")
Back to Journals » Cancer Management and Research » Volume 14
Clinical Significance of Peripheral Blood Lymphocyte Subtypes and Cytokines in Patients with Hepatocellular Carcinoma Treated with TACE
Authors Wang H, Zhang G, Fan W, Wu Y, Zhang J, Xue M, Zhao Y , Yao W, Li J
Received 3 October 2021
Accepted for publication 24 December 2021
Published 5 February 2022 Volume 2022:14 Pages 451—464
DOI https://doi.org/10.2147/CMAR.S342527
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kattesh Katti
Hongyu Wang,1,* Guixiong Zhang,1,* Wenzhe Fan,1 Yanqin Wu,1 Jiang Zhang,2 Miao Xue,1 Yue Zhao,1 Wang Yao,1 Jiaping Li1
1Department of Interventional Oncology, The First Affiliated Hospital of Sun Yat-Sen University, Guangzhou, 510080, People’s Republic of China; 2Department of Clinical Laboratory, The first Affiliated Hospital of Sun Yat-Sen University, Guangzhou, 510080, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiaping Li
Department of Interventional Oncology, The First Affiliated Hospital of Sun Yat-Sen University, Guangzhou, 510080, People’s Republic of China
, Tel +86-20-13352890908
, Fax +86-20-87755766
, Email [email protected]
Purpose: To examine the clinical significance of circulating lymphocyte subtypes and cytokines in patients with hepatocellular carcinoma (HCC) undergoing transarterial chemoembolization (TACE).
Patients and Methods: We enrolled 53 patients and assessed lymphocyte subsets (CD4+ T cells, CD8+ T cells, CD4+/CD8+ cell ratio, natural killer cells, and regulatory T cells) and cytokines (interleukin [IL]-2, IL-4, IL-6, IL-10, and interferon [IFN]-γ) on the day before TACE, and 1 day and 4– 8 weeks thereafter. The correlation between baseline inflammatory markers and IL-6, the differences between clinical subgroups, and the prognostic baseline inflammatory values and changes therein were analyzed.
Results: We found that baseline IL-6 was positively correlated with IL-10 and IFN-γ. Univariate analysis revealed that patients with higher baseline IL-6, IL-10, and IFN-γ levels had worse liver function and greater tumor burden, suggesting a poor prognosis. Multivariate analysis showed that higher baseline IFN-γ levels were associated with a shorter time to tumor progression (hazard ratio [HR] = 1.912; 95% confidence interval [CI] = 1.013– 3.607; p = 0.045), and higher IL-10 levels were associated with poor overall survival (HR = 2.576; 95% CI = 1.237– 5.364; p = 0.011). Baseline lymphocyte subtypes and changes therein did not have any significant association with prognosis.
Conclusion: This study confirmed the association between inflammation and poor prognosis. The prognostic significance of IFN-γ was different from previous studies, while the prognostic significance of lymphocyte subtypes remains to be verified.
Keywords: hepatocellular carcinoma, TACE, IFN-γ, cytokines, lymphocyte subtypes
Introduction
Hepatocellular carcinoma (HCC) is the most common primary liver cancer and is the sixth leading cause of cancer and third leading cause of cancer-related mortality.1 Hepatitis B virus (HBV) is the most common cause of HCC in China. HBV infection disrupts the balance between lymphocyte subsets by changing their proportions in the peripheral blood, suggesting the presence of inflammation in the body.2,3 According to the Barcelona Clinic Liver Cancer (BCLC) staging system, transarterial chemoembolization (TACE) is the standard treatment option for patients with intermediate-stage, unresectable HCC (BCLC stage B). TACE is also available as an alternative to, or as part of, combination therapy for patients with early or advanced HCC.4
In HCC patients with chronic inflammation, various immune effector cells and cytokines play a critical role in promoting or impeding cancer progression.5,6 Previous studies have suggested that CD8+ T cells, CD4+ T cells, and natural killer (NK) cells are associated with improved survival in many cancers, including liver cancer.7–10 In contrast, regulatory T (Treg) cells inhibit the secretion of interferon (IFN)-γ and upregulate inhibitory checkpoint molecules, leading to immune system dysfunction and, often, poor prognosis.11,12 Cytokines are important mediators of the link between inflammation and cancer; their balance regulates the inflammatory cell infiltrates and antitumor immunity.13 Generally, T helper (Th) 1 cytokines (interleukin [IL]-1β, IL-2, IL-12, tumor necrosis factor [TNF]-α, and IFN-γ) are associated with a good prognosis in patients with HCC; whereas Th2 cytokines (IL-4, IL-5, and IL-10) are associated with tumor growth and metastasis.14 However, most previous studies are based on analyses of tumor-infiltrating lymphocytes. Additionally, most studies of peripheral immune indicators have been retrospective or have had a small sample size or a single outcome variable.
Several studies have reported the prognostic value of peripheral blood lymphocyte subtypes and cytokines for outcomes of patients with HCC, including surgery, local ablation, radiation therapy, and TACE.10,15–17 However, there is a lack of high-quality clinical studies that comprehensively analyze the inflammatory markers during TACE for HCC. Several studies demonstrated that higher baseline serum IL-6 levels correlated with a larger tumor size and poor prognosis in HCC patients.18,19 Our previous study demonstrated that post-treatment IL-6 levels, rather than the pretreatment levels or dynamic changes of IL-6 levels, predicted the outcomes of HCC patients treated with TACE.20 Based on the study, we comprehensively analyzed the clinical significance of various circulating lymphocyte subtypes (CD4+ T cells, CD8+ T cells, CD4+/CD8+ cell ratio, NK cells, and Treg cells) and cytokines (IL-2, IL-4, IL-6, IL-10, and IFN-γ) in HCC patients during TACE, including their correlation with IL-6, differences in their levels among subgroups, and their ability to predict prognosis.
Materials and Methods
Patients
The protocol for this prospective, observational study was approved by the Ethics Committee of the First Affiliated Hospital of Sun Yat-sen University. This study was conducted in accordance with the Declaration of Helsinki, and written informed consent was obtained from all participants. All participants were diagnosed with HCC based on histology or elevated α-fetoprotein (AFP) levels (>200 ng/mL) and suggestive findings on computed tomography (CT)/magnetic resonance imaging. We enrolled patients aged 18–75 years who would receive TACE as recommended by a multidisciplinary panel, including newly diagnosed HCC, or residual active lesions after TACE or ablation, or recurrence after surgery, and had an Eastern Co-operative Group performance status of 0–1, Child–Pugh class A or B, and life expectancy >3 months. Patients were excluded if they had a coexisting immune disease, hematologic disorders, bleeding events, severe hypersplenism (platelet count <50 × 109/L) or received systemic chemotherapy; symptoms or signs of infection or sepsis; diffuse-type HCC; portal vein thrombosis and complete occlusion of main portal vein without adequate collateral circulation around the occluded portal vein; severe underlying cardiac or renal disease.
TACE and Follow-Up
TACE was performed by senior interventional radiologists, using a selective or superselective injection of a mixture of 20–40 mg doxorubicin in 5–20 mL lipiodol and a 350–560-µm gelatin sponge for embolization. Patients underwent abdominal contrast–enhanced CT scan 4–8 weeks after TACE, which was repeated every 1–3 months depending on the clinical condition.
