")
Back to Journals » Advances in Medical Education and Practice » Volume 10
Community-based education in the Institute of Medicine, Tribhuvan University, Nepal: a qualitative assessment
Authors Choulagai BP
Received 8 January 2019
Accepted for publication 29 April 2019
Published 27 June 2019 Volume 2019:10 Pages 469—478
DOI https://doi.org/10.2147/AMEP.S171377
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Video abstract presented by Bishnu P Choulagai.
Views: 1143
Bishnu P Choulagai
Department of Community Medicine and Public Health, Institute of Medicine, Tribhuvan University, Kathmandu, Nepal
Background: Community-based education (CBE) involves learning activities that take place in a community setting. CBE is now recognized as an important addition to medical education, because the skills of graduates are needed more in communities than in urban and tertiary hospitals. The goal of CBE is to help the students understand social dynamics of health promotion and disease prevention and to impart a sense of social justice and cultural humility. Since its establishment in 1972, the Institute of Medicine (IOM) has provided community-based education in the medical and public health programs.
Purpose: The objective of this study was to assess the organization and implementation of CBE in the IOM. This study also aimed to make recommendations based on the perspectives of students, faculty, education managers and administrative staff.
Methods: The methods employed in this study were descriptive and exploratory using primary as well as secondary data collection. Primary data were collected using a qualitative approach – five focus group discussions with the students of Bachelor of Medicine and Bachelor of Surgery and Bachelor of Public Health programs, and 13 interviews with faculty members, field coordinators, administrative staff and office-bearers of the IOM. Additionally, observation of the infrastructure for implementing CBE activities was conducted. Secondary data were collected from the field reports of the students. The results were grouped into the following themes – organization of CBE, implementation of CBE and beneficiary perspectives.
Results: The CBE has remained an important component of the undergraduate medical and public health curricula of the IOM since its establishment in 1972. The students and faculty members emphasized the importance of CBE in medical and public health education. The IOM has achieved the curricular objectives of the CBE by developing relevant guidelines and regularly conducting orientations and field activities.
Conclusions: The organization and implementation of the CBE need to be made more effective and efficient by simplifying the administrative and financial procedures, specifying teaching communities, acknowledging the support of community and stakeholders, increasing the service components in students’ field practice, and engaging the communities in planning, implementation and evaluation of CBE.
Keywords: community based education, community oriented medical education, Bachelor of Medicine and Bachelor of Surgery (MBBS), Bachelor of Public Health (BPH), health professions education, Nepal
Introduction
Community-based education (CBE) involves learning activities that take place in a community setting.1 CBE is recognized as an important addition to the methods available in medical education, because the skills of graduates are needed in the community more than in the tertiary hospital. CBE has remained an important component of the curricula in Nepalese medical schools.2–4 Community-oriented medical education (COME) refers to the objectives of a medical school and their relevance to community health needs.1 In this approach to medical education, the content of the curriculum is directly relevant to the community and to the population-based methods in which the students are trained.
Community-based education is not only learning in the community but also learning with and from the community. As the communities actively participate in CBE, they not only contribute but also benefit from the CBE process. The ultimate goal of CBE is to help the students understand social dynamics of health promotion and disease prevention and to impart a sense of social justice and cultural humility in the health professions through the education process.
Community field programs develop a student’s ability to understand community problems and to learn to address those problems. Therefore, field activities are designed to be both community-based and need-responsive which encourages students to render service while they learn and develop clinical, public health management and communication skills. The CBE programs can be classified into three main categories – service-oriented programs, research-oriented programs and training-focused programs.1
Tribhuvan University is the first university in Nepal established in 1959. This government–funded university started its medical campus – Maharajgunj Medical Campus (MMC) in Kathmandu in 1972 under the Institute of Medicine (IOM). The MMC runs academic programs in health sciences at undergraduate, graduate and doctoral levels. Certificate level health science courses were introduced in 1972, Bachelor of Medicine and Bachelor of Surgery (MBBS) in 1978 and Bachelor of Public Health (BPH) in 1986. Since its inception, the teaching and learning approach of MMC has been guided by the objectives of COME. CBE occupies a large portion of MBBS and BPH curricula.5,6 The Department of Community Medicine and Public Health (DCMPH) is engaged in developing curricula and relevant guidelines and in implementing the CBE components of the medical and public health programs of IOM. All of the affiliated medical colleges of Tribhuvan University follow the same curriculum and guidelines.
