")
Back to Journals » Patient Preference and Adherence » Volume 11
Coming full circle in the measurement of medication adherence: opportunities and implications for health care
Authors Whalley Buono E, Vrijens B, Bosworth HB , Liu LZ, Zullig LL, Granger BB
Received 9 November 2016
Accepted for publication 3 February 2017
Published 2 June 2017 Volume 2017:11 Pages 1009—1017
DOI https://doi.org/10.2147/PPA.S127131
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Elizabeth Whalley Buono,1 Bernard Vrijens,2 Hayden B Bosworth,3 Larry Z Liu,4 Leah L Zullig,5,6 Bradi B Granger7,8
1VP, Global Quality, External and Regulatory Affairs, MWV Healthcare, Richmond, VA, USA; 2WestRock Healthcare, Visé, Belgium; 3Division of General Internal Medicine, Department of Medicine, Duke University School of Medicine, Durham, NC, 4Center for Observational and Real World Evidence, Merck, Rahway, NJ and Weill Medical College of Cornell University, New York, NY, 5Division of General Internal Medicine, Duke University School of Medicine, 6Center for Health Services Research in Primary Care, Durham Veterans Affairs Health Care System, 7Duke University School of Nursing, 8Heart Center Nursing Research Program, Duke University Health System, Durham, NC, USA
Abstract: There is little debate that medication nonadherence is a major public health issue and that measuring nonadherence is a crucial step toward improving it. Moreover, while measuring adherence is becoming both more feasible and more common in the era of electronic information, the reliability and usefulness of various measurements of adherence have not been well established. This paper outlines the most commonly used measures of adherence and discusses the advantages and disadvantages of each that depend on the purpose for which the measure will be used. International consensus statements on definitions and guidelines for selection and use of medication adherence measures were reviewed. The quality of recommended measures was evaluated in selected publications from 2009 to 2014. The most robust medication adherence measures are often ill suited for large-scale use. Less robust measures were found to be commonly misapplied and subsequently misinterpreted in population-level analyses. Adherence assessment and measurement were rarely integrated into standard patient care practice patterns. Successful scalable and impactful strategies to improve medication adherence will depend on understanding how to efficiently and effectively measure adherence.
Keywords: adherence measures, medication adherence, study design, patient-reported outcomes, research methods
Introduction
Poor medication adherence is a burgeoning public health issue, the management of which is limited by our inability to accurately measure it. Though measuring adherence is becoming more feasible and more common in the era of electronic information, the selection of the most appropriate measure remains largely a matter of convenience and ease of data access. Similar to the convenience sampling, convenience-based measurement introduces bias and data quality error that pose a risk for interpretation and threaten the apt use of findings for policy and practice.
In this era of big data, we have become both enabled and obsessed with measurement and analytics in the context of medication use. From prescription order to fill date, pick-up, and refill, we measure frequency, accuracy, omissions, and errors. We forget, however, that “how” and “when” we measure is as important as “what” we measure. In the business of health care, decisions informed by incomplete or inaccurate measurement pose risk far beyond unprofitability. Arguably, in no other sector is the need for appropriate measurement so crucial as it is in health care – and the cost of inaccuracy so potentially injurious.1 And yet, many of the practices and standard metrics for medication adherence implemented at the bedside or at the pharmacy counter have been developed to address the economics of health care, and often by stakeholders who lack a sophisticated understanding of the medication counseling experience, the patient experience, or the intricacies of clinical data. Furthermore, existing published research does not yet provide a basis for the formulation of clear use case guidelines. Accordingly, all one can currently do is to better understand the purpose and utility of each measurement type and select a metric that most closely aligns with the desired outcome.
