")
Back to Journals » Patient Preference and Adherence » Volume 13
Cognition and drug adherence to oral hypoglycemic and antihypertensive agents in older adults
Authors Bakouni H, Gentil L , Vasiliadis HM
Received 23 November 2018
Accepted for publication 21 March 2019
Published 30 May 2019 Volume 2019:13 Pages 891—899
DOI https://doi.org/10.2147/PPA.S195756
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Hamzah Bakouni,1,2 Lia Gentil,3 Helen-Maria Vasiliadis1–2,4
1Faculty of Medicine and Health Sciences, Université de Sherbrooke, Sherbrooke, Quebec, Canada; 2Centre de recherche Charles-Le Moyne – Saguenay–Lac-Saint-Jean sur les innovations en santé (CR-CSIS), Greenfield Park, Quebec, Canada; 3Douglas Mental Health University Institute, McGill University, Montreal, Quebec, Canada; 4Department of Community Health Sciences, Faculty of Medicine and Health Sciences, Université de Sherbrooke, Sherbrooke, Quebec, Canada
Background and objectives: Chronic disorders such as diabetes mellitus type II and hypertension have been associated with cognitive decline in older adults. It is unclear whether adherence to antihypertensive and oral hypoglycemic agents impact cognitive health. The objectives are to study the association between adherence to antihypertensive and oral hypoglycemic agents and cognitive status in community-living older adults.
Methods: We used data from a large representative sample of older adults (N=2,286) covered under a public drug insurance plan in Quebec and participating in Quebec’s health survey on older adults (ESA-study) with a Mini-Mental State Examination (MMSE) score ≥22 at baseline (T1) and examined one year later (T2). Participants with hypertension and diabetes mellitus type II were identified according to criteria used in the Canadian Chronic Disease Surveillance System. Antihypertensive and oral hypoglycemic prescriptions delivered were ascertained via Quebec’s pharmaceutical database (RAMQ). Medication adherence was calculated using the medication possession ratio as a continuous variable in the year prior to and following baseline interview. Multivariate linear regressions were used to study the percentage change in MMSE scores between interviews (T1,T2) as a function of adherence to antihypertensive and oral hypoglycemic agents (before and after T1) controlling for potential confounders.
Results: In participants with diabetes mellitus type II only, adherence to oral hypoglycemics was not associated with a change in MMSE scores. In participants with hypertension only, the change in MMSE scores was associated with adherence to antihypertensives (β 1.23; 95%CI: 0.29–2.17). In participants with comorbid hypertension and diabetes mellitus type II, the change in MMSE scores was associated with adherence to both antihypertensive and oral hypoglycemic agents (β 0.75; 95%CI: 0.01–1.48).
Conclusions: Adherence to oral hypoglycemic agents and antihypertensive agents among older adults with hypertension and comorbid diabetes mellitus type II can have a preserving effect on cognitive health in older adults. Further research on the long-term impact on cognition is recommended.
Keywords: diabetes mellitus type II, hypertension, cognition, medication adherence, oral hypoglycemic agents
Corrigendum for this paper has been published
Introduction
Cognitive decline and dementia are associated with an important economic and societal burden.1,2 Many have identified modifiable lifestyle risk factors3,4 and chronic medical conditions as probable causes.5,6 In Canada, hypertension and diabetes mellitus type II are the most common chronic disorders with a prevalence reaching up to 50% and 20% among older adults.7–9 Also of great concern, up to 75% of older adults with diabetes mellitus type II have concomitant hypertension.10
Recent population-based prospective studies in older adults have shown an association between cognitive health and diabetes,11–13 and hypertension.14–17 Diabetes mellitus type II has been associated with elevated blood cholesterol and increased β-amyloid accumulation,6 which in turn may negatively influence cognition. Hypertension leading to cerebral ischemia has also been associated with cognitive decline.13,18,19 An earlier prospective study also reported an increased risk of cognitive decline with the presence of comorbid diabetes and hypertension in older adults.20
Oral hypoglycemic agents represent first-line treatment for reaching satisfactory blood glycemic control in diabetes mellitus type II patients.21,22 In a large prospective study, poor control of glycated hemoglobin A1c levels (≥7%) in diabetic middle-aged and older adults was associated with cognitive decline over a 20 year period.23 Earlier smaller clinical studies, however, did not find evidence of an association between glycemic control in diabetic patients and cognition.24,25 Studies on the impact of antihypertensive agents on cognition have also shown inconsistent results. Some clinical studies have shown a positive effect of antihypertensive agents on cognition,26–28 while others have not.29,30
This study aims to evaluate the association between cognitive change during a one-year period and adherence to antihypertensive drugs and oral hypoglycemics in a large representative sample of community-living older adults. Associations will be verified in three mutually exclusive groups. Older adults with hypertension only, diabetes only and comorbid hypertension and diabetes. This study adds to the present literature by using health survey and health administrative data which limits the potential for information and recall bias and allows the control for a number of potential confounding clinical factors and the control of comorbid hypertension and diabetes. The hypothesis is that patient’s adherence to oral antihypertensive and oral hypoglycemic agents will protect against cognitive decline in a sample of older adults not presenting with important cognitive problems.
