")
Back to Journals » Research and Reports in Urology » Volume 12
Color Doppler Ultrasonography in Evaluating the Outcomes of Pyeloplasty in Ureteropelvic Junction Obstruction
Authors Hamedanchi S, Sedokani A
Received 13 August 2019
Accepted for publication 9 February 2020
Published 24 February 2020 Volume 2020:12 Pages 53—59
DOI https://doi.org/10.2147/RRU.S227046
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jan Colli
Sepehr Hamedanchi,1 Amin Sedokani2
1Urology & Nephrology Research Center, Department of Urology, Imam Medical Center, Urmia University of Medical Sciences, Urmia, Iran; 2Student Research Committee, Urmia University of Medical Sciences, Urmia, Iran
Correspondence: Amin Sedokani
Urmia University of Medical Sciences, Ershad Street, Urmia, West Azarbayjan, Iran
Tel +98 914 324 1375
Fax +098 443 345 7277
Email [email protected]
Purpose: To evaluate the accuracy of Color Doppler ultrasonography for diagnosing post pyeloplasty elimination of obstruction in Ureteropelvic Junction Obstruction patients.
Methodology: Patients with the diagnosis of UPJO enrolled in the study and underwent open pyeloplasty. Three to 6 months after the operation, patients were recalled and underwent isotope scan as the gold standard test and renal color Doppler ultrasonography to assess the success rate of pyeloplasty.
Results: A total of 39 patients were evaluated and analyzed. The average follow-up time for patients was 9.1 months. The success rate of surgery in the study population was 100%. The mean RI of the affected side before the operation was 0.69 ± 0.01 and after the pyeloplasty, it reached to 0.65 ± 0.01. The difference between the mean RI of the affected side before and after the operation is 0.04 (P < 0.001). Age, type and severity of obstruction and the technique of surgery did not have any impact on these parameters. The difference between the RI of the affected and healthy side was termed ΔRI. ΔRI before and after the operation was 0.084 and 0.014, respectively. The decrease of ΔRI in the case of pyeloplasty is 0.07 on average (P < 0.001), which can be predicted for pyeloplasty success.
Discussion: Color Doppler ultrasonography can be used as a non-invasive, fast, non-expensive, and available modality for evaluating the outcome of pyeloplasty instead of the nuclear scan or IVP.
Keywords: urogenital abnormality, ureteropelvic junction obstruction, pyeloplasty, color doppler ultrasonography, resistive index
Introduction
Ureteropelvic junction obstruction (UPJO) is the most common cause of childhood hydronephrosis with the prevalence of 0.05–0.1% and also most common cause of neonatal obstructive uropathy.1,2 Ultrasound examination of the kidneys and bladder is a safe and the preferred primary postnatal imaging not only for fetal hydronephrosis but also for detecting most of the Congenital anomalies of the kidney and urinary tract (CAKUT).3,4 With the aid of Color Doppler Ultrasonography (cDUS), we can evaluate the flow of the vessels in the kidney and calculate the Resistive Index (RI; that is calculated by (peak systolic velocity – end diastolic velocity)/peak systolic velocity) by the normal range of <0.7 that increases by obstruction;5 however, there are controversy on the sensitivity.6 Computed tomography (CT) scan is an alternative imaging in the symptomatic patient; but, it is not the choice modality because of radiation exposure. In UPJO, the CT scan shows hydronephrosis without a dilated ureter.7 Magnetic Resonance Imaging (MRI) is commonly used in children to role out UPJO. Contrast-enhanced MRI, can measure differential renal function and Renal Transient Time.8 Even in terms of decision-making for surgery, MRI has shown a sensitivity equivalent to the nuclear scan and higher attribute.9,10 In this study, our aim is to evaluate the accuracy and sensitivity of Color Doppler ultrasonography as a cheap, available, non-invasive, and rapid modality for post-pyeloplastic evaluation of UPJO patients.
