")
Back to Journals » International Journal of General Medicine » Volume 14
Clinicopathological Characteristics and Survival Predictions for Adenocarcinoma of the Esophagogastric Junction: A SEER Population-Based Retrospective Study
Authors Liu X , Jiang Q, Yue C, Wang Q
Received 11 October 2021
Accepted for publication 6 December 2021
Published 24 December 2021 Volume 2021:14 Pages 10303—10314
DOI https://doi.org/10.2147/IJGM.S341405
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Xin Liu,1,* Qingtao Jiang,2,* Chao Yue,3 Qin Wang2
1Department of Prevention and Control for Occupational Disease, Jiangsu Provincial Center for Disease Control and Prevention & Jiangsu Preventive Medicine Association, Nanjing, People’s Republic of China; 2Department of Clinical Medicine, Jiangsu Health Vocational College, Nanjing, People’s Republic of China; 3Department of General Surgery, Jiangsu Cancer Hospital & Jiangsu Institute of Cancer Research & The Affiliated Cancer Hospital of Nanjing Medical University, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chao Yue
Department of General Surgery, Jiangsu Cancer Hospital & Jiangsu Institute of Cancer Research & The Affiliated Cancer Hospital of Nanjing Medical University, 42 Baiziting Road, Nanjing, Jiangsu, People’s Republic of China
Email [email protected]
Qin Wang
Department of Clinical Medicine, Jiangsu Health Vocational College, 69 Huangshanling Road, Nanjing, Jiangsu, People’s Republic of China
Email [email protected]
Objective: Adenocarcinoma of the esophagogastric junction (AEJ) is a relatively rare malignancy in Western countries whose specific clinicopathological characteristics and associated prognosis have not been comprehensively described.
Methods: Data on patients with AEJ between 2005 and 2015 in the Surveillance, Epidemiology, and End Results (SEER) database were extracted, evaluated, and compared with patients with gastric cancer (GC) in general. Overall survival (OS) was evaluated using the Kaplan–Meier method. Univariate and multivariate analyses were performed using the Cox proportional hazards regression model to identify risk factors predictive for OS, and the results were used to construct a nomogram to predict 1-, 3-, and 5-year OS among patients with AEJ.
Results: A total of 8013 patients diagnosed with AEJ were identified from the records of 30,179 patients with GC. The mean age was 65.4 (SD = 12.0) years, 79.5% were men, 87.2% were Caucasian, 91.5% were moderately-to-poorly differentiated, 34.4% had AJCC stage I AEJ, and 28.8% had stage IV. The median OS was 18 months, and the 5-year OS was 25.8% (95% CI: 24.8– 26.8%). Fewer patients with AEJ had undergone surgical resection, fewer had T+ and N+ (N2∼N3) disease (P < 0.001), and fewer had distant metastases compared to the patients with GC (P < 0.05). In the univariate and multivariate analyses, age, race, summary stage, N stage, M stage, and surgery were identified as independent risk factors. The nomogram had a calibration index of 0.726.
Conclusion: AEJ was found to have distinct clinicopathological characteristics. Age, race, summary stage, N stage, M stage, and surgery were independently associated with OS. The nomogram accurately predicted 1-, 3-, and 5-year OS rates.
Keywords: adenocarcinoma of the esophagogastric junction, AEJ, clinicopathological characteristics, survival
Introduction
Adenocarcinoma of the esophagogastric junction (AEJ) has a high morbidity worldwide, with variable 5-year survival rates among institutions.1 An analysis of 43 cancer registries in Europe, Australia, the United States, and Canada conducted by Chevallay et al found a rapid rise in the incidence of AEJ in the last 20 years.2
AEJ is predominantly located at the distal esophagus and the esophagogastric junction (EJ) and represents 75% of esophageal cancers in the United States since the 1970s.3 The EJ has histological characteristics of both the esophageal squamous epithelium and gastric glandular cells. Considering this special anatomic location, the histological origin of AEJ as well as the appropriate treatments and prognosis are controversial.4,5 Previously, Mochizuki et al claimed, in their study, that the poor prognosis of AEJ is largely attributable to early and frequent metastases.6 However, a retrospective study of 1002 patients with AEJ conducted by Siewert et al found that the postoperative death rate depended on the surgical approach.7 For AEJ, both esophageal and stomach cancer staging systems have been used. Additional clinical and pathologic factors have also been suggested to improve the staging systems that are currently available.8,9 Matsuda et al examined the clinicopathological features, prognostic factors, and risk factors associated with each recurrence pattern.10 Ito et al distinguished AEJ subtypes by the clinicopathological and prognostic differentiation.11 Furthermore, Imamura and Wang et al developed models on immune and genomic characteristics associated with clinical phenotype as well as prognosis.12,13 However, there is no guidance or expert consensus on AEJs for clinical practice.
Given the distinct characteristics of AEJ, population-based analyses are critical to provide an overview of epidemiological and therapeutic trends. Therefore, this study aimed to review the clinical and pathological characteristics and survival rates of patients with AEJ from the Surveillance, Epidemiology, and End Results (SEER) database to better understand the factors that affect clinical behavior and survival.
Materials and Methods
Data Extraction
Data on patients with AEJ diagnosed and treated between 2005 and 2015 were extracted from the SEER database (http://seer.cancer.gov/) using SEER*Stat software (version 8.3.8; https://seer.cancer.gov/seerstat/). The study cohort included patients identified by the Site and Morphology term “EsophagusGEJunction”. All eligible patients had a single primary tumor (sequence number 0 or 1), histologically confirmed malignant AEJ, data on age and race, and no missing follow-up data. Signed authorization and permission to access and use the dataset were obtained from the SEER. Approval was waived by the Ethics Committee of Jiangsu Provincial Center for Disease Control and Prevention, as the SEER data were publicly available and de-identified.
