")
Back to Journals » Cancer Management and Research » Volume 14
Clinical Utility of Azacitidine in the Management of Acute Myeloid Leukemia: Update on Patient Selection and Reported Outcomes
Authors Moreno Vanegas Y, Badar T
Received 29 August 2022
Accepted for publication 23 November 2022
Published 23 December 2022 Volume 2022:14 Pages 3527—3538
DOI https://doi.org/10.2147/CMAR.S271442
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kattesh Katti
Yenny Moreno Vanegas, Talha Badar
Division of Hematology-Oncology and Blood and Marrow Transplantation and Cellular Therapy Program, Mayo Clinic, Jacksonville, FL, USA
Correspondence: Talha Badar, Mayo Clinic, 4500 San Pablo Road, Jacksonville, FL, 32224, USA, Email [email protected]
Abstract: Acute myeloid leukemia (AML) is predominantly a disease of the elderly, and a significant proportion of these patients are not candidates for intensive, curative-intent therapies. Epigenetic dysregulation resulting in abnormal DNA hypermethylation is one of the hallmarks of AML pathogenesis. For the past two decades, hypomethylating agents including azacitidine (AZA) have been the mainstay of treatment for AML patients who are ineligible to receive intensive chemotherapies. As our understanding of AML disease biology has improved, several novel treatment combinations have been developed to improve the outcome of AML patients, with remarkable success. A considerable proportion of these novel combinations have utilized AZA as the backbone of their treatment scheme. In this review, we have highlighted the evolution of AML treatment, focusing on novel AZA-based treatment combinations and their clinical efficacy.
Keywords: azacitidine, elderly AML, hypomethylating agent, azacitidine plus venetoclax
Introduction
Acute myeloid leukemia (AML) is a heterogeneous disorder characterized by clonal expansion of myeloid progenitors in the bone marrow, peripheral blood, or other tissues.1–3 Conventional therapy for AML is composed of induction chemotherapy with cytarabine and anthracycline-containing regimens, followed by consolidation therapy to prolong remission.4 A long-term response with these regimens is achieved in 30–40% of adults who are 60 years of age or younger.5 Although effective, this approach may be poorly tolerated, with a higher risk of induction mortality in patients with comorbidities, poor performance status, or advanced age.4 Historically, when used in patients older than 60 years of age, “7+3” chemotherapy has resulted in 5-year survival rates of less than 10%.5,6 Taking into account significant toxicity and poor outcomes with intensive chemotherapy (IC), older patients with comorbidities are often selected to receive lower intensity regimens with hypomethylating agents (HMAs), such as azacitidine (AZA) or decitabine.4 A large Surveillance, Epidemiology, and End Results–Medicare (SEER) database study identified 2263 older adults (age ≥66 years) diagnosed with AML during 2005–2015 who received a first-line HMA; 1154 (51%) patients received AZA. The median survival was 7.1 months compared to the historical 2.7 months of survival without any therapy.7 The inclusion of HMA therapy into the AML armamentarium represents an important expansion in treatment options for older and unfit patients with AML.8 Moreover, with the approval of the B-cell lymphoma-2 (BCL2) inhibitor venetoclax and several targeted agents in combination with AZA over the past few years, the AML therapeutic landscape continues to evolve towards more individualized therapy, necessitating careful patient selection and optimization of combination therapies.9 This review discusses studies evaluating the clinical utility of AZA-based treatments for the management of AML, focusing on patient selection and clinical outcomes.
Azacitidine
Mechanism of Action and Pharmacology
Hypermethylation of the tumor suppressor gene and the resulting epigenetic silencing is one of the main events leading to pathogenesis of myeloid malignancies.10 AZA is a pyrimidine nucleoside analogue of cytidine that can be incorporated directly into RNA, with subsequent disruption of RNA, protein synthesis, and metabolism.11 It is incorporated into DNA to a lesser extent, where it covalently binds to DNA methyltransferases and targets them for degradation. DNA synthesis in the absence of methyltransferases results in the hypomethylation of daughter cells and reactivation of silenced gene expression.12,13 Subsequently, in landmark studies, AZA (a DNA methyltransferase inhibitor) has demonstrated restoration of tumor suppressor gene function and differentiation of cells in patients with myelodysplastic syndrome (MDS) and AML.14
AZA is available for intravenous (IV) and subcutaneous (SC) administration, with comparable bioavailability between IV and SC administration.15 In vitro, studies have shown that AZA is not metabolized by the cytochrome P450 enzyme, uridine diphosphate, or glutathione transferase. Rather, it undergoes deamination by cytidine deaminase and it is mainly excreted by the kidneys.16 There is a sparsity of data regarding the use of AZA in patients with hepatic or renal impairment; however, no difference was observed in pharmacokinetics after AZA administration in patients with renal insufficiency versus those with normal renal function.16
Clinical Data
Azacitidine as a Single Agent
AZA is often used for patients with high-risk MDS and AML who are ineligible for IC. In 1984, the Cancer and Leukemia Group B (CALGB) began a series of clinical trials with AZA in patients with MDS and AML.17 The patients enrolled in three CALGB protocols (8421, 8921, and 8921) were analyzed to compare outcomes between AZA and best supportive care (BSC).17 The study showed higher response rates and prolonged time to AML transformation/death with AZA compared to BSC.12 Based on this and other observations showing the effectiveness of AZA in achieving transfusion independence and improvement in overall survival (OS),18 the US Food and Drug Administration (FDA) approved AZA for the treatment of MDS in 2004. In these studies, MDS was defined using the French–American–British (FAB) classification, which included patients with 20–30% bone marrow (BM) blasts, who are now classified by the World Health Organization (WHO) as having AML.19 One of the earliest clinical trials evaluating the use of AZA in MDS, which also included AML patients, was the AZA-001 trial, a phase III international, multicenter, controlled, open-label trial, where patients with higher-risk MDS were randomly assigned to receive either AZA (75 mg/m2 per day for 7 days every 28 days) or a conventional care regimen (CCR), including BSC, low-dose cytarabine, or IC, as selected by the investigators before randomization). After a median follow-up of 21.1 months, the median OS was 24.5 months with AZA compared to 15.0 months with CCR (hazard ratio [HR] 0.58, 95% confidence interval [CI] 0.43–0.77; p=0.0001). Cytopenias were the most common grade 3–4 adverse events for all treatments.20 Based on the promising results in this subset of MDS (BM blast ≥20%) patients, two phase III trials were conducted in AML.21,22 Fenaux et al conducted a randomized study on 113 elderly AML patients (AZA [n=55] vs CCR [n=58]) with low BM blast counts (20–30%).22 The median age of the patients was 70 years and 86% of them were considered unfit to receive IC. At the median follow-up of 20.1 months, the median OS for AZA-treated patients was 24.5 months compared with 16.0 months for patients treated with CCR (HR 0.47, 95% CI 0.28–0.29; p=0.005). The 2-year OS rates were higher in the AZA group than in the CCR group in patients who were deemed unfit for IC.22 Second, Dombret et al conducted the