")
Back to Journals » International Journal of Women's Health » Volume 7
Clinical utility of exemestane in the treatment of breast cancer
Authors Zucchini G, Geuna E, Milani A, Aversa C, Martinello R, Montemurro F
Received 28 February 2015
Accepted for publication 4 May 2015
Published 27 May 2015 Volume 2015:7 Pages 551—563
DOI https://doi.org/10.2147/IJWH.S69475
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Elie Al-Chaer
Giorgia Zucchini,1 Elena Geuna,1 Andrea Milani,1 Caterina Aversa,2 Rossella Martinello,2 Filippo Montemurro1
1Investigative Clinical Oncology, Fondazione del Piemonte per l’Oncologia-Candiolo Cancer Institute (IRCCs), Candiolo, 2University of Turin Medical School, Turin, Italy
Abstract: Breast cancer is the most prevalent cancer in women, causing a significant mortality worldwide. Different endocrine strategies are available for the treatment of hormone-sensitive breast cancer, including antiestrogen tamoxifen and fulvestrant, as well as third-generation aromatase inhibitors (AIs), such as letrozole, anastrozole, and exemestane. In this review, we will focus on exemestane, its clinical use, and its side effects. Exemestane is a steroidal third-generation AI now used in all treatment settings for breast cancer. In the metastatic disease, it has been extensively investigated as the first-, second-, and further-line treatment and it is now registered for the treatment of postmenopausal women with advanced estrogen-receptor-positive breast cancer whose disease has progressed following antiestrogen therapy. A potential lack of cross-resistance with nonsteroidal AIs has been described, giving additional therapeutic opportunities in sequences of endocrine agents. Exemestane is also approved for the adjuvant treatment of postmenopausal early breast cancer, either as upfront monotherapy for 5 years, as a switch following 2–3 years of tamoxifen, or as extended therapy beyond 5 years of adjuvant treatment. New promising data also showed a beneficial effect in young premenopausal early breast cancer patients, when administered together with ovarian suppression. Interesting results have also emerged when exemestane has been investigated as neodjuvant treatment as well as preventive agent in healthy women at high risk for breast cancer. Exemestane is generally well tolerated, with a side effect profile similar to that of other AIs, including menopausal symptoms, arthralgia, and bone loss. In conclusion, exemestane can be considered an effective and well-tolerated endocrine treatment option for all stages of breast cancer.
Keywords: breast cancer, endocrine therapy, aromatase inhibitors, exemestane
Introduction
Breast cancer is one of the most frequently diagnosed cancers among women, with approximately 232,340 new cases and 39,620 deaths estimated among US women in 2013.1 Corresponding figures in the European Union are 358,967 and 90,800, respectively.2,3
Estrogen hormones have been implicated in promoting breast cancer development and progression in the majority of women. Endocrine manipulation has been exploited therapeutically for more than a century, starting from empirical observations of regression of locally advanced breast cancers after oophorectomy in premenopausal patients.4
While ovaries represent the main source of estrogens in premenopausal women, the principal source of circulating estrogens in the postmenopausal stage is the aromatization of the adrenal and ovarian androgens androstenedione and testosterone to estrogens. Aromatase, a member of the cytochrome P-450 (CYP) family located predominantly in the liver, adrenal glands, and fat tissue, is responsible for this reaction.5
Different endocrine strategies have been developed for the treatment of hormone-sensitive breast cancer, depending on the patient’s menopausal status: 1) blockade/downregulation of estrogen receptor (ER) obtained with the selective ER modulator (SERM) tamoxifen and the selective ER downregulator (SERD) fulvestrant, 2) inhibition of estradiol biosynthesis by blocking the production of gonadotropins (follicle-stimulating hormone/luteinizing hormone) with gonadotropin-releasing hormone (GnRH) agonists in premenopausal women and, finally 3) inhibition of peripheral tissue production of estrogen using aromatase inhibitors (AIs) in postmenopause.
AIs can be subdivided into two major groups: steroidal AIs (SAIs) and nonsteroidal AIs (NSAIs) and, according to the chronologic order of their clinical development, they are classified as first-, second-, and third-generation inhibitors.
Early first-generation inhibitors, such as aminoglutethimide, showed reasonable efficacy against metastatic breast cancer.6 However, they lacked specificity, antagonizing the production of mineralocorticoids and glucocorticoids in addition to sex steroids, resulting in excessive toxicity.7
Second-generation agents, namely, formestane and fadrozole, had fewer side effects compared with aminoglutethimide, but they showed limited efficacy.8–12
Subsequently, more specific antagonists of aromatase have been developed and, at the present time, the three third-generation compounds available are anastrozole, letrozole, and exemestane. The first two are categorized as reversible NSAIs, whereas exemestane is an irreversible SAI.13,14
This review will address the steroidal irreversible antagonist exemestane, with a major focus on its developmental steps and clinical applications in the treatment of hormone-sensitive breast cancer.
Pharmacology and preclinical development
Exemestane (6-methylenandrosta-1,4-diene-3,17-dione) is an irreversible SAI. Due to its androstenedione-like structure, exemestane competes with the natural substrates androstenedione and testosterone. By forming covalent bonds with the substrate-binding site of the enzyme, it finally leads to irreversible aromatase inactivation, a mechanism that has been defined “suicidal inhibition.”15–17
Preliminary in vitro studies described exemestane to be a potent inhibitor with a higher aromatase affinity when compared with other structurally related compounds.18,19
The antitumor activity of exemestane was then assessed and confirmed in vivo in animal rat models harboring 7,12-dimethylbenzanthracene (DMBA)-induced mammary tumors. These experiments revealed that exemestane was highly effective when administered by both subcutaneous and oral routes,20 with a greater efficacy than that observed for the steroidal AIs formestane, atamestane, and plomestane in similar models.21,22
An oral dose of exemestane is rapidly absorbed, with peak plasma concentrations reached within 2 hours of administration. After 4 hours, plasma concentrations fall to undetectable levels, although inhibitory activity persists for at least 5 days despite a plasma half-life of only 27 hours. This long-lasting effect may be due to the irreversible aromatase inhibition; thus a new enzyme biosynthesis is required to renew estrogen production, leading to a persistent inhibitory effect even after clearance.23
Metabolism occurs through CYP3A4; however, inhibition of the activity of the major CYP enzymes experienced in healthy volounteers does not seem to influence exemestane disposition.24
The main exemestane metabolite identified in the plasma is 17-hydroxyexemestane, showing concentrations nearly ten times less than that of the parental compound. Other metabolites are inactive or inhibit aromatase with decreased potency.23
Because exemestane and its metabolites are excreted in both urine and feces, impaired renal as well as hepatic function both lead to reduced metabolism, with consequent elevated plasma levels.25
Exemestane induces maximal estradiol suppression after 3–7 days, reaching steady-state levels within 7 days with daily dosing.23,26
The initial Phase I clinical trials identified a daily exemestane oral dose of 25 mg as the minimum effective dose producing the highest degree of estrogen suppression.23,27,28 This dosage was found to inactivate 98% of the total aromatase activity, resulting in a 85%–95% reduction of plasma estrone, estradiol, and estrone sulfate levels, compared to pretreatment levels.29 This level of inhibition appears in the range of that described for the other third-generation AIs and compares favorably with the <90% inhibition described for first- and second-generation inhibitors.30
Comparative studies revealed exemestane administered at 25 mg/day to inhibit aromatization as efficiently as anastrozole administered at 1 mg/day,31 while letrozole 2.5 mg/day appeared to be a more potent inhibitor compared with these two agents.32
However, the limits related to plasmatic estrogen level measurements do not allow drawing solid conclusions regarding potential differences among the three inhibitors. Indeed, clinical studies attempting to compare clinical efficacy of SAIs and NSAIs in patients with hormone-dependent metastatic breast cancer have provided inconclusive results.33–35 This would suggest that the minor differences in inhibitory degrees detected for the three third-generation AIs would not translate into significant clinical differences in terms of efficacy.
Clinical applications
Metastatic setting
The third-generation AIs anastrozole, letrozole, and exemestane have a well-established role in the treatment of hormone-receptor-positive locally advanced or metastatic breast cancer.36–43 Having shown superiority over tamoxifen in a number of randomized Phase III studies, they represent the treatment of choice in postmenopausal women who are endocrine naïve or have been previously exposed to tamoxifen.39–43
Exemestane was initially assesssed in clinical studies as a third-line therapy for metastatic breast cancer, demonstrating meaningful antitumor activity in patients previously exposed to tamoxifen and megestrol acetate,44 as well as to NSAIs.45 A subsequent study revealed the superiority of exemestane in terms of time-to-tumor progression (TTP) and overall survival (OS) relative to megestrol acetate in patients with tamoxifen-resistant disease.38 As a result, exemestane received US Food and Drug Administration approval in October 1999 for the treatment of advanced breast cancer in postmenopausal women whose disease had progressed following tamoxifen (Table 1).
