")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 10
Clinical utility of implantable neurostimulation devices as adjunctive treatment of uncontrolled seizures
Authors Cox J, Seri S , Cavanna A
Received 18 August 2014
Accepted for publication 11 September 2014
Published 14 November 2014 Volume 2014:10 Pages 2191—2200
DOI https://doi.org/10.2147/NDT.S60854
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Joanna H Cox1 Stefano Seri2,3 Andrea E Cavanna1,2,4,5
1College of Medical and Dental Sciences, University of Birmingham, 2School of Life and Health Sciences, Aston Brain Centre, Aston University, 3Children’s Epilepsy Surgery Programme, The Birmingham Children’s Hospital NHS Foundation Trust, 4Department of Neuropsychiatry, Birmingham and Solihull Mental Health NHS Foundation Trust, Birmingham, UK; 5Sobell Department of Motor Neuroscience and Movement Disorders, Institute of Neurology and UCL, London, UK
Abstract: About one third of patients with epilepsy are refractory to medical treatment. For these patients, alternative treatment options include implantable neurostimulation devices such as vagus nerve stimulation (VNS), deep brain stimulation (DBS), and responsive neurostimulation systems (RNS). We conducted a systematic literature review to assess the available evidence on the clinical efficacy of these devices in patients with refractory epilepsy across their lifespan. VNS has the largest evidence base, and numerous randomized controlled trials and open-label studies support its use in the treatment of refractory epilepsy. It was approved by the US Food and Drug Administration in 1997 for treatment of partial seizures, but has also shown significant benefit in the treatment of generalized seizures. Results in adult populations have been more encouraging than in pediatric populations, where more studies are required. VNS is considered a safe and well-tolerated treatment, and serious side effects are rare. DBS is a well-established treatment for several movement disorders, and has a small evidence base for treatment of refractory epilepsy. Stimulation of the anterior nucleus of the thalamus has shown the most encouraging results, where significant decreases in seizure frequency were reported. Other potential targets include the centromedian thalamic nucleus, hippocampus, cerebellum, and basal ganglia structures. Preliminary results on RNS, new-generation implantable neurostimulation devices which stimulate brain structures only when epileptic activity is detected, are encouraging. Overall, implantable neurostimulation devices appear to be a safe and beneficial treatment option for patients in whom medical treatment has failed to adequately control their epilepsy. Further large-scale randomized controlled trials are required to provide a sufficient evidence base for the inclusion of DBS and RNS in clinical guidelines.
Keywords: deep brain stimulation, epilepsy, implantable neurostimulation device, responsive neurostimulation, seizures, vagus nerve stimulation
Background
Epilepsy is a common neurological disorder affecting approximately 50 million people worldwide, and is associated with considerable morbidity and mortality.1 Epilepsy is defined as a predisposition to experience seizures as a result of abnormal (excessive or hypersynchronous) neuronal activity in the brain.2 Seizures are classified as partial (focal) or generalized, depending on the extent to which they affect the brain.3 The majority of patients are diagnosed with idiopathic epilepsy (where a structural cause cannot be found), whereas the remaining are described as symptomatic, and may be the result of structural abnormalities, such as tumor, stroke, head injury, or infection. These definitions are undergoing a significant review in the light of new concepts that have emerged from recent research, such as that of “network epilepsy”, which has challenged the traditional dichotomy between partial/focal and generalized epilepsy.4 Antiepileptic drugs (AEDs) are the mainstay of treatment for epilepsy. Seizure freedom is achieved in around 50% of patients with the first trial of pharmacotherapy, and this is increased with add-on medications.5 Unfortunately AEDs can have suboptimal tolerability profiles, especially with regard to behavioral6,7 and cognitive8,9 aspects. When a patient fails to respond to adequate trials of two AEDs because of poor efficacy and/or tolerability, a diagnosis of “treatment resistant” or “refractory” epilepsy is formulated.10 This occurs in up to one-third of patients with epilepsy.11 In such cases, other treatments are available, including novel AEDs, ketogenic diet, epilepsy surgery, and more recently, implantable neurostimulation devices.11
Three types of implantable neurostimulation devices have been introduced and approved for the management of refractory epilepsy: vagus nerve stimulation (VNS), deep brain stimulation (DBS), and responsive neurostimulation systems (RNSs). After considering the background and proposed mechanisms of action of each of these, we will review the available evidence about their clinical efficacy, safety, and tolerability.
Methods
We conducted a systematic literature search on the PubMed and PsycInfo databases, and retrieved all randomized controlled trials (RCTs) assessing the clinical efficacy of the implantable neurostimulation devices (VNS, DBS, and RNS). Open-label studies assessing clinical efficacy were also included; however, due to large numbers of low-powered studies in the VNS literature, selection criteria were applied. Studies were excluded if they focused on experimental/molecular models, were published in languages other than English, did not report seizure reduction and/or response rates (≥50% reduction in seizures), or if they were conducted on sample sizes smaller than 50 patients. Case reports, letters to the editor, conference abstracts, and commentaries were also excluded. Finally, reference lists from recent review articles were also scanned for further relevant studies.
VNS
VNS is an invasive extracranial neurostimulation technique involving implantation of a device at the level of the subclavian region. Two or three leads are woven around the left vagus nerve and connected to a generator producing electrical impulses that modulate the signals conducted by its afferent fibers. While the electrical test of the device is performed intraoperatively, the device tends to be activated only 1 to 2 weeks postoperatively, often at the first outpatient follow-up. The exact mechanism by which VNS reduces seizure activity is unknown, although several models have been proposed. In particular, it has been suggested that VNS works by increasing cerebral blood flow and activating neuronal networks in the thalamus and other deep brain structures. A potential role for norepinephrine has also been postulated.12
VNS was approved by the US Food and Drug Administration in 1997 as adjunctive treatment in patients over 12 years of age with partial-onset seizures which are refractory to AED treatment. VNS is also approved for use in the treatment of resistant depression and studies are being undertaken assessing its efficacy in a number of other neurological and psychiatric disorders.13
The earliest trials in humans assessing the effect of VNS on seizure outcome in patients with refractory epilepsy were published in the early 1990s, and their encouraging results prompted two large RCTs (Table 1) to build an evidence base for its safety and efficacy.