The metrics for medication adherence, flagged as a major cost driver,2–4 and a focus of reform,5,6 have become the focus of a frenzy of activity associated with understanding and affecting medication-related health care spending in the US. This is understandable, given the proportion of gross domestic product spent on health care, increasing from 4.4% in 1950 to 17.9% in 2012.7,8 Yet, the enormity of the issue of medication nonadherence extends well beyond the immediate health care market, with overall medication-related losses to the US economy estimated at $317 billion.9 With the advent of health care reform, medication nonadherence quickly emerges as a front running opportunity for improvement. The opportunity, however, is complex – with the need to evaluate and compare large-scale health systems and profit centers juxtaposed against the need to improve patient-level medication-taking behavior. This commentary outlines current measures of adherence, discusses advantages and disadvantages of various approaches, and provides clear examples of well-suited uses relative to the practices of pharmacists, clinicians, payers, and researchers. In addition, limitations in current measures of medication adherence and persistence are highlighted to increase awareness and to improve the accuracy of appropriate selection of adherence metrics according to research design and study purpose. Ultimately, successful strategies to improve medication adherence on a large scale will depend on improving the efficiency and effectiveness of adherence measures that benefit patients, practitioners, payers, and policy makers. Given the import, further research is needed to establish and validate clear use cases for the myriad of measurement metrics available.
Measurement challenges
The push to improve medication adherence has resulted in a surfeit of data generated by pharmacy claims that, when used haphazardly, is neither quantitatively or qualitatively advantageous. For example, claims data can effectively be harnessed to evaluate efficiency in dispensing systems, gauge improvement in productivity and refill trends and identify “best practices” across plans, physicians, and pharmacists – but this type of measurement has limitations when used for medication therapy management (MTM) and selection of patient-level interventions. The limitation for use of claims data in practice is the wide range of data discrepancy and the variations in precursors to poor adherence. In fact, appropriate patient-level interventions are often dependent upon changes in social support or daily routines in the home; factors that are not components of calculated medication possession ratio (MPR) or other usual adherence calculations in claims-based data.10,11
Similar challenges exist in the context of clinical treatment. For example, direct measures used in controlled research may have limited usefulness for practice, where the pressures of time constraints and limited resources may render the choice of direct measurement, such as pill counts, unreasonable. Likewise, accurate pharmacokinetic measures (such as International Normalized Ratio measures for warfarin effect) are available for only a few medications and where available, associated measurement techniques may be too intrusive and costly to administer. Finally, while dispensing records, bioavailability markers, and pill counts may assist with building a picture of each patient’s adherence over time, they will not ultimately yield the type of data necessary to assess adherence at a specific point in time and may not be useful for continuous routine monitoring – data that pharmacists and clinicians often rely upon in their day-to-day practice. Accordingly, those who measure adherence – or evaluate existing research results for decision-making purposes – must pay particular attention to both the value and limitations of the array of measurement metrics available.
Matching the hammer to the nail – purposeful measurement
In the absence of a “gold standard” of adherence measurement, the choice of metric must take into account the purpose of each individual assessment. This decision must consider the potential usefulness and reliability of the data in light of the user and recognize that some methods are appropriate only for certain situations. For example, if the user is a payer, researcher, physician, or pharmacist, the metric selected must reliably measure the goals of that user (e.g., reimbursement, comparisons of effectiveness, clinical treatment, or medication counseling, respectively).