Methods
Data came from Quebec’s longitudinal survey on seniors’ health (ESA, Enquête sur la Santé des Ainés) conducted between 2005 and 2008 (N=2,811) using a probabilistic sample of Francophone community-living older adults. Participants residing in the northern regions representing 10% of the provinces’ population were excluded due to feasibility issues. The sampling method of the ESA study has been presented elsewhere.31 Close to 77% of those contacted have participated in the ESA study. Analyses showed no statistically significant difference between participants and nonparticipants concerning sociodemographic factors such as age, gender and region.
All participants gave written informed consent to participate in the study. Participants also gave written consent permitting the research team to access their health and pharmaceutical services data from the Régie d’Assurance-Maladie du Québec (RAMQ) and the health ministry’s database on hospitalizations (MED-ECHO) for a 2-year follow-up period, including one year prior to and one year following baseline interview. Health survey data were collected during a face-to-face at-home interview conducted by trained health professionals. Older adults scoring <22 on the MiniMental State Examination (MMSE), suggesting cognitive impairment, were excluded (N=27).32 Among the 2,494 eligible participants, N=2,286 (91.5%) were covered under the province’s public drug insurance plan for whom prescription drug information was available. Among these participants, N=2,004 (80.3%) were available for a follow-up interview one year later and constituted the analytic sample.
Study sample
Participants in the ESA study with hypertension and diabetes mellitus type II were defined using National Diabetes Surveillance System criteria for diabetes and hypertension respectively.33,34 The minimum requirement for such a diagnosis, that is hypertension or type II diabetes, was at least one related hospitalization or two physician claims according to administrative data during the 2-year period. Thus, for hypertension, we used the International Classification of Diseases, ninth revision (ICD-9) codes: 401–405 and the International Classification of Diseases, tenth version (ICD-10): I10–I11. For a diagnosis of diabetes, we included the (ICD-9) codes of 250 and the (ICD-10) codes of E11–E14 in the year prior to and following baseline interview.
In this study, 966 participants diagnosed with hypertension also received an antihypertensive drug, of which N=40 received only one prescription during the 2-year follow-up period and were excluded from the analyses. Also, 358 participants were diagnosed with diabetes mellitus type II among which N=313 were taking oral hypoglycemic agents alone without insulin during the 2-year follow-up period. Participants who did not receive at least two consecutive prescriptions of oral hypoglycemic agents (N=4) were excluded. In addition, participants who switched to insulin (N=8) were also excluded. The presence of an antihypertensive and oral hypoglycemic agents delivered was ascertained from the RAMQ pharmaceutical database using the medication common identification number of American Hospital Formulary Service (AHFS) classification.16
The final analytical sample consisted of N=809 participants with hypertension and no diabetes, and n=184 participants with diabetes mellitus type II with no hypertension, and N=117 participants with comorbid hypertension and diabetes mellitus type II.
Measures
Cognitive status
Cognitive status was assessed using the MMSE score at baseline (T1) and at the one-year follow-up (T2). We used the difference of MMSE scores between T1 and T2, in order to prospectively quantify the change in cognitive status among participants. This change in MMSE scores observed at T1 and T2 was calculated as the percentage change in MMSE scores, that is: [(T2−T1)/(T1)] ×100%. The MMSE is a valid and reliable measure in assessing cognitive decline in older adults. In fact, the Cronbach’s α is estimated at 0.91 in older adult populations.35
Medication adherence
Medication adherence was measured using the medication possession ratio.36 The medication possession ratio (%) was calculated as the total day's supply of a medication divided by the number of days in the evaluation period, multiplied by one hundred: ([total day’s supply of medication/number of days in evaluation period] ×100). The medication possession ratio was calculated for the year prior and the year following baseline interview and studied as two continuous variables (0–100%) for each drug type. The medication possession ratio was also truncated and capped at 100%. In the subsample of participants filling the criteria for comorbid hypertension and diabetes mellitus type II, we calculated medication possession ratio for both antihypertensive and oral hypoglycemic agents. This medication possession ratio was then summarized into one dichotomous variable (Yes/No) based on whether the medication possession ratio was ≥80% for both drugs in the year prior to T1 and then in the year following T1.37,38 Finally, we considered only participants that were persistent to treatment. The nonpersistence to oral hypoglycemic and antihypertensive agents was identified as the presence of a continuous gap of 30 or more days between an expected refill and the actual refill.37
We also considered potential variables which might affect cognition in older adults as possible confounding factors. The following baseline interview (T1) factors were considered: age (65–74 vs ≥75 years); sex (female vs male); marital status (married or living as a couple vs single/separated/divorced/widowed); education level (primary/secondary vs post-secondary/university), Charlson comorbidity index (measured as a continuous variable);39 the self-reported presence of a probable (major and minor) depressive and/or anxiety disorder based on Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria,31 and the presence of antidepressant and benzodiazepine drug use. The research study was approved by the ethics committee of the University Institute of Geriatrics of Sherbrooke.
