")
Back to Journals » Journal of Pain Research » Volume 12
Co-Administered Low Doses Of Ibuprofen And Dexamethasone Produce Synergistic Antinociceptive Effects On Neuropathic Mechanical Allodynia In Rats
Authors Park MK, Kang SH, Son JY, Lee MK, Ju JS, Bae YC, Ahn DK
Received 5 July 2019
Accepted for publication 21 September 2019
Published 30 October 2019 Volume 2019:12 Pages 2959—2968
DOI https://doi.org/10.2147/JPR.S222095
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Katherine Hanlon
Min K Park,1,* Song H Kang,2,* Jo Y Son,2 Min K Lee,3 Jin S Ju,2 Yong C Bae,4 Dong K Ahn2
1Department of Dental Hygiene, Kyungwon University, Gumi, Korea; 2Department of Oral Physiology, School of Dentistry, Kyungpook National University, Daegu, Korea; 3Department of Dental Hygiene, Dong-Eui University, Busan, Korea; 4Department of Oral Anatomy, School of Dentistry, Kyungpook National University, Daegu, Korea
*These authors contributed equally to this work
Correspondence: Dong K Ahn
Department of Oral Physiology, School of Dentistry, Kyungpook National University, 2177 Dalgubeol-daero, Chung-gu, Daegu 41940, Korea
Tel +82-53-660-6840
Email [email protected]
Background: The traditional analgesics used to treat neuropathic pain such as anticonvulsants, opioids, and nonsteroidal anti-inflammatory drugs (NSAIDs) lack efficacy and/or carry unpleasant side effects. The present study aimed to investigate the synergistic antinociceptive effects of co-administered low doses of ibuprofen and dexamethasone in rats with trigeminal neuropathic pain.
Materials and methods: A Sprague-Dawley rat model for trigeminal neuropathic pain was produced using mal-positioned dental implants. The left mandibular second molar was extracted under anesthesia and replaced with a miniature dental implant to induce injury to the inferior alveolar nerve.
Results: Monotherapy with intraperitoneal injection of high-dose ibuprofen (30 mg/kg) or dexamethasone (10 mg/kg) but not low-dose ibuprofen (1, 5, 10 mg/kg) or dexamethasone (0.01, 1 mg/kg) attenuated the neuropathic mechanical allodynia in the rats with inferior alveolar nerve injury. We examined the synergistic antinociceptive effects of co-administered ibuprofen (5 mg/kg) and dexamethasone (0.01, 0.1, 1 mg/kg). The early co-administration of ibuprofen (5 mg/kg) with dexamethasone (0.1, 1 mg/kg) on postoperative days (POD) 1–3 significantly inhibited mechanical allodynia before the pain had been established. We also observed the synergistic antinociceptive effects of the same doses the combined treatment on mechanical allodynia on POD 7–9, when the pain had already been established. The attenuation of c-fos immuno-positive cells in the ipsilateral trigeminal subnucleus caudalis after the intraperitoneal co-administration of ibuprofen (5 mg/kg) with dexamethasone (1 mg/kg) confirmed these synergistic antinociceptive effects. Moreover, the magnitude of the effects of this co-administration was comparable with that of gabapentin both before and after the pain had been established.
Conclusion: These results suggest that a combination of ibuprofen and dexamethasone at low doses is an alternative therapeutic strategy for neuropathic pain and provide a rationale for the use of such drug combinations in patients who are unable to tolerate high-dose monotherapy.
Keywords: neuropathic pain, synergistic antinociceptive effects, ibuprofen, dexamethasone, trigeminal
Introduction
It has been well known that neuropathic pain results from conditions that compromise or abolish nerve function, including nerve injury, multiple sclerosis, and diabetes, and remains among the most challenging pain-related disorders to manage.1,2 A common symptom of neuropathic pain is allodynia, in which previously non-noxious stimuli are perceived as noxious following nerve injury.3 However, traditional analgesics including anticonvulsants, opioids, and nonsteroidal anti-inflammatory drugs (NSAIDs) lack efficacy in treating such pain and/or carry unpleasant side effects.2 Thus, neuropathic pain is an intractable disease from which only 40–60% of affected patients achieve even partial relief.4
NSAIDs are widely used for the symptomatic relief of all kinds of pain,2,5 but lack efficacy in treating neuropathic pain.4,6 Moreover, NSAIDs are associated with adverse side effects, including perforation and bleeding of the gastrointestinal tract, resulting from their inhibitory activity on gastrointestinal prostaglandin E2 synthesis.7 Nevertheless, the intrathecal administration of an NSAID, meloxicam was found to attenuate the thermal hyperalgesia and mechanical allodynia induced by spinal nerve ligation.8 Moreover, in rats, the intrathecal injection of ketorolac, a cyclooxygenase (COX)-1 inhibitor, or NS-398, a COX-2 inhibitor, attenuated the hyperalgesia and allodynia resulting from a chronic constriction injury of the sciatic nerve9 and partial sciatic nerve ligation.10 These findings suggest that although the COX pathways play an important role in the nociceptive processing of neuropathic pain, the efficacy of COX inhibitors in treating this type of pain has not been established.
Dexamethasone is used to treat a wide variety of inflammatory conditions because it is a synthetic glucocorticoid with anti-inflammatory activity and minimal mineralocorticoid effects.11 A previous study demonstrated that dexamethasone produced potent anti-inflammatory effects on carrageenan-induced inflammation.12 Additionally, dexamethasone has been used for the treatment of neuropathic pain conditions. Previous reports have indicated that a subcutaneous injection of dexamethasone or epidural injection of betamethasone attenuated mechanical allodynia in rats with spinal nerve ligation.13,14 However, the prolonged use of dexamethasone can also be associated with serious side effects15,16 suggesting that it has limited application in treating neuropathic pain conditions.