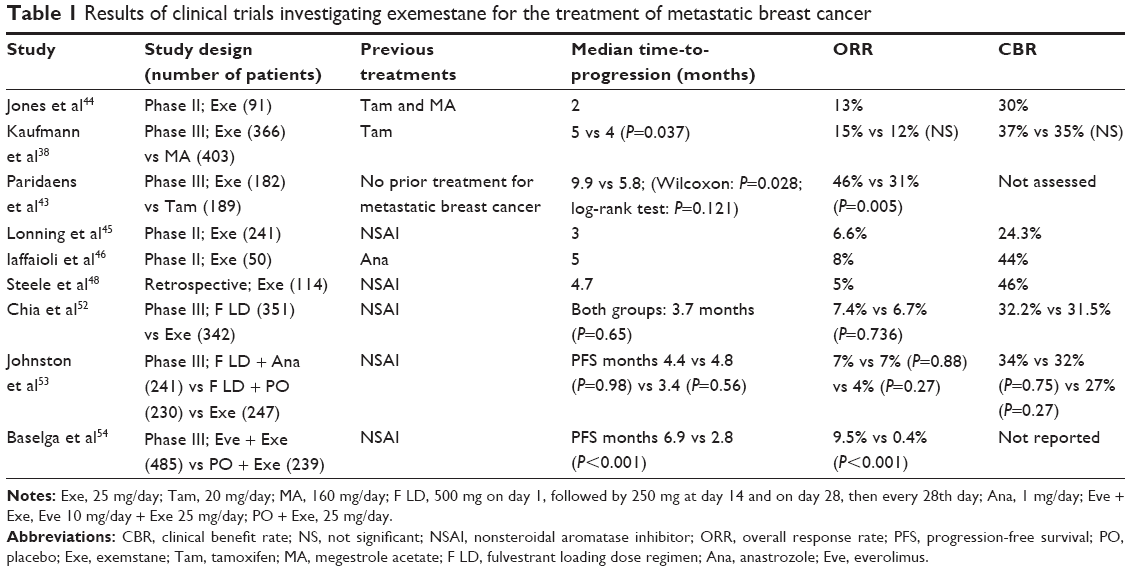 | Table 1 Results of clinical trials investigating exemestane for the treatment of metastatic breast cancer |
On the basis of these positive results, a subsequent European Organisation for the Research and Treatment of Cancer Phase III trial was conducted to investigate the activity of exemestane compared to tamoxifen as first-line treatment for postmenopausal hormone-dependent metastatic breast cancer patients.43 A total of 371 patients were enrolled and followed up for a median time of 46 months. Overall response rate (ORR) was higher for exemestane compared to tamoxifen (46% vs 31%; hazard ratio [HR] =1.85; 95% confidence interval [CI]: 1.21–2.82; P=0.005). However, despite a difference in median progression-free survival (PFS) favoring exemestane (9.9 months vs 5.8 months), the PFS curves converged at approximately 1.4 years. Consequently, no statistically significant difference was seen in long-term PFS, which was the primary end point of the study. Similarly, OS was comparable in the two treatment arms.
Several nonrandomized studies explored the efficacy of exemestane in patients resistant to previous third-generation NSAIs. Reports of activity of exemestane suggested a certain degree of non-cross-resistance between the third-generation steroidal and nonsteroidal compounds.45–51
In fact, on average, 25%–30% of patients in these studies experienced objective response or stable disease for 6 months or longer. Conversly, a degree of activity was observed even when NSAIs were administered in patients progressing after exemestane.47,50
By virtue of its potential non-cross-resistance with NSAIS, exemestane has been used as the conventional treatment arm in clinical trials aimed at developing effective endocrine therapy options in women failing prior treatment with anastrozole or letrozole.52–54
In the randomized, double-blind, placebo-controlled multicenter Phase III Evaluation of Faslodex vs Exemestane Clinical Trial (EFECT), the selective SERD fulvestrant (“loading dose”: 500 mg on Day 1, followed by 250 mg at Day 14 and on Day 28, then every 28 days) was compared with exemestane 25 mg/day in 693 postmenopausal women with hormone-receptor-positive advanced breast cancer after progression/recurrence with an NSAI. No significant differences in the primary end point of TTP were observed between the two groups (median TTP: 3.7 months for both treatments). Similarly, ORR (7.4% vs 6.7%; P=0.736) and clinical benefit rate (CBR) (32.2% vs 31.5%; P=0.853) were not different between the two treatment arms.52
The Study of Faslodex with or without concomitant Arimidex vs Exemestane (SoFEA) was a three-arm, randomized Phase III trial comparing the combination of fulvestrant (loading dose) plus anastrozole 1 mg/day versus fulvestrant (loading dose) with placebo, versus exemestane 25 mg/day, in 723 postmenopausal women with hormone-receptor-positive advanced breast cancer after progression on NSAIs. After a median follow-up of 37.9 months, no differences in the primary end point PFS were detected between patients assigned to fulvestrant plus anastrozole and fulvestrant plus placebo (4.4 vs 4.8 months, HR: 1.00, 95% CI: 0.83–1.21; P=0.56), or between those assigned to fulvestrant plus placebo and exemestane (4.8 vs 3.4 months; HR: 0.95; 95% CI: 0.79–1.14; P=0.56). The CBR rate was similar across the three groups (34%, 32%, and 27% for fulvestrant with anastrozole, fulvestrant with placebo, and exemestane, respectively). An ORR of 4% was observed for exemestane alone, compared to a 7% ORR observed for the two other treatment arms; these differences were not statistically significant.53
The Breast Cancer Trials of Oral Everolimus-2 (BOLERO-2), was a randomized Phase III study comparing the combination of the mammalian target of rapamycin (m-TOR) inhibitor everolimus 10 mg/day + exemestane 25 mg/day versus placebo + exemestane 25 mg/day in 724 postmenopausal women with hormone-receptor-positive advanced breast cancer refractory to previous NSAIs.
In this trial, exemestane yielded modest antitumor activity, with an ORR of 0.4% and a median PFS of only 2.8 months. The addition of everolimus was associated with higher ORR (9.5%) and, most importantly, with a 6.9 months median PFS.54 On the basis of these data, the association of exemestane and everolimus is now registered in patients with hormone-receptor-positive advanced breast cancer that is either in relapse after adjuvant NSAIs treatment or progressing during NSAIs administered for advanced disease.
Adjuvant setting: postmenopausal women
On the basis of a number of pivotal Phase III clinical trials, the three third-generation AIs anastrozole, letrozole, and exemestane are now the therapy of choice in the adjuvant treatment of postmenopausal women with hormone-receptor-positive, operable breast cancer.
In comparison with 5 years of tamoxifen, AIs were given as either upfront treatment for 5 years,55–57 as sequential treatment after a period of 2–3 years on tamoxifen (early switch),58–63 or following completion of 5 years of tamoxifen (late switch).64–66
Adjuvant exemestane was evaluated in three major adjuvant studies (Table 2): the Intergroup Exemestane Study (IES), the Tamoxifen, Exemestane, Adjuvant, Multicenter (TEAM) study, and the National Surgical Adjuvant Breast and Bowel Project (NSABP-B-33).
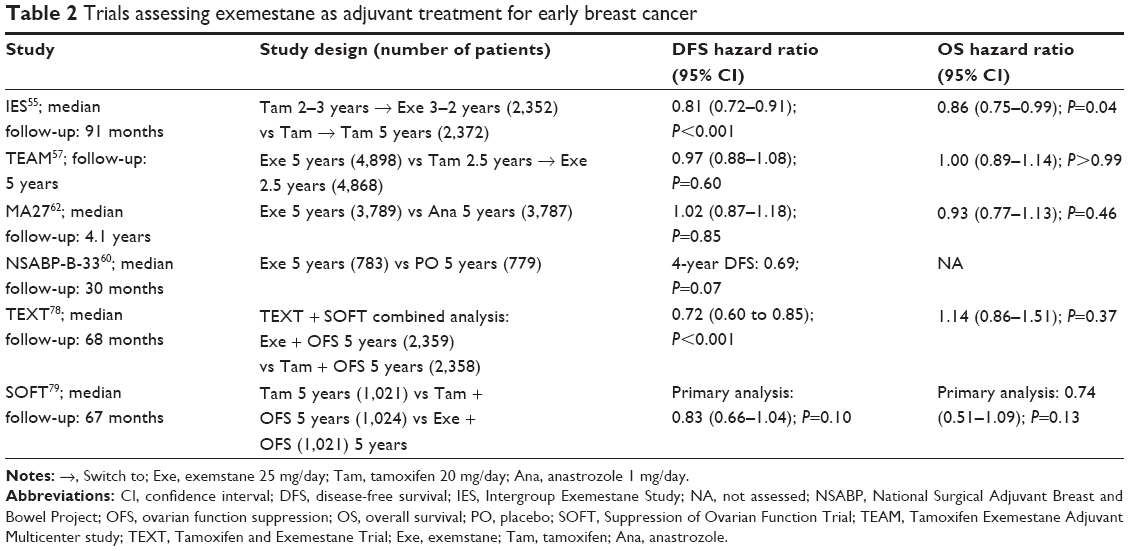 | Table 2 Trials assessing exemestane as adjuvant treatment for early breast cancer |
In the IES study, 4,724 postmenopausal hormone-receptor-positive/unknown early breast cancer patients, who had remained disease free after 2–3 years of adjuvant tamoxifen, were randomized to early switch to exemestane (n=2,352) or to continue on tamoxifen (n=2,372) to complete 5 years of endocrine therapy. Disease-free survival (DFS) was the primary end point.
