")
Back to Journals » OncoTargets and Therapy » Volume 14
Clinical Utility of Olaparib in the Treatment of Metastatic Castration-Resistant Prostate Cancer: A Review of Current Evidence and Patient Selection
Authors LeVee A , Lin CY, Posadas E, Figlin R, Bhowmick NA, Di Vizio D, Ellis L , Rosser CJ, Freeman MR, Theodorescu D, Freedland SJ , Gong J
Received 24 July 2021
Accepted for publication 3 September 2021
Published 15 September 2021 Volume 2021:14 Pages 4819—4832
DOI https://doi.org/10.2147/OTT.S315170
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Federico Perche
Alexis LeVee, 1 Ching Ying Lin, 1 Edwin Posadas, 1 Robert Figlin, 1 Neil A Bhowmick, 1 Dolores Di Vizio, 2 Leigh Ellis, 1 Charlos J Rosser, 3 Michael R Freeman, 2 Dan Theodorescu, 2 Stephen J Freedland, 3, 4 Jun Gong 1
1Department of Medicine, Division of Hematology and Oncology, Samuel Oschin Comprehensive Cancer Institute, Cedars-Sinai Medical Center, Los Angeles, CA, USA; 2Department of Surgery, Division of Cancer Biology and Therapeutics, Biomedical Sciences, and Pathology and Laboratory Medicine, Samuel Oschin Comprehensive Cancer Institute, Cedars-Sinai Medical Center, Los Angeles, CA, USA; 3Department of Surgery, Division of Urology, Samuel Oschin Comprehensive Cancer Institute, Cedars-Sinai Medical Center, Los Angeles, CA, USA; 4Section of Urology, Durham VA Medical Center, Durham, NC, USA
Correspondence: Jun Gong Email [email protected]
Abstract: Metastatic castration-resistant prostate cancer (mCRPC) is an aggressive and fatal disease with a median survival of 36 months. With the advent of genetic sequencing to identify individual genomic profiles and acquired tumor-specific pathways, targeted therapies have revolutionized cancer treatment, including the treatment strategy in mCRPC. Poly(adenosine 5ʹ-diphosphate) ribose polymerase inhibitors (PARPi) are oral drugs that target mutations in the homologous recombination repair (HRR) pathway, which are found in approximately 27% of prostate cancer patients. In May 2020, the first PARP inhibitor, olaparib, was approved by the US Food and Drug Administration for men with mCRPC with HHR gene mutations based on the findings of the Phase III PROfound trial that showed improved overall survival in men with mCRPC who received olaparib and whose disease had progressed on a novel hormonal agent. This review summarizes the current evidence and clinical utility of olaparib as treatment in men with mCRPC. We describe the mechanism of action of PARPi, key clinical trials of olaparib in men with mCRPC, and ongoing Phase II and III clinical trials investigating olaparib in combination therapy and as front-line therapy in mCRPC.
Keywords: olaparib, PARP inhibitors, prostate cancer, DNA damage repair, homologous recombination repair
Corrigendum for this paper has been published
Introduction
Metastatic castration-resistant prostate cancer (mCRPC) is an aggressive and fatal disease with an estimated 34,130 deaths in the US in 2021 and a median survival of 36 months.1,2 While metastatic prostate cancer is initially treated with androgen deprivation therapy (ADT), the majority of metastatic prostate cancers progress to mCRPC – a disease state which no longer responds to first-line ADT. There are a number of treatment options available for use in mCRPC, including taxanes, sipuleucel-T, abiraterone acetate, enzalutamide, and radium-223, but outcomes continue to remain poor due to progressive resistance to therapies. In the last decade, genetic sequencing has identified new molecular targets in prostate cancer in pathways that promote tumorigenesis and can be targeted therapeutically. In May 2020, the poly(ADP) ribose polymerase inhibitor (PARPi) olaparib (Lynparza, AstraZeneca Pharmaceuticals, LP) was granted approval by the US Food and Drug Administration (FDA) for use in mCRPC.3
The purpose of this review is to describe the evidence and clinical utility of olaparib as treatment for men with mCRPC. We describe the mechanism of action of PARPi, key clinical trials which resulted in the FDA approval of olaparib, and current guidelines and administration recommendations. Next, we outline clinical trials of combination therapies with olaparib and conclude with ongoing clinical trials and areas for future research for the use of olaparib in mCRPC.
Mechanism of Action of PARP Inhibition
The PARP family of enzymes repair DNA damage caused by single-stranded breaks (SSB) in DNA that arise from replication errors or damage from external agents such as radiation, free radicals/reactive oxygen species, or toxins. Mutations in prostate cancer are commonly found in DNA-damage repair (DDR) pathways, and when they occur in the homologous recombination repair (HRR) pathway specifically, tumors rely on poly(ADP) ribose polymerase (PARP) to correct DNA damage and prevent cell lysis.4
PARP acts by repairing SSB in DNA and preventing progression to double-stranded breaks (DSB) by maintaining the integrity of the replication fork.4 When SSB occur, PARP1 acts by recruiting the necessary proteins to repair DNA, including proteins to process the damaged DNA, the DNA polymerase which fills the gap, and DNA ligase III which seals the nick. When DSB occur, DNA is repaired by two major mechanisms: non-homologous end-joining (NHEJ) and HRR.4 NHEJ repair involves the direct ligation of the free ends of the DNA DSB, whereas HRR involves using a homologous chromatid sequence as a template. HRR results in more accurate replication because it utilizes a homologous template, whereas NHEJ does not return DNA to its original sequence resulting in less precise replication and is thus error prone.5
PARPi such as olaparib act by trapping both PARP1 and PARP2 enzymes at damaged DNA.6 PARPi also bind to nicotinamide adenine dinucleotide on DNA, which further activates the binding of PARP to DNA and preventing PARP function.6 When the PARP enzyme is inhibited in normal cells, the HRR pathway can repair DSB in DNA which progress from SSB. However, when PARPi are present in HRR-mutated cells, DSB accumulate. This results in only NHEJ repair being available to repair DSB, which is less accurate DNA repair than HRR, and leads to the accumulation of damaged DNA. This buildup of damaged DNA ultimately leads to apoptosis and inhibition of tumor growth.4 This concept of targeting two different genetic mutations, in which either alone is compatible with viability but in combination leads to cell death, is termed synthetic lethality.
Mutations in HRR genes are commonly observed in a variety of tumor types, with an estimated frequency of 17.4% in solid tumors.7 HRR mutations can be inherited (eg, a germline mutation) or acquired by a tumor (eg, a somatic mutation). The most well-characterized HRR genes are BRCA1 and BRCA2; mutations in these genes place individuals at increased risk of breast cancer, ovarian cancer, prostate cancer, pancreatic cancer, and melanoma. There are numerous other HRR mutations that promote carcinogenesis in affected individuals due to the reduced ability to repair DNA.7
In one study which sequenced 451 patients with locoregional, metastatic non-castrate, and metastatic castration-resistant prostate cancer, 19% of patients had a germline mutation across a number of DDR genes, and 27% had either a germline or somatic mutation in BRCA2, BRCA1, ATM or CHEK2.8 In mCRPC specifically, the Phase III PROfound trial which screened 2792 patients with mCRPC for aberrations in 15 DDR genes involved in the HHR pathway found that 28% of patients with mCRPC have DDR gene defects.9 In patients with mCRPC, BRCA2 is the most common (9.7%) germline HRR mutation, followed by CDK12 (7.1%), ATM (6.3%), CHEK2 (1.6%), PP2R2A (1.5%), and BRCA1 (1.3%).10 Studies show that patients with a germline BRCA2 mutation are five times more likely to be diagnosed with prostate cancer than the general population and BRCA1/2 carriers are more likely to have an aggressive tumor with higher risk of nodal involvement and distant metastasis.11,12 The occurrence of BRCA2 mutations may also have a deleterious impact on mCPRC outcomes. For example, in the prospective PROREPAIR-B trial, Castro et al found that germline BRCA2 mutation is an independent prognostic factor for cause-specific mortality in mCRPC (HR 2.11; p=0.033) and caused cause-specific mortality to be cut in half compared to noncarriers (median, 17.4 vs 33.2 months; p = 0.027).13 However, the impact of the BRCA2 mutation may have been affected by the first line of treatment used as a statistically significant interaction between the BRCA2 mutation and treatment type was observed.