Materials and Methods
Population Study
Patients who referred to the urology clinic of Urmia Imam hospital, who were evaluated for renal hydronephrosis, enrolled in the study. In the complementary assessments, intravenous pyelogram (IVP), dynamic renal scans (diethylene triamine penta acetic acid [DTPA], ethylenedicysteine [EC], or mercapto acetyl tri glycine [MAG3]) and voiding cystourethrography (VCUG) were performed. All of the patients who have been nominated for pyeloplasty in an open surgical procedure were examined by routine paraclinical tests including complete blood count, prothrombin time, INR, partial thromboplastin time (PTT), blood urea nitrogen (BUN), creatinine, Na, K, urine analysis and urine culture after admission.
Exclusion Criteria
Patients with UPJO who have had a history of previous failed pyeloplasty, patients with renal anomalies including vascular anomalies, horseshoe and pelvic kidneys, obstructions secondary to the nephrolithiasis, tumor or abdominal mass, patients with surgery contraindication, including active urinary tract infections and uncorrected coagulopathy or severe comorbidity preventing anesthesia and patients who have no follow-up condition in terms of social culture and situations, delisted from the study.
RI has been measured with interlobar vascular flow and all ultrasonographies were taken by one expert radiologist by Toshiba nemio 30 with curve array probe 3.7–6 MHz.
Treatment and Follow Up
Patients underwent open pyeloplasty. The surgical technique was determined according to renal pelvic anatomy and stenosis length during operation. For all patients, ureteral and urethral catheters were inserted. Foley catheters were removed 24–36 hrs later and the patient was discharged on the second or third day of post-operation. Double J stents were removed 6 weeks after surgery. After 3 to 6 months of operation, patients were recalled and underwent isotope scan and renal color Doppler ultrasonography to assess the success rate of pyeloplasty. The ultrasound was again performed by the radiologist, and radiologist was blinded to the primary results. The results of a renal scan as gold standard determined the success rate of the pyeloplasty. The results of the color Doppler ultrasound compared with renal scan results.
Data Analysis
After collecting data, Kolmogorov–Smirnov’s nonparametric test was performed to determine the normality of the variables. In case of normalization, independent t-test was used for dual comparison and in case of non-normality, Mann–Whitney nonparametric test was used. Paired t-test was used to compare the effects of independent variables on RI. The significance level of all tests was considered to be 5%.
Ethics
This study was approved by the ethics committees of Imam Medical Center and Urmia University of Medical Sciences, and was conducted in accordance with the Declaration of Helsinki. After oral and written explanations all patients provided written informed consent. For any patient under the age of 18 years, a parent or legal guardian provided written informed consent. All patients had the opportunity to withdraw from the study at any time. Patient information remained confidential. Patients beared no costs for the evaluation with color Doppler ultrasonography or nuclear imaging.
Results
The number of patients enrolled in the study was 42, of whom 2 were missed in the next follow-up and one patient was excluded from the study due to the fact that she was pregnant during the follow-up period and did not undergo a nuclear scan. Therefore, a total of 39 patients were evaluated and analyzed.
The average follow-up time for patients was 9.1 months (range 3 to 18 months). The primary surgery success rate in the study population was 100% (in 2 weeks). A dynamic renal nuclear scan (as the gold standard method) was performed in the follow-up phase. It should be noted that the reported final success rate of the pyeloplasties was >95% (Table 1).
