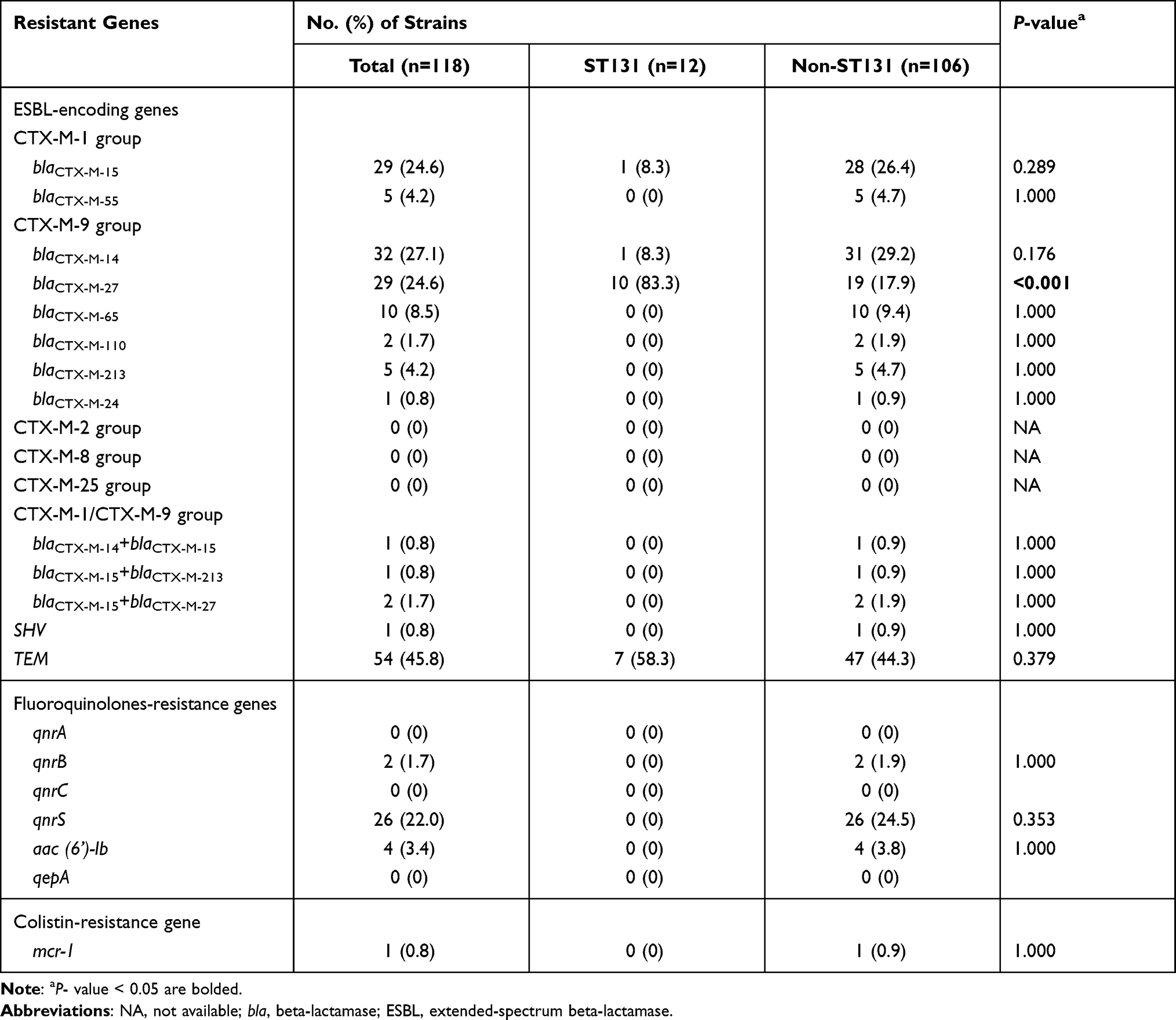 |
Table 2 Prevalence of Resistant Genes Among 118 ESBL-EC from Healthy Children |
Virulence Genotyping and Phylogenetic Group
For ESBL-EC (n=118), the most frequent virulence genes in their genome were fimH (88.1%), fyuA (72.9%), traT (65.3%), kpsMTII (61.0%), and iutA (54.2%). Other virulence genes, such as papG allele I, gafD, cdtB, and cnf1 were not present. The median virulence score was 4.2 (ranging from 0 to 15) and approximately 52.5% of the isolates were ExPEC (Table 3). For CP-EC (n=3), the most frequent virulence genes observed were fimH (66.7%), kpsMTII (66.7%), and traT (66.7%), and two of the isolates were ExPEC (Table S1). All isolates were classified into seven phylogenetic groups (A, B1, B2, C, D, E, and F). The results revealed that the majority of isolates belonged to group B2 (33.1%), followed by groups D (18.1%), B1 (12.4%), F (9.9%), A (9.1%), E (6.6%), and C (2.5%). However, there were ten isolates that could not be classified into any group (Table S2).
