")
Back to Journals » International Medical Case Reports Journal » Volume 15
Coarctation of the Aorta with Arterial Tortuosity Syndrome – A Case Report with Cinematic Rendering
Authors Asafu Adjaye Frimpong G, Aboagye E, Tannor EK , Chigbu CNC, Daboner VT
Received 27 February 2022
Accepted for publication 26 May 2022
Published 5 July 2022 Volume 2022:15 Pages 349—354
DOI https://doi.org/10.2147/IMCRJ.S362434
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
George Asafu Adjaye Frimpong,1,2 Evans Aboagye,1 Elliot Koranteng Tannor,3,4 Naomi Cindy Chinenyenwa Chigbu,5 Victoria Temabore Daboner5
1Spectra Health Imaging and Interventional Radiology, Kumasi, Ghana; 2Department of Radiology, School of Medicine and dentistry, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana; 3Department of Medicine, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana; 4Renal Unit, Directorate of Medicine, Komfo Anokye Teaching Hospital, Kumasi, Ghana; 5School of Medicine and Dentistry, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana
Correspondence: George Asafu Adjaye Frimpong, Spectra Health Imaging and Interventional Radiology, Kumasi, Ghana, Tel +233201169108, Email [email protected]
Abstract: Coarctation of the aorta (CoA) with arterial tortuosity syndrome (ATS) is a rare hereditary condition characterized by elongation and tortuosity of the medium- and large-sized arteries, pulmonary hypertension, pulmonary artery stenosis, and constriction or narrowing of the aorta. Considering the non-specific indications and the overlap of ATS with other disorders of the connective tissue such as Williams Beuren syndrome (elastin), Marfan syndrome (fibrillin-1) and Ehlers Danlos syndrome (Type III collagen), it is vital to keep a high diagnostic suspicion in the analysis of the condition. We therefore report on a rare occurrence of coarctation of the aorta with arterial tortuosity syndrome in a teenage female who initially presented with severe resistant hypertension, providing additional literature to aid in the differential diagnosis of COA with ATS. Cinematic rendering delivered a markedly enhanced view of the condition, allowing for greater accuracy in the diagnosis.
Keywords: coarctation of the aorta, arterial tortuosity, cinematic rendering, connective tissue disorder
Introduction
Coarctation of the aorta (CoA), which involves constriction or narrowing of the aorta, is a relatively common defect, accounting for 5–8% of all congenital heart diseases. It may occur as an isolated defect or in association with various other lesions, such as ventricular septal defect (VSD) and bicuspid aortic valve. However, in rare circumstances as in our case presentation, coarctation of the aorta occurs with arterial tortuosity syndrome. Literature on the association of COA with ATS is scarce considering the rarity of the condition.
Arterial tortuosity syndrome (ATS), on the other hand, is an extremely rare inherited, autosomal recessive connective tissue disorder, which was first described in 1967 by Ertugrul.1 Clinically, ATS presentation is variable but the most common features include elongation and tortuosity of the medium- and large-sized arteries, pulmonary hypertension, pulmonary artery stenosis, laxity of the skin and joint, bowel hernia and dysmorphic facial features.2 However, the clinical manifestations and prognosis are related to a great extent to the presence of stenosis of the aorta or pulmonary arteries.3
In this case presentation, we report on a rare occurrence of coarctation of the aorta with arterial tortuosity syndrome in a teenage female who initially presented with severe resistant hypertension, thus providing additional literature to aid in differential diagnosis of COA with ATS. Cinematic rendering, which uses a global lighting model to generate photorealistic representation of 3D reconstructions of images, was employed for the first time in the diagnosis of the condition.
Clinical Presentation
A 16-year-old female initially presented at a screening exercise and was found to have a blood pressure of 200/110 mmHg. Further enquiries showed that she had been started on an antihypertensive but could not give an exact duration due to non-adherence. Also, she admitted to having palpitations and occasional headaches. She, however, did not have a family history of hypertension, kidney disease or diabetes, and she did not take illicit drugs, alcohol or smoke.