There are three major types of field activities under CBE – community health diagnosis (CHD), family health exercise (FHE) and district health systems management. Community health diagnosis is a comprehensive assessment of health status of a community in its social, physical and biological environment.7 It is a 1-month residential field visit in the first academic year of MBBS and the second academic year of BPH. In the family health exercise MBBS students make three visits to each family of five selected patients to understand the roles of the family and the patient in disease causation and recovery.5 The district health systems management field program occurs in the fourth year of the MBBS and the third year of the BPH where students spend 2 months studying district health systems and management of health institutions in a district.
A review of organization of COME in IOM in 2003 revealed that the graduates valued the contribution of COME in their education, however there was a need of improvement in orientation, supervision and logistic support.8 There has not been a more recent assessment of the organization and implementation of CBE in IOM. An assessment of the issues and challenges in organization and implementation of CBE and possible solutions are vital to strengthen the academic programs and incorporate necessary improvements in CBE. This study explored the perceived strengths and weaknesses of CBE in IOM and made recommendations. The findings of this study help initiate changes in the organization and implementation of community-based education in universities and schools of health sciences in Nepal and in other countries that share similar settings.
Methodology
Study design
The study design was descriptive and exploratory. We conducted focus group discussions (FGD) and in-depth interviews with stakeholders involved in CBE at the IOM. The curricula of MBBS and BPH, CBE guidelines, students’ field reports, the physical facilities and the availability of logistics in the academic department were also studied.
Study area and study population
We conducted this study in the medical campus of the IOM in Kathmandu. Our study population included students, faculty members, program coordinators, administrators and the office-bearers involved in organization, implementation and decision making for CBE.
Data collection
Focus group discussions and in-depth interviews
Two trained research assistants including one Master of Public Health graduate conducted the individual interviews and FGDs. All interviews and FGDs were digitally audio recorded with informed consent except for one faculty member who preferred his interview not to be audio-recorded and detailed notes were taken instead. All interviews took place in settings preferred by the participants including offices and staff-rooms. The FGDs with students occurred in a hall of the medical campus.
We conducted focus group discussions with current students and recent graduates that had completed their field program within previous 12 months. Additionally, in-depth interviews were conducted with faculty members and office-bearers involved in CBE. Three FGDs were conducted with the MBBS students – one each for community health diagnosis, family health exercise and district health systems management. Two FGDs were conducted with the BPH students – one each for community health diagnosis and district health systems management. A total of 52 students including 29 males and 23 females participated in the five FGDs. Each FGD included both male and female students.
We used an interview guide to conduct individual in-depth interviews with 13 participants including faculty members, academic program coordinators, department head, coordinator of CBE, Campus Chief, Assistant Dean of the Academic Department, faculty supervisors and staff of administration and finance from the campus. The in-depth interview guide included prompts for key issues such as organization and implementation of each field activity under CBE, strengths and weaknesses of CBE, and recommendations. Similarly, FGD guidelines included prompts for key issues such as the implementation of CBE activities, students’ perceived needs regarding orientation program, logistics, supervision and support, and recommendations. The themes emerging from earlier interview and discussions were added as key prompts in later discussions and interviews to achieve saturation.
Review of curricula and students’ field reports
We reviewed the curricula of BPH and MBBS programs and randomly selected 20 field reports prepared by the students. The information obtained from the curricula and recommendations, learning reflections and conclusions of the students’ reports were incorporated into relevant themes and categories.
Observation of physical infrastructure and resources for CBE
We collected information on physical infrastructure and resources available for organization and implementation of CBE activities. An observation checklist was used to assess these facilities.
Data analysis
The notes and audio-records of FGDs and in-depth interviews were transcribed, compiled and labelled according to participant type. Following a thorough review of individual transcriptions, we entered them into a computer in the original Nepali language. We then translated the Nepali transcriptions into English and reviewed each translation to understand the meaning of its content. During content analysis, a deductive approach was used and results were grouped into three themes, 1) organization of CBE; 2) implementation of CBE; and 3) beneficiary (students’) perspectives on strengthening CBE (Table 1).9,10 A data triangulation was done integrating information from different sources and methods.