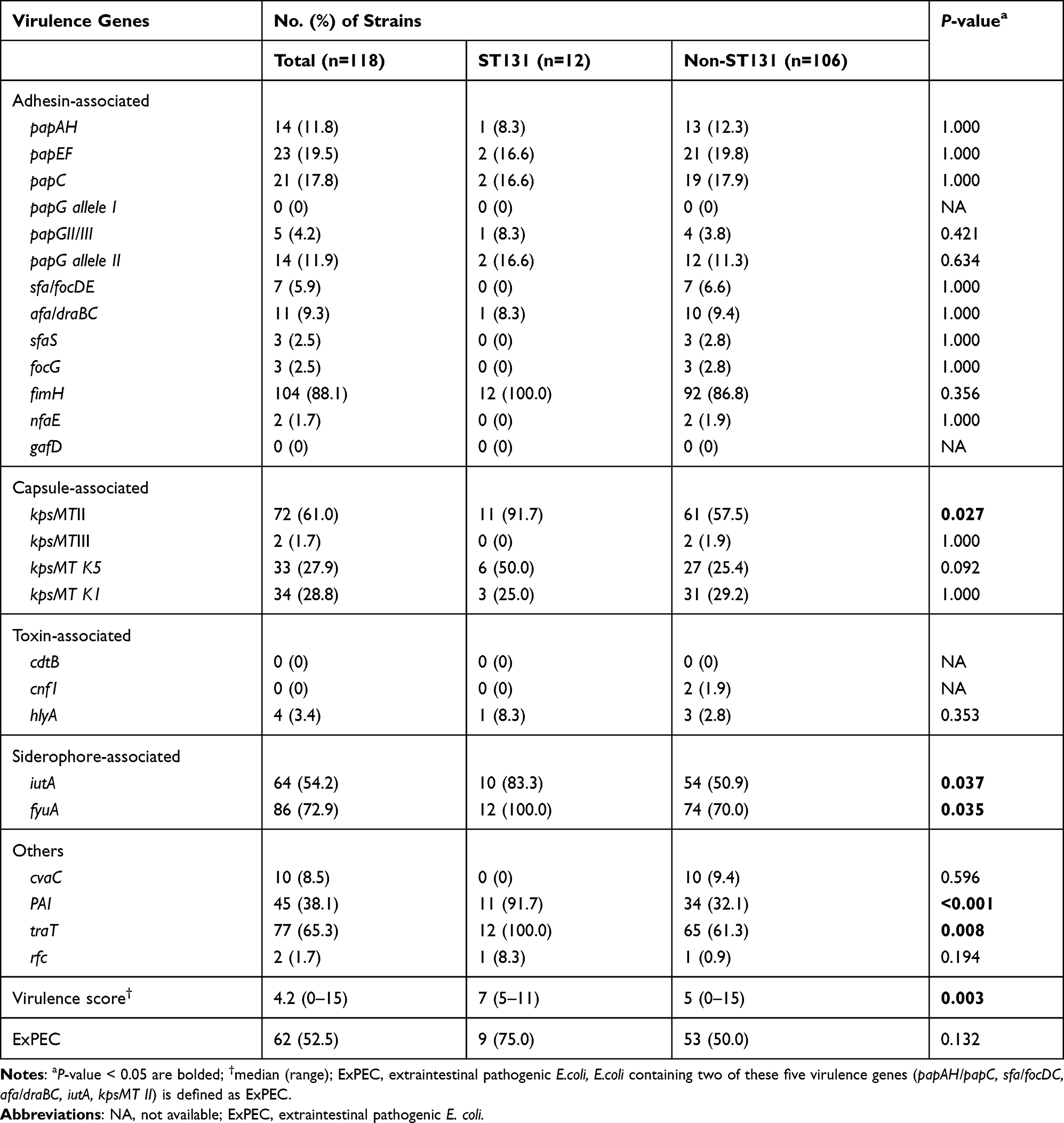 |
Table 3 Prevalence of Virulence Traits Among 118 ESBL-EC from Healthy Children |
MLST
The strains in the E. coli B2 group were classified into 13 different STs. ST131 (30.0%) was the most common ST, followed by ST1193 (27.5%), ST95 (10.0%), ST73 (7.5%), and ST2372 (5.0%). In addition, ST14, ST3483, ST4888, ST4508, ST1163, ST493, ST589, and ST92 each accounted for 2.5% (Table S3).