Characteristic Variables and Survival Data
The baseline characteristics of patients were obtained from the following datasets: age, sex, race, year of diagnosis, primary site, tumor size, TNM and histological stages, surgical resection (yes or no), survival data, and vital status. The TNM stage was manually adjusted according to the AJCC eighth edition criteria. Patient age at diagnosis was converted to 10-year intervals to construct the Cox regression-based analysis. The primary endpoint of this analysis was OS derived from vital status and months of survival, which was calculated from the day of surgery to the last follow-up or death. Patients who survived less than 1 month were coded in the SEER database as having a survival time of zero.
Statistical Analysis
To investigate the clinicopathological characteristics of the study population, the Student’s t-test, χ2 test (or Fisher’s exact test), and the Mann–Whitney method were used. Survival analyses were evaluated using Kaplan-Meier estimates with the Log rank test, with OS as the primary outcome. Cox proportional hazard regression models, including univariate analysis (UVA) and multivariate analysis (MVA), were adopted to calculate hazard ratios (HRs) and 95% confidence intervals (95% CIs) to assess the impact of clinical indicators on patient outcomes. A nomogram was generated based on the MVA results. The concordance index (c-index) and calibration plots were used to evaluate the model performance. The c-index statistic ranged from 0.5 (no discrimination) to 1 (perfect discrimination). Nomogram plot calibration was performed to estimate the overall agreement between predicted and observed survival. Statistical analyses were performed by R 4.0.0 (http://www.r-project.org/) using survival, rms, and ggplot2 packages. Statistical significance was set at a two-sided P-value < 0.05.
Results
Patients’ Demographic and Pathological Characteristics