In our present study, we investigated the synergistic antinociceptive effects of co-administered low doses of ibuprofen and dexamethasone in rats with inferior alveolar nerve injury. Although these drugs were found to be largely ineffective against the pain when administered alone, we confirmed their synergistic antinociceptive effects when given in combination at a low dose by examining the changes in c-fos expression in the trigeminal subnucleus caudalis.
Materials And Methods
Trigeminal Neuropathic Pain Animal Model
Male Sprague-Dawley rats (total number = 163; Central Lab. Animal, Inc., Korea) weighing 200–230 g were used to generate the trigeminal neuropathic pain model. The animals were maintained in a temperature-controlled room (23 ± 1°C) on a 12/12 hr light-dark cycle. To generate the animal model, the rats were anesthetized with a mixture of ketamine (40 mg/kg, intramuscularly; i.m.) and xylazine (4 mg/kg, i.m.) solution. Briefly, under anesthesia, the left lower second molar was extracted and replaced with a mini–dental implant (diameter, 1 mm; length, 4 mm; donated by Megagen, Gyengsan, Korea) to intentionally injure the inferior alveolar nerve, as described previously.17,18 For the sham group, the operation was identical but without the placement of a dental implant. Only data from the rats presenting with an inferior alveolar nerve injury due to the mal-positioned dental implants were used in the final analyses.
All procedures involving the use of animals were approved by the Institutional Care and Use Committee of the School of Dentistry, Kyungpook National University. The animal experiments were also conducted in accordance with the ethical guidelines of the International Association for the Study of Pain (IASP) for investigations of experimental pain in conscious animals. All experiments were undertaken in a blind manner.
Evaluation Of Mechanical Allodynia
Mechanical allodynia was measured as described previously.19,20 Briefly, for behavioral observations, each rat was placed in a customized cage in a darkened and noise-free room. The animals were allowed to acclimate for at least 30 mins. Their withdrawal behavior was evaluated over 10 trials at a constant air-puff pressure (4-second duration and 10-second intervals). The intensity and intervals of the air-puff pressure were controlled using a pico-injector (Harvard Apparatus, Holliston, MA). The air-puffs were applied through a 26-gauge metal tube (length, 10 cm) located 1 cm from the skin at 90°. After inferior alveolar nerve injury, we identify the most sensitive areas by air-puff stimulation, as described previously,18 that included the ipsilateral lower jaw and mouth angle area of the facial region. The air-puff thresholds were determined using the air-puff pressure at which each rat responded in 50% of the trials. The cut-off pressure for the air-puffs was 40 psi, as determined previously.21,22 The naïve animals did not respond to a pressure lower than 40 psi.
Administration Of Drugs
The present study examined the antinociceptive effects of ibuprofen (2-(4-isobutylphenyl propionic acid) as an analgesic agent. After the intraperitoneal administration of ibuprofen (1, 5, 10, 30 mg/kg) on postoperative day (POD) 3, changes in the air-puff thresholds were investigated (n=6, each group). We also examined the antinociceptive effects of dexamethasone (0.1, 1, 10 mg/kg) after its intraperitoneal injection on POD 3 (n=6, each group). Vehicle was administered intraperitoneally on POD 3 in the control group. Low doses of ibuprofen (1, 5 mg/kg) or dexamethasone (0.1, 1 mg/kg) when administered alone, did not affect the air-puff thresholds and we selected previously employed doses of ibuprofen (5 mg/kg) and dexamethasone (0.01, 0.1, 1 mg/kg) in the combined treatment protocols. We then examined the synergistic antinociceptive effects of these co-administered low doses.
A previous study reported that central hypersensitivity was established within POD 3 and may be independent of the peripheral input after pain has been established.23 Hence, we examined the synergistic antinociceptive effects of co-administered ibuprofen (5 mg/kg) and dexamethasone (0.01, 0.1, 1 mg/kg) both prior to and after pain establishment on POD 1–3 and POD 7–9, respectively (n=6, each group). We also measured the antinociceptive effects of the intraperitoneal administration of gabapentin (30, 100 mg/kg) in a positive control group of rats with inferior alveolar nerve injury before and after the pain was established (n=6, each group).
Ibuprofen was purchased from Sigma–Aldrich (St. Louis, MO) and dissolved in 5% dimethyl sulfoxide (DMSO). Dexamethasone was purchased from Sigma–Aldrich and dissolved in sterile saline. Gabapentin was purchased from Tokyo Chemical Industry Co., LTD. and dissolved in sterile saline. All chemicals were stored at 4°C before use.
Immunohistochemical Staining Of c-Fos
On POD 3, we applied air-puff pressure (10 sec on/off, 20 psi intensity) for 10 mins after the co-administration of ibuprofen (5 mg/kg) with dexamethasone (1 mg/kg) in rats with inferior alveolar nerve injury. The rats (n = 5 per group) were transcardially perfused with 0.9% saline at 3 hrs after air-puff stimulation followed by 4% paraformaldehyde in 0.1 M phosphate buffer (PB, pH 7.4). The caudal medulla was dissected and post-fixed in the same fixative at 4°C for 2 hrs, and then incubated with 30% sucrose in 0.1 M PB overnight. The specimens were frozen and cut into 30 μm thick transverse sections. The free-floating sections were rinsed in phosphate-buffered saline (PBS) and blocked with 2.5% normal horse serum (Vector Laboratories, Burlingame, CA) for 1 hr at room temperature. The sections were incubated at 4°C overnight with the rabbit polyclonal anti-c-fos antibody (1:200; Santa Cruz Biotechnology, Dallas, TX) and then incubated in peroxidase-conjugated anti-rabbit IgG (Vector Laboratories) for 2 hrs at room temperature. After washing, the sections were incubated in a buffer containing diaminobenzidine (DAB, Vector Laboratories) and hydrogen peroxide (pH 7.5, Vector Laboratories) for approximately 1 min. The stained sections were analyzed under BX 41 and U-RFL-T microscopes (Olympus, Tokyo, Japan). Neurons that were immunopositive for c-fos were counted in the superficial laminae (I-II) of the ipsilateral trigeminal subnucleus caudalis on three sections since lamina I and II participate in pain processing in the spinal cord as well as the trigeminal spinal nucleus.24,25
Statistical Analysis
Statistical analysis of the animal behavioral data was performed by repeated-measures analysis of variance (ANOVA) followed by Holm-Sidak post hoc analysis. The c-fos expression data were analyzed by one-way ANOVA followed by Holm-Sidak post hoc analysis. In all statistical comparisons, P< 0.05 was considered significant. All data are presented as a mean ± SEM.