Evidence for Olaparib for the Treatment of mCRPC
Olaparib was first FDA-approved in December 2014 for metastatic ovarian cancer in germline BRCA-positive (gBRCAm) patients after studies showed improved survival with olaparib in women who had progressed with three or more prior lines of therapy.14 Subsequently, olaparib was FDA-approved as maintenance treatment for recurrent epithelial ovarian, fallopian, or primary peritoneal cancer in 2017, and as monotherapy for gBRCAm, HER2-negative, locally advanced or metastatic breast cancer in 2018.15,16 Olaparib was also FDA-approved in 2019 as maintenance treatment of gBRCAm pancreatic adenocarcinoma as studies showed olaparib improved progression-free survival (PFS).17
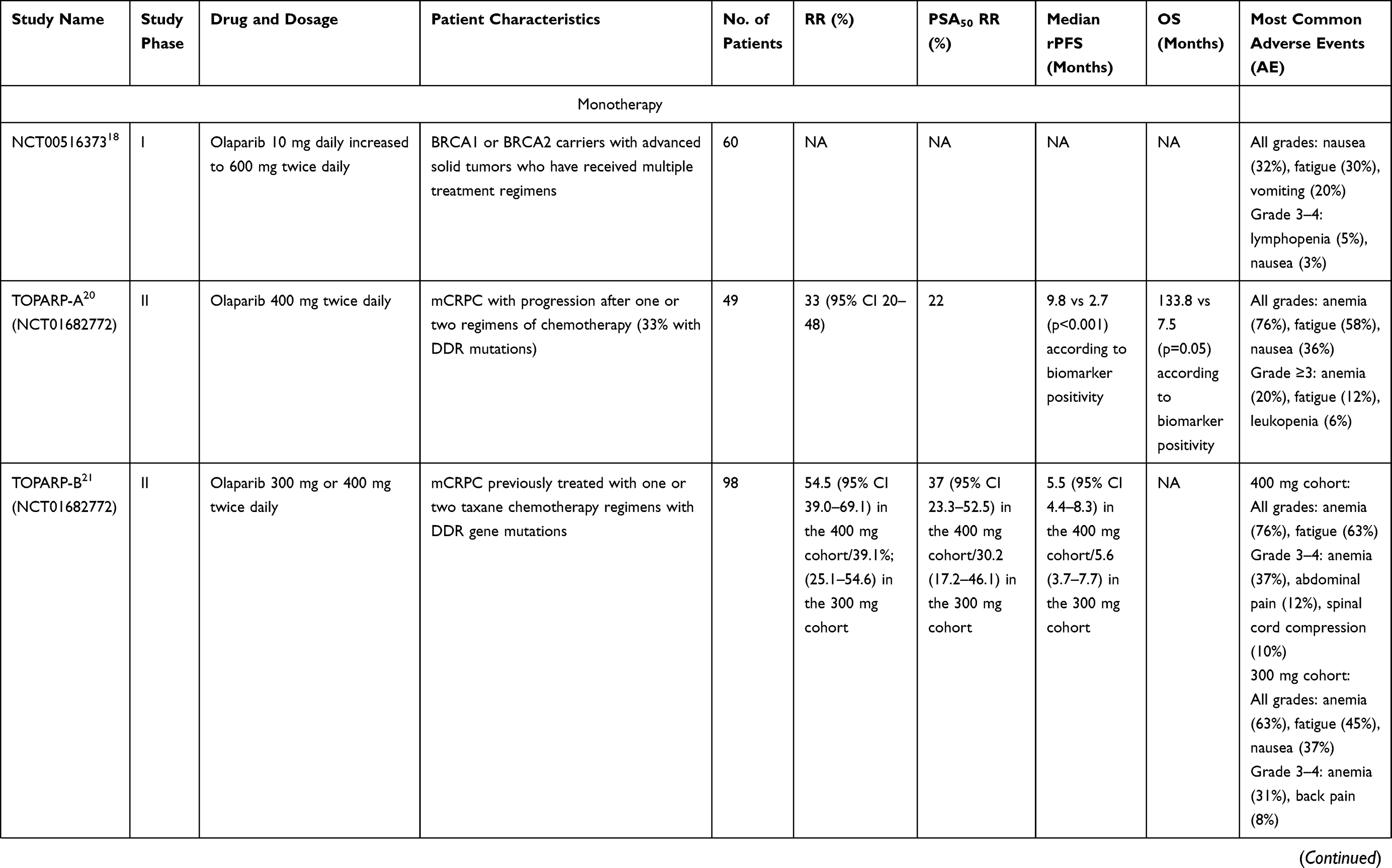
The first study to evaluate olaparib in solid tumors was a Phase I trial in 2009 which included 60 patients, 22 of which with BRCA1 or BRCA2 mutations and 3 patients with prostate cancer (Table 1).18 The olaparib dose and schedule were increased from 10 mg daily for 2 of every 3 weeks to 600 mg twice daily continuously. Reversible dose-limiting toxicity was seen with dosing schedules greater than 400mg twice daily in 3 patients, which included grade 4 thrombocytopenia and grade 3 somnolence, mood alternation, and fatigue. This established the maximum tolerated dose of olaparib at 400 mg twice daily. Notably, durable objective antitumor activity was only observed in patients with a BRCA1 or BRCA2 mutation. Of the three patients with prostate cancer, one who was BRCA2-positive was noted to have more than a 50% reduction in the prostate-specific antigen (PSA) level and resolution of bone metastases.18 Subsequently, a Phase II trial established the efficacy of olaparib at 400 mg twice daily in patients with germline BRCA1/2 mutations in prostate cancer with a tumor response rate of 50.0% (95% CI 15.7–84.3).19
 |
 |
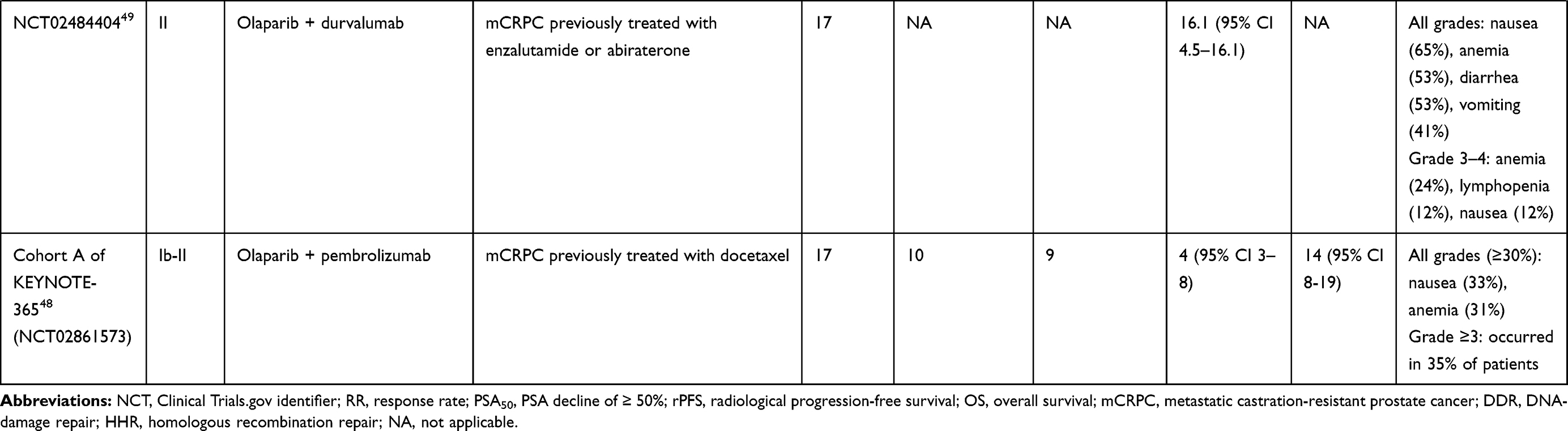 |
Table 1 Completed Clinical Trials with Olaparib in mCRPC |
These early, promising results of olaparib in prostate cancer led to the landmark, multicenter Phase II TOPARP-A trial in 2015 which evaluated olaparib in 50 patients with mCRPC who progressed after one or two regimens of chemotherapy.20 Forty-nine of 50 (98%) patients had received a novel hormonal agent (abiraterone or enzalutamide), and 16 of 49 patients (33%) who could be evaluated had mutations in DDR genes, including BRCA1/2, ATM, FANCA, CHEK2, and PALB2. The primary endpoint was the response rate, defined either as an objective response rate (ORR) according to Response Evaluation Criteria in Solid Tumors, version 1.1 (RECIST 1.1), reduction of at least 50% in the PSA level (PSA50), or conversion of circulating tumor cells (CTC) (to <5 cells per 7.5 mL of blood).
