")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 12
Clinical utility of daylight photodynamic therapy in the treatment of actinic keratosis – a review of the literature
Authors Nguyen M, Sandhu SS, Sivamani RK
Received 31 March 2019
Accepted for publication 24 May 2019
Published 7 June 2019 Volume 2019:12 Pages 427—435
DOI https://doi.org/10.2147/CCID.S167498
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Mimi Nguyen,1 Simran S Sandhu,1 Raja K Sivamani1–4
1Department of Dermatology, University of California – Davis, Sacramento, CA, USA; 2Department of Biological Sciences, California State University Sacramento, Sacramento, CA, USA; 3College of Medicine, California Northstate University, Elk Grove, CA, USA; 4Department of Dermatology, Pacific Skin Institute, Sacramento, CA, USA
Abstract: Actinic keratosis (AK) is an early in situ squamous cell carcinoma that results from UV light exposure and has the potential to evolve into invasive tumor. Therefore, it is crucial that AKs are monitored and treated appropriately. Photodynamic therapy (PDT) is a treatment option that is minimally invasive and leaves patients with cosmetically superior results. However, disadvantages of PDT include pain and lengthy clinic visits. Accordingly, there has been much interest in the use of daylight photodynamic therapy (daylight-PDT) as a more convenient and less painful alternative to conventional photodynamic therapy (c-PDT). Current evidence shows that daylight-PDT is noninferior to c-PDT in the short and long term. Patients reported decreased pain with daylight-PDT and were more satisfied with the procedure (P<0.001). Current evidence suggests that 2 hrs of daylight exposure was sufficient for treatment, and its efficacy does not appear to be limited by weather conditions. Given the decreased intensity of treatment, daylight-PDT is better for mild disease, as it is less effective in moderate-to-thick AKs. Though further studies are still needed to refine the technique, daylight-PDT is a potential alternative to c-PDT for thin-to-moderate AKs and should be offered to patients with lower pain tolerance or busy schedules.
Keywords: daylight, conventional, photodynamic therapy, actinic keratosis, pretreatment
Introduction
Excessive sunlight exposure can have deleterious effects on one’s skin. Excess UV exposure has the capacity to induce genetic changes within keratinocytes – these changes can result in a dysfunctional apoptotic system. Disruptions of pathways that regulate cell growth and differentiation contribute to local inflammation and immunosuppression – resulting in proliferation of abnormal cells and the appearance of actinic keratoses (AKs).1 Since AKs serve as potential precursors for squamous cell carcinomas (SCCs), both pathologies share an underlying mechanism – genetic changes caused by UV light leading to dysregulated cell proliferation. With current estimated prevalence rates for AK ranging between 11% and 16% in the United States, and potentially as high as 60% in other locations, early treatment is important to reduce the risk of invasive SCC.2,3
When it comes to treatment for AKs, clinicians have a plethora of various therapy options at their disposal. Common topical treatments include 5-fluorouracil (5-FU), diclofenac, imiquimod, and ingenol mebutate.2 Procedural treatments such as cryotherapy are effective treatments, although they are not able to treat an entire field of AKs. In recent years, however, more advanced procedural field therapies such as photodynamic therapy (PDT), manual dermabrasion, cryopeeling, laser resurfacing, and chemical peels have been developed.2
PDT is of particular interest to clinicians as it is minimally invasive, does not require repeated applications of a topical therapy, can be performed in the medical office, and leaves patients with cosmetically superior results.4 Despite the benefits conferred by PDT, patients frequently complain of pain associated with the procedure and do not appreciate the length of clinic visits involved with the treatment. Accordingly, there has been much interest in the use of daylight photodynamic therapy (daylight-PDT) as a more convenient and less painful alternative to conventional photodynamic therapy (c-PDT).
Methods
We searched Embase and PubMed for published clinical studies assessing the efficacy of daylight-PDT on the treatment of actinic keratoses, using “daylight photodynamic therapy” and “actinic keratosis” as our keywords. No limits were placed on the search time frame. The search included articles published before May 22, 2019. Only clinical studies in English and those involving human studies were included. From there, studies unrelated to the topics covered in this review were excluded. Nine relevant studies were included in our review.
What is cPDT
PDT takes advantage of our heme synthesis pathway and causes a buildup of an endogenous photosensitizer – clinicians are able to use light to induce ROS(singlet oxygen) capable of cytotoxic effects. This generation of ROS overwhelms the cells’ inherent antioxidant defense and results in intracellular damage of proteins, lipids, and DNA molecules – eventually leading to cell death. With regard to efficacy, PDT has demonstrated excellent cosmetic results and is considered an alternative to 5-FU or cryotherapy for thin-to-moderate thickness AKs, as defined by the Olsen clinical classification scheme.5 This noninvasive treatment is based on the interaction of three pivotal components – oxygen, a photosensitizing compound, and light of the appropriate wavelength.