AZA-AML-001 trial, a multicenter, randomized, open-label, phase III trial evaluating the safety and efficacy of AZA vs CCR in 488 patients aged ≥65 years with treatment-naïve (TN) AML with >30% BM blasts.21 Thus, 241 patients were assigned to the AZA group (75 mg/m2 SC for 7 consecutive days in 28-day cycles) and 247 were assigned to the CCR group (BSC, SC low-dose cytarabine or IC). More than half of the patients were >75 years or older, median BM blasts at baseline were 72%, and 35% of patients had poor-risk cytogenetics (CG). Patients received a median of six cycles of AZA. With the median follow-up of 24.4 months, the median OS was 10.4 vs 6.5 months in the AZA group and CCR group, respectively (HR 0.85, 95% CI 0.69–1.03; p=0.1009). Univariate analysis for OS showed favorable trends for AZA compared with CCR in patients with poor-risk CG and AML with MDS-related changes (AML-MRC). Furthermore, a post-hoc analysis using data from the AZA-AML-001 trial was performed by Döhner et al, applying the 2010 European LeukemiaNet (ELN)-defined adverse karyotype definitions.23 In total, 220 patients (45.4%) had ELN-defined intermediate-I risk (ie, normal) CG (AZA, n=114; CCR, n=106), 111 patients (22.9%) had an intermediate-II risk CG (AZA, n=53; CCR, n=58), and 154 patients (31.8%) had an adverse risk CG (AZA, n=73; CCR, n=81). The “biomarker cohort” included 156 patients who were assessed at study entry for the presence of gene mutations (5-AZA, n=83; CCR, n=73). The median OS was comparable between AZA and CCR among patients with intermediate-I risk (14.1 vs 10.1 months, respectively; HR 0.83, 95% CI 0.60–1.1; p=0.44) and intermediate-II risk (8.9 vs 9.6 months; HR 1.19, 95% CI 0.79–1.8; p=0.78) CG. There was a significant difference in median OS in favor of AZA among patients with adverse risk CG (5.3 vs 2.9 months; HR 0.71, 95% CI 0.51–0.99; p= 0.046), with estimated 1-year survival rates of 29.1% vs 14.7% for patients treated with AZA and CCR, respectively. The patients with complex CG (n=113; 23%) who were treated with AZA had a statistically significant improvement in OS compared with those who received CCR (median OS 4.8 months vs 2.8 months, respectively; HR 0.64, 95% CI 0.43–0.94; p=0.037). There was also a trend for improvement in median OS with AZA for patients with monosomal karyotypes (n=101, 21%) (5.0 vs 2.8 months with CCR; HR 0.65, 95% CI 0.42–1.01; p=0.055). Among the biomarker cohort, in 153 (98.1%) of the 156 patients who had molecular abnormalities, the most frequently mutated genes were DNMT3A (27%), TET2 (25%), IDH2 (23%), TP53 (21%), RUNX1 (18%), NPM1 (16%), NRAS (12%), FLT3 (12% [internal tandem duplications (ITD) 10%, tyrosine kinase domain mutations (TKD) 5%]), ASXL1 (11%), and STAG2 (10%). Within the AZA cohort, the median OS was not significantly different between patients with (n=15) and those without (n=68) TP53 mutations (7.2 vs 12.0 months, respectively; p=0.40) or between patients with mutated (n = 10) and those with wild-type (n=73) NRAS (11.8 vs 8.9 months; p=0.95). However, the median OS in the AZA cohort was reduced in patients with mutated FLT3 (n=9) vs wild-type FLT3 (n=74) (5.4 vs 12.0 months, respectively; p=0.017). The median OS between AZA and CCR treatment cohorts was comparable for patients with or without mutations in any of the genes known to influence DNA methylation (ie, DNMT3A, IDH1, IDH2, and TET1). The patients with TET2 mutations had a slightly worse median OS with AZA compared to CCR (9.6 vs 11.1 months, respectively; p=0.036). The Groupe Francophone des Myelodysplasies (GFM) reported clinical outcomes with AZA in patients with therapy-related MDS (t-MDS) and AML (t-AML).24 Their cohort included 54 patients (t-MDS n=42; t-AML n=12) who received AZA 75 mg/m2 daily for 7 days every 28 days for at least four cycles, with a 5-day schedule also being accepted. The median age at diagnosis was 68.5 years, and 71% of patients had complex CG, with the majority having deletion 5q and chromosome 7 abnormalities. With a median of four cycles of AZA, the overall response rate (ORR) was 39% (CR 15%): 36%, 14%, and 8% of patients were alive at 1, 2, and 3 years, respectively. There was a trend towards inferior OS in patients with chromosome 7 abnormalities.
Following these clinical trials, several retrospective studies were conducted to obtain a real-world perspective. Smith et al completed a retrospective analysis of 487 elderly AML patients who received induction chemotherapy with AZA (n=288) or decitabine (DAC) (n=199).25 The baseline characteristics were comparable between the two treatment arms. The median OS was better with AZA treated compared to DAC (10.1 vs 6.9 months, respectively; p=0.007). The hospitalization rates were lower in the AZA-treated arm (2.9 vs 3.42 per person-year). Thépot et al reviewed retrospective data of 149 AML patients from 34 centers in France who were treated with AZA.26 The median age was 74 years, 26% had adverse risk CG, and 20% had t-AML. The median number of AZA cycles was five, with a median follow-up of 31.5 months. The best response rate was 33%, including 19% of patients who achieved CR, 4% who achieved CR with incomplete count recovery (CRi), and 10% who achieved partial remission (PR). The median time to best response was 145 days. The median OS was 9.4 months, with OS at 1 and 2 years of 38% and 17%, respectively. Adverse risk CG, white blood cell counts >15×109 and Eastern Cooperative Oncology Group (ECOG) performance status >2 were predictors for shorter OS in the univariate and multivariate analysis. The most frequent adverse event was sepsis and febrile neutropenia, with most of these patients requiring hospitalization. The largest retrospective trial was conducted by Pleyer et al from 14 specialized centers in Austria, evaluating 302 elderly AML patients treated with at least one cycle of AZA.27 The median age at diagnosis was 73 years, with 43% being older than 75 years; 19% of patients had unfavorable CG and 7% of patients had t-AML. Forty-six percent of patients received AZA as first-line therapy; a median of four cycles of AZA was given, with 77% of patients having received 7 days as opposed to 5 days of therapy. The ORR was 48%, with 17% of patients achieving CR. The median time to response was 3 months, and the median response duration was 3.4 months. The median OS was 9.6 months, and median progression-free survival (PFS) was 9.1 months. Among responders, the median OS was 16.1 months vs 3.7 months among non-responders. In the relapsed/refractory (RR) setting, Ivanoff et al conducted a retrospective evaluation of 47 AZA-treated patients after at least one course of IC in three different French institutions.28 The median age of the cohort was 63 years, 64% of patients had de novo AML, and 36% of patients had secondary AML (sAML). Twenty-eight percent of patients had unfavorable cytogenetics. The median number of AZA cycles received was four. The ORR was 38% (CR 21%, PR 11%, hematologic improvement [HI] 6%), and the median OS was 9 months. BM blasts >20% retained significance for adverse survival outcome in the multivariate analysis.
The initial AZA-MDS-001 trial demonstrated an impressive median OS compared to conventional therapy in patients with MDS with BM blast counts of 20–30% (considered to have AML by WHO criteria). These results were not reproduced in the AML-AZA-001 trial or in the real-world data, including in patients with higher (≥30%) BM blasts.7,19,26,29–31
Azacitidine Combination Therapies
Considering the lack of significant survival benefit with AZA alone in AML patients with higher (≥ 30%) BM blasts, several AZA combination therapies have been explored in clinical trials to improve outcomes.
