")
Back to Journals » International Journal of Women's Health » Volume 6
Combining oral contraceptives with a natural nuclear factor-kappa B inhibitor for the treatment of endometriosis-related pain
Authors Maia Jr H, Haddad C, Casoy J
Received 1 October 2013
Accepted for publication 13 November 2013
Published 21 December 2013 Volume 2014:6 Pages 35—39
DOI https://doi.org/10.2147/IJWH.S55210
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Hugo Maia Jr,1–3 Clarice Haddad,3 Julio Casoy3
1Department of Gynecology and Obstetrics, School of Medicine, Federal University of Bahia, 2Itaigara Memorial Day Hospital, 3Centro de Pesquisas e Assistência em Reprodução Humana (CEPARH), Salvador, Bahia, Brazil
Abstract: Endometriosis is a chronic disease in which a persistent state of heightened inflammation is maintained by nuclear factor-kappa B (NF-κB) activation. The progestins present in oral contraceptives are potent inhibitors of NF-κB translocation to cell nuclei, while Pycnogenol® (Pinus pinaster) acts by blocking post-translational events. In this study, the effects of Pycnogenol on pain scores were investigated in patients with endometriosis using oral contraceptives containing either gestodene or drospirenone in extended regimens. Pain scores were determined using a visual analog scale before and after 3 months of treatment. Oral contraceptives, used alone (groups 1 and 3) or in association with Pycnogenol (groups 2 and 4), resulted in significant decreases in pain scores after 3 months of treatment; however, this reduction was significantly greater in the groups using oral contraceptives + Pycnogenol (groups 2 and 4) compared with those using oral contraceptives alone (groups 1 and 3). In the groups using oral contraceptives alone, 50% of patients became pain-free by the end of the third month of treatment. These results suggest that Pycnogenol increases the efficacy of oral contraceptives for the treatment of endometriosis-related pain.
Keywords: Pycnogenol®, aromatase, endometriosis, nuclear factor-kappa B
Introduction
Endometriosis is an inflammatory pathology in which there is an increase in positivity for nuclear factor-kappa B (NF-κB), cyclooxygenase (Cox)-2, and aromatase expression in the eutopic endometrium.1 These functional changes create a vicious cycle of increased inflammation and local estrogen production that helps perpetuate the survival of endometrial cells in ectopic locations by blocking their phagocytosis via activated macrophages.1,2 Progression of endometriosis depends on continuous seedling of aromatase-positive cells carried to the pelvis by retrograde menstruation.3 In patients submitted to endometrial resection following laparoscopic treatment for endometriosis, the recurrence rate of the disease has been reported to be much lower.4 These results suggest that the presence of an intact endometrium rather than completeness of surgery may be a key factor in the success of treatment. Therefore, inducing long-lasting amenorrhea is a necessary step in the treatment of endometriosis and involves use of medication over prolonged periods of time.1
One promising approach is the use of oral contraceptives, since they are not only extremely effective in controlling pain and curbing inflammation, but they also prevent the recurrence of endometriosis following surgical treatment.5 The mechanism of action of oral contraceptives is complex and involves a central ovulation-blocking effect in addition to local effects on the endometrium and endometriosis lesions.2 This local action involves blockade of several enzymatic pathways, such as Cox and aromatase p450, that are necessary for the survival and progression of endometriosis.1
Progesterone and oral contraceptives containing gestodene have been reported to obstruct NF-κB activation and its translocation to cell nuclei where it would activate the genes responsible for the inflammatory cascade.1,6,7 However, not every woman using oral contraceptives in a continuous regimen for the treatment of endometriosis becomes amenorrheic, and the occurrence of breakthrough bleeding is associated with activation of NF-κB in the endometrium, initiating a cascade of inflammatory events and leading to persistent Cox-2 and aromatase expression in this tissue.1,6 Unabated aromatase expression leading to an enhanced local inflammatory, prostaglandin-mediated response may be the underlying mechanism behind the persistent pain and bleeding in endometriosis patients using oral contraceptives.8 These hypotheses may also explain the greater efficacy of the combination of oral contraceptives and aromatase inhibitors in managing endometriosis-related pain in patients who fail to respond satisfactorily to hormone therapy alone.9
Resveratrol, a polyphenolic compound isolated from the skin of red grapes, is a natural aromatase inhibitor. In addition to its anti-inflammatory properties, at pharmacologic doses resveratrol also inhibits aromatase activity at both the enzyme and gene transcription levels.8,10 It was recently reported that resveratrol exerts a potentiating effect on pain management when used in association with oral contraceptives in patients with endometriosis.8 These preliminary results suggest that the association of oral contraceptives with plant-derived anti-inflammatory drugs may improve the efficacy of oral contraceptives for the treatment of endometriosis-related pain by increasing amenorrhea rates without exacerbating the side effects of the treatment.1,8
Another promising compound is Pycnogenol® (Horphag, Geneva, Switzerland), a complex mixture of procyanidins and polyphenol components harvested from the bark of the French maritime pine (Pinus pinaster). Pycnogenol has been shown to exert anti-inflammatory and antithrombotic effects11 by inhibiting both Cox-1 and Cox-2 enzymatic activity.12 Suppression of NF-κB-dependent gene expression, which activates the inflammatory cascade, also contributes to the pain-ameliorating effects of Pycnogenol.13,14 Since endometriosis is an inflammatory pathology in which expression of these inflammatory markers is exacerbated, combining oral contraceptives with this natural NF-κB inhibitor would appear logical.1
In the present report, the effects of an association of Pycnogenol and oral contraceptives on pelvic pain were investigated in patients with endometriosis.