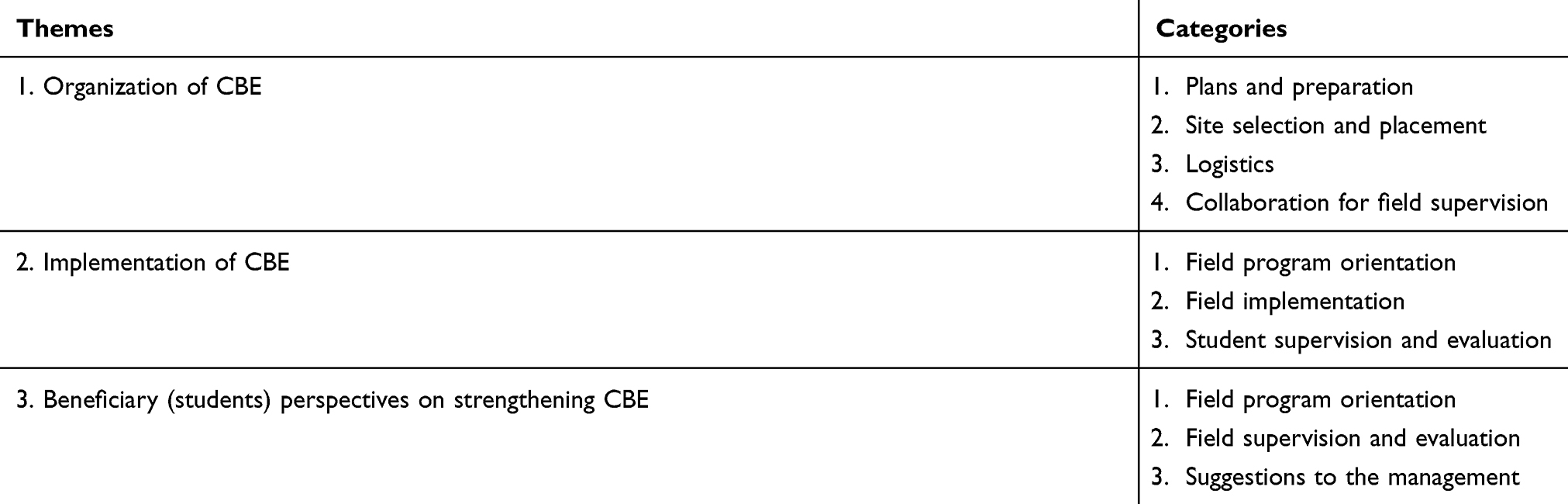 |
Table 1 Themes and categories of analysis |
Ethical considerations
Before conducting each interview and discussion, an explanation was made about the study objectives, its rationale and the extent of involvement expected from the participants. All participants gave written informed consent. We maintained the confidentiality of all interviews and discussions and no individual identifiers were mentioned in the results. The Institutional Review Board of the Institute of Medicine at Tribhuvan University provided an ethical clearance for this study.
Results
Characteristics of study participants
The participants of this study were the students that had completed their respective CBE components, the faculty members involved in CBE, the academic coordinators of MBBS and BPH programs, coordinator of CBE, administrative and financial staff, Department Head, the Campus Chief and the Assistant Dean of the Academics (Table 2).
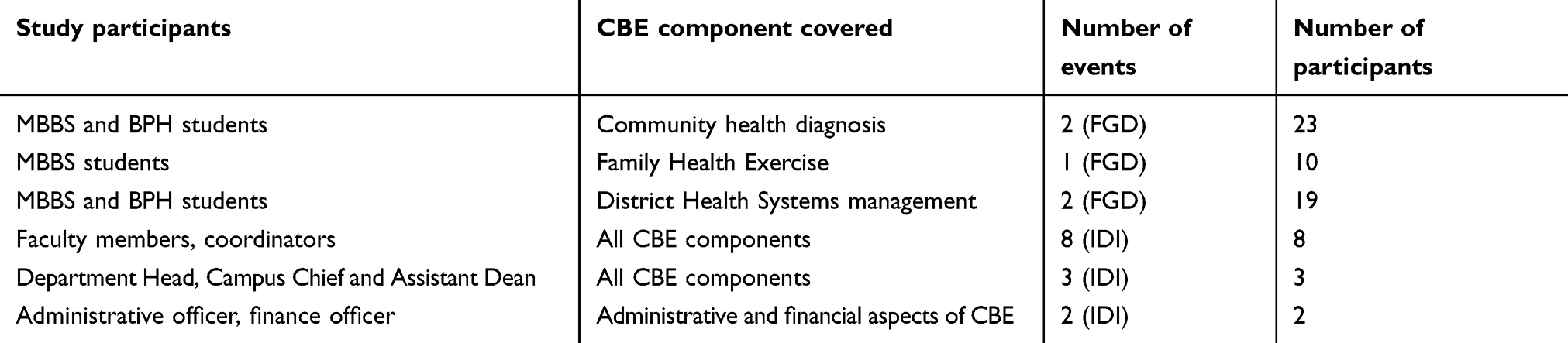 |
Table 2 Study participants and CBE components |
Community-based education is an important component of the undergraduate medical and public health programs run by our IOM. The assessment of CBE programs is discussed under various headings based on different aspects of CBE with reference to the objectives of each CBE program. The strengths, weaknesses, challenges and constraints of the CBE components and participants’ suggestions are detailed under each heading
Organization of CBE
Plans and preparation
A community-based learning unit was formed in 2012 in the DCMPH to manage all CBE activities. Prior to the formation of the unit a faculty member was appointed field coordinator to manage the CBE activities.