Tumor response was evaluated using the modified Response Evaluation Criteria in Solid Tumors and designated as complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD). Patients with CR and PR were grouped as responders and all others were grouped as non-responders. Subsequent treatments, including TACE, ablation, and systemic treatment, were performed after a consensus decision made by a multidisciplinary team.
Data Collection
Clinical characteristics of the patients recorded at baseline (1 day before TACE) included age, sex, liver cirrhosis, previous treatments, tumor control status, and tumor characteristics (such as size, number, margins, vascular invasion, and metastasis). Laboratory data recorded at baseline and at day 1 and 4–8 weeks after TACE included lymphocyte subtypes and cytokines.
Fresh blood samples, collected at three time points, were delivered to our clinical laboratory within 4 h of collection. We performed flow cytometry analysis using BD MultitestTM TBNK reagent (for CD3, CD4, CD8, NK, and Treg cells) to evaluate the proportion of lymphocyte subtypes. A multiplex biometric enzyme-linked immunosorbent assay using antibodies against IL-2, IL-4, IL-6, IL-10, and IFN-γ was used to detect five cytokines (Hangzhou Clongene Biotech Co. Ltd., Hangzhou, China). All immunoassay procedures were performed in accordance with the manufacturer’s protocols.
Statistical Analysis
Continuous variables are presented as the mean ± standard deviation, or as the median (lower quartile–upper quartile). Categorical variables are presented as numbers and percentages. The levels of inflammatory markers before and after treatment were compared using a paired sample t-test or Wilcoxon test, and the differences between the subgroups were compared using an independent sample t-test, analysis of variance, Mann–Whitney U-test, or Kruskal–Wallis test. The associations between different inflammatory markers were analyzed using Spearman correlation.
Time to progression (TTP) was defined as the interval between TACE and disease progression or last observation. Overall survival (OS) was defined as the interval between TACE and death or last observation. Univariate and multivariate Cox regression (backward logistic regression [LR]) were used for survival analysis. The Cox proportional-hazards regression model was used to evaluate prognostic factors and calculate hazard ratios (HRs) and 95% confidence intervals (CIs). The survival curve was plotted using the Kaplan–Meier method. Because there are no recognized cut-off values of inflammatory markers for survival analyses, lymphocyte subtypes were divided into three subgroups based on quartiles, and cytokines were divided into high or low subgroups based on medians. In addition, patients were divided into three subgroups based on the degree of change (lower quartile, middle quartile, and upper quartile) in immune indicators.
