")
Back to Journals » Cancer Management and Research » Volume 14
Combination of Estrogen Receptor Alpha and Histological Type Helps to Predict Lymph Node Metastasis in Patients with Stage IA2 to IIA2 Cervical Cancer
Authors Ke Y, Zu S, Chen L, Liu M, Yang H, Wang F, Zheng H, He F
Received 16 October 2021
Accepted for publication 19 December 2021
Published 26 January 2022 Volume 2022:14 Pages 317—325
DOI https://doi.org/10.2147/CMAR.S343518
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Harikrishna Nakshatri
Yumin Ke,1,* Shuiling Zu,2,* Lijun Chen,3,* Meizhi Liu,4 Haijun Yang,5 Fuqiang Wang,5 Huanhuan Zheng,6 Fangjie He7,8
1Department of Obstetrics and Gynecology, The Second Affiliated Hospital of Fujian Medical University, Quanzhou, 362000, People’s Republic of China; 2Nursing Department, The Third Affiliated People’s Hospital of Fujian University of Traditional Chinese Medicine, Fuzhou, 350100, People’s Republic of China; 3Department of Gynecological Oncology, Fujian Cancer Hospital, Fujian Medical University Cancer Hospital, Fuzhou, 350014, People’s Republic of China; 4Department of Gynecology, The Third Affiliated People’s Hospital of Fujian University of Traditional Chinese Medicine, Fuzhou, 350100, People’s Republic of China; 5Department of Pathology, The Anyang Tumor Hospital, Anyang, 455000, People’s Republic of China; 6Department of Endocrinology, Ji’an Central People’s Hospital, Ji’an, 343000, People’s Republic of China; 7Department of Obstetrics and Gynecology, The First People’s Hospital of Foshan, Foshan, 528000, People’s Republic of China; 8State Key Laboratory of Oncology in South China, Sun Yat-sen University Cancer Center, Guangzhou, 510060, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fangjie He
Department of Obstetrics and Gynecology, The First People’s Hospital of Foshan, Foshan, People’s Republic of China; State Key Laboratory of Oncology in South China, Sun Yat-sen University Cancer Center, Guangzhou, 510060, People’s Republic of China
, Tel +86-18038864533
, Fax +86 757-83162610
, Email [email protected]; [email protected]
Objective: This study aimed to identify a subset of patients with stage IA2 to IIA2 cervical cancer who are at low risk of lymph node metastasis (LNM) using pathological parameters including estrogen receptor alpha (ERα) and progesterone receptor (PR).
Methods: The clinical data of patients with stage IA2 to IIA2 cervical cancer who underwent radical surgery between 2014 and 2015 were retrospectively reviewed. Immunohistochemical staining was used to determine the expression of ERα and PR. A low-risk criterion for LNM was identified using logistic regression analysis, and its performance was estimated through receiver-operating characteristic curve analysis.
Results: Of 263 patients, 57 (21.7%) had pathological LNM. ERα (adjusted odds ratio [aOR], 7.582; 95% confidence interval [CI], 2.991– 19.222; P < 0.001) and squamous cell carcinoma (aOR, 3.520; 95% CI, 1.887– 6.568; P < 0.001) were identified as independent predictors for no LNM by multivariate logistic regression analysis, while PR had no effect on LNM. The rate of LNM was 1.4% for low-risk patients (n = 73) identified as ERα positive with squamous cell carcinoma. The 5-year disease-free survival in low-risk patients was significantly greater than in those negative for ERα and/or those with non-squamous cell carcinoma (96.9% vs 80.1%, P = 0.002).
Conclusion: ERα positivity and squamous cell carcinoma are associated with a low risk of LNM in patients with stage IA2 to IIA2 cervical cancer. Hence, those patients without a low risk of LNM could be considered for definitive chemoradiotherapy to avoid unnecessary surgery.
Keywords: cervical cancer, lymph node, estrogen receptor alpha, progesterone receptor, squamous cell carcinoma
Introduction
Cervical cancer is the fourth most common cancer among women worldwide.1 Currently, the primary treatment methods for patients with cervical cancer include radical surgery and concurrent chemoradiotherapy.2
The presence or absence of lymph node metastasis (LNM) determines the treatment strategy. Patients found to have LNM on histopathology after radical surgery require additional adjuvant radiotherapy to lower the risk of tumor recurrence and to prolong survival.2,3 However, unnecessary surgery combined with additional adjuvant radiotherapy may lead to severe comorbidities, such as genitourinary complications, gastrointestinal morbidities, lymphedema, and lymphocysts.4,5 Therefore, radical hysterectomy and bilateral pelvic lymphadenectomy are more suitable treatments for patients with early-stage cervical cancer without LNM. The identification of patients at low risk for LNM before surgery is an important research topic.