Patients and methods
This open, office-based study was conducted to evaluate the effect of Pycnogenol on the management of endometriosis-related pain in patients using postoperative hormonal therapy. Forty-five patients of reproductive age (range 22–37 years) with a laparoscopically confirmed diagnosis of endometriosis and whose main indication for laparoscopy was pelvic pain were treated at the outpatient clinic of the Instituto da Mulher with oral contraceptives in extended regimens, either alone or in association with Pycnogenol. Laparoscopy was performed at the Itaigara Memorial Day Hospital by the same team of surgeons (HM, CH) in all cases. The diagnosis of endometriosis was made visually during laparoscopy, the lesions were digitally photographed for medical records, and the extent of endometriosis was staged according to American Society for Reproductive Medicine guidelines.15 In accordance with this staging system, 26 patients were classified as having stage I or II, while the remaining 16 were classified as having stage III or IV of the disease. Before beginning hormonal treatment at the Instituto da Mulher, the patients were interviewed to determine the severity of dysmenorrhea and at that time were randomly allocated to one of the four treatment groups according to the week of the month (weeks 1–4) in which they were first seen. In group 1 (n=7) the patients were treated with an oral contraceptive containing gestodene 75 μg and ethinylestradiol 30 μg, administered in a continuous regimen. In group 2, the same oral contraceptive regimen was used in association with 100 mg of Pycnogenol (n=14). In group 3 (n=13), the patients were treated with an oral contraceptive containing drospirenone 3 mg and ethinylestradiol 30 μg (n=13) administered in a continuous regimen and in group 4 (n=11), patients followed the same contraceptive regimen used by the women in group 3 but in association with a daily dose of 100 mg of Pycnogenol. Pycnogenol (pinus pinaster extract), prescribed at a dose of 50 mg every 12 hours, was obtained either from a compound pharmacy (Fagron, Rotterdam, the Netherlands) or in the form of a commercially available product (Flebon®, Farmoquimica, Rio de Janeiro, Brazil). In all cases, the contraceptive pills containing either drospirenone or gestodene were used in a continuous regimen. The study was approved by the internal review board of the Instituto da Mulher and the Itaigara Memorial Day Hospital. Neither Flebon nor the oral contraceptive pills used in extended regimens are new investigational drugs. Flebon is approved by the Brazilian regulatory authorities (National Health Surveillance Agency) for the treatment of varicose veins and there is no contraindication to its use by oral contraceptive users. Contraceptives containing either gestodene or drospirenone (Libbs Farmacêutica, São Paulo, Brazil) are already approved by the National Health Surveillance Agency for use in extended regimens; therefore, this indication is not off-label in Brazil. Because this study involved no new investigational drugs and since all the drugs used in the study are readily available at any dispensing pharmacy in Brazil, the institution’s internal review board dispensed with the need for the patients to sign an informed consent form. However, the attending physician discussed the medication with each patient individually and the patients verbally agreed to use the treatment selected. For this reason, neither the physician nor the patients were blinded to the treatment.
During office evaluation conducted prior to initiation of treatment and after 3 months’ use of the medication, the patients were asked to grade the severity of their pelvic pain, including dysmenorrheal, in accordance with a visual analog pain scale graded from 0 to 10, on which 0 was indicative of no pain and 10 the most excruciating pain. This evaluation was carried out by the same investigators (HM, CH) prior to oral contraceptive use and after 3 months of pill use. Statistical analysis was performed using the Student’s t-test, with P-values<0.05 being considered statistically significant.