The typical approach clinicians take with PDT is by initially photosensitizing the affected area with topical application of δ-5-aminolaevulinic acid (ALA) or its methyl ester (MAL).6 ALA is an early intermediate in the heme biosynthesis pathway and is also a precursor to the natural photosensitizer protoporphyrin IX (PpIX). Topical administration of ALA nonselectively penetrates into the epidermis and is metabolized by the enzymatic machinery of the heme synthesis pathway, found in almost all human cells, into the active sensitizer PpIX. Typically, PpIX generated from ALA is converted into heme via the enzyme ferrochelatase – a rate-limiting step that occurs on the inner surface of the inner mitochondrial membrane, resulting in the insertion of Fe2+ into PpIX. This exogenous application of ALA bypasses the normal negative feedback mechanism of the heme synthesis pathway and results in PpIX being produced at a faster rate than ferrochelatase can covert PpIX into heme – thus leading to an accumulation of PpIX.7
Though ALA nonselectively enters cells, PpIX tends to preferentially accumulate in tumor cells. This can be attributed to enzymatic activity differences between neoplastic and normal cells – most notably, the decreased activity of ferrochelatase in tumor cells may contribute to PpIX buildup in the mitochondria.8,9
The incubation time for adequate photosensitization of skin using topical ALA varies based on both the concentration of the solution being used and the area of application. Incubation times can vary from 0 to 18 hrs, but has been highly effective with incubation times of as little as 1 hr.10–12
According to the American Society of Photodynamic Therapy Board and British Dermatology group, there are currently no standardized guidelines as it relates to selecting an optimal irradiance, wavelength, and total dose for c-PDT.7 However, lasers and light sources are chosen based on its ability to activate the photosensitizer. PpIX has absorption peaks at multiple regions, including 400–410 nm (Soret band) and 630–635 nm (Q band), which correlates with wavelengths in the blue and red regions of the visible light spectrum, respectively.13 PpIX has a maximum absorption band at 408 nm; therefore, blue light is more effective in activating PpIX.14 Photoactivation of PpIX in the presence of oxygen leads to the generation of free radical oxygen singlets that lead to destruction of the cell.7 Ultimately, the most appropriate light source for c-PDT is determined by which light source provides the greatest efficacy for the specific condition being treated. Photons in the blue wavelength range of 400–500 nm are able to penetrate up to 2 mm in the skin and are thus recommended for superficial lesions. Red light can penetrate up to 6 mm into the skin and is thus recommended for the therapy of deeper lesions.15
c-PDT for AKs is not without its drawbacks. Patients frequently report pain as the most common side effect. The standard procedure for c-PDT calls for occlusive treatment with a photosensitizer for 1–3 hrs, allowing for enough time for accumulation of PpIX.12,16–18 However, FDA approval for use of photosensitizers in the treatment of AK involves incubation periods of 3 hrs for MAL, 18 hrs for ALA, and 3 hrs for nanoemulsions for ALA.4,19,20 The accumulated PpIX is then rapidly activated by red light, resulting in the generation of ROS which may be the cause of pain associated with c-PDT. This discomfort combined with frequent and lengthy clinic visits has collectively motivated researchers to find more tolerable and convenient uses of PDT.21
Daylight-PDT is an example of such an endeavor. Daylight-PDT relies on daylight instead of an artificial light source, allowing for decreased pain and shorter clinic visits. The diffuse and direct sunlight that strikes the earth’s surface has a visible light range approximately between 380 and 780 nm.22 Because all of the absorption peaks for PpIX are within the visual spectrum of light, daylight is able to effectively activate the accumulated PpIX, thus leading to targeted tissue injury and cell death. The largest absorbance for PpIX is in the Soret band (410 nm), while the remaining Q bands elicit a small absorbance peak. Accordingly, 87% of the PpIX activated from daylight exposure is due to blue light.5 Of note, red light penetrates deeper than blue light, which may also contribute to efficacy.