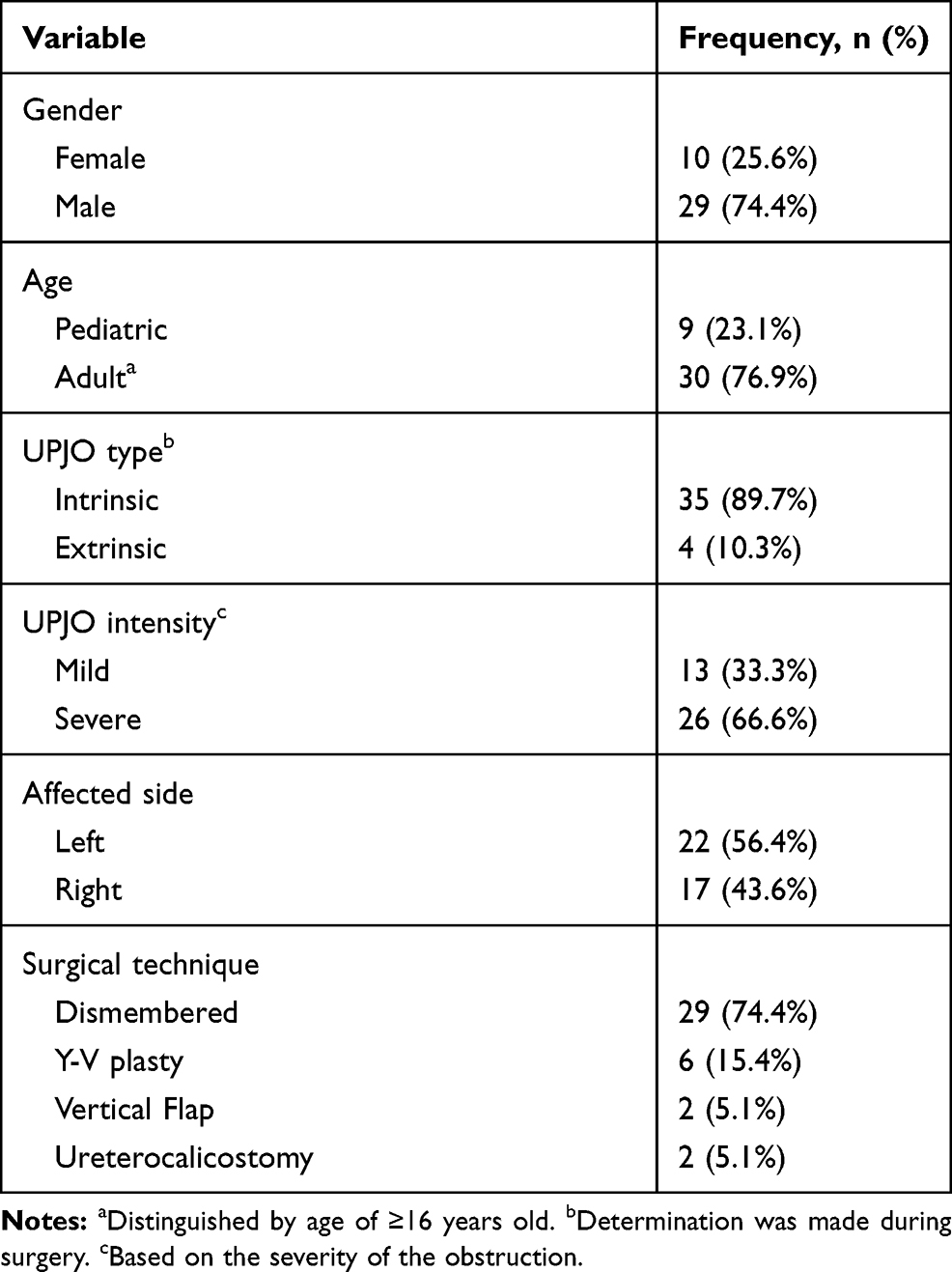 |
Table 1 Demographic Information and Variable Frequencies |
The difference between the RI of the affected and healthy side was termed ΔRI and was calculated by differing of before and after the operation values. The mean ΔRI before the operation was 0.084 with a range of 0–0.22 ± 0.008 which and after pyeloplasty, was 0.014 ± 0.003 (range 0–0.09). The difference between these two numbers was significant by P<0.001. The decrease of ΔRI in the case of pyeloplasty was 0.07 on average, which can be predicted the pyeloplasty success if the decrease is within the range (0.052–0.088) with a 95% confidence interval.
Affected Side
The mean RI of the affected side before the operation was 0.69 ± 0.01 (range 0.57–0.80) with a 95% confidence interval. The mean RI of the affected side after the pyeloplasty was 0.65 ± 0.01 (range 0.56–0.81). The difference between the mean RI of the affected side before and after the operation is 0.04 (P<0.001) which shows a significant difference between these two numbers, and it can be declared that the RI of affected side after pyeloplasty is decreased 0.04 on average. On the right UPJO: The mean of ΔRI before the operation was 0.08 ± 0.013 and after operation 0.014 ± 0.001, and the difference between these two numbers was significant with P<0.001. Also on the left UPJO, mean ΔRI before the operation was 0.087 ± 0.012 and after the operation was 0.014 ± 0.005 (with a mean difference of 0.073), which difference with P<0.001 is significant. In comparison of two sides, did not show a significant difference between them.