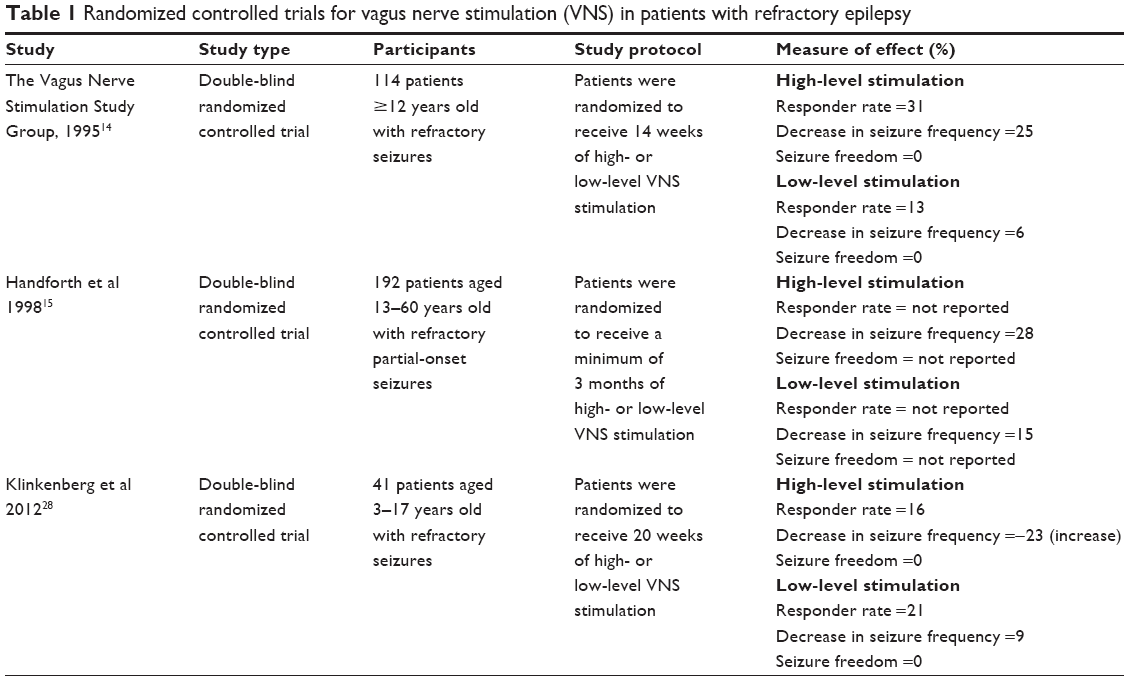 | Table 1 Randomized controlled trials for vagus nerve stimulation (VNS) in patients with refractory epilepsy |
Adult populations
The first RCT was undertaken by The Vagus Nerve Stimulation Study Group, and published in 1995.14 The trial was conducted in 17 centers across North America and Europe, and recruited 114 patients with medically intractable seizures and a wide range of seizure types, who were taking, on average, two AEDs. This study compared efficacy of VNS at high levels versus low stimulation intensity. Patients were blinded to their stimulation setting, as was the investigator responsible for data collection. Each patient received a 14-week trial of VNS, after which their seizure frequency was compared to baseline. In the group receiving high-intensity VNS (presumed therapeutic dose), seizure frequency was reduced by 25%, from a median 0.73 seizures per day at baseline to 0.42 seizures per day after stimulation. Furthermore, a responder rate of 31% was observed. In the group receiving low-intensity VNS (presumed sub-therapeutic dose), seizure frequency was reduced by 6% (from 0.82 seizures per day to 0.80 seizures per day) and a responder rate of 13% was observed. The results of this study confirmed the preliminary findings from smaller open-label studies, and the authors concluded that chronic intermittent left vagus nerve stimulation might be an effective treatment for patients with medically intractable seizures who are not candidates for resective epilepsy surgery.
The second RCT was carried out and published in 1998, looking specifically at the use of VNS in the management of partial-onset seizures.15 A total of 192 patients were randomized to receive either high- or low-level chronic VNS, and were followed-up for a minimum of 3 months. In the group receiving high-level VNS, median seizure frequency was 0.58 seizures per day, which was reduced by 28%, compared to 15% in the group receiving low-level VNS (P=0.04). Patients from this study were followed-up as part of a long-term prospective study,16 where all patients received high-level VNS. At 12 months post-implantation, median seizure reduction was 45%, and responder rate was 35%.
The results of a follow-up study of 440 patients from five clinical trials, including the two RCTs, were published in 1999.17 At baseline, patients had an average of 1.73 seizures per day, and average disease duration was over 20 years. Responder rates were 37% at 1 year, 43% at 2 years, and 43% at 3 years. The efficacy of VNS as a long-term treatment for refractory epilepsy was confirmed by the long-term data. A large number of open-label studies have since been undertaken, looking at the efficacy and safety of VNS as a treatment for different seizure types across several patient populations, including both adults and children. Seven studies looked at VNS as a treatment of refractory epilepsy in predominantly adult populations. Responder rates ranged between 64%18 and 36%,19 although some smaller studies reported rates as high as 86%20 and as low as 10%.21 The largest study to date was undertaken in 2008, and retrospectively analyzed data collected in the VNS therapy patient outcome registry.22 The authors compared VNS treatment in patients who had previously undergone cranial surgery to those who had not. Responder rates for the cranial surgery group were 55%, compared to 62% in the group who had not had surgery. The authors concluded that VNS may be an effective palliative therapy where cranial surgery had previously failed, although it was more beneficial in those who had not undergone surgery.
Other studies compared the effectiveness of VNS for different seizure types, with mixed results. A recent multicenter trial in Israel23 found that VNS was most effective in partial seizures, where the responder rate was 52%, compared to 43% for the whole cohort. The results also showed that VNS was more effective in reducing seizure frequency in patients over the age of 21. However, a previous study of 165 patients19 reported higher responder rates in idiopathic generalized epilepsies (57%) compared to partial epilepsies (47%) or symptomatic generalized epilepsies (46%). In most of the reviewed studies, seizure frequency was recorded between 12 and 24 months post-implantation. Moreover, the duration of follow-up tended to correlate positively with the responder rate. One retrospective study18 recorded seizure frequency in 65 patients who had received VNS therapy over 10 years, and found a responder rate of 86% and a mean decrease in seizure frequency of 76%. The efficacy of VNS as an adjunctive treatment for management of intractable epilepsy was confirmed by a large number of open-label studies.24–27 In one study,24 19% of patients became “seizure-free” or “almost seizure-free” and 49% showed a “worthwhile improvement” post-VNS, according to the Engel Classification, a rating that takes the impact of seizures on daily life into account.