The data were analyzed using SPSS Statistics software (version 25.0; IBM Corp., Armonk, NY, USA) and GraphPad Prism 8 (GraphPad Software, Inc., San Diego, CA, USA). Two-sided p-values <0.05 were considered statistically significant.
Results
Patients
We enrolled 53 patients between April and October 2018. The mean age was 54.9 ± 11.2 years. All patients had HBV infection, 44 had liver cirrhosis on CT imaging, 11 had BCLC stage A, 12 had BCLC stage B, and 30 had BCLC stage C (Table 1). At enrollment, 26 patients had been treated, including 2 who had undergone surgical resection and 24 who had received 1–5 sessions of TACE and/or ablation; 9 responders and 17 non-responders were evaluated. Thirty-one patients agreed to have inflammatory markers measured on the first day after TACE, and 20 patients agreed to have inflammatory markers measured at 4–8 weeks (Figure 1). Two patients with BCLC stage A underwent surgical resection, and four were lost to follow-up within 3 months. At the last follow-up in October 2020, TTP and OS were analyzed in 51 and 47 patients, respectively.
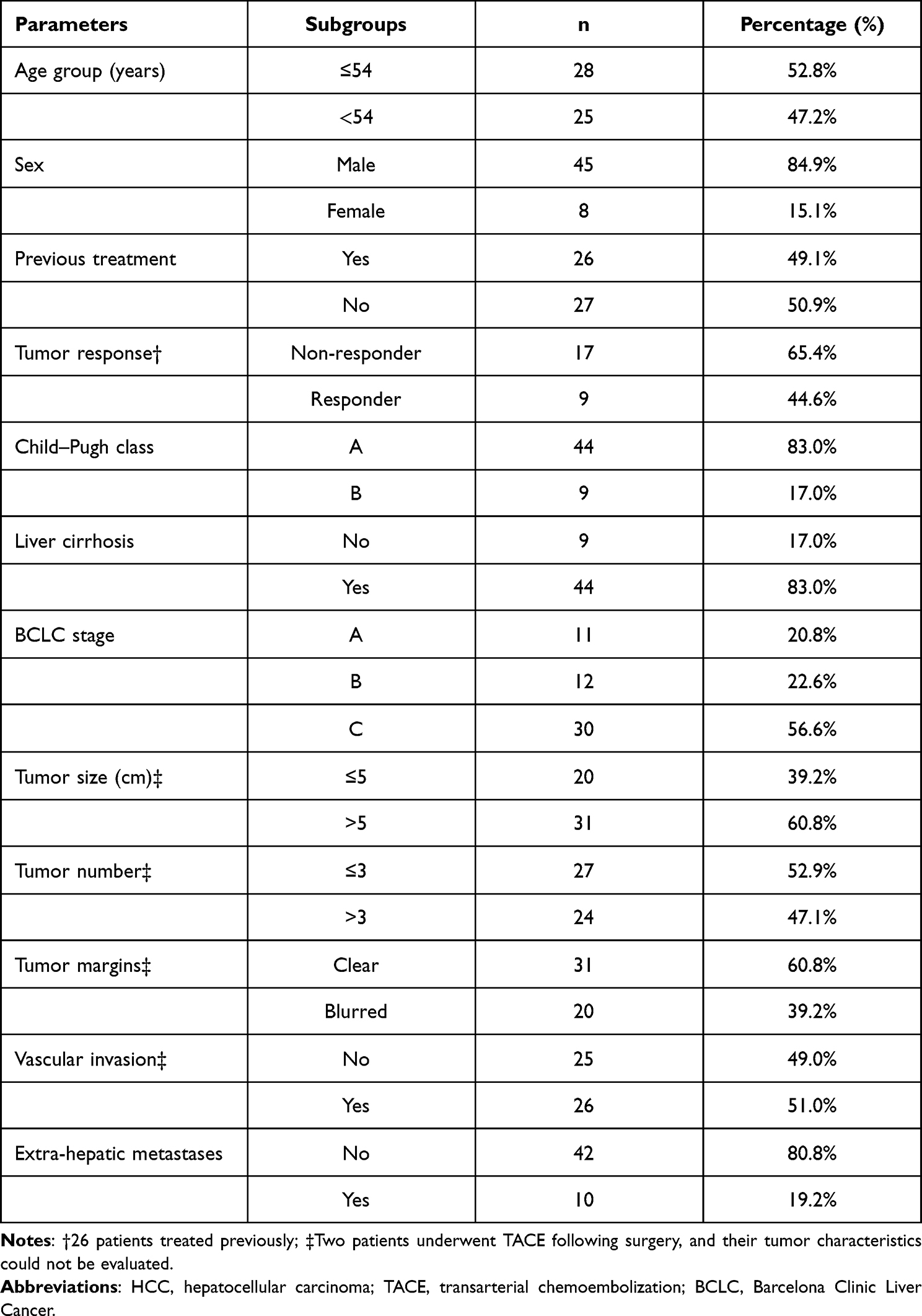 |
Table 1 Baseline Characteristics of HCC Patients Treated with TACE |
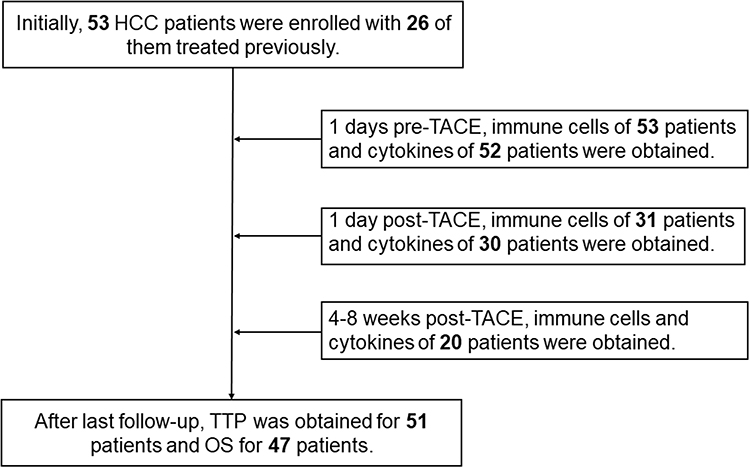 |
Figure 1 Patient enrollment and follow-up data. Notes: Blood samples were available for 53, 31, and 20 patients at the three time points, respectively. The cytokine assay failed for one patient at the first two time points. |
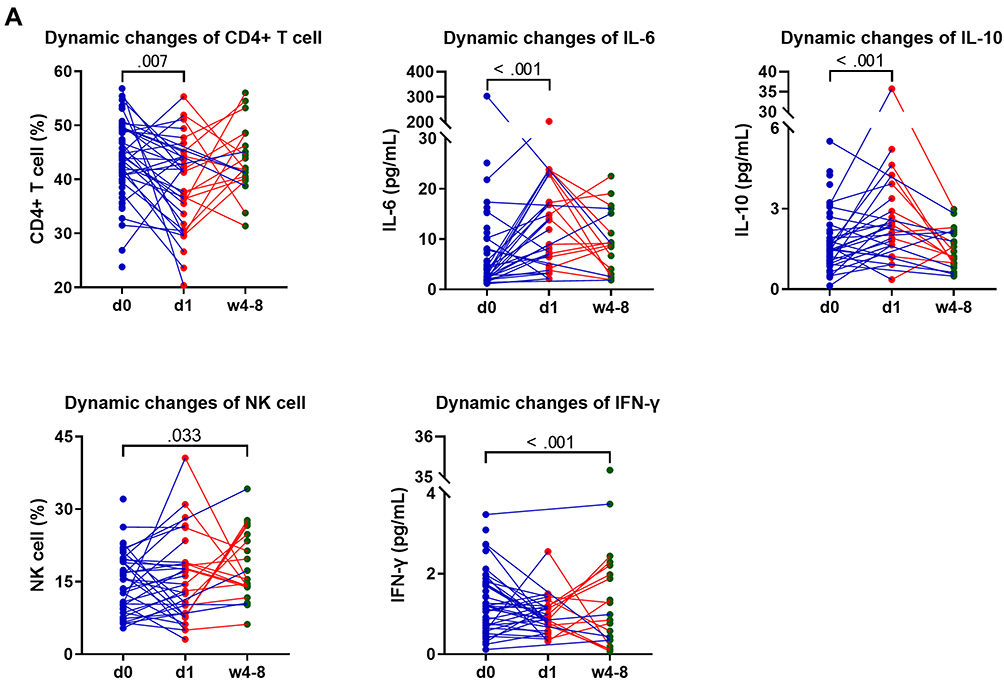 |
Figure 2 Continued. |
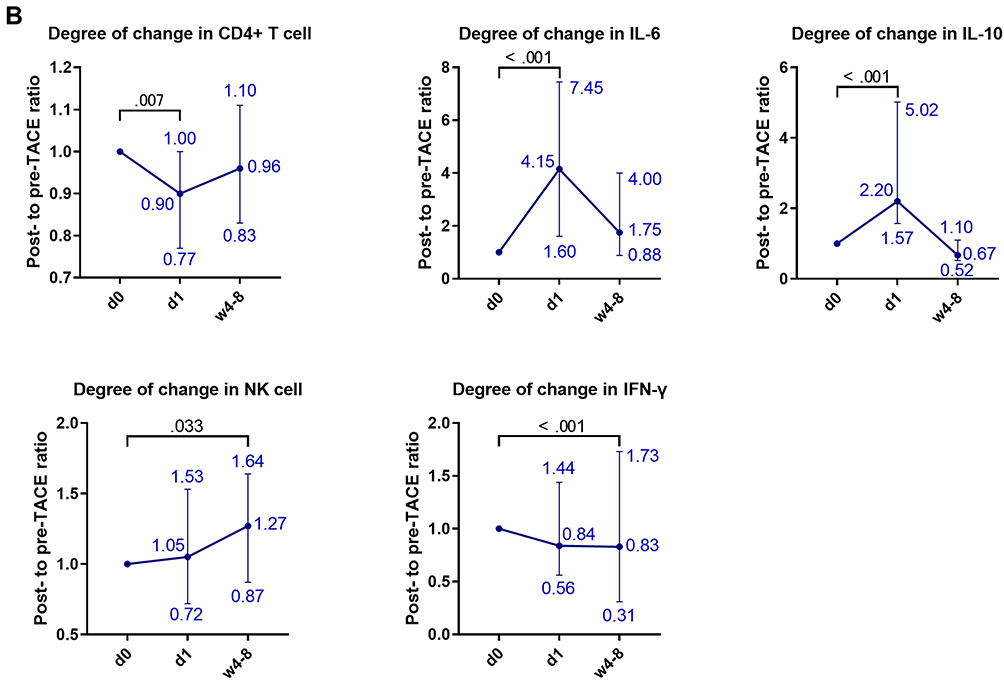 |
Figure 2 Dynamic changes in inflammatory markers before and after TACE. Notes: (A) Changes in lymphocyte subtypes and cytokine values. (B) Changes in the ratio of post- to pre-TACE lymphocyte subtypes and cytokines. The preoperative level was taken as the baseline and has a value of 1. The ratios of changes are presented as median values (lower quartile–upper quartile).Abbreviations: d0, 1 day pre-TACE; d1, 1 day post-TACE; w4–8, 4–8 weeks post-TACE. |
Changes in Inflammatory Markers
The proportions of CD4+ T, CD 8+ T, and Treg cells were relatively evenly distributed (mean ± standard deviation), whereas the concentrations other inflammatory indicators varied greatly (median [lower quartile–upper quartile]) (Table 2). One day after TACE, early changes included decreased CD4+ T cells, as well as increased IL-6 and IL-10 levels (p < 0.05); they recovered 4–8 weeks after TACE (p > 0.05). Four to 8 weeks after TACE, late changes included increased NK cells and decreased IFN-γ (p < 0.05) (Figure 2A). The degree of change is shown in Figure 2B.