A total of 30,179 eligible patients with gastric cancer (GC) were identified in the SEER database, including 8013 (26.6%) with AEJ. As shown in Table 1, there were 6371 men and 1642 women (mean age, 65.4 ± 12.0 years) with AEJ. The majority (6989; 87.2%) were Caucasian. The most common AEJ site was the cardia (7934 patients; 99.0%) with a median size of 40.0 mm and an interquartile range (IQR) of 24.0–55.0 mm. Regarding the histological grades, 7.0% and 39.1% had grades I and II (well or moderately differentiated), 52.4% had grade III (poorly differentiated), and 1.5% had grade IV (undifferentiated). Tumor development was categorized by summary stage as localized (27.8%), regional (43.7%), or distant (28.5%). Most patients (34.4%) had AJCC stage I, 28.8% had stage IV, 21.5% had stage II, and 15.4% had stage III. Fewer patients with AEJ had undergone surgical resection, had T+ and N+ (N2~N3) disease (P < 0.001), and had distant metastases compared to the patients with GC (P < 0.05).
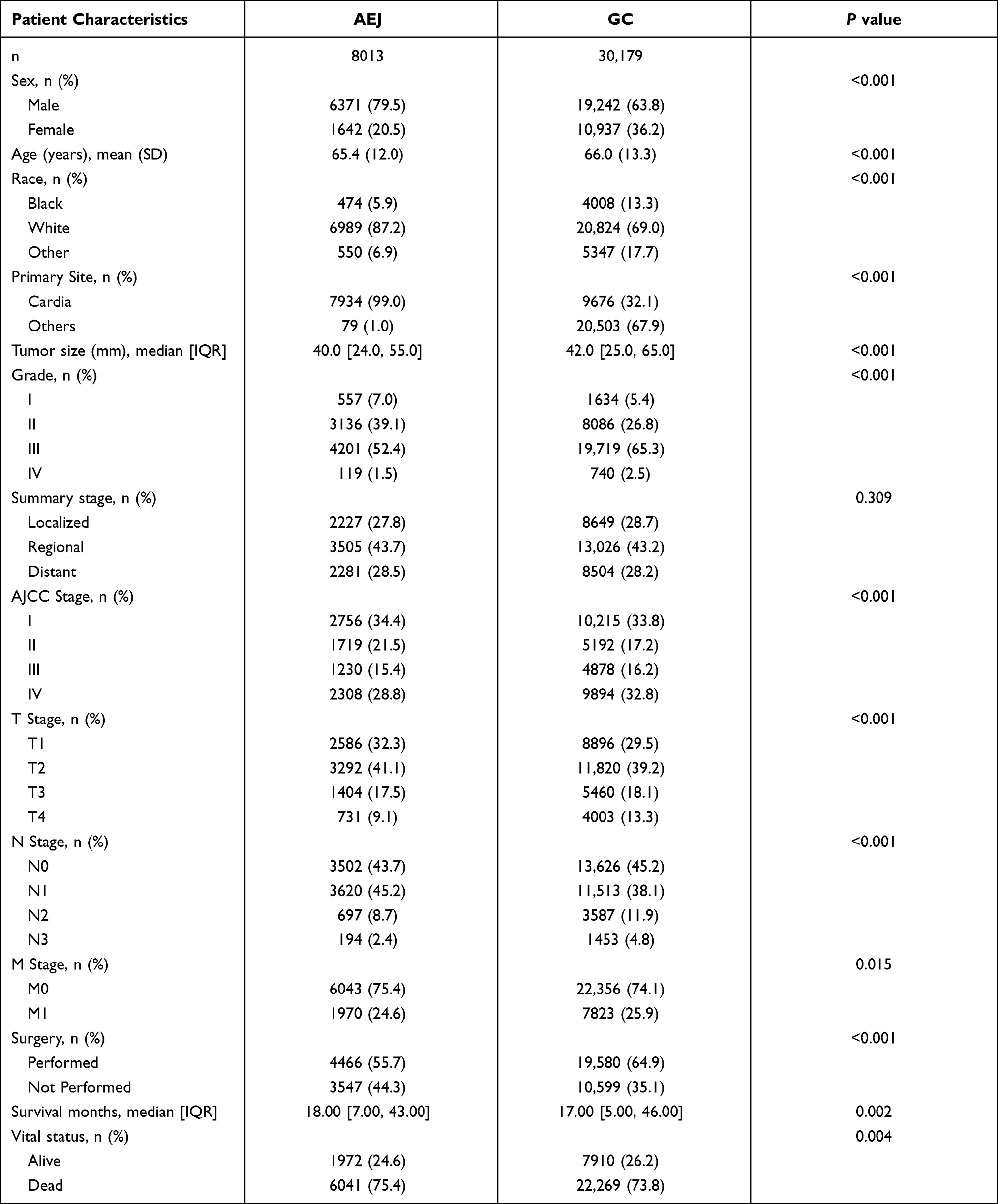 |
Table 1 Baseline Characteristics of AEJ and GC Patients |
Survival
The median OS of the 8013 patients with AEJ in the current study was 18 months, and the 5-year OS was 25.8% (95% CI: 24.8–26.8%). In the GC cohort, the median OS was 17 months, with a 5-year OS of 27.8% (95% CI: 27.3–28.3%). The Kaplan-Meier curve for OS is shown in Figure 1. A total of 6041 patients died during the follow-up period, and 4920 deaths were primary cancer-specific, attributable to AEJ. The remaining 1121 patients died from other causes, including heart disease (21.8%) and various complications.
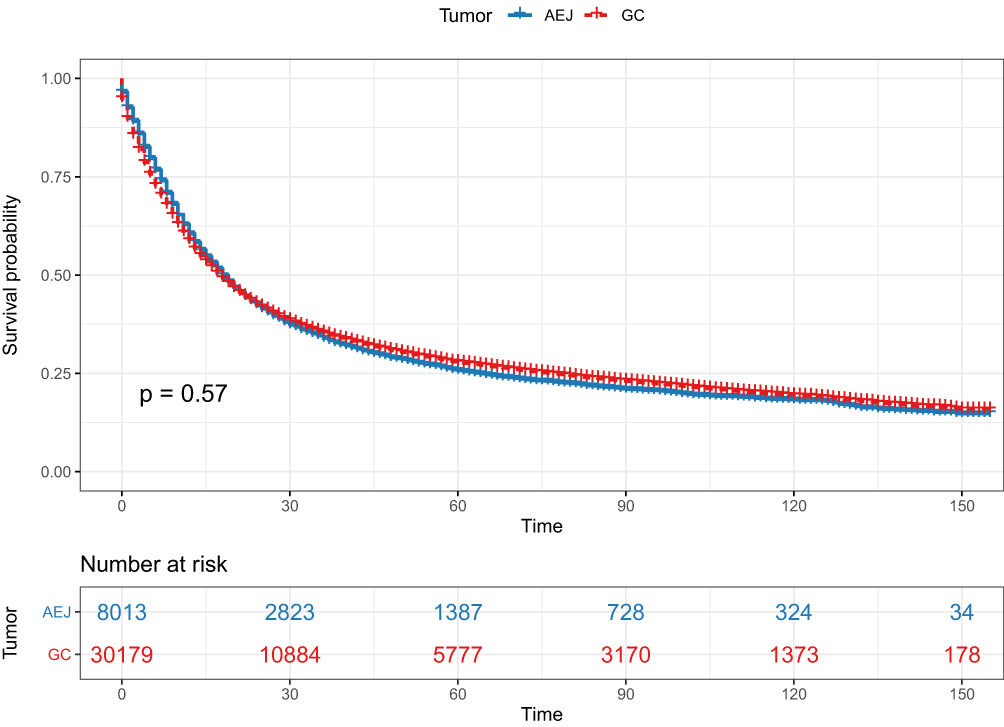 |
Figure 1 Kaplan-Meier estimate of overall survival in adenocarcinoma of the esophagogastric junction (AEJ) and gastric cancer (GC) patients. |
The cumulative survival of patients among the groups is shown in Figure 2. The likelihood of survival for patients aged < 45, 45–54, 55–64, 65–74, 75–84, and > 84 years differed significantly among the groups (P < 0.0001, Figure 2A), with OS noticeably worse in patients aged > 75 years compared to the other groups. Sex had a non-significant influence on OS (P = 0.690, Figure 2B), and African-Americans had the worst prognosis among the races studied (P < 0.0001, Figure 2C).