Analyses
Multivariate linear regression models were used to study the percent change in MMSE scores between T1 and T2 as a function of (1) adherence to antihypertensive agents in participants with hypertension only; (ii) adherence to oral hypoglycemic agents in participants with diabetes only, and; (iii) adherence to both antihypertensive and oral hypoglycemic agents in participants with both diabetes and hypertension. Additional analyses were also carried out focusing on adherence to metformin. The adjusted unstandardized beta-values (β) and their 95%CIs are presented and used as a measure of association. IBM SPSS Statistics (version 25; IBM Corporation, Armonk, NY, USA) was used for all statistical analyses.40
Results
When comparing those lost to follow-up from those who remained in the study, no significant difference was observed regarding age (P=0.77), sex (P=0.93), marital status (P=0.15) and the probable presence of depression (P=0.38) and anxiety (P=0.47) at baseline interview (T1). The study sample characteristics are presented in Table 1.
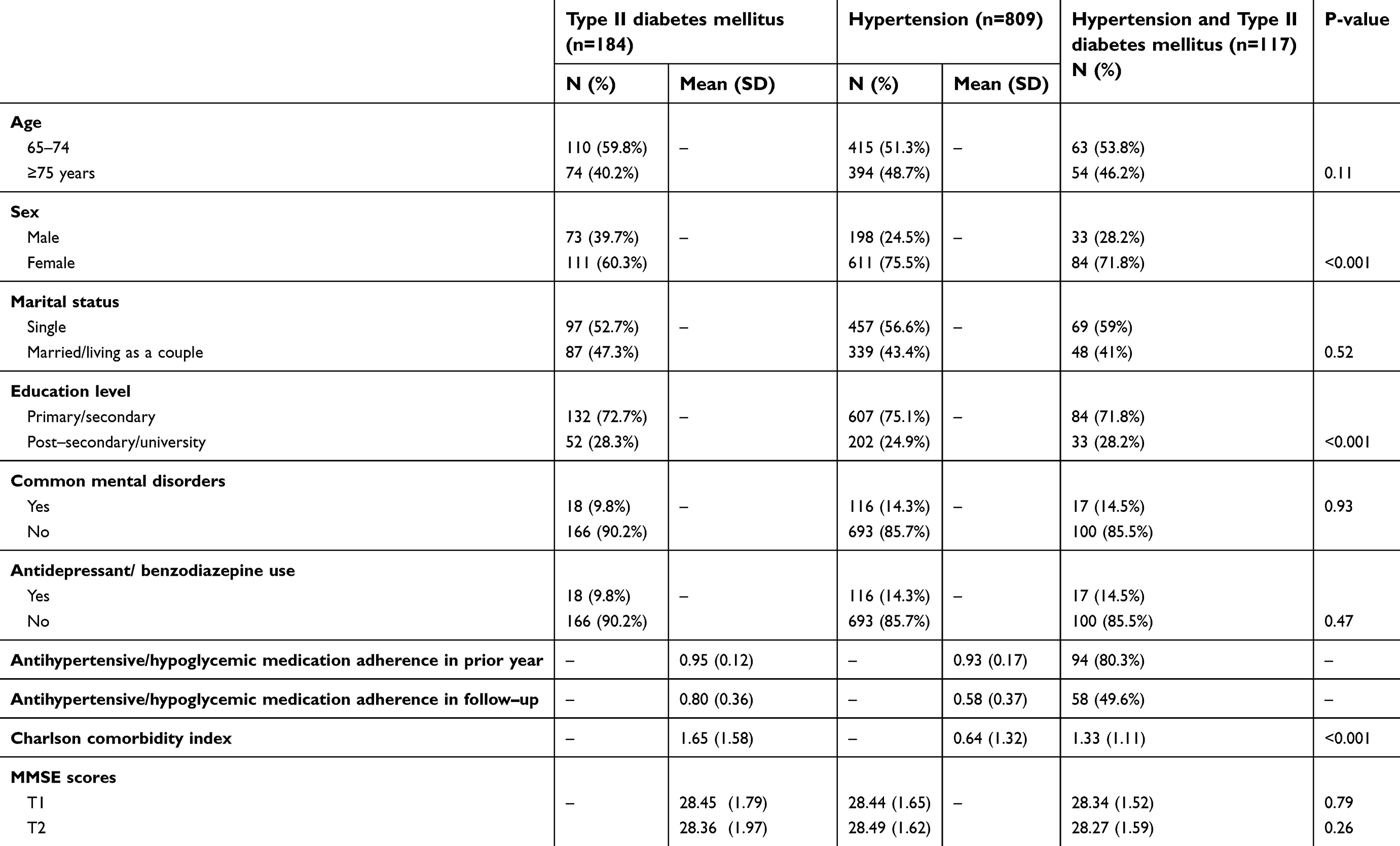 | Table 1. Sociodemographic and clinical variables description at baseline (T1) of study sample |