Pediatric populations
An RCT assessing the efficacy of VNS in children with refractory epilepsy was recently undertaken in the Netherlands.28 This study included 41 children aged 3–17 years with a diagnosis of either partial-onset or generalized epilepsy which was refractory to medical treatment. Patients were randomized to receive either high- or low-output VNS. Baseline median seizure frequency was 2.1 seizures per day in the high-output group, and 0.9 seizures per day in the low-output group. Results showed a seizure reduction over 50% in 16% of the high-output and 21% of the low-output group with a weak negative correlation between age at onset and clinical response. The study also reported a positive outcome in terms of quality of life in both groups and the authors concluded that although the effects of VNS on seizure frequency in children may be limited, VNS remains a worthwhile treatment to be considered in children with refractory epilepsy.
In open-label studies assessing VNS in pediatric populations, responder rates varied between 22%29 and 90%.30,31 Even though over 600 young patients have been recruited in prospective and retrospective studies so far, most of these studies have a small sample size, and a number of them focus on specific epilepsy syndromes or etiologies, such as Lennox–Gastaut syndrome32,33 or tuberous sclerosis.30 Although the results of these studies overall suggest that VNS can be a useful treatment for refractory epilepsy in children, generalizing these findings to the broader pediatric population requires large-scale RCTs.
In conclusion, VNS has been shown to be effective in reducing seizure frequency in both adults and children with refractory epilepsy. Acute side effects occur in approximately 3%–6% of patients, and include hoarseness, lower facial palsies, and infections. The most common long-term side effects include an alteration in voice, throat pain, and hoarseness, which can occur in up to 40% of patients.17 Serious side effects such as asystole and bradycardia have been reported, but their incidence is lower than 0.1%.34
DBS
DBS involves the placement of one or more electrode leads into the brain parenchyma. These are connected to a battery-powered implanted pulse generator positioned in the subclavian space.35 Different deep brain structures are targeted depending on the condition to be treated. Stimulation of basal ganglia structures has been widely used in the management of treatment refractory movement disorders such as Parkinson’s disease, dystonia, and tremor.36 DBS has also been used in the treatment of neuropsychiatric conditions such as depression, obsessive-compulsive disorder, chronic pain, cluster headache, and Tourette syndrome.37,38
The exact mechanism of action of DBS in reducing seizure frequency is unknown, and a number of theories have been proposed. It is unclear whether the stimulation from the implanted electrodes results in excitation or inhibition of the local neurons,39 or whether its effects are due to disruption of neuronal transmission.40 A number of RCTs (Table 2) and open-label trials have been conducted looking into the clinical efficacy of DBS as an adjunctive treatment in refractory epilepsy.
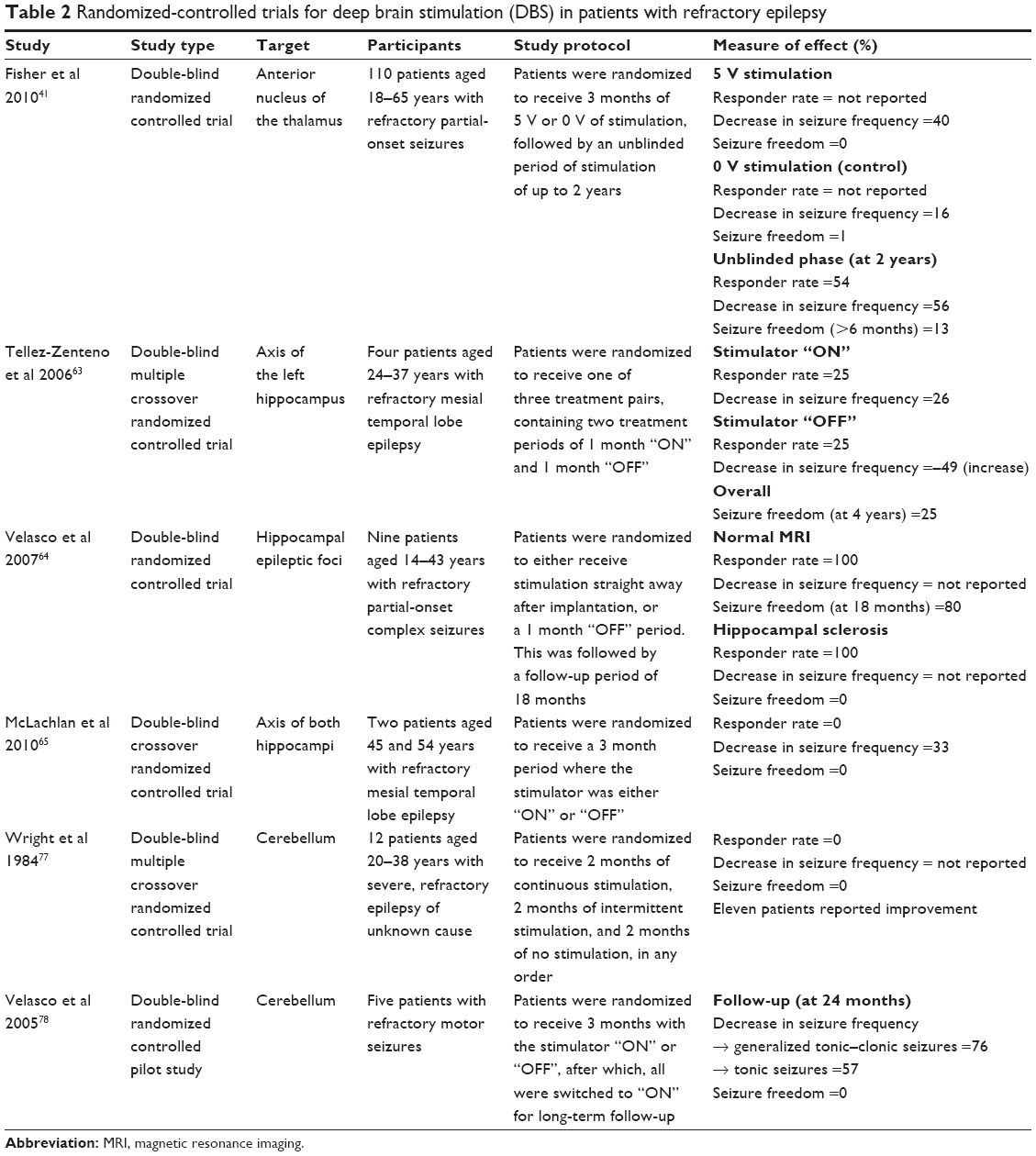 | Table 2 Randomized-controlled trials for deep brain stimulation (DBS) in patients with refractory epilepsy |
Thalamus
Several trials have assessed thalamic structures as targets for DBS, primarily focusing on either the anterior nucleus of the thalamus (ATN) or the centromedian nucleus of the thalamus (CMT).