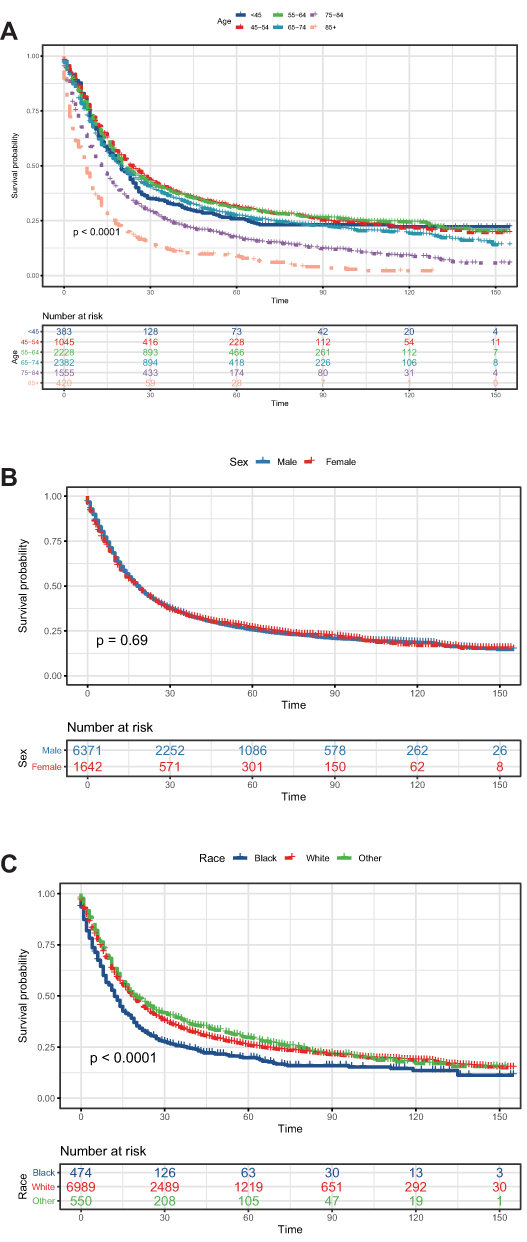 |
Figure 2 Kaplan-Meier estimate of overall survival of patients by (A) age, (B) sex, (C) race. |
The data indicated that patients with AEJ originating from the cardia had better survival compared to those with AEJ originating from other sites (P = 0.0052, Figure 3A). However, patients with tumor cells that had spread to other sites had worse survival than those with local growth (P < 0.0001, Figure 3B).
 |
Figure 3 Kaplan-Meier estimate of overall survival of patients by (A) primary site, (B) summary stage. |
The OS varied significantly according to histological grade and AJCC stage (P < 0.001, Figure 4A and B), clearly revealing a worse outcome for patients with advanced disease. As shown in Figure 4C, patients who underwent surgery had a significantly more favorable OS compared to those who did not (P < 0.0001). The median survival was 32 months, and the 5-year OS was 41.3% (95% CI: 39.8–42.9%) in patients who underwent surgery. The corresponding values were 8 months and 6.1% (95% CI: 5.3–7.0%) for those who did not undergo surgery.
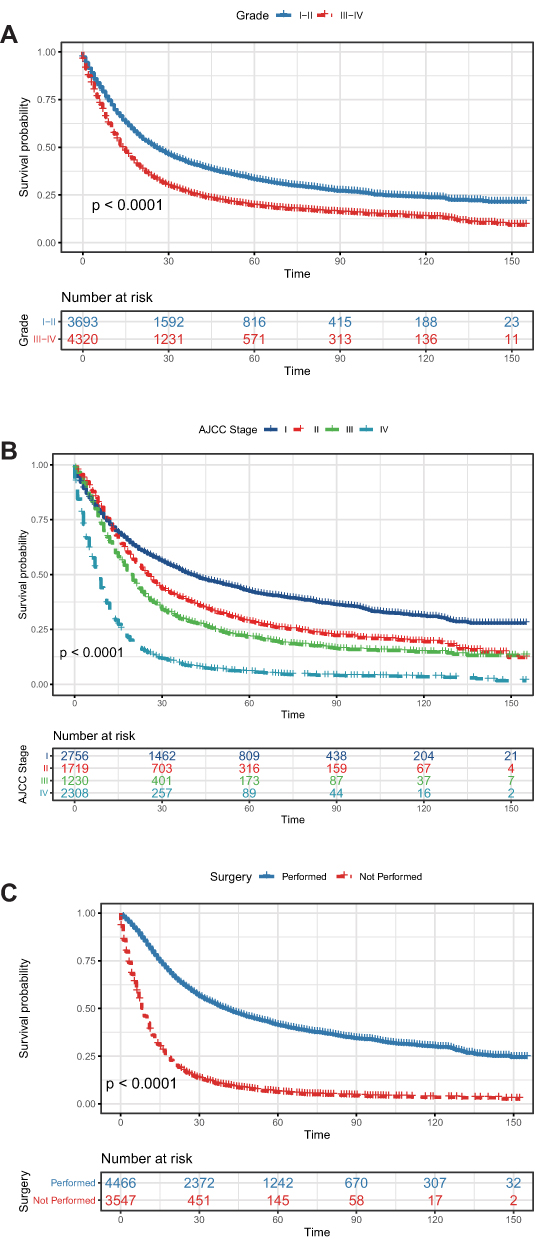 |
Figure 4 Kaplan-Meier estimate of overall survival in patients categorized by (A) grade, (B) AJCC stage, (C) surgery. |
The MVA included all covariates with a P-value < 0.10 in the UVA. Due to the potential correlation with TNM stage, the AJCC stage was not included in the MVA to avoid collinearity among the factors. The results of the UVA and MVA Cox proportional hazards regression models are presented in Table 2. Age (P < 0.001), race (P = 0.035), summary stage (P = 0.001), N stage (P = 0.020), M stage (P < 0.001), and surgery (P < 0.001) were independent predictors of survival.