Azacitidine in Combination with Histone Deacetylase Inhibitors
Histone deacetylases (HDACs) and DNA methyltransferases (DNMTs) are enzymes that control gene expression through histone acetylation and DNA methylation, respectively.10,32,33 Studies have shown that overexpression of these enzymes can lead to silencing of tumor suppressor genes and tumorigenesis. AZA and HDAC inhibitors (HDACi) have shown synergy in inducing gene re-expression, leading to differentiation and cancer cell apoptosis.34–36 One of the initial combinations explored in this field was AZA plus valproic acid (VPA).37 The combination of VPA and all-trans retinoic acid (ATRA) was also evaluated in patients with MDS and AML, with modest efficacy.38,39 Later, Adès et al published the results of the GFM’s “pick a winner” trial, a phase II trial comparing AZA monotherapy to three drug combinations: 5-AZA with either lenalidomide (AZA + LEN), VPA (AZA + VPA), or idarubicin (AZA + IDA), in patients with high-risk MDS or low blast AML (20–30% blasts).40 Among 322 patients enrolled in the study, AZA was given at a dose of 75 mg/m2 SC daily for 7 days for both monotherapy and combination arms, LEN 10 mg/day orally on days 1–14, VPA 50 mg/kg/day on days 1–7 or 35 mg/kg/day in patients 60 years or older, and idarubicin 10 mg/m2 on day 1 for cycles 1–9. Eighty-one patients were assigned to AZA monotherapy, 80 patients to AZA + VPA, 68 patients to AZA + LEN, and 81 patients to AZA + IDA. Baseline characteristics were well balanced between all arms, except for the lower proportion of AML patients in the AZA + LEN arm. The median age was 74.6 years; 73%, 21%, and 6% of patients had MDS, oligoblastic AML, and chronic myelomonocytic leukemia (CMML), respectively. The CR rate and event-free survival (EFS) were not significantly different between treatment groups. The median OS was 19.7 months, and 23.1, 18.9, 17.5, and 20.1 months with AZA alone, AZA + VPA, AZA + LEN, and AZA + IDA, respectively (Table 1). Compared to AZA monotherapy, hazard ratios were greater than one in all of the combination groups and were not statistically significant. Myelosuppression and infections were more commonly seen in the combination arms compared to AZA alone.
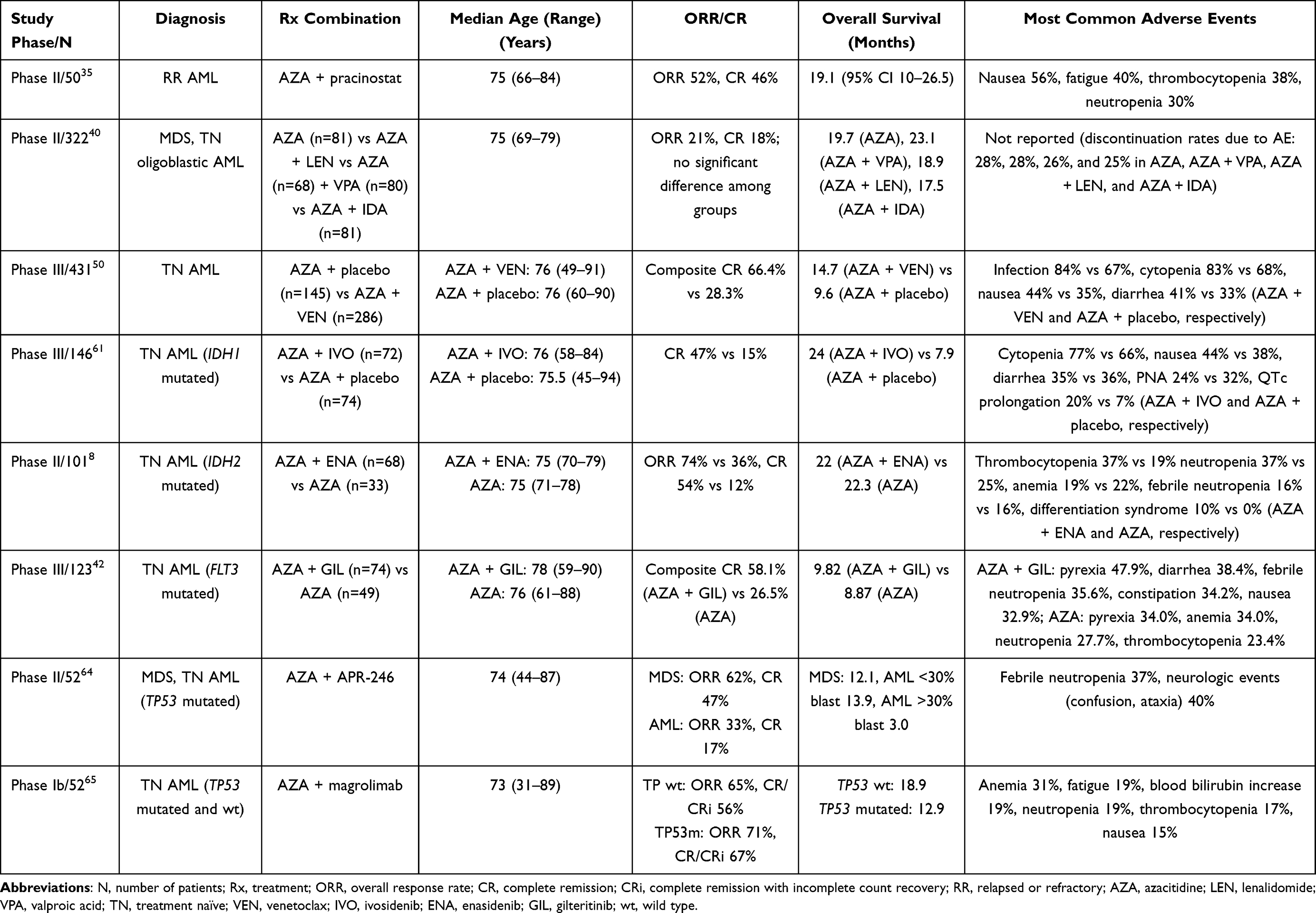 |
Table 1 Selected Trials of Azacitidine Combinations for Treatment of Patients with Acute Myeloid Leukemia |
Pracinostat is the most potent HDACi evaluated in clinical trials. In a phase II study, 50 AML patients with RR disease or AML patients ineligible for IC were evaluated.35 Pracinostat was given at a dose of 60 mg on 3 days/week, and the median number of cycles that patients received was 6.5 (range 1–27 cycles). The ORR was 52% (n=21 CR, n=2 CRi, and n=3 morphologic leukemia-free state [MLFS]). The median duration of response was 11.5 months. No significant difference in ORR was observed between de novo AML and secondary AML. The most common grade 3 or higher treatment-related adverse events were cytopenia (thrombocytopenia 38%, neutropenia 30%) and fatigue (28%) (Table 1). Promising results in a phase II study led to a phase III trial comparing AZA vs AZA + pracinostat. Unfortunately, the study was terminated early by the internal data monitoring committee (IDMC) for lack of efficacy, as it was unlikely to reach its primary endpoint of OS.45
Frequent dose interruption, mainly due to gastrointestinal toxicities, and treatment discontinuation due to the proliferative nature of AML were suggested reasons for the lower efficacy of the AZA plus HDACi combination in clinical trials.
Azacitidine in Combination with Immunomodulators
Thalidomide is an effective modulator of immune functions that can induce T-cell/natural killer cell-mediated tumor cell killing, direct cytotoxicity, and inhibition of cancerous angiogenesis. Thalidomide has been studied in MDS, and although it seems to be effective in certain patients, the majority could not tolerate it owing to its side-effect profile.