E. coli ST131 Characterization
As indicated in Table S4, 12 (9.9%) of the 121 E. coli strains belonged to the ST131 lineage, including seven O16-ST131 and five O25b-ST131 isolates.The fimH alleles of all O16-ST131 isolates were fimH41, and the fimH alleles of O25b-ST131 isolates were fimH30 (n=4) and fimH89 (n=1). Among the 12 ST131 isolates, clade A (n=8) was the most common subclade, followed by clade C (n=4) which were C1-M27 subclades. All 12 ST131 isolates were found to harbor ESBL genes, including blaCTX-M-27, blaCTX-M-14, and blaCTX-M-15. The ST131 isolates had a significantly higher prevalence rate of blaCTX-M-27 compared with that of non-ST131 isolates (P < 0.05) (Table 2). In general, the virulence scores of the ST131 isolates were higher than those of the non-ST131 isolates (P < 0.05). In terms of the prevalence of virulence genes, kpsMII, traT, iutA, fyuA, and PAI appeared more frequently in the ST131 isolates (P < 0.05) (Table 3).
Discussion
This study assessed the fecal carriage of ESBL-EC and CP-EC and their molecular characteristics in healthy children in China and showed a high rate of ESBL-EC carriage and predominance of the clone ST131 in the B2 group of E. coli. The correlation between infections caused by ESBL-producing bacteria and their colonization in feces has been demonstrated.4 The emergence of resistant bacteria in intestinal commensal flora is a serious threat, as the intestine is an important site for the transmission of bacterial resistance, which may consequently lead to an increased risk of community- or hospital-acquired resistant infections.23 Considering that the antimicrobial use for children differs from that for adults and that studies on fecal carriage of resistant bacteria in children have been mainly focused in a clinical setting, there is a need to monitor the prevalence of resistant bacteria in children in the community. To the best of our knowledge, this is the first systematic study focusing on the fecal carriage of ESBL-EC and CP-EC in healthy children from a community in China.
The carriage of ESBL-EC in feces was 35.8% in this study, which is higher than that in a study based in Taiwan (5.1%), in which the study population comprised of community children that were hospitalized within three days.24 The higher prevalence in this study may be related to high contact rates between school children, indicating that schools may play a role in the transmission of ESBL-producing bacteria. In the study by Bunt et al, daycare center attendance has been shown to be a risk factor for preschoolers carrying ESBL/AmpC-producing bacteria.25 The prevalence of ESBL-EC carriage in the healthy children in the present study was higher than that in France (7.6%) and Spain (31%)26,27 and lower than that in Cambodia (55%) and Pakistan (43%),28,29 which may be partly due to the differences in sanitary conditions, climate, and eating habits in different regions of the world. Although the carriage rate of ESBL-EC in this study was relatively high compared to that observed in the above studies, it was still lower than that in pediatric patients in China, which has been reported to be 46.7%.30 Moreover, Babu et al reported that fecal carriage of ESBL-producing Enterobacteriaceae in hospitalized patients was almost twice as high as in healthy individuals.31 In addition, the carriage of CP-EC in the present study was 0.9%, which is lower than that of outpatient (1.4%) and inpatient children (1.9%) in Shanghai, China.20,32 Although few countries have reported CP-EC carriage among community healthy children to date, a report from Pakistan showed that a quarter of infants in their research harbored CP-EC, indicating that the intestine of healthy children may be a reservoir of CP-EC and should be considered as a serious health issue.29
The global distribution of CTX-M variants showed that the CTX-M-1 group (especially CTX-M-15) was the dominant genotype in most regions, while the CTX-M-9 group (especially CTX-M-14) was dominant in China.1,33 In consistent with the above report, CTX-M-14 was the predominant CTX-M subtype in this study. The prevalence of CTX-M-27 was 24.6%, higher than the results of our previous study of healthy adults in 2015 (15.0%).34 Such an increase has also been seen in France, where the proportion of CTX-M-27 increased from 4.5% to 25% between 2010 and 2015 among the 1886 children screened.26 Furthermore, in the present study, we observed a significantly higher prevalence rate of blaCTX-M-27 among ST131 isolates than that in non-ST131 samples. In line with this, Birgy et al also reported a high proportion of CTX-M-27 in ST131 isolates.26 Therefore, ST131 isolates may play a role in the transmission of blaCTX-M-27.
Like the resistance pattern of ESBL-EC from pediatric patients, ESBL-EC isolates from healthy children were highly resistant to ampicillin, ceftriaxone, and cefazolin, and were susceptible to meropenem, colistin, and tigecycline.30 This underscores the importance of investigating resistant strains in human fecal matter, as clinical strains may originate from the intestinal tract. Fluoroquinolones are first-line antimicrobial agents for E. coli infections but they are not recommended for children.35 Surprisingly, the isolates in this study showed up to 40.7% resistance to levofloxacin, and the resistance to ciprofloxacin reported in pediatrics was also as high as 60%.30 The reason for this high resistance rate may be related to the PMQR genes, which can undergo horizontal transfer between strains.35 PMQR genes were also detected in 27.1% of the ESCL-EC strains in this study. However, the mechanisms of the high resistance to fluoroquinolones in children remain to be explored further.