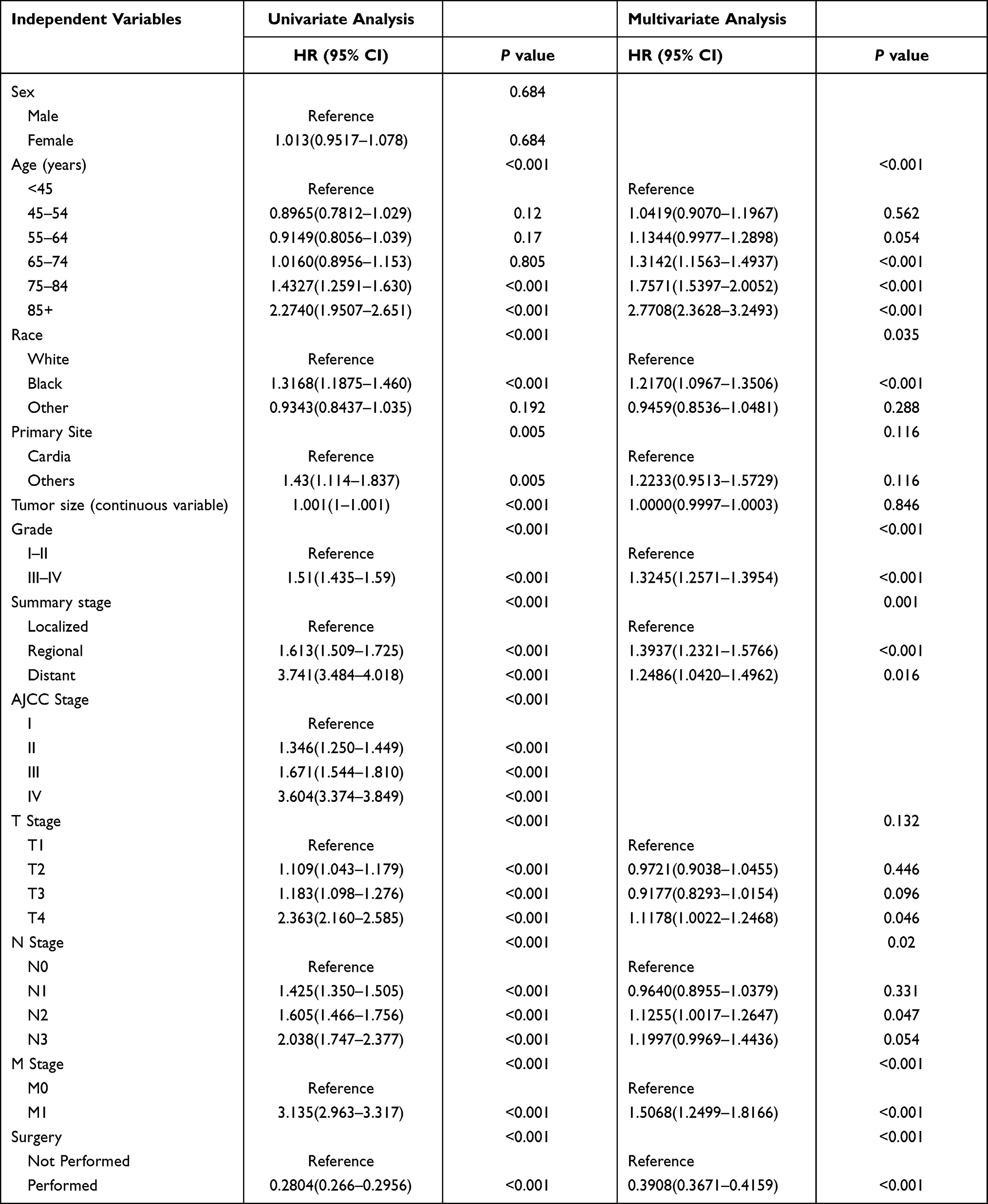 |
Table 2 Univariate and Multivariate Cox Proportional Hazards Analysis |
The nomogram generated using the variables independently associated with survival is shown in Figure 5. The estimated probability of 1-, 3-, and 5-year survival was calculated by combining the points corresponding to the patient’s characteristics. The nomogram had a c-index of 0.726, indicating a good discriminative capacity. Calibration plots of the nomogram prediction accuracy are shown in Figure 6, showing good agreement between the actual and presumptive 1-, 3-, and 5-year OS, with a slope close to 45°.
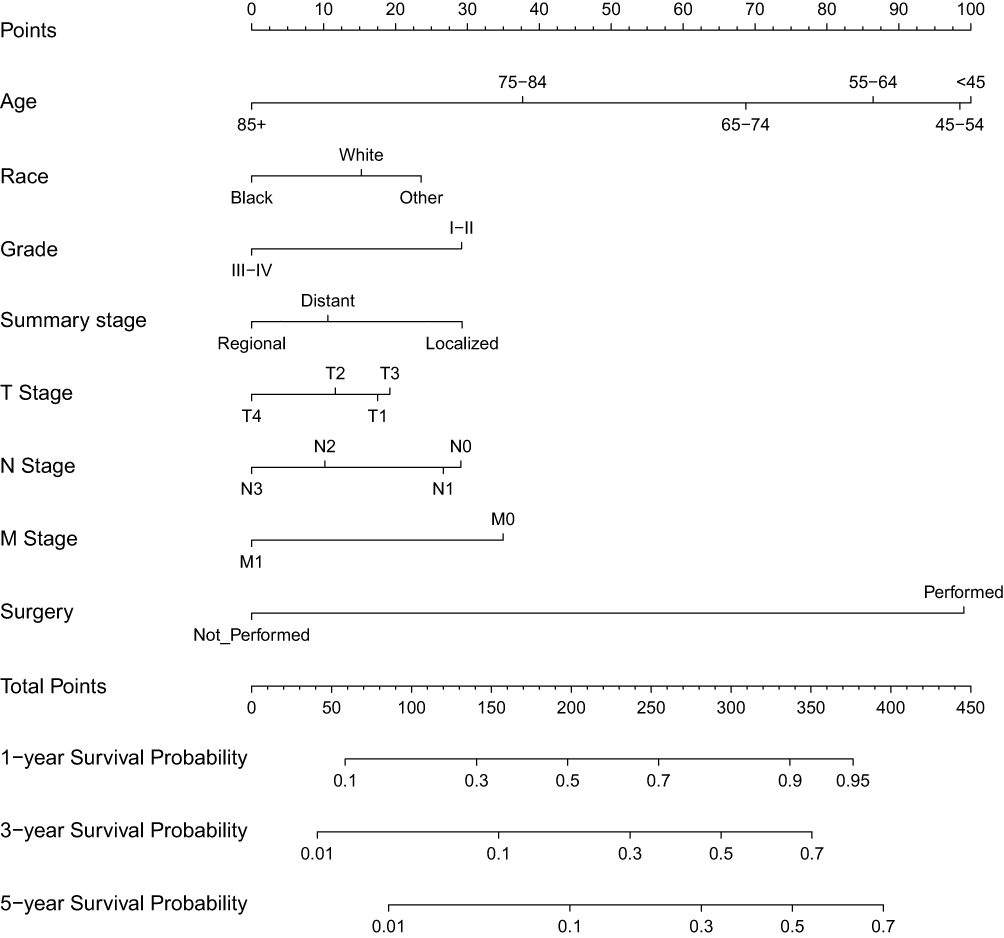 |
Figure 5 Nomogram to predict 1-, 3-, and 5-year overall survival of patients with adenocarcinoma of the esophagogastric junction (AEJ). |
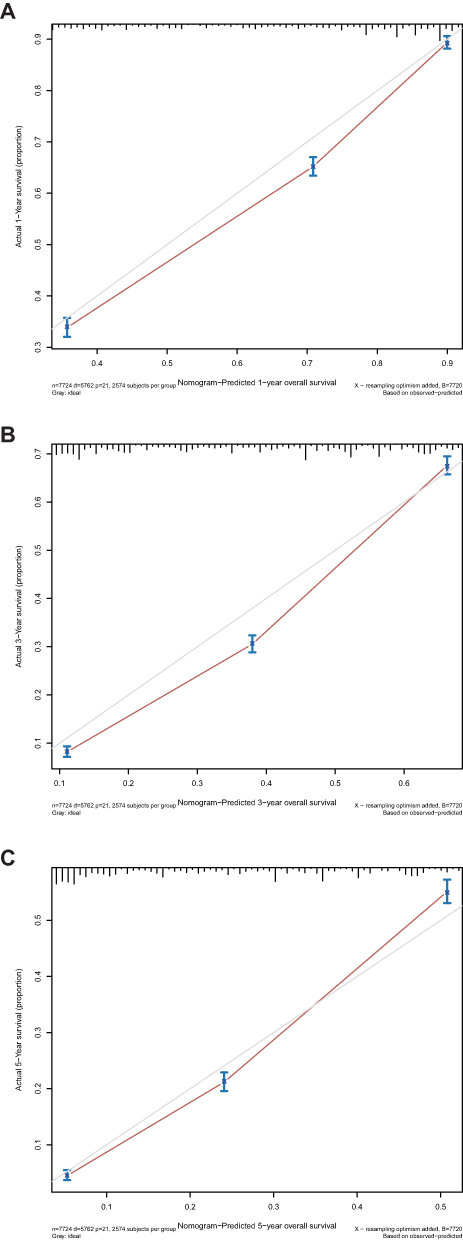 |
Figure 6 Calibration plots of the nomogram prediction of (A) 1-year, (B) 3-year, and (C) 5-year overall survival in adenocarcinoma of the esophagogastric junction (AEJ) patients. The red line represents equality of the observed and predicted probability. |
Discussion
AEJ is on the rise worldwide, but its clinical features have not been independently profiled and reported, potentially limiting appropriate treatment plans and impeding the development of drugs to manage this malignancy. Due to its location between the esophagus and stomach, the staging of AEJ as gastric or esophageal carcinoma is controversial.14 Siewert and Stein defined AEJ as a tumor with an epicenter < 5 cm from the anatomic location of the EJ.15 Traditionally, cardia cancer refers to a cancer found 2 cm proximal or distal to the junction.16 Therefore, AEJ covers a wider area than traditional cardia cancers. This is reflected in the vast differences in surgical approaches and long-term survival rates after surgical resection.17,18
