")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Community Attitude Towards Epilepsy Patients and Associated Factors in South Achefer District, Northwest Ethiopia: A Mixed-Methods Study
Authors Tirukelem H, Nigatu SG , Angaw DA , Azale T
Received 27 November 2020
Accepted for publication 13 January 2021
Published 9 February 2021 Volume 2021:17 Pages 365—377
DOI https://doi.org/10.2147/NDT.S292257
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Roger Pinder
Hewan Tirukelem,1 Solomon Gedlu Nigatu,2 Dessie Abebaw Angaw,2 Telake Azale1
1Department of Health Education and Behavioral Science, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Solomon Gedlu Nigatu Email [email protected]
Background: Epilepsy, defined as seizure activity that is recurrent, unpredictable, and typically unprovoked. It is one of the most common disorders of the nervous system. Sociocultural attitudes in many African nations continue to have a negative impact on epilepsy management. It has been found that stigma and discrimination against people with epilepsy are more devastating and harmful than the illness itself. This is mainly attributed to misconceptions about the disease with fear and fright of the public on confronting an epileptic seizure. So, the current study assesses the community’s attitude toward epilepsy patients and associated factors towards epilepsy in South Achefer District, Northwest Ethiopia.
Methods: Community-based cross-sectional study triangulated with the qualitative method was conducted from March 1 to May 30, 2020 in South Achefer District. A systematic sampling technique was used to select a total of 762 individuals. Data were collected by face-to-face interview using a structured questionnaire and analyzed using SPSS version 23. Logistic regression analysis was performed and P < 0.05 with a 95% confidence interval was considered to measure statistically significant variables. For the qualitative study participants were selected purposively. Focus Group Discussion, key Informant Interview, and Individual Depth Interview were conducted until it reaches the point of saturation. Thematic analysis was done by using an open code software version 4.2.
Results: A total of 753 respondents participated which gave a 98.8% response rate. Among those 60.8% (95% CI: 57.2– 64.3) were found to have a favorable attitude towards epilepsy patients. Being informed about epilepsy (AOR=1.47; 95% CI, 1.02– 2.11), witnessing seizure in the past (AOR=1.6; 95% CI, 1.14– 2.27), and having good knowledge about epilepsy (AOR=2.08; CI, 1.49– 2.89) were the variables that showed statistically significant association with a favorable attitude.
Conclusion: The favorable attitude of the community towards epilepsy patients was found high in the study area. Information about epilepsy, witnessing seizure, and knowledge about epilepsy showed a significant association with attitude. Therefore, health professional and health extension workers should provide a larger and comprehensive community-based education to enhance people’s knowledge about epilepsy to bring attitude change against a negative attitude towards epilepsy.
Keywords: attitude, epilepsy, Ethiopia
Introduction
Epilepsy is one of the most common disorders of the nervous system characterized by a recurrent seizure due to sudden excessive disorderly discharge of the cerebral neurons. The type of seizure, however, depends on which part of the brain is affected, how much of the brain is affected, and what happens during the seizure.1,2
Epilepsy had a high prevalence in the world among neurological disorders, affecting more than 69 million people annually.3 More than 85% of cases occur in low- and middle-income countries.4 In Sub-Saharan Africa, active epilepsy is estimated at around 4.4 million people.5 In Ethiopia, the lifetime prevalence of epilepsy was reported at 7.60 per 1000 persons. The cumulative incidence was recorded as 67.77 per 100,000 persons annually.6
There are many different causes of epilepsy include genetics, head trauma, meningitis, brain tumors, stroke, and multiple sclerosis are possible causes. However, in many instances, the cause is unknown.7 One of the bad consequences of epilepsy is sudden and unexpected death which accounts for around 17% of deaths in epilepsy.8 In addition, People with Epilepsy (PWE) are directly affected by fractures, scalding, and bruising due to seizures, suicide, pneumonia, and status epilepticus.9 This can affect not only PWE but also their families and the country at large, directly or indirectly.
Stigma and discrimination affect PWE more than the disease-related effects such as disability associated with repeated seizures or side-effects of antiepileptic drugs. This discouraging them from discuses about the problem and gaining treatment freely, due to fear of being known by others.10,11 In developing countries, children with epilepsy in particular be banned from school due to the stigma and discrimination.12,13
Community attitude is an important determinant in the early treatment and care of epilepsy patients. A study conducted in Trinidad and Tobago indicates that 93% of study participants have a favorable attitude towards epilepsy.14 A similar study in south India also showed that 77.7% of the respondents have a positive attitude toward epilepsy.15 Whereas a study has been conducted in Vietnam, 33% of individuals have a favorable attitude towards epilepsy patients.16 In our country, a study conducted in Menit communities indicated that about 13.2% had a favorable attitude towards epilepsy patients.17 In Ethiopia, there is a widespread cultural belief about the cause of epilepsy as demon possessions, by evil spirits, ancestors’ spirits, and evil eyes.18
The attitude of the community in epileptic patient care is a paramount determinant because it affects the help-seeking behavior of PWE, their adherence to medication, and their interaction with the community. Therefore, this study aims to assess the community’s attitude and associated factors in South Achefer District.
Materials and Methods
Study Design and Participants
Community-based cross-sectional and phenomenology study designs were conducted in South Achefer District, West Gojjam Zone, Northwest Ethiopia from March 1 to May 30, 2020. The District is located 110 km from Bahir Dar and 500 km from Addis Ababa, the capital city. Based on the 2007 national census conducted by the Central Statistical Agency of Ethiopia (CSA), it has a total population of 165,408 (79,927 are males and 85,481 are females), of whom 138, 755 resides in the rural kebeles (the smallest administrative unit of Ethiopia) and 26,653 are urban inhabitants. Regarding health facility, there are 23 health posts, 8 health centers, one primary hospital, and 2 medium private clinics, and 11 drug stores in the District.19 All adults in South Achefer District were considered as the source population; for qualitative study: religious leaders, health extension workers, health development army (HAD) leaders, and PWE were included. For the quantitative study, sample size has calculated using a previous study done in the East Gojjam zone as 65.7% of the participants have a favorable attitude toward epilepsy patients.20 This was calculated using a single population proportion formula. The following assumptions were taken in to consideration to come up with the final sample size; Zα/2 = 1.96 confidence level (CI) = 95%, margin of error (d) = 5%. A design effect of 2 was taken. The non-response rate was considered as 10% of the calculated sample size. Our final sample size was 762 study participants. A multistage sampling technique was employed. A simple random sampling technique was used to select six kebeles (26%). Households’ in the selected kebeles were selected by a systematic random sampling technique and the first house was selected by a lottery method from the first 13 households. Every 13th household was interviewed. For those households that had more than one eligible Participants, one study unit was selected by using the lottery method.