Infections due to carbapenem-resistant Enterobacteriaceae (CRE) in children are often associated with adverse clinical outcomes.36 Disconcertingly, we found three E. coli strains carrying blaNDM-1 gene. In 2016, a study conducted in eastern China also reported that NDM-1 was the major carbapenemase produced by ESBL-EC isolated from the feces of outpatient children. NDM-1 is a metal-β-lactamase (MBL) and cannot be inhibited by β-lactamase inhibitors, which significantly limits the utility of β-lactam-β-lactamase inhibitors, such as ceftazidime-avibactam.37 A systematic review showed that blaNDM-1 was the most common carbapenem-resistant genotype causing neonatal sepsis in China.38 Therefore, given the complexity of treating CRE (especially MBL-induced CRE) infections, it is necessary to monitor the prevalence of such resistant bacteria among commensal bacteria.
In addition, a lot of focus has recently been drawn to the emergence of mcr-1. A high prevalence of mcr-1 in healthy children has been reported in Bolivia (38.8%) and Lebanon (33.3%).39,40 However, the carriage of mcr-1 in the intestine of healthy children remains understudied in China. Only Hu et al reported a carriage rate of 9.6% for mcr-1 among hospitalized children who did not suffer from diarrhea.41 In our study, two ESBL-EC isolates showing colistin-resistance were identified, one of which co-harbored both mcr-1 and blaCTX-M-14 and was isolated from a child with pets, including dogs and pet mice. This was consistent with a report from Guangzhou, China, suggesting that animals may be the source of presence of mcr-1 in humans.42 Colistin resistance in another isolate may be mediated by other subtypes of the mcr gene or other resistance mechanisms, which needs further investigation.
Pathogenic E. coli strains are usually assigned to the B2 phylogenetic group,43 which accounted for the main proportion (33.1%) in our research, in which ST131 E. coli was the predominant clone. ST131 ESBL-EC is commonly found in community-acquired infections, and ST131 carriers can transmit it within the families,44,45 highlighting the potential health threat from ST131 carriers. Even though in this research, it was found that the detected ST131 ESBL-EC carried several virulence genes (kpsMTII, traT, iutA, fyuA, and PAI), the carrier did not show infection symptoms. ESBL and virulence genes (fyuA) were the risk factors of E. coli infection.46 However, the occurrence of infection is also host-dependent. Therefore, infection by the virulent ST131 E. coli does not necessarily occur when the body is immunocompetent and the intestinal barrier is intact. Ferjani et al reported that E. coli carried virulence genes and resistance genes in the feces of healthy children.47 Barrios-Villa et al reported four ST131 E. coli strains isolated from healthy humans with a high adherence/invasive phenotype.48
O25b has traditionally been considered the predominant serotype of ST131, but the prevalence of E. coli O16-ST131 has increased significantly in recent years.49 In our study, the detection rate of O16-ST131 was higher than that of O25b-ST131, which was consistent with our past results of a study on healthy adults in Changsha.34 The rise of O16-ST131 may be related to the improvement of novel PCR detection methods.22 Clade A ST131 E. coli predominated (66.6%) in our study and the others belonged to clade C1-M27 (33.3%); moreover, in another multi-center study, it was observed that all clade A ST131 E. coli were associated with the community infections.50 This finding implies clade A may become a major clade of ST131 in the community in China. However, a similar study in France reported that the predominant ST131 clade was clade C (74%), followed by clade A (26%).51 This may be due to the geographical differences between the two regions. Additionally, C1-M27 is a novel subclade of clade C1 carrying CTX-M-27, which has a higher degree of dissemination in the hospital setting.52 Currently, clade C1-M27 has emerged and become prominent in many countries, such as Japan and Canada,53,54 and the present study is the first to show the presence of clade C1-M27 in China. More studies are needed to further monitor the prevalence of this clade.
Notably, ST1193 accounted for a high proportion of the B2 group. E. coli ST1193 was first described in 2012, and its incidence has risen dramatically in recent years.55 Birgy et al reported a significant increase (from zero to 9.3%) in the detection of E. coli ST1193 among children with febrile urinary tract infections in France from 2014 to 2017.56 Ding et al found that E. coli ST1193 accounted for 21.4% of E. coli clinical isolates that cause neonatal invasive infections in the population of China.57 Meanwhile, clones related to urinary tract infection were also detected, such as ST95 and ST73. The current findings suggest that the specific global risk clones are lurking in humans, even in non-clinical settings, which also poses a potential but not negligible risk to public health.