The following guidelines and manuals were available in the department centered at CBE activities:
- Implementation guidelines for each field program.
- Guidelines for students on writing field reports.
- Guidelines for the presentation seminar in the department.
- A checklist for students’ field supervision.
Site selection and placement
The Department of Community Medicine and Public Health requests the Campus Chief to make the necessary arrangements for field activities. The campus provides resources including stationery for students and vehicles for transporting students and faculty supervisors to the field. The campus also provides daily allowances to students and faculty supervisors.
The site selection for community placement is done by agreement between campus and study sites (district or community) following a feasibility study. The feasibility study ensures there is adequate accommodation for students, obtains permission from the community or district stakeholders, orients stakeholders and ensures they will support the students. A faculty member recalled:
During 1990s, the institute defined teaching districts which students would attend regularly. At that time Dhading and Sindhupalchowk districts were proposed as teaching districts and a field training center was established in Chautara, Sindhupalchowk. This center is still running and has residential facilities. However, this concept did not receive sustained attention and currently teaching districts identified by IOM are non-existent. Now, the villages or districts are assigned for community placement from the feasibility study before placement of each field.
As the teaching districts have not been specified, the academic department conducts separate feasibility studies in potential field sites each time students are sent to field for CBE. With the increasing number of students in both MBBS (current intake of 76 students per annum while the student intake in the first batch of MBBS was 20 in 1978) and BPH (current intake of 40 students per annum while the student intake in the first batch of BPH was 10 in 1986), the department has to identify a large number of new sites each academic year.
Logistics
The vehicles at the campus are inadequate for the CBE purposes, so faculties are required to hire vehicles for the feasibility study and for student supervision. From the year 2012, campus started to allow faculty members to hire private vehicles for CBE activities, however, faculty members perceived that there is still a need to simplify the process of hiring vehicles and the financial clearance after returning from the field.
The faculties perceived that the daily allowance provided during field supervision was inadequate and a disincentive to going to the field to supervise. The perception of both faculty members and leadership agreed about the inadequacy of the allowances that the faculties received during the field supervision. A faculty member stated:
The daily allowance a faculty receives during supervision visit is insufficient to cover daily living expenses; they have to use their own financial resources and thus faculties are not motivated to go for field supervision. The campus has to provide an enabling environment. Even after returning from the field, we still have to justify and prove the normal expenses that have occurred in field.
Collaboration for field supervision
The health institutions, where the students are based, are supposed to provide the students with data and a designated staff member as the local supervisor during whole period in the field. The local supervisor is also required to evaluate the students’ field activities based on the curriculum. The district stakeholders are concerned that their support to the IOM students is not well recognized. This could be addressed by providing the stakeholders an opportunity to take part in the students’ presentation in IOM, providing them with an appreciation letter or providing the staff honorarium for the supervision and support they extend to the students during their field visit. A BPH student mentioned during the FGD: “The authorities of health institutions hesitate to cooperate us because they are not getting any monetary incentive.”
Although the students felt that the field programs were useful for them, they mentioned improvements that could be made to CBE. Both the students and faculties have suggested adding a service component. BPH students in the FGD mentioned:
Many colleges are sending their students in the communities, we also go there and collect information on the community problems but cannot really help them solve the problems. Hence, it has been difficult for us to deal with the community leaders.