For the qualitative study, a purposive sampling technique was used. Participants were selected purposively to include people with the most information about the topic. One IDI (Individual Depth Interview), five KIIs (key Informant Interview), and seven FGDs (Focus Group Discussion) sessions were conducted based on saturation. KIIs were taken from religious leaders, health development army (HDA) leaders, and from health extension workers and IDI from people with epilepsy. The participants in FGD were with the same socio-demographic status to get detailed information from participants and to express their opinions freely. There was a total of seven FGDs, three from rural dwellers, and four from urban dwellers, with an average of seven participants in each FGD and a total of 50 study participants in seven FGD.
Data Collection Tools and Measurement
The quantitative data were collected by a face-to-face interview using a structured questionnaire. It was adapted and modified from different kinds of literatures.17,20–22 The questionnaire has five components: socio-demographic characteristics, Health facility-related factors, experience with epilepsy, knowledge about epilepsy, and attitude towards epilepsy. To measure knowledge (17) items were used (4 Yes/No items, 2 single answer multiples choose and 3 multiples choose with multiple answers). For the correct knowledge answer, we assigned 1 and for the wrong answer, we gave 0. The composite score of knowledge range from 0−17. It was dichotomized a score ≥9 as good knowledge and <9 score poor knowledge., Internal consistency (reliability) of the knowledge item was checked by using Cronbach alpha and we found 0.652. For information and health facility-related factors (4) items and experience about epilepsy (3) items was used. Attitude towards epilepsy patient’s subscale was assessed using 14 items. It was measured by a Likert-scale question which is rated from 1 to 5 values (lowest value strongly disagree to highest value strongly agree). A response that is either strongly agree or agree consider as favorable attitude regarding epilepsy patient and coded to “1” the remaining response: strongly disagree, disagree or neutral coded to “0”. By adding those 14 attitude questions, it yields maximum 14 score or minimum 0 score. The mean score value ≥7 (50% and above) of attitude response was taken as having a favorable attitude towards epilepsy patients. Similarly, attitude response scored a mean value less than 7 taken as an unfavorable attitude towards epilepsy patients. The Cronbach’s alpha value of attitude subscale was 0.79.
Qualitative data were collected by using open-ended questions. Questions were accompanied by several probes to get a deep insight into participants’ beliefs. The guides were pretested to ensure their relevance and appropriateness. FGD, KIIs, and IDI were used to collect the data. Items in the qualitative data include socio-demographic data, knowledge about epilepsy, attitude towards epilepsy, and cultural beliefs of the community about causes and treatments of epilepsy.
Data Quality Control Measures
The questionnaire was first prepared in English then translated into the local language (Amharic) and a backward translation was done by different language experts to increase the consistency. Data were collected by five-diploma holding nurses and supervision was made by two health officers. Two days of training was given to the data collectors and supervisors on how to conduct the data collection. During data collection, close supervision was made by the supervisor, for observing how data collectors run the questions to the respondents, and the collected data were checked for accuracy and clarity. This quality checking was done daily after data collection and correction was made before the next data collection. Data clean up and cross-checking was done before analysis. To assure the quality of data the questionnaire was pretested among 5% (38 individuals) of the study from an adjacent district 1 week before the data collection time which was not included in the study and after the pretest, the questionnaire was modified accordingly.
For the qualitative part, FGD, IDI, and KII guides were first prepared in English and translated into a local language (Amharic) by the principal investigator. The IDI, KII, and FGD session was moderated by the principal investigator. The responses were tape-recorded, and notes were taken by one diploma-holding nurse. Separate and silent rooms were used to conduct the interview. The rigor of the findings was ensured by different approaches. There were debriefing sessions every day during data collection. An effort was made to ensure consistency between the data before and after translation.
Data Processing and Analysis
The collected data were checked for its completeness and given the code and entered into EPI-data of version 4.6 and exported to SPSS version 23 for further analysis. Frequencies and cross-tabulations were done to summarize descriptive statistics of the data and tables and graphs were used for data presentation. Bivariate analysis has been used to check which Variable is individually associated with the dependent variable. Those variables that showed statistical association (P < 0.2) with the dependent variables were then entered into multivariate analysis to control the possible effect of confounders and finally, the variables which have significant association were identified based on OR, 95% CI, and p-value <0.05 to fit into the final regression model. Model adequacy by Hosmer and Lemeshow was fulfilled, which was 0.53. For the qualitative study data, collection and analysis were undertaken simultaneously in line with the iterative nature of qualitative methods. Data from the FGD, IDI, and KII were transcribed (verbatim transcription) and translated into English. The transcripts and translations were cross-checked for accuracy and consistency. Thematic analysis was done by using an open code software version 4.2. Then, similar codes were brought together forming categories. Thematic areas were identified based on the objective of the study. Different ideas were organized under the themes. The ideas were organized into concepts and presented in narratives using a transcribed form of the study participant’s explanation. Finally, the narrative qualitative information was triangulated with quantitative findings.
Operational Definitions
Knowledge About Epilepsy
Community knowledge about epilepsy was obtained by self-rated responses from 17 items that have “Yes”/No choices. For the correct response “one” point was given and a “zero” point was given for wrong answers. Based on this those who scored >50% (9−17 points) were considered as having good knowledge about epilepsy.20,23
Attitude Towards Epilepsy Patients
Community attitude towards epilepsy patients was obtained by self-rated responses from 14 items. Those who scored >50% or greater than or equal to 7 items from attitude-related questions were considered as having a favorable attitude.20,23
Results
Socio-Demographic Characteristics
A total of 753 respondents had participated in the study with a response rate of 98.8%. The mean age was 40 (SD±13) years. Among the study participants, 399 (53%) were females. Three hundred sixty (47.8%) of the participants cannot read and write. The majority of (712, 94.6%) were orthodox Christian religion followers. Most of the respondents (613,81.4%) were rural dwellers. More than two-third, 599 (79.5%) of the respondents were married (Table 1).