A large cohort of 8013 patients with AEJ included in the SEER database was currently analyzed. The aim of this study was to comprehensively decipher the clinicopathological characteristics of patients with AEJ compared to those of other GC populations. Age, race, summary stage, N stage, M stage, and surgery were found to be independently associated with survival. Moreover, a nomogram derived from the Cox regression model was built to accurately predict the prognosis of patients with AEJ in the study cohort.
Of the patients with GC retrieved from the SEER database, 26.6% had AEJ. In the study population, the mean age at diagnosis was 65.4 years, and 79.5% of all patients with AEJ were male which is in consistent with the research by Matsuda et al, indicating that males may have a strong predisposition to developing AEJ.10 Clinical characteristics that were reported as unique to AEJ in this study included Caucasian race, moderate-to-poor differentiation, less T+ and N+ (N2~N3) disease, fewer distant metastases, and more frequent treatment with surgical resection. Interestingly, Chen et al and Dong et al also confirmed that patients suffering from AEJ usually have a higher incidence of lymph node or hematogenous metastases.19,20
We found no difference in the OS between patients with AEJ and those with GC overall. The median OS of the patients with AEJ in this study was 18 months vs 17 months in those with GC, which was not significant probably due to lack of case-matching analysis. Patients with AEJ had a poor prognosis even when early-stage disease was treated effectively. The median OS for advanced-stage AEJ was extremely poor, at 19 months for AJCC stage III, and 8 months for AJCC stage IV, and a sharp decrease in the likelihood of survival in the first year after diagnosis.