The existing body of literature provides little guidance on how best to match measurement metrics with appropriate use. Rigorous research and in-depth review has been identified as a critical limiting factor to the development of much needed adherence-informed tools for health care professionals.12,13 Relevant published literature broadly assigns methods for measuring adherence into two categories, direct and indirect, based upon mode of observation employed by each. To begin to distinguish relative value among many measures, Table 1 describes both direct and indirect measures and denotes advantages for each. Optimal metric selection depends on the type of adherence being assessed, the precision required, and the intended use of the results.14 For example, while measurement of medication adherence rates at the population level through consistent use of calculations based on pharmacy claims data has value, population-based measures provide minimal information about the individual. Appreciation of the strengths and limitations of each measure may prevent negative consequences, both at the patient level, such as over-prescribing in resistant hypertension,15 and the policy level, such as imprecise empirical justification of payment bundling.16
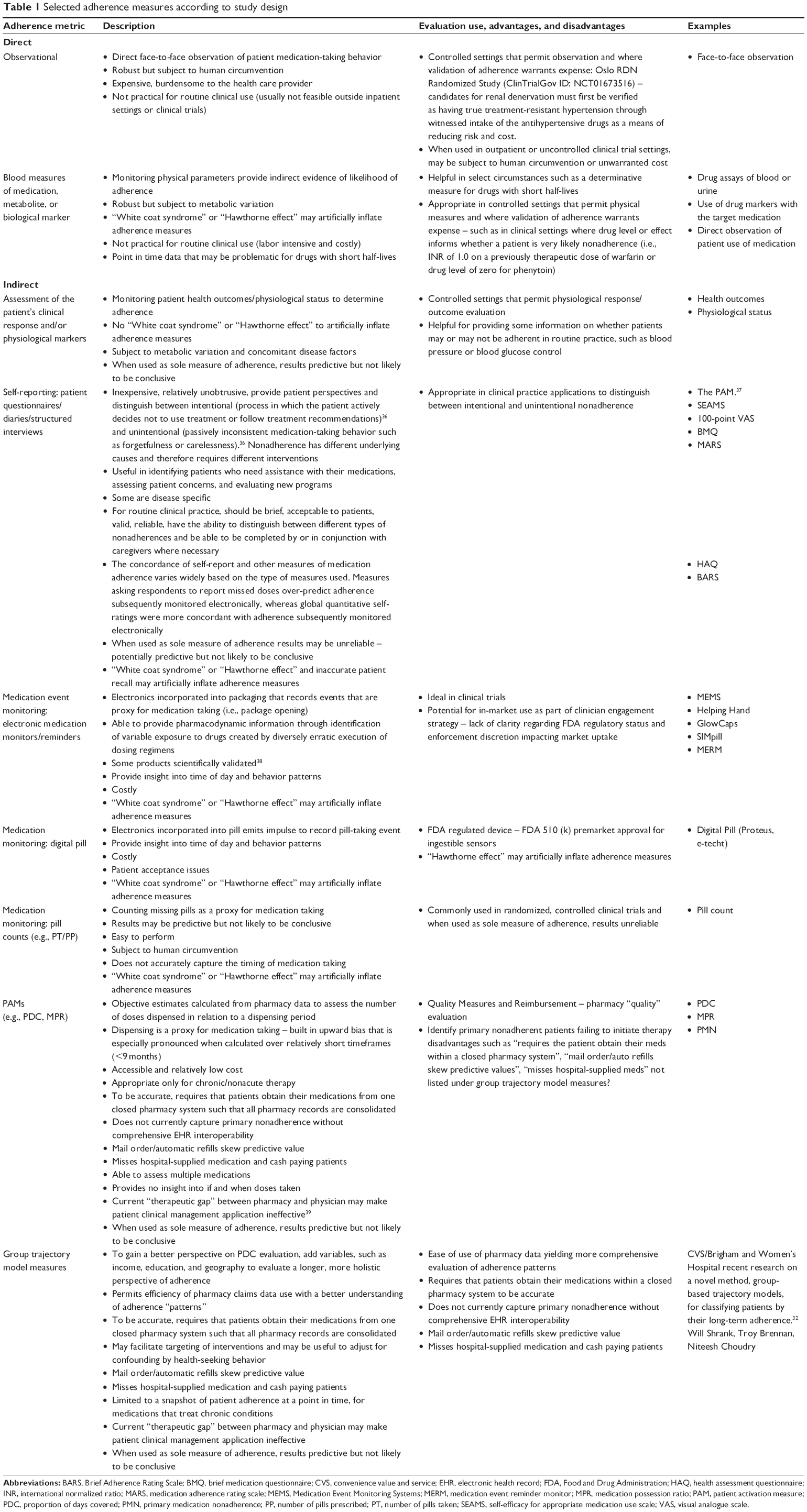 | Table 1 Selected adherence measures according to study design |
“Robust” measures are characterized as measures that have the potential to yield the type and amount of data necessary for understanding comprehensive patterns of daily adherence. For this purpose, the best measures may include direct or indirect assessment of the patient’s medication-taking behavior, clinical response to therapy, and/or related physiological markers, such as the concentrations of drug or metabolite in blood or urine, or detection or measurement in blood of a biologic marker added to the drug formulation. As valuable as these measures can be in clinical practice, they can often be predictive but not conclusive. Complicating factors can give a false impression of real-life adherence behavior. For example, unobserved and unmeasured individual traits may be related to both the explanatory variable and the outcome being examined. This problem, known as “endogeneity,”17 is found to obscure and confound the relationship between medication adherence, health services utilization measures such as readmission rates, and cost.