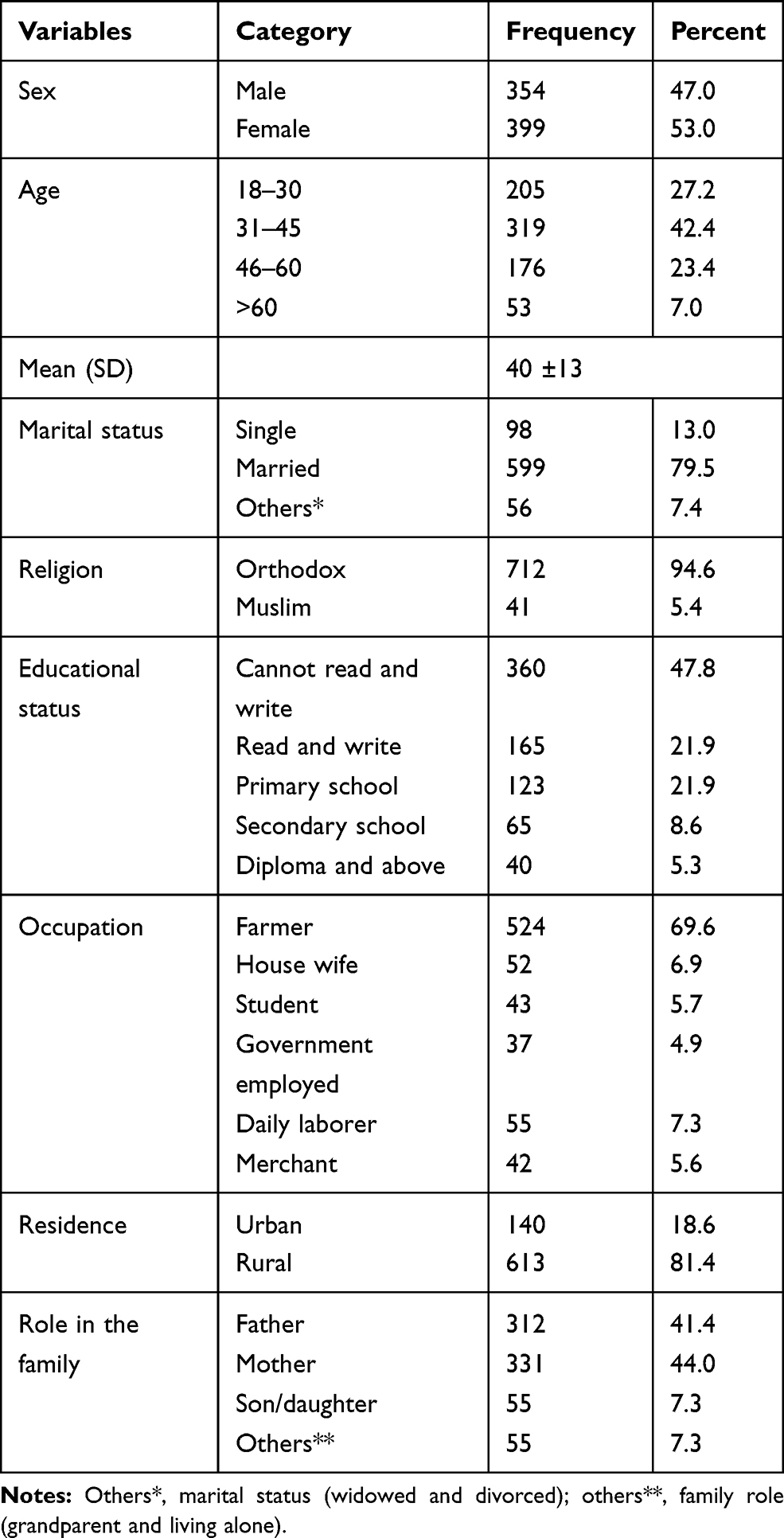 |
Table 1 Socio-Demographic Characteristic of the Study Participants (n=753), in South Achefer District, Northwest Ethiopia, 2020 |
A total of 58 respondents had participated in the qualitative study. Among them 50 from the FGD, 7 from KII, and 1 from IDI. In the FGD majority of the respondents were orthodox religious followers. Regarding age, most of the study participants were within the age range from 28 to 52 years. Of the total participants, 26 of them were males and 24 of them were rural dwellers. The majority of them were married. Regarding occupation, almost half of the study participants were farmers (Table 2).
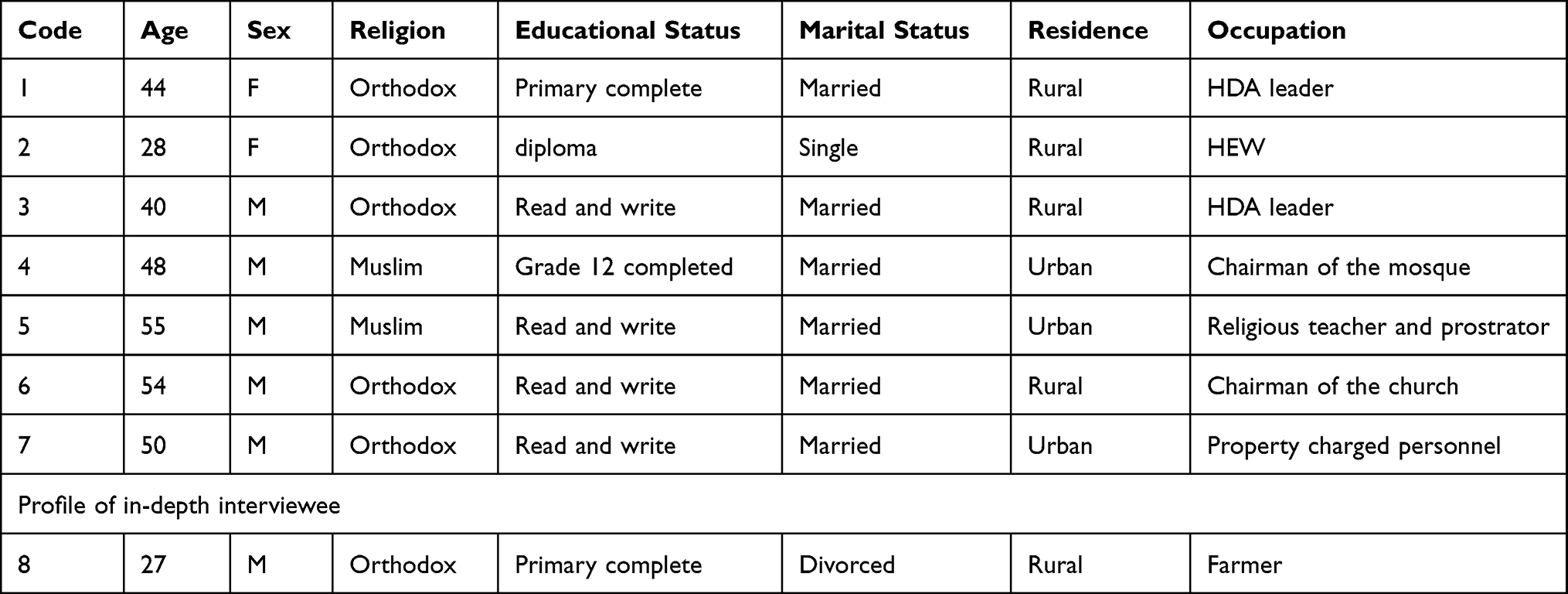 |
Table 2 Profile of Study Participants in KIIs in South Achefer District, Northwest Ethiopia, 2020 |
Information, Experience, and Health Facility-Related Factors
Participants were asked whether they have heard or read about epilepsy. Only 299 (39.7%) had heard about epilepsy. Regarding the prior source of information about epilepsy 98 (13.0%) of the participants had got the information from their family.