The multivariate analyses are presented in Table 2. In participants with only diabetes mellitus type II, no significant association between change in MMSE scores and adherence to oral hypoglycemic agents was observed. Additional analyses focusing specifically on adherence to Metformin did not show a significant association with change in MMSE scores. Among the variables studied, females had on average a lower decline in MMSE scores than males (β: 2.91; 95%CI: 0.71, 5.11) and those with a common mental disorder had a significant decline in MMSE scores (= β: −3.49; 95%CI: −6.46, −0.53) than those reporting no common mental disorders.
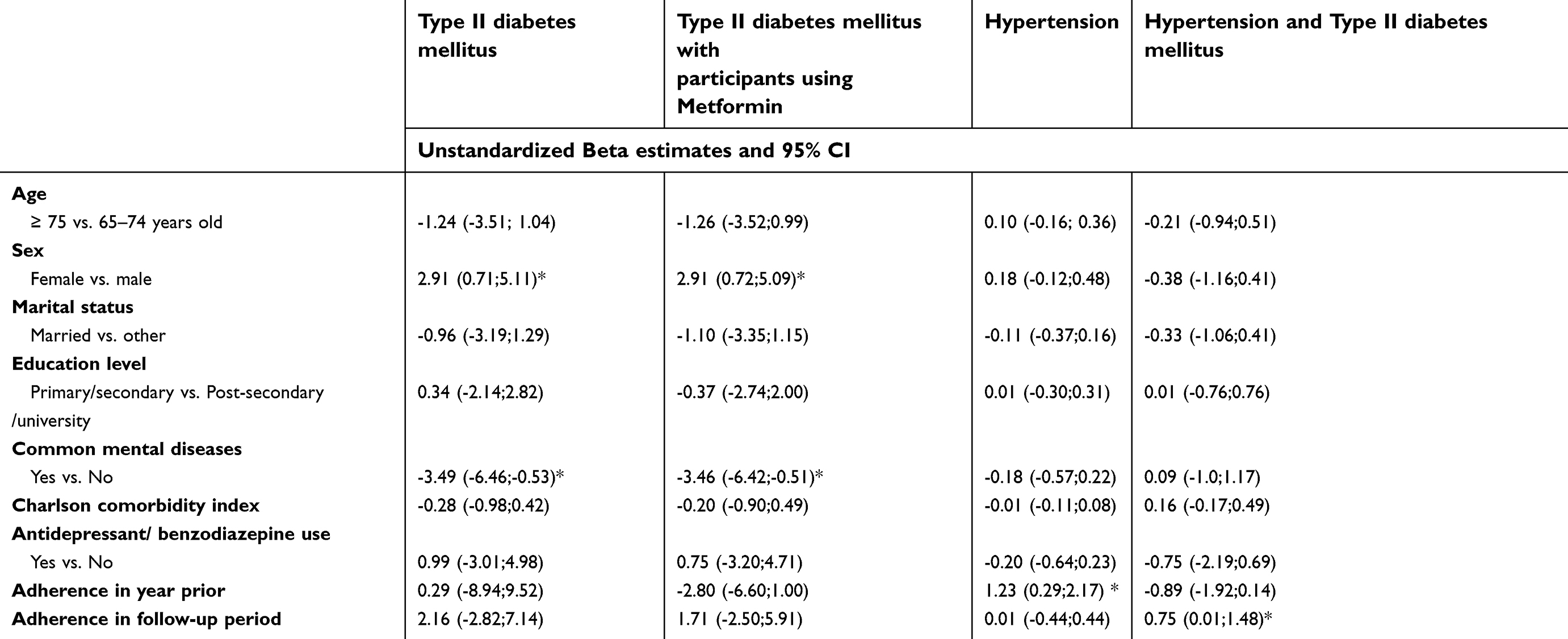 | Table 2. Multivariate linear regression analyses studying change in Mini-Mental State Examination scores and study variables estimates |
In the sample with hypertension, the change in cognitive status was positively associated with adherence to antihypertensive agents taken in the year prior to baseline interview 1.23; 95%CI: 0.29, 2.17). No other study variable was associated with change in cognitive status in participants with hypertension.