On examination, she was found to be stable of normal body habitus for her age, no moon face and neither was she obese. She had a blood pressure of 170/110mmHg, a pulse of 88 bpm regular good volume and non-collapsing with a radio radial delay, the apex was not displaced and the precordium was not active. She had normal first and second heart sounds and an ejection systolic murmur. The respiratory rate was 16 cpm, chest was clinically clear with no added sounds. The abdominal examinations were essentially normal except for an abdominal bruit that was heard on the left side of the umbilicus. Urine examination reveals no proteinuria nor hematuria and a specific gravity of 1.020. Accompanying renal function test done reveals serum creatinine of 80 umol/L and a serum urea of 3.9 mmol/L, serum sodium of 146 mmol/L and serum potassium of 5 mmol/L. Based on these observations, refractory hypertension with differentials of a suspected renal artery stenosis was suspected. Subsequently, computed tomography (CT) abdominal angiogram, followed by CT scan of the chest, was requested to confirm the diagnosis.
CT abdominal angiogram was performed from the top of the aortic arch to the level of the bifurcation. The aorta was normal in caliber from the origin to the bifurcation. There were no significant atherosclerotic changes. The main pathology was a vascular anomaly involving the abdominal wall predominantly caused by anomalous arteries arising from both common femoral arteries, which run superficially and form a web of vessels bilateral before joining dilated vessels, which appear to arise from the chest wall. Also noted were dilated vessels on the lateral part of both chest walls. Applying cinematic rendering, it was shown that there were extensive collateralization and dilation of the abdominal wall vasculature including the superior epigastric artery, the inferior epigastric artery and the superficial artery forming an intricate arterial mesh in the middle third of the abdominal wall (Figure 1). The inferior epigastric artery transcends deep enough to join the common femoral artery bilaterally. The superficial epigastric artery is also seen connected to the external iliac artery. The superior epigastric arteries are also seen originating from severely dilated internal mammary arteries (Figure 2).