Results
Effects Of Intraperitoneal Injections Of Ibuprofen Or Dexamethasone Alone On Trigeminal Neuropathic Mechanical Allodynia
Figure 1 illustrates the effects of intraperitoneally administered ibuprofen or dexamethasone alone on neuropathic mechanical allodynia on POD 3. A single intraperitoneal injection of the vehicle or low doses of ibuprofen (1, 5 mg/kg) did not affect the air-puff thresholds. A single 10 mg/kg dose of ibuprofen increased the air-puff thresholds slightly but this was not statistically significant. Only a high dose of ibuprofen (30 mg/kg) significantly attenuated mechanical allodynia compared with the vehicle-treated control group; and these anti-allodynic effects persisted for over 6 hrs after the injection and abated within 24 hrs (Figure 1A and F(4,25)=122.674, P <0.05).
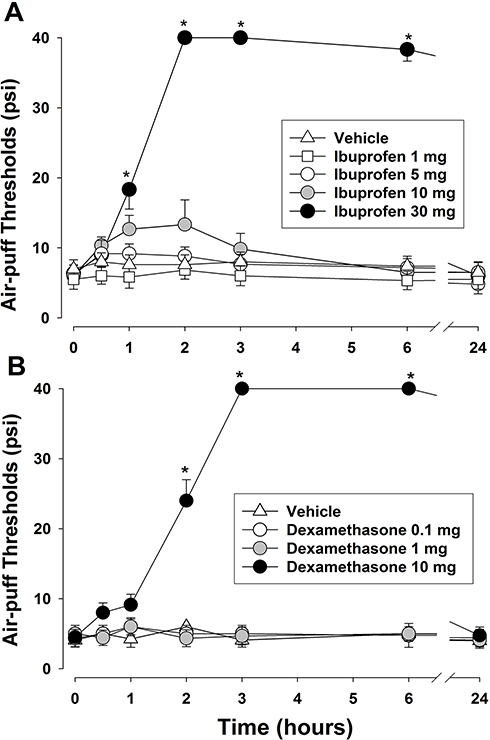 |
Figure 1 Effects of the intraperitoneal administration of ibuprofen (A) or dexamethasone (B) on the air-puff thresholds in rats with an inferior alveolar nerve injury. A high dose of ibuprofen (30 mg/kg) or dexamethasone (10 mg/kg) produced significant antiallodynic effects compared with the vehicle-treated control group. These effects persisted for over 6 hrs after the injection and dissipated within 24 hrs. Neither the intraperitoneal injection of the vehicle nor low doses of ibuprofen (1, 5, 10 mg/kg) or dexamethasone (0.1, 1mg/kg) affected the air-puff thresholds. The values shown are the mean ± SEM. There were 6 animals in each group. *p < 0.05, vehicle- vs. drug-treated group. |
The dose-dependent effects of intraperitoneally administered dexamethasone on neuropathic mechanical allodynia on POD 3 are illustrated in Figure 1B. Neither the vehicle control nor the low doses of dexamethasone (0.1, 1 mg/kg) had any impact on the neuropathic mechanical allodynia in the rats. Only high dose of dexamethasone (10 mg/kg) significantly attenuated this mechanical allodynia compared with the vehicle-treated control group and again these anti-allodynic effects persisted for over 6 hrs after the injection and had dissipated by 24 hrs (F(3,20)=50.001, P< 0.05).
Effects Of Co-Administered Low Doses Of Ibuprofen And Dexamethasone On Trigeminal Neuropathic Mechanical Allodynia
Figures 2 and 3 illustrate the effects of co-administered low doses of ibuprofen and dexamethasone on the air-puff thresholds in the experimental rats with inferior alveolar nerve injury. We examined the synergistic antinociceptive effects of this co-treatment on POD 1, 2, 3 (early-phase) before the pain had been established in this model (Figure 2). Vehicle administration did not affect the air-puff thresholds in the animals. In contrast, the co-administration of 5 mg/kg of ibuprofen with 0.01 mg/kg of dexamethasone attenuated the neuropathic mechanical allodynia in the rats, although it was not a statistically significant finding. Moreover, the combined daily treatments with ibuprofen (5 mg/kg) and dexamethasone (0.1 or 1 mg/kg) produced significant anti-allodynic effects compared with the vehicle treatment on POD 1–3 (F(3,20)=50.001, P <0.05). These anti-allodynic effects appeared immediately after the co-treatment and persisted for over 6 hrs but disappeared by 24 hrs post-injection.