Among our study participants, 294 (39.0%) needed 31–60 minutes to reach a health facility. Whereas 233 (30.9%) takes less than 30 minutes and 226 (30.0%) of the participants take more than one hour to reach the health facility. Almost half of the respondents (395, 52.5%) had witnessed a seizure in the past but only 184 (24.4%) and 83 (11.0%) had a friend and a family member with epilepsy, respectively.
Knowledge About Epilepsy
Participants were asked if they know about the causes of epilepsy 345 (45.8%) said that spirit possession was the main cause. About the treatment of epilepsy 241 (32.0%) respondents suggested holy water as the specific treatment. Regarding seizure treatment 88 (25.0%) let patients smell the lit match smoke. About affected age groups 319 (42.4%) said that epilepsy affects all age groups (Table 3).
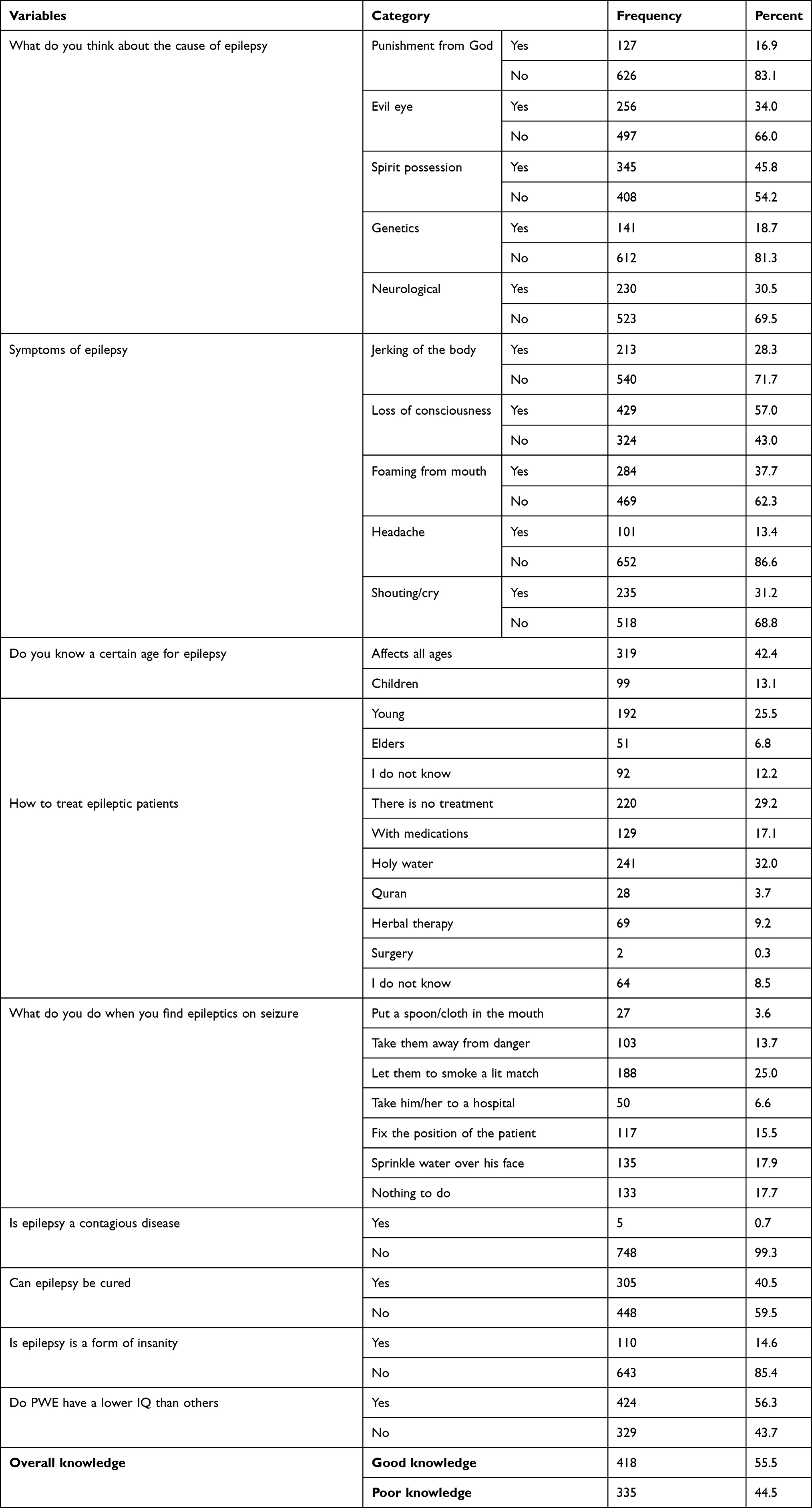 |
Table 3 Knowledge About Epilepsy of the Study Participants (n=753) in South Achefer District, Northwest Ethiopia, 2020 |
From the qualitative study majority of the FGD participants argued on the cause and treatment of epilepsy traditionally.
A 41 years old male participant from the urban FGD said about the causes of epilepsy as;
I do not know the real cause Scientifically, but from my perspective, epilepsy is caused by evil or bad spirits. It occurs when the rule of God is broken by someone. Then, by demonstrating this person’s illness, God wants to teach others. Like when God wants to treat you. People in this community believe that the cause is because of God’s punishment.
A 40 years old male HDA leader from the KII said;
In many ways, People in our community think about the causes of epilepsy. Some people believe that epilepsy happens at mid-day when someone moves alone in the forest and around the river, and others say during a mother delivers her baby. Culturally, when a mother gives birth in our society, she should not be left alone. When a mother is left alone before the 10th day following childbirth, epilepsy occurs. Others also believe demons possession and witchcraft to be the causes of epilepsy.
Another 44 years old female HAD leader from the KII also said;
Epilepsy is a disease that is transmitted through inheritance. In our village, for instance, I know two people in one family with epilepsy. Because of this, people think heredity is the cause of epilepsy.
Most FGD participants explained traditional and religious healings as the better option rather than biomedical treatment with respect to the treatment of epilepsy. They believe that contemporary medicine epilepsy does not treat epilepsy.
A 28 years old participant from the male FGD said;
The therapy depends on the cause of epilepsy. If the cause is by the evil eye and through demons, the patient takes to a health facility and also an injection is given., it is calls “adfin new” a local phrase. This means it guarantees that the illness never recovers after he/she takes the injection. He is going to die, maybe. Thus, instead of sending them to hospital, we assume that holy water is the only option.