At a median follow-up of 91 months, a DFS advantage emerged in favor of exemestane (HR: 0.81; 95% CI: 0.72–0.91; P=0.001), which resulted in an absolute increase of 4.5% (95% CI: 1.9%–6.8%) in terms of the probability of being alive and disease free at 8 years. An improvement in OS was also demonstrated with the switch strategy, (HR: 0.86; 95% CI: 0.75–0.99; P=0.04), with an absolute survival gain of 2.4% at 8 years.61
The TEAM trial was designed initially as an open-label study comparing the efficacy of 5 years of tamoxifen versus exemestane in postmenopausal early breast cancer patients. However, following the publication of the IES results,67 its design was modified and the control arm was converted into an early-switch arm of 2.5–3 years of tamoxifen followed by exemestane for a total of 5 years.
At a median follow-up of 5.1 years, no DFS (HR: 0.97; 95% CI: 0.88–1.08; P=0.60) or OS (HR: 1.00; 95% CI: 0·89–1.14; P>0.99) differences between the two arms of the study were observed.63 These results were consistent with those obtained from similar comparisons, but using the NSAI letrozole, in the Breast International Group (BIG) 1-98.62
The only fully published study that compared 5 years with exemestane with 5 years of an NSAI in the adjuvant setting is the National Cancer Institute of Cancer Clinical Trials Group (NCIC CTG) MA.27.68 In this multicenter open-label trial, 7,576 postmenopausal women with ER-positive early breast cancer were randomized to either anastrozole or exemestane.68 At a median follow-up of 4.1 years, there was no difference in the primary end point event-free survival, being 91% for exemestane and 91.2% for anastrozole (stratified HR: 1.02; 95% CI: 0.87–1.18; P=0.85). The secondary end points distant DFS (4.1% vs 4.3%, respectively; HR: 0.95; 95% CI: 0.76–1.18; P=0.64) and disease-specific survival (2.4% vs 2.6%, respectively; HR: 0.93; 95% CI: 0.70–1.24; P=0.62) were also similar.
Adjuvant setting: extended therapy in postmenopausal women
Women with hormone-receptor-positive operable breast cancer remain at risk of relapse for many years beyond the completion of adjuvant therapy.69
Considering this long-term risk of recurrence, a number of trials have been conducted in both pre- and postmenopausal women addressing whether extending adjuvant endocrine therapy beyond the conventional 5 years of duration would reduce the risk of late recurrence. Despite initial negative results,70–72 two large clinical trials have recently confirmed consistent benefits of continuing tamoxifen beyond 5 years.73,74 Well before the publication of positive results for extended therapy with tamoxifen, one pivotal study, the NCIC-CTG MA.17/BIG 1–97 trial, confirmed the effectiveness of 5 years of letrozole versus placebo in postmenopausal women who completed 4–6 years of adjuvant tamoxifen.64 At a median follow-up of 2.4 years, letrozole yielded a highly significant reduction in the risk of recurrence compared to placebo (DFS HR: 0.57; P=0.00008). Additionally, letrozole significantly reduced the risk of distant metastases in patients with both node-negative and node-positive disease (P=0.002) and significantly improved the OS by 39% in patients with involved axillary lymph nodes (HR: 0.61; P=0.04).75 These results, which were subject to early disclosure due to their potential clinical relevance, had an impact on other similar initiatives that were being conducted by other groups. One of these was the NSABP-B-33 trial, which was investigating extended adjuvant therapy with exemestane in postmenopausal women with clinical T1–3N1M0 breast cancer and who were disease free after 5 years of adjuvant tamoxifen.66 The trial was prematurely closed after the publication of the NCIC-CTG MA.17/BIG 1–97 trial’s positive results, to allow patients in the placebo arm to receive exemestane. At the time of unblinding, 1,598 patients had been randomly assigned; 72% of those in the exemestane group continued on exemestane, and 44% of those in the placebo group crossed over to exemestane. Despite this, with a median follow-up of 30 months, intent-to-treat analysis resulted in a borderline statistically significant improvement in 4-year DFS (91% vs 89%; relative risk =0.68; P=0.07) and in a statistically significant improvement in 4-year relapse-free survival (96% vs 94%; relative risk =0.44; P=0.004).
As for the NSABP-B-33, the smaller Adjuvant post-Tamoxifen Exemestane versus Nothing Applied (ATENA) trial, which was designed to compare exemestane with observation after 5 years of previous tamoxifen, was prematurely closed after recruiting only 448 patients, giving no results regarding the primary end point DFS.76
A subsequent Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) meta-analysis confirmed extended adjuvant AI treatment to be associated with an absolute 2.9% decrease in breast cancer recurrence (relative decrease, 43%; P<0.00001) and an absolute 0.5% decrease in breast cancer mortality (relative decrease, 27%; P=0.11) after a median follow-up of 2.5 years, with the magnitude of these effects probably underestimated because of crossover after unblinding.77
Adjuvant setting: premenopausal women
For decades, tamoxifen has been the gold standard for the adjuvant treatment of hormone-receptor-positive breast cancer in premenopausal women.78
Due to their mechanism of action, AIs can be used safely in premenopausal women only when ovarian function is concomitantly suppressed. The results of AI activity in postmenopausal early breast cancer patients,55,56 as well as in premenopausal women in the metastatic setting,79–81 provided the background for studying the combination of AIs and ovarian function suppression (OFS) as adjuvant therapy in premenopausal patients.
The Austrian Breast and Colorectal Cancer Study Group trial 12 (ABCSG-12) study randomized 1,803 premenopausal women with hormone-receptor-positive breast cancer to OFS (with the GnRH analog goserelin) in combination with anastrozole versus the same OFS in combination with tamoxifen for 3 years. After a median follow-up of 47.8 months, no difference in the primary end point DFS was seen between anastrozole and tamoxifen.82 Surprisingly, a worse OS has been shown with anastrozole (46 vs 27 deaths; HR: 1.75; 95% CI: 1.08–2.83; P=0.02). Of note, only 18% of randomized women were ≤40 years of age.83
Two large randomized trials coordinated by the Internation Breast Cancer Study Group were designed to address whether adjuvant therapy with exemestane improved DFS as compared with tamoxifen, among premenopausal women treated plus subject to OFS and to determine the value of OFS in suitable women candidates for treatment with adjuvant tamoxifen.
The Tamoxifen and Exemestane Trial (TEXT) was designed to evaluate 5 years of exemestane plus the GnRH analog triptorelin versus tamoxifen plus triptorelin in women who received OFS from the start of adjuvant therapy.
The Suppression of Ovarian Function Trial (SOFT) was designed to evaluate 5 years of exemestane plus OFS (triptorelin, bilateral oophorectomy, or ovarian irradiation), versus tamoxifen plus OFS, versus tamoxifen alone in women who remained premenopausal after the completion of adjuvant or neoadjuvant chemotherapy or in women for whom adjuvant tamoxifen alone was suitable treatment.
The two trials were conducted over the same time frame and in similar patient populations of premenopausal women with hormone-receptor-positive early breast cancer with an average age of 43 years. Although the original plan was to analyze each trial separately as well as jointly, a further amendment was introduced to allow a combined analysis of data regarding the comparison of exemestane and tamoxifen in the context of OFS and release the data separately.84 In the 4,690 patients involved in this comparison, 5-year DFS was 91.1% in the exemestane plus OFS group versus 87.3% in the tamoxifen plus OFS group (HR for disease recurrence, second invasive cancer, or death: 0.72; 95% CI: 0.60–0.85; P<0.001). Compared to patients receiving tamoxifen, those receiving exemestane had a 34% relative reduction in the risk of breast cancer recurrence and a 22% relative reduction in the risk of distant recurrence.