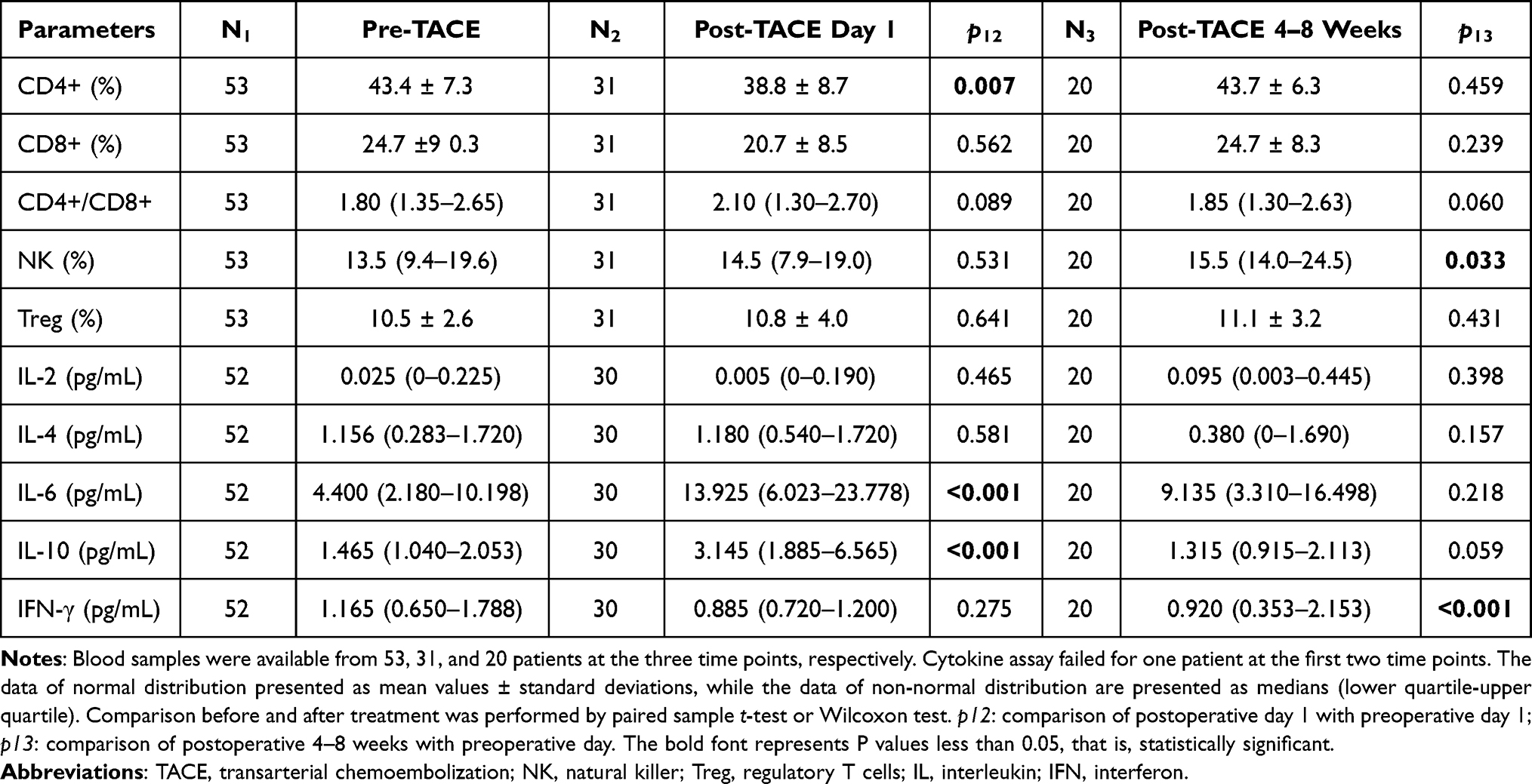 |
Table 2 Pre- and Post-TACE Levels of Lymphocyte Subtypes and Cytokines |
Correlations of Baseline Lymphocyte Subtypes and Cytokines with IL-6, and Their Differences Between Clinical Subgroups
We analyzed the correlations of lymphocyte subtypes and cytokines with IL-6. Baseline IL-6 levels were positively correlated with IL-2, IL-10, and IFN-γ levels (Spearman correlation coefficient = 0.329, p = 0.017; 0.456, p = 0.001; 0.349, p = 0.011, respectively) (Figure 3). However, IL-6 was not correlated with lymphocyte subtypes.
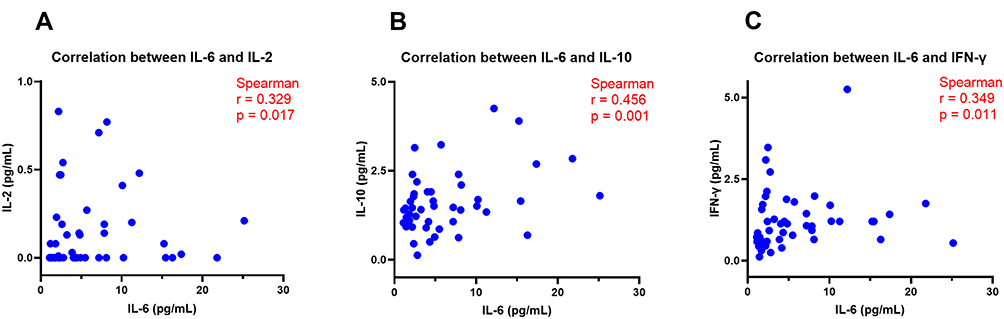 |
Figure 3 Correlations of IL-6 with (A) IL-2, (B) IL-10, and (C) IFN-γ. Abbreviations: IL, interleukin; IFN, interferon. |
We compared the baseline levels of these inflammatory markers between the subgroups. IL-6 differed between subgroups based on Child–Pugh class, BCLC stage, tumor margins, vascular invasion, and extrahepatic metastases (p <0.05), and was associated with poor liver function and high tumor burden (Supplementary Table 1; p-values only, data not shown). IL-10 was associated with BCLC stage, vascular invasion, and extrahepatic metastases (p < 0.05). CD4+ T cells were lower in Child–Pugh class A patients (p = 0.019). CD8+ T cells were lower and the CD4+/CD8+ ratio was higher in patients who had received previous treatment compared to other patients (p < 0.05). However, there were no differences in the lymphocyte subtypes or cytokines between responders and non-responders at baseline (p > 0.05). In addition, Treg cells, IL-4, and IFN-γ did not differ between the subgroups (p > 0.05).
Associations of Baseline Inflammatory Markers with TTP and OS
The median duration of follow-up was 28.7 (95% CI: 28.3–29.0) months, median TTP was 4.2 (95% CI: 2.8–5.7) months, and median survival was 17.60 (95% CI: 12.7–22.6) months. In univariate survival analysis for TTP, the factors with significant results (p < 0.05) included age, tumor response, tumor size, number of tumors, tumor margins, vascular invasion, extra-hepatic metastases, and the levels of IL-2, IL-6, IL-10, and IFN-γ (Figure 4A and Table 3). Factors identified as significant in the univariate analysis were studied using multivariate Cox analysis. There were statistically significant differences in the number of tumors (HR = 7.919; 95% CI = 1.831–34.244; p = 0.006), extra-hepatic metastases (HR = 5.091; 95% CI = 0.975–26.579; p = 0.054), tumor response (HR = 0.204; 95% CI = 0.049–0.854; p = 0.030), and IFN-γ (HR = 5.177; 95% CI = 1.326–20.207; p = 0.018).