Daylight-PDT offers the benefit of convenience and minimal discomfort due to the use of natural light. Rather than applying a photosensitizer and then returning to the clinic after 3 hrs for light treatment, patients are able to complete their therapy at home. The dramatically shorter incubation time for the photosensitizer with daylight-PDT compared to c-PDT (30 mins vs 1–3 hrs, respectively) allows for a smaller and more continuous rate of production and activation of PpIX. This continuous activation instead of rapid activation of large amounts of PpIX with blue or red light may be the reason for the lower pain intensity associated with daylight-PDT.5
Efficacy of daylight-PDT
In order for daylight-PDT to be considered a reasonable alternative to c-PDT, it needs to be equally effective, both in the short and long term. Here, we discuss the available evidence for use of daylight-PDT in the treatment of AKs (Table 1).
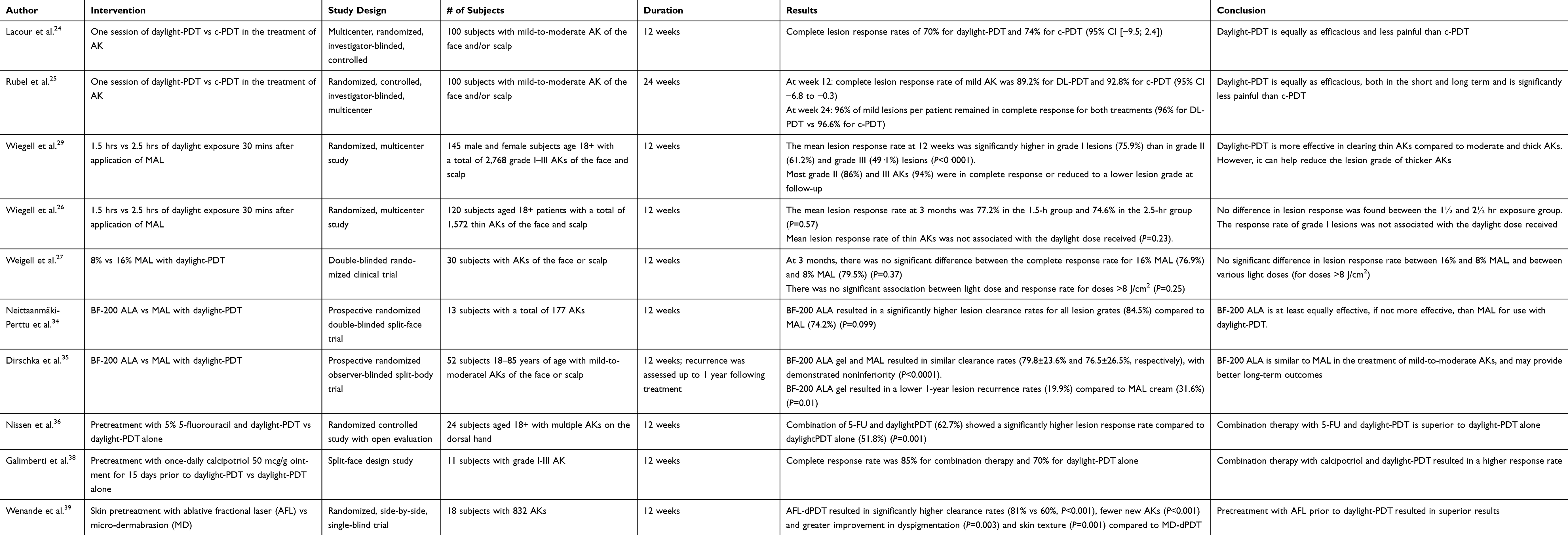 | Table 1 Summary of available evidence on the efficacy of daylight photodynamic therapy in the treatment of actinic keratosis |
A recent meta-analysis of 6 randomized controlled trials comparing daylight-PDT and c-PDT concluded that daylight-PDT is noninferior to c-PDT in the treatment of grade I and II AKs.23 Two of the studies included in the meta-analysis were large, randomized, controlled, investigator-blinded, split-body, multicenter studies in Australia and Europe of 100 patients with grade I and II AKs.24,25 Both studies excluded individuals with severe AK and other skin diseases and required 2 hrs of daylight exposure time, 30 mins following MAL application. The study conducted in Australia demonstrated a complete lesion response rate of 89.2% and 92.8% for daylight-PDT and c-PDT, respectively, while the study in Europe resulted in complete lesion response rates of 70% for daylight-PDT and 74% for c-PDT.24,25 Daylight-PDT demonstrated noninferiority to c-PDT at 12-week follow-up in both studies.