Another male participant from the urban FGD also said;
From a religious point of view, the treatment varies in each religion. Muslims, Protestants, orthodox Christianity, and others have their own way of treating epilepsy. The best treatment for epilepsy in orthodox Christianity is holy water. They did not get relief from their illness with biomedical treatment. That is why people in our community have not preferred to treat epilepsy with modern medicine. I didn’t hear Until now that someone was being treated with medicine. But I have seen those who have been cured from their disease by holy water and traditional medicine.
A 32 years old from male FGD explained about modern medicine as
… … it depends on the community. Some people choose traditional healers while others go to holy water. But it is better for me to go to health facilities to get the appropriate treatment.
A 51 year’s old male orthodox religious leader from the KII said:
In our community, those who believe with God want to treat people with epilepsy in religious healings like holy water. Especially those with symptom of mouth foaming. They take them to the hospital If they have other symptoms. By taking them to magicians and traditional healers, some people waste their money without any improvement.
A 28 years old female health extension worker from the KII also said;
Most of the people take people with epilepsy to holy water. Since they believe it is caused by spirit possession, they did not prefer to take these individuals to the hospital. Culturally, they think that the patients may die when we take these individuals to the hospital and if they get any injection. So, they are afraid to take them to health facility.
About Intervention methods that they do if they encounter epileptic patients most of the participants explained as smelling the smoke of ignited a match as the first-line intervention for seizure.
A 29 years old male FGD participant said;
The issue in our culture is that we did not want to offer any intervention to a person who was not familiar. But my question is, what is the problem with helping these individuals we don’t know about? If I help someone because of I know him or her. I fail to help if I do not know. This is not expected from a person. There is something that has happened to these guys, whether I know him or not. So, I do what is required of me to do.
A 26 years old male FGD participant said;
First I ignited a match and made the patient smell the smoke afterwards if there was no improvement. I am going to take him to the closest health facility. Again, if there is no improvement, I take him to the holy water.
A 44 years old female participant from the KII also said;
This relies on one’s character. Some individuals ignited a match and made the patient smell the smoke while others may place the patient in a position which avoid harm to him. Some individuals do not want people with epilepsy to be touched. Since they are worried that the disease will transmit to us.
Attitude of the Community Towards Epilepsy
The favorable attitude of the community toward epilepsy patients was found 60.8% (95% CI: 57.2–64.3). Among study participants, only 75 (10.0%), 36 (4.8%), and 71 (9.4%) reported that they strongly agree to have close relation with epileptics, to live together and to work with them, respectively. Nearly one-third (30.5%) agree to shake hands with epileptics. A very small number of participants 2.8% and 3.2% would be willing to marry a patient with epilepsy and agree to recruit epileptics as servants, respectively (Table 4).
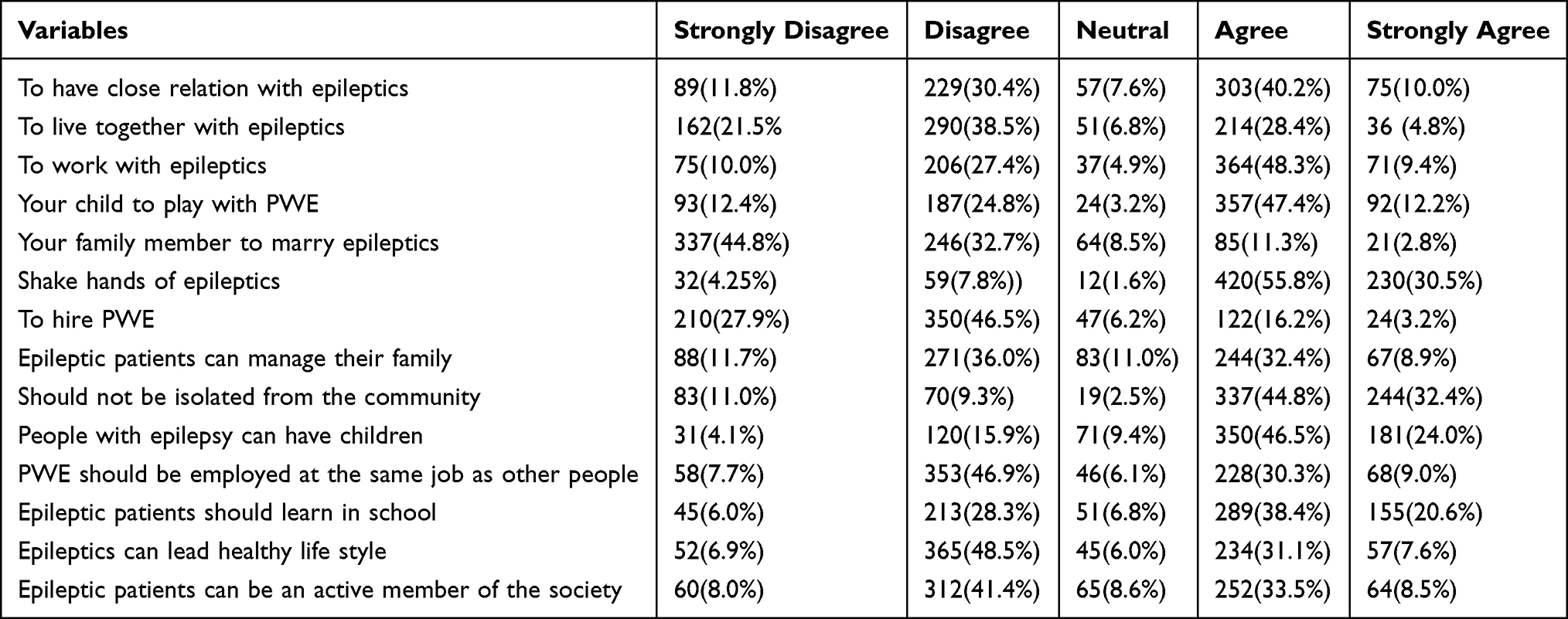 |
Table 4 Attitude of the Community Towards Epilepsy in South Achefer District, Northwest Ethiopia, 2020 |
Concerning marriage majority of the FGD participants described that they did not want to marry epileptic patients. But if it occurs after marriage, they can live together.
A 25 years old male FGD participant said;
In our community, people with epilepsy and healthy people don’t marry each other. In case if they unknowingly marry epileptic patients, they immediately decide to divorce. But if it occurs after marriage and they bear a child, they live together to grow their child. The same is true for me. I pray to God to help me from this type of event in the future. If it happens after I marry her and we have children, I will try to treat her and I will live together until she dies. But if we do not have kids, I will send her to her families. Because I want to have children. God creates human beings to replicate himself or herself on the earth.
Another female participant from FGD, 31 years old, also said:
I didn’t want to marry him If I knew he had epilepsy. Because I have the opportunity to find another person who is healthy. But if it happens after I married him, I will try to help him with everything.