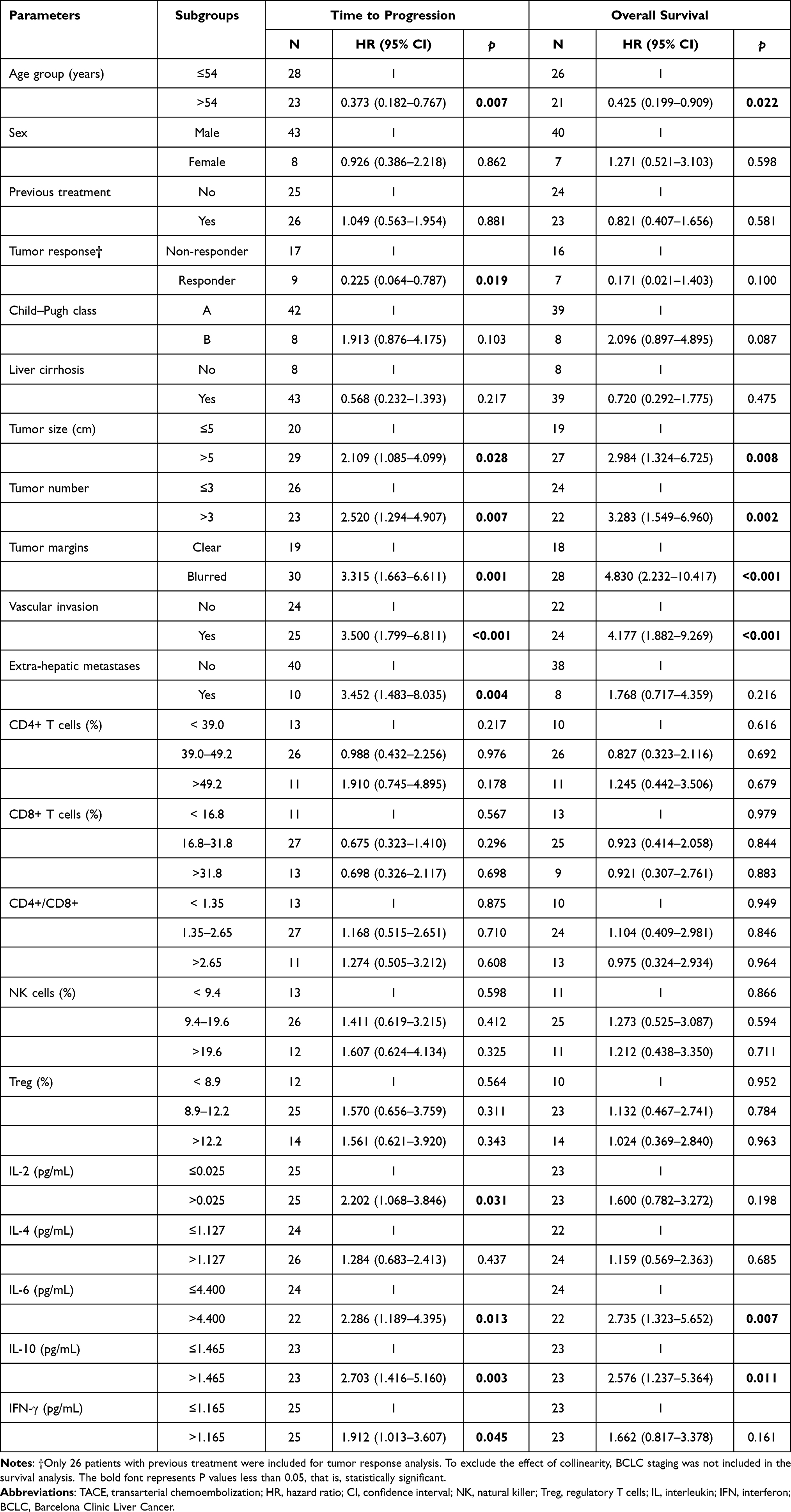 |
Table 3 Univariate Analysis for Factors Associated with Time to Progression and Overall Survival After TACE for HCC |
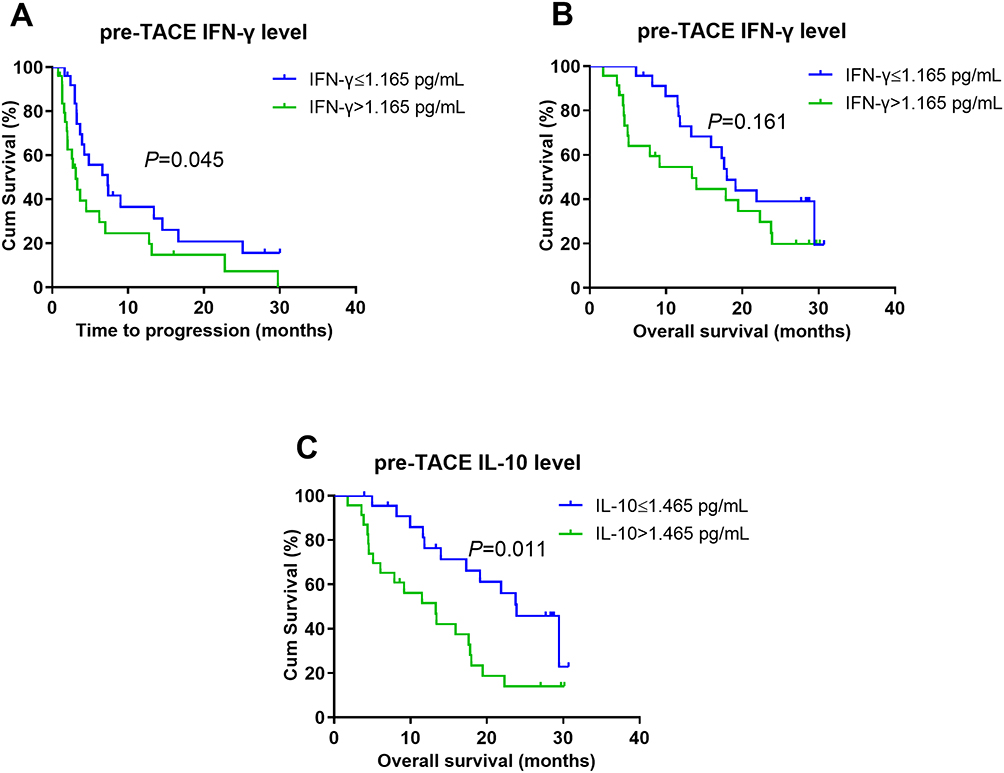 |
Figure 4 Kaplan–Meier curves for baseline IFN-γ and IL-10. (A) Kaplan–Meier curves of TTP for baseline IFN-γ. (B) Kaplan–Meier curves of OS for baseline IFN-γ. (C) Kaplan–Meier curves of OS for baseline IL-10. Abbreviations: IL, interleukin; IFN, interferon; TTP, time to tumor progression; OS, overall survival. |
In univariate survival analysis for OS, the factors with significant results included age, BCLC stage, tumor size, number of tumors, tumor margins, vascular invasion, and levels of IL-6 and IL-10 (Table 3). Although there was no difference in survival by IFN-γ level (HR = 1.662; 95% CI = 0.817–3.378; p = 0.161), high IFN-γ showed a tendency toward an association with poor survival (Figure 4B). In multivariate Cox analysis, independent prognostic factors included the number of tumors (HR = 3.328; 95% CI = 1.552–7.136; p = 0.002), vascular invasion (HR = 3.980; 95% CI = 1.765–8.973; p = 0.001), and IL-10 levels (HR = 1.889; 95% CI = 0.896–3.983; p = 0.095) (Figure 4C).