Imaging examinations, including computed tomography or magnetic resonance imaging, are typically used to determine lymph node status, with a relatively high specificity (>85%) and low sensitivity (<65%).6–8 The low sensitivity of these imaging examinations indicates that more than 35% of patients experience a missed diagnosis of LNM and require additional adjuvant radiotherapy. Tumor relative protein secreted by tumor cells may be useful to evaluate lymph node status.9 In addition, the detection of this protein may be useful in preoperative biopsies for cervical cancer. Estrogen receptor alpha (ERα) and progesterone receptor (PR) have been reported to be of significant importance in the occurrence and development of cervical cancer.10–12 One previous study demonstrated that ERα can mediated the PI3K/Akt-NF-κB pathway and further activates the downstream genes of nuclear NF-κB p65 to regulate cell proliferation.13 Another study revealed that estrogen receptors mediate the PI3K/Akt/mTOR pathway to inhibit tumor growth.14 However, the relationship between these two receptors and lymph node metastasis is unclear.
The aim of this study was to determine the predictive value of ERα and PR for LNM in patients with stage IA2-IIA2 cervical cancer, and to identify patients at low risk for LNM using preoperative clinical parameters and immunohistochemistry.
Methods
Study Design and Cohort
This retrospective study was approved by the Institutional Review Board of the First People’s Hospital of Foshan (L2020-17). The requirement of informed consent was waived due to the retrospective nature of the study. The study was conducted in accordance with the Declaration of Helsinki. The clinicopathological records and data of patients who underwent surgical treatment for stage IA2 to IIA2 cervical cancer between January 1, 2014 and December 31, 2015, at our institution were collected and reviewed. This study included patients with stage IA2 to IIA2 cervical cancer according to the 2009 International Federation of Gynecology and Obstetrics (FIGO) staging system;15 squamous cell carcinoma, adenocarcinoma, or adenosquamous carcinoma; and those who underwent a type C radical hysterectomy and bilateral pelvic lymphadenectomy (Querleu-Morrow classification). Patients were excluded if they received adjuvant chemotherapy or radiotherapy before surgery or were lost to follow-up.
In total, 263 patients were included in the study. Patients were divided into two groups by lymph node status: the LNM group (n = 57) and the non-LNM group (n = 206).
Immunohistochemistry
Cervical specimens for immunohistochemistry were collected at our institution. Specimens were fixed with formalin, embedded in paraffin, sectioned to a thickness of 4 µm, and stained with hematoxylin and eosin. All hematoxylin and eosin-stained slides for each case were reviewed, and those with a rich cervical tumor were selected for immunohistochemical staining. Paraffin-embedded tissue blocks were sectioned to a thickness of 4 µm and mounted on polylysine-treated slides. Then, sections were baked at 60 °C for 3 h, followed by deparaffinization with two jars of xylene for 10 min each and rehydrated through 100%, 95%, 85%, and 75% alcohol solutions for 5 min to deionized H2O. The antibodies included rabbit monoclonal antibodies for ERα (dilution 1:200; Abcam, UK) and PR (dilution 1:100; Abcam, UK). Sections for the detection of ERα and PR were pretreated in the microwave in a Tris-EDTA solution (pH=9.0) for 20 min. The slides were then covered with 3% hydrogen peroxide for 10 min to block endogenous peroxidase activity. The specimens were incubated with primary antibodies for 1 h, followed by incubation with HRP-labeled anti-rabbit secondary antibodies. Furthermore, a 3,3-diaminobenzidine incubation was performed for visualization of immunoreactive proteins, and nuclei were counterstained with hematoxylin. Appropriate positive and negative controls were also prepared to assess the quality control of this immunohistochemistry staining protocol.
Pathological Examination
The immunohistochemical evaluation of the expressions of ERα and PR was conducted independently by two pathologists who were blinded to the patients’ clinical information.