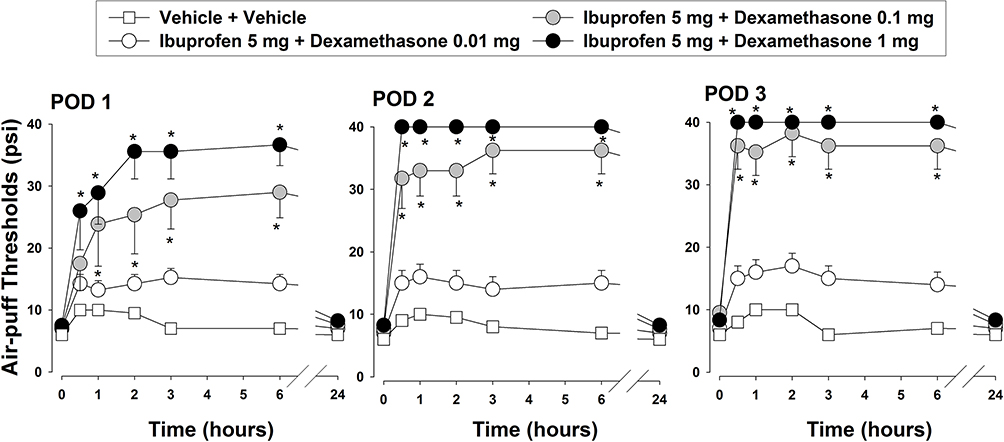 |
Figure 2 Synergistic antinociceptive effects of co-administered low doses of ibuprofen and dexamethasone on POD 1–3. The early intraperitoneal co-administration of ibuprofen (5 mg/kg) with dexamethasone (0.1, 1 mg/kg) produced significant antiallodynic effects prior to pain establishment in the rat model. These effects appeared immediately and persisted for over 6 hrs. The values shown are the mean ± SEM. There were 6 animals in each group. *p <0.05, vehicle- vs. drug-treated group. Abbreviation: POD, postoperativeday. |
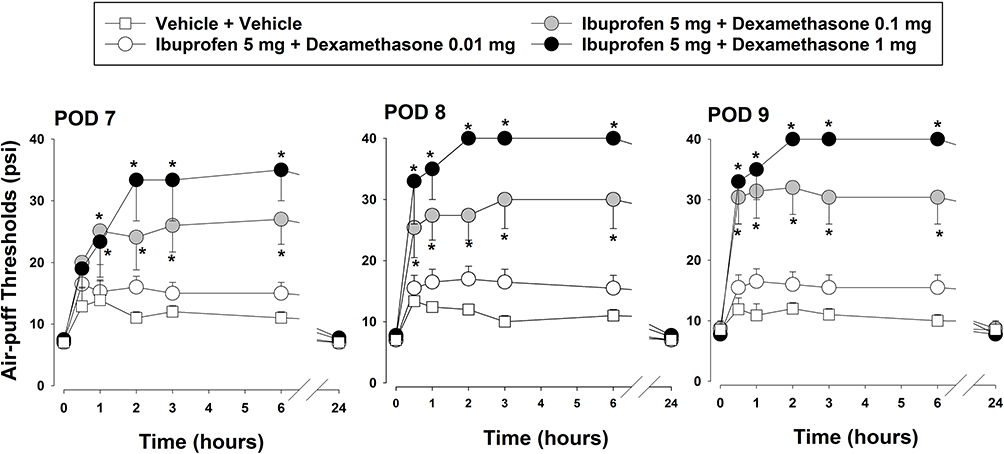 |
Figure 3 Synergistic antinociceptive effects of co-administered low doses of ibuprofen and dexamethasone on POD 7–9. The late intraperitoneal co-administration of ibuprofen (5 mg/kg) with dexamethasone (0.1, 1 mg/kg) produced significant antiallodynic effects after the pain had been established in the rat model. These effects appeared immediately and persisted for over 6 hrs. The values shown are the mean ± SEM. There were 6 animals in each group. *p <0.05, vehicle- vs. drug-treated group. Abbreviation: POD, postoperativeday. |
We also examined the synergistic anti-nociceptive effects of these same low doses of ibuprofen (5 mg/kg) and dexamethasone (0.1, 1 mg/kg) after the pain had already been established in the rat model on POD 7–9, and found again that it produced significant anti-allodynic effects (F(3,20)=44.675, P <0.05) that persisted for over 6 hrs after injection and dissipated within 24 hrs (Figure 3). However, neither the vehicle nor the co-administration of 5 mg/kg of ibuprofen with 0.01 mg/kg of dexamethasone affected the air-puff thresholds in this late treatment period.
Effects Of Co-Administered Low Doses Of Ibuprofen And Dexamethasone On c-Fos Expression
The effects of co-administering low doses of ibuprofen and dexamethasone on c-fos expression at POD 3 are indicated in Figure 4. The inferior alveolar nerve injury in the rats significantly augmented the number of c-fos immunoreactive cells compared with the sham-operated rats on POD 3 (P <0.05). Almost all of the c-fos-positive neurons were observed in the superficial layer (lamina I and II) of the ipsilateral trigeminal subnucleus caudalis and this number was significantly reduced by the co-administration of ibuprofen (5 mg/kg) and dexamethasone (1 mg/kg) compared to the vehicle-treated group (P <0.05). Neither ibuprofen nor dexamethasone treatments alone affected the production of c-fos immunopositive neurons following inferior alveolar nerve injury.