A 51 year’s old Muslim male KII said:
In our community, when a person first wants to marry, he or she asks every information about that family from another person. No one agree to marries a person with epilepsy. It is written in Quran In the Muslim religion, as those who are Healthy must marry a healthy person and those who have a disease can marry a person with a disease. It doesn’t allow us to marry person who are healthy and person who have epilepsy. But they try to tolerate each other if it happens after marriage.
A 27 years old male patient with epilepsy also explained as:
There is a negative attitude towards this disease. People think that epilepsy is more severe than HIV. But it is very simple. It is not transmitted as HIV. But people want their children to marry people with HIV rather than those having epilepsy. They understand in this way. For example, I got married and divorced because of this.
Misunderstandings and/or misconceptions about this health issue should affect one’s attitude towards epilepsy. This finding was supplemented by a qualitative study. A 54 years old orthodox religious leader from the KII said;
Those People who do not have enough knowledge about the disease think people with epilepsy as mentally ill. They also insult them by saying mania. Especially in rural areas when they see these people, they say ‘close your door a crazy man coming’. Because there is a great lack of knowledge about epilepsy in our community. They have a negative attitude towards the disease.
A 27 years old epileptic patient also said that;
People who have poor knowledge about epilepsy have a negative attitude towards people with epilepsy. They think this disease comes due to a sinful act of that person and from punishment from God. So, they didn’t want to give any intervention during the seizure. Because they fear the disease may transfer to me if I touch him.
This finding was supplemented by a qualitative study. A 27 years old epileptic patient said that;
My close friends have a good attitude for me as well as for the disease. Because during seizure they saw everything about the disease from me. But those who didn’t know me don’t understand like them, they think the disease is very serious.
A 44 years old female participant from the KII also said that;
Someone who has epilepsy in the family and those who have close relatives with this disease has a good attitude about the disease. But people who have never seen this disease do not want to help these people during a seizure. Because they afraid that the disease will transmit to me.
Factors Associated with a Favorable Attitude Towards Epilepsy
After Bivariate logistic regression analysis had done variables: respondent’s age, sex, family role, marital status, educational status, residence, occupation, being informed about epilepsy, witnessing seizure, having a family member with epilepsy, having a friend with epilepsy and the distance of their home from a health institution had been met the requirement to proceed to multivariable logistic regression analysis. The Multivariate analysis showed being informed about epilepsy, witnessing seizure, and knowledge about epilepsy had a statistically significant association with an attitude towards epilepsy.
Those who had heard information about epilepsy were found to increase the odds of favorable attitude by 1.47 times as compared with those who had not heard information about epilepsy (AOR=1.47; 95% CI, 1.02–2.11). Whereas the odds of favorable attitude towards epilepsy were higher by 1.6 times in respondents who had witnessed seizure compared to those who did not witness seizure in the past (AOR=1.6; 95% CI, 1.14–2.27). Having good knowledge about epilepsy increases the odds of a favorable attitude by 2.08 times as compared to those who have poor knowledge about epilepsy (AOR=2.08; CI, 1.49–2.89) (Table 5).
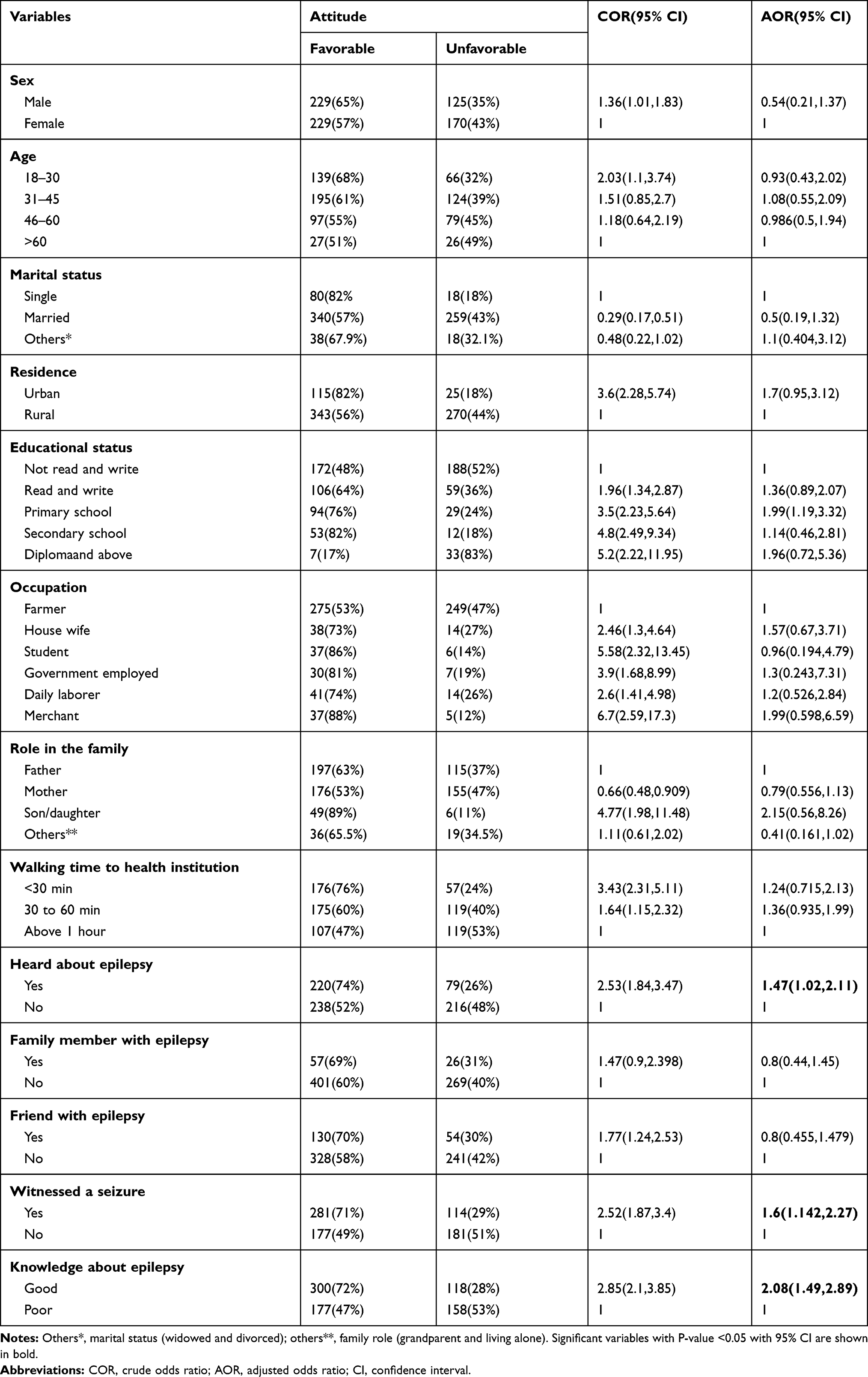 |
Table 5 Bivariable and Multivariable Logistic Regression Table Showing the Factors Associated with Attitude of the Community Related to Epilepsy (n=753) in South Achefer District, Northwest Ethiopia, 2020 |
Discussion
The result of this study indicated that about, 60.8% of the participants had a favorable attitude towards PWE, which is in line with a study conducted in Debre Berhan town (59.7%).21 The possible explanation of this similarity both study has done in a population with major of dweller from Amhara ethnicity, they share a more or less similar culture, believe how disease occurs and attitude. However, it is higher than the study conducted in Ethiopia, Oromia region (35.6%), and the south region of Ethiopia in Menit communities (13.2%).17,23 This difference could be due to a difference in culture and methodological differences as well as through time measurements taken by the government of Ethiopia yield result, also Our study consists of both urban and rural dwellers. Our result is higher than the study conducted in Egypt (8%). This inconsistency can be due to differences in the period and socio-demographic characteristics of the respondents. Participants in Egypt were only secondary school students with an age range from 15 to 18 years.24 In addition to those reasons, our attitude question item also had an extra question like shake hands of epilepsy and recruit epilepsy patients as servant.