Treatment with olaparib resulted in a composite response rate of 33% (95% CI 20–48) for patients with and without DDR mutations combined. Of those with a response to olaparib, 14 (88%) had a response by the RECIST 1.1 criteria, including all 7 patients with BRCA2 mutation and 4 of 5 patients with ATM aberrations. Radiologic progression-free survival (rPFS) and overall survival (OS) were both significantly longer in patients with DDR mutations, with median rPFS 9.8 vs 2.7 months (p < 0.001) and median OS 13.8 vs 7.5 months (p=0.05). Grade 3 or 4 adverse events included anemia (20%), fatigue (12%), leukopenia (6%), thrombocytopenia (5%) and neutropenia (4%). Based on the TOPARP-A trial, olaparib received FDA breakthrough therapy designation in January 2016 for patients with mCRPC and BRCA1/2 or ATM gene mutations who had received prior taxane-based chemotherapy and an androgen receptor-directed therapy.3
Given the success of olaparib in mCRPC patients with DDR genes noted in these previous trials, the Phase II TOPARP-B trial in 2020 evaluated olaparib as treatment for only DDR-mutated mCRPC patients.21 Ninety-eight patients with mCRPC with DDR gene alterations were included and randomly assigned to receive either olaparib 400 mg twice daily or 300 mg twice daily. The primary endpoint was response rate as defined by the previously mentioned TOPARP-A trial.
Confirmed complete response was observed in 25 of 46 (54.3%; 95% CI 39.0–69.1) patients in the 400 mg cohort and 18 of 46 (39.1%; 25.1–54.6) in the 300 mg cohort. Although no statistically significant difference was seen between the two groups, only the 400 mg cohort met the predefined criteria for success with an efficacy of >50% composite response rate. The safety profile was similar to that seen in the TOPARP-A trial, with anemia being the most common grade 3 or 4 adverse event (31% of patients in the 300 mg cohort; 37% of patients in the 400mg cohort) and the most common adverse event leading to discontinuation. Even though the 400 mg cohort had a higher complete response rate, 37% of patients in the 400 mg cohort reduced their dose to 300 mg due to adverse events. The authors of the study also posit that the inferior composite response in the 300 mg cohort may be due to an imbalance of the CDK12 aberration, which had no response to olaparib by RECIST 1.1 or PSA50 criteria.21
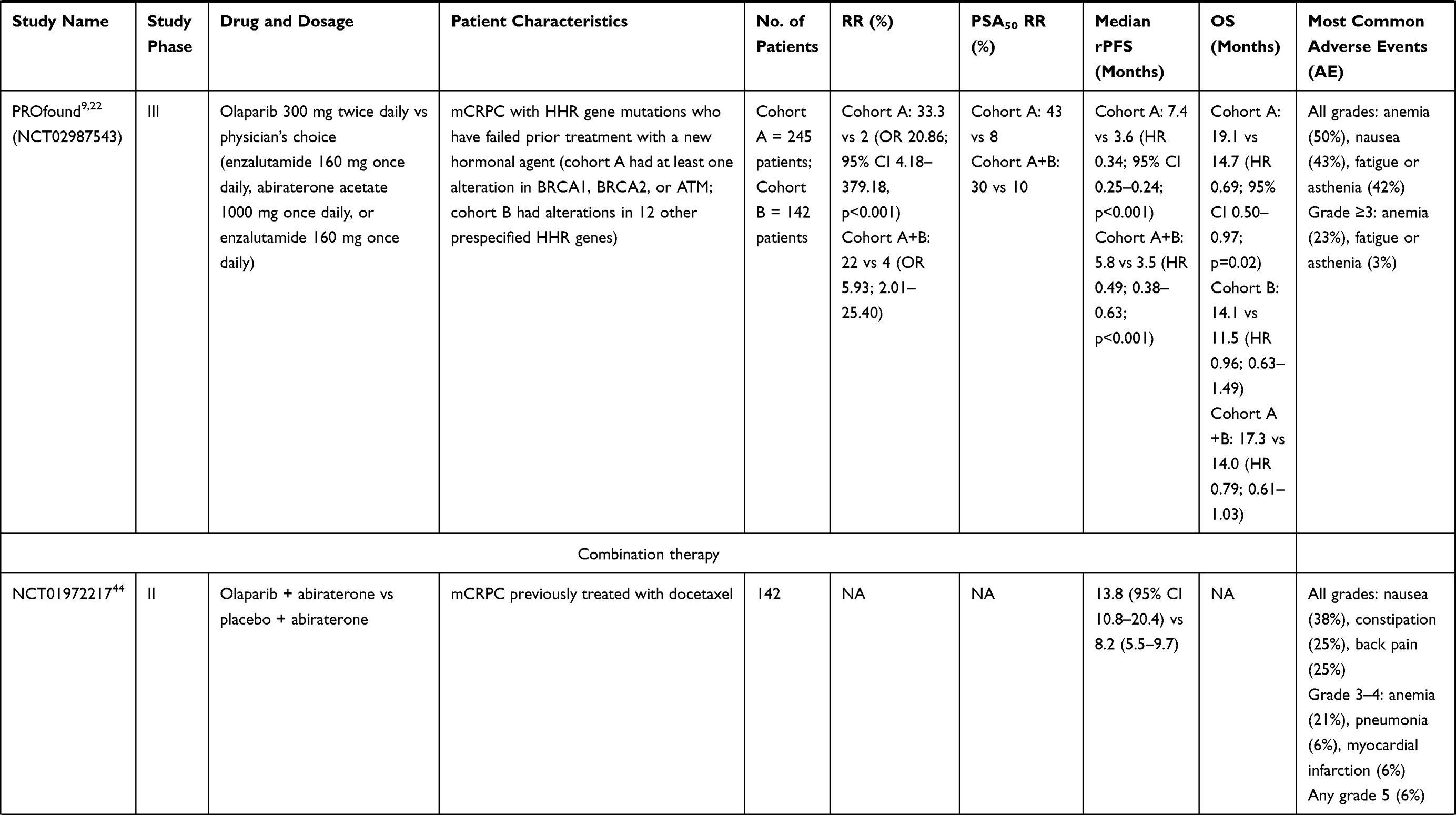
The randomized, Phase III PROfound trial published in May 2020 subsequently evaluated olaparib in men with mCRPC with mutations in DDR genes whose disease had progressed while receiving first-line treatment with a new hormonal agent (eg, enzalutamide or abiraterone).9 The trial consisted of two cohorts: cohort A included 245 patients with at least one alteration in BRCA1, BRCA2, or ATM, while cohort B included 142 patients with alterations in any of the other DDR genes (including BRIP1, BARD1, CDK12, CHEK1, CHEK2, FANCL, PALB2, PPP2R2A, RAD51B, RAD51C, RAD51D, and RAD54L). Men were randomly assigned in a 2:1 ratio to receive olaparib 300 mg twice daily or to physician’s choice of enzalutamide or abiraterone plus prednisone (the control).