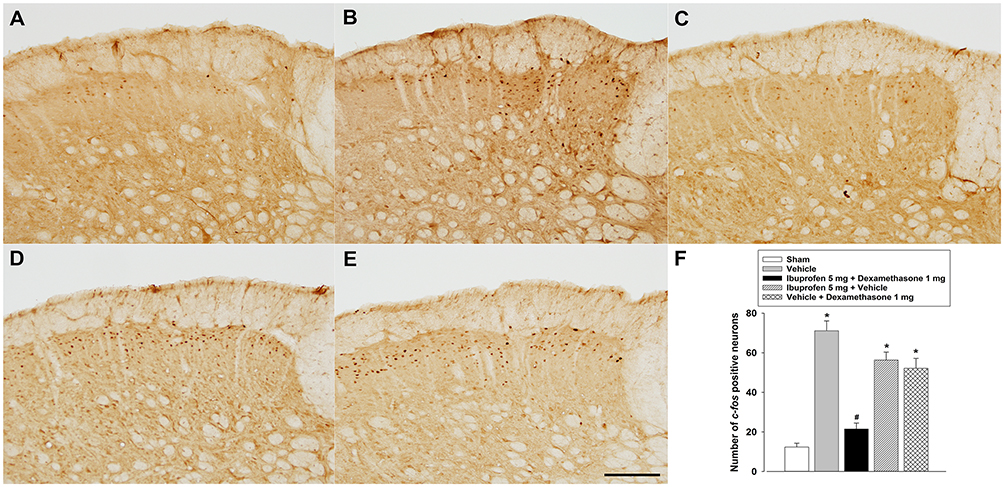 |
Figure 4 Effects of co-administered ibuprofen and dexamethasone on c-fos expression in the ipsilateral trigeminal subnucleus caudalis of the rat model on POD 3. (A) c-fos immunoreactive neurons in sham rats. (B) c-fos immunoreactive neurons after vehicle treatment in the rats with inferior alveolar nerve injury. (C) c-fos immunoreactive neurons after the intraperitoneal co-administration of ibuprofen (5 mg/kg) with dexamethasone (1 mg/kg) in the rats with inferior alveolar nerve injury. (D) c-fos immunoreactive neurons after the intraperitoneal injection of ibuprofen (5 mg/kg) in the rats with inferior alveolar nerve injury. (E) c-fos immunoreactive neurons after the intraperitoneal injection of dexamethasone (1 mg/kg) in the rats with inferior alveolar nerve injury. (F) Histograms showing the changes in the mean number of c-fos immunoreactive neurons. Inferior alveolar nerve injury in the rats significantly increased the number of c-fos- immunoreactive cells compared with the sham-operated rats. The co-administration of ibuprofen (5 mg/kg) with dexamethasone (1 mg/kg) significantly attenuated the number of c-fos immunopositive neurons compared to the vehicle-treated group. The values shown are the mean ± SEM. There were 5 animals in each group. Scale bar, 50 μm. *p< 0.05, sham- vs. vehicle/drug-treated group; #p< 0.05, vehicle- vs. drug-treated group. |
Effects Of Intraperitoneal Treatment With Gabapentin On Trigeminal Neuropathic Mechanical Allodynia
The anti-nociceptive effects of gabapentin on neuropathic mechanical allodynia were also tested in rats with an inferior alveolar nerve injury (Figure 5). Before the pain had been established in this animal model, the daily ntraperitoneal injection of gabapentin at 30 and 100 mg/kg significantly increased the air-puff thresholds compared to the vehicle-treated group on POD 1–3 (F(2,15)=103.916, P <0.05). Moreover, both doses of gabapentin produced anti-allodynic effects on POD 7–9 when the pain had already been established (F(2,15)=112.213, P <0.05). Once again, these anti-allodynic effects persisted for over 6 hrs after injection and had dissipated by 24 hrs.
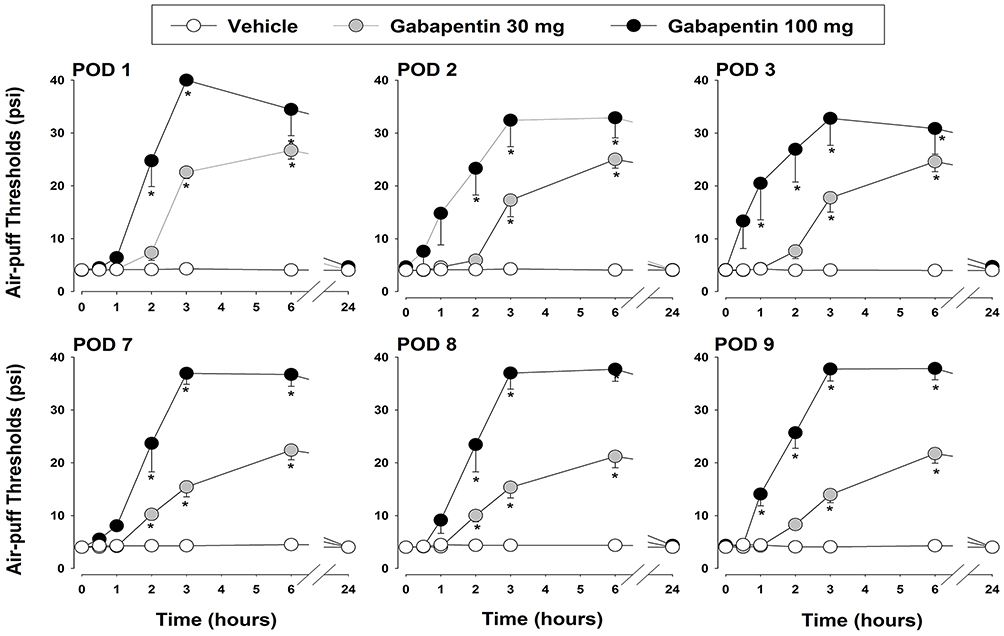 |
Figure 5 Anti-nociceptive effects of gabapentin on neuropathic mechanical allodynia in the rats with inferior alveolar nerve injury. The daily intraperitoneal administration of gabapentin (30, 100 mg/kg) produced significant anti-allodynic effects both before and after the pain was established in the animals. These effects persisted for 6 hrs and had dissipated within 24 hrs. The values shown are the mean ± SEM. There were 6 animals in each group. *p< 0.05, vehicle- vs. drug-treated group. Abbreviation: POD, postoperativeday. |
Discussion
Our present study provides evidence of the synergistic analgesic effects of intraperitoneally co-administered low doses of ibuprofen and dexamethasone on trigeminal neuropathic pain, both before and after the pain was established in a rat model. Significant attenuation of c-fos expression in the ipsilateral trigeminal subnucleus caudalis in the experimental rats confirmed the synergistic antinociceptive effects of this low dose co-treatment and we further found that they were comparable to the effects of gabapentin. A combination of ibuprofen and dexamethasone at low doses thus appears to represent an alternative therapeutic strategy for the treatment of trigeminal neuropathic pain.