An immunoreactive score (IRS) system was used to evaluate the immunohistochemical results. Several previous studies have reported that the expressions of ERα and PR in tumor cells are associated with cancer development, whereas stromal ERα and PR expression remained essentially unchanged.16–18 Therefore, the percentage of positively stained tumor cells was scored as 0 (<1%), 1 (1%-10%), 2 (11%-50%), 3 (51%-80%), or 4 (˃80%), and the intensity of staining was scored as 0 (none), 1 (weak), 2 (moderate), or 3 (strong). Multiplying these scores yielded an IRS of 0 to 12. Stratified comparison was performed by defining the following two categories: negative expression (IRS 0) and positive expression (IRS ≥1) (Figure 1).14,16
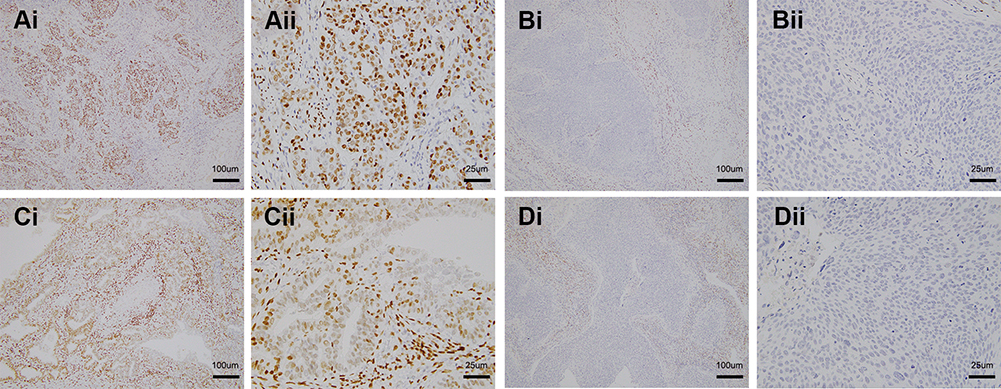 |
Figure 1 Immunohistochemical staining of ER and PR expressions. (1Ai, 1Aii) (cervical squamous cell carcinoma with stage IB1) and (1Bi, 1Bii) (cervical squamous cell carcinoma with stage IB1) show the positive and negative ERα expression, respectively; (1Ci, 1Cii) (cervical adenocarcinoma with stage IB1) and (1Di, 1Dii) (cervical squamous cell carcinoma with stage IB1) show the positive and negative PR expression, respectively. (1Aii, 1Bii, 1Cii and 1Dii) are the enlarged images of (1Ai, 1Bi, 1Ci and 1Di), respectively. Tumor cells and stromal cells with positive ERα and PR expression display yellow or brown granules in the nucleus. |
In addition, a retrospective review of hematoxylin and eosin-stained lymph nodes and cervical tumor tissue specimens was independently performed by the two pathologists. The results of the review of histological types and lymph node status were consistent with those in the original pathological reports.
Endpoints
The primary endpoint was pathological lymph node status after surgery. The secondary endpoint was 5-year disease-free survival (DFS), calculated as the number of months from the date of diagnosis to the first evidence of recurrence or death from cervical cancer, whichever occurred first.
Statistical Analysis
