")
Back to Journals » Biologics: Targets and Therapy » Volume 13
Clinical utility of ramucirumab in non-small-cell lung cancer
Authors Uprety D
Received 4 March 2019
Accepted for publication 6 July 2019
Published 22 July 2019 Volume 2019:13 Pages 133—137
DOI https://doi.org/10.2147/BTT.S175034
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Doris Benbrook
Dipesh Uprety
Department of Medical Oncology, Mayo Clinic, Rochester, MN, USA
Abstract: Lung cancer is the leading cause of cancer-related mortality worldwide. Non-small-cell lung cancer (NSCLC) accounts for about 85% of all lung cancer cases and approximately 70% of patients with NSCLC have locally advanced or metastatic disease at presentation. In NSCLC patients with advanced or metastatic disease, second line treatment with chemotherapy is associated with a poor response rate. In this article, we have reviewed the role of ramucirumab in patients with NSCLC. Ramucirumab is not current standard of care in the first line setting in the treatment of advanced or metastatic NSCLC, based on phase II data which did not show any progression-free survival (PFS) and overall survival (OS) benefit when ramucirumab was compared with non-ramucirumab arm. The REVEL study was a phase III, placebo-controlled trial which included patients with stage IV NSCLC who had progressed during or after platinum-based chemotherapy, with or without bevacizumab. Median OS was 9.1 months vs 10.5 months (HR 0.86, 95% CI 0.75–0.98) in the placebo and ramucirumab group respectively. Seventy-nine percent of patients in ramucirumab arm and 71% of patients in non-ramucirumab arm had grade ≥3 treatment-related adverse events. The addition of ramucirumab to docetaxel can be considered in younger patients with good performance status as a second line treatment option. Additionally, combined blockage of the VEGFR and EGFR pathway has been utilized to overcome resistance to EGFR therapy. The RELAY trial was a phase III, placebo-controlled trial which included patients with sensitizing EGFR mutation positive stage IV NSCLC. Patients were randomized to either ramucirumab plus erlotinib or erlotinib. The trial showed that the combination therapy showed superior PFS benefit.
Keywords: ramucirumab, non-small-cell lung cancer, NSCLC
Background
Lung cancer is the leading cause of cancer incidence and cancer-related mortality worldwide.1 It remains a highly fatal disease with an average 5-year survival, at best, of 15% in the US.1 Non-small-cell lung cancer (NSCLC) accounts for about 85% of all lung cancer cases and approximately 70% of patients with NSCLC have locally advanced or metastatic disease at presentation.2,3 For patients with locally advanced or metastatic disease and an actionable driver mutation (EGFR, ALK, ROS1, BRAF, and NTRK), targeted therapy is the current standard of care.4 However, a significant number of patients lack actionable mutation. Chemotherapy in the form of platinum doublet used to be the standard of care for these patients with docetaxel as one of the second line treatment options. Second line chemotherapy was associated with poor response rate (<10%) and a median survival of 8 months at best.5,6 In 2015, the US Food and Drug Administration approved nivolumab based on two large, randomized, phase III trials which showed longer overall survival (OS) with nivolumab than with docetaxel.7,8 Since its approval, two other check-point inhibitors, namely, atezolizumab and pembrolizumab (for PD-L1≥1%) were also approved in second line settings for patients with advanced or metastatic NSCLC.9,10 With the arrival of immunotherapy, it was felt that the docetaxel-based treatment regimen would no longer be utilized. Recently, pembrolizumab plus platinum doublet became the preferred treatment option for patients who do not have actionable driver mutation, based on data from two landmark studies, namely, KEYNOTE-189 and KEYNOTE-407.11,12 The survival benefit with chemotherapy plus immunotherapy was seen irrespective of PD-L1 expression. Pembrolizumab monotherapy is an option for those with high PD-L1 expression of ≥50%. This is based on the KEYNOTE-024 study which showed significant survival benefit with pembrolizumab as compared with standard platinum doublet.13 Platinum doublet plus atezolizumab plus bevacizumab is another preferred treatment option for these subsets of patients, based on recent data from the IMPOWER 150 trial. This study showed significant survival benefit with the addition of atezolizumab to bevacizumab plus platinum doublet.14 Almost all patients with locally advanced or metastatic NSCLC will now be treated with a combination of chemotherapy and immunotherapy in coming months. Unfortunately, 40%–50% of patients will not respond to the combination chemo-immunotherapy and the majority of them will progress in the future, thus necessitating second line treatment. There is therefore a substantial need for second line treatment options in patients with advanced NSCLC. In this article, we will focus on the role of ramucirumab in patients with NSCLC.