Long-term efficacy
Furthermore, in the Australian study, both daylight-PDT and c-PDT maintained lesion clearance for 96% of grade I lesions at 6 months following treatment, demonstrating that there was no difference between the two treatments at long-term follow-up.25
Length of exposure
One study directly compared the response rate by length of exposure to daylight. A randomized multicenter study with 120 patients in Denmark, Norway, and Sweden compared lesion response rates after 1.5–2 hrs and 2.5–3 hrs of exposure to daylight. Their study included 120 patients, totaling 1,572 grade I AK lesions on the face and scalp. SPF 20 sunscreen and 16% MAL cream were applied to the treatment area, and the subjects were exposed to daylight within 30 mins. They were instructed to end daylight exposure either 2 hrs or 3 hrs after MAL application, depending on which treatment group they were randomized to, resulting in at least 1.5 and 2.5 hrs of daylight exposure. There was no difference in mean light dose received by both groups (1.5–2 hr group: 8.6 J/cm2 vs 2.5–3 hr group: 10.2 J/cm2) (P=0.23), with some patients receiving less than 3 J/cm2. There was no difference in the lesion response rate at 3 months following treatment, between the two groups. The 1.5–2 hr group showed a 77.2% mean lesion response rate compared to 74.6% in the 2.5–3 hr group (P=0.57).
The authors concluded that the lesion response rate was not correlated with increased exposure duration and that 2 hrs of daylight exposure was sufficient to receive the minimum light dose (3 J/cm2) needed for treatment of thin AKs, unless rainy or cold weather conditions are present. Further studies are needed to quantify the minimum duration of daylight exposure.26
Joules of exposure
In the aforementioned study, the authors used an electronic dosimeter to measure the effective light dose. Those in the 1.5 hr and 2.5 hr group were exposed to a mean effective light dose of 8.6 J/cm2 and 10.2 J/cm2, respectively. The mean lesion response rate of grade I lesions was not associated with the daylight dose received (P=0.23), and those exposed to <3 J/cm2 still demonstrated a lesion response rate as high as 70%.26
This contradicted their earlier findings, which showed no association between light dose and response rate for doses >8 J/cm2, but a linear association when comparing all doses (1.2–69.8J/cm2) (P=0.005).27 They argue that use of different dosimeters and differences in sample size led to these contradictory findings. The same group also found no association between mean red light dose and response rate in 30 patients with AK (grades I–III).28
A higher effective light dose, was, however, associated with a higher maximum pain score (P=0.03).26 Therefore, given current evidence that there is no association between response rate and light dose, a dose of at least 3 J/cm2 is recommended to provide a high response rate with minimal pain.
Patient satisfaction
Subjects from both studies reported daylight-PDT was less painful than c-PDT, with average pain scores (rated on a 10 point scale) between 0.7 and 0.8 for daylight-PDT compared to 4.4–5.7 for c-PDT (P<0.001). They were also more satisfied with daylight-PDT compared to c-PDT and would consider using daylight-PDT again.24,25
Thin vs thick lesions
Although daylight-PDT may be efficacious, it has its limitations. In a study of 145 patients, daylight-PDT was less effective for moderate-to-thick AKs compared to thin AKs. At 3 months following a single treatment of daylight-PDT, 73% of grade I lesions showed a complete response, compared to 63% of grade II lesions and 55% of grade III lesions.29 However, 23% of grade II and 39% of grade III lesions were reduced to a lower lesion grade, demonstrating that it remains somewhat efficacious in the treatment of thicker AKs. It is important to note that the clinical thickness of AK does not relate to histological type so the clinical thickness of an AK is not a reliable predictor of its evolution toward an SCC.30
Weather
Weather does not appear to play a role in the efficacy of daylight-PDT, as similar response rates have been seen in both sunny and cloudy weather.24–26 However, all authors are in agreement that daylight-PDT should not be performed in rainy weather.24–26
Overall, mean response rates of daylight-PDT (70–89.2%)24–27 have been comparable to those of c-PDT (75–92.8%31–33) and regardless of weather conditions D-PDT may be less painful and demonstrate higher patient satisfaction than c-PDT.