In cohort A, olaparib resulted in improved objective response (33.3 vs 2%; OR 20.86; 95% CI 4.18–379.18, p < 0.001) and improved PFS (7.4 months vs 3.6 months; HR 0.34; 95% CI 0.25–0.24) compared to the control. With both cohorts combined, olaparib resulted in improved objective response (22 vs 4%; OR 5.93; 2.01–25.40) and improved PFS (5.8 months vs 3.5 months; HR 0.49; 0.38–0.63; p < 0.001) compared to the control. In the final OS analysis, cohort A showed a significantly longer duration of OS with olaparib compared to cohort B. The median duration of OS for cohort A was 19.1 months (HR 0.69; 0.50–0.97) with olaparib compared to 14.7 months with control therapy, whereas the median duration of OS for cohort B was 14.1 months (HR 0.96; 0.63–1.49) with olaparib compared to 11.5 months with control therapy.22 In the overall population, the median duration of OS was 17.3 months with olaparib and 14.0 months with the control (HR 0.79; 0.61–1.03). Based on the prolonged survival in men with HRR gene mutations and acceptable toxicity profile, the FDA approved olaparib in May 2020 as treatment for patients with mCRPC with HRR genes who have progressed following prior treatment with androgen-receptor directed therapy.3
Other PARP Inhibitors
Other PARPi have been developed and are being evaluated for use in mCRPC, although only one other PARPi has been FDA-approved for use in mCRPC. Rucaparib (Rubraca) is an oral PARP 1/2/3 inhibitor approved for use in women with ovarian, fallopian tube, or primary peritoneal cancer which was granted accelerated approval in May 2020 for use in men with mCRPC patients based on the TRITON2 study.23 The Phase II TRITON2 study evaluated rucaparib (600 mg twice daily) in patients with HHR-mutated mCRPC who progressed on prior androgen receptor-directed treatment and taxane-based chemotherapy. In the BRCA1 or BRCA2 cohort, rucaparib demonstrated significant response rates according to RECIST criteria (ORR 43.5%; 95% CI 31–56.7) and PSA response (54.8%; 95% CI 45.2–64.1).24 However, in patients with DDR genes other than BRCA1/2 including ATM, CDK12, or CHEK2, response rates were less impressive, with no radiographic or PSA response in patients with biallelic ATM loss or ATM germline mutations.25 Given that rucaparib primarily showed benefit for BRCA patients, rucaparib is FDA-approved for use only in BRCA-mutated mCRPC following both androgen receptor-directed therapy and taxane-based chemotherapy.
Niraparib (Zejula) is an oral PARP 1/2 inhibitor used in women with ovarian, fallopian tube, or primary peritoneal cancer that is being evaluated in the Phase II GALAHAD trial for mCRPC patients with DDR mutations who progressed on a taxane and an androgen-receptor directed treatment. Interim analysis for niraparib presented at ASCO in September 2019 showed improved ORR by RECIST 1.1 criteria of 41% for patients with BRCA1/2 mutations compared to 9% for those without BRCA mutations. Composite response rate (defined as ORR, CTC < 5/7.5mL blood or PSA50) was also significantly better for those with BRCA1/2 mutations (63%; 95% CI 47.6–76.8) compared to those without BRCA mutations (17%; 95% CI 6.6–33.7).26 Thus, the FDA granted breakthrough therapy designation for niraparib in men with BRCA1/2-mutated mCRPC in 2019 based on these initial results.27
Talazoparib (Talenna) is another oral PARP 1/2 inhibitor that is FDA-approved for use in gBRCAm, HER2-negative, locally advanced or metastatic breast cancer that is undergoing evaluation in the Phase II TALAPRO-1 trial in men with mCRPC with DDR genes who previously received taxane-based chemotherapy and progressed on at least one androgen receptor-directed treatment. Interim analysis presented at ASCO in May 2020 are also encouraging for this PARPi in mCRPC with an ORR of 28.0% for all DDR gene mutations and an ORR of 43.9% for BRCA1/2 mutations.28
Each of these PARPi has shown efficacy in BRCA1/2-positive men with mCRPC, but a head-to-head analysis comparing the efficacies and toxicity profiles of each of these PARPi in mCRPC has not yet been done and is unlikely to be done in the near future. There are also other PARPi that have been developed that have not resulted in as robust a response in mCRPC. For example, veliparib showed evidence for activity in BRCA2-mutated mCRPC in a Phase I clinical trial with an ORR defined as complete response (CR) and partial response (PR) of 37% and clinical benefit rate defined as CR plus PR plus stable disease for over 6 cycles of 40%.29 However, other studies investigating combination therapy with veliparib have been discouraging. In a Phase I study, veliparib plus temozolomide in docetaxel-treated patients with mCRPC resulted in a confirmed PSA response (decline ≥ 30%) in only 2 of 25 patients.30 In a randomized, Phase II trial that examined veliparib combined with abiraterone plus prednisone (arm A) versus abiraterone plus prednisone alone (arm B), there were no statistically significant differences between the two study arms in PSA RR (63.9 vs 62.7; p=0.27), ORR (45 vs 52.2; p=0.51), or median PFS (10.1 months vs 11.3 months; p=0.95).31
Indications and Selection of Patient
Mutational status should be carefully considered prior to starting a patient with mCRPC on olaparib. In the Phase II TOPARP-A trial, olaparib showed a significantly improved response rate, PFS, and OS in patients with DDR gene mutations compared to those who were biomarker-negative, and of the DDR mutations, BRCA2 carriers had the best response.20 All 7 BRCA2 patients had PSA levels that fell by 50% or more from baseline, and 5 of the 7 BRCA2 patients had a radiologic partial response. In addition, 4 of the 5 patients with deleterious ATM mutations had a response to olaparib.
TOPARP-B specifically tested olaparib in patients with DDR mutations. Secondary analysis by gene subgroup found that mutations in BRCA1/2 had the best composite overall response (83.3%; 95% CI 65.3–94.4), RECIST objective response (52.4%; 29.8–74.3), and PSA reduction (76.7%; 57.7–90.1) as well as the longest median rPFS (8.3 months) of all the DDR gene aberration subgroups.21 However, other DDR genes also had strong overall response rates, including PALB2 (57.1%; 18.4–90.1), ATM (36.8%; 16.3–61.6), CDK12 (25.0%; 8.7–49.1), and others (20.0%; 5.7–43.7).
Lastly, as mentioned above, the PROfound trial evaluated olaparib in patients with mCRPC with BRCA1/2 and ATM mutations (cohort A) compared to those with 12 other HHR genes (cohort B). Although the trial showed improved significant response rates and PFS for cohort A and cohort A+B, exploratory analysis of gene subtypes showed that the BRCA1 and/or BRCA2 mutation was associated with significantly improved OS compared to other DDR gene mutations, with a HR of 0.42 (95% CI 0.12–1.53) for BRCA1 and a HR of 0.59 (0.37–0.95) for BRCA2.22 Non-BRCA gene mutations had a HR of 0.95 (95% CI 0.68–1.34), and the ATM mutation (which was included in Cohort A) had a HR of 0.93 (0.53–1.75). Subgroup analysis by gene type also showed that the PPP2R2A gene resulted in worse outcomes with olaparib (HR 5.11; 95% CI 1.10–35.73). However, the trial notes that these exploratory analyses should be interpreted cautiously given that the trial was not powered to detect differences in gene subtype.
The findings from the PROfound trial suggest that patients with BRCA1 and BRCA2 mutations may have the greatest benefit from olaparib, and that olaparib may have less promising effects for the other DDR genes. Nevertheless, the trial was not sufficiently powered to perform this gene subtype analysis, and the separate analyses of cohorts A and B were generated for predefined endpoints with randomization as opposed to exploratory, post hoc subgroup analyses.32 Therefore, while we await more data, olaparib is strongly indicated for BRCA1/2 patients, and clinical caution is warranted for the use of olaparib in patients with other mutations of HRR genes. Olaparib should also be carefully used in patients with the PPP2R2A gene given the significantly worse outcomes in this subset of patients in the PROfound trial.
In addition to patient selection based on biomarker positivity, olaparib is currently indicated as second-line treatment for patients with mCRPC. Both the TOPARP-A and the TOPARP-B trial included patients who had progressed after one or two regimens of chemotherapy, whereas the PROfound trial included patients who had progressed after a new hormonal agent. However, nearly two-thirds of patients (66%) in the PROfound trial had also previously received a taxane-based chemotherapy. The trial showed efficacy of olaparib regardless of whether olaparib was administered before chemotherapy or after chemotherapy. Interestingly, subgroup analysis showed that olaparib had greater benefit in patients with previous taxane use (HR 0.56; 95% CI 0.38–0.84) compared to no prior taxane use (HR 1.03; 0.57–1.2), but in exploratory analysis patients with BRCA1/2 mutations without a prior history of taxane use experienced improved OS (HR 0.30; 0.10–0.78).22 On the other hand, those with an ATM mutation showed benefit from prior taxane use (HR 0.45; 0.22–0.95).