The largest of these was the stimulation of the anterior nuclei of the thalamus for epilepsy (SANTE) RCT, which was undertaken in 2010.41 DBS electrodes were implanted in 110 patients, who were then randomized to receive either 5 V or 0 V (control) stimulation intensity for 3 months. At baseline, patients in the DBS group had a median of 18.4 seizures per month, compared to 20.4 per month in the control group. After this blinded period, all patients received stimulation from months 4 to 13, followed by a long-term open-label follow-up assessment. At the end of the blinded phase, a median decrease in seizure frequency of 40% was reported in the DBS group, compared to 16% in the control group. Two years after the implantation, median seizure reduction was 56% and responder rate was 54%. This trial provided significant support for the use of ATN DBS in refractory epilepsy, confirming results of previous, smaller scale trials.42–46
Seven open-label studies assessing ATN stimulation for treatment of refractory epilepsy have been undertaken to date, with sample sizes ranging between three and 15 patients.42–48 Responder rates varied between 25%45 and 100%44,46 and the reduction in seizure frequency ranged between 49%45 and 76%.46 Overall, these studies consolidated the findings of the SANTE trial,41 providing supporting evidence that ATN DBS can be an effective treatment for refractory epilepsy.
Seven studies have been undertaken assessing stimulation of the CMT in the treatment of epilepsy. The earliest study was a placebo-controlled crossover pilot trial involving seven patients in which seizure frequency was reduced by 30%.49 More recent studies have been more encouraging with responder rates of 73%,50 92%,51,52 and 100%.53 In a study conducted on 13 patients with Lennox-Gastaut syndrome,52 seizure frequency was reduced by 80%, with a responder rate of 92%. Overall, CMT DBS has been shown to be effective in treating refractory epilepsy, with particular benefit in management of generalized seizures.50,54,55 Large-scale RCTs are needed to provide robust evidence for the use of CMT DBS in clinical practice.
Basal ganglia
A small number of studies have been carried out assessing stimulation of basal ganglia structures as a treatment for refractory epilepsy, making the clinical efficacy of caudate nucleus DBS difficult to assess. Early studies showed that DBS of the caudate nucleus can reduce epileptic electrical activity,56–58 however, only one long-term clinical study has been undertaken to date.59 Of the 38 patients treated with stimulation of the head of the caudate nucleus, 35 (92%) showed a “worthwhile improvement” in mean seizure frequency, which was eleven seizures per month at baseline.
The subthalamic nucleus (STN) has also been investigated as a potential target for DBS in epilepsy. We were able to identify only four studies on STN DBS for epilepsy, reflecting the paucity of scientific literature in this area. Two small open-label studies44,60 and two case reports (each reporting on two patients)61,62 suggested that the use of STN DBS in refractory epilepsy is plausible, although the two patients followed-up in the study by Capecci et al62 showed no improvement and worsening of seizures after treatment. It is evident that this is an area where more research would be valuable, as the current evidence is lacking in statistical power.
Hippocampus
One of the most studied DBS targets in the treatment of refractory epilepsy is the hippocampus. Ten studies have been undertaken, including three small double-blind RCTs,63–65 all of which involved patients with refractory mesial temporal lobe epilepsy. In the first of these,63 four patients with a baseline median seizure frequency of four per month, underwent implantation of a stimulating electrode into the left hippocampus. Patients were randomized to receive three consecutive 2-month treatment regimes, during which the stimulator was randomized to be “ON” for 1 month and “OFF” for another month. Outcomes were assessed at monthly intervals, and the authors reported a 15% median reduction in seizure frequency. They concluded that hippocampal DBS may be beneficial, and has few adverse effects, however their study did not show statistically significant improvements in seizure outcome, unlike other studies.
The second RCT64 followed up nine patients who had undergone electrode implantation into hippocampal foci, which were determined using diagnostic electrode studies. Five of the patients had normal brain magnetic resonance imaging (MRI) scans, and seizure frequency was reduced by over 95% in this group, from a baseline frequency of between 15 and 50 seizures per month. In the remaining four patients, who had hippocampal sclerosis documented by neuroimaging, seizure frequency was reduced by 50%–75%, from a baseline frequency of between 23 and 70 seizures per month. The authors concluded that electrical stimulation of the hippocampus improves seizure outcome in patients with hippocampal epileptic foci, without having detrimental effects on patient memory.
A third study65 used a double-blind, randomized, controlled crossover design to assess bilateral hippocampal DBS in two patients with refractory mesial temporal lobe epilepsy. After implantation, patients underwent a 3-month “baseline” period, during which there was no stimulation. This was followed by a 3-month period during which the stimulator was either “ON” or “OFF” and all “ON” periods were followed by a 3-month “OFF” washout period to look for holdover effect. During stimulation, seizure frequency was decreased by 33%, and a decrease of 25% was maintained during the washout period, despite the lack of stimulation. The authors concluded that hippocampal DBS can have a positive effect on seizure frequency, both during and after stimulation; however, the effect sizes demonstrated in this study were not as large as in previous studies.
Seven further open-label studies have been undertaken since 2002, the majority of which demonstrated encouraging results, albeit with small sample sizes. These studies were fairly homogeneous as far as samples and methods, and reported strikingly similar results. Published responder rates for these studies varied between 57%66 and 100%;67 however, rates for five of the studies were very consistent, between 70% and 78%.68–72
Overall, there is a reasonable evidence base for the use of hippocampal DBS in the treatment of refractory mesial temporal lobe epilepsy. RCTs have been undertaken, albeit with small sample sizes that limit the generalization of the findings. However, encouraging results have been reported in both RCTs and open-label trials, indicating the need for further large trials.
Cerebellum
In the 1970s, Cooper et al73 studied the potential for cerebellar DBS as a treatment for epilepsy, with some encouraging results. One study of 15 patients reported cerebellar stimulation to be useful in two-thirds of the sample,74 while another study demonstrated a significant improvement in 62%.75 These early observational pilot studies73–76 prompted further research to be carried out; however, there is still a lack of evidence in this area.