Angiogenesis is an important step in cancer proliferation and growth. VEGF is one of the most important factors associated with angiogenesis; its inhibition can suppress tumor growth.15 Ramucirumab is a recombinant monoclonal antibody of immunoglobulin G1 class that targets the extracellular domain of VEGFR-2.16 VEGFR-2 is significantly upregulated in tumor vasculature in the majority of solid cancers including lung, liver, colorectal, stomach, etc.17 By blocking VEGFR-2, ramucirumab prevents tumor angiogenesis and growth.18,19 As a second line agent, ramucirumab has shown significant survival benefit in patients with gastric cancer either alone or in combination with paclitaxel.20,21 It also has clinical utility in patients with colorectal cancer, hepatocellular cancer, and NSCLC.
Two randomized trials have evaluated ramucirumab in patients with treatment-naïve advanced or metastatic NSCLC.22,23 A study by Camidge et al was a phase II, multi-center, open-label, single-arm study.22 Forty patients with histologically confirmed stage IIIB or IV NSCLC were enrolled in the study. Each of these patients received ramucirumab at the dose of 10 mg/kg via intravenous infusion in addition to standard platinum doublet (carboplatin-paclitaxel) every 3 weeks. The treatment continued for up to six cycles or until there was evidence of disease progression or intolerable toxicity. The overall response rate (ORR) was 55% including, 52.5% (n=21) partial response, 35.0% (n=14) stable disease, and only one patient achieved a complete response. Median progression-free survival (PFS) was 7.85 months and median OS was 16.85 months. Eighty-five percent of patients (n=35) experienced treatment-related adverse effects. Most of them were either grade 2 or 3 and the most common events were fatigue, peripheral neuropathy, nausea, epistaxis, and myalgia. Of note, there was no grade ≥3 hemoptysis reported in this study. Doebele et al's study was a phase II, randomized, open-label, multi-center study23 which enrolled 140 patients with histologically confirmed stage IV NSCLC. Non-squamous NSCLC patients were randomized in a 1:1 fashion to either receive platinum doublet (pemetrexed plus carboplatin or cisplatin) or platinum doublet with ramucirumab every 3 weeks for up to 4–6 cycles. Maintenance therapy included pemetrexed with or without ramucirumab. Squamous NSCLC patients received gemcitabine instead of pemetrexed and half of the patients received maintenance ramucirumab. The ORR, PFS, and OS were not significantly different between the two arms: ORR was 49.3% vs 38.0% (p=0.1797), Median PFS was 7.2 vs 5.6 months (p=0.1318), median OS was 13.9 vs 10.4 months (p=0.8916) in the ramucirumab and non-ramucirumab arm respectively. Ramucirumab is therefore not a current standard of care in the first line setting in the treatment of advanced or metastatic NSCLC.
The REVEL study was a phase III, multi-center, randomized, double-blind, placebo controlled study which included patients with pathologically confirmed stage IV NSCLC who have progressed during or after platinum-based chemotherapy, with or without bevacizumab.24 A total of 1,253 patients were randomized in 1:1 fashion to either receive docetaxel with placebo (n=628) or docetaxel with ramucirumab (n=625) every 3 weeks. The ORR was 14% vs 23% (OR 1.89, 95% CI 1.41–2.54, p<0.0001), median PFS was 3.0 months vs 4.5 months (HR 0.76, 95% CI 0.68–0.86), and median OS was 9.1 months