The study has several limitations. First, although we chose three schools from different urban areas to represent the characteristics of the Changsha region, inevitably, the representativeness of our study population remains limited. In addition, there was one colistin-resistant isolate in need of further research to explore its resistance mechanism.
Conclusion
In conclusion, high fecal carriage and significant CTX-M genetic diversity of ESBL-EC were detected in children from Changsha, China. The emergence of the mcr-1 gene, blaNDM-1 gene, and ST131 E. coli (especially C1-M27) among community children should not be taken lightly.
Abbreviations
ESBL-EC, extended-spectrum β-lactamase-producing Escherichia coli; CP-EC, carbapenemase-producing E. coli; MLST, multi-locus sequence typing; ST, sequence type; bla, beta-lactamase; MDR, multidrug-resistant; ExPEC, extraintestinal pathogenic E. coli; PCR, polymerase chain reaction; CRE, carbapenem-resistant Enterobacteriaceae; MBL, metal-β-lactamase; R, resistant; I, intermediate; S, susceptible; CZO, cefazolin; CXM, cefuroxime; CRO, ceftriaxone; CAZ, ceftazidime; FEP, cefepime; FOX, cefoxitin; AMK, amikacin; GEN, gentamicin; TZP, piperacillin/tazobactam; MEM, meropenem; TGC, tigecycline; ATM, aztreonam; AMP, ampicillin; SAM, ampicillin-sulbactam; COL, colistin; MNO, minocycline; SXT, trimethoprim/sulphamethoxazole; LVX, levofloxacin; NIT, nitrofurantoin; CSL, cefoperazone/sulbactam.
Ethics Statement
All procedures of this study involving humans (individuals, human samples, isolates) were reviewed and approved by Ethics Committee of the Xiangya Hospital of Central South University (reference number 202110445). This study was conducted in accordance with the Declaration of Helsinki. The parents or legal guardians of the children have been informed of the purpose of this study.
Consent for Publication
All authors confirm that the details of any images/recordings can be published.
Acknowledgments
We thank all the staff from the three schools for their kind help.
Funding
This work was supported by Hunan Provincial Science and Technology Department Key R&D Program Project (2015SK2018) and Natural Science Foundation of Changsha (kq2014297), and Hunan Province Natural Sciences Foundation of China (2021JJ31116).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bevan ER, Jones AM, Hawkey PM. Global epidemiology of CTX-M β-lactamases: temporal and geographical shifts in genotype. J Antimicrob Chemother. 2017;72(8):2145–2155. doi:10.1093/jac/dkx146
2. Bezabih YM, Sabiiti W, Alamneh E, et al. The global prevalence and trend of human intestinal carriage of ESBL-producing Escherichia coli in the community. J Antimicrob Chemother. 2021;76(1):22–29. doi:10.1093/jac/dkaa399
3. Birgy A, Cohen R, Levy C, et al. Community faecal carriage of extended-spectrum beta-lactamase-producing Enterobacteriaceaein French children. BMC Infect Dis. 2012;12(1):315. doi:10.1186/1471-2334-12-315
4. Karanika S, Karantanos T, Arvanitis M, et al. Fecal colonization with extended-spectrum beta-lactamase-producing Enterobacteriaceae and risk factors among healthy individuals: a systematic review and metaanalysis. Clin Infect Dis. 2016;63(3):310–318. doi:10.1093/cid/ciw283
5. Verschuuren TD, Van Hout D, Arredondo-Alonso S, et al. Comparative genomics of ESBL-producing Escherichia coli (ESBL-Ec) reveals a similar distribution of the 10 most prevalent ESBL-Ec clones and ESBL genes among human community faecal and extra-intestinal infection isolates in the Netherlands (2014–17). J Antimicrob Chemother. 2021;76(4):901–908. doi:10.1093/jac/dkaa534
6. Bi Z, Berglund B, Sun Q, et al. Prevalence of the mcr-1 colistin resistance gene in extended-spectrum β-lactamase-producing Escherichia coli from human faecal samples collected in 2012 in rural villages in Shandong Province, China. Int J Antimicrob Agents. 2017;49(4):493–497. doi:10.1016/j.ijantimicag.2016.12.018
7. Pallecchi L, Malossi M, Mantella A, et al. Detection of CTX-M-type beta-lactamase genes in fecal Escherichia coli isolates from healthy children in Bolivia and Peru. Antimicrob Agents Chemother. 2004;48(12):4556–4561. doi:10.1128/AAC.48.12.4556-4561.2004