Two RCTs have been carried out assessing cerebellar DBS as a treatment for refractory epilepsy, with notably different results. The first trial was undertaken in 1984,77 where 12 patients had two electrodes implanted into their cerebellum, after which they were randomized to a 6-month treatment regime. Each regime comprised of three 2-month periods during which the stimulator was either continuously firing, intermittently firing, or not firing at all. There was no significant decrease in seizure frequency, however, patients did report feeling an improvement during the trial.
The second, more recent, RCT was a small pilot study undertaken in 2005 to assess the effects of cerebellar DBS on seizure outcome in refractory epilepsy.78 Five patients underwent bilateral cerebellar electrode implantation, after which the stimulators were “OFF” for 1 month. After this, patients were randomized into two groups, in which stimulators were either “ON” or “OFF” for 3 months. Following this, all stimulators were set to “ON” for the remainder of the study. During the initial double-blind phase, frequency of generalized tonic–clonic seizures decreased significantly in the group receiving stimulation compared to the control group (P=0.023). After both groups had received stimulation for 6 months, mean seizure rate had decreased to 41% of baseline levels. The authors concluded that cerebellar DBS may be an effective and safe treatment for refractory epilepsy, especially generalized tonic–clonic seizures.
While some positive results have been demonstrated, larger trials should be undertaken to estimate the potential benefit of cerebellar DBS, which appears to be a useful and safe treatment option for refractory epilepsy.
Overall, DBS has been shown to be effective in reducing seizure frequency in patients with refractory epilepsy. Evidence is strongest for stimulation of certain targets such as the ATN and the hippocampus, whereas other targets require further investigation in order to build more robust evidence. Although DBS has been shown to be a safe and well-tolerated treatment in most cases, the proportion of patients who achieved seizure freedom was either low or not reported at all. Further studies investigating rates of seizure freedom after DBS treatment may be useful, as absolute seizure freedom is arguably a more important clinical outcome measure than decrease in seizure frequency in this patient population. The majority of large-scale data on the safety of DBS are available only for trials on movement disorders patient populations, and relatively little is known about possible disease-specific adverse effects in patients with epilepsy. Serious complications such as status epilepticus and sudden death have been reported, however these are rare.79 The most commonly reported adverse effects include bleeding, infection, mechanical complications, and neuropsychiatric changes.80–82
Responsive neurostimulation
RNS are a new method of implantable neurostimulation used to treat refractory epilepsy.83 RNS can detect seizure activity in the brain by monitoring electrocorticographic activity and deliver electrical stimulation directly to the seizure foci, in order to suppress seizure activity in a targeted way.84 This process is known as closed-loop stimulation. Implantation involves insertion of electrodes in the target area of the brain, which is then connected to a small device positioned under the skin.85
The results of a large RCT exploring RNS as a novel treatment strategy for refractory epilepsy were published in 2011.83 Responsive neurostimulators were implanted in 191 adults with refractory partial epilepsy, and after 1 month the patients were randomized to receive either stimulation in response to seizure activity (treatment group) or no stimulation (control group). Mean baseline seizure frequency rates did not vary between the two groups, where patients had an average of 1.2 seizures per day. Seizure outcomes were assessed over the 12-week blinded period, after which all patients received responsive stimulation as part of an 84-week open-label continuation study. Seizure frequency was reduced by 38% in the treatment group compared to 17% in the control group (P=0.012), and seizure reduction was maintained during the open-label period. The authors also found that treatment with RNS was associated with improvements in quality of life. Adverse effects reported included pain at the site of implantation, headache, seizure worsening, and memory impairment. The majority of adverse effects were self-limiting and mild, whereas severe side effects were rare.
A number of smaller open-label studies and case reports yielded results in line with those of this RCT. Median seizure frequency reduction ranged between 41% and 76%, demonstrating the benefits of RNS in refractory seizures. These studies were carried out on small samples (between one and eight patients), and used a range of brain targets, including cortical and thalamic zones, as well as identified epileptogenic zones.86–88 Despite limitations in sample size and study methodology, these studies provided promising pilot data for the large RCT.83
Overall, RNS appears to be a promising technique for the treatment of refractory epilepsy; however, it has recently been highlighted that there is considerable room for improvement.89 In particular, potential options are currently being explored in order to improve the accuracy of the seizure prediction method.90 Furthermore, the electrical stimulation parameters need to be standardized, as a wide range of settings were used in the open-label studies. Standardization of study methodology will allow the development of clinical guidelines incorporating this implantable neurostimulation device. In conclusion, RNS is a new method of implantable stimulation that has shown initial improvements in seizure outcome for patients with refractory epilepsy. In order to strengthen the existing evidence base, further large-scale RCTs need to be carried out.
Conclusion
Implantable neurostimulation devices, including VNS, DBS, and RNS, offer promising avenues for reduction in seizure frequency in patients with refractory epilepsy, a group of patients that present high morbidity, mortality, and reduced quality of life. Seizure freedom appears to be a less realistic expectation according to published data, possibly reflecting selection bias. Furthermore, average seizure frequencies before and after treatment are inconsistently reported across the reviewed studies, making it difficult to fully appreciate the exact magnitude of percentage decreases. Future studies will certainly continue to refine our ability to determine the impact of these treatment options on clinical practice. Further research should be carried out to explore other potential benefits of implantable neurostimulation devices; for example, reducing seizure severity. This may include prevention of spread of epileptic discharge or the occurrence of loss of consciousness across both partial-onset and generalized seizures.91–95 A further aspect to make this therapeutic option appealing is the relatively low prevalence of serious adverse effects, a factor contributing to significant improvement in health-related quality of life.
Disclosure
Joanna H Cox has no conflicts of interest to declare; Stefano Seri has received unrestricted educational grants from Eisai Pharmaceuticals, UCB Pharma, and Beacon Pharmaceuticals Limited; Andrea E Cavanna has received Board Membership fees and research grants from Eisai Pharmaceuticals and lectureship grants from Eisai Pharmaceuticals and Janssen-Cilag. The authors report no other conflicts of interest in this work.