Gender
In the female group, the preoperative RI was 0.71 ± 0.01, which was reduced to 0.68 after the operation. This change was not significant (P=0.06). In the male group mean RI before the operation was 0.69, which decreased to 0.63 ± 0.009 after the operation which was significant (P <0.001). In the female group, the mean ΔRI before surgery was 0.091 ± 0.006, which after the operation was changed to 0.02 ± 0.009, which is equivalent to 0.071 in ΔRI. The difference between the data before and after the operation is significant with P<0.001. In the men’s group, the mean ΔRI before the operation was 0.082 ± 0.11, that after the operation was changed to 0.122 ± 0.014, which there is a significant difference between the two numbers by P<0.001. Analysis of ΔRI decreases in men and women showed a decrease of 0.071 in women and a decrease of 0.07 in men with a P=0.9 which means that the sex of the patient has no significant effect on the rate of ΔRI reduction following pyeloplasty.
Age
In children, the mean RI before and after surgery was 0.69 and 0.64 ± 0.02, and with P=0.01: this was a significant decrease in RI. In adults, the mean RI before surgery was 0.69 ± 0.01 and the follow up was 0.64 ± 0.01, which indicates a significant difference between the two scales. Therefore, it can be concluded that the patient’s age does not affect the outcome of the RI. On the other hand, in children, the mean ΔRI before surgery was 0.118 ± 0.025 and after the operation was 0.009 ± 0.003, the difference between them was significant (P=0.003). In adults, mean ΔRI before the operation was 0.074 ± 0.008 and after the operation changed to 0.016 ± 0.004 that P<0.001 showed a significant difference between the two numbers. In comparison of the two groups, the ΔRI changes in children were 0.109 and 0.058 in adults, and the difference between these two numbers is not significant with P=0.09.
UPJO Type
In the intrinsic types, the mean RI of the affected side was 0.69 before surgery, and 0.64 ± 0.009 after the operation, and with respect to P <0.001, this change was significant in RI. In extrinsic types, the mean RI before surgery was 0.67 ± 0.05, which was the same after the operation, but due to the small number of samples (4 cases), statistical analysis was not possible. In the intrinsic types, the mean ΔRI before the operation was 0.086 ± 0.009 and after the operation was 0.012 ± 0.002 and in extrinsic types, the mean ΔRI before the operation was 0.065 ± 0.009), which after the pyeloplasty, reached 0.033 ± 0.021, with an average drop of 0.032. However, statistical analysis was not feasible due to the small sample size.
UPJO Intensity
In mild types, the mean RI before the operation was 0.69 ± 0.02 and after the operation, it was changed to 0.64 ± 0.02. Also in severe UPJO types, the mean RI before and after the operation was 0.69 ± 0.01 and 0.65 ± 0.01, respectively, which both were significant with P<0.001. In mild types, the mean ΔRI before the operation was 0.082 ± 0.018 and after the operation was 0.006 ± 0.002 which P<0.001 showed a significant difference between the two numbers. In severe types, the mean ΔRI before and after the operation was 0.085 ± 0.009 and 0.018 ± 0.004 that is significant with P<0.001. Comparing the changes in ΔRI in these two groups showed, the mean ΔRI reduction in the mild group following the pyeloplasty was 0.076 and in the severe group was 0.067, which were not significant (P=0.7). Therefore, the UPJO intensity has no effect on the amount of ΔRI changes following pyeloplasty.