vs 10.5 months (HR 0.86, 95% CI 0.75–0.98) in the placebo and ramucirumab group respectively. Most of the subgroups had better survival with ramucirumab, although the study was not powered for subgroup analysis. Of note, there was no obvious benefit of ramucirumab in elderly patients and this was not fully related to toxicity. Seventy-nine percent of patients in ramucirumab arm and 71% of patients in non-ramucirumab arm experienced grade ≥3 treatment-related adverse events. Thirty-seven percent of patients (n=231) in ramucirumab group had grade 4 neutropenia as compared to 28% in the non-ramucirumab group. Also, incidence of febrile neutropenia, hospital admission for febrile neutropenia, and incidence of anemia were higher in ramucirumab group. Also, patients in ramucirumab arm had more bleeding, fatigue, stomatitis, mucosal inflammation, and dysgeusia. There was no difference in gastrointestinal and respiratory tract bleeding events between the two groups. Based on an improvement in survival with a net gain of 1.4 months, the US Food and Drug Administration approved ramucirumab for use in conjunction with docetaxel for patients with metastatic NSCLC with disease progression on or after platinum doublet chemotherapy, on December 12, 2014. It is a category 2A recommendation as per National Comprehensive Cancer Network and category I, B recommendation as per the European Society for Medical Oncology.4,25 Given the survival benefit of only 1.4 months and increased toxicity profile, many clinicians believe that these data are only statistically significant without any meaningful clinical benefit and hence shy away from this combination. The addition of ramucirumab to docetaxel should therefore be individualized to younger patients with good performance status. The findings of the previously mentioned three trials are summarized in Table 1. Docetaxel in combination with nintedanib (especially in patients with adenocarcinoma) or paclitaxel in combination with bevacizumab could also be potential therapeutic options, especially after disease progression on combination chemo-immunotherapy treatment.26,27
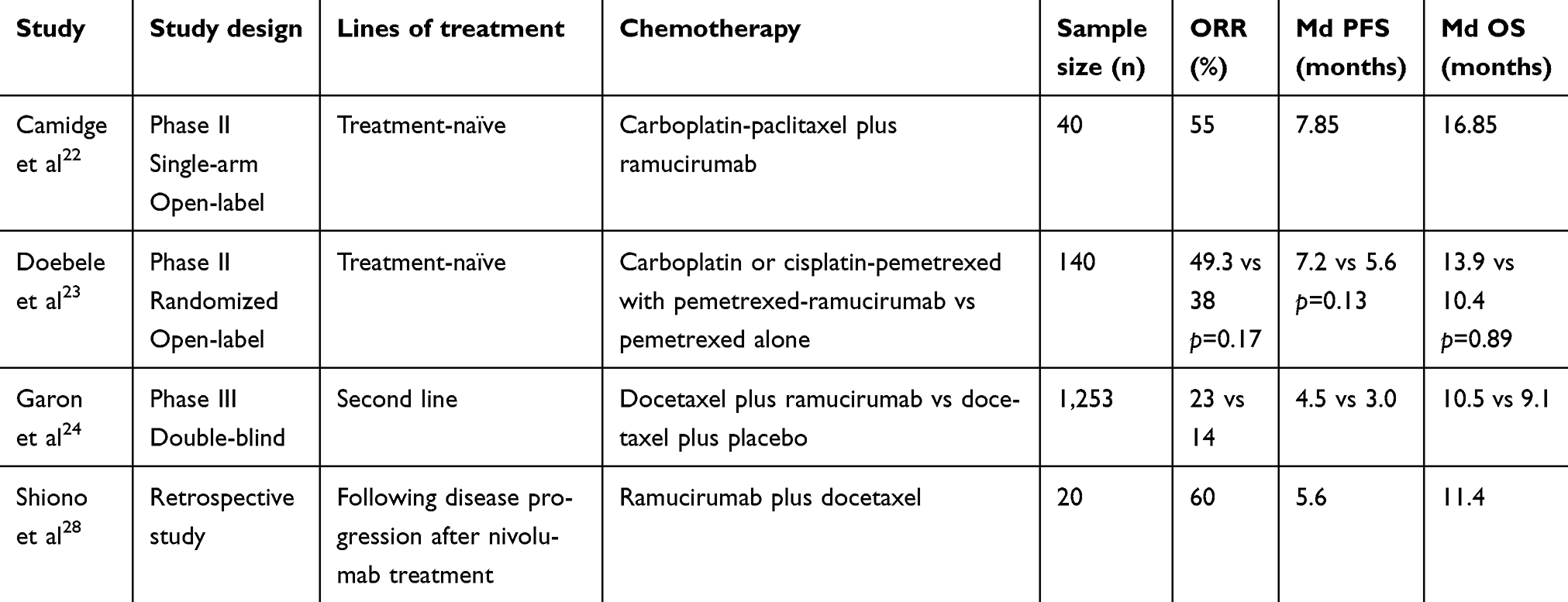 |
Table 1 Ramucirumab in non-small-cell lung cancer |
Ramucirumab plus docetaxel has shown a good rate of response when administered after nivolumab failure.28 Naumov et al showed that VEGF inhibition can enhance antitumor activity in T790M positive cancer cells.29 Combined blockage of the VEGFR and EGFR pathway has been utilized to overcome resistance to EGFR therapy. The findings of the phase III RELAY trial were recently presented at the 2019 American Society of Clinical Oncology annual conference. In this trial, patients with stage IV sensitizing EGFR mutation positive NSCLC were randomized either to receive erlotinib or ramucirumab plus erlotinib combination. The combination therapy yielded better PFS (median PFS of 19.4 months, 95% CI 15.4–21.6 vs 12.4 months, 95% CI 11.0–13.5), better duration of response (median 18.0 months, 95% CI 13.9–19.8 vs 11.1 months, 95% CI 9.7–12.3), and side effect profile consistent with the established safety profiles of the individual compounds.30 Additionally, a phase Ib study utilizing osimertinib with ramucirumab in EGFR-mutated, T790M-positive patients with disease progression on standard EGFR-TKI therapy is underway.31 Hopefully, this trial will add value to the role ramucirumab can play in treating T790M-positive patients.