References
World Health Organization. The World Health Report 2001 – Mental Health: New Understanding, New Hope. Geneva: World Health Organization; 2001. Available from: http://www.who.int/whr/2001/en/whr01_en.pdf?ua=1. Accessed September 18, 2014. | ||
Fisher RS, Acevedo C, Arzimanoglou A, et al. ILAE Official Report: A practical clinical definition of epilepsy. Epilepsia. 2014;55(4):475–482. | ||
Shorvon SD. The etiologic classification of epilepsy. Epilepsia. 2011;52(6):1052–1057. | ||
Berg AT, Scheffer IE. New concepts in classification of the epilepsies: Entering the 21st century. Epilepsia. 2011;52(6):1058–1062. | ||
Brodie MJ, Barry SJ, Bamagous GA, Norrie JD, Kwan P. Patterns of treatment response in newly diagnosed epilepsy. Neurology. 2012;78(20):1548–1554. | ||
Eddy CM, Rickards H, Cavanna AE. Behavioral adverse effects of antiepileptic drugs in epilepsy. J Clin Psychopharmacol. 2012;32(3):362–375. | ||
Piedad J, Rickards H, Besag F, Cavanna AE. Beneficial and adverse psychotropic effects of antiepileptic drugs in patients with epilepsy: A summary of prevalence, underlying mechanisms and data limitations. CNS Drugs. 2012;26(4):319–335. | ||
Cavanna AE, Ali F, Rickards HE, McCorry D. Behavioural and cognitive effects of anti-epileptic drugs. Discov Med. 2010;9(45):138–144. | ||
Eddy CM, Rickards HE, Cavanna AE. The cognitive impact of antiepileptic drugs. Ther Adv Neurol Disord. 2011;4(6):385–407. | ||
Berg AT. Identification of pharmacoresistant epilepsy. Neurol Clin. 2009;27(4):1003–1013. | ||
Mitchell JW, Seri S, Cavanna AE. Pharmacotherapeutic and non-pharmacological options for refractory and difficult-to-treat seizures. J Cent Nerv Syst Dis. 2012;4:105–115. | ||
Ben-Menachem E. Vagus nerve stimulation for the treatment of epilepsy. Lancet Neurol. 2002;1(8):477–482. | ||
Howland RH. Vagus nerve stimulation. Curr Behav Neurosci Rep. 2014;1(2):64–73. | ||
A randomized controlled trial of chronic vagus nerve stimulation of medically intractable seizures. The Vagus Nerve Stimulation Study Group. Neurology. 1995;45(2):224–230. | ||
Handforth A, DeGiorgio CM, Schachter SC, et al. Vagus nerve stimulation therapy for partial-onset seizures: a randomized active-control trial. Neurology. 1998;51(1):48–55. | ||
DeGiorgio CM, Schachter SC, Handforth A, et al. Prospective long-term study of vagus nerve stimulation for the treatment of refractory seizures. Epilepsia. 2000;41(9):1195–1200. | ||
Morris GL, Mueller WM. Long-term treatment with vagus nerve stimulation in patients with refractory epilepsy. The Vagus Nerve Stimulation Study Group E01–E05. Neurology. 1999;53(8):1731–1735. | ||
Elliott RE, Morsi A, Kalhorn SP, et al. Vagus nerve stimulation in 436 consecutive patients with treatment-resistant epilepsy: long-term outcomes and predictors of response. Epilepsy Behav. 2011;20(1):57–63. | ||
Ng M, Devinsky O. Vagus nerve stimulation for refractory idiopathic generalised epilepsy. Seizure. 2004;13(3):176–178. | ||
Elliott RE, Morsi A, Tanweer O, et al. Efficacy of vagus nerve stimulation over time: review of 65 consecutive patients with treatment-resistant epilepsy treated with VNS >10 years. Epilepsy Behav. 2011;20(3):478–483. | ||
Ben-Menachem E, Rydenhag B, Silander H. Preliminary experience with a new system for vagus nerve stimulation for the treatment of refractory focal onset seizures. Epilepsy Behav. 2013;29(2):416–419. | ||
Amar AP, Apuzzo ML, Liu CY. Vagus nerve stimulation therapy after failed cranial surgery for intractable epilepsy: results from the vagus nerve stimulation therapy patient outcome registry. Neurosurgery. 2008;62 Suppl 2:506–513. | ||
Menascu S, Kremer U, Schiller Y, et al. The Israeli retrospective multicenter open-label study evaluating vagus nerve stimulation efficacy in children and adults. Isr Med Assoc J. 2013;15(11):673–677. | ||
Wheeler M, De Herdt V, Vonck K, et al. Efficacy of vagus nerve stimulation for refractory epilepsy among patient subgroups: a re-analysis using the Engel classification. Seizure. 2011;20(4):331–335. | ||
Ghaemi K, Elsharkaway AE, Schulz R, et al. Vagus nerve stimulation: outcome and predictors of seizure freedom in long-term follow-up. Seizure. 2010;19(5):264–268. | ||
De Herdt V, Boon P, Ceulemans B, et al. Vagus nerve stimulation for refractory epilepsy: a Belgian multicenter study. Eur J Paediatr Neurol. 2007;11(5):261–269. | ||
Vonck K, Thadani V, Gilbert K, et al. Vagus nerve stimulation for refractory epilepsy: a transatlantic experience. J Clin Neurophysiol. 2004;21(4):283–289. | ||
Klinkenberg S, Aalbers MW, Vles JS, et al. Vagus nerve stimulation in children with intractable epilepsy: a randomized controlled trial. Dev Med Child Neurol. 2012;54(9):855–861. | ||
Saneto RP, Sotero de Menezes MA, Ojemann JG, et al. Vagus nerve stimulation for intractable seizures in children. Pediatr Neurol. 2006;35(5):323–326. | ||
Parain D, Penniello MJ, Berquen P, Delangre T, Billard C, Murphy JV. Vagal nerve stimulation in tuberous sclerosis complex patients. Paediatr Neurol. 2001;25(3):213–216. | ||
Wakai S, Kotagal P. Vagus nerve stimulation for children and adolescents with intractable epilepsies. Paediatr Int. 2001;43(1):61–65. | ||
Frost M, Gates J, Helmers SL, et al. Vagus nerve stimulation in children with refractory seizures associated with Lennox-Gastaut syndrome. Epilepsia. 2001;42(9):1148–1152. | ||