Pyeloplasty Technique
In the dismembered technique, the mean of RI before and after surgery was 0.7 ± 0.01 and 0.65 ± 0.01 after surgery, which is significant with P<0.001. In the Y-V plasty technique, the mean RI before and after surgery was 0.72 ± 0.009 and 0.69 ± 0.009 after surgery. In the vertical Flap method, the mean RI before and after surgery was 0.69 ± 0.03 and 0.6 ± 0.03. In the ureterocalicostomy method, the mean RI before and after the operation was 0.57 ± 0.02 and 0.56 ± 0.02. There were no statistical analyzes in the last three techniques due to the low sample size; however, there seems to be no significant reduction in RI after surgery in the ureterocalicostomy technique. In the dismembered technique, the mean ΔRI before surgery was, 0.083 ± 0.01 and after the operation was 0.019 ± 0.003, which is significant with P<0.001. In the Y-V plasty technique, the mean ΔRI before and after the operation was 0.087 ± 0.004 and 0.02 ± 0.006, respectively, which with P<0.001 indicated a significant difference between the two numbers. In the Vertical Flap technique, the mean ΔRI before surgery was 0.16 and after the operation was zero. In the ureterocalicostomy technique, the mean ΔRI before surgery was 0.02 and after the operation was 0.02. The vertical Flap and ureterocalicostomy technique techniques were not statistically analyzable because of the small number of samples (Figure 1).
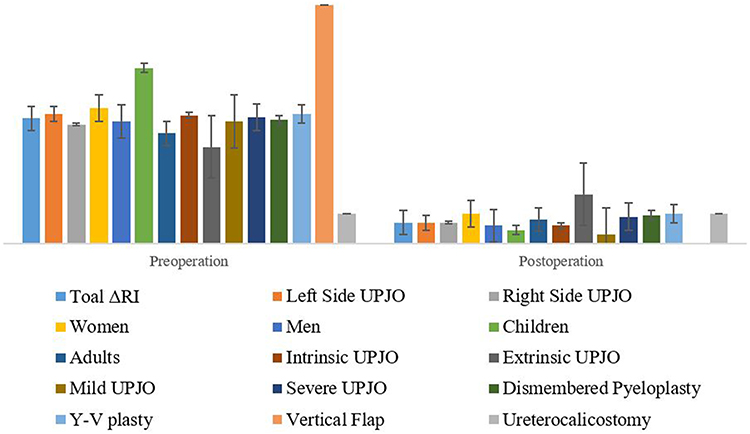 |
Figure 1 The comparison of pre- and post-operation resistive index changes (ΔRI) based on the affected side, age, sex, UPJO type, and intensity and pyeloplasty technique. |
Non-Affected Side
In non-affected side evaluation, we found that the mean RI before the operation was 0.61 (range 0.52–0.75), which has increased to 0.63 after pyeloplasty of the opposite side. (range 0.54–0.76). According to statistical analyze P-value was equal to 0.02 suggesting a significant difference between the two numbers (Figure 2).
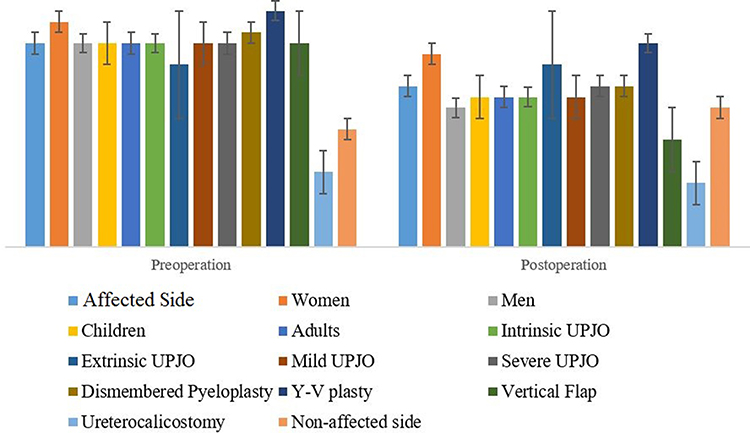 |
Figure 2 The comparison of pre- and post-operation resistive index (RI) based on the affected side, age, sex, UPJO type, and intensity and pyeloplasty technique. |
Discussion
UPJO is the most common cause of childhood hydronephrosis and obstructive uropathy.–2 In UPJO, intra-pelvic pressure increases, the pelvis dilates, and if this continues, gradual dilatation of renal tubules will lead to glomerulosclerosis, inflammation, fibrosis, cortex atrophy and reduction of GFR. After relief of the obstruction, destruction process will stop and the function of tubules and glomeruli improves.11 Open pyeloplasty is a standard method of UPJO treatment. According to available statistics, the success rate of pyeloplasty is more than 90–95%.12 Routine follow-up technique after the pyeloplasty is performing an ultrasound 6 weeks after surgery and by nuclear scan or IVP, 3 months after surgery. Further follow-ups are recommended by performing ultrasonography for 12 to 24 months after surgery, and in the case of no clinical symptoms, there will be no need for further examinations.13 Since IVP and renal scans have problems like high cost, radioactivity exposure, nephrotoxicity and allergic reaction, the idea of using a color Doppler ultrasound as a non-invasive, affordable, quick and available modality to examine the level of UPJ obstruction and evaluate the success of pyeloplasty was introduced.