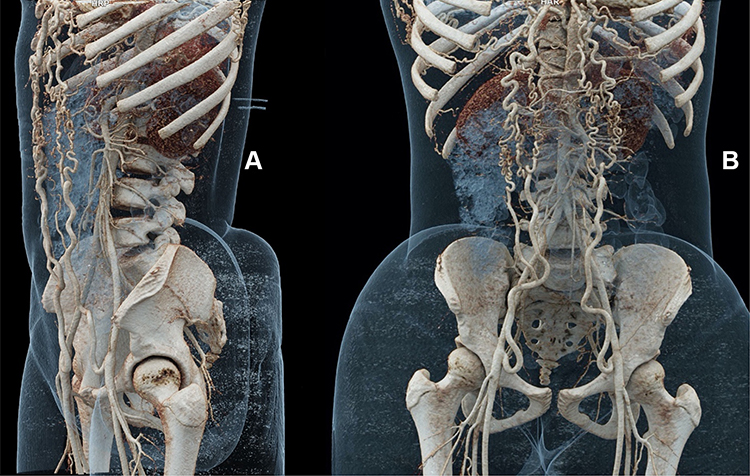 |
Figure 1 Cinematic rendering of the abdominal angiogram highlighting the collateralization and the mesh of arteries of the anterior abdominal arteries. (A) is the oblique view and (B) is the anterior view. |
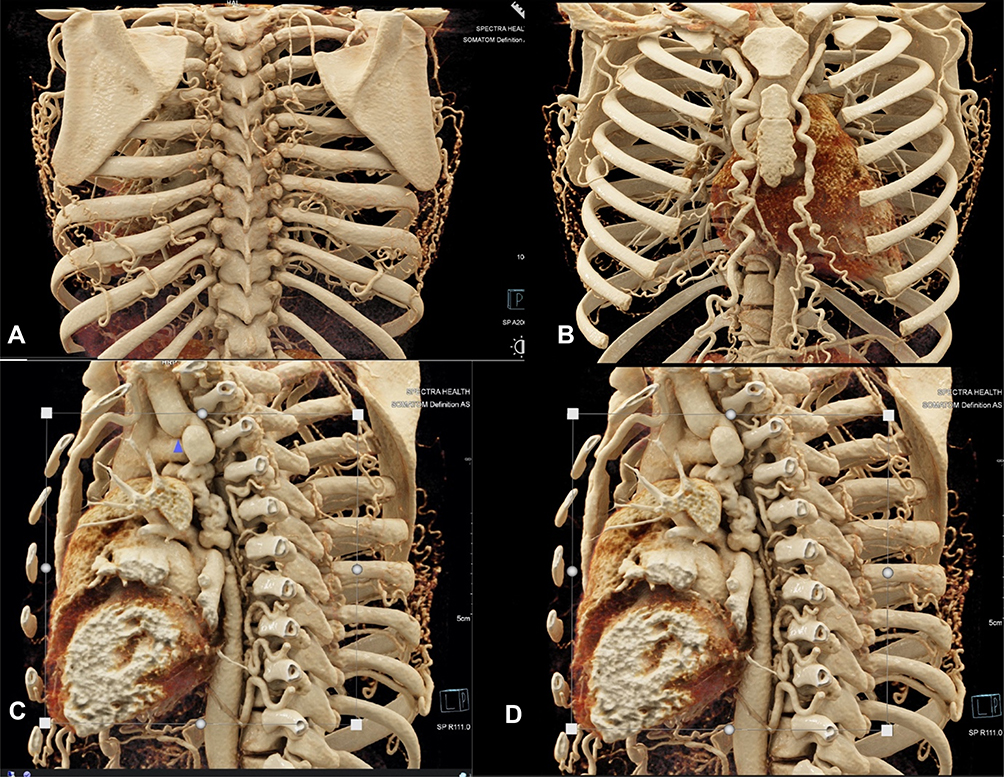 |
Figure 2 Cinematic rendering showing extensive arterial collateral circulation with severe dilatation of the internal mammary arteries (posterior (A) and anterior (B) view), with a sagittal reconstruction showing about 50% narrowing of the distal part of the aortic arch (blue arrow head) and sclerosing tortuosity involving the proximal part of the descending thoracic aorta (C and D). |
A follow-up CT angiogram of the thoracic aorta was also performed from the thoracic inlet through to the level of the adrenals. Findings showed that there was about 50% short segment narrowing of the distal part of the aortic arch (Figure 2) and severe narrowing of the thoracic aorta beginning from the distal part of the aortic arch (diameter 0.9 cm) covering a length of about 10 cm, with significant tortuosity of the descending aorta (Figure 2). Multiple dilated anterior and posterior chest wall vessels were seen (Figure 2). Also, extensive arterial wall calcifications were seen in the maximum intensity projection images (Figure 3). Based on these observations, a diagnosis of coarctation of the aorta with arterial tortuosity syndrome was made.
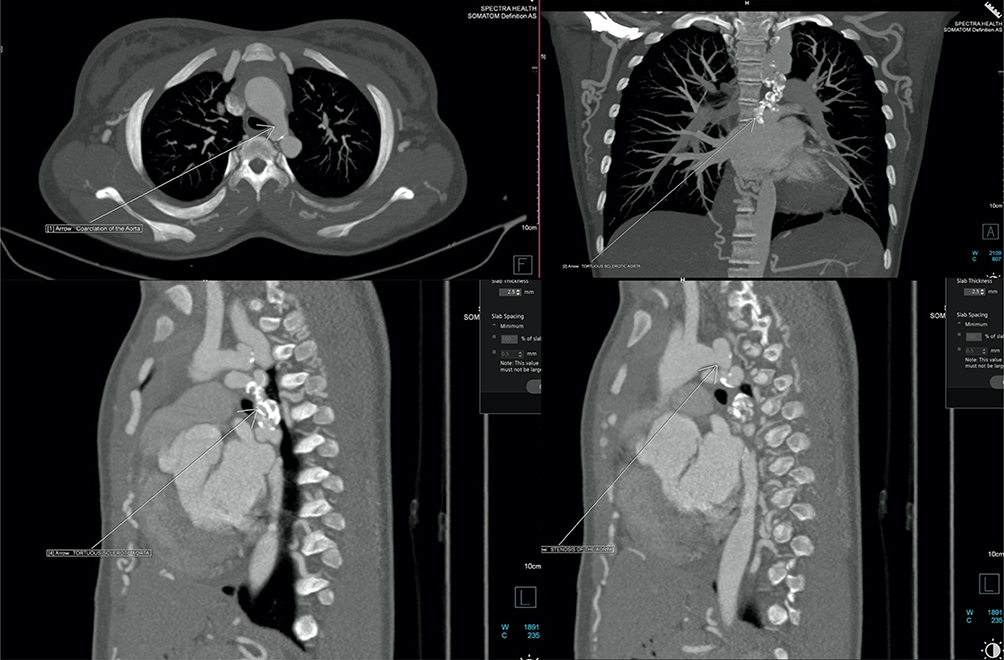 |
Figure 3 Maximum intensity reconstuction (MIP) in axial, coronal and sagittal reformatting depicting the coarctation and the sclerotic arterial tortuosity of the proximal part of the descending aorta. |
The patient was initially started on Nifedipine (30 mg) twice daily, bendrofluazide (2.5 mg daily) and methyldopa (250 mg) twice a day. She was finally referred to see a cardiothoracic surgeon for a possible surgical intervention.