Results
Pycnogenol and pain control in oral contraceptive users
There was no statistically significant difference in mean pain score prior to initiation of treatment between the four groups. The use of oral contraceptives alone, both those containing gestodene (group 1) and those containing drospirenone (group 3), used in a continuous regimen, resulted in a significant decrease in menstrual-related pain (dysmenorrhea) at the end of the third month of treatment when compared with pretreatment values. However, in patients using oral contraceptives together with Pycnogenol (groups 2 and 4), the reduction in mean pain score was more pronounced and significantly greater than that found in groups 1 and 3 in which the oral contraceptives were used alone. On the other hand, there were no statistically significant differences in post-treatment pain scores between groups 1 and 3 or between groups 2 and 4. In users of Pycnogenol + oral contraceptives, 8/14 (57%) of patients in group 2 and 6/11 (54%) of those in group 4 reported complete resolution of pain, while none of the patients in groups 1 and 3 had become completely pain-free by the end of the third month of treatment. These results are summarized in Table 1. No additional side effects were observed with the use of Pycnogenol therapy compared with those recorded with the use of oral contraceptives alone.
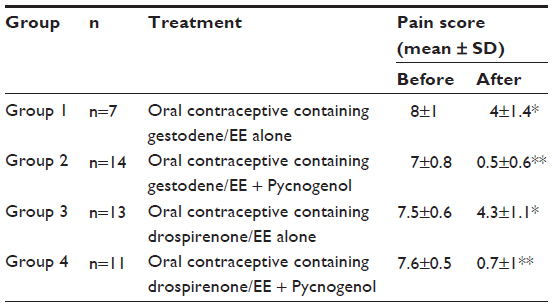 | Table 1 Pain scores of patients with endometriosis when using oral contraceptives alone or in association with Pycnogenol® |
Discussion
Based on the results of this preliminary observational study, the use of Pycnogenol combined with oral contraceptives in a continuous regimen appears to be more effective than oral contraceptives alone for the treatment of endometriosis-related pain. This increased efficacy likely results from the more effective suppression of NF-κB activation at both the pre and post translational level following combined use of these compounds.13,14 The greater reduction in pain scores during use of oral contraceptives combined with Pycnogenol when compared with oral contraceptives alone is therefore the consequence of more effective blockade of NF-κB activation in endometriosis lesions and in the eutopic endometrium because of a synergetic effect of the combined therapy on both pre and post DNA binding of this transcription factor.1,6
The combination of hormone therapy with plant-derived NF-κB blockers may represent a viable alternative for the treatment of endometriosis-related pain, since these agents may increase the efficacy of oral contraceptives in controlling this symptom without augmenting the incidence of undesirable side effects.1 Previous reports showed that Pycnogenol alone was as effective as gonadotropin-releasing hormone analogs for the treatment of endometriosis after the second month of treatment.16
Pycnogenol affects the transactivation capacity of NF-κB, thus reducing expression of the inflammatory genes regulated by this transcription factor.17 However, Pycnogenol does not prevent NF-κB from binding to DNA, suggesting that its mechanism of action is different from that of progesterone, which acts by preventing translocation of the activated NF-κB subunit to the cell nucleus and its consequent binding to DNA, where it will activate translation of genes such as Cox-2 that are involved in the inflammatory cascade.17 Cox-2 will stimulate prostaglandin production, which in turn will activate the aromatase gene, thus stimulating local estrogen synthesis in the endometrium and enhancing the inflammatory reaction, as occurs in the breast.1,18 Although both progestins and Pycnogenol reduce inflammation by modulating NF-κB-induced gene transcription, they act on different steps in this mechanism, which explains the greater efficacy of the combination therapy for the control of endometriosis-related pain. When given together with an oral contraceptive, not only is the DNA binding activity reduced but also the transactivation capacity of the bound NF-κB.13,14,17 This distinctive effect on the NF-κB activation pathway may provide a plausible explanation at the molecular level for the results reported here. It is also noteworthy that the increased efficacy in terms of pain control in endometriosis is not accompanied by any increase in incidence of side effects.
The disappearance of dysmenorrhea in almost 50% of the patients as reported here also confirms previous observations that use of Pycnogenol alone is effective in treating this ailment.19–21 However, these findings, albeit encouraging, should be considered as preliminary, and larger, well designed, blinded clinical trials are required to confirm these initial observations. The idea of combining a progestin with a post-translation inhibitor of NF-κB action may constitute a new approach that will not only increase the efficacy of hormonal treatment in inducing long-lasting amenorrhea but will also reduce endometriosis pain scores.
Disclosure
The authors report no conflicts of interest in this work.