Raza et al46 prospectively evaluated AZA (75 mg/m2 SC for 5 days in 28-day cycles) in combination with thalidomide (starting at 50 mg/day and increasing to 100 mg/day) in a total of 40 patients with MDS (n=19), AML (n=16), primary myelofibrosis (n=1), and CMML (n=4). The median age was 72 years. Among the 36 patients who were evaluated for response, the ORR was 58% (CR 17%, HI 42%), and the median OS was 18.5 and 13.2 months in patients with MDS and AML, respectively.
Lenalidomide is approved for the treatment of MDS with or without 5q deletion, and previous phase I data indicated its safety and modest activity in patients with RR AML.47 Pollyea et al evaluated the efficacy AZA + LEN in RR AML.48 In total, 18 patients were eligible for the trial, with a median age of 72 years. Fifty-six percent of the patients had MDS-related changes. The patients were divided into five cohorts, and all cohorts received AZA 75 mg/m2/day for 7 days IV or SC. Cohort 1 received AZA + LEN 5 mg orally daily from day 8 to 21 in a 42-day cycle. Cohorts 2–4 received increasing doses of LEN with the aforementioned schedule at doses of 10, 25, and 50 mg. The median number of cycles to achieve best response was 2.5, with an ORR of 56%. Four patients achieved CR; lower BM blast count was predictive for a better CR rate. The median duration of response was 6.2 months and median OS was 8.2 months. The most common side effect was neutropenic fever. Sequential AZA + LEN was then further explored in a phase II trial by Narayan et al.49 The study included 32 patients with high-risk MDS, de novo AML, and secondary AML (patients with prior immunomodulatory drugs or HMA therapy were included). The patients were considered eligible if they were not immediate candidates for allogeneic stem cell transplant (allo-HSCT) or were unwilling or unable to receive IC. The patients received AZA 75 mg/m2 SC or IV for 7 days, followed by LEN 50 mg orally daily (days 8–28 in a 42-day cycle). Out of the 32 patients who received the treatment, 26 had AML (including sAML [n=18]). The ORR was 25%, with a median duration of response of 4.9 months and median OS of 5 months. Responders to therapy had a significantly longer median OS than patients who were non-responders (9.8 vs 4 months). In the multivariate analysis, blast percentage and prior HMA response were predictive of survival. In terms of adverse events, an early death rate of 12.5% (predominantly secondary to complications of infections) and grade 3 neutropenic fever were the most common adverse effects observed. Several patients needed dose modification of LEN owing to fatigue, thrombocytopenia, rash, and shortness of breath.
AZA in combination with thalidomide or lenalidomide was not further explored owing to modest activity, poor tolerance, and high complication rates.
Azacitidine in Combination with Venetoclax
BCL2 is a family of proteins that plays a crucial role in the intrinsic mitochondrial apoptotic response.50 A high proportion of AML stem cells express BCL2 and are dependent on BCL2 for survival. Moreover, high expression of BCL2 is linked to an inferior response to conventional chemotherapy and poor survival.51 Venetoclax (VEN) is a selective small-molecule BCL2 inhibitor, which has been shown to induce apoptosis in malignant cells that are dependent on BCL2 for survival. VEN as a single agent has demonstrated limited activity in AML.52 The ORR was 19%; an additional 19% of patients demonstrated antileukemic activity not meeting International Working Group (IWG) criteria (partial bone marrow response and incomplete hematologic recovery). DiNardo et al combined VEN with an HMA (AZA or decitabine) in a multicenter, phase Ib, dose escalation trial that included 145 TN elderly AML patients. In the dose expansion cohort, VEN at 400 or 800 mg with HMA was given. The median age of the patients was 74 years and 49% of patients had poor-risk CG. At the median follow-up of 15.1 months, the rate of CR/CRi was 68%, with superior response in patients who received VEN at a dose of 400 mg (CR/CRi rate 73%).53 The high CR/CRi rate resulted in significant improvement in median OS to 17.5 months in elderly AML patients. This led to a phase III, multicenter, randomized, double-blind, placebo controlled trial evaluating the efficacy and safety of AZA + VEN vs AZA alone in elderly patients with TN AML who were ineligible to receive IC.50 VEN + AZA was administered orally, once daily, at a dose of 100 mg on day 1, 200 mg on day 2, and 400 mg on day 3 onwards. In total, 431 patients were included in the intention-to-treat population, with 286 patients in the AZA + VEN group and 145 in the AZA + placebo (control) group. Baseline characteristics were comparable between both groups. Of note, secondary AML patients with prior HMA therapy were excluded. The rate of CR was higher with AZA + VEN than in the control group (36.7% vs 17.9%; p<0.001), as was the rate of composite CR (CR or CRi) (66.4% vs 28.3%; p<0.001). The median time to response was 1.3 vs 2.8 months in the AZA + VEN and control group, respectively. The median OS was 14.7 and 9.6 months with AZA + VEN and in the control group, respectively (HR 0.66, 95% CI 0.52–0.85; p<0.001). Cytopenia(s) and neutropenic fever were more common with AZA + VEN compared to the control group. In subgroup analysis for OS, the HR was not significantly in favor of AZA + VEN in patients with FLT3, TP53, or NPM1 mutated AML, or in AML patients with MDS-related changes. Nevertheless, the combination of AZA + VEN has been a game changer in improving outcomes in elderly patients with AML.
Real-world data on AZA + VEN combination have also shown promising results. Winters et al presented their real-world single-institution experience with AZA + VEN, comparing outcomes with a clinical trial cohort that administered this regimen at the same institution. Thirty-three newly diagnosed AML patients, who were unfit or unwilling to receive induction chemotherapy, were treated.54 The CR/CRi rate was 63.3% for off-trial patients who received treatment and 84.9% for trial patients (p=0.081). The median OS for off-trial patients who received treatment was 381 days vs 880 days for trial patients (p=0.041). Prior exposure to hypomethylating agents was associated with worse outcomes. Of note, the VIALE-A trial excluded sAML patients with prior exposure to HMA.
Cherry et al compared AZA + VEN (n=142) vs IC (n=149) in patients with newly diagnosed AML.55 Response rates were 76.9% vs 70.5% for AZA + VEN vs IC, respectively. The median OS was 884 days (approximately 29 months) for IC vs 483 days (approximately 16 months) for AZA + VEN (p=0.002). In a propensity match cohort, matching for age, biological risk, and transplantation, the median OS for IC was 705 days and was not reached in the AZA + VEN group (p=0.0667). The factors that favored response to AZA + VEN over IC included older age, secondary AML, and RUNX1 mutations. The patients with acute monocytic leukemia had a better response with IC compared to AZA + VEN. The patients with ELN intermediate-risk AML, FLT3-ITD, and RAS mutation had a better response with IC compared to AZA + VEN. De Bellis et al retrospectively evaluated the outcome of 56 newly diagnosed AML patients who received HMA + VEN at eight different centers in Italy.56 Patients received AZA (n=43) or DAC (n=13) in addition to VEN. No differences in terms of response were seen when stratified by age (55–75 vs >75 years), BM blast (20–30% vs >30%), cytogenetic risk group, categories by WHO classification, or type of HMA utilized. The median number of cycles that patients received was seven, and the complete remission rate was 67.9% (CR 53.6% and CRi 14.3%). The median time to CR was two cycles. After median follow-up of 9.9 months, the median OS was 11.3 months and the median PFS was 11.3 months. The major adverse events observed in patients were pneumonia (n=15/56 [27%]), sepsis (n=10/56 [18%]), and febrile neutropenia (n=7/56 [12.5%]).