COX inhibitors have generally been used as anti-inflammatory, analgesic, and antipyretic drugs because of their effectiveness and minimal side effects.26 Moreover, COX inhibitors are frequently prescribed to treat diabetic neuropathy, postherpetic neuralgia, and back/neck pain with neuropathic involvement5 because the involvement of the COX pathways in the sensitization of nociceptive processing at the spinal cord level has been well-described.27 In animal studies, the intrathecal administration of PGE2 has been reported to produce dose-dependent hyperalgesia in rats.28 This acute anti-hyperalgesic action has been shown to be mediated through the spinal COX-1 or COX-2 pathway in rats.27,29 Moreover, intrathecal injection of ketorolac, a COX-1 inhibitor, or NS-398, a COX-2 inhibitor, has been found to attenuate the thermal hyperalgesia and cold allodynia produced by chronic constriction injury of the sciatic nerve9 and also lessen the tactile allodynia in neuropathic pain following partial sciatic nerve ligation.10 However, a previous clinical trial showed that blockade of COX pathways by ibuprofen, a non-selective COX 1/2 inhibitor, failed to effectively treat the pain in patients with postherpetic neuralgia.30 Consistently, our present findings in rats indicate that low doses of ibuprofen do not attenuate neuropathic mechanical allodynia and that only a high dose of this drug (30 mg/kg) produces significant analgesic effects. Therefore, the collective evidence to date suggests that patients with neuropathic pain generally do not respond to NSAIDs and that the efficacy of COX inhibitors in the treatment of neuropathic pain has not been established.
Although dexamethasone treatment in rats has been reported to induce potent anti-inflammatory, antihyperalgesic and antiallodynic effects against carrageenan-induced inflammation12 and chronic arthritis,31 the analgesic effects of dexamethasone in neuropathic pain remains controversial. For instance, previous investigations reported that the systemic or intrathecal administration of dexamethasone failed to prevent mechanical and cold allodynia32 or reduce the activation of microglia33 in rats with a spared nerve injury. Similarly, in our current experimental rat model of neuropathic pain, the intraperitoneal injection of 0.1 or 1 mg/kg of dexamethasone did not produce antinociceptive effects and only a high dose of this agent (10 mg/kg) attenuated the neuropathic mechanical allodynia. Another previous study also demonstrated that only a high dose of dexamethasone produced significant antinociceptive effects in rats with inferior alveolar nerve injury before the pain was established.17 Moreover, early treatment with dexamethasone (25 mg/kg) decreased the upregulated expression of p38 MAPK and NF-κB in the glial cells following inferior alveolar nerve injury20 and spinal nerve injury34 in rats. These results suggest that early treatment with dexamethasone at high doses is important in the treatment of neuropathic pain, including trigeminal pain. However, dexamethasone has limited application in the treatment of neuropathic pain because of its unwanted side effects at high dosages. The present study demonstrated that combined treatments with ibuprofen (5 mg/kg) and dexamethasone (0.1 or 1 mg/kg) produced significant anti-allodynic effects, which were comparable with those of a high dose (10 mg) of dexamethasone administered alone. Thus, the combined treatment with low doses of ibuprofen and dexamethasone would reduce the unwanted side effects of high dose dexamethasone treatment and can be a good alternative therapeutic tool.
It is widely known that combination treatments with analgesics at lower doses can have beneficial effects against neuropathic pain when compared to monotherapy. Our present investigation in a rat pain model demonstrated that the intraperitoneal co-administration of ibuprofen (5 mg/kg) with dexamethasone (0.1, 1 mg/kg) produced significant anti-allodynic effects that were not seen when these drugs were administered individually. This kind of anti-inflammatory synergism resulting from co-treatments with an NSAID and steroid has been demonstrated in previous studies. Co-administered diclofenac and dexamethasone produced supra-additive anti-inflammatory effects in the carrageenan rat paw edema model35 and synergistic anti-inflammatory activity against lipopolysaccharide-induced inflammation in mice.36,37 However, there have been no previous reports on the co-administration of ibuprofen with dexamethasone in the treatment of neuropathic pain. Our current study findings have indicated that the co-administration of these drugs at low doses produces significant antinociceptive effects in rats, which were confirmed by the significantly reduced c-fos expression in the ipsilateral trigeminal subnucleus caudalis. Although a previous clinical study demonstrated that a combination of ibuprofen and dexamethasone decreased the pain intensity at 24 and 48 hrs after a lower third molar surgical extraction,38 our current results provide evidence of the synergistic analgesic effects of these drugs on neuropathic pain. Moreover, the efficacy of this combination was found to be comparable with that of gabapentin in our rat model. Hence, the co-administration of low doses of NSAIDs and steroids may minimize the potential side effects of high dose monotherapies using these agents. On the other hand, a previous study reported the potential risk of an ulcerogenic phenomenon following combination treatment with NSAIDs and steroids in rats. Indomethacin (10 mg/kg) administered in combination with prednisolone (10 mg/kg), a corticosteroid, showed the ulcerogenic potential including the deficiency of endogenous prostaglandins, an increase in neutrophil activation, and gastric hypermobility.39 However the present study employed low doses of ibuprofen (5 mg/kg) and dexamethasone (0.01, 0.1, 1 mg/kg) in combined treatment protocols to reduce the side effects produced by co-administration of NSAIDs and steroids in high doses. Therefore, the combination of ibuprofen and dexamethasone at low doses offers an alternative therapeutic strategy for neuropathic pain and provides a rationale for using such drug combinations in patients who are unable to tolerate a high-dose monotherapy.