Genetic Testing Options
Genetic testing for HRR mutations at metastatic prostate cancer diagnosis is recommended to identify patients who may benefit from targeted treatment. Germline genetic testing is recommended for patients with metastatic prostate cancer, a strong family history of malignancy, Ashkenazi Jewish ancestry, or family history of germline mutations.33 Germline testing can be performed from a blood or saliva sample and should involve a genetic counselor given the psychological, legal, and ethical consequences to the patient and family. Somatic tumor sequencing should also be performed in order to identify mutations that evolved in tumor tissue due to genetic instability and selective pressure from therapy.34 The optimal choice of sample depends on the availability of tissue, with metastatic tissue preferred over archival/primary tumor tissue in order to detect the current disease biology. When metastatic tissue is unavailable, plasma circulating tumor DNA (ctDNA) can be obtained which has demonstrated high concordance with metastatic tissue biopsy in prostate cancer.35 Next-generation sequencing (NGS) using tumor tissue or a blood sample may test for as many as 300 cancer-related genes and molecular rearrangements, including copy number changes, gene rearrangement, and single nucleotide variants.36 If somatic testing identifies a mutation in a gene associated with cancer predisposition, it may be difficult to identify if the mutation is inherited or acquired; therefore, follow-up with genetic counseling is indicated when this occurs.
There are a number of commercial germline testing options available, such as BRACAnalysis® by Myriad Genetics and ProstateNext® by Ambry Genetics. Commercial options also exist for somatic testing, such as Foundation Medicine which offers NGS for both tumor testing (FoundationOne® CDx) and liquid biopsy for ctDNA (FoundationOne® Liquid CDx), Caris Life Sciences, and Tempus, for example. Costs among the various types of genetic tests vary widely, with NGS often $3000–6000 per test.37 Given the recent development of genetic testing in prostate cancer, insurance policies also vary significantly. Currently, most major insurers do not universally cover prostate cancer genetic testing, but may cover genetic testing if certain approved indications are met.36 For example, Medicare covers FDA-approved genetic testing for patients with metastatic cancer only if the patient has not been previously tested using the same genetic test for the same cancer diagnosis previously and decides to seek further treatment.38 For patients without insurance, financial assistance programs are often available to help alleviate out-of-pocket expenses.
Current Guidelines and Dosing
Olaparib is FDA-approved for patients with HRR mutations in mCRPC who have progressed following prior treatment with a new hormonal agent.3 The recommended olaparib tablet dose is 300 mg orally twice daily.39 The 300 mg twice daily dosing regimen was found to be effective and less toxic than the 400 mg twice daily dosing regimen based on the data from the TOPARP-B trial.21 For patients with moderate renal impairment (CrCl 31–50 mL/min), olaparib should be reduced to 200 mg orally twice daily. However, currently there are limited data on olaparib in patients with severe renal impairment, end-stage renal disease, or severe hepatic impairment.39 Olaparib should be continued until disease progression or unacceptable toxicity.
Olaparib has been incorporated into the National Comprehensive Cancer Network (NCCN) guidelines for prostate cancer as a Category 1 indication for men with mCRPC with HRR gene mutations (including BRCA1, BRCA2, ATM, BARD1, BRIP1, CDK12, CHEK2, FANCL, PALB2, RAD51B, RAD51C, RAD51D, and RAD54L) after prior androgen receptor-directed therapy or docetaxel chemotherapy. ADT should be continued while on olaparib to maintain castrate levels of serum testosterone (<50 ng/dL). Patients with PPP2R2A mutations are excluded from this recommendation.33
Adverse Reactions
The most common adverse reactions of olaparib in the Phase III PROfound trial were anemia (50%), nausea (43%), fatigue or anesthesia (42%), decreased appetite (31%), diarrhea (21%), vomiting (20%), and constipation (19%).22 Grade 3 or higher adverse events occurred in 52% of patients. Pulmonary embolism was reported in 5% of patients in the olaparib compared with 1% in the control group, but none were fatal. No reports of myelodysplastic syndrome (MDS) or acute myeloid leukemia (AML), toxicities noted in prior PARPi trials, were noted during the duration of treatment or the 30-day safety follow-up period. Dose reductions due to an adverse reaction occurred in 23% of patients, and 20% of patients discontinued olaparib due to an adverse reaction. Fatal adverse reactions occurred in 4% of patients treated with olaparib.
Although MDS/AML did not occur in patients in the PROfound trial, there is a warning label on olaparib for MDS/AML as these secondary malignancies arose in approximately 7% of patients on olaparib for other solid cancers.40 There are also warning labels for the increased risk of venous thromboembolic events (which occurred in 7% of patients in the PROfound trial) and the increased risk of pneumonitis in 7% of patients on olaparib monotherapy.39
Combination Therapy with Olaparib for Treatment of mCRPC
Combination therapies with olaparib are also undergoing investigation for mCRPC. Olaparib and androgen-targeted treatments have shown synergistic effects in preclinical research through androgen receptor signal modulation of the HRR pathway.41 This effect was observed in a study that treated C4-2 cells, a human prostatic cell line, with antiandrogens (bicalutamide and enzalutamide), leading to increased PARP activity.41 The study postulated that the androgen receptor promotes DNA damage repair and homologous recombination through ATM kinase coordinated response. As a result, the addition of both hormonal blockade and olaparib led to a lethal synergistic effect on cell culture viability as well as volume of tumor xenografts. Furthermore, when PARP molecules were introduced into androgen receptor-positive prostate cancer cells, PARP was recruited to sites of androgen receptor function, promoting androgen receptor activity and disease progression.42 Subsequently, mouse models showed that combination therapy with PARPi and androgen deprivation therapy resulted in the downregulation of androgen receptor-regulated homologous recombination gene expression, which caused sensitization to PARP inhibition and an increase in DNA damage-induced cell death.43
Following these studies in vivo, Clarke et al conducted a multicenter Phase II trial (NCT01972217) comparing olaparib plus abiraterone versus abiraterone with placebo in 142 unselected patients (i.e., no requirement for specific DDR mutations) with mCRPC who were previously treated with docetaxel (Table 1).44 The combination of PARPi and androgen-receptor directed therapy showed a therapeutic benefit in comparison to androgen-receptor directed therapy alone when evaluated by rPFS (HR 0.65; 95% CI 0.44–0.97). Patients treated with combination therapy had a mean rPFS of 13.8 months versus 8.2 months in those treated with abiraterone alone. However, the patients who received combination therapy also experienced increased rates of grade 3 or higher adverse events, most notably anemia (21% versus none).
Based on the improved rPFS of combination therapy with olaparib and abiraterone, the international multi-center Phase III PROPEL trial is currently underway to investigate the combination of olaparib and abiraterone compared to abiraterone alone as first-line therapy for mCRPC (Table 2).45 Although the trial will not preselect for HRR genes, an exploratory analysis will be performed to confirm the efficacy of this combination independent of HRR status. In addition, the randomized, multicenter Phase II BRCAaway trial (NCT03012321) is underway to investigate olaparib alone, abiraterone alone, or abiraterone plus olaparib specifically in patients with BRCA1, BRCA2, or ATM mutations.