Cukiert A, Cukiert CM, Burattini JA, et al. A prospective long-term study on the outcome after vagus nerve stimulation at maximally tolerated current intensity in a cohort of children with refractory secondary generalized epilepsy. Neuromodulation. 2013;16(6):551–556; discussion 556. | ||
Tatum WO, Vale FL. Vagus nerve stimulation and cardiac asystole. Epilepsia. 2009;50(12):2671–2672. | ||
Miocinovic S, Somayajula S, Chitnis S, Vitek JL. History, applications, and mechanisms of deep brains stimulation. JAMA Neurol. 2013;70(2):163–171. | ||
Gross RE, Lozano AM. Advances in neurostimulation for movement disorders. Neurol Res. 2000;22(3):247–258. | ||
Kringelbach ML, Jenkinson N, Owen SL, Aziz TZ. Translational principles of deep brain stimulation. Nat Rev Neurosci. 2007;8(8):623–635. | ||
Cavanna AE, Eddy CM, Mitchell R, et al. An approach to deep brain stimulation for severe treatment-refractory Tourette syndrome: the UK perspective. Br J Neurosurg. 2011;25(1):38–44. | ||
Hammond C, Ammari R, Bioulac B, Garcia L. Latest view on the mechanism of action of deep brain stimulation. Mov Disord. 2008;23(15):2111–2121. | ||
Chiken S, Nambu A. Disrupting neuronal transmission: mechanism of DBS? Front Syst Neurosci. 2014;8:33. | ||
Fisher R, Salanova V, Witt T, et al; SANTE Study Group. Electrical stimulation of the anterior nucleus of thalamus for treatment of refractory epilepsy. Epilepsia. 2010;51(5):899–908. | ||
Hodaie M, Wennberg RA, Dostrovsky JO, Lozano AM. Chronic anterior thalamus stimulation for intractable epilepsy. Epilepsia. 2002;43(6):603–608. | ||
Kerrigan JF, Litt B, Fisher RS, et al. Electrical stimulation of the anterior nucleus of the thalamus for the treatment of intractable epilepsy. Epilepsia. 2004;45(4):346–354. | ||
Lee KJ, Jang KS, Shon YM. Chronic deep brain stimulation of subthalamic and anterior thalamic nuclei for controlling refractory partial epilepsy. Acta Neurochir Suppl. 2006;99:87–91. | ||
Lim SN, Lee ST, Tsai YT, et al. Electrical stimulation of the anterior nucleus of the thalamus for intractable epilepsy: a long-term follow-up study. Epilepsia. 2007;48(2):342–347. | ||
Osorio I, Overman J, Giftakis J, Wilkinson SB. High frequency thalamic stimulation for inoperable mesial temporal epilepsy. Epilepsia. 2007;48(8):1561–1571. | ||
Lee KJ, Shon YM, Cho CB. Long-term outcome of anterior thalamic nucleus stimulation for intractable epilepsy. Stereotact Funct Neurosurg. 2012;90(6):379–385. | ||
Oh Y, Kim HJ, Lee KJ, Kim YI, Lim S, Shon Y. Cognitive improvement after long-term electrical stimulation of bilateral anterior thalamic nucleus in refractory epilepsy patients. Seizure. 2012;21(3):183–187. | ||
Fisher RS, Uematsu S, Krauss GL, et al. Placebo-controlled pilot study of centromedian thalamic stimulation in treatment of intractable seizures. Epilepsia. 1992;33(5):841–851. | ||
Valentín A, García Navarrete E, Chelvarajah R, et al. Deep brain stimulation of the centromedian thalamic nucleus for the treatment of generalized and frontal epilepsies. Epilepsia. 2013;54(10):1823–1833. | ||
Velasco F, Velasco M, Jiménez F, et al. Predictors in the treatment of difficult-to-control seizures by electrical stimulation of the centromedian thalamic nucleus. Neurosurgery. 2000;47(2):295–304; discussion 304–305. | ||
Velasco AL, Velasco F, Jiménez F, et al. Neuromodulation of the centromedian thalamic nuclei in the treatment of generalized seizures and the improvement of the quality of life in patients with Lennox-Gastaut syndrome. Epilepsia. 2006;47(7):1203–1212. | ||
Cukiert A, Burattini JA, Cukiert CM, et al. Centro-median stimulation yields additional seizure frequency and attention improvement in patients previously submitted to callosotomy. Seizure. 2009;18(8):588–592. | ||
Velasco F, Velasco M, Velasco AL, Jimenez F, Marquez I, Rise M. Electrical stimulation of the centromedian thalamic nucleus in control of seizures: long-term studies. Epilepsia. 1995;36(1):63–71. | ||
Velasco F, Velasco M, Jimenez F, Velasco AL, Marquez I. Stimulation of the central median thalamic nucleus for epilepsy. Stereotact Funct Neurosurg. 2001;77(1–4):228–232. | ||
Sramka M, Fritz G, Galanda M, Nádvornik P. Some observations in treatment stimulation of epilepsy. Acta Neurochir (Wien). 1976;(23 Suppl):257–262. | ||
Sramka M, Chkhenkeli SA. Clinical experience in intraoperational determination of brain inhibitory structures and application of implanted neurostimulators in epilepsy. Stereotact Funct Neurosurg. 1990;54–55:56–59. | ||
Chkhenkeli SA, Chkhenkheli IS. Effects of therapeutic stimulation of nucleus caudatus on epileptic electrical activity of brain in patients with intractable epilepsy. Stereotact Funct Neurosurg. 1997;69(1–4 Pt 2):221–224. | ||
Chkhenkeli SA, Sramka M, Lortkipanidze GS, et al. Electrophysiological effects and clinical results of direct brain stimulation for intractable epilepsy. Clin Neurol Neurosurg. 2004;106(4):318–329. | ||
Chabardes S, Kahane P, Minotti L, Koudsie A, Hirsch E, Benabid AL. Deep brain stimulation in epilepsy with particular reference to the subthalamic nucleus. Epileptic Disord. 2002;4 Suppl 3:S83–S93. | ||
Handforth A, DeSalles AA, Krahl SE. Deep brain stimulation of the subthalamic nucleus as adjunct treatment for refractory epilepsy. Epilepsia. 2006;47(7):1239–1241. | ||
Capecci M, Ricciuti RA, Ortenzi A, et al. Chronic bilateral subthalamic stimulation after anterior callosotomy in drug-resistant epilepsy: long-term clinical and functional outcome of two cases. Epilepsy Res. 2012;98(2–3):135–139. | ||