Survival Analysis for Changes in Inflammatory Markers
The changes in IL-6, IL-10, and CD4+ T cells after 1 day, as well as in NK cells and IFN after 4–8 weeks of TACE, were significantly different, suggesting potential prognostic value. Patients were divided into three subgroups based on the degree of change for survival analysis (Supplementary Tables 2 and 3). There was a difference in OS between the subgroups with CD4+ T cells in the middle quartile (change ratios: 0.77–1.00) and upper quartile (ratio >1.00) (Log rank p = 0.014) (Figure 5A). However, there was no difference in OS between the subgroups with CD4+ T cells in the lower (ratio <0.77) and upper (ratio >1.00) quartiles, suggesting that CD4+ T cells changes had a non-linear association with prognosis. OS was significantly longer in patients with changes in NK in the middle quartile (ratio: 0.87–1.64) compared to the lower quartile (ratio <0.87) (Log rank p = 0.005) (Figure 5B). However, longest OS did not coincide with patients in the upper quartile of NK cells (ratio >1.64), suggesting a non-linear association of NK cells with prognosis. Changes in IL-6, IL-10, or IFN-γ levels did not affect prognosis (p > 0.05).
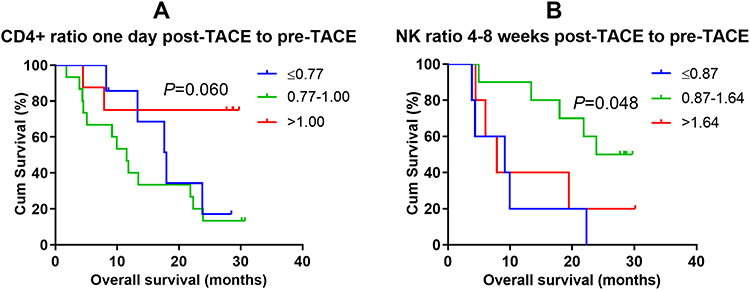 |
Figure 5 Kaplan–Meier curves of OS for changes in (A) CD4+ cells and (B) NK cells. Notes: Patients in the upper quartile of CD4+ cell changes (ratio >1.00) 1 day after TACE lived longer compared to those in the middle quartile (ratio: 0.77–1.00) (Log rank p = 0.014). Patients in the middle quartile of NK cell changes (ratio: 0.87–1.64) 4–8 weeks after TACE lived longer compared to those in the lower quartile (ratio <0.87) (Log rank p = 0.005). Abbreviations: OS, overall survival; NK, natural killer. |
Discussion
The clinical significance of lymphocyte subtypes and cytokines in peripheral blood has not been evaluated in a high-quality study previously. We performed comprehensive immunoassays to evaluate changes in inflammatory markers in HCC patients during TACE, their associations with IL-6, the differences in these markers among clinical subgroups, and the prognostic value for TTP and OS. Our study results suggest that lymphocyte subtypes do not predict prognosis in HCC patients; thus, the clinical significance is not clear. However, analysis of cytokines revealed that higher baseline IFN-γ levels were associated with a poor prognosis, different from previous studies. The immunological mechanisms deserve further study.
Lymphocytes are the most important cells involved in maintaining an immunological balance by suppressing the immune response.21 A study of surgical treatment for HCC showed lower NK cells and higher CD8+ cells in 715 newly treated HCC patients compared to 100 healthy controls. After 1 year, the CD8+ cells levels were reduced, while the CD19+ and NK cells were increased. The recurrence and survival rates were 33.71% and 83.64%, respectively.15 Similarly, another study showed reduced peripheral blood CD4+ cells and NK cells as well as increased CD8+ cells in HCC patients compared to healthy people. The CD4+ cells, CD4+/CD8+ ratio, and NK cells dramatically increased and CD8+ cells significantly decreased 4 weeks after TACE.17 Additionally, Ren et al22 found that lymphocyte subtypes were associated with tumor burden, and the proportion of CD4+ cells and the CD4+/CD8+ ratio were significantly increased at 1–2 weeks and 3–5 weeks after TACE in HCC patients; CD8+ cells were significantly decreased at 1–2 weeks and slightly increased at 3–5 weeks after TACE; Treg cells continuously decreased 1–2 weeks and 3–5 weeks after TACE; and NK cells remained unchanged after TACE.15,22 Another study partially explained the prognostic significance of the changes of lymphocyte subtypes, in terms of an increase in the peripheral blood activation of CD4+ and NK cells, a decrease in Treg cells, an increase in serum IFN-γ after ablation with irreversible electroporation, and an increase in tumor CD8+ cell infiltration.23
However, we did not observe significant differences in lymphocyte subtypes among most clinical subgroups or significant changes during treatment. These discrepancies may have three explanations. First, the follow-up interval was different between our study and previous studies. Previous studies evaluated changes in lymphocyte subtypes 10 days to 1 year after treatment. Different lymphocyte subtypes and cytokines show different patterns of change after treatment.24 A previous study found that inflammatory cytokine changes peak at day 3 after TACE and resolve by day 60.25 Therefore, our follow-up interval may not have been appropriate. Second, different treatments have different effects on immunity. In a study that compared TACE and cryoablation, the changes in CD4+ cells, CD8+ cells, CD4+/CD8+ ratio, and NK cells were similar between monotherapy and combination groups. However, the effects on lymphocyte subtypes were more significant in the combination group compared to the monotherapy group, and were associated with the prognosis.17 In a study of radiotherapy for HCC, the levels of CD3+ cells, CD4+ cells, CD8+ cells, CD19+ cells, and NK cells decreased significantly after 10 days and gradually recovered after 2 months, which was different from previous studies.10 Numerous studies have demonstrated the potential of local ablation to improve anti-tumor immunity.26 However, the abscopal effects of TACE have not been reported yet, and we speculate that the immune-activating effects of TACE may be weaker than those of local ablation. Additionally, previous studies differed in measuring the proportions or counts of lymphocyte subtypes and their statistical methods.
Higher levels of CD4+ cells after TACE were significantly associated with longer OS, possibly because tissue necrosis stimulates CD4 + cells to produce IFN-γ, thereby promoting the destruction of tumor cells by cytotoxic CD8+ cells.27,28 To ensure true-positive results, we divided patients into three subgroups based on the quartile of lymphocyte subtype, rather than receiver operating characteristic (ROC) curve analysis, to determine the optimal cut-off value. However, none of the lymphocyte subtypes were able to predict TTP or OS. In chronic inflammation, lymphocyte function is often impaired,29 which may affect the prognosis more than the number of lymphocytes. Several studies have found that lymphocyte functional phenotypes, such as CD8+ central memory T cells, activated NKp30+NK cells, and CD4+PD1+ cells, are more effective predictors of prognosis after ablation or radiotherapy of HCC than the frequency of total CD4+ and CD8+ T cells.16,30 The results for the lymphocyte subtypes in this prospective study were not significant, different from previous studies mentioned above, possibly due to the heterogeneity of the patient population and differences in study protocols and testing techniques. Given these differences, caution is needed when interpreting the results.