Antifungal prophylaxis with azoles (voriconazole, posaconazole) is recommended in neutropenic patients receiving AML therapies. When using VEN with strong CYP3A4 inhibitors such as voriconazole and posaconazole, the manufacturer’s recommendations are to ramp up VEN without an azole to prevent tumor lysis syndrome, followed by a 75% reduction in VEN dose with the initiation of azole, which increases the serum concentration of VEN by eight-fold.57
Azacitidine in Combination with FLT3 Inhibitors
FLT3-mutated AML patients who are ineligible to receive IC have inferior outcomes. VEN + AZA combination improved the outcome of a certain subset of AML patients; however, in the pivotal study, AZA + VEN combination compared to AZA alone failed to demonstrate significant improvement in the survival of FLT3-mutated AML patients. Preclinical studies have shown synergistic activity between FLT3 and DNA methyltransferase inhibitor.58 Gilteritinib is an FLT3 inhibitor that has shown superior efficacy in RR FLT3-mutated AML compared to conventional chemotherapy.59 Subsequently, a randomized study was conducted to investigate the efficacy and safety of gilteritinib + AZA vs AZA alone in adults with newly diagnosed FLT3-mutated AML who were ineligible for IC.42 The primary endpoint of the study was OS. At the interim analysis, 123 patients were randomized (gilteritinib + AZA, n=74; AZA, n=49). The median OS was 9.82 and 8.87 months with gilteritinib + AZA vs AZA, respectively (p=0.753). The study was closed based on the protocol-specified boundary for futility. The leukemia group at MD Anderson Cancer Center conducted a phase I/II study in patients with TN and RR FLT3-mutated AML or high-risk MDS/CMML who were unsuitable for IC.60 Twenty-six patients (TN, n=11; RR, n=15) were enrolled. The ORR (CR + CRi + MLFS) was 98% (CR/CRi: 80%) in TN patients and 67% (CR/CRi 27%) in the RR group. In the TN group, the median follow-up was 3.8 months (range 0.5–8 months), none of the patients had relapse, and one patient died as a result of sepsis. In the RR AML group, with a median follow-up of 9.9 months, the median duration of response was 9.0 months and the median OS was 10.5 months. Myelosuppression was the main adverse event, requiring frequent attenuation of AZA and VEN. Longer follow-up and a more tolerable dosing schedule are needed to better evaluate this triplet combination.
Azacitidine in Combination with IDH1/IDH2 Inhibitors
Somatic mutations in the gene encoding isocitrate dehydrogenase 1 or 2 (IDH1/IDH2) occur in 6–19% of patients with AML. Studies have shown that elderly AML patients with normal CG harboring IDH1/2 mutation had inferior outcomes.8,61
Ivosidenib is an oral, small molecule inhibitor of mutant IDH1, which has shown clinical efficacy as a single agent in patients with RR AML. In a phase I study, 258 patients received ivosidenib and had safety outcomes assessed.62 In 179 RR AML patients, treatment-related adverse events of grade 3 or higher that occurred in at least three patients were prolongation of the QT interval (7.8%), differentiation syndrome (3.9%), anemia (2.2%), thrombocytopenia (3.4%), and leukocytosis (1.7%). In the primary efficacy population (125 patients), the rate of CR/CRi was 30.4% (95% CI 22.5–39.3), the rate of CR was 21.6% (95% CI 14.7–29.8), and the ORR was 41.6% (95% CI 32.9–50.8). The median durations of these responses were 8.2 months (95% CI 5.5–12.0), 9.3 months (95% CI 5.6–18.3), and 6.5 months (95% CI 4.6–9.3), respectively. Among patients with complete remission, seven (21%) had no residual detectable IDH1 mutations on digital polymerase chain reaction assay. No pre-existing co-occurring single gene mutation predicted the clinical response or resistance to treatment. Ivosidenib subsequently received FDA approval as a single-agent therapy in RR AML or TN AML patients who are ineligible to receive IC.62 This was followed by a randomized study in AML patients (AZA + ivosidenib vs AZA + placebo [control group]) who were ineligible to receive IC. The primary endpoint was EFS.61 The intention-to-treat population included 146 patients (AZA + ivosidenib [n=72] and control group [n=74]), and EFS was significantly longer in the AZA + ivosidenib group than in the control group (HR for treatment failure, relapse from remission, or death 0.33, 95% CI 0.16–0.69; p=0.002). The probability that a patient would remain event free at 12 months was 37% in the AZA + ivosidenib group and 12% in the control group. The median OS was 24.0 and 7.9 months in the AZA + ivosidenib and control group, respectively (HR 0.44, 95% CI 0.27–0.73; p=0.001). Differentiation syndrome of any grade occurred in 14% and 8% of patients in the AZA + ivosidenib and control group, respectively. This trial demonstrated a significant benefit of AZA + ivosidenib combination compared to AZA alone, and the drug received FDA approval to treat newly diagnosed patients with IDH1-mutated adult AML who are 75 years or older, or who have comorbidities that preclude the use of intensive induction chemotherapy. Another novel, effective and tolerable AZA combination therapy for elderly AML patients with novel target. Now it is up to the treating physician to choose AZA + VEN or AZA + ivosidenib as an upfront treatment strategy in TN elderly AML patients with IDH1 mutation. One school of thought claims that using AZA + VEN upfront gives an option of effective and tolerable second-line therapy in the form of ivosidenib in elderly patients with AML and IDH1 mutation.
Enasidenib is an oral inhibitor of mutant IDH2, which has also demonstrated significant clinical benefit as a single agent in patients with IDH2-mutated RR AML and received FDA approval as a single-agent therapy for RR AML.41 Later, a single-arm, phase Ib and randomized, phase II trial was conducted with enasidenib + AZA vs AZA alone in newly diagnosed IDH2-mutated AML patients. Six patients were enrolled in the phase Ib dose-finding portion of the trial and three each received enasidenib 100 mg and 200 mg with AZA. No dose-limiting toxicities (DLTs) were seen, and enasidenib 100 mg dose was chosen for the phase II portion of the trial. In a phase II trial, 101 patients were randomly assigned to receive enasidenib + AZA (n=68) or AZA only (n=33). The median age of the enrolled patients was 75 years. The ORR was 74% in the enasidenib + AZA group compared to 36% in the AZA-alone group (odds ratio 4.9, 95% CI 2.0–11.9; p=0.0003). The median OS was not significantly different between the AZA + enasidenib (22 months) and AZA (22.3 months) groups (p=0.97). Serious treatment-related adverse events (eg, febrile neutropenia, differentiation syndrome, pneumonia) were reported in 43% of patients in the enasidenib + AZA group and 44% in the AZA-alone group.
Azacitidine Plus Magrolimab/APR-246
While the outcome of TP53-mutated AML continues to be poor in the era of novel therapies,63 some emerging therapies have shown promise. APR-246 (eprenetapopt) is a novel molecule that has been shown to restore the transcriptional activity of mutant p53, leading to apoptosis and death of mutant p53 cells. Therefore, a phase II study was conducted using the combination of eprenetapopt + AZA in patients with TP53-mutated MDS (n=34) and AML (n=18).64 In the MDS cohort, the ORR was 62% (CR 47%), with a median duration of response of 10.4 months. In the AML cohort, the ORR was 33%, including 17% CR. In this study, 73% of responders achieved TP53 next-generation sequencing negativity. The median OS was 12.1 months in MDS, and 13.9 and 3.0 months in AML with <30% and >30% BM blasts, respectively. Subsequently, a randomized study was conducted on AZA + eprenetapopt vs AZA alone in TP53-mutated MDS patients. However, this trial did not meet its primary endpoint of significantly improving CR rates (33.3% vs 22.4%; p=0.13).