In the sample including participants diagnosed with both hypertension and diabetes mellitus type II, the change in MMSE scores was positively associated with adherence to both antihypertensive and oral hypoglycemic agents in the year following the baseline interview (β: 0.75; 95%CI: 0.01, 1.48). No other study variable was associated with change in MMSE scores.
Discussion
To our knowledge, this is the first study evaluating the association between change in cognitive function measured with MMSE and adherence to antihypertensive and oral hypoglycemic agents in a representative sample of community-living older adults.
Earlier studies have shown that diabetes is associated with cognitive decline in older adults.9,41 In our study, no significant association was observed between adherence to oral hypoglycemic agents and change in cognitive status. In the Herath et al (2016) study no association was observed between the use of oral hypoglycemic agents and the change in cognitive status measured with a series of neurological cognitive tests over a 4-year period.42 The study however did show better memory and verbal capacity associated with the use of metformin at baseline.42 In our study, no significant change in cognitive status was observed with metformin adherence. The results seem to suggest a preservation of cognition with adherence to oral hypoglycemic agents. The lack of association in our study may also in part be due to the fact that the sample included participants without cognitive impairment, which usually have a relatively slow rate of cognitive decline.43 Further research is recommended to elucidate the long-term impact of adherence to oral hypoglycemic agents on cognition in older adults.
In participants with diabetes only, females as opposed to males did not show cognitive decline. Sociodemographic factors have been associated with cognitive status but not with its change in a previous study conducted among older adults.9 Further, the presence of a common mental disorder such as anxiety or depression at baseline was associated with cognitive decline during the one-year follow-up. Similarly, Potvin et al (2011) also reported a negative association between cognitive functioning and common mental disorders.44 A review conducted by Thomas et al (2008) reported neurocognitive problems lasting beyond recovery from depression in older adults, which also increases the risk of cognitive decline.45
In participants with hypertension, adherence to antihypertensive agents had a positive and preserving effect on cognition measured with the MMSE. Secondary data analyses of a prospective study conducted by Yasar et al (2013) showed a decreased risk of Alzheimer’s dementia in older adults aged ≥75 years, with normal cognition at baseline, receiving antihypertensive agents over a median of 6 years.46 Guimaraes et al (2015) similarly reported that the presence of a caregiver assisting in antihypertensive administration, a proxy measure for drug adherence, was associated with better MMSE scores in hypertensive older adults.47 Others have also shown a preserving effect on cognitive functioning with the use of antihypertensive agents in those with mild cognitive problems.48
This study also showed improved cognitive status in participants with comorbid hypertension and diabetes adhering to both oral antihypertensive and hypoglycemic agents, which might reflect a positive additive effect on cognition. While adherence to antihypertensive agents in the previous year had a positive effect on cognition in hypertensive older adults, this effect was not significant in the comorbid diabetes and hypertension group. This could reflect the importance of a continued adherence regimen to both hypertensive and oral hypoglycemic agents in patients with comorbid diabetes and hypertension.