8. Woerther PL, Burdet C, Chachaty E, et al. Trends in human fecal carriage of extended-spectrum β-lactamases in the community: toward the globalization of CTX-M. Clin Microbiol Rev. 2013;26(4):744–758. doi:10.1128/CMR.00023-13
9. Shafiq M, Huang J, Shah JM, et al. Characterization and resistant determinants linked to mobile elements of ESBL-producing and mcr-1-positive Escherichia coli recovered from the chicken origin. Microb Pathog. 2021;150:104722. doi:10.1016/j.micpath.2020.104722
10. Abdallah HM, Alnaiemi N, Reuland EA, et al. Fecal carriage of extended-spectrum β-lactamase- and carbapenemase-producing Enterobacteriaceae in Egyptian patients with community-onset gastrointestinal complaints: a hospital -based cross-sectional study. Antimicrob Resist Infect Control. 2017;6(1):62. doi:10.1186/s13756-017-0219-7
11. Nicolas-Chanoine MH, Bertrand X, Madec JY. Escherichia coli ST131, an intriguing clonal group. Clin Microbiol Rev. 2014;27(3):543–574. doi:10.1128/CMR.00125-13
12. Peirano G, Pitout JDD. Extended-spectrum β-lactamase-producing Enterobacteriaceae: update on molecular epidemiology and treatment options. Drugs. 2019;79(14):1529–1541. doi:10.1007/s40265-019-01180-3
13. Farra A, Frank T, Tondeur L, et al. High rate of faecal carriage of extended-spectrum β-lactamase-producing Enterobacteriaceae in healthy children in Bangui, Central African Republic. Clin Microbiol Infect. 2016;22(10):
14. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing: Twenty-Ninth Informational Supplement M100-S29. Wayne, PA, USA: CLSI; 2019.
15. Hijazi SM, Fawzi MA, Ali FM, et al. Prevalence and characterization of extended-spectrum beta-lactamases producing Enterobacteriaceae in healthy children and associated risk factors. Ann Clin Microbiol Antimicrob. 2016;15(1):3. doi:10.1186/s12941-016-0121-9
16. Li B, Lu Y, Lan F, et al. Prevalence and characteristics of ST131 clone among unselected clinical Escherichia coli in a Chinese university hospital. Antimicrob Resist Infect Control. 2017;6(1):118. doi:10.1186/s13756-017-0274-0
17. Subramanya SH, Bairy I, Metok Y, et al. Detection and characterization of ESBL-producing Enterobacteriaceae from the gut of subsistence farmers, their livestock, and the surrounding environment in rural Nepal. Sci Rep. 2021;11(1):2091. doi:10.1038/s41598-021-81315-3
18. Robicsek A, Strahilevitz J, Sahm DF, et al. qnr prevalence in ceftazidime-resistant Enterobacteriaceae isolates from the United States. Antimicrob Agents Chemother. 2006;50(8):2872–2874. doi:10.1128/AAC.01647-05
19. Zhong YM, Liu WE, Zheng ZF. Epidemiology and molecular characterization of mcr-1 in Escherichia coli recovered from patients with bloodstream infections in Changsha, central China. Infect Drug Resist. 2019;12:2069–2076. doi:10.2147/IDR.S209877
20. Pan F, Tian D, Wang B, et al. Fecal carriage and molecular epidemiology of carbapenem-resistant Enterobacteriaceae from outpatient children in Shanghai. BMC Infect Dis. 2019;19(1):678. doi:10.1186/s12879-019-4298-3
21. Clermont O, Christenson JK, Denamur E, et al. The Clermont Escherichia coli phylo-typing method revisited: improvement of specificity and detection of new phylo-groups. Environ Microbiol Rep. 2013;5(1):58–65. doi:10.1111/1758-2229.12019
22. Johnson JR, Clermont O, Johnston B, et al. Rapid and specific detection, molecular epidemiology, and experimental virulence of the O16 subgroup within Escherichia coli sequence type 131. J Clin Microbiol. 2014;52(5):1358–1365. doi:10.1128/JCM.03502-13
23. Li S, Duan X, Peng Y, et al. Molecular characteristics of carbapenem-resistant Acinetobacter spp. from clinical infection samples and fecal survey samples in Southern China. BMC Infect Dis. 2019;19(1):900. doi:10.1186/s12879-019-4423-3
24. Huang IF, Lee WY, Wang JL, et al. Fecal carriage of multidrug-resistant Escherichia coli by community children in southern Taiwan. BMC Gastroenterol. 2018;18(1):86. doi:10.1186/s12876-018-0807-x