Impressive initial results have also been observed with magrolimab (anti-CD47 monoclonal antibody), which is a macrophage immune checkpoint and has been shown to eliminate leukemia stem cells by inducing tumor phagocytosis.65 Preclinical studies have shown that HMA can work synergistically with magrolimab. A phase Ib study of magrolimab + AZA, especially in TP53-mutated high-risk MDS and TN AML (ineligible for IC) patients, found an objective response rate of 69% (CR 45%), with a median OS of 12.9 months.43 Subsequently, a phase III randomized study is being conducted to evaluate the safety/tolerability and efficacy of magrolimab + AZA vs physician’s choice of VEN + AZA or 7+3 chemotherapy in patients with previously untreated TP53-mutated AML.65 In future, we envision more novel combination therapies utilizing an AZA backbone for the management of high-risk AML, especially TP53-mutated AML.
Azacitidine as a Maintenance Therapy in Transplant-Ineligible Patients
In AML, the duration of remission is highly predictive of survival; hence, preventing relapse is the focus of AML treatment. While allo-HSCT remains the potential curative option for patients with high-risk AML, it is not feasible in patients with poor performance status and comorbidities. A phase III randomized double-blind, placebo-controlled study was conducted with an oral formulation of AZA (CC-486; not bioequivalent to IV AZA) as a maintenance therapy in patients with AML who were in first remission after IC.44 A total of 472 patients were enrolled; 238 and 234 patients were randomized to the CC-486 and placebo group, respectively. The median age was 68 years (range 55–86 years). The median OS (24.7 vs 14.8 months; p<0.001) and median relapse-free survival (10.2 vs 4.8 months; p<0.001) were significantly longer with CC-486 than with placebo, respectively. The most common adverse events in both groups were gastrointestinal related. The incidence of grade 3 or 4 adverse events, including neutropenia, was higher in the CC-486 group (41%) compared to the placebo group (24%). This led to FDA approval of oral AZA (CC-486) in the United States, Canada, and European Union for the treatment of adult AML patients in first remission following induction chemotherapy who are ineligible for allo-HSCT.
Most recently, post-hoc analysis of the phase III QUAZAR AML-001 trial demonstrated the benefit of oral AZA in improving survival independent of NPM1 or FLT3 mutational status, cytogenetic risk, or post-IC measurable residual disease status.66 In this pivotal study, 469/472 randomized patients (99.4%) had mutational data; 137 patients (29.2%) had NPM1 mutations, 66 patients (14.1%) had FLT3 mutations (with ITD, TKD, or both), and 30 patients (6.4%) had NPM1 and FLT3-ITD at diagnosis. Among patients with NPM1 mutation, OS and relapse-free survival improved with oral AZA by 37% (HR 0.63, 95% CI 0.41–0.98) and 45% (HR 0.55, 95% CI 0.35–0.84), respectively, vs placebo. Among patients with FLT3 mutation, oral AZA improved OS and relapse-free survival by 37% (HR 0.63, 95% CI 0.35–1.12) and 49% (HR 0.51, 95% CI 0.27–0.95), respectively, vs placebo. The data suggest that oral AZA maintenance is an effective maintenance strategy to prolong survival in high-risk as well as favorable-risk AML patients who are ineligible for consolidation allo-HSCT.
Conclusion
Historically, the outcome of AML patients who are ineligible to receive intensive chemotherapy was poor owing to the lack of effectiveness of low-intensity therapies. AZA or decitabine had been the mainstay of treatment for these patients to prolong survival. With better understanding of AML disease biology, the development of novel mutation-specific combination therapies has yielded improved outcomes. AZA has been the backbone of these combination therapies (eg, AZA + venetoclax, AZA + ivosidenib, AZA + magrolimab), with a paradigm shift in the management of AML, especially in patients who are not candidates for intensive therapies. However, a certain subset of AML patients continues to have inferior outcome in the era of these novel combinations, such as those with AML post-HMA progression, TP53-mutated AML, and FLT3-mutated AML (who are ineligible for intensive chemotherapies). Effective treatment combinations with or without AZA are needed to improve the outcome of these high-risk patients.
Disclosure
TB received a Mayo Clinic Cancer Center Research Support Grant (grant number P30 CA015083). The authors report no other conflicts of interest in this work.
References
1. Döhner H, Weisdorf DJ, Bloomfield CD. Acute myeloid leukemia. N Engl J Med. 2015;373(12):1136–1152. doi:10.1056/NEJMra1406184
2. Badar T, Patel KP, Thompson PA, et al. Detectable FLT3-ITD or RAS mutation at the time of transformation from MDS to AML predicts for very poor outcomes. Leuk Res. 2015;39(12):1367–1374. doi:10.1016/j.leukres.2015.10.005
3. Badar T, Szabo A, Sallman D, et al. Interrogation of molecular profiles can help in differentiating between MDS and AML with MDS-related changes. Leuk Lymphoma. 2020;61(6):1418–1427. doi:10.1080/10428194.2020.1719089
4. Daver N, Wei AH, Pollyea DA, Fathi AT, Vyas P, DiNardo CD. New directions for emerging therapies in acute myeloid leukemia: the next chapter. Blood Cancer J. 2020;10(10):107. doi:10.1038/s41408-020-00376-1
5. Kantarjian H, Kadia T, DiNardo C, et al. Acute myeloid leukemia: current progress and future directions. Blood Cancer J. 2021;11(2):41. doi:10.1038/s41408-021-00425-3
6. Badar T, Ravandi F. Relapsed acute myeloid leukemia: need for innovative treatment strategies to improve outcome. Clin Lymphoma Myeloma Leuk. 2015;15:S104–S108. doi:10.1016/j.clml.2015.03.012
7. Zeidan AM, Wang R, Wang X, et al. Clinical outcomes of older patients with AML receiving hypomethylating agents: a large population-based study in the United States. Blood Adv. 2020;4(10):2192–2201. doi:10.1182/bloodadvances.2020001779
8. DiNardo CD, Schuh AC, Stein EM, et al. Enasidenib plus azacitidine versus azacitidine alone in patients with newly diagnosed, mutant-IDH2 acute myeloid leukaemia (AG221-AML-005): a single-arm, phase 1b and randomised, phase 2 trial. Lancet Oncol. 2021;22(11):1597–1608. doi:10.1016/S1470-2045(21)00494-0
9. Andreozzi F, Massaro F, Wittnebel S, Spilleboudt C, Lewalle P, Salaroli A. New perspectives in treating acute myeloid leukemia: driving towards a patient-tailored strategy. Int J Mol Sci. 2022;23:7. doi:10.3390/ijms23073887
10. Badar T, Atallah E. Do histone deacytelase inhibitors and azacitidine combination hold potential as an effective treatment for high/very-high risk myelodysplastic syndromes? Expert Opin Investig Drugs. 2021;30(6):665–673. doi:10.1080/13543784.2021.1915986
11. Keating GM. Azacitidine. Drugs. 2012;72(8):1111–1136. doi:10.2165/11209430-000000000-00000
12. Bernstein I, Byun HM, Mohrbacher A, et al. A Phase I biological study of azacitidine (Vidaza™) to determine the optimal dose to inhibit DNA methylation. Epigenetics. 2010;5(8):750–757. doi:10.4161/epi.5.8.13105
13. Cruijsen M, Lübbert M, Wijermans P, Huls G. Clinical results of hypomethylating agents in AML treatment. J Clin Med. 2014;4(1):1–17. doi:10.3390/jcm4010001
14. Leone G, Teofili L, Voso MT, Lübbert M. DNA methylation and demethylating drugs in myelodysplastic syndromes and secondary leukemias. Haematologica. 2002;87(12):1324–1341.