The 5-year OS rates were high in both groups: 95.9% in the exemestane plus OFS group and 96.9% in the tamoxifen plus OFS group (HR for death in the exemestane–OFS group: 1.14; 95% CI: 0.86–1.51; P=0.37) and longer follow-up is needed to accurately assess the impact of the two treatments on long-term survival.
Later the same year, the results of the SOFT study were published.85 The SOFT study enrolled 3,066 premenopausal early ER-positive breast cancer patients and randomized them to receive tamoxifen alone for 5 years or tamoxifen + OFS or exemestane + OFS. Women randomly assigned to OFS in either arm had the choice of monthly injections of triptorelin, bilateral oophorectomy, or radiation. After a protocol amendment in 2011, the comparison of tamoxifen plus OFS over tamoxifen alone became the primary analysis of the trial and the comparison of exemestane plus OFS with tamoxifen alone became a secondary objective. As previously mentioned, the comparison of exemestane plus OFS with tamoxifen plus OFS was analyzed by a combined analysis with the TEXT data.
Treatments were compared in two prespecified groups of women: those who needed chemotherapy (younger age, higher-risk tumors, larger tumors, and more likely to be node positive) and those who were eligible to adjuvant endocrine therapy alone. Women who had chemotherapy entered the trial 8 months postchemotherapy, a time interval needed to confirm premenopausal levels of estradiol, while those who did not receive chemotherapy entered the trial soon after surgery. At a median follow-up of 5.6 years, the addition of OFS to tamoxifen compared to tamoxifen alone did not result in better DFS, which was the primary study end point. Indeed, the 5-year DFS rate was 86.6% vs 84.7% for tamoxifen + OFS versus tamoxifen alone, respectively (HR for recurrence, second invasive cancer, or death: 0.83; 95% CI: 0.66–1.04; P=0.10).
However, some patient subgroups derived a significant and clinically meaningful benefit from OFS. The largest effect was seen in the 350 women who were ≤35 years, representing 11.5% of the enrolled women, nearly all of whom (94%) had received adjuvant chemotherapy. In this group, the 5-year breast-cancer-free rate was 67.7% with tamoxifen alone, 78.9% with the combination tamoxifen + OFS, and 83.4% in those on exemestane + OFS.
Another significant advantage was seen in a subgroup of 1,084 women (median age: 40 years) who remained premenopausal (documented by estradiol blood levels) after chemotherapy.
In this group, the 5-year breast-cancer-free rate was 78.0% with tamoxifen alone compared to 82.5% with tamoxifen + OFS and 85.7% with exemestane + OFS. This translated into a 22% reduction in relative risk of recurrence for tamoxifen + OFS versus tamoxifen alone and into a 35% relative risk reduction for exemestane + OFS versus tamoxifen alone, leading to an absolute improvement of 4.5% and 7.7% at 5 years, respectively.
In contrast, no benefit from adding OFS to endocrine therapy was observed in the subgroup of 949 women who did not receive chemotherapy. These women had a median age of 46 years and experienced high event-free survival rates at 5 years (95.8% with tamoxifen alone, 95.1% with tamoxifen + OFS, and 97.1% with exemestane + OFS).
In terms of tolerability, adding OFS to endocrine therapy increased adverse effects, most notably menopausal symptoms (hot flushes and sweats), decreased libido, vaginal dryness, and depression. Further, exemestane + OFS combination was associated with more adverse events than tamoxifen + OFS, including musculoskeletal and bone density effects.
Exemestane for breast cancer prevention
Chemoprevention of breast cancer is an effective strategy to reduce the incidence of this disease in women at risk. The first agents to show a significant chemopreventive effect were the SERMs tamoxifen and raloxifen. An updated comprehensive analysis of all SERM prevention trials showed that they are able to reduce the incidence of breast cancer in high- and average-risk women, an effect that is sustained by a reduction in ER-positive invasive breast cancer.86
The role of AIs for breast cancer prevention was hypothesized based on the results form early adjuvant trials showing that NSAIs and SAIs were more effective than tamoxifen in reducing the incidence of contralateral primary breast cancer.87 Thus, two major clinical trials have assessed the preventive role of NSAIs88 and SAIs89 in women at high risk for developing breast cancer.
The NCIC Mammary Prevention 3 (MAP.3) Trial was a randomized, placebo-controlled, double-blind trial of exemestane administered to postmenopausal women who had an increased risk for breast cancer.89 A total of 4,560 women (median age: 62.5 years; median Gail risk score: 2.3%) were randomly assigned to either exemestane or placebo. At a median follow-up of 35 months, eleven invasive breast cancers were detected in those assigned to exemestane and in 32 of those assigned to placebo, with a 65% relative reduction in the annual incidence of invasive breast cancer (0.19% vs 0.55%; HR: 0.35; 95% CI: 0.18–0.70; P=0.002). The annual incidence of invasive plus noninvasive (ductal carcinoma in situ) breast cancer was 0.35% for exemestane and 0.77% for placebo (HR: 0.47; 95% CI: 0.27–0.79; P=0.004). Adverse events occurred in 88% of the exemestane group and 85% of the placebo group (P=0.003), with no significant differences between the two groups in terms of skeletal fractures, cardiovascular events, other cancers, or treatment-related deaths.
Similar results were recently reported for anastrozole, assessed in the IBIS II trial. This international, double-blind, placebo-controlled trial randomized 3,864 postmenopausal women at high risk of breast cancer to receive the NSAI anastrozole or placebo daily for 5 years. After a median follow-up of 5 years, 40 (2%) of 1,920 women in the anastrozole group and 85 (4%) of 1,944 in the placebo group had developed breast cancer (HR: 0·47; 95% CI: 0.32–0.68, P<0.0001). No differences in breast cancer and all-cause mortality were detected within the two groups.88
Safety and tolerability
Bone health
AIs decrease circulating estrogen concentrations in postmenopausal women, resulting in accelerated bone loss, decreased bone mineral density (BMD), and increased risk of bone fractures.32,90,91
Data from large Phase III adjuvant trials indicate an increased risk of bone fractures with exemestane, as well as anstrozole and letrozole, compared to tamoxifen.55,67,92,93
However, due to the agonistic effects on bone metabolism induced by tamoxifen,94 caution is required when interpreting these data as differences in fracture rate may not be due to a detrimental effect of AIs alone.
Indeed, when compared with placebo, the effects of exemestane,95 letrozole,96 and anastrozole88 reveal that the loss in BMD is moderate and not as dramatic as suggested in the studies where the comparator is tamoxifen.
Notably, AIs’ negative effect on bone metabolism seems to reverse and disappear upon termination of therapy.55,97
The most comprehensive data on long-term safety of exemestane come from the adjuvant trials. In the IES trial, with a median follow-up of 58 months, fractures were reported for 162 (7%) and 115 (5%) patients in the exemestane and tamoxifen groups, respectively (P=0.003).98 In the bone substudy of this trial, within 6 months of switching to exemestane, BMD decreased by 2.7% (95% CI: 2.0–3.4; P<0.0001) at the lumbar spine and 1.4% (95% CI: 0.8–1.9; P<0.0001) at the hip compared with baseline, but the BMD became only 1.0% (95% CI: 0.4–1.7; P=0.002) and 0.8% (95% CI: 0.3–1.4; P=0.003) in Year 2 at the lumbar spine and hip, respectively.
Notably, no patient with normal BMD at trial entry developed osteoporosis. Bone resorption and formation markers increased at all time points in women receiving exemestane (P<0.001).99 Similarly, in a German bone substudy of TEAM, patients receiving exemestane registered a decrease in BMD at the spine and total hip after 6 months, with the rate of bone loss stabilizing from months 6 to 12.100
In the NSABP-B-33 study, 28 fractures were observed in the exemestane group and 20 in the placebo group (3.5% vs 2.6%; not significant) up to the time of unblinding.66
Similarly, in the MAP.3 prevention trial, no differences in clinical fracture rates were described between exemestane and placebo, and the proportion of women in each group who were prescribed bisphosphonate therapy during the trial was also similar (24.5% for exemestane and 24.1% for placebo).89
Compared to NSAIs, animal studies suggested that the partial androgenic activity of exemestane may be responsible of a minor bone loss compared with the nonsteroidal AIs.101
The NCIC CTG MA.27 bone substudy (MA27B) was designed to confirm this hypothesis. The trial was a substudy of the larger MA27 study and investigated the effects of adjuvant exemestane versus anastrozole given daily for 5 years on the BMD of postmenopausal women with early breast cancer. Approximately 500 women eligible for MA.27 were randomly assigned to exemestane or anastrozole based on baseline T-scores: the first group contained women with both hip and lumbar spine T-scores of −2.0 or more, and the second contained women with at least one T-score of less than −2.0. All participants were prescribed calcium and vitamin D supplementation and women with baseline T-scores less than −2.0 were on oral bisphosphonates as well.