ALA vs MAL
Though there is limited research done comparing the efficacy of ALA and MAL in daylight-PDT, two studies have concluded that ALA is similar and potentially more effective than MAL in daylight-PDT. A randomized observer-blinded study involving a split-face trial with 13 patients and a collective total of 177 grade I–III AKs compared daylight-PDT treatments using 5-ALA nanoemulsion gel or methyl-5-aminolaevulinic cream as the photosensitizer.34 Grade I AKs were treated once and grade II–III AKs were treated twice with a 0.25-mm layer of photosensitizer. Overall, nanoemulsion ALA daylight-PDT cleared 85% of the AKs, whereas MAL daylight-PDT cleared 74% of the total AKs (P=0.099). When the results were broken down by lesion thickness, ALA was more effective at clearing grade I AKs than MAL (P=0.027), but they had similar rates of clearance for thicker grade AKs (P=0.564).34 A more recent study compared BF‐200 ALA (a nanoemulsion gel containing 7.8% 5‐ALA) to MAL in the treatment of mild‐to‐moderate AK with daylight-PDT. This was a split-body randomized, observer‐blind, clinical trial involving 52 patients from seven centers in Germany and Spain. Twelve weeks following treatment, complete clearance rates for BF-200 ALA gel and MAL were similar (79.8±23.6% and 76.5±26.5%, respectively, P<0.0001). The sides treated with BF‐200 ALA gel also had lower 1‐year lesion recurrence rates (19.9%) compared with sides treated with MAL cream (31.6%) (P=0.01).35 Current evidence suggests that nanoemulsion ALA is similar in efficacy to MAL cream in the treatment of AKs and that ALA may provide better clearance of thinner AKs and greater efficacy of clearance at 1 year.
Topical dose
Additionally, in another study involving 30 patients with thin grade AK on the face or scalp, the response rates after daylight-PDT using either 16% or 8% MAL were examined. The results showed no difference in response rates or adverse effects between the two treatment groups.27 There were no available studies investigating the effective dose of ALA.
Pretreatments /adjuncts
Pretreatment of the skin prior to treatment with daylight-PDT is suggested to improve efficacy by increasing penetration of the ALA or MAL.
Pretreatment with 5-FU
A randomized intraindividual study involving 24 patients with AKs on their hands examined whether pretreatment with 5-FU enhanced the efficacy of daylight-PDT. The participants were instructed to apply 5-FU twice daily for 7 days to one of their randomly assigned hands, whereas the other hand only received daylight-PDT. On day 8, patients returned to clinic and underwent daylight-PDT with 16% MAL and 2 hrs of daylight exposure 30 mins after application of the photosensitizer. At 3 months follow-up, combination therapy with 5% 5-FU cream yielded higher mean clearance rates than just daylight-PDT alone (63% vs 52%, respectively) (P=0.001).36
Pretreatment with calcipotriol
A split-face design study involving 11 participants with grade I–III AKs were instructed to apply calcipotriol (shown to have some effects against AK) 1 hr before bed once daily to half their face or scalp for 15 days prior to their daylight-PDT session. Using a 16% MAL cream and 2 hr sunlight exposure, the results showed a 85% complete response rate for treatment with calcipotriol and daylight-PDT and 70% for daylight-PDT alone. Though the pretreatment group did show improved treatment, patients reported adverse events related to the pretreatment – including marked erythema and desquamation.37,38
Pretreatment with ablative fractional laser or microdermabrasion
A randomized, blinded, clinical trial involving 18 patients with 832 AKs total investigated if pretreatment with ablative fractional laser (AFL-dPDT) or microdermabrasion (MDA-dPDT) increased the efficacy of daylight-PDT. The results showed that AFL had higher rates of AK clearance than MDA (81% and 60%, respectively), consistently across all grades (P<0.001).39 Another study compared AFL‐assisted daylight photodynamic therapy (AFL‐dPDT), with daylight-PDT, cPDT, and AFL alone (AFL) in organ-transplant recipients and found significant differences in complete response rates. At 1 and 3 months following treatment, the authors found a median complete response of 74% with AFL-dPDT, which was higher than daylight-PDT (46%) (P=0.026), cPDT (50%) (P=0.042), and AFL (5%) (P=0·004).40 Altogether, it appears pretreatment with AFL can augment the effects of daylight-PDT. Though the clearance rate is similar to those observed in other studies with daylight-PDT alone (clearance rates of 70–89%),5 the benefit is clear in organ transplant patients, who tend to have AKs that are more resistant to treatment. AFL appears to be effective in augmenting d-PDT in patients with difficult-to-treat AKs.
Treatment guidelines
Groups of experts from Europe and Australia have independently published treatment guidelines for the use of daylight-PDT for AK. Based on current evidence, both groups recommend the use of daylight-PDT for those with thin-to-moderate (grades I and II) AK lesions on the face and scalp, which is similar to current recommendations for c-DPT.41,42
Prior to application of a photosensitizer, the treatment site should be clean, and a chemical sunscreen with SPF 30+ should be applied to all sun-exposed areas.41,42 Concomitant use of physical sunscreens containing zinc oxide, iron oxide, and titanium dioxide may reduce treatment efficacy by preventing penetration of visible light.41 Pretreatment of the area with microneedling, curettage, or chemical peels may be done before or after sunscreen application, but prior to application of the photosensitizer.