Limitations
The results of this study should be considered while deliberating the following limitations. First, the one year follow-up period may not be sufficient to observe a change in cognitive status due to adherence to oral antihypertensive and hypoglycemic agents. Second, the presence of diabetes and hypertension was ascertained from administrative databases which may be subject to information bias due to missing or inaccurate disease codes. There was no available patient data on participant glucose and glycated hemoglobin (HbA1c) levels and thus the clinical profile and severity of diabetic patients was unknown. In addition, severe cases of diabetic patients using insulin were excluded from our study and this might have weakened the strength of the association between adherence to hypoglycemic medication and change in cognitive status. In fact, other authors have reported more important cognitive decline in insulin-dependent diabetic patients in comparison with other diabetic patients.49,50 Third, the results may have been subject to a possible selection bias that may be difficult to predict. Those lost to follow-up had scored lower on the MMSE at baseline in comparison with study participants. There was no difference however in medication adherence between those lost to follow-up and the study sample. Fourth, it is possible that participants discontinued use of their drugs on the advice of their doctors. The definition of adherence was based on administrative data and therefore we could not distinguish participant nonadherence from cancellation of medication by physician. This may have introduced information bias that may have underestimated adherence. Adherence was also based on data from the RAMQ pharmaceutical drug database which captures the deliverance of a prescription and not the consumption of a drug. Nevertheless, administrative databases have been reported to be reliable at evaluating drugs for long-term therapy.51–53 Fifth, drug classes, aside from metformin, were not considered in the analyses as more than 50% of participants used one class of antihypertensive and hypoglycemic medications. Sixth, the medication possession ratio based on refill information may overestimate adherence. In this study we caped adherence to 100% to limit this bias. The medication possession ratio has also been recommended for evaluating adherence with hypertension therapy.54,55 Seventh, the study results did not include populations living in northern regions of the province. These populations have a higher prevalence of chronic disorders and their access to health services may be limited. The results of this study may therefore not apply.56,57
Conclusion
Adherence to oral antihypertensive and hypoglycemic agents in older adults with diabetes and hypertension can improve cognitive outcomes. Targeted public health programs are recommended to raise awareness about the negative cognitive effects of nonadherence to treatment with antihypertensive and oral hypoglycemic agents.
Acknowledgments
The ESA study was supported by the Canadian Institute of Health Research (CIHR) operating grant (200403MOP) and a Quebec Health Research fund—Fonds de Recherche Quebec—Santé (FRQS) grant (ref: 9854 and ref: 22251).
Dr Bakouni holds a PhD scholarship from Sherbrooke University. Dr Vasiliadis is a senior research scholar with the FRQ-S. Sponsors had no role in the design, methods, subject recruitment, data collections, analysis and preparation of paper.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Black SE, Gauthier S, Dalziel W, et al. Canadian Alzheimer‘s disease caregiver survey: baby-boomer caregivers and burden of care. Int J Geriatr Psychiatry. 2010;25(8):807–813. doi:10.1002/gps.2421
2. Wimo A, Guerchet M, Ali GC, et al. The worldwide costs of dementia 2015 and comparisons with 2010. Alzheimers Dement. 2016:S1552–5260. (16):30043–47. doi:10.1016/j.jalz.2016.07.150
3. Norton S, Matthews FE, Barnes DE, Yaffe K, Brayne C. Potential for primary prevention of Alzheimer’s disease: an analysis of population-based data. Lancet Neurol. 2014;13:788–794. doi:10.1016/S1474-4422(14)70136-X
4. Beydoun MA, Beydoun HA, Gamaldo AA, Teel A, Zonderman AB, Wang Y. Epidemiologic studies of modifiable factors associated with cognition and dementia: systematic review and meta-analysis. BMC Public Health. 2014;14:643. doi:10.1186/1471-2458-14-643
5. Baumgart M, Snyder H, Carrillo M, Fazio S, Kim H, Johns H. Summary of the evidence on modifiable risk factors for cognitive decline and dementia: a population-based perspective. Alzheimers Dement. 2015;11(6):718–726. doi:10.1016/j.jalz.2015.05.016
6. Dar TA, Sheikh IA, Ganie SA, et al. Molecular linkages between diabetes and Alzheimer’s disease: current scenario and future prospects. CNS Neurol Disord Drug Targets. 2014;13(2):290–298. doi:10.2174/18715273113126660135
7. Yaffe K, Falvey C, Hamilton N. Diabetes, glucose control, and 9-year cognitive decline among older adults without dementia. Arch Neurol. 2012;69(9):1170–1175. doi:10.1001/archneurol.2012.1117
8. Bordier L, Doucet J, Boudet J, Bauduceau B. Update on cognitive decline and dementia in elderly patients with diabetes. Diabetes Metab. 2014;40(5):331–337. doi:10.1016/j.diabet.2014.02.002
9. Bakouni H, Gontijo Guerra S, Chudzinski V, Berbiche D, Vasiliadis HM. One-year prospective study on the presence of chronic diseases and subsequent cognitive decline in older adults. J Public Health (Oxf). 2016;39(4):e170–e178. doi:10.1093/pubmed/fdw124
10. Gifford KA, Badaracco M, Liu D, et al. Blood pressure and cognition among older adults: a meta-analysis. Arch Clin Neuropsychol. 2013;28(7):649–664. doi:10.1093/arclin/act046
11. Jefferson AL, Hohman TJ, Liu D, et al. Adverse vascular risk is related to cognitive decline in older adults. J Alzheimers Dis. 2015;44(4):1361–1373. doi:10.3233/JAD-141812
12. Oremus M, Girouard H, Raina P. A systematic review of reviews to examine the association between hypertension and cognitive impairments in adults. In: Girouard H, editor. Hypertension and the Brain as an End-Organ Target. Cham (Switzerland): Springer;2016. doi:10.1007/978-3-319-25616-0_1day
13. Anson O, Paran E. Hypertension and cognitive functioning among the elderly: an overview. Am J Ther. 2005;12(4):359–365.