Investigators found both AIs to have a similar effect on hip and spine BMD at 2 years for patients with both T-scores of −2.0 or greater (hip P=0.10; spine P=0.08) and those with T-scores of less than −2.0 (spine P=0.26 and hip P=0.28). No differences in bone turnover biomarkers between the two AIs were reported.102
Thus, MA.27B showed safety for both adjuvant SAIs and NSAIs in women with osteopenia or osteoporosis, provided they were concomitantly prescribed bisphosphonates, calcium, and vitamin D.
Muscoloskeletal events
Joint pain and stiffness, including carpal tunnel syndrome, is a frequent type of toxiciy related to AIs complained by nearly half of patients in the clinical setting.103
In the IES study, musculoskeletal pain (21% vs 16.1%, P<0.0001), carpal tunnel syndrome (2.8% vs 0.3%, P<0.0001), joint stiffness (1.9% vs 1%, P<0.009), paraesthesia (2.8% vs 1%, P<0.0001), and arthralgia (18.6% vs 11.8%, P<0.0001) were reported more frequently in patients who switched to exemestane than in those who remained on tamoxifen, respectively, and the same results were reported by the TEAM trialists, where exemestane monotherapy was associated with a significantly higher incidence of musculoskeletal adverse events in general (2,448 [50%] vs 2,133 [44%]).63
Lipid metabolism and cardiovascular events
The low levels of circulating estrogens caused by AIs have been implicated in increased low-density lipoprotein (LDL) cholesterol and decreased high-density cholesterol levels, and these changes are considered to increase the risk of cardiovascular disease.
Most studies, however, did not show marked changes in lipid parameters induced by letrozole or anastrozole,104 and exemestane showed no effect on levels of total cholesterol or its fractions, nor on lipoprotein levels.105
A substudy of the TEAM compared the effect of exemestane on lipid metabolism to that of tamoxifen76; the study confirmed the already well-known beneficial effects of tamoxifen on cholesterol and LDL serum levels and showed a neutral effect on the lipidemic profile for exemestane.
The absence of major metabolic effects for exemestane was also observed in a small, randomized study designed to evaluate the effects of 2 years of adjuvant exemestane versus placebo on bone and lipid metabolism in early breast cancer postmenopausal patients.95
Cardiovascular toxicity has been suggested to be more frequently associated with AIs than with tamoxifen.55,56 Once again, however, studies comparing AIs with placebo do not convincingly confirm this potential side effect.
In the IES study, no statistically significant differences were reported between exemestane and tamoxifen in terms of the incidence of cardiovascular events reported either during treatment or including the posttreatment period: the number of patients with myocardial infarction was low in both the exemestane and tamoxifen groups (0.6% vs 0.2%, P=0.06) and the incidence of ischemic heart disease was also not significantly different (8.0% vs 6.9%, P=0.17). On the other hand, a statistically significant increase in thromboembolic events among patients continuing with tamoxifen was described (2.3% vs 1.2%, P=0.004).98
No differences in cardiovascular events were reported in the MAP.3 prevention trial (exemestane vs placebo: 4.7% vs 4.9% respectively, P=0.78)89 and in the MA.27 study, where myocardial infarction, stroke, and transient ischemic attacks were not significantly different between exemestane and anastrozole.68
Finally, these observations do not suggest that AIs in general, and exemestane in particular, are associated with an increased risk of cardiovascular mortality.
Gynecological and menopausal symptoms
Because AIs block peripheral estrogen production, they are usually associated with an increased incidence of vaginal dryness and consequent sexual dysfunction. At this level, their side effect profile differs from that of tamoxifen which, by virtue of tissue-specific partial agonist action, is associated with frequent vaginal discharge and endometrial abnormalities.
In the direct comparisons between tamoxifen and exemestane in the TEAM and IES adjuvant studies, gynecological symptoms (overall incidence) were reported more frequently in the tamoxifen-containing arms, whereas vaginal dryness was more frequent in the exemestane arm of the TEAM study (P=0.038).63,98
A TEAM substudy specifically compared menopausal symptoms during the first year of adjuvant exemestane or tamoxifen. As expected, patients receiving exemestane reported more frequent vaginal dryness (P=0.0004), whereas tamoxifen was associated with more frequent vaginal discharge (P<0.0001).106
An IES quality-of-life (QOL) substudy reported, at a 7.5-year follow-up after start of endocrine treatment, a significantly higher vaginal discharge rate associated with tamoxifen (P<0.01) during treatment, with no more differences detectable after study treatment completion. No differences were observed between treatment groups concerning vaginal dryness.107
As expected, the MAP3 prevention trial reported more frequent menopausal symptoms and worsening menopause-related vasomotor and sexual symptoms in patients taking exemestane, compared to patients on placebo, although no detrimental effect on health-related QOL was observed.89
Effects on cognitive functioning
At present, limited data from the main multicentric adjuvant studies are available on the effects of AIs on cognitive functioning.108,109
Regarding exemestane, a neuropsychological cross-sectional study from the TEAM trial was conducted to evaluate the cognitive functioning during the first year of treatment.110 After the first year of adjuvant endocrine therapy, exemestane was not significantly associated with worsening in cognitive functioning compared to healthy controls. In contrast, patients on tamoxifen performed worse than healthy controls on verbal memory (P<0.01) and executive functioning (P=0.01).
Conclusion
Exemestane is a third-generation irreversible steroidal inactivator of the aromatase enzyme and is effective in all the treatment settings for breast cancer, including chemoprevention.
In the metastatic setting, exemestane has been extensively investigated as the first-line, second-line, and further-line treatment and is now registered for the treatment of postmenopausal women with advanced hormone-receptor-positive breast cancer whose disease has progressed following antiestrogen therapy. Of note, the potential lack of cross-resistance with NSAIs yields additional opportunities in the treatment sequence of endocrine agents. Furthermore, based on clinically meaningful results, exemestane with everolimus represents an effective therapeutic option for a disease that has progressed after exposure to NSAIs.
As fas as adjuvant therapy is concerned, several options are feasible, including up-front monotherapy for 5 years, a switch following 2–3 years of tamoxifen, or extended therapy with exemestane beyond 5 years of adjuvant treatment. New promising data also showed a beneficial effect in young premenopausal early breast cancer patients, when administered together with OFS.
Exemestane is generally well tolerated, with a side effect profile similar to that of other AIs and including menopausal symptoms, arthralgia, bone loss, and altered lipid metabolism.
Furthermore, compared with tamoxifen, exemestane causes fewer thromboembolic and gynecological events.
In conclusion, exemestane represents an effective and well-tolerated hormonal therapeutic option for the treatment of both early and advanced hormone-receptor-positive breast cancer, independently from menopausal status.
Disclosure
FM has served as a member of the Speaker’s Bureau for Astra Zeneca and for Hoffmann La Roche. Supported by Fondazione Piemontese per la Ricerca sul Cancro, 5× mille 2012. The authors report no other conflicts of interest in this work.