The Student’s t-test and chi-squared test, or Fisher’s exact test, were used to compare the continuous and categorical variables between the two groups, respectively. A multivariate, forward stepwise logistic regression analysis was performed to identify the independent risk factors for LNM. The performance of parameters for LNM prediction was determined using receiver-operating characteristic (ROC) curve analysis. Five-year DFS was estimated and compared between groups using the Kaplan-Meier method and Log rank test, respectively. All statistical analyses were performed using SPSS version 26.0 (IBM Inc., Chicago, IL, USA) and STATA version 15.0 (College Station, TX, USA). A two-sided P-value <0.05 was considered statistically significant.
Results
Patient Characteristics
The patient flow chart is shown in Figure S1. The clinical and pathological characteristics of the patients are summarized in Table S1. Of 263 patients, 57 (21.7%) were found to have LNM and 206 (78.3%) did not have LNM, as diagnosed on the pathology reports.
The patients’ clinical and pathological characteristics were compared between patients with and without LNM (Table 1). Patients with LNM had more advanced cervical cancer (p=0.003), a larger tumor diameter (p=0.016), received adjuvant radiotherapy (p<0.001), and had a lower expression of ERα on immunohistochemistry findings (p<0.001); they were also more likely to have a histological type of adenocarcinoma or adenosquamous carcinoma (p<0.001).
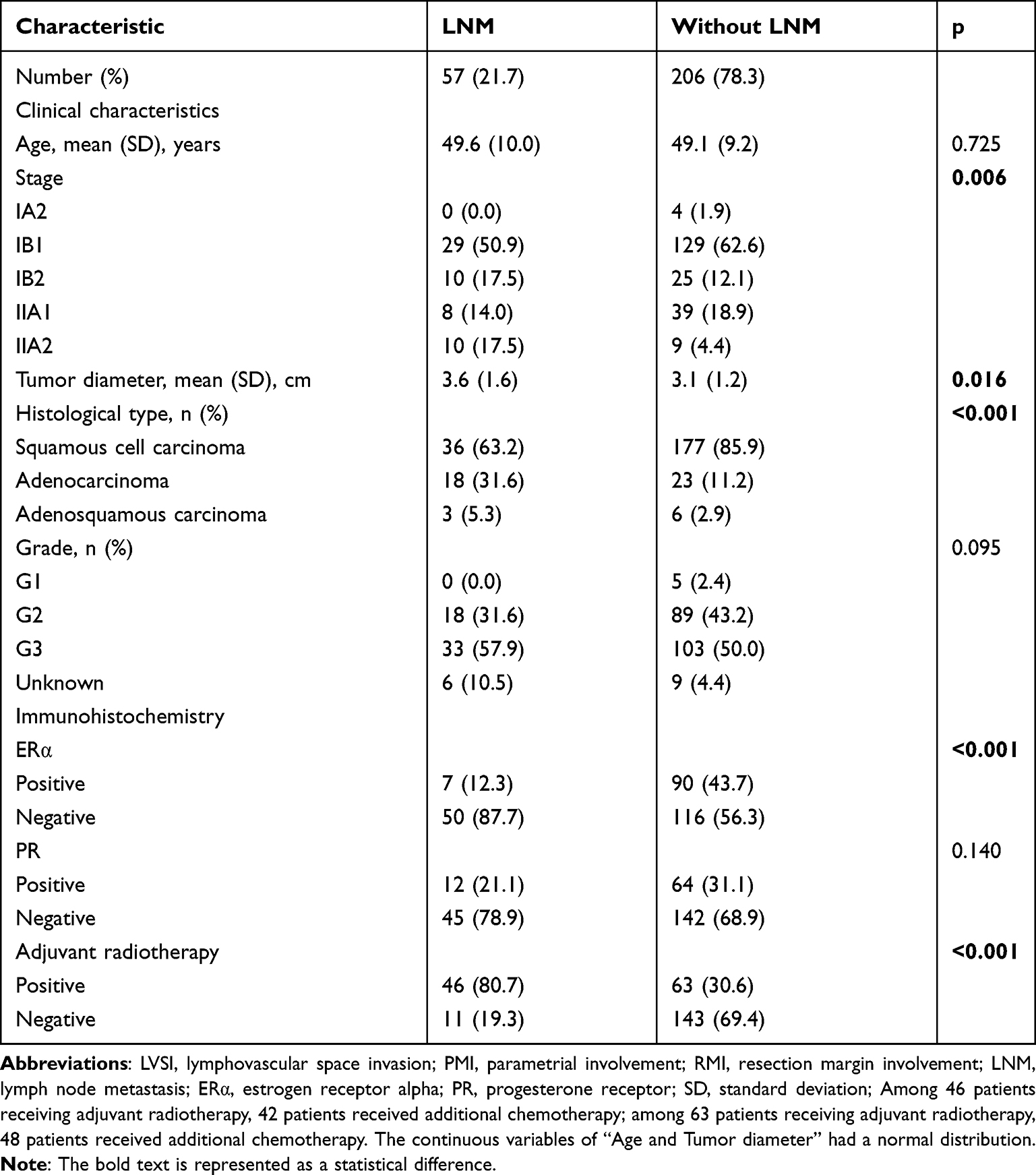 |
Table 1 Preoperative Clinical Characteristics and Immunohistochemistry Findings of Patients with LNM or without LNM |
Expressions of ERα and PR
Representative images defined as positive and negative staining of ERα and PR are shown in Figure 1. Tumor cells and stromal cells with positive ERα and PR expression display yellow or brown granules in the nucleus. Even in patients with negative ERα and PR expression in the tumor cells, the stromal cells showed positive staining. Patients without LNM were found to have a significantly higher rate of positive staining for ERα (43.7% vs 12.3%, p<0.001), whereas the rate of positive staining for PR was not significantly different between the two groups (31.1% vs 21.1%, p=0.140) (Table 1).
Risk Factors for LNM
The univariate and multivariate analyses of preoperative risk factors for LNM by binary logistic regression models are shown in Table 2. In the univariate analysis, stage, tumor diameter, histological type, grade, and ERα expression were found to be significantly associated with LNM. In the multivariate analysis, except stage, the other four variables were identified as independent predictors for LNM.