Written informed consent was obtained from the parent to have the case details and accompanying images published. Subsequently, institutional approval was sought and obtained from Spectra Health Imaging and Interventional Radiology.
Discussion
Coarctation of the aorta (COA) with arterial tortuosity syndrome is a rare case presentation characterized by elongation and tortuosity of the medium- and large-sized arteries, pulmonary hypertension, pulmonary artery stenosis, and constriction or narrowing of the aorta.2,3 Coarctation of the aorta is, however, relatively common, prevalent in approximately 3 cases per 10,000 live births globally. It has a male predilection with male-to-female ratio between 1.27:1 and 1.74:1.5 Coarctation in an older child usually presents as an isolated and asymptomatic lesion, mostly discovered following an evaluation for upper extremity hypertension (as in our case) or for a murmur. It is estimated that about 89% to 92% of children with COA have upper extremity hypertension.6,7 However, a minority of older children with COA show signs of systemic hypertension, as found in our patient during the initial screening.8 Arterial tortuosity syndrome (ATS), on the other hand, is very rare, and until the last decade, ATS patients were frequently diagnosed with other disorders of the connective tissues such as Ehlers-Danlos syndrome, mostly due to nonspecific symptoms and overlap with other connective tissue disorders. However, the former has been shown to be associated with more extensive vascular changes. Clinical manifestations in ATS are highly variable, ranging from early mortality during infancy to limited manifestations in adulthood, indicating that the first years of life are the most critical.9 Although there are no formal diagnostic criteria for ATS, subjects usually present with characteristic dysmorphic features including an elongated face, a beaked nose, micrognathia, arched palate and blepharophimosis. In the present case presentation, there were no clear dysmorphic features, which might be due to the younger age of the patient, as the typical phenotype in most cases becomes prominent with aging.9,10
The patient in our case report initially presented with severe resistant hypertension. Upon initial clinical examination, renal artery stenosis was suspected but was subsequently ruled out by radiological examinations. Initial examination with CT abdominal angiogram showed an anterior abdominal wall vascular malformation, to which chest CT was indicated to aid in the diagnosis of the cause of hypertension. Results from the chest CT showed significant narrowing (50% stenosis) of the distal part of the aortic arch of the thoracic aorta, and severe narrowing and tortuosity of the descending aorta (Figure 2). There were also multiple surrounding collaterals and multiple dilated chest wall vessels as seen in Figures 2. The diagnosis of coarctation of the aorta (COA) with arterial tortuosity syndrome (ATS) was subsequently made based on these observations. Moreover, the application of cinematic rendering allowed for a greater degree of accuracy in the diagnosis of the condition than achieved with standard volume rendering.11 This underscores the critical role played by radiological examinations in the differential diagnosis of COA with ATS. Also, in the evaluation of patients with the condition, non-invasive modalities like CT and MRI have replaced invasive diagnostic procedures due to increased fragility and tendency of the vascular collagen and blood vessels to rupture.4
Management of COA with ATS usually includes the initial corrective procedure and the management of long-term cardiovascular complications. Percutaneous balloon angioplasty (with or without stent placement) and surgical repair are the general treatment options. They are both effective in managing the condition, but balloon angioplasty has been associated with the risk of aneurysm and recoarctation. A successful intervention is marked by a general decrease in blood pressure, but recurrent hypertension is often seen in subjects whose repair is performed later in life.