Inflammatory cytokines are a broad category of signaling molecules that reflect concomitant inflammation and may be an adverse prognostic factor.18 In previous reports, an elevated baseline IL-6 level was associated with poor prognosis of HCC patients treated with TACE or sorafenib.19 A possible explanation for this is that high levels of IL-6 lead to increased levels of Treg cells, and elevated programmed cell death protein-1 (PD-1) expression in CD4+, CD8+, Treg, and Th17 cells.31 Additionally, we did not observe correlations between IL-6 and lymphocyte subtypes, suggesting the need to investigate the functional phenotypes of lymphocytes. IL-6 was closely related to liver function, tumor characteristics, and poor prognosis in univariate survival analysis, consistent with previous reports. Furthermore, IL-6 was positively correlated with IL-2, IL-10, and IFN-γ levels, indicating that these levels increased during the inflammatory response.
To avoid the collinear effect between strong prognostic factors, we used a backward regression method. The multivariate survival analysis showed that IL-10 and IFN-γ were independent prognostic factors for OS and PD, respectively. IL-10, an anti-inflammatory factor, suppresses immune function by blocking the synthesis of pro-inflammatory cytokines (such as IL-1, IL-6, IFN-γ, and TNF-α) and inhibiting the expression of cell surface molecules involved in antigen presentation and co-stimulation. In previous studies, serum IL-10 levels were higher in cancer patients compared to healthy controls, and were also involved in the progression of chronic inflammation, which leads to HCC; also, higher serum IL-10 levels were associated with a worse prognosis.32,33 Another study found that serum levels of IL-10 before TACE predicted the local tumor response and OS.24 Our results are consistent with the findings of these studies.
Importantly, in contrast to previous studies, high IFN-γ levels were associated with short TTP and OS in our study. IFN-γ is an antitumor cytokine secreted by antigen-specific T cells.34 Higher baseline IFN-γ levels are associated with early tumor stage and small tumor size in HCC patients, and with delayed tumor recurrence after curative treatment.35 A recent study found that an increased IFN-γ/IL-10 ratio, without increased IL-6 levels, was associated with prolonged survival,36 indicating that IFN-γ may exert anti-tumor activity only in the non-inflammatory state. Inflammatory conditions may lead to the overactivation of T cells, and elevated IFN-γ induces increased expression of co-suppressive receptors, such as cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4), PD-1 and programmed cell death protein-L1 (PD-L1) in the tumor microenvironment through a feedback mechanism.29,34,37,38 This may explain the positive correlation between IFN and IL6, and the poor prognosis. Therefore, the dual biological effects of IFN-γ in antitumor immunity are related to the complex inflammatory microenvironment. The discrepancies in results among previous studies need further investigation.
TACE induces hypoxia and aggravates local inflammation, leading to the secretion of a variety of inflammatory cytokines that contribute to malignant progression.39,40 In contrast, TACE has also been shown to induce inflammation and immunogenic cell death with cytokine production, which may favor immune activation and presentation of tumor-specific antigens.41,42 Therefore, we analyzed the prognostic value of changes in lymphocyte subtypes or cytokines after TACE. However, there are no accepted cut-off values for lymphocyte changes. Therefore, our patients were divided into three subgroups based on the degree of change in lymphocytes. The changes in CD4+ and NK cells did not show differences between the upper and lower quartiles, suggesting a non-linear relationship with the prognosis. Due to the small sample size, the clinical significance of our results is limited. We are conducting a study on lymphocyte functional phenotypes to explore their prognostic value for HCC; the results will be published in the future.
In our study, there were early changes in IL-6 and IL-10 and late changes in IFN-γ. However, the magnitude of these changes varied greatly within each individual. A dynamic study of cytokines in HCC patients found that IL-6 levels peak on the third day after TACE and gradually decrease by the seventh day, suggesting that the early changes in pro-inflammatory cytokines may be related to acute inflammation and acute liver injury.43 There were also late changes in the IL-4 and IL-10 levels,43 which is in contrast to our results. In a previous study, there were no changes in IL-6 and IL-10 levels 24 h after microwave ablation of HCC, followed by more than a two-fold increase at 15 days, and recovery at 1 month. In addition, there was a slight increase in IFN levels at 15 days and 1 month after ablation.44 Another study found a significant increase in IFN-γ and IL-2, and decrease in IL-4 and IL-10 levels 3 months after ultrasound ablation for liver cancer.45 In summary, the changes in cytokines differ among studies, and whether these changes are related to tumor immunity remain uncertain. We also did not observe an effect of changes in IL-6, IL-10, and IFN-γ on prognosis. Future studies should include more patients to allow dynamic observations at multiple time points.
Our study had several limitations. First, the sample size was small and there were complex baseline characteristics and subsequent treatments. Therefore, our results should be interpreted with caution. Second, inflammatory markers were measured only three times, within a short period, for each patient. Many patients refused to repeat the measurements after TACE, which prevented a comprehensive analysis of the patterns of changes. Future studies should attempt to overcome these limitations.
Conclusions
In conclusion, patients in a high inflammatory state (with raised IL-6 and IL-10 levels) have a poor prognosis. In contrast to previous studies, we found that higher baseline IFN-γ levels were associated with a poor prognosis, possibly due to the IFN-γ-induced immune tolerance seen in a chronic inflammation microenvironment. The prognostic value of lymphocyte subtypes in the context of TACE treatment of HCC patients also requires further study.
Data Sharing Statement
Data used and generated in this work are available from the corresponding author upon reasonable request.
Funding
This work was supported by the major scientific and technological project of Guangdong Province (No. 2020B0101130016), Guangzhou key R & D project, China (202103000021) and National Natural Science Foundation of China (NSFC) (No. 81971719).
Disclosure
All authors have no conflicts of interest to disclose.
References
1. Raoul JL, Forner A, Bolondi L, Cheung TT, Kloeckner R, de Baere T. Updated use of TACE for hepatocellular carcinoma treatment: how and when to use it based on clinical evidence. Cancer Treat Rev. 2019;72:28–36.
2. Song B, Zhen S, Meng F. T cell inflammation profile after surgical resection may predict tumor recurrence in HBV-related hepatocellular carcinoma. Int Immunopharmacol. 2016;41:35–41.
3. Nandi M, Pal S, Ghosh S, et al. CD8CD28 T cells: key cytotoxic players impacting disease pathogenesis in chronic HBV infection. Clin Sci (Lond). 2019;133:1917–1934.
4. European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L. EASL Clinical Practice Guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69:182–236.
5. Greten FR, Grivennikov SI. Inflammation and cancer: triggers, mechanisms, and consequences. Immunity. 2019;51:27–41.
6. Sachdeva M, Chawla YK, Arora SK. Immunology of hepatocellular carcinoma. World J Hepatol. 2015;7:2080–2090.
7. Guo M, Yuan F, Qi F, et al. Expression and clinical significance of LAG-3, FGL1, PD-L1 and CD8(+)T cells in hepatocellular carcinoma using multiplex quantitative analysis. J Transl Med. 2020;18:306.