References
DeSantis C, Ma J, Bryan L, Jemal A. Breast cancer statistics, 2013. CA Cancer J Clin. 2014;64(1):52–62. | ||
Malvezzi M, Bertuccio P, Rosso T, et al. European cancer mortality predictions for the year 2015: does lung cancer have the highest death rate in EU women? Ann Oncol. 2015;26(4):779–786. | ||
Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer. 2013;49(6):1374–1403. | ||
Beatson G. On the treatment of inoperable cases of carcinoma of the mamma: suggestions for a new method of treatment with illustrative cases. Lancet. 1869;2:104–107. | ||
Geisler J, Lonning PE. Aromatase inhibition: translation into a successful therapeutic approach. Clin Cancer Res. 2005;11(8):2809–2821. | ||
Santen RJ, Worgul TJ, Lipton A, et al. Aminoglutethimide as treatment of postmenopausal women with advanced breast carcinoma. Ann Intern Med. 1982;96(1):94–101. | ||
Santen RJ, Manni A, Harvey H, Redmond C. Endocrine treatment of breast cancer in women. Endocr Rev. 1990;11(2):221–265. | ||
Buzdar AU, Smith R, Vogel C, et al. Fadrozole HCL (CGS-16949A) versus megestrol acetate treatment of postmenopausal patients with metastatic breast carcinoma: results of two randomized double blind controlled multiinstitutional trials. Cancer. 1996;77:2503–2513. | ||
Thürlimann B, Castiglione M, Hsu-Schmitz SF, et al. Formestane versus megestrol acetate in postmenopausal breast cancer patients after failure of tamoxifen: a phase III prospective randomised cross over trial of second-line hormonal treatment (SAKK 20/90). Swiss Group for Clinical Cancer Research (SAKK). Eur J Cancer. 1997;33:1017–1024. | ||
Thürlimann B, Beretta K, Bacchi M, et al. First-line fadrozole HCI (CGS 16949A) versus tamoxifen in postmenopausal women with advanced breast cancer. Prospective randomised trial of the Swiss Group for Clinical Cancer Research SAKK 20/88. Ann Oncol. 1996;7(5):471–479. | ||
Falkson CI, Falkson HC. A randomised study of CGS 16949A (fadrozole) versus tamoxifen in previously untreated postmenopausal patients with metastatic breast cancer. Ann Oncol. 1996;7(5):465–469. | ||
Pérez Carrión R, Alberola Candel V, Calabresi F, et al. Comparison of the selective aromatase inhibitor formestane with tamoxifen as first-line hormonal therapy in postmenopausal women with advanced breast cancer. Ann Oncol. 1994;5(Suppl 7):S19–S24. | ||
Lombardi P. Exemestane, a new steroidal aromatase inhibitor of clinical relevance. Biochim Biophys Acta. 2002;1587(2–3):326–337. | ||
Smith IE, Dowsett M. Aromatase inhibitors in breast cancer. N Engl J Med. 2003;348(24):2431–2442. | ||
Lombardi P. The irreversible inhibition of aromatase (oestrogen synthetase) by steroidal compounds. Curr Pharm Des. 1995;1:23–50. | ||
Brodie AM. Aromatase, its inhibitors and their use in breast cancer treatment. Pharmacol Ther. 1993;60(3):501–515. | ||
Hong Y, Yu B, Sherman M, Yuan YC, Zhou D, Chen S. Molecular basis for the aromatization reaction and exemestane-mediated irreversible inhibition of human aromatase. Mol Endocrinol. 2007;21(2):401–414. | ||
Giudici D, Ornati G, Briatico G, Buzzetti F, Lombardi P, di Salle E. 6-Methylenandrosta-1,4-diene-3,17-dione (FCE 24304): a new irreversible aromatase inhibitor. J Steroid Biochem. 1988;30(1–6):391–394. | ||
di Salle E, Giudici D, Briatico G, Ornati G. Novel irreversible aromatase inhibitors. Ann N Y Acad Sci. 1990;595:357–367. | ||
Zaccheo T, Di Salle E. Effect of the irreversible aromatase inhibitor FCE 24304 on DMBA-induced mammary tumors in ovariectomized rats treated with testosterone. Cancer Chemother Pharmacol. 1989;25(2):95–98. | ||
di Salle E, Briatico G, Giudici D, Ornati G, Zaccheo T. Aromatase inhibition and experimental antitumor activity of FCE 24304, MDL 18962 and SH 489. J Steroid Biochem. 1989;34(1–6):431–434. | ||
Zaccheo T, Giudici D, Ornati G, Panzeri A, di Salle E. Comparison of the effects of the irreversible aromatase inhibitor exemestane with atamestane and MDL 18962 in rats with DMBA-induced mammary tumours. Eur J Cancer. 1991;27(9):1145–1150. | ||
Evans TR, Di Salle E, Ornati G, et al. Phase I and endocrine study of exemestane (FCE 24304), a new aromatase inhibitor, in postmenopausal women. Cancer Res. 1992;52(21):5933–5939. | ||
Lonning PE, Paridaens R, Thurlimann B, Piscitelli G, di Salle E. Exemestane experience in breast cancer treatment. J Steroid Biochem Mol Biol. 1997;61(3–6):151–155. | ||
Jannuzzo MG, Poggesi I, Spinelli R, Rocchetti M, Cicioni P, Buchan P. The effects of degree of hepatic or renal impairment on the pharmacokinetics of exemestane in postmenopausal women. Cancer Chemother Pharmacol. 2004;53(6):475–481. | ||
Zilembo N, Noberasco C, Bajetta E, et al. Endocrinological and clinical evaluation of exemestane, a new steroidal aromatase inhibitor. Br J Cancer. 1995;72(4):1007–1012. | ||
Paridaens R, Thomas J, Wildiers J, et al. Safety, activity and estrogen inhibition by exemestane in postmenopausal women with advanced breast cancer: a phase I study. Anticancer Drugs. 1998;9(8):675–683. | ||
Johannessen DC, Engan T, Di Salle E, et al. Endocrine and clinical effects of exemestane (PNU 155971), a novel steroidal aromatase inhibitor, in postmenopausal breast cancer patients: a phase I study. Clin Cancer Res. 1997;3(7):1101–1108. | ||
Scott LJ, Wiseman LR. Exemestane. Drugs. 1999;58(4):675–680. discussion 681–672. | ||
Lonning PE, Eikesdal HP. Aromatase inhibition 2013: clinical state of the art and questions that remain to be solved. Endocr Relat Cancer. 2013;20(4):R183–R201. | ||
Lonning PE, Geisler J. Evaluation of plasma and tissue estrogen suppression with third-generation aromatase inhibitors: of relevance to clinical understanding? J Steroid Biochem Mol Biol. 2010;118(4–5):288–293. | ||
Geisler J, Haynes B, Anker G, Dowsett M, Lonning PE. Influence of letrozole and anastrozole on total body aromatization and plasma estrogen levels in postmenopausal breast cancer patients evaluated in a randomized, cross-over study. J Clin Oncol. 2002;20(3):751–757. | ||
Campos SM, Guastalla JP, Subar M, Abreu P, Winer EP, Cameron DA. A comparative study of exemestane versus anastrozole in patients with postmenopausal breast cancer with visceral metastases. Clin Breast Cancer. 2009;9(1):39–44. | ||
Llombart-Cussac A, Ruiz A, Antón A, et al. Exemestane versus anastrozole as front-line endocrine therapy in postmenopausal patients with hormone receptor-positive, advanced breast cancer: final results from the Spanish Breast Cancer Group 2001–03 phase 2 randomized trial. Cancer. 2012;118(1):241–247. | ||
Riemsma R, Forbes CA, Kessels A, et al. Systematic review of aromatase inhibitors in the first-line treatment for hormone sensitive advanced or metastatic breast cancer. Breast Cancer Res Treat. 2010;123(1):9–24. | ||
Buzdar AU, Jonat W, Howell A, et al. Anastrozole versus megestrol acetate in the treatment of postmenopausal women with advanced breast carcinoma: results of a survival update based on a combined analysis of data from two mature phase III trials. Arimidex Study Group. Cancer. 1998;83(6):1142–1152. | ||
Dombernowsky P, Smith I, Falkson G, et al. Letrozole, a new oral aromatase inhibitor for advanced breast cancer: double-blind randomized trial showing a dose effect and improved efficacy and tolerability compared with megestrol acetate. J Clin Oncol. 1998;16(2):453–461. | ||
Kaufmann M, Bajetta E, Dirix LY, et al. Exemestane is superior to megestrol acetate after tamoxifen failure in postmenopausal women with advanced breast cancer: results of a phase III randomized double-blind trial. The Exemestane Study Group. J Clin Oncol. 2000;18(7):1399–1411. | ||
Bonneterre J, Buzdar A, Nabholtz JM, et al; Arimidex Writing Committee; Investigators Committee Members. Anastrozole is superior to tamoxifen as first-line therapy in hormone receptor positive advanced breast carcinoma. Cancer. 2001;92(9):2247–2258. | ||
Nabholtz JM, Buzdar A, Pollak M, et al. Anastrozole is superior to tamoxifen as first-line therapy for advanced breast cancer in postmenopausal women: results of a North American multicenter randomized trial. Arimidex Study Group. J Clin Oncol. 2000;18(22):3758–3767. | ||
Milla-Santos A, Milla L, Portella J, et al. Anastrozole versus tamoxifen as first-line therapy in postmenopausal patients with hormone-dependent advanced breast cancer: a prospective, randomized, phase III study. Am J Clin Oncol. 2003;26(3):317–322. | ||