Implementation of CBE
Field program orientation
Student orientation occured a week before the students go into the field. Departmental faculties facilitated various sessions of orientation. Faculties from other departments eg, department of psychiatry discussed psychosocial aspects. Additionally, experts from other organizations were also invited to facilitate a few sessions as per need eg, officials from the Ministry of Health and Population were sometimes invited to discuss the organizational structure and functions of the ministry from central to peripheral level. Based on the knowledge they acquired during their regular classes, students developed methods and tools during the orientation. For community diagnosis, students also performed pre-testing of tools in a nearby community and finalized the tool with the help of faculties during the orientation. During orientation, students acquainted themselves with the conceptual framework of what they would be studying in the community. The following contents were covered during the orientation:
- Information about the study district and community including the contact details of key persons.
- Proposal for field study including methods and action plan.
- Discussion on each component of activities to be accomplished in the field eg, epidemiological study, five year plan on dealing with a selected health problem, micro health project and critical analysis of an issue in program implementation.
- Presentation skills and report writing.
- Criteria for student evaluation.
The students prepared a proposal and tools required for carrying out the field study under the faculty’s guidance.
Implementation of field programs
The IOM and the Ministry of Health have an agreement that the IOM does not need to pay any monetary incentives to the stakeholders (eg, the hospitals or the public health office) in the field where the students are sent for their learning practice. However, there were instances where the stakeholders were not aware of the agreement. Stakeholders in some districts (eg, the hospital development committees) decided that they would charge a fee for student field placement for any institution. In some instances, this caused the department to seek another district for field placement than that which was originally planned, as mentioned by a faculty member:
Two years back, we met the superintendent of a public hospital as part of our feasibility study and requested to allow our students for field placement. He told us that the hospital development committee has decided to charge a fee for the students coming from any institution to allow for field practice in the hospital. Then we had to choose another hospital for students’ field placement.
Faculties and academic coordinators also emphasized that this issue gained more importance recently since there were many health science colleges established in the private sector. The private colleges pay fees to organizations where they send students for field practice. With the increasing number of medical, public health and nursing colleges, the hospitals and institutions are overburdened with the students that come for field practice. Thus, IoM also has to find some way to recognize the support of the stakeholders in the field.
Both the faculties and students agreed that the service component is essential for ensuring effective cooperation from the districts and communities. Students emphasized the involvement of specialist physicians as well in their family visit. These specialists could provide some services and expert advice to the patient and their family that eventually results in greater cooperation from the family members. An FGD participant MBBS student mentioned: “It would be useful if the physicians also accompany the supervisor’s team that accompanies us in some of the family visits. This way the family also gets some services.”
The faculty and students highlighted challenges and constraints in implementation. The faculty members highlighted the importance of regular dialogue between the academic department, the campus administration and the dean office so that the officials would have the same level of understanding regarding all aspects of the CBE. The faculties have suggested that the administrative and financial procedures including financial clearance after completion of field supervision be made less time consuming.
The department head, campus chief and assistant dean of academics also emphasized the importance of dialogue among management, faculties and the students to deal with any problems. In addition, they also felt the need to discuss similar programs with other universities and medical schools and mutually learn the best practices in CBE.
As there was a unit for CBE established within the department, faculties suggested that administrative and financial matters related to CBE could be best dealt by the unit with support from the campus. Faculties were dissatisfied with the level of cooperation received from the campus administration during financial clearance. The leadership also emphasized the importance of logistic support to the department: “Sufficient number of faculties is important but it is also equally important to provide adequate administrative support to the department.”
Student evaluation
The evaluation of students for CBE activities started from orientation and continued in field and final viva. Student evaluation was done during orientation based on attendance, participation in group work and development of tools and proposals. Further, evaluation was done with a checklist during the field supervision by faculties.
In community health diagnosis, usually two supervision visits by faculty members to the field were made during the total length of field study. The first supervision took place after students had completed 10–12 days of stay in the field and the second during the last week of the field placement. In district health systems management two to three supervision visits to the field were made. Local supervisors were usually the district health officers, public health officers or health institution in-charge.
Students learning reflections from CBE
Students appreciated the CBE components of the curriculum and considered it as a useful opportunity to put the theory into practice for the development of essential skills and very helpful for their career after they graduate. BPH students in the FGD stated:
After graduation, we are supposed to work in the community. Hence, CBE is useful because we can already have such exposure in the community and learn how to effectively deal with community and other stakeholders.