In summary, ramucirumab in combination with docetaxel is an option for patients with metastatic NSCLC who have progressed on platinum chemotherapy. The combination confers 1.4 months of improvement in median survival. Since the survival gain is modest, the addition of ramucirumab should be individualized to younger patients with good performance status.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6): 394–424. doi:10.3322/caac.21492
2. Sher T, Dy GK, Adjei AA. Small cell lung cancer. Mayo Clin Proc. 2008;83(3):355–367. doi:10.4065/83.3.355
3. Molina JR, Yang P, Cassivi SD, Schild SE, Adjei AA. Non-small cell lung cancer: epidemiology, risk factors, treatment, and survivorship. Mayo Clin Proc. 2008;83(5):584–594. doi:10.4065/83.5.584
4. Ettinger DS, Wood DE, Aisner DL, et al. NCCN Clinical Practice Guidelines in Oncology: Non–Small Cell Lung Cancer. Version 3; 2019.
5. Shepherd FA, Dancey J, Ramlau R, et al. Prospective randomized trial of docetaxel versus best supportive care in patients with non-small-cell lung cancer previously treated with platinum-based chemotherapy. J Clin Oncol. 2000;18(10):2095–2103. doi:10.1200/JCO.2000.18.10.2095
6. Hanna N, Shepherd FA, Fossella FV, et al. Randomized phase III trial of pemetrexed versus docetaxel in patients with non-small-cell lung cancer previously treated with chemotherapy. J Clin Oncol. 2004;22(9):1589–1597. doi:10.1200/JCO.2004.08.163
7. Borghaei H, Paz-Ares L, Horn L, et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N Engl J Med. 2015;373(17):1627–1639. doi:10.1056/NEJMoa1507643
8. Brahmer J, Reckamp KL, Baas P, et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N Engl J Med. 2015;373(2):123–135. doi:10.1056/NEJMoa1504627
9. Rittmeyer A, Barlesi F, Waterkamp D, et al. Atezolizumab versus docetaxel in patients with previously treated with non-small-cell lung cancer (OAK): a phase 3, open-label, multicenter randomized controlled trial. Lancet. 2017;389(10066):255–265. doi:10.1016/S0140-6736(16)32517-X
10. Herbst RS, Baas P, Kim DW, et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomized controlled trial. Lancet. 2016;387(10027):1540–1550. doi:10.1016/S0140-6736(15)01281-7
11. Gandhi L, Rodríguez-Abreu D, Gadgeel S, et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. 2018;378(22):2078–2092. doi:10.1056/NEJMoa1801005
12. Paz-Ares L, Luft A, Vicente D, et al. Pembrolizumab plus chemotherapy for squamous non-small-cell lung cancer. N Engl J Med. 2018;379(21):2040–2051. doi:10.1056/NEJMoa1810865
13. Reck M, Rodríguez-Abreu D, Robinson AG, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. 2016;375(19):1823–1833. doi:10.1056/NEJMoa1606774
14. Socinski MA, Jotte RM, Cappuzzo F, et al. Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. N Engl J Med. 2018;378(24):2288–2301. doi:10.1056/NEJMoa1716948
15. Kim KJ, Li B, Winer J, et al. Inhibition of vascular endothelial growth factor-induced angiogenesis suppresses tumour growth in vivo. Nature. 1993;362(6423):841–844. doi:10.1038/362841a0
16. Spratlin JL, Cohen RB, Eadens M, et al. Phase I pharmacologic and biologic study of ramucirumab (IMC-1121B), a fully human immunoglobulin G1 monoclonal antibody targeting the vascular endothelial growth factor receptor-2. J Clin Oncol. 2010;28(5):780–787. doi:10.1200/JCO.2009.23.7537
17. Smith NR, Baker D, James NH, et al. Vascular endothelial growth factor receptors VEGFR-2 and VEGFR-3 are localized primarily to the vasculature in human primary solid cancers. Clin Cancer Res. 2010;16(14):3548–3561.