However, this finding is lower than a study done in Ethiopia, East Gojjam (65.7%).20 This inconsistency could be due to differences in socio-demographic status, the majority of participants in our study are illiterate and live in rural areas. Our result is also lower than studies conducted in Jimma (70%) and Iran (87.9%).25,26 This is due to that both studies are facility-based. A study conducted in Jimma was among patients with epilepsy on follow-up at epilepsy clinic and participants in Iran were among close family members of people with epilepsy. A student conducted in Trinidad and Tobago (93%)14 had a positive attitude towards PWE Which was higher than our finding. This could be explained their study participants were college students, which may help them to have a good understanding of the disease epilepsy and PWE. In addition, their sample size was nearly half what we have.
Having good knowledge about epilepsy increases the odds of a favorable attitude by 2.18 times as compared to those who have poor knowledge about epilepsy. Similarly, a study conducted in Egypt, Turkey, Nigeria, and a systematic review from Malaysia showed that attitude towards epilepsy was influenced by knowledge about the disease.24,27–29 A better understanding of the disease among the public would allay fears and lessen stigmatization about epileptics in the community.
Those who had heard information about epilepsy were found to increase the odds of favorable attitude by 1.53 times as compared with those who had not heard. This is in line with the study done in Ethiopia, in Sululta and Debre Berhan town.21,23 Hearing the term epilepsy may invite individuals to ask or read more about epilepsy leading them to get accurate information about the disease. This may avoid miss conceptions rising from the community about epilepsy.
The odds of a favorable attitude towards epilepsy were higher by 1.59 times in respondents who had witnessed seizure compared to those who did not witness seizure in the past. This finding is in line with studies done in Debre Berhan town, Thailand, and the general public of Cameroon.21,30–32 Those who know someone with epilepsy have witnessed an epileptic event. This may lead to having more understanding and fewer misconceptions about epilepsy.
This study has an implication for researcher and policymakers. For researchers, the impact of the negative attitude of the community towards PWE on their treatment outcome, the level of marginalization on social events such as marriage and the chance to get work may need to be investigated. The Community’s unfavorable attitude towards PWEs has an impact on their mental health, so clinicians should give dual attention to the issue during their clinical follow-up time. The study had policy implications by stating that strategies should be developed to reduce misconception about the community regarding PWE.
Limitation of the Study
Since attitude was determined by the patients’ self-reports, social desirability bias might be there which could affect the magnitude of favorable attitude.
Conclusion and Recommendation
Based on the findings of this study two-third of participants had a favorable attitude towards epilepsy patients. Factors such as having good knowledge about epilepsy, being informed about epilepsy, and witnessing seizures were found to be significantly associated with a favorable attitude. Therefore, health professional and health extension workers should provide a larger and comprehensive community-based health education to enhance people's knowledge about epilepsy. This helps to bring attitude change against a negative attitude towards PWE. Mass media also play its role to inform the large community about epilepsy.
Data Sharing Statement
The datasets used and analyzed during this study are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
Ethical clearance was obtained from the ethical committee of the institute of public health, college of medicine and health science, University of Gondar by Ref No/IPH/837/6/2020. A support letter was obtained from the South Achefer District administration office. Data was collected after informed the study participants about the objectives and purpose of the study. Their anatomized response will be published. They also informed that they have the right to withdraw from the study at any time with no further explanation. We received verbal informed consent from each study participant who were willing to participate in the study and for tape recording (in the qualitative study). The verbal informed consent was approved by the ethics committee of the institute of public health, college of medicine and health science, University of Gondar. The verbal informed consent also included the publication of anonymized responses of the study participants. The collected data were kept in secret and was not be disclosed to anyone except the investigator. This study protocol was conducted in accordance with the World Medical Association (WMA) Declaration of Helsinki.
Acknowledgments
We would like to thank the data collectors and supervisors for their commitments; the respondents for being cooperative during the data collection period.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
No fund was obtained for this study.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Ezeala-Adikaibe BA, Achor JU, Nwabueze AC, et al. Knowledge, attitude and practice of epilepsy among community residents in Enugu, South East Nigeria. Seizure. 2014;23(10):882–888. doi:10.1016/j.seizure.2014.08.003
2. Shafiq M, Tanwir M, Tariq A, et al. Epilepsy: public knowledge and attitude in a slum area of Karachi, Pakistan. Seizure. 2007;16(4):330–337. doi:10.1016/j.seizure.2007.02.002
3. Wagner RG, Ngugi AK, Twine R, et al. Prevalence and risk factors for active convulsive epilepsy in rural northeast South Africa. Epilepsy Res. 2014;108(4):782–791. doi:10.1016/j.eplepsyres.2014.01.004
4. Ngugi AK, Bottomley C, Kleinschmidt I, et al. Prevalence of active convulsive epilepsy in sub-Saharan Africa and associated risk factors: cross-sectional and case-control studies. Lancet Neurol. 2013;12(3):253–263. doi:10.1016/S1474-4422(13)70003-6
5. Paul A, Adeloye D, George-Carey R, Kolcic I, Grant L, Chan KY. An estimate of the prevalence of epilepsy in Sub-Saharan Africa: a systematic analysis. J Glob Health. 2012;2(2):020405. doi:10.7189/jogh.02.020405
6. Fiest KM, Sauro KM, Wiebe S, et al. Prevalence and incidence of epilepsy: a systematic review and meta-analysis of international studies. Neurology. 2017;88(3):296–303. doi:10.1212/WNL.0000000000003509
7. Cobb S. Causes of epilepsy. Arch Neurol Psychiatry. 1932;27(5):1245–1263. doi:10.1001/archneurpsyc.1932.02230170261009
8. Surges R, Sperling MR, DeGiorgio CM. Editorial: sudden unexpected death in epilepsy: bio-markers, mechanisms, risk identification and prevention. Front Neurol. 2019;10:1277.