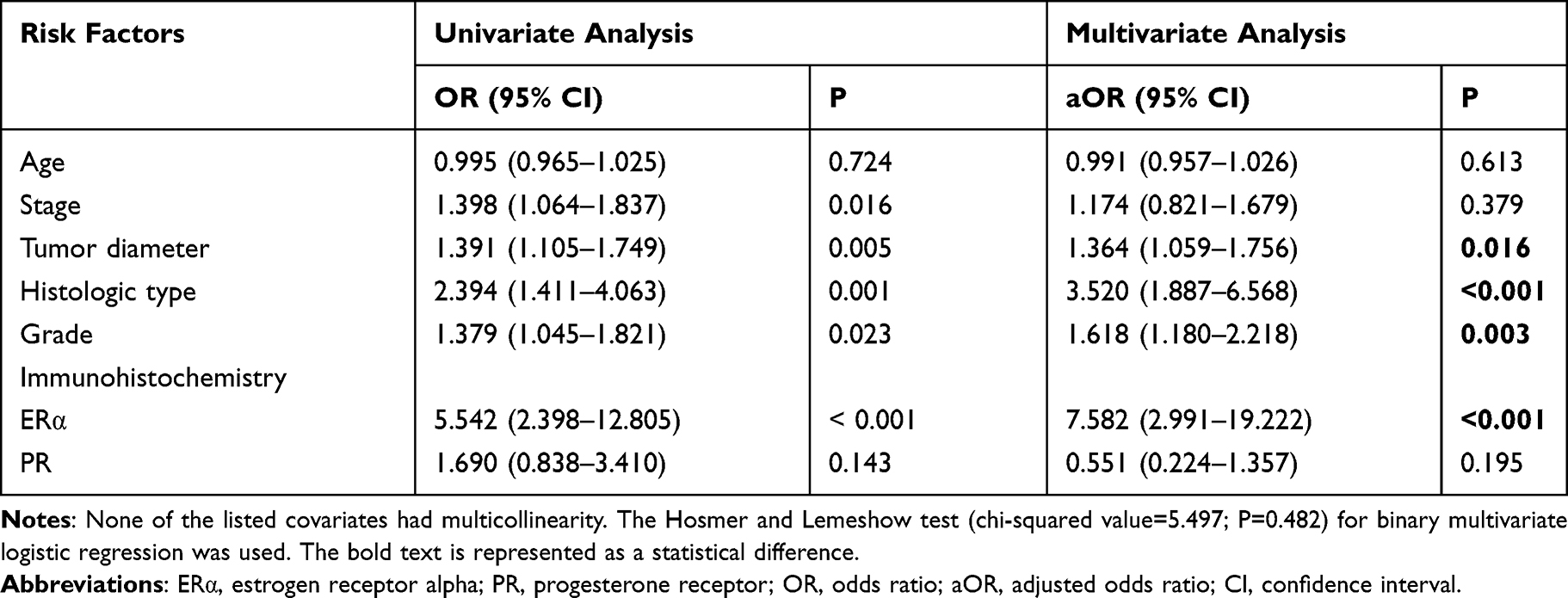 |
Table 2 Univariate and Multivariate Analyses of Preoperative Risk Factors for LNM by Binary Logistic Regression Models |
Low-Risk Group for LNM
The predictive performance of ERα for LNM was determined via ROC curve analysis, and found to have an optimal value of sensitivity and a low specificity (area under the ROC curve, 0.657; 95% confidence interval [CI], 0.584–0.730; p < 0.001) (Table 3, Figure 2A). To improve the sensitivity and decrease the risk of missed diagnosis, squamous cell carcinoma, another independent risk factor with the highest odds ratios for LNM, was combined with ERα as a predictive model. This model was found to have a sensitivity of 98.2% (area under the ROC curve, 0.666; 95% CI, 0.597–0.735; p < 0.001) (Table 3, Figure 2A). In total, 73 patients (27.8%) were assigned to the low-risk group, and only one of these patients (1.4%) had LNM. The pathological risk factors and adjuvant radiotherapy in the low-risk group are shown in Table 4.
 |
Table 3 Predictive Model Performance and Preoperative Variables for LNM |
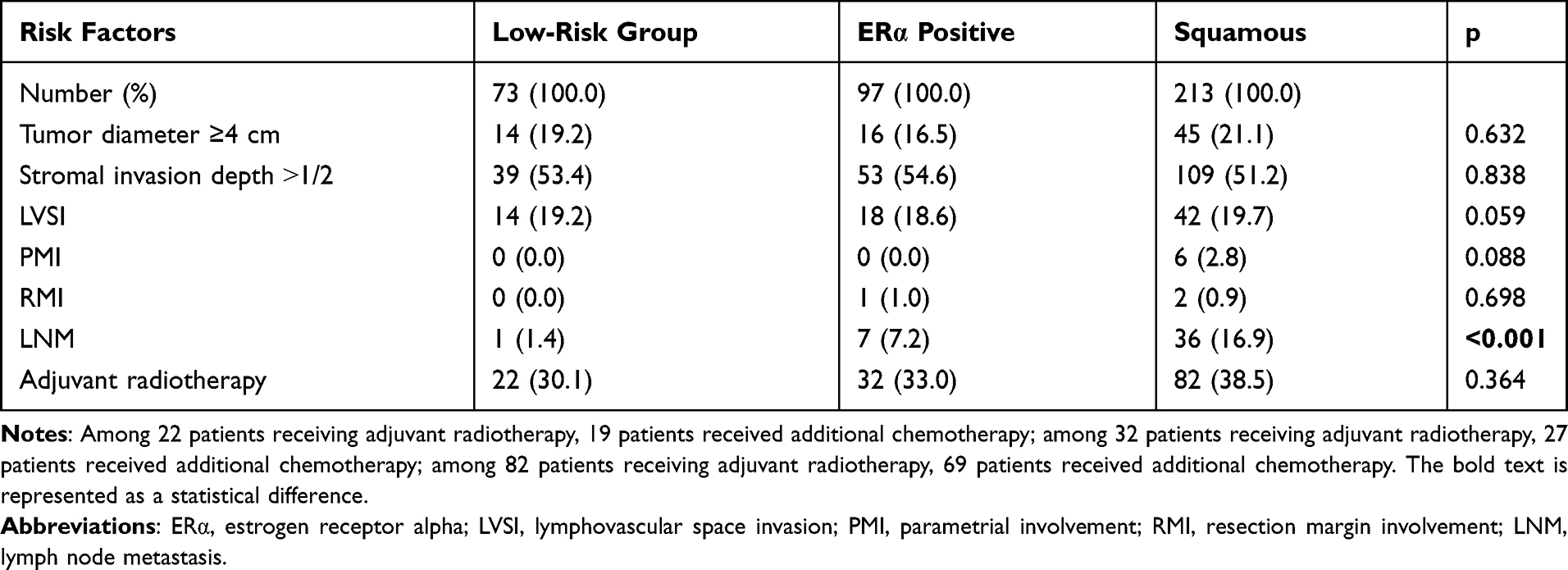 |
Table 4 Predictive Performance of Pathological Risk Factors and Adjuvant Radiotherapy for the Low-Risk Group |
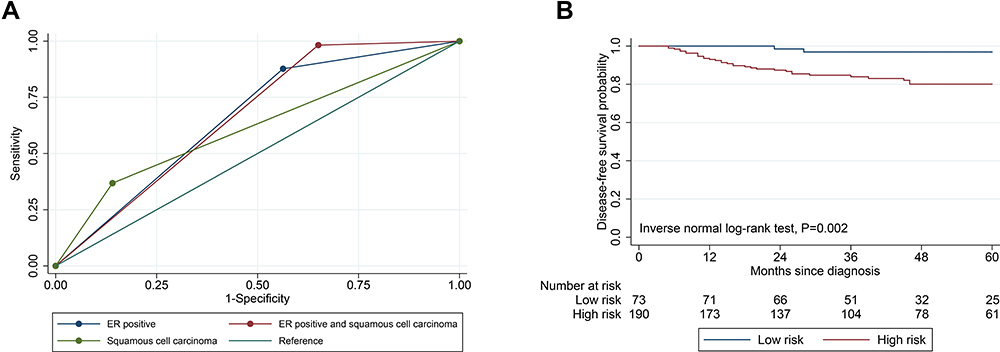 |
Figure 2 (A) ROC curves for LNM prediction: ERα positive, squamous cell carcinoma, and predictive performance. (B) Secondary outcomes: 5-year DFS of the predictive performance for LNM. Low risk (ERα positive and squamous cell carcinoma); High risk (ERα negative and/or non-squamous cell carcinoma). |
Survival Analysis
The median follow-up period for all patients was 43 months. The 5-year DFS in the low-risk group was 96.9%, whereas the 5-year DFS for patients who were negative for ERα and/or had non-squamous cell carcinoma was 80.1%. (p = 0.002) (Figure 2B).
Discussion
This study demonstrated that patients with stage IA2-IIA2 cervical cancer with ERα positivity and squamous cell carcinoma have a low risk of LNM. Furthermore, these pathology findings can be identified by cervical biopsy prior to radical surgery. Hence, those patients without a low risk of LNM could be considered for definitive chemoradiotherapy to avoid unnecessary surgery.