Age, race, summary stage, N stage, M stage, and surgery remained significantly associated with survival in the MVA, which is consistent with previous studies. Zhang et al retrospectively reviewed 382 consecutive patients with AEJ and found that lymph node metastasis, lymphovascular invasion, and age were significant and independent factors of poor prognosis after the complete tumor resection (R0 resection) of AEJ.21 Al-Refaie et al reported a worse outcome in black patients of gastric adenocarcinoma and the explanation for such disparity is not clear. The differences in socioeconomic status, access to care and response to cancer therapy may be underlying contributors.22 Furthermore, Siewert et al demonstrated that R0 resection and lymph node status (pN0) were the dominant independent prognostic factors for the entire patient population, irrespective of the surgical approach.7 Subsequently, the Cox regression results were applied to construct a nomogram to predict 1-, 3-, and 5-year OS, which is a convenient statistical tool that can be used to accurately forecast individual risk and has been widely established clinically as a measure to estimate the prognosis of several cancers. The nomogram showed that surgery had the strongest impact on OS. However, the high predictive accuracy of a nomogram might not always be clinically relevant. Therefore, the effect of nomogram-assisted clinical decision-making on patient survival needs to be assessed.23,24
Our study included over 10 years of cases from the SEER database and is currently the largest cohort study on AEJ. We systematically and comprehensively illustrated the clinical features and prognostic factors of AEJ. However, this study also had some limitations, including the lack of data on recurrence and the presence of genetic mutations in the SEER records. In addition, the treatment variables that influenced prognosis could not be fully evaluated because complete information on surgical procedures, chemotherapy regimens, and radiation dose/technology were not available on the SEER registries. Other studies have reported that the postoperative death rate after esophagectomy is higher than that after extended total gastrectomy.25–27 Lin et al revealed that genomic and transcriptomic changes in AEJ for Chinese patients could be associated with drug vulnerability and survival.28 Currently, the most problematic unresolved issue for oncologists is the effect of tumor staging and surgical procedures (and their interaction) on patient prognosis.29–31 More detailed clinical data and accurate epidemiological measures are needed to assist doctors with clinical judgment and decision-making.
Conclusions
AEJ has clinicopathological characteristics that are distinct from other GCs, including a predominance of males and Caucasians, moderate-to-poor differentiation, less T+ and N+ (N2~N3) disease, fewer distant metastases, and more frequent treatment by surgical resection. Age, race, summary stage, N stage, M stage, and surgery were independently associated with OS. A nomogram could be used to effectively predict the 1-, 3-, and 5-year OS of these patients.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author (Chao Yue).
Ethical Statement
As SEER data is publicly available and de-identified, the IRB exemption is granted by Jiangsu Provincial Center for Disease Control and Prevention.
Funding
This work was supported by Natural Science Foundation of Jiangsu Province (BK20151017), Six Talent Peaks Project in Jiangsu Province (WSW-050), National Natural Science Foundation of China (81502052), Qinglan Talents Project of Jiangsu Province and Natural Science Project in Colleges and universities of Jiangsu Province (21KJD320006).
Disclosure
The authors have no conflicts of interest to declare.
References
1. Greally M, Agarwal R, Ilson DH. Optimal management of gastroesophageal junction cancer. Cancer. 2019;125(12):1990–2001. doi:10.1002/cncr.32066
2. Chevallay M, Bollschweiler E, Chandramohan SM, et al. Cancer of the gastroesophageal junction: a diagnosis, classification, and management review. Ann N Y Acad Sci. 2018;1434(1):132–138. doi:10.1111/nyas.13954
3. Chiappa A, Andreoni B, Dionigi R, et al. A rationale multidisciplinary approach for treatment of esophageal and gastroesophageal junction cancer: accurate review of management and perspectives. Crit Rev Oncol Hematol. 2018;132:161–168. doi:10.1016/j.critrevonc.2018.10.002
4. Lagarde SM, Ten Kate FJ, Reitsma JB, et al. Prognostic factors in adenocarcinoma of the esophagus or gastroesophageal junction. Am J Clin Oncol. 2006;24(26):4347–4355. doi:10.1200/JCO.2005.04.9445
5. Anker CJ, Dragovic J, Herman JM, et al. Executive summary of the American Radium Society appropriate use criteria for operable esophageal and gastroesophageal junction adenocarcinoma: systematic review and guidelines. Int J Radiat Oncol Biol Phys. 2021;109(1):186–200. doi:10.1016/j.ijrobp.2020.08.050
6. Mochizuki K, Kondo T, Oishi N, et al. Esophagogastric junction carcinomas - discriminating histological types through immunohistochemistry. Anticancer Res. 2017;37(12):6855–6861. doi:10.21873/anticanres.12147
7. Rudiger Siewert J, Feith M, Werner M, et al. Adenocarcinoma of the esophagogastric junction: results of surgical therapy based on anatomical/topographic classification in 1002 consecutive patients. Ann Surg. 2000;232(3):353–361. doi:10.1097/00000658-200009000-00007