In pre-operative and post-pyeloplastic RI assessment, our data indicated that the pre-operative mean RI of 0.69, with a confidence level of 95%, in the range of 0.67 to 0.71, suggests the presence of urinary obstruction. After the pyeloplasty, this rate dropped to 0.65, indicating a significant change in RI with P<0.001. According to previous studies, RI <0.7 is a sign of non-obstructive hydronephrosis,14 which our findings are consistent with them, but obstruction RI was considered to be RI ≥0.7 in previous studies, which is 0.67 in our study. When comparing pre and post-operative RI and effect of different variables on that, it was found that age, type of UPJO and surgical techniques have no significant effect on the results of RI. However, there was no significant difference in the RI of pre- and post-operation in the women group comparing to the men. This difference was significant in men, so it seems that RI is not a valid criterion for assessing urinary obstruction in women. Of course, to prove such a claim, there is a need for more cases, because it should be noted that the number of women in our study was only 10. Such a difference has not been reported in previous studies.
According to some of the in-vivo studies, RI only increases in acute and in complete ureteral obstruction.15,16 Therefore, according to the previous studies, there should be no significant difference in the RI, but our results concluded against this issue. RI assessment of contralateral intact kidney revealed that increasing of RI in normal kidney after pyeloplasty in the opposite side is significant and previous studies conformed this finding.17 So the question is why the RI changes significantly over time, without any manipulation in the healthy kidney, and does not this invalidate the results of RI in the pyeloplasty side? It seems we need to use a scale that compares both kidneys rather than merely a one-way examination, and that scale is ΔRI. In ΔRI assessment pre and post-operation, there was a highly significant decrease after pyeloplasty in mean ΔRI. Some studies have reported such a decrease17 and some others have not.15 On the evaluation of ΔRI changes, it was determined that the gender, the affected side, the grade of obstruction and the technique of pyeloplasty are not effective factors to change ΔRI after the pyeloplasty. However, there is two important points to mention: 1. In the comparison of the age group of pediatric patients and adults, ΔRI changes after pyeloplasty are not significant, so the age factor is not effective on ΔRI. Thus, maybe with larger sample size, we can declare that the ΔRI decrease in the pediatric group may be more significant. It should be noted that previous studies have suggested that RI is higher in all children less than 1 year old than in adults.18 2. The mean ΔRI in extrinsic UPJO after pyeloplasty, had a decrease of 0.032, but it was not statistically significant due to the small number of extrinsic UPJO samples (4 cases). But it seems to be much lower than the mean reduction of ΔRI (0.07). Therefore, it may be hypothesized that in extrinsic UPJOs, after pyeloplasty, the ΔRI reduction is less than what is expected. ΔRI do not depend on any of the underlying variables including age, sex, affected side, UPJO severity and type, and surgical technique. However, in the pediatric age group, ΔRI reduction may be more obvious after pyeloplasty. Considering all evidence, we recommend color Doppler ultrasonography to post-surgery evaluation of UPJO. However, more extended studies with greater study populations can be more accurate to redecide about post-surgery patient follow-ups.
Conclusion
Color Doppler ultrasonography can be used as a non-invasive, fast, non-expensive, and available modality for evaluating the outcome of pyeloplasty instead of the nuclear scan or IVP.
Disclosure
The authors report no conflicts of interest in this work.