Several previous studies have reported an interesting phenomenon in which there was low or no expression of ERα and PR in tumor cells of cervical cancer, despite an obvious expression in cervical stromal cells.16,17 Furthermore, ERα and PR have been associated with survival in patients with cervical cancer.16 In the current study, the expression of ERα and PR in tumor cells was used as an assessment criterion to make the model more practical, as cervical biopsy tissue includes tumor cells, but may not include normal stroma. Cervical tumor cells were found to have a low expression of ERα and PR in this study. However, Fan et al have found opposing results. They found that positive ERα is associated with a worse prognosis in patients with cervical adenocarcinoma.19 One study may explain this inconsistent result. This study revealed that the canonical estrogen receptor, Erα, is frequently deficient while its variant, ERα-36, is highly expressed in cervical cancer cells. Furthermore, they found that ERα suppressed, while ERα-36 promoted, the migration and invasion of cervical cancer.20 This study aims to demonstrate the relationship of ERα, PR, and LNM, and we found that ERα is an independent predictor of no LNM with a high sensitivity. To decrease the risk of missed diagnoses for LNM and to render the model more practical, ERα and histological type were combined in this study to identify a group of patients at low risk for LNM.
In this study, we did not demonstrate a mechanistic association of ERα and LNM. However, previous studies have revealed that the expression of ERα is significant in the suppression of tumor cell proliferation in cervical cancer.21,22 Similarly, the absence of ERα contributes to cervical cancer development.18 Hence, we believe that ERα expression and activation have an inhibitory effect on tumor cell infiltration into the lymph node system. Previous studies have revealed that ERα suppression promoted the migration and invasion of cervical cancer cells through the Wnt/β-catenin/MRTF-A signaling pathway which is activated by HPV E7. Furthermore, miR-130a-3p may contribute to tumor progression by suppressing ERα.20,23 PR has also been reported to play a role in the prevention of cervical carcinogenesis in mice tests.11,24 However, PR was not associated with LNM and survival in the current study, which may be because PR only functions in the early stage of carcinogenesis.