References
Maia H Jr, Haddad C, Coelho G, Casoy J. Role of inflammation and aromatase expression in the eutopic endometrium and its relationship with the development of endometriosis. Womens Health (Lond Engl). 2012;8:647–658. | |
Maia H Jr, Casoy J, Correia T, Freitas LA, Pimentel K, Athayde C. The effect of oral contraceptives on aromatase expression in the eutopic endometrium of patients with endometriosis. Gynecol Endocrinol. 2008;24:123–128. | |
Maia H Jr, Haddad C, Casoy J. Correlation between aromatase expression in the eutopic endometrium of symptomatic patients and the presence of endometriosis. Int J Womens Health. 2012;4:61–65. | |
Bulletti C, DeZiegler D, Stefanetti M, Cicinelli E, Pelosi E, Flamigni C. Endometriosis: absence of recurrence in patients after endometrial ablation. Hum Reprod. 2001;16:2676–2679. | |
Maia H Jr, Casoy J. Non contraceptive health benefits of oral contraceptives. Eur J Contracept Reprod Health Care. 2008;13:17–24. | |
Maia H Jr, Casoy J, Correia T, Athayde C, Valente J, Coutinho EM. Activation of NF-kappaB and COX-2 expression is associated with breakthrough bleeding in patients using oral contraceptives in extended regimens. Gynecol Endocrinol. 2010;26:265–269. | |
Pan DS, Liu WG, Yasng XF, Cao F. Inhibitory effect of progesterone on inflammatory factors after experimental brain injury. Biomed Environ Sci. 2007;20:432–438. | |
Maia H Jr, Haddad C, Pinheiro N, Casoy J. Advantages of the association of resveratrol with oral contraceptives for management of endometriosis-related pain. Int J Womens Health. 2012;4:543–549. | |
Amsterdam LL, Gentry W, Jobanputra S, Wolf M, Rubin SD, Bulun SE. Anastrozole and oral contraceptives: a novel treatment for endometriosis. Fertil Steril. 2005;84:300–304. | |
Harikumar KB, Aggarwal BB. Resveratrol: a multitargeted agent for age-associated chronic disease. Cell Cycle. 2008;7:1020–1035. | |
Belcaro G, Cesarone MR, Rohdewald P, et al. Prevention of venous thrombosis and thrombophlebitis in long haul flights with pycnogenol. Clin Appl Thromb Hemost. 2004:10:373–377. | |
Schafer A, Chovanova Z, Muchova J, et al. Inhibition of Cox-1 and Cox-2 activity by plasma of human volunteers after ingestion of French maritime pine bark extract (Pycnogenol). Biomed Pharmacother. 2006;60:5–9. | |
Saliou C, Rimbach G, Moini H, et al. Solar ultraviolet-induced erythema in human skin and nuclear factor-kappa B-dependent gene expression in keratinocytes are modulated by French maritime pine bark extract. Free Radic Biol Med. 2001;30:154–160. | |
Peng Q, Wei Z, Lau BH. Pycnogenol inhibits tumor necrosis factor-alpha-induced nuclear factor kappa B activation and adhesion molecule expression in human vascular endothelial cells. Cell Mol Life Sci. 2000;57:834–841. | |
American Society for Reproductive Medicine. Revised American Society for Reproductive Medicine classification of endometriosis 1996. Fertil Steril. 1997;67:817–821. | |
Kohama T, Herai K, Inoue M. Effect of French maritime pine bark extract on endometriosis as compared with leuprorelin acetate. J Reprod Med. 2007;52:703–708. | |
Grimm T, Chovanova Z, Muchova J, et al. Inhibition of NF-kappaB activation and MMP-9 secretion by plasma of human volunteers after ingestion of maritime pine bark extract (Pycnogenol). J Inflamm (Lond). 2006;3:1. | |
Mendelson CR, Hardy DB. The role of progesterone receptor (PR) in the regulation of inflammatory response pathways and aromatase in the breast. J Steroid Biochem Mol Biol. 2006;102:241–249. | |
Kohama T, Suzuki N, Ohno S, Inoue M. Analgesic efficacy of French maritime pine bark extract in dysmenorrhea: an open clinical trial. J Reprod Med. 2004;49:828–832. | |
Kapoor S. Pycnogenol: a rapidly expanding role in the management of systemic diseases besides dysmenorrhea. J Reprod Med. 2009;54:117. | |
Suzuki N, Uebaba K, Kohama T, Moniwa N, Kanayama N, Koike K. French maritime pine bark extract significantly lowers the requirement for analgesic medication in dysmenorrhea: a multicenter, randomized, double-blind, placebo-controlled study. J Reprod Med. 2008;53:338–346. |
 © 2013 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2013 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.