The students were sent to the field in groups of 5–10. The department instructed students select their own team members so that they feel comfortable during the field visit and perform effective teamwork. However, the department valued inclusivity and balance was sought with respect to gender, nationality and ethnicity. Foreign nationals were sent with Nepali students and not in a separate group. This was because it could be difficult for foreign students to perform field activities owing to language barriers and cultural differences. The field unit facilitated the formation of the students’ team. Students got the opportunity to learn how to work within a group and with the community and stakeholders during the field work. The field activities provided them a learning opportunity to work in a team and effectively deal with the community and stakeholders in a real setting. A BPH student during FGD stated:
We collect and analyze data by dividing work among us. Then we share our findings with the community. In such process we identify felt needs, observed needs and determine the real needs for conducting a micro health project.
The team coordinator, selected among each group of students, is the contact person of the team for communicating with the department on the matters related to the field. Thus, the coordinator was expected to communicate effectively with his or her team members, as well as with the departmental faculties. The students learned group dynamics and developed the skills of effective team work.
Beneficiary (students’) perspectives on strengthening CBE
Field program orientation
Students were not uniform in their views about the effectiveness of the field orientation. While most of the students found orientation helpful in understanding the concepts needed to carry out field activities, a few students opined that the orientation was hardly useful for them when it actually came to applying it in a field situation. It was difficult for the students to grasp the DHSM orientation sessions because it was not adequately backed up by theory classes on district health systems as outlined in the curriculum. The MBBS students in FGD mentioned:
Faculties tried to make orientation classes effective but it was not backed adequately by the required theories. The district health systems theory coverage is inadequate in regular classes. Without required theoretical backup, what is the meaning of orientation?
Further, students had difficulty in remembering some of the topics covered during orientation. They emphasized the importance of more practical sessions and facilitation by the assigned faculty supervisors in their groups. The MBBS students in FGD mentioned:
We tend to forget the things discussed in orientation by the time we actually work in the field. It would be better if faculties incorporated more practical sessions like role-play which help us better understand the topic and retain the knowledge and skills taught. Moreover, if the supervisors are assigned to us on first or second day of orientation, we can work with them in developing proposal and tools, then it would be more effective.
In the family health exercise four half-day orientation sessions were conducted. Before going to this field in the MBBS third year, students had already become familiar with the concept of family health which they studied in the first academic year. The orientation sessions focused on how to appropriately deal with the family in various situations including effectively dealing with the psychological aspects. Students were also oriented on the techniques of studying how the illness of a member affects a family and the role of family in the progression and recovery of diseases. During FHE orientation, students developed the proposal and tools.
Field supervision and evaluation
The students’ perception differed in some issues regarding the adequacy and quality of supervision they received in the field. A few students found the field supervision as very short and inadequate, as stated by BPH students in an FGD:
Faculties came twice for supervision during our community health diagnosis field. In the first supervision, they met us in a teashop and talked with us briefly for two to three hours. In the second supervision, the faculties came at the time we were packing our stuff after completing our field stay.
A few students expressed dissatisfaction over not receiving a valid reason for not getting pass marks even for those who were regularly present in the field. Students of MBBS mentioned in FGD:
Some of our friends failed in the results of final viva. They were regularly present during the field. While we approached the department to learn the reason for the results, we were told "it was an accident, I do not know how you failed".
Suggestions to management
There were pick up and drop off services to students for the field. If the campus was unable to provide pick up and drop off services, the students used public vehicles to reach the field and during their return which were later reimbursed by the campus. In the family health exercise field, however, the students managed their transportation expenses themselves.
For the period of field stay, students received a fixed allowance per day for food and accommodation. The field allowance did not cover all of their field expenses and students had to arrange supplementary finance to support them in the field. Although the students’ fees increased annually, the allowance they received increased only every few years. MBBS students mentioned in the FGD: “Since fees increase each year, the allowance that a student receives for the field should also increase accordingly.”
Discussion
The findings and recommendations generated from this qualitative assessment are not intended to be prescriptive, but to provide universities and academies as an evidence base for the improvement in existing CBE.