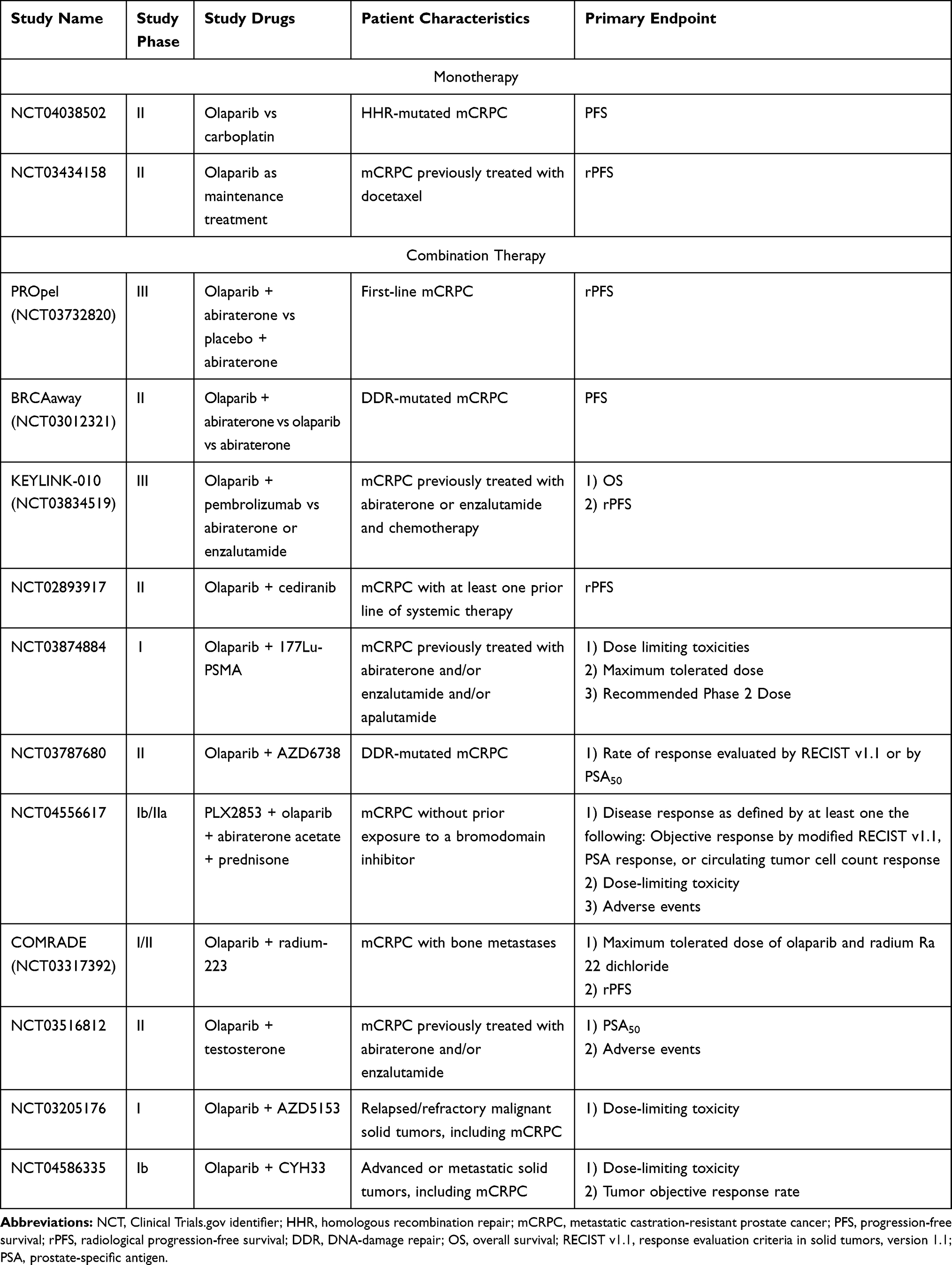 |
Table 2 Ongoing Clinical Trials Involving Olaparib in mCRPC |
The immunomodulatory effects of PARP inhibition have also been studied and raise the possibility of combining PARPi with immune checkpoint inhibitors. PARP inhibition leads to the accumulation of damaged DNA in the cytosol, which triggers interferons and chemoattractants and amplifies the anti-tumor immune response.46 In addition, PARP inhibition increases expression of programmed death ligand 1 (PD-L1) through the IFN-gamma signaling pathway by activating cyclic GMP-AMP synthase/stimulation of IFN genes (cGAS/STING).47 Therefore, by combining immune checkpoint inhibition of the PD-L1/PD-1 axis and PARP inhibition, the anti-tumor immune response is up-regulated and immune escape mechanisms may be overcome.
The combination of PD-1 blockade and PARP inhibition is currently being studied in KEYNOTE-365, a Phase 1b/2 study evaluating pembrolizumab with olaparib versus other therapeutic agents in mCRPC.48 In cohort A, which evaluated pembrolizumab with olaparib, 26% of patients were PD-L1 positive, and HRR mutations were not preselected. The latest data show that the composite response rate (ORR RECIST v1.1, confirmed PSA response, or decrease in CTC count) was 8 out of 84 (10%) patients and grade 3–5 adverse events occurred in 29 (35%) of patients. This same therapeutic combination of pembrolizumab and olaparib is also under investigation in one treatment arm of KEYLINK-010 (NCT03834519), although notably with a lower dosage of olaparib, in patients who have previously failed to respond to either abiraterone acetate or enzalutamide and to chemotherapy.
Other immune checkpoint inhibitors have also been evaluated in combination with olaparib. Durvalumab, a human IgG1-K monoclonal antibody that targets PD-L1, was tested in combination with olaparib in a limited Phase II clinical trial with 17 patients and demonstrated a rPFS of 16.1 months (95% CI 4.5–16.1), with a similar rPFS in patients with DDR mutations.49 However, patients with DDR mutations had a longer 12-month PFS of 83.3% (95% CI 27.3–94.5) compared to those without mutations (36.4%; 11.2–62.7). An additional Phase II study comparing olaparib plus durvalumab in patients with DDR mutations specifically is in progress for recurrent non-metastatic prostate cancer (NCT03810105).
Combination therapy with olaparib and chemotherapy may also prove clinically effective with a synergistic effect seen in preclinical studies; however, as both PARPi and chemotherapeutic agents are non-specific, systemic adverse effects (particularly myelosuppression) may prove too challenging to overcome.50 For instance, the combination of veliparib and topotecan was studied in a Phase I–II trial for cervical cancer, but over half (59%) of the 27 participants developed anemia, 44% thrombocytopenia, and 19% neutropenia.51 Nevertheless, a Phase II randomized trial (NCT03263650) is currently investigating olaparib maintenance versus observation following cabazitaxel-carboplatin combination therapy in aggressive variant prostate cancer (AVPC).
Finally, there are ongoing clinical trials evaluating olaparib in combination with other investigational treatments for mCRPC, such as olaparib in combination with cediranib (an inhibitor of vascular endothelial growth factor receptor tyrosine kinase), 177Lu-PSMA-617 (a targeted radioligand therapy), AZD6738 (an ATR kinase inhibitor), PLX2853 and AZD5153 (BRD4 inhibitors), CYH33 (a PI3K inhibitor), radiotherapy, and radium-223, as summarized in Table 2.
Controversies with Olaparib
Although olaparib improves PFS and OS in patients with mCRPC and certain HRR genes, controversy exists regarding the use and feasibility of olaparib. First, olaparib is estimated at $12,000 per month compared to $2600 per month of docetaxel.52 Somatic and/or germline testing to determine HRR-mutated patients also adds expensive, as previously mentioned, and only one-third of mCRPC patients have HRR mutations. With the myriad of options and substantial cost of olaparib use, the question of cost-effectiveness of olaparib use for patients with mCRPC compared to standard care has been raised. One study demonstrated that olaparib treatment has an incremental cost-effectiveness ratio (ICER) of $116,903 per quality-adjusted life year (QALY) for men with mCRPC and at least one gene alteration in BRCA1, BRCA2, and ATM.53 Depending on the resources available, this estimation may be within the willingness-to-pay (WTP) threshold.
Methodological concerns with the PROfound trial have also been raised that question whether olaparib should be indicated following novel hormonal agents.54,55 For example, the control arm of abiraterone or enzalutamide may not have been optimal given a true “physician’s choice” control arm would have included prior docetaxel, cabazitaxel, and/or radium-223.54 As a result, there are currently no direct comparisons between olaparib and cabazitaxel, radium-223 or re-treatment with docetaxel on improved PFS and OS. In addition, 82% of men in the control arm were permitted to crossover to the olaparib arm. This may have confounded the treatment effect of the control arm given that patients in the control arm may have had a delay in other effective treatments, such as taxane therapy.54 Given the uncertain benefit of olaparib compared to other agents and the cost-effectiveness of olaparib, the appropriateness of olaparib use in mCRPC has been questioned. As such, in February 2021, the United Kingdom’s National Institute for Health and Care Excellence (NICE) did not recommend olaparib for patients with mCRPC.56
Conclusions and Future Perspectives
The efficacy of PARPi and the incorporation of germline and tumor sequencing testing in men with mCRPC have changed the treatment paradigm for this aggressive disease. Although olaparib has demonstrated efficacy for men with HRR mutations and is currently FDA-approved for all HHR mutations, exploratory analysis from the Phase III PROfound trial suggests that olaparib may be most beneficial for BRCA1 and BRCA2 mutations.32 Further studies to evaluate the efficacy of olaparib in specific genetic subtypes are warranted in order to determine which HRR mutations benefit most from olaparib and whether men without HRR mutations will benefit at all. Although clinical trials may be limited by small sample size for HRR mutations other than BRCA1/2, CHEK2, and ATM, meta-analyses of all PARPi for mCRPC, retrospective studies, and further subgroup analyses by genetic mutation in mCRPC may help act as a guide.