Tellez-Zenteno JF, McLachlan RS, Parrent A, Kubu CS, Wiebe S. Hippocampal electrical stimulation in mesial temporal lobe epilepsy. Neurology. 2006;66(10):1490–1494. | ||
Velasco AL, Velasco F, Velasco M, Trejo D, Castro G, Carrillo-Ruiz JD. Electrical stimulation of the hippocampal epileptic foci for seizure control: a double-blind, long-term follow-up study. Epilepsia. 2007;48(10):1895–1903. | ||
McLachlan RS, Pigott S, Tellez-Zenteno JF, Wiebe S, Parrent A. Bilateral hippocampal stimulation for intractable temporal lobe epilepsy: impact on seizures and memory. Epilepsia. 2010;51(2):304–307. | ||
Vonck K, Boon P, Achten E, De Reuck J, Caemaert J. Long-term amygdalohippocampal stimulation for refractory temporal lobe epilepsy. Ann Neurol. 2002;52(5):556–565. | ||
Vonck K, Boon P, Claeys P, Dedeurwaerdere S, Achten R, Van Roost D. Long-term deep brain stimulation for refractory temporal lobe epilepsy. Epilepsia. 2005;46 Suppl 5:98–99. | ||
Boon P, Vonck K, De Herdt V, et al. Deep brain stimulation in patients with refractory temporal lobe epilepsy. Epilepsia. 2007;48(8):1551–1560. | ||
Boëx C, Seeck M, Vulliémoz S, et al. Chronic deep brain stimulation in mesial temporal lobe epilepsy. Seizure. 2011;20(6):485–490. | ||
Vonck K, Sprengers M, Carrette E, et al. A decade of experience with deep brain stimulation for patients with refractory medial temporal lobe epilepsy. Int J Neural Syst. 2013;23(1):1250034. | ||
Bondallaz P, Boëx C, Rossetti AO, et al. Electrode location and clinical outcome in hippocampal electrical stimulation for mesial temporal lobe epilepsy. Seizure. 2013;22(5):390–395. | ||
Cukiert A, Cukiert CM, Burattini JA, Lima AM. Seizure outcome after hippocampal deep brain stimulation in a prospective cohort of patients with refractory temporal lobe epilepsy. Seizure. 2014;23(1):6–9. | ||
Cooper IS, Amin I, Gilman S. The effect of chronic cerebellar stimulation upon epilepsy in man. Trans Am Neurol Assoc. 1973;98:192–196. | ||
Cooper IS, Amin I, Riklan M, Waltz JM, Poon TP. Chronic cerebellar stimulation in epilepsy. Clinical and anatomical studies. Arch Neurol. 1976;33(8):559–570. | ||
Cooper IS, Amin I, Upton A, Riklan M, Watkins S, McLellan L. Safety and efficacy of chronic stimulation. Neurosurgery. 1977;1(2):203–205. | ||
Cooper IS, Upton AR. Effects of cerebellar stimulation on epilepsy, the EEG and cerebral palsy in man. Electroencephalogr Clin Neurophysiol Suppl. 1978;(34):349–354. | ||
Wright GD, McLellan DL, Brice JG. A double-blind trial of chronic cerebellar stimulation in twelve patients with severe epilepsy. J Neurol Neurosurg Psychiatry. 1984;47(8):769–774. | ||
Velasco F, Carrillo-Ruiz JD, Brito F, et al. Double-blind, randomized controlled pilot study of bilateral cerebellar stimulation for treatment of intractable motor seizures. Epilepsia. 2005;46(7):1071–1081. | ||
Fountas KN, Kapsalaki E, Hadjigeorgiou G. Cerebellar stimulation in the management of medically intractable epilepsy: A systematic and critical review. Neurosurg Focus. 2010;29(2):E8. | ||
Boviatsis EJ, Stavrunou LC, Themistocleous M, Kouyialis AT, Sakas DE. Surgical and hardware complications of deep brain stimulation. A seven-year experience and review of the literature. Acta Neurochir (Wien). 2010;152(12):2053–2062. | ||
Sharma A, Szeto K, Desilets AR. Efficacy and safety of deep brain stimulation as an adjunct to pharmacotherapy for the treatment of Parkinson disease. Ann Pharmacother. 2012;46(2):248–254. | ||
Kulisevsky J, Berthier ML, Gironell A, Pascual-Sedano B, Molet J, Parés P. Mania following deep brain stimulation for Parkinson’s disease. Neurology. 2002;59(9):1421–1424. | ||
Morrell MJ; RNS System in Epilepsy Study Group. Responsive cortical stimulation for the treatment of medically intractable partial epilepsy. Neurology. 2011;77(13):1295–1304. | ||
Fridley J, Thomas JG, Navarro JC, Yoshor D. Brain stimulation for the treatment of epilepsy. Neurosurg Focus. 2012;32(3):E13. | ||
Ge Y, Hu W, Liu C, Zhang JG, Meng FG. Brain stimulation for treatment of refractory epilepsy. Chin Med J (Engl). 2013;126(17):3364–3370. | ||
Osorio I, Frei MG, Sunderam S, et al. Automated seizure abatement in humans using electrical stimulation. Ann Neurol. 2005;57(2):258–268. | ||
Anderson WS, Kossoff EH, Bergey GK, Jallo GI. Implantation of a responsive neurostimulator device in patients with refractory epilepsy. Neurosurg Focus. 2008;25(3):E12. | ||
Smith JR, Fountas KN, Murro AM, et al. Closed-loop stimulation in the control of focal epilepsy of insular origin. Stereotact Funct Neurosurg. 2010;88(5):281–287. | ||
Ryvlin P, Rheims S. Epilepsy: new epidemiological and therapeutic perspectives. Lancet Neurol. 2012;11(1):5–7. | ||
Liu C, Wen XW, Ge Y, et al. Responsive neurostimulation for the treatment of medically intractable epilepsy. Brain Res Bull. 2013;97:39–47. | ||
Cavanna AE, Monaco F. Brain mechanisms of altered conscious states during epileptic seizures. Nat Rev Neurol. 2009;5(5):267–276. | ||
Bagshaw AP, Cavanna AE. Brain mechanisms of altered consciousness in focal seizures. Behav Neurol. 2011;24(1):35–41. | ||
Seri S, Brazzo D, Thai NJ, Cerquiglini A. Brain mechanisms of altered consciousness in generalised seizures. Behav Neurol. 2011;24(1):43–46. | ||
Blumenfeld H. Impaired consciousness in epilepsy. Lancet Neurol. 2012;11(9):814–826. | ||
Foley E, Cerquiglini A, Cavanna A, et al. Magnetoencephalography in the study of epilepsy and consciousness. Epilepsy Behav. 2014;30:38–42. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.