A community-based approach to medical education has remained an integral part of Nepalese medical school curricula.2–4,11 Community-based education (CBE) is the broad set of teaching and learning strategies that enable youth and adults to learn what they want to learn from any segment of the community. It may also be defined as experiential learning where students and lecturers collaborate with communities to address problems and issues. Simultaneously both are gaining knowledge and skills and advancing personal development. There is an equal emphasis on helping communities and providing learning experience to students.12 The physicians trained in traditional curricula viewed disease and its remedy through the biomedical model, however, a search for alternative strategies for training physicians was initiated by the third quarter of the last century. COME came as a response to the need for reorienting medical education.13 CBE is one of the important teaching learning approaches of Tribhuvan University’s Institute of Medicine, and occupies a large portion of MBBS and BPH curricula. The Bachelor of Nursing (BN) curriculum has also emphasized community-based education based on the problems and needs of the country.14
Community-oriented medical education (COME) of the IoM has covered three distinct kinds of CBE activities.5 The community diagnosis field focuses on imparting necessary skills on comprehensively assessing health status of a community, identifying resources and devising micro health projects to address the priority health problems. The family health exercise gives students an opportunity to look at the patient in their family context and to understand the role of the family in recovery from illness. Finally, the health systems management field prepares the students for the roles they are expected to perform in a health system after they graduate. Thus, the curriculum of IOM can be viewed as covering the essential aspects of community-oriented medical education. International bodies and educational experts in the country view COME approach of IOM with great favor.8
The available literature on the COME in medical curricula reveals that all institutes and universities running the MBBS and BPH programs have given strong emphasis to community-based education.3–6 The approach to COME, however varies from one institute to another. Thus, it is important that all the related institutes, universities, professional councils and government stakeholders come together and discuss how to find out most relevant approach to COME in the Nepalese context. This will also be an opportunity for the respective institutions to review their stated institutional objectives and success in the actual implementation, and thus come up with realistic curricula that will maximize both the learning of the students and the service to the communities.
CBE consists of learning activities that utilize the community extensively as a learning environment in which not only students, but also teachers, members of the community, and representatives of other sectors are actively involved throughout the educational experience.15 Thus, it is also important to involve the communities in such discussion. It has been emphasized that to strengthen community-based medical education, medical institutions must design innovative intervention strategies to address health problems using the available resources with active participation of the community.2
The Nepal Health Professional Council’s minimum requirements for the BPH Program make it mandatory to include “community health diagnosis” and “comprehensive field training” as part of the BPH Curriculum.16 The Nepal Medical Council’s accreditation standards for the MBBS program and regulations for post-graduate medical education regarding MD in Community Medicine have also made it mandatory to have community-based learning as well as exposure to the public health office at district levels for both the MBBS and MD Community Medicine programs.17,18
The BP Koirala Institute of Health Sciences in Dharan, Nepal has introduced “multiprofessional exposure to community diagnosis program” in MBBS first year with the objectives of fostering team work, bridging the gap between the professionals and identify current scenario of different systems. Similarly, in the second year of MBBS, they have field work for studying health care delivery systems and in the third year they have a family health exercise.3 These three kinds of field work in CBE are similar to those that are included in IOM MBBS curriculum. However, in IOM the students of different programs are not sent together in the field. The MBBS curriculum of BP Koirala Institute of Health Sciences has also included “educational research methodology” and “Community Oriented Compulsory Residential Rotatory Internship Program”.3 The CBE components of Kathmandu University School of Medical Sciences include community diagnosis in the first year, community intervention project in the second year (including awareness of health and disease, promotion of maternal and child health, promotion of hygiene and sanitation and uplifting the health care utilization) and a specific intervention project in the third year that includes school health, occupational health, and the health delivery system.4
The community-based approach in medical and public health education is helpful to students in their further study, as an assessment of graduate public health education in Nepal found that the Master of Public Health Program of Nepalese universities emphasized community-based thesis as a part of their curricula.19 A study among the Master of Public Health alumni from low- and middle-income countries emphasized the importance of collaboration in community-based participatory efforts for enhanced competency of public health graduates.20 The results from the current study also showed demand from the students to increase the CBE components that involve research because most of the graduates were directly pursuing their post graduate education. Further, this study has shown a need to increase service components and identification of teaching districts and communities to facilitate active cooperation from the community and stakeholders.
Conclusions
The community-oriented medical education has remained an important objective of the IOM at Tribhuvan University since its establishment in 1972. The CBE activities are an integral part of the undergraduate medical and public health curricula of the IOM. The faculties and management at the campus and institute have adequate understanding of the importance of CBE. The institute is regularly implementing the field activities and has met the objectives of CBE as mentioned in the curricula of MBBS and BPH Programs.
There is a need of revision in the operational aspects of CBE in IOM including the simplification of administrative and financial procedures. Identification of teaching communities and districts and increasing service components and following up the communities would result in enhanced cooperation from the community stakeholders and richer learning opportunities for the students.