15. Marcucci G, Silverman L, Eller M, Lintz L, Beach CL. Bioavailability of azacitidine subcutaneous versus intravenous in patients with the myelodysplastic syndromes. J Clin Pharmacol. 2005;45(5):597–602. doi:10.1177/0091270004271947
16. Laille E, Goel S, Mita AC, et al. A phase I study in patients with solid or hematologic malignancies of the dose proportionality of subcutaneous Azacitidine and its pharmacokinetics in patients with severe renal impairment. Pharmacotherapy. 2014;34(5):440–451. doi:10.1002/phar.1371
17. Silverman LR, McKenzie DR, Peterson BL, et al. Further analysis of trials with azacitidine in patients with myelodysplastic syndrome: studies 8421, 8921, and 9221 by the Cancer and Leukemia Group B. J Clin Oncol. 2006;24(24):3895–3903. doi:10.1200/JCO.2005.05.4346
18. Kantarjian H, Issa JPJ, Rosenfeld CS, et al. Decitabine improves patient outcomes in myelodysplastic syndromes: results of a Phase III randomized study. Cancer. 2006;106(8):1794–1803. doi:10.1002/cncr.21792
19. Schuh AC, Döhner H, Pleyer L, Seymour JF, Fenaux P, Dombret H. Azacitidine in adult patients with acute myeloid leukemia. Crit Rev Oncol Hematol. 2017;116:159–177. doi:10.1016/j.critrevonc.2017.05.010
20. Fenaux P, Mufti GJ, Hellstrom-Lindberg E, et al. Efficacy of azacitidine compared with that of conventional care regimens in the treatment of higher-risk myelodysplastic syndromes: a randomised, open-label, phase III study. Lancet Oncol. 2009;10(3):223–232. doi:10.1016/S1470-2045(09)70003-8
21. Dombret H, Seymour JF, Butrym A, et al. International phase 3 study of azacitidine vs conventional care regimens in older patients with newly diagnosed AML with >30% blasts. Blood. 2015;126(3):291–299. doi:10.1182/blood-2015-01-621664
22. Fenaux P, Mufti GJ, Hellström-Lindberg E, et al. Azacitidine prolongs overall survival compared with conventional care regimens in elderly patients with low bone marrow blast count acute myeloid leukemia. J Clin Oncol. 2010;28(4):562–569. doi:10.1200/JCO.2009.23.8329
23. Döhner H, Estey E, Grimwade D, et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 2017;129(4):424–447. doi:10.1182/blood-2016-08-733196
24. Bally C, Thépot S, Quesnel B, et al. Azacitidine in the treatment of therapy related myelodysplastic syndrome and acute myeloid leukemia (tMDS/AML): a report on 54 patients by the Groupe Francophone Des Myelodysplasies (GFM). Leuk Res. 2013;37(6):637–640. doi:10.1016/j.leukres.2013.02.014
25. Smith BD, Beach CL, Mahmoud D, Weber L, Henk HJ. Survival and hospitalization among patients with acute myeloid leukemia treated with azacitidine or decitabine in a large managed care population: a real-world, retrospective, claims-based, comparative analysis. Exp Hematol Oncol. 2014;3(1):10. doi:10.1186/2162-3619-3-10
26. Thépot S, Itzykson R, Seegers V, et al. Azacitidine in untreated acute myeloid leukemia: a report on 149 patients. Am J Hematol. 2014;89(4):410–416. doi:10.1002/ajh.23654
27. Pleyer L, Burgstaller S, Girschikofsky M, et al. Azacitidine in 302 patients with WHO-defined acute myeloid leukemia: results from the Austrian Azacitidine Registry of the AGMT-Study Group. Ann Hematol. 2014;93(11):1825–1838. doi:10.1007/s00277-014-2126-9
28. Ivanoff S, Gruson B, Chantepie SP, et al. 5-Azacytidine treatment for relapsed or refractory acute myeloid leukemia after intensive chemotherapy. Am J Hematol. 2013;88(7):601–605. doi:10.1002/ajh.23464
29. Pleyer L, Döhner H, Dombret H, et al. Azacitidine for front-line therapy of patients with AML: reproducible efficacy established by direct comparison of international phase 3 trial data with registry data from the Austrian Azacitidine Registry of the AGMT study group. Int J Mol Sci. 2017;18:2. doi:10.3390/ijms18020415
30. Maurillo L, Venditti A, Spagnoli A, et al. Azacitidine for the treatment of patients with acute myeloid leukemia: report of 82 patients enrolled in an Italian Compassionate Program. Cancer. 2012;118(4):1014–1022. doi:10.1002/cncr.26354
31. Itzykson R, Thépot S, Berthon C, et al. Azacitidine for the treatment of relapsed and refractory AML in older patients. Leuk Res. 2015;39(2):124–130. doi:10.1016/j.leukres.2014.11.009
32. de Ruijter AJ, van Gennip AH, Caron HN, Kemp S, van Kuilenburg AB. Histone deacetylases (HDACs): characterization of the classical HDAC family. Biochem J. 2003;370(Pt 3):737–749. doi:10.1042/bj20021321
33. Johnstone RW. Histone-deacetylase inhibitors: novel drugs for the treatment of cancer. Nat Rev Drug Discov. 2002;1(4):287–299. doi:10.1038/nrd772
34. Yang H, Hoshino K, Sanchez-Gonzalez B, Kantarjian H, Garcia-Manero G. Antileukemia activity of the combination of 5-aza-2’-deoxycytidine with valproic acid. Leuk Res. 2005;29(7):739–748. doi:10.1016/j.leukres.2004.11.022
35. Garcia-Manero G, Abaza Y, Takahashi K, et al. Pracinostat plus azacitidine in older patients with newly diagnosed acute myeloid leukemia: results of a phase 2 study. Blood Adv. 2019;3(4):508–518. doi:10.1182/bloodadvances.2018027409
36. Badar T, Guru Murthy GS, Runaas L, et al. Phase I study of pracinostat in combination with gemtuzumab ozogamicin (PraGO) in patients with relapsed/refractory Acute Myeloid Leukemia (AML). Blood. 2019;134(Supplement_1):5068. doi:10.1182/blood-2019-123237
37. Phiel CJ, Zhang F, Huang EY, Guenther MG, Lazar MA, Klein PS. Histone deacetylase is a direct target of valproic acid, a potent anticonvulsant, mood stabilizer, and teratogen. J Biol Chem. 2001;276(39):36734–36741. doi:10.1074/jbc.M101287200
38. Kuendgen A, Strupp C, Aivado M, et al. Treatment of myelodysplastic syndromes with valproic acid alone or in combination with all-trans retinoic acid. Blood. 2004;104(5):1266–1269. doi:10.1182/blood-2003-12-4333
39. Kuendgen A, Knipp S, Fox F, et al. Results of a phase 2 study of valproic acid alone or in combination with all-trans retinoic acid in 75 patients with myelodysplastic syndrome and relapsed or refractory acute myeloid leukemia. Ann Hematol. 2005;84(Suppl 1):61–66. doi:10.1007/s00277-005-0026-8
40. Adès L, Duployez N, Guerci-Bresler A, et al. A randomised Phase II study of azacitidine (AZA) alone or with Lenalidomide (LEN), Valproic acid (VPA) or Idarubicin (IDA) in higher-Risk MDS or low blast AML: GFM’s “pick a winner” trial, with the impact of somatic mutations. Br J Haematol. 2022;198(3):535–544. doi:10.1111/bjh.18193
41. Pollyea DA, Tallman MS, de Botton S, et al. Enasidenib, an inhibitor of mutant IDH2 proteins, induces durable remissions in older patients with newly diagnosed acute myeloid leukemia. Leukemia. 2019;33(11):2575–2584. doi:10.1038/s41375-019-0472-2
42. Wang ES, Montesinos P, Minden MD, et al. Phase 3 trial of gilteritinib plus azacitidine vs azacitidine for newly diagnosed FLT3 mut+ AML ineligible for intensive chemotherapy. Blood. 2022;140:1845–1857. doi:10.1182/blood.2021014586
43. Sallman DA, Asch AS, Al Malki MM, et al. The first-in-class anti-CD47 antibody magrolimab (5F9) in combination with azacitidine is effective in MDS and AML patients: ongoing phase 1b results. Blood. 2019;134(Supplement_1):569. doi:10.1182/blood-2019-126271
44. Wei AH, Döhner H, Pocock C, et al. Oral azacitidine maintenance therapy for acute myeloid leukemia in first remission. N Engl J Med. 2020;383(26):2526–2537. doi:10.1056/NEJMoa2004444
45. Helsinn.com. Helsinn Group and MEI Pharma Discontinue the Phase 3 Study with Pracinostat in AML after Completing Interim Analysis. Available from: https://helsinn.com/helsinn-group-and-mei-pharma-discontinue-the-phase-3-study-with-pracinostat-in-aml-after-completing-interim-analysis/. Accessed December 16, 2022.