9. Millogo A, Ngowi AH, Carabin H, Ganaba R, Da A, Preux PM. Knowledge, attitudes, and practices related to epilepsy in rural Burkina Faso. Epilepsy Behav. 2019;95:70–74.
10. Gzirishvili N, Kasradze S, Lomidze G, et al. Knowledge, attitudes, and stigma towards epilepsy in different walks of life: a study in Georgia. Epilepsy Behav. 2013;27(2):315–318. doi:10.1016/j.yebeh.2013.02.011
11. Fong CY, Hung A. Public awareness, attitude, and understanding of epilepsy in Hong Kong Special Administrative Region, China. Epilepsia. 2002;43(3):311–316. doi:10.1046/j.1528-1157.2002.31901.x
12. Abubakar A, Kariuki SM, Tumaini JD, et al. Community perceptions of developmental and behavioral problems experienced by children living with epilepsy on the Kenyan coast: a qualitative study. Epilepsy Behav. 2015;45:74–78. doi:10.1016/j.yebeh.2015.02.023
13. Quereshi C, Standing HC, Swai A, Hunter E, Walker R, Owens S. Barriers to access to education for young people with epilepsy in Northern Tanzania: a qualitative interview and focus group study involving teachers, parents and young people with epilepsy. Epilepsy Behav. 2017;72:145–149. doi:10.1016/j.yebeh.2017.04.005
14. Youssef FF, Dial S, Jaggernauth N, et al. Knowledge of, attitudes toward, and perceptions of epilepsy among college students in Trinidad and Tobago. Epilepsy Behav. 2009;15(2):160–165. doi:10.1016/j.yebeh.2009.01.027
15. Panda SB, Prabhu K, Rao S, et al. Evaluation of knowledge of and attitudes toward epilepsy among the health science students of Manipal University. Epilepsy Behav. 2011;20(3):447–449. doi:10.1016/j.yebeh.2010.12.024
16. Tuan NA, Cuong LQ, Allebeck P, Chuc NTK, Tomson T. Knowledge attitudes and practice toward epilepsy among adults in BaVi, Vietnam: first report from the population‐based EPIBAVI study. Epilepsia. 2007;48(10):1914–1919. doi:10.1111/j.1528-1167.2007.01174.x
17. Henok A, Lamaro T. Knowledge about and attitude towards epilepsy among menit community, Southwest Ethiopia. Ethiop J Health Sci. 2017;27(1):47–58. doi:10.4314/ejhs.v27i1.7
18. Bifftu BB, Dachew BA, Tiruneh BT. Perceived stigma and associated factors among people with epilepsy at Gondar University Hospital, Northwest Ethiopia: a cross-sectional institution based study. Afr Health Sci. 2015;15(4):1211–1219. doi:10.4314/ahs.v15i4.21
19. Berhe R, Nigusie A. Perceptions of home delivery risk and associated factors among pregnant mothers in North Achefer District, Amhara Region of Ethiopia: the health belief model perspective. Fam Med Med Sci Res. 2019;8:238.
20. Zeleke H, Gualu T, Sharew Y, Alem G. Knowledge, practice and attitude towards epilepsy and associated factors among adults in Goncha Siso Enesie Woreda Rural Kebeles, East Gojjam, Ethiopia 2016. Epilepsy J. 2018;4(1000126):2472–0895.1000126. doi:10.4172/2472-0895.1000126
21. Dargie A, Alemnew N, Admasu E. Public knowledge and attitude towards epilepsy and its associated factors in Debre Berhan, North Shoa, Amhara Region, Ethiopia, 2018/19. Community based cross sectional study. medRxiv. 2019;19001578.
22. Al-Dossari KK, Al-Ghamdi S, Al-Zahrani J, et al. Public knowledge awareness and attitudes toward epilepsy in Al-Kharj Governorate Saudi Arabia. J Family Med Prim Care. 2018;7(1):184–190. doi:10.4103/jfmpc.jfmpc_281_17
23. Teferi J, Shewangizaw Z. Assessment of knowledge, attitude, and practice related to epilepsy: a community-based study. Neuropsychiatr Dis Treat. 2015;11:1239–1246. doi:10.2147/NDT.S82328
24. Shehata GA, Mahran DG. Knowledge and attitude of epilepsy among secondary schools students (epileptic and non-epileptic) in Assiut city Egypt. Epilepsy Res. 2011;95(1–2):130–135. doi:10.1016/j.eplepsyres.2011.03.011
25. Kassie GM, Kebede TM, Duguma BK. Knowledge, attitude, and practice of epileptic patients towards their illness and treatment in Jimma University specialized hospital, Southwest Ethiopia. N Am J Med Sci. 2014;6(8):383. doi:10.4103/1947-2714.139288
26. Karimi N, Akbarian SA. Knowledge and attitude toward epilepsy of close family members of people with epilepsy in north of Iran. Adv Med. 2016;2016. doi:10.1155/2016/8672853
27. Lim KS, Lim CH, Tan CT. Attitudes toward epilepsy, a systematic review. Neurol Asia. 2011;16:4.
28. Ojinnaka NC. Teachers’ perception of epilepsy in Nigeria: a community-based study. Seizure. 2002;11(6):386–391. doi:10.1053/seiz.2001.0664
29. Macit C, Clark PM, Taner N, Bingol C, Mercanoglu G, Yuksel G. A survey on awareness, knowledge, and attitudes toward epilepsy in an urban community in Turkey. Niger J Clin Pract. 2018;21(8):979–987. doi:10.4103/njcp.njcp_199_17
30. Saengpattrachai M, Srinualta D, Lorlertratna N, Pradermduzzadeeporn E, Poonpol F. Public familiarity with, knowledge of, and predictors of negative attitudes toward epilepsy in Thailand. Epilepsy Behav. 2010;17(4):497–505. doi:10.1016/j.yebeh.2010.01.164
31. Njamnshi AK, Tabah EN, Bissek A-CZ-K, et al. Knowledge, attitudes and practice with respect to epilepsy among secondary school students in the Kumbo West Health District-North West Region-Cameroon. Epilepsy Behav. 2010;18(3):247–253. doi:10.1016/j.yebeh.2010.03.013
32. Dorota T, Witkowska M, Michalak M. Attitudes of employees of service and trading companies towards people with epilepsy and their professional activity in Poland. Seizure. 2014;23(3):178–183. doi:10.1016/j.seizure.2013.11.008
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.