25. Van Den Bunt G, Liakopoulos A, Mevius DJ, et al. ESBL/AmpC-producing Enterobacteriaceae in households with children of preschool age: prevalence, risk factors and co-carriage. J Antimicrob Chemother. 2017;72(2):589–595. doi:10.1093/jac/dkw443
26. Birgy A, Levy C, Bidet P, et al. ESBL-producing Escherichia coli ST131 versus non-ST131: evolution and risk factors of carriage among French children in the community between 2010 and 2015. J Antimicrob Chemother. 2016;71(10):2949–2956. doi:10.1093/jac/dkw219
27. Colmenarejo C, Hernández-García M, Muñoz-Rodríguez JR, et al. Prevalence and risks factors associated with ESBL-producing faecal carriage in a single long-term-care facility in Spain: emergence of CTX-M-24- and CTX-M-27-producing Escherichia coli ST131-H30R. J Antimicrob Chemother. 2020;75(9):2480–2484. doi:10.1093/jac/dkaa219
28. Van Aartsen JJ, Moore CE, Parry CM, et al. Epidemiology of paediatric gastrointestinal colonisation by extended spectrum cephalosporin-resistant Escherichia coli and Klebsiella pneumoniae isolates in north-west Cambodia. BMC Microbiol. 2019;19(1):59. doi:10.1186/s12866-019-1431-9
29. Saleem AF, Allana A, Hale L, et al. The gut of healthy infants in the community as a reservoir of ESBL and carbapenemase-producing bacteria. Antibiotics. 2020;9(6):286. doi:10.3390/antibiotics9060286
30. Wang L, Yang YH, Lu Q, et al. Prevalence of extended-spectrum beta-lactamase producing Escherichia coli in pediatric patients in China. Zhonghua Yi Xue Za Zhi. 2008;88(20):1372–1375. Chinese.
31. Babu R, Kumar A, Karim S, et al. Faecal carriage rate of extended-spectrum β-lactamase-producing Enterobacteriaceae in hospitalised patients and healthy asymptomatic individuals coming for health check-up. J Glob Antimicrob Resist. 2016;6:150–153. doi:10.1016/j.jgar.2016.05.007
32. Xu Q, Pan F, Sun Y, et al. Fecal carriage and molecular epidemiology of carbapenem-resistant Enterobacteriaceae from inpatient children in a pediatric hospital of Shanghai. Infect Drug Resist. 2020;13:4405–4415. doi:10.2147/IDR.S275549
33. Liu W, Chen L, Li H, et al. Novel CTX-M β–lactamase genotype distribution and spread into multiple species of Enterobacteriaceae in Changsha, Southern China. J Antimicrob Chemother. 2009;63(5):895–900. doi:10.1093/jac/dkp068
34. Zhong YM, Liu WE, Liang XH, et al. Emergence and spread of O16-ST131 and O25b-ST131 clones among faecal CTX-M-producing Escherichia coli in healthy individuals in Hunan Province, China. J Antimicrob Chemother. 2015;70(8):2223–2227. doi:10.1093/jac/dkv114
35. Xue G, Li J, Feng Y, et al. High prevalence of plasmid-mediated quinolone resistance determinants in Escherichia coli and Klebsiella pneumoniae isolates from pediatric patients in China. Microb Drug Resist. 2017;23(1):107–114. doi:10.1089/mdr.2016.0004
36. Chiotos K, Tamma PD, Flett KB, et al. Increased 30-day mortality associated with carbapenem-resistant Enterobacteriaceae in children. Open Forum Infect Dis. 2018;5(10):ofy222. doi:10.1093/ofid/ofy222
37. Chiotos K, Hayes M, Gerber JS, et al. Treatment of carbapenem-resistant Enterobacteriaceae infections in children. J Pediatric Infect Dis Soc. 2020;9(1):56–66. doi:10.1093/jpids/piz085
38. Ding Y, Wang Y, Hsia Y, et al. Systematic review of carbapenem-resistant Enterobacteriaceae causing neonatal sepsis in China. Ann Clin Microbiol Antimicrob. 2019;18(1):36. doi:10.1186/s12941-019-0334-9
39. Giani T, Sennati S, Antonelli A, et al. High prevalence of carriage of mcr-1-positive enteric bacteria among healthy children from rural communities in the Chaco region, Bolivia, September to October 2016. Euro Surveill. 2018;23(45):1800115. doi:10.2807/1560-7917.ES.2018.23.45.1800115
40. Hassan J, Mann D, Li S, et al. Emergence of the mobile colistin resistance gene, mcr-1, in multidrug-resistant E. coli isolated from the fecal matter of toddlers in a community. Antimicrob Agents Chemother. 2021;65(5):e00243–21. doi:10.1128/AAC.00243-21
41. Hu YY, Wang YL, Sun QL, et al. Colistin resistance gene mcr-1 in gut flora of children. Int J Antimicrob Agents. 2017;50(4):593–597. doi:10.1016/j.ijantimicag.2017.06.011