Of all robust measures, face-to-face observation of medication taking, or direct observation therapy, provides the most accurate point in time evaluation data and can facilitate even richer insight through provider–patient engagement. However, the limitations to the utility of this method are obvious – and the realistic value of this measure outside of an inpatient or research setting is limited to the family caregiver. Other direct methods, such as measurement of drug or metabolite levels in blood or urine, or detection of blood-levels of biological markers added to the drug formulation, prove drug ingestion and are thus very reliable estimates of medication adherence. They are, however, less robust in that they are subject to bias from variations in metabolism and “white coat adherence,” and can give a false impression of real-life adherence behavior.18 In addition, they are expensive and complex to administer, are not available for the majority of medications, and on a population basis, they may not be scalable or feasible.19 Accordingly, these direct measures of adherence are largely reserved for the clinical trial setting or situations such as tuberculosis or HIV, where exigent circumstances justify the means.
Measures that use an identified proxy event (such as package opening) to evaluate medication-taking behavior can also be robust when the proxy event is closely related to the ingestion or application of the medication. Technological advances in indirect adherence measurement including digital pills, technology-equipped packaging, and Medication Event Monitoring Systems (MEMS) use proxy events ranging from package opening to actual pill ingestion to measure and analyze medication-taking behavior. Automatic compilation of drug dosing history data facilitated by smart technology allows reliable and detailed assessment of adherence behavior over time. These products have been successfully validated to show that the clinical explanatory and predictive value of the resulting adherence data is significant.20 Accordingly, the US Food and Drug Administration recommended use of smart technology for drug development as a feedback mechanism to enhance patient adherence in clinical trials.21 Although these technologies provide richly sampled dosing history data that are critical for pharmacometric interpretation, technology-informed data alone are insufficient for patient care purposes.
Measures that use an identified proxy event remote from the actual medication-taking event produce less robust data. For example, calendared blister packaging has been proven to improve pharmacy claims-based adherence and persistence rates but these results tell little about individual pill-taking behavior.22 Unfortunately, convenience appears to be inversely correlated with insight into causes of nonadherence. In general, this further removed the proxy event from the ingestion or application of the medication, the less expensive and easier the method is to administer, yet the less valuable the data.