Mouridsen H, Gershanovich M, Sun Y, et al. Phase III study of letrozole versus tamoxifen as first-line therapy of advanced breast cancer in postmenopausal women: analysis of survival and update of efficacy from the International Letrozole Breast Cancer Group. J Clin Oncol. 2003;21(11):2101–2109. | ||
Paridaens RJ, Dirix LY, Beex LV, et al. Phase III study comparing exemestane with tamoxifen as first-line hormonal treatment of metastatic breast cancer in postmenopausal women: the European Organisation for Research and Treatment of Cancer Breast Cancer Cooperative Group. J Clin Oncol. 2008;26(30):4883–4890. | ||
Jones S, Vogel C, Arkhipov A, et al. Multicenter, phase II trial of exemestane as third-line hormonal therapy of postmenopausal women with metastatic breast cancer. Aromasin Study Group. J Clin Oncol. 1999;17(11):3418–3425. | ||
Lønning PE, Bajetta E, Murray R, et al. Activity of exemestane in metastatic breast cancer after failure of nonsteroidal aromatase inhibitors: a phase II trial. J Clin Oncol. 2000;18(11):2234–2244. | ||
Iaffaioli RV, Formato R, Tortoriello A, et al; Southern Italy Oncology Group. Phase II study of sequential hormonal therapy with anastrozole/exemestane in advanced and metastatic breast cancer. Br J Cancer. 2005;92(9):1621–1625. | ||
Bertelli G, Garrone O, Merlano M, et al. Sequential treatment with exemestane and non-steroidal aromatase inhibitors in advanced breast cancer. Oncology. 2005;69(6):471–477. | ||
Steele N, Zekri J, Coleman R, et al. Exemestane in metastatic breast cancer: effective therapy after third-generation non-steroidal aromatase inhibitor failure. Breast. 2006;15(3):430–436. | ||
Chin YS, Beresford MJ, Ravichandran D, Makris A. Exemestane after non-steroidal aromatase inhibitors for post-menopausal women with advanced breast cancer. Breast. 2007;16(4):436–439. | ||
Mayordomo J, Llombart A, Martin M, et al. Randomized multicenter crossover phase II trial to compare exemestane (E) vs. anastrozole (A) in postmenopausal patients (pt) withadvanced breast cancer (ABC) and positive hormone receptors (HR). Final efficacy analysis of GEICAM 2001–03 study. J Clin Oncol. 2006;24(Suppl):638. | ||
Carlini P, Michelotti A, Ferretti G, et al. Clinical evaluation of the use of exemestane as further hormonal therapy after nonsteroidal aromatase inhibitors in postmenopausal metastatic breast cancer patients. Cancer Invest. 2007;25(2):102–105. | ||
Chia S, Gradishar W, Mauriac L, et al. Double-blind, randomized placebo controlled trial of fulvestrant compared with exemestane after prior nonsteroidal aromatase inhibitor therapy in postmenopausal women with hormone receptor-positive, advanced breast cancer: results from EFECT. J Clin Oncol. 2008;26(10):1664–1670. | ||
Johnston SR, Kilburn LS, Ellis P, et al; SoFEA Investigators. Fulvestrant plus anastrozole or placebo versus exemestane alone after progression on non-steroidal aromatase inhibitors in postmenopausal patients with hormone-receptor-positive locally advanced or metastatic breast cancer (SoFEA): a composite, multicentre, phase 3 randomised trial. Lancet Oncol. 2013;14(10):989–998. | ||
Baselga J, Campone M, Piccart M, et al. Everolimus in postmenopausal hormone-receptor-positive advanced breast cancer. N Engl J Med. 2012;366(6):520–529. | ||
Forbes JF, Cuzick J, Buzdar A, Howell A, Tobias JS, Baum M. Effect of anastrozole and tamoxifen as adjuvant treatment for early-stage breast cancer: 100-month analysis of the ATAC trial. Lancet Oncol. 2008;9(1):45–53. | ||
Coates AS, Keshaviah A, Thürlimann B, et al. Five years of letrozole compared with tamoxifen as initial adjuvant therapy for postmenopausal women with endocrine-responsive early breast cancer: update of study BIG 1-98. J Clin Oncol. 2007;25(5):486–492. | ||
Jones SE, Seynaeve C, Hasenburg A, et al. Results of the first planned analysis of the TEAM (tamoxifen exemestane adjuvant multinational) prospective randomized phase III trial in hormone sensitive postmenopausal early breast cancer. Cancer Res. 2009;69:67s. [abstract 15]. | ||
Kaufmann M, Jonat W, Hilfrich J, et al. Improved overall survival in postmenopausal women with early breast cancer after anastrozole initiated after treatment with tamoxifen compared with continued tamoxifen: the ARNO 95 Study. J Clin Oncol. 2007;25(19):2664–2670. | ||
Dubsky PC, Jakesz R, Mlineritsch B, et al. Tamoxifen and anastrozole as a sequencing strategy: a randomized controlled trial in postmenopausal patients with endocrine-responsive early breast cancer from the Austrian Breast and Colorectal Cancer Study Group. J Clin Oncol. 2012;30(7):722–728. | ||
Boccardo F, Guglielmini P, Bordonaro R, et al. Switching to anastrozole versus continued tamoxifen treatment of early breast cancer: long term results of the Italian Tamoxifen Anastrozole trial. Eur J Cancer. 2013;49(7):1546–1554. | ||
Bliss JM, Kilburn LS, Coleman RE, et al. Disease-related outcomes with long-term follow-up: an updated analysis of the intergroup exemestane study. J Clin Oncol. 2012;30(7):709–717. | ||
Regan MM, Neven P, Giobbie-Hurder A, et al; BIG 1-98 Collaborative Group, International Breast Cancer Study Group (IBCSG). Assessment of letrozole and tamoxifen alone and in sequence for postmenopausal women with steroid hormone receptor-positive breast cancer: the BIG 1-98 randomised clinical trial at 8.1 years median follow-up. Lancet Oncol. 2011;12(12):1101–1108. | ||
van de Velde CJ, Rea D, Seynaeve C, et al. Adjuvant tamoxifen and exemestane in early breast cancer (TEAM): a randomised phase 3 trial. Lancet. 2011;377(9762):321–331. | ||
Goss PE, Ingle JN, Martino S, et al. A randomized trial of letrozole in postmenopausal women after five years of tamoxifen therapy for early-stage breast cancer. N Engl J Med. 2003;349(19):1793–1802. | ||
Jakesz R, Greil R, Gnant M, et al; Austrian Breast and Colorectal Cancer Study Group. Extended adjuvant therapy with anastrozole among postmenopausal breast cancer patients: results from the randomized Austrian Breast and Colorectal Cancer Study Group Trial 6a. J Natl Cancer Inst. 2007;99(24):1845–1853. | ||
Mamounas EP, Jeong JH, Wickerham DL, et al. Benefit from exemestane as extended adjuvant therapy after 5 years of adjuvant tamoxifen: intention-to-treat analysis of the National Surgical Adjuvant Breast and Bowel Project B-33 trial. J Clin Oncol. 2008;26(12):1965–1971. | ||
Coombes RC, Hall E, Gibson LJ, et al; Intergroup Exemestane Study. A randomized trial of exemestane after two to three years of tamoxifen therapy in postmenopausal women with primary breast cancer. N Engl J Med. 2004;350(11):1081–1092. | ||
Goss PE, Ingle JN, Pritchard KI, et al. Exemestane versus anastrozole in postmenopausal women with early breast cancer: NCIC CTG MA.27 – a randomized controlled phase III trial. J Clin Oncol. 2013;31(11):1398–1404. | ||
Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;365(9472):1687–1717. | ||
Fisher B, Dignam J, Bryant J, Wolmark N. Five versus more than five years of tamoxifen for lymph node-negative breast cancer: updated findings from the National Surgical Adjuvant Breast and Bowel Project B-14 randomized trial. J Natl Cancer Inst. 2001;93(9):684–690. | ||
Tormey DC, Gray R, Falkson HC. Postchemotherapy adjuvant tamoxifen therapy beyond five years in patients with lymph node-positive breast cancer. Eastern Cooperative Oncology Group. J Natl Cancer Inst. 1996;88(24):1828–1833. | ||
Stewart HJ, Prescott RJ, Forrest AP. Scottish adjuvant tamoxifen trial: a randomized study updated to 15 years. J Natl Cancer Inst. 2001;93(6):456–462. | ||
Davies C, Pan H, Godwin J, et al; Adjuvant Tamoxifen: Longer Against Shorter (ATLAS) Collaborative Group. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet. 2013;381(9869):805–816. | ||
Davies C, Pan H, Godwin J, et al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 in 6,953 women with early breast cancer. J Clin Oncol. 2013;381(9869):805–816. | ||
Goss PE, Ingle JN, Martino S, et al. Randomized trial of letrozole following tamoxifen as extended adjuvant therapy in receptor-positive breast cancer: updated findings from NCIC CTG MA.17. J Natl Cancer Inst. 2005;97(17):1262–1271. | ||