14.
15.
16.
17. Long AN, Dagogo-Jack S. Comorbidities of diabetes and hypertension: mechanisms and approach to target organ protection. J Clin Hypertens (Greenwich). 2011;13(4):244–251. doi:10.1111/j.1751-7176.2011.00434.x
18. Iadecola C, Yaffe K, Biller J, et al. Impact of hypertension on cognitive function: a scientific statement from the american heart association. Hypertension. 2016;68(6):e67–e94. doi:10.1161/HYP.0000000000000053
19. Plassman BL, Williams JR, Jw B, et al. Systematic review: factors associated with risk for and possible prevention of cognitive decline in later life. Ann Intern Med. 2010;153(3):152–193. doi:10.7326/0003-4819-153-1-201007060-00004
20. Hassing LB, Hofer SM, Nilsson SE, et al. Comorbid type 2 diabetes mellitus and hypertension exacerbates cognitive decline: evidence from a longitudinal study. Age Ageing. 2004;33(4):355–361. doi:10.1093/ageing/afh100
21. Khattab M, Khader YS, Al-Khawaldeh A, Ajlouni K. Factors associated with poor glycemic control among patients with type 2 diabetes. J Diabetes Complicat. 2010;24(2):84–89. doi:10.1016/j.jdiacomp.2008.12.008
22. Duckworth W, Abraira C, Moritz T, et al. VADT investigators. Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med. 2009;360(2):129–139. doi:10.1056/NEJMoa0808431
23. Rawlings AM, Sharrett AR, Schneider AL, et al. Diabetes in midlife and cognitive change over 20 years: a cohort study. Ann Intern Med. 2014;161(11):785–793. doi:10.7326/M14-0737
24. Meneilly GS, Cheung E, Tessier D, Yakura C, Tuokko H. The effect of improved glycemic control on cognitive functions in the elderly patient with diabetes. J Gerontol. 1993;48(4):M117–M21.
25. Mussell M, Hewer W, Kulzer B, Bergis K, Rist F. Effects of improved glycaemic control maintained for 3 months on cognitive function in patients with type 2 diabetes. Diabet Med. 2004;21(11):1253–1256. doi:10.1111/j.1464-5491.2004.01322.x
26. Esposti LD, Saragoni S, Batacchi P, Geppetti P, Buda S, Esposti ED. Antihypertensivetherapy among newly treated patients: an analysis of adherence and cost of treatment over years. Clinico Econ Outcomes Res. 2010;2:113–120. doi:10.2147/CEOR.S11933
27.
28. Starr JM, Whalley LJ, Deary IJ. The effects of antihypertensive treatment on cognitive function: results from the HOPE study. J Am Geriatr Soc. 1996;44(4):411–415.
29. Prince MJ, Bird AS, Blizard RA, Mann AH. Is the cognitive function of older patients affected by antihypertensive treatment? Results from 54 months of the Medical Research Council‘s trial of hypertension in older adults. BMJ. 1996;312(7034):801–805.
30. Alrawi YA, Panerai RB, Myint PK, Potter JF. Pharmacological blood pressure lowering in the older hypertensive patients may lead to cognitive impairment by altering neurovascular coupling. Med Hypotheses. 2013;80(3):303–307. doi:10.1016/j.mehy.2012.12.010
31. Préville M, Boyer R, Grenier S, et al. The epidemiology of psychiatric disorders in Quebec‘s older adult population. Can J Psychiatry. 2008;53(12):822–832. doi:10.1177/070674370805301208
32. Folstein MF, Folstein SE, McHugh PR. Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198.
33.
34.
35. Marioni RE, Chatfield M, Brayne C, Matthews FE;
36. Steiner JF, Prochazka AV. The assessment of refill compliance using pharmacy records: methods, validity, and applications. J Clin Epidemiol. 1997;50(1):105–116. doi:10.1016/S0895-4356(96)00268-5
37. Cramer JA, Roy A, Burrell A, et al. Medication compliance and persistence: terminology and definitions. Value Health. 2008;11(1):44–47. doi:10.1111/j.1524-4733.2007.00213.x
38. Karve S, Cleves MA, Helm M, Hudson TJ, West DS, Martin BC. Good and poor adherence: optimal cut-point for adherence measures using administrative claims data. Curr Med Res Opin. 2009;25(9):2303–2310. doi:10.1185/03007990903126833
39. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383.