Furthermore, while olaparib has shown positive results in patients following prior treatment with an androgen receptor-directed therapy, the question of whether olaparib could be used as first-line therapy or in earlier stages of prostate cancer remains unanswered. The results of the ongoing clinical trials with olaparib as first-line treatment, as monotherapy, and in metastatic castration-sensitive prostate cancer will hopefully shed some light on these issues. Lastly, combination therapies with olaparib have shown synergistic effect in Phase II trials, and we await the results of the Phase III PROpel and KEYLINK-010 trials to determine whether combination treatment with an androgen receptor-directed agent or an immune checkpoint inhibitor, respectively, will improve outcomes. As targeted therapy continues to revolutionize cancer therapies, olaparib highlights the importance of multigene molecular testing and is becoming a mainstay in the treatment for mCRPC.
Funding
There is no funding to report.
Disclosure
Stephen Freedland: Consulting or Advisory Role – Merck, Astellas, AstraZeneca, Pfizer, Janssen, Bayer, Clovis, Sanofi, Myovant, and Exact Sciences. Edwin Posadas: Consulting or Advisory Role – CytoLumina, Genentech/Roche, Janssen Oncology, Janssen Oncology, Novartis; Speakers’ Bureau – Bayer; Research Funding – Pfizer; Patents, Royalties, Other Intellectual Property – Patent on NanoVelcro Assay for CTCs in prostate cancer; Travel, Accommodations, Expenses – TRACON Pharma. Robert Figlin: Leadership – 4Dx, Apollomics; Consulting or Advisory Role – Bristol-Myers Squibb, CBT Pharmaceuticals, Johnson & Johnson; Research Funding – Bristol-Myers Squibb (Inst), Calithera Biosciences (Inst), Exelixis (Inst), Merck (Inst), Peloton Therapeutics (Inst). Dan Theodorescu: Consulting or Advisory Role – Aurora Oncology, Machavert Pharmaceuticals, Merck, Urogen Pharma. Jun Gong: Consultant or Advisory Role – EMD Serono, Elsevier, Exelixis, QED Therapeutics, Natera, Basilea, HalioDx, Eisai, Janssen, Astellas and Amgen. The authors report no other conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021. Ca Cancer J Clin. 2021;71(1):7–33. doi:10.3322/caac.21654
2. Armstrong AJ, Lin P, Tombal B, et al. Five-year survival prediction and safety outcomes with enzalutamide in men with chemotherapy-naïve metastatic castration-resistant prostate cancer from the PREVAIL trial. Eur Urol. 2020;78(3):347–357. doi:10.1016/j.eururo.2020.04.061
3. FDA approves olaparib for HRR gene-mutated metastatic castration-resistant prostate cancer. U.S. Food & Drug Administration; 2020
4. Shaheen M, Allen C, Nickoloff JA, Hromas R. Synthetic lethality: exploiting the addiction of cancer to DNA repair. Blood. 2011;117(23):6074–6082. doi:10.1182/blood-2011-01-313734
5. Lieber MR. The mechanism of human nonhomologous DNA end joining. J Biol Chem. 2008;283(1):1–5. doi:10.1074/jbc.R700039200
6. Murai J, Huang S-N, Das BB, et al. Trapping of PARP1 and PARP2 by clinical PARP inhibitors. Cancer Res. 2012;72(21):5588–5599. doi:10.1158/0008-5472.can-12-2753
7. Heeke AL, Pishvaian MJ, Lynce F, et al. Prevalence of homologous recombination-related gene mutations across multiple cancer types. JCO Precis Oncol. 2018;2:1–3. doi:10.1200/po.17.00286
8. Abida W, Armenia J, Gopalan A, et al. Prospective genomic profiling of prostate cancer across disease states reveals germline and somatic alterations that may affect clinical decision making. JCO Precis Oncol. 2017;1(1):1–16. doi:10.1200/po.17.00029
9. de Bono J, Mateo J, Fizazi K, et al. Olaparib for metastatic castration-resistant prostate cancer. N Engl J Med. 2020;382(22):2091–2102. doi:10.1056/NEJMoa1911440
10. de Bono JS, Fizazi K, Saad F, et al. 847PD - Central, prospective detection of homologous recombination repair gene mutations (HRRm) in tumour tissue from >4000 men with metastatic castration-resistant prostate cancer (mCRPC) screened for the PROfound study. Ann Oncol. 2019;30:v328–v329. doi:10.1093/annonc/mdz248.004
11. Mersch J, Jackson MA, Park M, et al. Cancers associated with BRCA1 and BRCA2 mutations other than breast and ovarian. Cancer. 2015;121(2):269–275. doi:10.1002/cncr.29041
12. Castro E, Goh C, Olmos D, et al. Germline BRCA mutations are associated with higher risk of nodal involvement, distant metastasis, and poor survival outcomes in prostate cancer. J Clin Oncol. 2013;31(14):1748–1757. doi:10.1200/JCO.2012.43.1882
13. Castro E, Romero-Laorden N, Del Pozo A, et al. PROREPAIR-B: a prospective cohort study of the impact of germline DNA repair mutations on the outcomes of patients with metastatic castration-resistant prostate cancer. J Clin Oncol. 2019;37(6):490–503. doi:10.1200/JCO.18.00358
14. Kim G, Ison G, McKee AE, et al. FDA approval summary: olaparib monotherapy in patients with deleterious germline BRCA-mutated advanced ovarian cancer treated with three or more lines of chemotherapy. Clin Cancer Res. 2015;21(19):4257–4261. doi:10.1158/1078-0432.ccr-15-0887
15. FDA approves olaparib tablets for maintenance treatment in ovarian cancer. U.S. Food & Drug Administration; 2017
16. FDA approves olaparib for germline BRCA-mutated metastatic breast cancer. U.S. Food & Drug Administration; 2018
17. FDA approves olaparib for gBRCAm metastatic pancreatic adenocarcinoma. U.S. Food & Drug Administration; 2019
18. Fong PC, Boss DS, Yap TA, et al. Inhibition of poly(ADP-ribose) polymerase in tumors from BRCA mutation carriers. N Engl J Med. 2009;361(2):123–134. doi:10.1056/NEJMoa0900212
19. Kaufman B, Shapira-Frommer R, Schmutzler RK, et al. Olaparib monotherapy in patients with advanced cancer and a germline BRCA1/2 mutation. J Clin Oncol. 2015;33(3):244–250. doi:10.1200/jco.2014.56.2728
20. Mateo J, Carreira S, Sandhu S, et al. DNA-repair defects and olaparib in metastatic prostate cancer. N Engl J Med. 2015;373(18):1697–1708. doi:10.1056/NEJMoa1506859
21. Mateo J, Porta N, Bianchini D, et al. Olaparib in patients with metastatic castration-resistant prostate cancer with DNA repair gene aberrations (TOPARP-B): a multicentre, open-label, randomised, phase 2 trial. Lancet Oncol. 2020;21(1):162–174. doi:10.1016/S1470-2045(19)30684-9
22. Hussain M, Mateo J, Fizazi K, et al. Survival with olaparib in metastatic castration-resistant prostate cancer. N Engl J Med. 2020;383(24):2345–2357. doi:10.1056/NEJMoa2022485
23. FDA grants accelerated approval to rucaparib for BRCA-mutated metastatic castration-resistant prostate cancer. U.S. Food & Drug Administration. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-rucaparib-brca-mutated-metastatic-castration-resistant-prostate.