Markopoulos C, Dafni U, Misitzis J, et al. Extended adjuvant hormonal therapy with exemestane has no detrimental effect on the lipid profile of postmenopausal breast cancer patients: final results of the ATENA lipid substudy. Breast Cancer Res. 2009;11(3):R35. | ||
Goss P, Mamounas E, Jakesz R, et al. Aromatase Inhibitors (AIs) versus not (placebo/observation) as late extended adjuvant therapy for postmenopausal women with early stage breast cancer (BC): overviews of randomized trials of AIs after ~5 years of tamoxifen. Cancer Res. 2009;69(24 Suppl):abstr 4081. | ||
Goldhirsch A, Winer EP, Coates AS, et al; Panel Members. Personalizing the treatment of women with early breast cancer: highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann Oncol. 2013;24(9):2206–2223. | ||
Forward DP, Cheung KL, Jackson L, Robertson JF. Clinical and endocrine data for goserelin plus anastrozole as second-line endocrine therapy for premenopausal advanced breast cancer. Br J Cancer. 2004;90(3):590–594. | ||
Cheung KL, Agrawal A, Folkerd E, Dowsett M, Robertson JF, Winterbottom L. Suppression of ovarian function in combination with an aromatase inhibitor as treatment for advanced breast cancer in pre-menopausal women. Eur J Cancer. 2010;46(16):2936–2942. | ||
Carlson RW, Theriault R, Schurman CM, et al. Phase II trial of anastrozole plus goserelin in the treatment of hormone receptor-positive, metastatic carcinoma of the breast in premenopausal women. J Clin Oncol. 2010;28(25):3917–3921. | ||
Gnant M, Mlineritsch B, Schippinger W, et al; Austrian Breast and Colorectal Cancer Study Group, Vienna, Austria. Endocrine therapy plus zoledronic acid in premenopausal breast cancer. N Engl J Med. 2009;360(7):679–691. | ||
Gnant M, Mlineritsch B, Stoeger H, et al. Adjuvant endocrine therapy plus zoledronic acid in premenopausal women with early-stage breast cancer: 62-month follow-up from the ABCSG-12 randomised trial. Lancet Oncol. 2011;12(7):631–641. | ||
Pagani O, Regan MM, Walley BA, et al; TEXT and SOFT Investigators; International Breast Cancer Study Group. Adjuvant exemestane with ovarian suppression in premenopausal breast cancer. N Engl J Med. 2014;371(2):107–118. | ||
Francis PA, Regan MM, Fleming GF, et al; SOFT Investigators; International Breast Cancer Study Group. Adjuvant ovarian suppression in premenopausal breast cancer. N Engl J Med. 2015;372(5):436–446. | ||
Cuzick J, Sestak I, Bonanni B, et al; SERM Chemoprevention of Breast Cancer Overview Group. Selective oestrogen receptor modulators in prevention of breast cancer: an updated meta-analysis of individual participant data. Lancet. 2013;381(9880):1827–1834. | ||
Dowsett M, Cuzick J, Ingle J, et al. Meta-analysis of breast cancer outcomes in adjuvant trials of aromatase inhibitors versus tamoxifen. J Clin Oncol. 2010;28(3):509–518. | ||
Cuzick J, Sestak I, Forbes JF, et al; IBIS-II investigators. Anastrozole for prevention of breast cancer in high-risk postmenopausal women (IBIS-II): an international, double-blind, randomised placebo-controlled trial. Lancet. 2014;383(9922):1041–1048. | ||
Goss PE, Ingle JN, Alés-Martínez JE, et al; NCIC CTG MAP.3 Study Investigators. Exemestane for breast-cancer prevention in postmenopausal women. N Engl J Med. 2011;364(25):2381–2391. | ||
Geisler J, King N, Anker G, et al. In vivo inhibition of aromatization by exemestane, a novel irreversible aromatase inhibitor, in postmenopausal breast cancer patients. Clin Cancer Res. 1998;4(9):2089–2093. | ||
Chien AJ, Goss PE. Aromatase inhibitors and bone health in women with breast cancer. J Clin Oncol. 2006;24(33):5305–5312. | ||
Eastell R, Adams JE, Coleman RE, et al. Effect of anastrozole on bone mineral density: 5-year results from the anastrozole, tamoxifen, alone or in combination trial 18233230. J Clin Oncol. 2008;26(7):1051–1057. | ||
Breast International Group (BIG) 1-98 Collaborative Group; Thürlimann B, Keshaviah A, et al. A comparison of letrozole and tamoxifen in postmenopausal women with early breast cancer. N Engl J Med. 2005;353(26):2747–2757. | ||
Powles TJ, Hickish T, Kanis JA, Tidy A, Ashley S. Effect of tamoxifen on bone mineral density measured by dual-energy x-ray absorptiometry in healthy premenopausal and postmenopausal women. J Clin Oncol. 1996;14(1):78–84. | ||
Lønning PE, Geisler J, Krag LE, et al. Effects of exemestane administered for 2 years versus placebo on bone mineral density, bone biomarkers, and plasma lipids in patients with surgically resected early breast cancer. J Clin Oncol. 2005;23(22):5126–5137. | ||
Perez EA, Josse RG, Pritchard KI, et al. Effect of letrozole versus placebo on bone mineral density in women with primary breast cancer completing 5 or more years of adjuvant tamoxifen: a companion study to NCIC CTG MA.17. J Clin Oncol. 2006;24(22):3629–3635. | ||
Geisler J, Lønning PE, Krag LE, et al. Changes in bone and lipid metabolism in postmenopausal women with early breast cancer after terminating 2-year treatment with exemestane: a randomised, placebo-controlled study. Eur J Cancer. 2006;42(17):2968–2975. | ||
Coombes RC, Kilburn LS, Snowdon CF, et al; Intergroup Exemestane Study. Survival and safety of exemestane versus tamoxifen after 2-3 years’ tamoxifen treatment (Intergroup Exemestane Study): a randomised controlled trial. Lancet. 2007;369(9561):559–570. | ||
Coleman RE, Banks LM, Girgis SI, et al; Intergroup Exemestane Study Group. Skeletal effects of exemestane on bone-mineral density, bone biomarkers, and fracture incidence in postmenopausal women with early breast cancer participating in the Intergroup Exemestane Study (IES): a randomised controlled study. Lancet Oncol. 2007;8(2):119–127. | ||
Hadji P, Ziller M, Kieback DG, et al. Effects of exemestane and tamoxifen on bone health within the Tamoxifen Exemestane Adjuvant Multicentre (TEAM) trial: results of a German, 12-month, prospective, randomised substudy. Ann Oncol. 2009;20(7):1203–1209. | ||
Goss PE, Qi S, Cheung AM, Hu H, Mendes M, Pritzker KP. Effects of the steroidal aromatase inhibitor exemestane and the nonsteroidal aromatase inhibitor letrozole on bone and lipid metabolism in ovariectomized rats. Clin Cancer Res. 2004;10(17):5717–5723. | ||
Goss PE, Hershman DL, Cheung AM, et al. Effects of adjuvant exemestane versus anastrozole on bone mineral density for women with early breast cancer (MA.27B): a companion analysis of a randomised controlled trial. Lancet Oncol. 2014;15(4):474–482. | ||
Presant CA, Bosserman L, Young T, et al. Aromatase inhibitor-associated arthralgia and/or bone pain: frequency and characterization in non-clinical trial patients. Clin Breast Cancer. 2007;7(10):775–778. | ||
Nabholtz JM. Long-term safety of aromatase inhibitors in the treatment of breast cancer. Ther Clin Risk Manag. 2008;4(1):189–204. | ||
Atalay G, Dirix L, Biganzoli L, et al. The effect of exemestane on serum lipid profile in postmenopausal women with metastatic breast cancer: a companion study to EORTC Trial 10951, ‘Randomized phase II study in first line hormonal treatment for metastatic breast cancer with exemestane or tamoxifen in postmenopausal patients’. Ann Oncol. 2004;15(2):211–217. | ||
Jones SE, Cantrell J, Vukelja S, et al. Comparison of menopausal symptoms during the first year of adjuvant therapy with either exemestane or tamoxifen in early breast cancer: report of a Tamoxifen Exemestane Adjuvant Multicenter trial substudy. J Clin Oncol. 2007;25:4765–4771. | ||
Fallowfield LJ, Kilburn LS, Langridge C, Snowdon CF, Bliss JM, Coombes RC. Long-term assessment of quality of life in the Intergroup Exemestane Study: 5 years post-randomisation. Br J Cancer. 2012;106:1062–1067. | ||
Bender CM, Sereika SM, Brufsky AM, et al. Memory impairments with adjuvant anastrozole versus tamoxifen in women with early-stage breast cancer. Menopause. 2007;14(6):995–998. | ||
Phillips KA, Ribi K, Sun Z, et al. Cognitive function in postmenopausal women receiving adjuvant letrozole or tamoxifen for breast cancer in the BIG 1-98 randomized trial. Breast. 2010;19:388–395. | ||
Schilder CM, Seynaeve C, Beex LV, et al. Effects of tamoxifen and exemestane on cognitive functioning of postmenopausal patients with breast cancer: results from the neuropsychological side study of the tamoxifen and exemestane adjuvant multinational trial. J Clin Oncol. 2010;28:1294–1300. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.