Time is very important factor in the development of neuropathic pain in the trigeminal area. A previous study reported that central plasticity was established within POD 3 and may be independent of the peripheral input.23 Moreover, early administration of dexamethasone at high doses produced prolonged anti-allodynic effects before the pain had been established, but failed to reduce mechanical allodynia once the pain had already been established.17 This finding suggests that early treatment is necessary to overcome neuropathic pain after nerve injury. The present study examined the synergistic antinociceptive effects of co-administered ibuprofen (5 mg/kg) and dexamethasone (0.01, 0.1, 1 mg/kg) both, prior to and after pain establishment. Although co-administered ibuprofen and dexamethasone produced antinociceptive effects before the pain had been established, the effects were reversed within 24 hrs. The synergistic anti-nociceptive effects were also observed after the pain had already been established in the rat model. These results suggest that daily co-administered ibuprofen and dexamethasone can be a good alternative treatment strategy instead of long-term treatment with conventional analgesics for neuropathic pain.
Acknowledgments
This research was supported by the National Research Foundation of Korea (NRF) grant, which is funded by the Korea government (NRF-2017R1A5A2015391 and NRF-2018R1D1A1B07049025).
Author contributions
M.K. Park, S.H. Kang, and D.K. Ahn contributed to conception and design, analysis, drafting and critical revision of the manuscript. J.Y. Son and J.S. Ju, contributed to conception, interpretation, drafting and critical revision of the manuscript. M.K. Lee contributed to conception, data analysis, drafting and critical revision of the manuscript. Y.C. Bae contributed to conception and design, interpretation, drafting and critical revision of the manuscript. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work, ensuring integrity and accuracy.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Campbell JN, Meyer RA. Mechanisms of neuropathic pain. Neuron. 2006;52(1):77–92. doi:10.1016/j.neuron.2006.09.021
2. Attal N, Cruccu G, Baron R, et al.; European Federation of Neurological Societies. EFNS guidelines on the pharmacological treatment of neuropathic pain: 2010 revision. Eur J Neurol. 2010;17(9):1113–e88. doi:10.1111/j.1468-1331.2010.02999.x
3. Treede RD, Jensen TS, Campbell JN, et al. Neuropathic pain: redefinition and a grading system for clinical and research purposes. Neurology. 2008;70(18):1630–1635. doi:10.1212/01.wnl.0000282763.29778.59
4. Dworkin RH, O’Connor AB, Backonja M, et al. Pharmacologic management of neuropathic pain: evidence-based recommendations. Pain. 2007;132(3):237–251. doi:10.1016/j.pain.2007.08.033
5. Gore M, Dukes E, Rowbotham DJ, Tai KS, Leslie D. Clinical characteristics and pain management among patients with painful peripheral neuropathic disorders in general practice settings. Eur J Pain. 2007;11(6):652–664. doi:10.1016/j.ejpain.2006.10.004
6. Attal N, Cruccu G, Haanpaa M, et al.; EFNS Task Force. EFNS guidelines on pharmacological treatment of neuropathic pain. Eur J Neurol. 2006;13(11):1153–1169. doi:10.1111/j.1468-1331.2006.01511.x
7. Alhava E. Reported adverse drug reactions and consumption of non-steroidal anti-inflammatory drugs. Pharmacol Toxicol. 1994;75(Suppl 2):37–43. doi:10.1111/j.1600-0773.1994.tb01994.x
8. Takeda K, Sawamura S, Tamai H, Sekiyama H, Hanaoka K. Role for cyclooxygenase 2 in the development and maintenance of neuropathic pain and spinal glial activation. Anesthesiology. 2005;103(4):837–844. doi:10.1097/00000542-200510000-00023
9. Parris WC, Janicki PK, Johnson B
10. Ma W, Du W, Eisenach JC. Role for both spinal cord COX-1 and COX-2 in maintenance of mechanical hypersensitivity following peripheral nerve injury. Brain Res. 2002;937(1–2):94–99. doi:10.1016/s0006-8993(02)02593-3
11. Coutinho AE, Chapman KE. The anti-inflammatory and immunosuppressive effects of glucocorticoids, recent developments and mechanistic insights. Mol Cell Endocrinol. 2011;335(1):2–13. doi:10.1016/j.mce.2010.04.005
12. Miyasaka K, Mikami T. Comparison of the anti-inflammatory effects of dexamethasone, indomethacin and BW755C on carrageenin-induced pleurisy in rats. Eur J Pharmacol. 1982;77(4):229–236. doi:10.1016/0014-2999(82)90123-6
13. Caram-Salas NL, Reyes-García G, Medina-Santillán R, Granados-Soto V. Thiamine and cyanocobalamin relieve neuropathic pain in rats: synergy with dexamethasone. Pharmacology. 2006;77(2):53–62. doi:10.1159/000092643
14. Xie W, Liu X, Xuan H, et al. Effect of betamethasone on neuropathic pain and cerebral expression of NF-kappaB and cytokines. Neurosci Lett. 2006;393(2–3):255–259. doi:10.1016/j.neulet.2005.09.077
15. Lieberthal J, Sambamurthy N, Scanzello CR. Inflammation in joint injury and post-traumatic osteoarthritis. Osteoarthr Cartil. 2015;23(11):1825–1834. doi:10.1016/j.joca.2015.08.015
16. Wernecke C, Braun HJ, Dragoo JL. The effect of intra-articular corticosteroids on articular cartilage: a systematic review. Orthop J Sports Med. 2015;3(5):2325967115581163. doi:10.1177/2325967115581163
17. Han SR, Yeo SP, Lee MK, Bae YC, Ahn DK. Early dexamethasone relieves trigeminal neuropathic pain. J Dent Res. 2010;89(9):915–920. doi:10.1177/0022034510374056
18. Yang KY, Kim MJ, Ju JS, et al. Antinociceptive effects of botulinum toxin type a on trigeminal neuropathic pain. J Dent Res. 2016;95(10):1183–1190. doi:10.1177/0022034516659278
19. Ahn DK, Lim EJ, Kim BC, et al. Compression of the trigeminal ganglion produces prolonged nociceptive behavior in rats. Eur J Pain. 2009;13(6):568–575. doi:10.1016/j.ejpain.2008.07.008
20. Lee MK, Han SR, Park MK, et al. Behavioral evidence for the differential regulation of p-p38 MAPK and p-NF-ĸB in rats with trigeminal neuropathic pain. Mol Pain. 2011;7:57. doi:10.1186/1744-8069-7-57
21. Jeon HJ, Han SR, Park MK, Yang KY, Bae YC, Ahn DK. A novel trigeminal neuropathic pain model: compression of the trigeminal nerve root produces prolonged nociception in rats. Prog Neuropsychopharmacol Biol Psychiatry. 2012;38(2):149–158. doi:10.1016/j.pnpbp.2012.03.002
22. Kim MJ, Shin HJ, Won KA, et al. Progesterone produces antinociceptive and neuroprotective effects in rats with microinjected lysophosphatidic acid in the trigeminal nerve root. Mol Pain. 2012;8:16. doi:10.1186/1744-8069-8-16
23. Curatolo M, Petersen-Felix S, Arendt-Nielsen L, Giani C, Zbinden AM, Radanov BP. Central hypersensitivity in chronic pain after whiplash injury. Clin J Pain. 2001;17(4):306–315.