40.
41. Gregg EW, Yaffe K, Cauley JA, et al. Is diabetes associated with cognitive impairment and cognitive decline among older women? study of osteoporotic fractures research group. Arch Intern Med. 2000;160(2):174–180.
42. Herath PM, Cherbuin N, Eramudugo Lla R, Anstey KJ. The effect of diabetes medication on cognitive function: evidence from the PATHthrough life study. Biomed Res Int. 2016;2016:7208429. doi:10.1155/2016/7208429
43. Xie H, Mayo N, Koski L. Identifying and characterizing trajectories of cognitive change in older persons with mild cognitive impairment. Dement Geriatr Cogn Disord. 2011;31(2):165–172. doi:10.1159/000323568
44. Potvin O, Forget H, Grenier S, Préville M, Hudon C. Anxiety, depression, and 1-year incident cognitive impairment in community-dwelling older adults. J Am Geriatr Soc. 2011;59(8):1421–1428. doi:10.1111/j.1532-5415.2011.03521.x
45. Thomas AJ, O‘Brien JT. Depression and cognition in older adults. Curr Opin Psychiatry. 2008;21(1):8–13. doi:10.1097/YCO.0b013e3282f2139b
46. Yasar S, Xia J, Yao W, et al. Antihypertensive drugs decrease risk of Alzheimer disease: ginkgo evaluation of memory study. Neurology. 2013;81(10):896–903. Epub 2013 Aug 2. doi: 10.1212/WNL.0b013e3182a35228
47. Guimarães FC, Amorim PR, Reis FF, et al. Physical activity and better medication compliance improve mini-mental state examination scores in the elderly. Dement Geriatr Cogn Disord. 2015;39(1–2):25–31. doi:10.1159/000366413
48. Skoog I, Lithell H, Hansson L, et al. Effect of baseline cognitive function and antihypertensive treatment on cognitive and cardiovascular outcomes: Study on COgnition and Prognosis in the Elderly (SCOPE). Am J Hypertens. 2005;18(8):1052–1059. doi:10.1016/j.amjhyper.2005.02.013
49. Campbell NL, Boustani MA, Skopelja EN, Gao S, Unverzagt FW, Murray MD. Medication adherence in older adults with cognitive impairment: a systematic evidence-based review. Am J Geriatr Pharmacother. 2012;10(3):165–177. doi:10.1016/j.amjopharm.2012.04.004
50. Wennberg AMV, Hagen CE, Edwards K, et al. Association of antidiabetic medication use, cognitive decline, and risk of cognitive impairment in older people with type 2 diabetes: results from the population-based Mayo clinic study of aging. Int J Geriatr Psychiatry. 2018;33(8):1114–1120. doi:10.1002/gps.4900
51. Choo PW, Rand CS, Inui TS, et al. Validation of patient reports, automated pharmacy records, and pill counts with electronic monitoring of adherence to antihypertensive therapy. Med Care. 1999;37(9):846–857. doi:10.1097/00005650-199909000-00002
52. Sperber CM, Samarasinghe SR, Lomax GP. An upper and lower bound of the medication possession ratio. Patient Prefer Adherence. 2017;11:1469–1478. doi:10.2147/PPA.S136890
53. Gentil L, Vasiliadis HM, Préville M, Berbiche D. Adherence to oral antihyperglycemic agents among older adults with mental disorders and its effect on health care costs, Quebec, Canada, 2005–2008. Prev Chronic Dis. 2015;12:E230. doi:10.5888/pcd12.150412
54. Dragomir A, Côté R, Roy L, et al. Impact of adherence to antihypertensive agents on clinical outcomes and hospitalization costs. Med Care. 2010;48(5):418–425. doi:10.1097/MLR.0b013e3181d567bd
55. Balkrishnan R, Rajagopalan R, Camacho FT, Huston SA, Murray FT, Anderson RT. Predictors of medication adherence and associated health care costs in an older population with type 2 diabetes mellitus: a longitudinal cohort study. Clin Ther. 2003;25:2958–2971. doi:10.1016/S0149-2918(03)80347-8
56. Horn OK, Jacobs-Whyte H, Ing A, Bruegl A, Paradis G, Macaulay AC. Incidence and prevalence of type 2 diabetes in the first nation community of kahnawa`: Ke, Quebec, Canada, 1986–2003. Can J Public Health. 2007;98(6):438–443.
57. Cazale L, Nanhou V, Laprise P. Maladies chroniques au Québec et au Canada: Évolution récente et comparaisons régionales: Série Enquête sur la santé dans les collectivités canadiennes. Montréal: Institut de la statistique du Québec; 2009.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.