18. Skobe M, Rockwell P, Goldstein N, Vosseler S, Fusenig NE. Halting angiogenesis suppresses carcinoma cell invasion. Nat Med. 1997;3(11):1222–1227.
19. Witte L, Hicklin DJ, Zhu Z, et al. Monoclonal antibodies targeting the VEGF receptor-2 (Flk1/KDR) as an anti-angiogenic therapeutic strategy. Cancer Metastasis Rev. 1998;17(2):155–161.
20. Fuchs CS, Tomasek J, Yong CJ, et al. Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (REGARD): an international, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet. 2014;383(9911):31–39. doi:10.1016/S0140-6736(13)61719-5
21. Wilke H, Muro K, Van Cutsem E, et al. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): a double-blind, randomised phase 3 trial. Lancet Oncol. 2014;15(11):1224–1235. doi:10.1016/S1470-2045(14)70420-6
22. Camidge DR, Berge EM, Doebele RC, et al. A phase II, open-label study of ramucirumab in combination with paclitaxel and carboplatin as first-line therapy in patients with stage IIIB/IV non-small-cell lung cancer. J Thorac Oncol. 2014;9(10):1532–1539. doi:10.1097/JTO.0000000000000273
23. Doebele RC, Spigel D, Tehfe M, et al. Phase 2, randomized, open-label study of ramucirumab in combination with first-line pemetrexed and platinum chemotherapy in patients with nonsquamous, advanced/metastatic non-small cell lung cancer. Cancer. 2015;121(6):883–892. doi:10.1002/cncr.29132
24. Garon EB, Ciuleanu TE, Arrieta O, et al. Ramucirumab plus docetaxel versus placebo plus docetaxel for second-line treatment of stage IV non-small-cell lung cancer after disease progression on platinum-based therapy (REVEL): a multicentre, double-blind, randomised phase 3 trial. Lancet. 2014;384(9944):665–673. doi:10.1016/S0140-6736(14)60845-X
25. Wu YL, Planchard D, Lu S, et al. Pan-Asian adapted Clinical Practice Guidelines for the management of patients with metastatic non-small-cell lung cancer: a CSCO-ESMO initiative endorsed by JSMO, KSMO, MOS, SSO and TOS. Ann Oncol. 2019;30(2):171–210. doi:10.1093/annonc/mdy554
26. Reck M, Kaiser R, Mellemgaard A, et al. Docetaxel plus nintedanib versus docetaxel plus placebo in patients with previously treated non-small-cell lung cancer (LUME-Lung 1): a phase 3, double-blind, randomized controlled trial. Lancet Oncol. 2014;15(2):143–155. doi:10.1016/S1470-2045(13)70586-2
27. Cortot AB, Audiger-Valette C, Molinier O, et al. Weekly paclitaxel plus bevacizumab versus docetaxel as second or third-line treatment in advanced non-squamous non-small cell lung cancer (NSCLC): results from the phase III study IFCT-1103 ULTIMATE. J Clin Oncol. 2016;34(no. 15_suppl):9005. doi:10.1200/JCO.2016.34.15_suppl.9005
28. Shiono A, Kaira K, Mouri A, et al. Improved efficacy of ramucirumab plus docetaxel after nivolumab failure in previously treated non-small cell lung cancer patients. Thorac Cancer. 2019;10(4):775–781. doi:10.1111/1759-7714.12998
29. Naumov GN, Nilsson MB, Cascone T, et al. Combined vascular endothelial growth factor receptor and epidermal growth factor receptor (EGFR) blockade inhibits tumor growth in xenograft models of EGFR inhibitor resistance. Clin Cancer Res. 2009;15(10):3484–3494. doi:10.1158/1078-0432.CCR-08-2904
30. Nakagawa K, Garon EB, Seto T, et al. RELAY: A multinational, double-blind, randomized phase 3 study of erlotinib (ERL) in combination with ramucirumab (RAM) or placebo (PL) in previously untreated patients with epidermal growth factor receptor mutation- positive (EGFRm) metastatic non-small cell lung cancer (NSCLC).
31. Akamatsu H, Koh Y, Ozawa Y, et al. Osimertinib with ramucirumab in EGFR-mutated, T790M-positive patients with progression during EGFR-TKI therapy: phase Ib study. Clin Lung Cancer. 2018;19(6):e871–e874. doi:10.1016/j.cllc.2018.08.001
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.