Simple indirect measurement techniques, such as self-reporting, structured interviews, and pill counts, are all subject to bias from a broad array of both provider and patient variables (e.g., recall, ineffective administration, and desirability bias). For example, the Patient Activation Measures23 and other self-report scales rely on direct assessment and results can be unpredictable due to human variability.24 As observed in their use with MTM, the quality of the data obtained is highly dependent upon the practitioner–patient relationship.25 The concordance of these types of measures with actual adherence behavior varies widely based on the skill of the practitioner.26–28 Furthermore, data capture, collection, and use challenges exist, making these measures more complicated to effectively integrate into electronic health records, automated data capture systems, and clinical practice workflows.29
Claims data derived from pharmaceutical distribution represent another example of indirect data capture. The Pharmacy Quality Alliance developed, tested, and endorsed the most widely and currently referenced set of adherence metrics, the Pharmacy Adherence Measures, which include Proportion of Days Covered and MPR.30 Focused on prescription filling dates and days of therapy supplied for each fill of a prescription, these adherence measures use the event of “a filled prescription leaves the pharmacy” as a proxy for medication taking. The measures are used predominantly as performance measures for health plans, pharmacy benefit managers and managed care organizations for which claims data are relatively accessible and inexpensive. In addition, because of their ease of use and scalability, these measures have become a mainstay in both the evaluation of personalized adherence interventions and the design of adherence programs in various settings. Although studies confirm that these type of data reliably indicate drug exposure and associated clinical effect, they can be used primarily to study chronic, not acute, treatments21 and do not provide the type of granularity necessary to understand causal factors once a nonadherent population is identified. Furthermore, adherence calculated through claims data is less reliable for nonoral medication types including injectable, transdermal, and inhaler dosage forms where the amount of medication associated with a single dose is less easy to quantify and for medications that require frequent titration and dose adjustment such as oral anticoagulants.19
The Pharmacy Quality Alliance’s most popular claims-based measure, the Primary Medication Non-Adherence measure, recently endorsed by the Centers for Medicare and Medicaid Services, attempts to refine the purpose for which claims analysis is undertaken.31 By refocusing from general nonadherence to noninitiation, this metric permits greater insight into patient medication-taking behavior and theoretically narrows the scope of choice of intervention to those geared toward addressing noninitiation. However, the measure alone renders insufficient data upon which to base comprehensive intervention design decisions. Other promising new methods of adherence measurement attempt to serve the same end by subjecting pharmacy claims data to group-based trajectory modeling.32 These measures show potential to help health care professionals appropriately target interventions and evaluate associated clinical outcomes. They allow researchers to move beyond over-simplified classification of patients as “adherent or not” and more accurately capture and describe adherence.32
For medication adherence measures to effectively inform decision making about supportive interventions at the individual patient level, the intervention selection, delivery and intensity must be matched with each patient’s needs.33 Without insight into those needs, decisions will necessarily be uninformed. Using well-selected, robust measures will yield comprehensive insight into behavior patterns, allowing pharmacists and providers to elicit patient feedback and address the root cause of individual nonadherence.34,35
Implications
The need to understand patient medication nonadherence at the individual level becomes more critical as the cost and complexity of available interventions increases. As stakeholders in the health care market contemplate solutions for nonadherence, success at both the patient and population level will depend upon an educated understanding of adherence measures and interventions. Counting “possession” devoid of an exponent for rationale will cause enough error in the equation as to render it useless for driving change in the real world. Indeed, the era of big data offers much to measure. We have come full circle to recognize that metrics for measurement’s sake, without a conversation to interpret, integrate, and accommodate the importance of the constraints of everyday life on the individual, yield numbers of little value for prospective treatment choices. As patient-reported outcome measures gain momentum on the national stage, opportunities to use these measures more effectively may help close the gap on the social costs of our current inaccuracy.
Disclosure
Dr Zullig is supported by a VA Health Services Research and Development (HSR&D) Career Development Award (CDA 13–025). Dr Bosworth is supported by a Research Career Scientist Award from VA Health Service Research and Development (VA HSR&D 08–27). The authors report no other conflicts of interest in this work.