For older patients, as in our case, preoperative management is very vital before considering surgical repair or balloon angioplasty. Due to the risk of preexisting hypertension in these patients as evident in our case, it is important to first treat them with beta-adrenergic–blocking drugs to control hypertension before surgery. In our case, for example, the patient was initially treated with Nifedipine (30 mg), bendrofluazide (2.5 mg) and methyldopa (250 mg) before she was referred to see a cardiothoracic surgeon. Failure to provide preoperative beta-blockade may lead to marked hypertensive responses to intubation. It should also be noted that vasodilators are contraindicated before surgery in the hypertensive child with CoA.
Conclusion
This paper reports on the rare occurrence of coarctation of the aorta with arterial tortuosity syndrome in a teenager. In the analysis of the condition, it is vital to maintain a high diagnostic suspicion due to non-specific indications and overlap with other disorders of the connective tissue. The paper thus highlights the critical role played by radiological examinations in the differential diagnosis of coarctation of the aorta with arterial tortuosity syndrome. The application of cinematic rendering allows for a greater degree of accuracy in the diagnosis, surgical planning and decision-making than achieved with standard volume rendering.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ertugrul A. Diffuse tortuosity and lengthening of the arteries. Circulation. 1967;36(3):400–407. doi:10.1161/01.CIR.36.3.400
2. Faiyaz Ul-Hague M, Zaidi SH, Al Sanna N, et al. A novel missense and a recurrent mutation in SLC2A10 gene of patients affected with arterial tortuosity syndrome. Atherosclerosis. 2009;203(2):466–471. doi:10.1016/j.atherosclerosis.2008.07.026
3. Cubero A, Ayala J, Hamzeh G, Cortes A, Udaondo J, Aramendi JI. Severe arterial tortuosity: report of three cases. World J Pediatr Congenit Heart Surg. 2017;8(2):231–234. doi:10.1177/2150135116629396
4. Bhat V. Arterial tortuosity syndrome: an approach through imaging perspective. J Clin Imaging Sci. 2014;4:44. doi:10.4103/2156-7514.139734
5. Campbell M, Polani PE. The aetiology of coarctation of the aorta. Lancet. 1961;1:463–468. doi:10.1016/S0140-6736(61)90055-1
6. Thoele DG, Muster AJ, Paul MH. Recognition of coarctation of the aorta. A continuing challenge for the primary care physician. Am J Dis Child. 1987;141:1201–1204. doi:10.1001/archpedi.1987.04460110071025
7. Strafford MA, Griffiths SP, Gersony WM. Coarctation of the aorta: a study in delayed detection. Pediatrics. 1982;69(2):159–163. doi:10.1542/peds.69.2.159
8. Johns KJ, Johns JA, Feman SS. Retinal vascular abnormalities in patients with coarctation of the aorta. Arch Ophthalmol. 1991;109(9):1266–1268. doi:10.1001/archopht.1991.01080090090029
9. Callewaert B, De Paepe A, Coucke P, et al. Arterial tortuosity syndrome. In: Pagon RA, Adam MP, Ardinger HH, editors. Genereviews. Seattle: University of Washington; 2014.
10. Ritelli M, Chiarelli N, Dordoni C, et al. Arterial tortuosity syndrome: homozygosity for two novel and one recurrent SLC2A10 missense mutations in three families with severe cardiopulmonary complications in infancy and a literature review. BMC Med Genet. 2014;15(1):122. doi:10.1186/s12881-014-0122-5
11. Eid M, De Cecco CN, Nance JW Jr, et al. Cinematic rendering in CT: a novel, lifelike 3D visualization technique. Am J Roentgenol. 2017;209(2):370–379. doi:10.2214/AJR.17.17850
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.