References
1. King LR, Coughlin PW, Bloch EC, Bowie JD, Ansong K, Hanna MK. The case for immediate pyeloplasty in the neonate with ureteropelvic junction obstruction. J Urol. 1984;132(4):725–728. doi:10.1016/S0022-5347(17)49843-0
2. Thomas DF, Gordon AC. Management of prenatally diagnosed uropathies. Arch Dis Child. 1989;64(1Spec No):58–63. doi:10.1136/adc.64.1_Spec_No.58
3. Dias CS, Silva JM, Pereira AK, et al. Diagnostic accuracy of renal pelvic dilatation for detecting surgically managed ureteropelvic junction obstruction. J Urol. 2013;190(2):661–666. doi:10.1016/j.juro.2013.02.014
4. Coplen DE, Austin PF, Yan Y, Blanco VM, Dicke JM. The magnitude of fetal renal pelvic dilatation can identify obstructive postnatal hydronephrosis, and direct postnatal evaluation and management. J Urol. 2006;176(2):
5. Gilbert R, Garra B, Gibbons MD. Renal duplex doppler ultrasound: an adjunct in the evaluation of hydronephrosis in the child. J Urol. 1993;150(4):1192–1194. doi:10.1016/S0022-5347(17)35723-3
6. Ordorica RC, Lindfors KK, Palmer JM. Diuretic doppler sonography following successful repair of renal obstruction in children. J Urol. 1993;150(2 Pt 2):774–777. doi:10.1016/S0022-5347(17)35611-2
7. Baskin LS, Basow D. Congenital Ureteropelvic Junction Obstruction. Waltham, MA: UpToDate; 2013.
8. Jones RA, Perez-Brayfield MR, Kirsch AJ, Grattan-Smith JD. Renal transit time with MR urography in children. Radiology. 2004;233(1):41–50. doi:10.1148/radiol.2331031117
9. Grattan-Smith JD, Perez-Bayfield MR, Jones RA, et al. MR imaging of kidneys: functional evaluation using F-15 perfusion imaging. Pediatr Radiol. 2003;33(5):293–304. doi:10.1007/s00247-003-0896-7
10. Pedersen M, Wen JG, Shi Y, et al. The effect of unilateral ureteral obstruction on renal function in pigs measured by diffusion-weighted MRI. APMIS Suppl. 2003;109:29–34.
11. Douville E, Hollinshead WH. The blood supply of the normal renal pelvis. J Urol. 1955;73(6):906–912. doi:10.1016/S0022-5347(17)67498-6
12. Casale P, Grady RW, Joyner BD, Zeltser IS, Figueroa TE, Mitchell ME. Comparison of dismembered and nondismembered laparoscopic pyeloplasty in the pediatric patient. J Endourol. 2004;18(9):875–878. doi:10.1089/end.2004.18.875
13. Cost GA, Merguerian PA, Cheerasarn SP, Shortliffe LM. Sonographic renal parenchymal and pelvicaliceal areas: new quantitative parameters for renal sonographic followup. J Urol. 1996;156(2 Pt 2):725–729. doi:10.1016/S0022-5347(01)65798-7
14. Lim GY, Jang HS, Lee EJ, et al. Utility of the resistance index ratio in differentiating obstructive from nonobstructive hydronephrosis in children. J Clin Ultrasound. 1999;27(4):187–193. doi:10.1002/(ISSN)1097-0096
15. Coley BD, Arellano RS, Talner LB, Baker KG, Peterson T, Mattrey RF. Renal resistive index in experimental partial and complete ureteral obstruction. Acad Radiol. 1995;2(5):373–378. doi:10.1016/S1076-6332(05)80337-X
16. Brkljacic B, Kuzmic AC, Dmitrovic R, Rados M, Vidjak V. Doppler sonographic renal resistance index and resistance index ratio in children and adolescents with unilateral hydronephrosis. Eur Radiol. 2002;12(11):2747–2751. doi:10.1007/s00330-001-1259-0
17. Kessler RM, Quevedo H, Lankau CA, et al. Obstructive vs nonobstructive dilatation of the renal collecting system in children: distinction with duplex sonography. AJR Am J Roentgenol. 1993;160(2):353–357. doi:10.2214/ajr.160.2.8424349
18. Vrtal R, Vrana J, Utikalova A. Doppler ultrasonography in evaluation of renal hemodynamics in hydronephrosis in children. Acta Univ Palacki Olomuc Fac Med. 1996;140:73–75.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.