References
Kohn LT, Corrigan J, Donaldson MS. To err is human: building a safer health system. Washington, DC: National Academy Press; 2000. | ||
Cutler DM, Everett W. Thinking outside the pillbox – medication adherence as a priority for health care reform. N Engl J Med. 2010;362(17): 1553–1555. | ||
Maciejewski ML, Wansink D, Lindquist JH, Parker JC, Farley JF. Value-based insurance design program in north Carolina increased medication adherence but was not cost neutral. Health Aff (Millwood). 2014;33(2):300–308. | ||
Elliott DJ, Robinson EJ, Anthony KB, Stillman PL. Patient-centered outcomes of a value-based insurance design program for patients with diabetes. Popul Health Manag. 2013;16(2):99–106. | ||
Maciejewski ML, Farley JF, Parker J, Wansink D. Copayment reductions generate greater medication adherence in targeted patients. Health Aff (Millwood). 2010;29(11):2002–2008. | ||
Farley JF, Wansink D, Lindquist JH, Parker JC, Maciejewski ML. Medication adherence changes following value-based insurance design. Am J Manag Care. 2012;18(5):265–274. | ||
Chernew ME, Baicker K, Hsu J. The specter of financial Armageddon – health care and federal debt in the United States. N Engl J Med. 2010;362(13):1166–1168. | ||
WorldBank. The World Bank Healthcare Expenditures Data. 2014. | ||
Capgemini Consulting. Estimated annual pharmaceutical revenue loss due to medication non-adherence. Available from: http://www.capgemini.com/sites/default/files/resource/pdf/Estimated_Annual_Pharmaceutical_Revenue_Loss_Due_to_Medication_Non-Adherence.pdf. Accessed August 1, 2016. | ||
Moore JM, Shartle D, Faudskar L, Matlin OS, Brennan TA. Impact of a patient-centered pharmacy program and intervention in a high-risk group. J Manag Care Pharm. 2013;19(3):228–236. | ||
Wittayanukorn S, Westrick SC, Hansen RA, et al. Evaluation of medication therapy management services for patients with cardiovascular disease in a self-insured employer health plan. J Manag Care Pharm. 2013;19(5):385–395. | ||
Bosworth HB, Zullig LL, Mendys P, et al. Health information technology: meaningful use and next steps to improving electronic facilitation of medication adherence. JMIR Med Inform. 2016;4(1):e9. | ||
Zullig LL, Granger BB, Bosworth HB. A renewed medication adherence alliance call to action: harnessing momentum to address medication nonadherence in the United States. Patient Prefer Adherence. 2016;10:1189–1195. | ||
Cooper J, Hall L, Penland A, Krueger A, May J. Measuring medication adherence. Popul Health Manag. 2009;12(1):25–30. | ||
Baggarly SA, Kemp RJ, Wang X, Magoun AD. Factors associated with medication adherence and persistence of treatment for hypertension in a Medicaid population. Res Social Adm Pharm. 2014;10(6):e99–e112. | ||
Park H, Rascati KL, Lawson KA, Barner JC, Richards KM, Malone DC. Adherence and persistence to prescribed medication therapy among Medicare part D beneficiaries on dialysis: comparisons of benefit type and benefit phase. J Manag Care Pharm. 2014;20(8):862–876. | ||
Brookhart MA, Patrick AR, Dormuth C, et al. Adherence to lipid-lowering therapy and the use of preventive health services: an investigation of the healthy user effect. Am J Epidemiol. 2007;166(3):348–354. | ||
Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–497. | ||
Raebel MA, Schmittdiel J, Karter AJ, Konieczny JL, Steiner JF. Standardizing terminology and definitions of medication adherence and persistence in research employing electronic databases. Med Care. 2013;51(8 Suppl 3):S11–S21. | ||
Demonceau J, Ruppar T, Kristanto P, et al. Identification and assessment of adherence-enhancing interventions in studies assessing medication adherence through electronically compiled drug dosing histories: a systematic literature review and meta-analysis. Drugs. 2013;73(6): 545–562. | ||
FDA. Enrichment Strategies for clinical trials to support approval of human drugs and biological products. In: Industry Gf, editor. Available from: http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM332181.pdf%5D.2013. Accessed August 1, 2016. | ||