46. Raza A, Mehdi M, Mumtaz M, Ali F, Lascher S, Galili N. Combination of 5-azacytidine and thalidomide for the treatment of myelodysplastic syndromes and acute myeloid leukemia. Cancer. 2008;113(7):1596–1604. doi:10.1002/cncr.23789
47. Blum W, Klisovic RB, Becker H, et al. Dose escalation of lenalidomide in relapsed or refractory acute leukemias. J Clin Oncol. 2010;28(33):4919–4925. doi:10.1200/JCO.2010.30.3339
48. Pollyea DA, Kohrt HE, Gallegos L, et al. Safety, efficacy and biological predictors of response to sequential azacitidine and lenalidomide for elderly patients with acute myeloid leukemia. Leukemia. 2012;26(5):893–901. doi:10.1038/leu.2011.294
49. Narayan R, Garcia JS, Percival M-EM, et al. Sequential azacitidine plus lenalidomide in previously treated elderly patients with acute myeloid leukemia and higher risk myelodysplastic syndrome. Leuk Lymphoma. 2016;57(3):609–615. doi:10.3109/10428194.2015.1091930
50. DiNardo CD, Jonas BA, Pullarkat V, et al. Azacitidine and venetoclax in previously untreated acute myeloid leukemia. N Engl J Med. 2020;383(7):617–629. doi:10.1056/NEJMoa2012971
51. Konopleva M, Contractor R, Tsao T, et al. Mechanisms of apoptosis sensitivity and resistance to the BH3 mimetic ABT-737 in acute myeloid leukemia. Cancer Cell. 2006;10(5):375–388. doi:10.1016/j.ccr.2006.10.006
52. Konopleva M, Pollyea DA, Potluri J, et al. Efficacy and biological correlates of response in a phase II study of venetoclax monotherapy in patients with acute myelogenous leukemia. Cancer Discov. 2016;6(10):1106–1117. doi:10.1158/2159-8290.CD-16-0313
53. DiNardo CD, Pratz KW, Letai A, et al. Safety and preliminary efficacy of venetoclax with decitabine or azacitidine in elderly patients with previously untreated acute myeloid leukaemia: a non-randomised, open-label, phase 1b study. Lancet Oncol. 2018;19(2):216–228. doi:10.1016/S1470-2045(18)30010-X
54. Winters AC, Gutman JA, Purev E, et al. Real-world experience of venetoclax with azacitidine for untreated patients with acute myeloid leukemia. Blood Adv. 2019;3(20):2911–2919. doi:10.1182/bloodadvances.2019000243
55. Cherry EM, Abbott D, Amaya M, et al. Venetoclax and azacitidine compared with induction chemotherapy for newly diagnosed patients with acute myeloid leukemia. Blood Adv. 2021;5(24):5565–5573. doi:10.1182/bloodadvances.2021005538
56. De Bellis E, Imbergamo S, Candoni A, et al. Venetoclax in combination with hypomethylating agents in previously untreated patients with acute myeloid leukemia ineligible for intensive treatment: a real-life multicenter experience. Leuk Res. 2022;114:106803. doi:10.1016/j.leukres.2022.106803
57. Lindsay J, Teh BW, Micklethwaite K, Slavin M. Azole antifungals and new targeted therapies for hematological malignancy. Curr Opin Infect Dis. 2019;32(6):538–545. doi:10.1097/QCO.0000000000000611
58. Chang E, Ganguly S, Rajkhowa T, Gocke CD, Levis M, Konig H. The combination of FLT3 and DNA methyltransferase inhibition is synergistically cytotoxic to FLT3/ITD acute myeloid leukemia cells. Leukemia. 2016;30(5):1025–1032. doi:10.1038/leu.2015.346
59. Perl AE, Martinelli G, Cortes JE, et al. Gilteritinib or chemotherapy for relapsed or refractory FLT3mutated AML. doi:10.1056/NEJMoa1902688
60. Short NJ, DiNardo CD, Daver N, et al. A triplet combination of azacitidine, venetoclax and gilteritinib for patients with FLT3mutated acute myeloid leukemia: results from a phase I/II study. doi:10.1182/blood-2021-153571
61. Montesinos P, Recher C, Vives S, et al. Ivosidenib and azacitidine in IDH1-mutated acute myeloid leukemia. N Engl J Med. 2022;386(16):1519–1531. doi:10.1056/NEJMoa2117344
62. DiNardo CD, Stein EM, de Botton S, et al. Durable remissions with ivosidenib in IDH1-mutated relapsed or refractory AML. N Engl J Med. 2018;378(25):2386–2398. doi: 10.1056/NEJMoa1716984
63. Badar T, Atallah E, Shallis RM, et al. Outcomes of TP53-mutated AML with evolving frontline therapies: impact of allogeneic stem cell transplantation on survival. Am J Hematol. 2022;97(7):E232–e5. doi:10.1002/ajh.26546
64. Cluzeau T, Sebert M, Rahmé R, et al. Eprenetapopt plus azacitidine in TP53-mutated myelodysplastic syndromes and acute myeloid leukemia: a phase II study by the Groupe Francophone des Myélodysplasies (GFM). J Clin Oncol. 2021;39(14):1575–1583. doi:10.1200/JCO.20.02342
65. Daver N, Vyas P, Chao M, et al. A phase 3, randomized, open-label study evaluating the safety and efficacy of magrolimab in combination with azacitidine in previously untreated patients with TP53-mutant acute myeloid leukemia. Blood. 2021;138:3426. doi:10.1182/blood-2021-145208
66. Döhner H, Wei AH, Roboz GJ, et al. Prognostic impact of NPM1 and FLT3 mutations in patients with AML in first remission treated with oral azacitidine. Blood. 2022;140(15):1674–1685. doi:10.1182/blood.2022016293
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.