A thin layer of photosensitizing cream (1–2 g for the entire face) is then applied to the treatment area, and daylight exposure should begin within 30 mins. European and Australian guidelines recommend the use of MAL, as there is more available evidence supporting its use in daylight-PDT for the treatment of AKs. However, some studies show that ALA – an option more widely available in the United States – appears similar to MAL, and may provide better long-term results.34,35,43
Patients are instructed to keep the treatment areas exposed to equal intensities of daylight and to avoid shaded areas.5 Both groups recommend continuous exposure for 2 hrs, as that is often sufficient to receive the appropriate light dose of >3 J/cm2. After the 2 hr period, the MAL cream should be washed off.
After treatment, patients should be counseled regarding the diligent use of sunscreen and moisturizer to minimize adverse events. Both groups recommend reevaluation of lesions at 3 months following treatment.41,42 One treatment is often sufficient to treat grade I and II AKs, but repeat sessions may be necessary.
Side effects
Common side effects of daylight-PDT are generally mild and include discomfort, erythema, blistering, itching, and crusting. Phototoxic reactions and pustular eruptions have been observed with daylight-PDT.21,25,27 More severe reactions including infection and scarring are rare with daylight-PDT.42 Ice packs, cooling therapy, and moisturizing can be used to reduce the severity of adverse events.
Conclusion
The current body of scientific evidence suggests that daylight-PDT is a safe and effective alternative to c-PDT for thin-to-moderate AK lesions. Though further studies are still needed to determine the minimum exposure time necessary to minimize side effects, clinicians should be aware that daylight-PDT is a potential treatment option for patients with low pain tolerance or schedule unavailability.
Disclosure
RKS serves as a medical editor for LearnHealth and as a consultant for Burt’s Bees, Dermala, and Tomorrow’s Leaf. The authors report no other conflicts of interest in this work.
References
1. Berman B, Cockerell CJ. Pathobiology of actinic keratosis: ultraviolet-dependent keratinocyte proliferation. J Am Acad Dermatol. 2013;68(1 Suppl 1):S10–S19. doi:10.1016/j.jaad.2012.09.053
2. Costa C, Scalvenzi M, Ayala F, Fabbrocini G, Monfrecola G. How to treat actinic keratosis? An update. J Dermatol Case Rep. 2015;9(2):29–35. doi:10.3315/jdcr.2015.1199
3. Lee PK, Kloser A. Current methods for photodynamic therapy in the US: comparison of MAL/PDT and ALA/PDT. J Drugs Dermatol. 2013;12(8):925–930.
4. Cohen DK, Lee PK. Photodynamic therapy for non-melanoma skin cancers. Cancers (Basel). 2016;8(10). doi:10.3390/cancers8100090
5. Morton CA, Braathen LR. Daylight photodynamic therapy for actinic keratoses. Am J Clin Dermatol. 2018;19:647–656. doi:10.1007/s40257-018-0360-y
6. Ericson MB, Wennberg A-M, Larkö O. Review of photodynamic therapy in actinic keratosis and basal cell carcinoma. Ther Clin Risk Manag. 2008;4(1):1–9.
7. Palm M, Goldman MP. Aminolevulinic acid: actinic keratosis and photorejuvenation. Photodynamic Therapy in Dermatology. SpringerLink. 2011;5–29. doi:10.1007/978-1-4419-1298-5_2.
8. Dailey HA, Smith A. Differential interaction of porphyrins used in photoradiation therapy with ferrochelatase. Biochem J. 1984;223(2):441–445. doi:10.1042/bj2230441
9. Iinuma S, Farshi SS, Ortel B, Hasan T. A mechanistic study of cellular photodestruction with 5-aminolaevulinic acid-induced porphyrin. Br J Cancer. 1994;70(1):21–28. doi:10.1038/bjc.1994.244