Patients in the low-risk group in this study had a very low incidence of LNM; therefore, the expression of ERα and presence of squamous cell carcinoma can be used to decrease the risk of a false-negative LNM diagnosis prior to radical surgery. Compared with the high specificity (>85%) and low sensitivity (<65%) of CT or MR in detecting LNM, our model had a lower risk of a missed diagnosis (1.8%) for LNM.6–8 Previous studies have reported that the sensitivity for detecting LNM ranged from 84.3% to 92.96% using MRI-based radiomics analyses,25–27 which, however, were slightly lower than those of our model (98.2%). Furthermore, the low-risk group in this study also had fewer pathological risk factors and lower rates of adjuvant therapy use. Finally, survival analysis revealed that patients in the low-risk group had higher DFS rates. Therefore, compared to patients with stage IA2 to IB1 cervical cancer, those in the low-risk group (especially young patients) are more suitable for radical surgery, as evidenced by the fewer cases of LNM and less severe comorbidities resulting from adjuvant therapy observed in this group.
This study had several limitations. First, due to the retrospective nature of this study, selection bias was inherent. Second, although the model had a perfect performance in decreasing the risk of false-negative LNM diagnoses, it has yet to be validated at other institutions. Third, the mechanistic association of ERα and LNM was not investigated in this study. More research is necessary to determine the mechanistic relationship between ERα and LNM.
In conclusion, we found that a combination of immunohistochemistry and histological evaluations can help identify lymph node status in patients with IA2-IIA2 cervical cancer. ERα positive tumor cells and the presence of squamous cell carcinoma were identified as independent predictive factors for LNM, and these two parameters can be determined via cervical biopsy prior to radical surgery. These criteria are valuable for excluding LNM and to help avoid unnecessary surgery among patients with IA2-IIA2 cervical cancer.
Data Sharing Statement
Data associated with this paper are provided in the supplement. The data that support the findings of this study are available from the corresponding author, Fangjie He, upon reasonable request.
Ethics Statement
This retrospective study was approved by the Institutional Review Board of the First People’s Hospital of Foshan (L2020-17). The requirement of informed consent was waived due to the retrospective nature of the study. The study was conducted in accordance with the Declaration of Helsinki. Patient identity could not be identified in the publication.
Acknowledgments
We would like to thank Editage for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by China Postdoctoral Science Foundation (2021M700779).
Disclosure
All authors declare no conflicts of interest.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Koh WJ, Abu-Rustum NR, Bean S, et al. Cervical cancer, Version 3.2019, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2019;17(1):64–84. doi:10.6004/jnccn.2019.0001
3. Bhatla N, Aoki D, Sharma DN, Sankaranarayanan R. Cancer of the cervix uteri. Int J Gynaecol Obstet. 2018;143(Suppl 2):S22–S36. doi:10.1002/ijgo.12611
4. Soisson AP, Soper JT, Clarke-Pearson DL, Berchuck A, Montana G, Creasman WT. Adjuvant radiotherapy following radical hysterectomy for patients with stage IB and IIA cervical cancer. Gynecol Oncol. 1990;37:390–395. doi:10.1016/0090-8258(90)90374-T
5. Fiorica JV, Roberts WS, Greenberg H, Hoffman MS, LaPolla JP, Cavanagh D. Morbidity and survival patterns in patients after radical hysterectomy and postoperative adjuvant pelvic radiotherapy. Gynecol Oncol. 1990;36(3):343–347. doi:10.1016/0090-8258(90)90139-C
6. Rizzo S, Calareso G, Maccagnoni S, et al. Pre-operative MR evaluation of features that indicate the need of adjuvant therapies in early stage cervical cancer patients. A single-centre experience. Eur J Radiol. 2014;83:858–864.