42. Zhang XF, Doi Y, Huang X, et al. Possible transmission of mcr-1-harboring Escherichia coli between companion animals and human. Emerg Infect Dis. 2016;22(9):1679–1681. doi:10.3201/eid2209.160464
43. Yair Y, Gophna U. Pandemic bacteremic Escherichia Coli strains: evolution and emergence of drug-resistant pathogens. Curr Top Microbiol Immunol. 2018;416:163–180. doi:10.1007/82_2018_109
44. Muller A, Gbaguidi-Haore H, Cholley P, et al. Hospital-diagnosed infections with Escherichia coli clonal group ST131 are mostly acquired in the community. Sci Rep. 2021;11(1):5702. doi:10.1038/s41598-021-85116-6
45. Mohamed M, Clabots C, Porter SB, et al. Large fecal reservoir of Escherichia coli sequence type 131-H30 subclone strains that are shared within households and resemble clinical st131-H30 isolates. J Infect Dis. 2020;221(10):1659–1668. doi:10.1093/infdis/jiz669
46. Yoon EJ, Choi MH, Park YS, et al. Impact of host-pathogen-treatment tripartite components on early mortality of patients with Escherichia coli bloodstream infection: prospective observational study. EBioMedicine. 2018;35:76–86. doi:10.1016/j.ebiom.2018.08.029
47. Ferjani S, Saidani M, Maamar E, et al. coli colonizing healthy children in Tunisia: high prevalence of extra-intestinal pathovar and occurrence of non-extended-spectrum-β-lactamase-producing ST131 clone. Int J Antimicrob Agents. 2018;52(6):878–885. doi:10.1016/j.ijantimicag.2018.07.015
48. Barrios-Villa E, Cortés-Cortés G. Lozano-Zaraín et al.Adherent/invasive Escherichia coli (AIEC) isolates from asymptomatic people: new E. coli ST131 O25: H4/H30-Rxvirotypes. Ann Clin Microbiol Antimicrob. 2018;17(1):42. doi:10.1186/s12941-018-0295-4
49. Zhang S, Zhang Q, Huang J, et al. Epidemic potential of Escherichia coli O16: H41-ST131:compared with pandemic O25b: H30-ST131Lineage. Infect Drug Resist. 2021;14:2625–2632. doi:10.2147/IDR.S313261
50. Harris PNA, Ben Zakour NL, Roberts LW, et al. Whole genome analysis of cephalosporin-resistant Escherichia coli from bloodstream infections in Australia, New Zealand and Singapore: high prevalence of CMY-2 producers and ST131 carrying blaCTX-M-15 and blaCTX-M-27. J Antimicrob Chemother. 2018;73(3):634–642. doi:10.1093/jac/dkx466
51. Birgy A, Levy C, Nicolas-Chanoine MH, et al. Independent host factors and bacterial genetic determinants of the emergence and dominance of Escherichia coli Sequence type 131 CTX-M-27 in a community pediatric cohort study. Antimicrob Agents Chemother. 2019;63(7):e00382–19. doi:10.1128/AAC.00382-19
52. Adler A, Gniadkowski M, Baraniak A, et al. Transmission dynamics of ESBL-producing Escherichia coli clones in rehabilitation wards at a tertiary care centre. Clin Microbiol Infect. 2012;18(12):E497–505. doi:10.1111/j.1469-0691.2012.03999.x
53. Peirano G, Lynch T, Matsumara Y, et al. Trends in population dynamics of Escherichia coli sequence type 131, Calgary, Alberta, Canada, 2006–2016 (1). Emerg Infect Dis. 2020;26(12):2907–2915. doi:10.3201/eid2612.201221
54. Matsumura Y, Pitout JD, Gomi R, et al. Global Escherichia coli sequence type 131 clade with bla (CTX-M-27) Gene. Emerg Infect Dis. 2016;22(11):1900–1907. doi:10.3201/eid2211.160519
55. Platell JL, Trott DJ, Johnson JR, et al. Prominence of an O75 clonal group (clonal complex 14) among non-ST131 fluoroquinolone-resistant Escherichia coli causing extraintestinal infections in humans and dogs in Australia. Antimicrob Agents Chemother. 2012;56(7):3898–3904. doi:10.1128/AAC.06120-11
56. Birgy A, Madhi F, Jung C, et al. Diversity and trends in population structure of ESBL-producing Enterobacteriaceae in febrile urinary tract infections in children in France from 2014 to 2017. J Antimicrob Chemother. 2020;75(1):96–105. doi:10.1093/jac/dkz423
57. Ding Y, Zhang J, Yao K, et al. Molecular characteristics of the new emerging global clone ST1193 among clinical isolates of Escherichia coli from neonatal invasive infections in China. Eur J Clin Microbiol Infect Dis. 2021;40(4):833–840. doi:10.1007/s10096-020-04079-0
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.