10. Photodynamic therapy. UpToDate; 2018.
11. Touma D, Yaar M, Whitehead S, Konnikov N, Gilchrest BA. A trial of short incubation, broad-area photodynamic therapy for facial actinic keratoses and diffuse photodamage. Arch Dermatol. 2004;140(1):33–40. doi:10.1001/archderm.140.1.33
12. Pariser DM, Houlihan A, Ferdon MB, Berg JE, Group P-AI. Randomized vehicle-controlled study of short drug incubation aminolevulinic acid photodynamic therapy for actinic keratoses of the face or scalp. Dermatol Surg. 2016;42(3):296–304. doi:10.1097/DSS.0000000000000630
13. Piacquadio DJ, Chen DM, Farber HF, et al. Photodynamic therapy with aminolevulinic acid topical solution and visible blue light in the treatment of multiple actinic keratoses of the face and scalp: investigator-blinded, phase 3, multicenter trials. Arch Dermatol. 2004;140(1):41–46. doi:10.1001/archderm.140.1.41
14. Kleinpenning MM, Otero ME, van Erp PE, Gerritsen MJ, van de Kerkhof PC. Efficacy of blue light vs. red light in the treatment of psoriasis: a double-blind, randomized comparative study. J Eur Acad Dermatol Venereol. 2012;26(2):219–225. doi:10.1111/j.1468-3083.2011.04039.x
15. Nootheti PK, Goldman MP. Aminolevulinic acid-photodynamic therapy for photorejuvenation. Dermatol Clin. 2007;25(1):35–45. doi:10.1016/j.det.2006.09.010
16. Wan MT, Lin JY. Current evidence and applications of photodynamic therapy in dermatology. Clin Cosmet Investig Dermatol. 2014;7:145–163. doi:10.2147/CCID.S35334
17. Gandy J, Labadie B, Bierman D, Zachary C. Photodynamic therapy effectively treats actinic keratoses without pre-illumination incubation time. J Drugs Dermatol. 2017;16(3):275–278.
18. Braathen LR, Paredes BE, Saksela O, et al. Short incubation with methyl aminolevulinate for photodynamic therapy of actinic keratoses. J Eur Acad Dermatol Venereol. 2009;23(5):550–555.
19.
20.
21. Wiegell SR, Wulf HC, Szeimies RM, et al. Daylight photodynamic therapy for actinic keratosis: an international consensus: international society for photodynamic therapy in dermatology. J Eur Acad Dermatol Venereol. 2012;26(6):673–679. doi:10.1111/j.1468-3083.2011.04386.x
22. Sliney DH. What is light? The visible spectrum and beyond. Eye. 2016;30(2):222–229. doi:10.1038/eye.2015.252
23. Mei X, Wang L, Zhang R, Zhong S. Daylight versus conventional photodynamic therapy for the treatment of actinic keratosis: a meta-analysis of randomized controlled trials. Photodiagnosis Photodyn Ther. 2018;25:23–28.
24. Lacour JP, Ulrich C, Gilaberte Y, et al. Daylight photodynamic therapy with methyl aminolevulinate cream is effective and nearly painless in treating actinic keratoses: a randomised, investigator-blinded, controlled, phase III study throughout Europe. J Eur Acad Dermatol Venereol. 2015;29(12):2342–2348. doi:10.1111/jdv.13228
25. Rubel DM, Spelman L, Murrell DF, et al. Daylight photodynamic therapy with methyl aminolevulinate cream as a convenient, similarly effective, nearly painless alternative to conventional photodynamic therapy in actinic keratosis treatment: a randomized controlled trial. Br J Dermatol. 2014;171(5):1164–1171. doi:10.1111/bjd.13138
26. Wiegell SR, Fabricius S, Stender IM, et al. A randomized, multicentre study of directed daylight exposure times of 1 (1/2)vs. 2 (1/2)h in daylight-mediated photodynamic therapy with methyl aminolaevulinate in patients with multiple thin actinic keratoses of the face and scalp. Br J Dermatol. 2011;164(5):1083–1090. doi:10.1111/j.1365-2133.2011.10209.x
27. Wiegell SR, Haedersdal M, Eriksen P, Wulf HC. Photodynamic therapy of actinic keratoses with 8% and 16% methyl aminolaevulinate and home-based daylight exposure: a double-blinded randomized clinical trial. Br J Dermatol. 2009;160(6):1308–1314. doi:10.1111/j.1365-2133.2009.09119.x
28. Wiegell SR, Haedersdal M, Philipsen PA, Eriksen P, Enk CD, Wulf HC. Continuous activation of PpIX by daylight is as effective as and less painful than conventional photodynamic therapy for actinic keratoses; a randomized, controlled, single-blinded study. Br J Dermatol. 2008;158(4):740–746. doi:10.1111/j.1365-2133.2008.08450.x
29. Wiegell SR, Fabricius S, Gniadecka M, et al. Daylight-mediated photodynamic therapy of moderate to thick actinic keratoses of the face and scalp: a randomized multicentre study. Br J Dermatol. 2012;166(6):1327–1332. doi:10.1111/j.1365-2133.2012.10833.x
30. Schmitz L, Kahl P, Majores M, Bierhoff E, Stockfleth E, Dirschka T. Actinic keratosis: correlation between clinical and histological classification systems. J Eur Acad Dermatol Venereol. 2016;30(8):1303–1307. doi:10.1111/jdv.13626
31. Morton C, Campbell S, Gupta G, et al. Intraindividual, right-left comparison of topical methyl aminolaevulinate-photodynamic therapy and cryotherapy in subjects with actinic keratoses: a multicentre, randomized controlled study. Br J Dermatol. 2006;155(5):1029–1036. doi:10.1111/j.1365-2133.2006.07470.x
32. Szeimies RM, Karrer S, Radakovic-Fijan S, et al. Photodynamic therapy using topical methyl 5-aminolevulinate compared with cryotherapy for actinic keratosis: a prospective, randomized study. J Am Acad Dermatol. 2002;47(2):258–262.