7. Zhang W, Zhang J, Yang J, et al. The role of magnetic resonance imaging in pretreatment evaluation of early-stage cervical cancer. Int J Gynecol Cancer. 2014;24:1292–1298. doi:10.1097/IGC.0000000000000169
8. Bipat S, Glas AS, van der Velden J, Zwinderman AH, Bossuyt PM, Stoker J. Computed tomography and magnetic resonance imaging in staging of uterine cervical carcinoma: a systematic review. Gynecol Oncol. 2003;91:59–66. doi:10.1016/S0090-8258(03)00409-8
9. Liu J, Li Y, Chen X, et al. Upregulation of miR-205 induces CHN1 expression, which is associated with the aggressive behaviour of cervical cancer cells and correlated with lymph node metastasis. BMC Cancer. 2020;20(1):1029. doi:10.1186/s12885-020-07478-w
10. Zhai Y, Bommer GT, Feng Y, Wiese AB, Fearon ER, Cho KR. Loss of estrogen receptor 1 enhances cervical cancer invasion. Am J Pathol. 2010;177(2):884–895. doi:10.2353/ajpath.2010.091166
11. Park Y, Baik S, Ho C, Lin CY, Chung SH. Progesterone receptor is a haploinsufficient tumor suppressor gene in cervical cancer. Mol Cancer Res. 2021;19(1):42–47. doi:10.1158/1541-7786.MCR-20-0704
12. Chung SH, Shin MK, Korach KS, Lambert PF. Requirement for stromal estrogen receptor alpha in cervical neoplasia. Horm Cancer. 2013;4(1):50–59. doi:10.1007/s12672-012-0125-7
13. Chen HH, Chen SP, Zheng QL, et al. Genistein promotes proliferation of human cervical cancer cells through estrogen receptor-mediated PI3K/Akt-NF-κB pathway. J Cancer. 2018;9:288–295. doi:10.7150/jca.20499
14. Zhang E, Zhang Y, Fan Z, Cheng L, Han S, Che H. Apigenin inhibits histamine-induced cervical cancer tumor growth by regulating estrogen receptor expression. Molecules. 2020;25(8):1960.
15. Pecorelli S, Zigliani L, Odicino F. Revised FIGO staging for carcinoma of the cervix. Int J Gynaecol Obstet. 2009;105(2):107–108. doi:10.1016/j.ijgo.2009.02.009
16. Hong MK, Wang JH, Su CC, Li MH, Hsu YH, Chu TY. Expression of estrogen and progesterone receptor in tumor stroma predicts favorable prognosis of cervical squamous cell carcinoma. Int J Gynecol Cancer. 2017;27(6):1247–1255. doi:10.1097/IGC.0000000000001004
17. Kwasniewska A, Postawski K, Gozdzicka-Jozefiak A, et al. Estrogen and progesterone receptor expression in HPV-positive and HPV-negative cervical carcinomas. Oncol Rep. 2011;26:153–160. doi:10.3892/or.2011.1256
18. den Boon JA, Pyeon D, Wang SS, et al. Molecular transitions from papillomavirus infection to cervical precancer and cancer: role of stromal estrogen receptor signaling. Proc Natl Acad Sci U S A. 2015;112(25):E3255–64. doi:10.1073/pnas.1509322112
19. Fan DM, Tian XY, Wang RF, Yu JJ. The prognosis significance of TGF-β1 and ER protein in cervical adenocarcinoma patients with stage Ib~IIa. Tumour Biol. 2014;35(11):11237–11242. doi:10.1007/s13277-014-2110-y
20. Zhang X, Zhang A, Zhang X, et al. ERa-36 instead of ERa mediates the stimulatory effects of estrogen on the expression of viral oncogenes HPV E6/E7 and the malignant phenotypes in cervical cancer cells. Virus Res. 2021;306:198602. doi:10.1016/j.virusres.2021.198602
21. Zhang Q, Wu YZ, Zhang YM, Ji XH, Hao Q. Activation of G-protein coupled estrogen receptor inhibits the proliferation of cervical cancer cells via sustained activation of ERK1/2. Cell Biochem Funct. 2015;33(3):134–142. doi:10.1002/cbf.3097
22. Son J, Park JW, Lambert PF, Chung SH. Requirement of estrogen receptor alpha DNA-binding domain for HPV oncogene-induced cervical carcinogenesis in mice. Carcinogenesis. 2014;35(2):489–496. doi:10.1093/carcin/bgt350
23. Fan Q, Huang T, Sun X, et al. miR-130a-3p promotes cell proliferation and invasion by targeting estrogen receptor α and androgen receptor in cervical cancer. Exp Ther Med. 2021;21(5):414. doi:10.3892/etm.2021.9858
24. Baik S, Mehta FF, Chung SH. Medroxyprogesterone Acetate Prevention of Cervical Cancer through Progesterone Receptor in a Human Papillomavirus Transgenic Mouse Model. Am J Pathol. 2019;189(12):2459–2468. doi:10.1016/j.ajpath.2019.08.013
25. Wu Q, Shi D, Dou S, et al. Radiomics analysis of multiparametric MRI evaluates the pathological features of cervical squamous cell carcinoma. J Magn Reson Imaging. 2019;49(4):1141–1148. doi:10.1002/jmri.26301
26. Xiao M, Ma F, Li Y, et al. Multiparametric MRI-based radiomics nomogram for predicting lymph node metastasis in early-stage cervical cancer. J Magn Reson Imaging. 2020;52(3):885–896. doi:10.1002/jmri.27101
27. Yu YY, Zhang R, Dong RT, et al. Feasibility of an ADC-based radiomics model for predicting pelvic lymph node metastases in patients with stage IB-IIA cervical squamous cell carcinoma. Br J Radiol. 2019;92(1097):20180986. doi:10.1259/bjr.20180986
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.