8. Lagarde SM, Ten Kate FJ, Richel DJ, et al. Molecular prognostic factors in adenocarcinoma of the esophagus and gastroesophageal junction. Ann Surg Oncol. 2007;14(2):977–991. doi:10.1245/s10434-006-9262-y
9. Abdi E, Latifi-Navid S, Zahri S, et al. Risk factors predisposing to cardia gastric adenocarcinoma: insights and new perspectives. Cancer Med. 2019;8(13):6114–6126. doi:10.1002/cam4.2497
10. Matsuda T, Kurokawa Y, Yoshikawa T, et al. Clinicopathological characteristics and prognostic factors of patients with Siewert Type II esophagogastric junction carcinoma: a Retrospective Multicenter Study. World J Surg. 2016;40(7):1672–1679. doi:10.1007/s00268-016-3451-z
11. Ito H, Inoue H, Odaka N, et al. Clinicopathological characteristics and optimal management for esophagogastric junctional cancer; a single center retrospective cohort study. J Exp Clin Cancer Res. 2013;32:2. doi:10.1186/1756-9966-32-2
12. Imamura Y, Toihata T, Haraguchi I, et al. Immunogenic characteristics of microsatellite instability-low esophagogastric junction adenocarcinoma based on clinicopathological, molecular, immunological and survival analyses. Int j Cancer. 2021;148(5):1260–1275. doi:10.1002/ijc.33322
13. Wang Y, Wang S, Zhu C, et al. The association between immune characteristic and clinical pathology in Chinese patients with adenocarcinoma of esophagogastric junction. Cancer Manag Res. 2020;12:3259–3269. doi:10.2147/CMAR.S235722
14. Imamura Y, Watanabe M, Oki E, et al. Esophagogastric junction adenocarcinoma shares characteristics with gastric adenocarcinoma: literature review and retrospective multicenter cohort study. Ann Gastroenterol Surg. 2021;5(1):46–59. doi:10.1002/ags3.12406
15. Siewert JR, Stein HJ. Classification of adenocarcinoma of the oesophagogastric junction. Br J Surg. 1998;85(11):1457–1459. doi:10.1046/j.1365-2168.1998.00940.x
16. Swisher SG, Pisters PW, Komaki R, et al. Gastroesophageal junction adenocarcinoma. Curr Treat Options Oncol. 2000;1(5):387–398. doi:10.1007/s11864-000-0066-1
17. Jung MK, Schmidt T, Chon SH, et al. Current surgical treatment standards for esophageal and esophagogastric junction cancer. Ann N Y Acad Sci. 2020;1482(1):77–84. doi:10.1111/nyas.14454
18. Nunobe S, Ida S. Current status of proximal gastrectomy for gastric and esophagogastric junctional cancer: a review. Ann Gastroenterol Surg. 2020;4(5):498–504. doi:10.1002/ags3.12365
19. Chen K, Deng X, Yang Z, et al. Survival nomogram for patients with metastatic Siewert type II adenocarcinoma of the esophagogastric junction: a population-based study. Expert Rev Gastroenterol Hepatol. 2020;14(8):757–764. doi:10.1080/17474124.2020.1784726
20. Dong H, Guo H, Xie L, et al. The metastasis-associated gene MTA3, a component of the Mi-2/NuRD transcriptional repression complex, predicts prognosis of gastroesophageal junction adenocarcinoma. PLoS One. 2013;8(5):e62986. doi:10.1371/journal.pone.0062986
21. Zhang H, Wang W, Cheng Y, et al. Adenocarcinomas of the esophagogastric junction: experiences at a single institution in China. World J Surg Oncol. 2013;11:155. doi:10.1186/1477-7819-11-155
22. Al-Refaie WB, Tseng JF, Gay G, et al. The impact of ethnicity on the presentation and prognosis of patients with gastric adenocarcinoma. Results from the national cancer data base. Cancer. 2008;113(3):461–469.
23. Zhong X, Xuan F, Qian Y, et al. A genomic-clinicopathologic Nomogram for the preoperative prediction of lymph node metastasis in gastric cancer. BMC Cancer. 2021;21(1):455.
24. Rubenstein JH, Raghunathan T, Doan C, et al. Validation of tools for predicting incident adenocarcinoma of the esophagus or esophagogastric junction. Am J Gastroenterol. 2021;116(5):949–957. doi:10.14309/ajg.0000000000001255
25. Graham AJ, Finley RJ, Clifton JC, et al. Surgical management of adenocarcinoma of the cardia. Am J Surg. 1998;175(5):418–421. doi:10.1016/S0002-9610(98)00040-3
26. Parshad R, Singh RK, Kumar A, et al. Adenocarcinoma of distal esophagus and gastroesophageal junction: long-term results of surgical treatment in a North Indian Center. World J Surg. 1999;23(3):277–283. doi:10.1007/PL00013179
27. Ellis FH
28. Lin Y, Luo Y, Sun Y, et al. Genomic and transcriptomic alterations associated with drug vulnerabilities and prognosis in adenocarcinoma at the gastroesophageal junction. Nat Commun. 2020;11(1):6091. doi:10.1038/s41467-020-19949-6
29. DeCesaris CM, Berger M, Choi JI, et al. Pathologic complete response (pCR) rates and outcomes after neoadjuvant chemoradiotherapy with proton or photon radiation for adenocarcinomas of the esophagus and gastroesophageal junction. J Gastrointest Oncol. 2020;11(4):663–673. doi:10.21037/jgo-20-205
30. Narayan RR, Poultsides GA. Advances in the surgical management of gastric and gastroesophageal junction cancer. Transl Gastroenterol Hepatol. 2021;6:16. doi:10.21037/tgh.2020.02.06
31. Schirren R, Novotny A, Slotta-Huspenina J, et al. Novel histologic categorization based on Lauren histotypes conveys prognostic information for gastroesophageal junction cancers-analysis from a large single center cohort in Germany. Cancers. 2021;13(6):1303.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.