33. Tarstedt M, Rosdahl I, Berne B, Svanberg K, Wennberg AM. A randomized multicenter study to compare two treatment regimens of topical methyl aminolevulinate (Metvix)-PDT in actinic keratosis of the face and scalp. Acta Derm Venereol. 2005;85(5):424–428. doi:10.1080/00015550510032887
34. Neittaanmäki-Perttu N, Karppinen TT, Grönroos M, Tani TT, Snellman E. Daylight photodynamic therapy for actinic keratoses: a randomized double-blinded nonsponsored prospective study comparing 5-aminolaevulinic acid nanoemulsion (BF-200) with methyl-5-aminolaevulinate. Br J Dermatol. 2014;171(5):1172–1180. doi:10.1111/bjd.13326
35. Dirschka T, Ekanayake-Bohlig S, Dominicus R, et al. A randomized, intraindividual, non-inferiority, phase III study comparing daylight photodynamic therapy with BF-200 ALA gel and MAL cream for the treatment of actinic keratosis. J Eur Acad Dermatol Venereol. 2019;33(2):288–297. doi:10.1111/jdv.15185
36. Nissen CV, Heerfordt IM, Wiegell SR, Mikkelsen CS, Wulf HC. Pretreatment with 5-fluorouracil cream enhances the efficacy of daylight-mediated photodynamic therapy for actinic keratosis. Acta Derm Venereol. 2017;97(5):617–621. doi:10.2340/00015555-2612
37. Seckin D, Cerman AA, Yildiz A, Ergun T. Can topical calcipotriol be a treatment alternative in actinic keratoses? A preliminary report. J Drugs Dermatol. 2009;8(5):451–454.
38. Galimberti GN. Calcipotriol as pretreatment prior to daylight-mediated photodynamic therapy in patients with actinic keratosis: a case series. Photodiagnosis Photodyn Ther. 2018;21:172–175. doi:10.1016/j.pdpdt.2017.11.019
39. Wenande E, Phothong W, Bay C, Karmisholt KE, Haedersdal M, Togsverd-Bo K. Efficacy and safety of daylight photodynamic therapy after tailored pretreatment with ablative fractional laser or microdermabrasion: a randomized, side-by-side, single-blind trial in patients with actinic keratosis and large area field cancerization. Br J Dermatol. 2018;180(4):756–764.
40. Togsverd-Bo K, Lei U, Erlendsson AM, et al. Combination of ablative fractional laser and daylight-mediated photodynamic therapy for actinic keratosis in organ transplant recipients - a randomized controlled trial. Br J Dermatol. 2015;172(2):467–474. doi:10.1111/bjd.13222
41. See JA, Shumack S, Murrell DF, et al. Consensus recommendations on the use of daylight photodynamic therapy with methyl aminolevulinate cream for actinic keratoses in Australia. Australas J Dermatol. 2016;57(3):167–174. doi:10.1111/ajd.12354
42. Philipp-Dormston WG, Sanclemente G, Torezan L, et al. Daylight photodynamic therapy with MAL cream for large-scale photodamaged skin based on the concept of ‘actinic field damage’: recommendations of an international expert group. J Eur Acad Dermatol Venereol. 2016;30(1):8–15. doi:10.1111/jdv.13327
43. Shive ML, Coakley BJ, Bierman DF, et al. Use of 5-aminolevulinic acid and daylight photodynamic therapy for the treatment of actinic keratoses. Dermatol Surg. 2019. doi:10.1097/DSS.0000000000001771
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.