Abbreviation list
BPH, Bachelor of Public Health; CBE, community-based education; COME, community-oriented medical education; DCMPH, Department of Community Medicine and Public Health; FGD, focus group discussion; IOM, Institute of Medicine; MBBS, Bachelor of Medicine and Bachelor of Surgery; MMC, Maharajgunj Medical Campus.
Acknowledgments
The author thanks Prof. Sharad Onta and Prof. Jagdish Prasad Agrawal for their encouragement to conduct this study and for offering their advice during preparation of the research proposal. I acknowledge the students of MBBS and BPH Programs, faculty members and program coordinators who participated in this study. Thanks go to Mr Prakash Joshi, Ms Poojan Sharma and Ms Ritu Paudel for their assistance in the collection and transcription of qualitative data. Thanks also go to Mr Shiva Prasad Sapkota, Dr Binjwala Shrestha, Ms Saraswoti Singh and Mr Rajan Paudel for sharing their ideas and comments on the proposal of this study. The author is grateful to Susan Clarke, MBBS, PhD from Australia for providing a thorough editing of English language of this article. This study received partial funding from the Faculty Research Grants of the University Grants Commission of Nepal.
Disclosure
Dr Bishnu P Choulagai reports partial funding from the University Grants Commission, Nepal, during the conduct of the study.
References
1. Magzoub ME, Schmidt HG. A taxonomy of community-based medical education. Acad Med. 2000;75(7):699–707.
2. Marahatta SB. Community-based medical education: prospects and challenges. Kathmandu Univ Med J. 2009;7(27):194–195.
3. BP Koirala Institute of Health Sciences. The MBBS Curriculum of BPKIHS. Dharan: BPKIHS; 2014.
4. Kathmandu University School of Medical Sciences. MBBS Curriculum. Dhulikhel: Kathmandu University; 2011.
5. Institute of Medicine. Curriculum of Bachelor of Medicine and Bachelor of Surgery. Kathmandu: National Center for Health Professions Education; 2008.
6. Institute of Medicine. Curriculum of Bachelor of Public Health. Kathmandu: National Center for Health Professions Education; 2011.
7. Hale C, Shrestha IB, Bhattacharya S. Community Diagnosis Manual.
8. Devkota MD, Adhikari RK, Shrestha B, Thakur AK. Community oriented medical education (COME): experiences at the Institute of Medicine. J Nepal Med Assoc. 2003;42(146):74–78. doi:10.31729/jnma.797
9. Mayring P. Qualitative content analysis. Forum Qual Soc Res. 2000;1. Available from: http://www.qualitative-research.net/index.php/fqs/article/view/1089/2385. Accessed December 28, 2018.
10. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24:105–112. doi:10.1016/j.nedt.2003.10.001
11. Dixit H. The Quest for Health: The Health Services of Nepal.
12. Wikiversity. Introduction to community-based learning. Available from: https://en.wikiversity.org/wiki/Introduction_to_Community-Based_Learning.
13. Adhikari RK, Onta SR. Essentials of Medical Education.
14. Shahi M, Agrawal JP. Feasibility study on upgrading the bachelor nursing curriculum in Nepal. Glob J Med Public Health. 2013;2(5):1–12.
15. World Health Organization. Community-Based Education of Health Personnel. Report of a WHO Study Group. Report number 746. Geneva: WHO; 1987. Available from: http://www.who.int/iris/handle/10665/41714. Accessed January 3, 2019.
16. Nepal Health Professional Council. Minimum Requirements for the Recognition of Bachelor in Public Health. Kathmandu: Nepal Health Professional Council; 2011.
17. Nepal Medical Council. Accreditation Standards for the MBBS Program. Kathmandu: Nepal Medical Council; 2017.
18. Nepal Medical Council. Regulations for Post-Graduate Medical Education. Kathmandu: Nepal Medical Council; 2017.
19. Mahat A, Bezruchka SA, Gonzales V, Connell FA. Assessment of graduate public health education in Nepal and perceived needs of faculty and students. Hum Resour Health. 2013;11(1):16. doi:10.1186/1478-4491-11-16
20. Zwanikken PAC, Alexander L, Huong NT, et al. Validation of public health competencies and impact variables for low- and middle-income countries. BMC Public Health. 2014;14(1):55. doi:10.1186/1471-2458-14-55
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.