24. Abida W, Patnaik A, Campbell D, et al. Rucaparib in men with metastatic castration-resistant prostate cancer harboring a BRCA1 or BRCA2 gene alteration. J Clin Oncol. 2020;38(32):3763–3772. doi:10.1200/jco.20.01035
25. Abida W, Campbell D, Patnaik A, et al. Non-BRCA DNA damage repair gene alterations and response to the PARP inhibitor rucaparib in metastatic castration-resistant prostate cancer: analysis from the phase II TRITON2 study. Clin Cancer Res. 2020;26(11):2487–2496. doi:10.1158/1078-0432.ccr-20-0394
26. Smith MR, Sandhu SK, Kelly WK, et al. LBA50 - pre-specified interim analysis of GALAHAD: a phase II study of niraparib in patients (pts) with metastatic castration-resistant prostate cancer (mCRPC) and biallelic DNA-repair gene defects (DRD). Ann Oncol. 2019;30:v884–v885. doi:10.1093/annonc/mdz394.043
27. Astor L. FDA grants breakthrough designation to niraparib for metastatic CRPC. Targeted oncology. Available from: https://www.targetedonc.com/view/fda-grants-breakthrough-designation-to-niraparib-for-metastatic-crpc.
28. Bono JSD, Mehra N, Higano CS, et al. TALAPRO-1: phase II study of talazoparib (TALA) in patients (pts) with DNA damage repair alterations (DDRm) and metastatic castration-resistant prostate cancer (mCRPC) – updated interim analysis (IA). J Clin Oncol. 2020;38(15_suppl):5566. doi:10.1200/JCO.2020.38.15_suppl.5566
29. Pahuja S, Appleman LJ, Belani CP, et al. Preliminary activity of veliparib (V) in BRCA2-mutated metastatic castration-resistant prostate cancer (mCRPC). J Clin Oncol. 2015;33(7_suppl):170. doi:10.1200/jco.2015.33.7_suppl.170
30. Hussain M, Carducci MA, Slovin S, et al. Targeting DNA repair with combination veliparib (ABT-888) and temozolomide in patients with metastatic castration-resistant prostate cancer. Invest New Drugs. 2014;32(5):904–912. doi:10.1007/s10637-014-0099-0
31. Hussain M, Daignault S, Twardowski P, et al. Abiraterone + prednisone (Abi) ± veliparib (Vel) for patients (pts) with metastatic castration-resistant prostate cancer (CRPC): NCI 9012 updated clinical and genomics data. J Clin Oncol. 2017;35(15_suppl):5001. doi:10.1200/JCO.2017.35.15_suppl.5001
32. Stopsack KH. Efficacy of PARP inhibition in metastatic castration-resistant prostate cancer is very different with non-BRCA DNA repair alterations: reconstructing prespecified endpoints for cohort B from the Phase 3 PROfound trial of olaparib. Eur Urol. 2021;79(4):442–445. doi:10.1016/j.eururo.2020.09.024
33. Network NCC. Prostate cancer (version 2.2021). Available from: https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf.
34. Cheng HH, Sokolova AO, Schaeffer EM, Small EJ, Higano CS. Germline and somatic mutations in prostate cancer for the clinician. J Natl Compr Canc Netw. 2019;17(5):515–521. doi:10.6004/jnccn.2019.7307
35. Wyatt AW, Annala M, Aggarwal R, et al. Concordance of circulating tumor DNA and matched metastatic tissue biopsy in prostate cancer. J Natl Cancer Inst. 2017;109(12):djx118. doi:10.1093/jnci/djx118
36. Zhen JT, Syed J, Nguyen KA, et al. Genetic testing for hereditary prostate cancer: current status and limitations. Cancer. 2018;124(15):3105–3117. doi:10.1002/cncr.31316
37. Gong J, Pan K, Fakih M, Pal S, Salgia R. Value-based genomics. Oncotarget. 2018;9(21):15792–15815. doi:10.18632/oncotarget.24353
38. Medicare National Coverage Determinations Manual. Chapter 1, Part 2 Sections 90-160.26. U.S. Department of Health and Human Services, Centers for Medicare & Medicaid Services; 2021.
39. Prescribing information. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/208558s014lbl.pdf.
40. Master SR, Mansour RP. Myelodysplastic syndrome and acute myeloid leukemia as side effect of PARP inhibitors. J Clin Oncol. 2020;38(15_suppl):3601. doi:10.1200/JCO.2020.38.15_suppl.3601
41. Asim M, Tarish F, Zecchini HI, et al. Synthetic lethality between androgen receptor signalling and the PARP pathway in prostate cancer. Nat Commun. 2017;8(1):374. doi:10.1038/s41467-017-00393-y
42. Schiewer MJ, Goodwin JF, Han S, et al. Dual roles of PARP-1 promote cancer growth and progression. Cancer Discov. 2012;2(12):1134–1149. doi:10.1158/2159-8290.cd-12-0120
43. Li L, Karanika S, Yang G, et al. Androgen receptor inhibitor–induced “BRCAness” and PARP inhibition are synthetically lethal for castration-resistant prostate cancer. Sci Signal. 2017;10(480):eaam7479. doi:10.1126/scisignal.aam7479
44. Clarke N, Wiechno P, Alekseev B, et al. Olaparib combined with abiraterone in patients with metastatic castration-resistant prostate cancer: a randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Oncol. 2018;19:975–986. doi:10.1016/S1470-2045(18)30365-6
45. Clarke NW, Armstrong AJ, Thiery-Vuillemin A, et al. PROPEL: a randomized, phase III trial evaluating the efficacy and safety of olaparib combined with abiraterone as first-line therapy in patients with metastatic castration-resistant prostate cancer (mCRPC). J Clin Oncol. 2019;37(7_suppl):TPS340. doi:10.1200/JCO.2019.37.7_suppl.TPS340
46. Vikas P, Borcherding N, Chennamadhavuni A, Garje R. Therapeutic potential of combining PARP inhibitor and immunotherapy in solid tumors. Front Oncol. 2020;10:570. doi:10.3389/fonc.2020.00570
47. Chabanon RM, Muirhead G, Krastev DB, et al. PARP inhibition enhances tumor cell–intrinsic immunity in ERCC1-deficient non–small cell lung cancer. J Clin Invest. 2019;129(3):1211–1228. doi:10.1172/JCI123319
48. Yu EY, Piulats JM, Gravis G, et al. KEYNOTE-365 cohort A updated results: pembrolizumab (pembro) plus olaparib in docetaxel-pretreated patients (pts) with metastatic castration-resistant prostate cancer (mCRPC). J Clin Oncol. 2020;38(6_suppl):100. doi:10.1200/JCO.2020.38.6_suppl.100
49. Karzai F, VanderWeele D, Madan RA, et al. Activity of durvalumab plus olaparib in metastatic castration-resistant prostate cancer in men with and without DNA damage repair mutations. J Immunother Cancer. 2018;6(1):141. doi:10.1186/s40425-018-0463-2
50. Matulonis UA, Monk BJ. PARP inhibitor and chemotherapy combination trials for the treatment of advanced malignancies: does a development pathway forward exist? Ann Oncol. 2017;28(3):443–447. doi:10.1093/annonc/mdw697
51. Kunos C, Deng W, Dawson D, et al. A Phase I-II evaluation of veliparib (NSC #737664), topotecan, and filgrastim or pegfilgrastim in the treatment of persistent or recurrent carcinoma of the uterine cervix: an NRG Oncology/Gynecologic Oncology Group study. Int J Gynecol Cancer. 2015;25(3):484–492. doi:10.1097/igc.0000000000000380
52. Memorial Sloan Kettering Cancer Center. Cancer drug costs for a month of treatment at initial Food and Drug Administration approval. Available from: www.mskcc.org/sites/default/files/node/25097/documents/111516-drug-costs-table.pdf.
53. Su D, Wu B, Shi L. Cost-effectiveness of genomic test-directed olaparib for metastatic castration-resistant prostate cancer. Front Pharmacol. 2021;11(2436). doi:10.3389/fphar.2020.610601
54. Kwon DH, Booth CM, Prasad V. Untangling the PROfound trial for advanced prostate cancer: is there really a role for olaparib? Eur Urol. 2021;79(6):710–712. doi:10.1016/j.eururo.2021.02.041
55. Rosa K. NICE recommends against olaparib for metastatic prostate cancer. OncLive. Available from: https://www.onclive.com/view/nice-recommends-against-olaparib-for-metastatic-prostate-cancer.
56. National Institute for Health and Care Excellence. Olaparib for Previously Treated BRCA-Mutation Positive Hormone-Relapsed Metastatic Prostate Cancer. National Institute for Health and Care Excellence; 2021:1–29.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.