Zillich AJ, Jaynes HA, Snyder ME, et al. Evaluation of specialized medication packaging combined with medication therapy management: adherence, outcomes, and costs among Medicaid patients. Med Care. 2012;50(6):485–493. | ||
Hibbard JH, Mahoney ER, Stockard J, Tusler M. Development and testing of a short form of the patient activation measure. Health Serv Res. 2005;40(6 Pt 1):1918–1930. | ||
Skolasky RL, Green AF, Scharfstein D, Boult C, Reider L, Wegener ST. Psychometric properties of the patient activation measure among multimorbid older adults. Health Serv Res. 2011;46(2):457–478. | ||
Tschida S, Aslam S, Khan TT, Sahli B, Shrank WH, Lal LS. Managing specialty medication services through a specialty pharmacy program: the case of oral renal transplant: immunosuppressant medications. J Manag Care Pharm. 2013;19(1):26–41. | ||
Kinney RL, Lemon SC, Person SD, Pagoto SL, Saczynski JS. The association between patient activation and medication adherence, hospitalization, and emergency room utilization in patients with chronic illnesses: a systematic review. Patient Educ Couns. 2015;98(5):545–552. | ||
Stirratt MJ, Dunbar-Jacob J, Crane HM, et al. Self-report measures of medication adherence behavior: recommendations on optimal use. Transl Behav Med. 2015;5(4):470–482. | ||
Denhaerynck K, Schafer-Keller P, Young J, Steiger J, Bock A, De Geest S. Examining assumptions regarding valid electronic monitoring of medication therapy: development of a validation framework and its application on a European sample of kidney transplant patients. BMC Med Res Methodol. 2008;8:5. | ||
Marcum ZA, Zheng Y, Perera S, et al. Prevalence and correlates of self-reported medication non-adherence among older adults with coronary heart disease, diabetes mellitus, and/or hypertension. Res Social Adm Pharm. 2013;9(6):817–827. | ||
Pillittere-Dugan D, Nau DP, McDonough K, Pierre Z. Development and testing of performance measures for pharmacy services. J Am Pharm Assoc (2003). 2009;49(2):212–219. | ||
PharmacyQualityAlliance. PQA measures used by CMS in the STAR ratings. 2012. Available from: http://pqaalliance.org/measures/cms.asp. Accessed August 1, 2016. | ||
Franklin JM, Shrank WH, Pakes J, et al. Group-based trajectory models: a new approach to classifying and predicting long-term medication adherence. Med Care. 2013;51(9):789–796. | ||
Zullig LL, Peterson ED, Bosworth HB. Ingredients of successful interventions to improve medication adherence. JAMA. 2013;310(24):2611–2612. | ||
van Driel ML, Morledge MD, Ulep R, Shaffer JP, Davies P, Deichmann R. Interventions to improve adherence to lipid-lowering medication. Cochrane Database Syst Rev. 2016;12:CD004371. | ||
Conn VS, Ruppar TM, Chase JA, Enriquez M, Cooper PS. Interventions to improve medication adherence in hypertensive patients: systematic review and meta-analysis. Curr Hypertens Rep. 2015;17(12):94. | ||
Hugtenburg J, Timmers L, Elders P, Vervloet M, van Dijk L. Definitions, variants, and causes of nonadherence with medication: a challenge for tailored interventions. Patient Prefer Adherence. 2013;7:675–682. | ||
Hibbard J, Stockard J, Mahoney E, Tusler M. Development of the Patient Activation Measure (PAM): conceptualizing and measuring activation in patients and consumers. Health Serv Res. 2004;39(4 Pt 1):1005–1026. | ||
Vrijens B, Tousset E, Rode R, et al. Successful projection of the time-course of drug concentration in plasma during a one-year period from electronically compiled dosing-time data used as input to individually parameterized pharmacokinetic models. J Clin Pharmacol. 2005;45:461–467. | ||
Duke University CRI – The Medication Adherence Alliance - Adherence Measures Working Group. Available from: http://managingyourmeds.org/wp-content/uploads/2016/02/Glossary-of-Terms-12_13_2015.pdf. Accessed August 1, 2016. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.