24. D’Mello R, Dickenson AH. Spinal cord mechanisms of pain. Br J Anaesth. 2008;101(1):8–16. doi:10.1093/bja/aen088
25. Peirs C, Williams SP, Zhao X, et al. Dorsal horn circuits for persistent mechanical pain. Neuron. 2015;87(4):797–812. doi:10.1016/j.neuron.2015.07.029
26. Adatia A, Rainsford KD, Kean WF. Osteoarthritis of the knee and hip. Part II: therapy with ibuprofen and a review of clinical trials. J Pharm Pharmacol. 2012;64(5):626–636. doi:10.1111/j.2042-7158.2012.01456.x
27. Samad TA, Moore KA, Sapirstein A, et al. Interleukin-1beta-mediated induction of Cox-2 in the CNS contributes to inflammatory pain hypersensitivity. Nature. 2001;410(6827):471–475. doi:10.1038/35068566
28. Taiwo YO, Levine JD. Prostaglandins inhibit endogenous pain control mechanisms by blocking transmission at spinal noradrenergic synapses. J Neurosci. 1988;8(4):1346–1349.
29. Yaksh TL, Dirig DM, Conway CM, Svensson C, Luo ZD, Isakson PC. The acute antihyperalgesic action of nonsteroidal, anti-inflammatory drugs and release of spinal prostaglandin E2 is mediated by the inhibition of constitutive spinal cyclooxygenase-2 (COX-2) but not COX-1. J Neurosci. 2001;21(16):5847–5853.
30. Max MB, Schafer SC, Culnane M, Dubner R, Gracely RH. Association of pain relief with drug side effects in postherpetic neuralgia: a single-dose study of clonidine, codeine, ibuprofen, and placebo. Clin Pharmacol Ther. 1988;43(4):363–371. doi:10.1038/clpt.1988.44
31. Cuzzocrea S, Mazzon E, Paola RD, et al. Effects of combination M40403 and dexamethasone therapy on joint disease in a rat model of collagen-induced arthritis. Arthritis Rheum. 2005;52(6):1929–1940. doi:10.1002/art.21211
32. Rodrigues-Filho R, Campos MM, Ferreira J, Santos AR, Bertelli JA, Calixto JB. Pharmacological characterisation of the rat brachial plexus avulsion model of neuropathic pain. Brain Res. 2004;1018(2):159–170. doi:10.1016/j.brainres.2004.05.058
33. Scholz J, Abele A, Marian C, et al. Low-dose methotrexate reduces peripheral nerve injury-evoked spinal microglial activation and neuropathic pain behavior in rats. Pain. 2008;138(1):130–142. doi:10.1016/j.pain.2007.11.019
34. Takeda K, Sawamura S, Sekiyama H, Tamai H, Hanaoka K. Effect of methylprednisolone on neuropathic pain and spinal glial activation in rats. Anesthesiology. 2004;100(5):1249–1257. doi:10.1097/00000542-200405000-00029
35. Bekemeier H, Hirschelmann R. On steroid-saving drug combinations in carrageenin paw edema and adjuvant arthritis. Arzneimittelforschung. 1986;36(10):1521–1524.
36. Buritova J, Honoré P, Chapman V, Besson JM. Enhanced effects of co-administered dexamethasone and diclofenac on inflammatory pain processing and associated spinal c-Fos expression in the rat. Pain. 1996;64(3):559–568. doi:10.1016/0304-3959(95)00167-0
37. Bamgbose BO, Akinwande JA, Adeyemo WL, Ladeinde AL, Arotiba GT, Ogunlewe MO. Effects of co-administered dexamethasone and diclofenac potassium on pain, swelling and trismus following third molar surgery. Head Face Med. 2005;1:11. doi:10.1186/1746-160X-1-11
38. Jarrah MH, Al-Rabadi HF, Imrayan M, Al-Share AA. Single dose of dexamethasone with or without ibuprofen effects on post-operative sequelae of lower third molar surgical extraction. J R Med Serv. 2015;22(1):41–45. doi:10.12816/0009785
39. Kataoka H, Horie Y, Koyama R, Nakatsugi S, Furukawa M. Interaction between NSAIDs and steroid in rat stomach: safety of nimesulide as a preferential COX-2 inhibitor in the stomach. Dig Dis Sci. 2000;45(7):1366–1375. doi:10.1023/a:1005560104847
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.