8. Gabrielson A, Wu Y, Wang H, et al. Intratumoral CD3 and CD8 T-cell densities associated with relapse-free survival in HCC. Cancer Immunol Res. 2016;4:419–430.
9. Yao W, He JC, Yang Y, et al. The prognostic value of tumor-infiltrating lymphocytes in hepatocellular carcinoma: a systematic review and meta-analysis. Sci Rep. 2017;7:7525.
10. Zhuang Y, Yuan BY, Chen GW, et al. Association between circulating lymphocyte populations and outcome after stereotactic body radiation therapy in patients with hepatocellular carcinoma. Front Oncol. 2019;9:896.
11. Langhans B, Nischalke HD, Kramer B, et al. Role of regulatory T cells and checkpoint inhibition in hepatocellular carcinoma. Cancer Immunol Immunother. 2019;68:2055–2066.
12. Tanaka A, Sakaguchi S. Regulatory T cells in cancer immunotherapy. Cell Res. 2017;27:109–118.
13. Sun B, Karin M. Inflammation and liver tumorigenesis. Front Med. 2013;7:242–254.
14. Budhu A, Forgues M, Ye Q-H, et al. Prediction of venous metastases, recurrence, and prognosis in hepatocellular carcinoma based on a unique immune response signature of the liver microenvironment. Cancer Cell. 2006;10:99.
15. Liu HZ, Deng W, Li JL, et al. Peripheral blood lymphocyte subset levels differ in patients with hepatocellular carcinoma. Oncotarget. 2016;7:77558–77564.
16. Rochigneux P, Nault JC, Mallet F, et al. Dynamic of systemic immunity and its impact on tumor recurrence after radiofrequency ablation of hepatocellular carcinoma. Oncoimmunology. 2019;8:1615818.
17. Huang M, Wang X, Bin H. Effect of transcatheter arterial chemoembolization combined with argon-helium cryosurgery system on the changes of NK cells and T cell subsets in peripheral blood of hepatocellular carcinoma patients. Cell Biochem Biophys. 2015;73:787–792.
18. Loosen SH, Schulze-Hagen M, Leyh C, et al. IL-6 and IL-8 serum levels predict tumor response and overall survival after TACE for primary and secondary hepatic malignancies. Int J Mol Sci. 2018;19:1766.
19. Taniguchi K, Karin M. IL-6 and related cytokines as the critical lynchpins between inflammation and cancer. Semin Immunol. 2014;26:54–74.
20. Wu Y, Fan W, Xue M, et al. Postintervention Interleukin-6 (IL-6) level, rather than the pretreatment or dynamic changes of IL-6, as an early practical marker of tumor response in hepatocellular carcinoma treated with transarterial chemoembolization. Oncologist. 2019;24:e1489–e95.
21. Rehermann B. Pathogenesis of chronic viral hepatitis: differential roles of T cells and NK cells. Nat Med. 2013;19:859–868.
22. Ren Z, Yue Y, Zhang Y, et al. Changes in the peripheral blood treg cell proportion in hepatocellular carcinoma patients after transarterial chemoembolization with microparticles. Front Immunol. 2021;12:624789.
23. Guo X, Du F, Liu Q, et al. Immunological effect of irreversible electroporation on hepatocellular carcinoma. BMC Cancer. 2021;21:443.
24. Qi F, Wang L, Huang P, Zhao Z, Yang B, Xia J. Time-series clustering of cytokine expression after transarterial chemoembolization in patients with hepatocellular carcinoma. Oncol Lett. 2020;19:1175–1186.
25. Jekarl DW, Lee S, Kwon JH, et al. Complex interaction networks of cytokines after transarterial chemotherapy in patients with hepatocellular carcinoma. PLoS One. 2019;14:e0224318.
26. Shao Q, O’Flanagan S, Lam T, et al. Engineering T cell response to cancer antigens by choice of focal therapeutic conditions. Int J Hyperthermia. 2019;36:130–138.
27. Ayaru L, Pereira SP, Alisa A, et al. Unmasking of alpha-fetoprotein-specific CD4(+) T cell responses in hepatocellular carcinoma patients undergoing embolization. J Immunol. 2007;178:1914–1922.
28. Liao Y, Wang B, Huang ZL, et al. Increased circulating Th17 cells after transarterial chemoembolization correlate with improved survival in stage III hepatocellular carcinoma: a prospective study. PLoS One. 2013;8:e60444.
29. Lim CJ, Lee YH, Pan L, et al. Multidimensional analyses reveal distinct immune microenvironment in hepatitis B virus-related hepatocellular carcinoma. Gut. 2019;68:916–927.
30. Agdashian D, ElGindi M, Xie C, et al. The effect of anti-CTLA4 treatment on peripheral and intra-tumoral T cells in patients with hepatocellular carcinoma. Cancer Immunol Immunother. 2019;68:599–608.
31. Rice SJ, Liu X, Zhang J, Jia B, Zheng H, Belani CP. Advanced NSCLC patients with high IL-6 levels have altered peripheral T cell population and signaling. Lung Cancer. 2019;131:58–61.
32. Zhao S, Wu D, Wu P, Wang Z, Serum HJ. IL-10 predicts worse outcome in cancer patients: a meta-analysis. PLoS One. 2015;10:e0139598.
33. El-Emshaty HM, Nasif WA, Mohamed IE. Serum Cytokine of IL-10 and IL-12 in chronic liver disease: the immune and inflammatory response. Dis Markers. 2015;2015:707254.
34. Wilke CM, Wei S, Wang L, Kryczek I, Kao J, Zou W. Dual biological effects of the cytokines interleukin-10 and interferon-gamma. Cancer Immunol Immunother. 2011;60:1529–1541.
35. Lee IC, Huang Y-H, Chau G-Y, et al. Serum interferon gamma level predicts recurrence in hepatocellular carcinoma patients after curative treatments. Int J Cancer. 2013;133:2895–2902.
36. Lee HL, Jang JW, Lee SW, et al. Inflammatory cytokines and change of Th1/Th2 balance as prognostic indicators for hepatocellular carcinoma in patients treated with transarterial chemoembolization. Sci Rep. 2019;9:3260.
37. Liu X, Li M, Wang X, et al. PD-1 TIGIT CD8 T cells are associated with pathogenesis and progression of patients with hepatitis B virus-related hepatocellular carcinoma. Cancer Immunol Immunother. 2019;68:2041–2054.
38. Qian J, Wang C, Wang B, et al. The IFN-γ/PD-L1 axis between T cells and tumor microenvironment: hints for glioma anti-PD-1/PD-L1 therapy. J Neuroinflammation. 2018;15:290.
39. Singh N, Baby D, Rajguru JP, Patil PB, Thakkannavar SS, Pujari VB. Inflammation and cancer. Ann Afr Med. 2019;18:121–126.
40. Gai X, Zhou P, Xu M, Liu Z, Zheng X, Liu Q. Hyperactivation of IL-6/STAT3 pathway leaded to the poor prognosis of post-TACE HCCs by HIF-1α/SNAI1 axis-induced epithelial to mesenchymal transition. J Cancer. 2020;11:570–582.
41. Mizukoshi E, Nakamoto Y, Arai K, et al. Enhancement of tumor-specific T-cell responses by transcatheter arterial embolization with dendritic cell infusion for hepatocellular carcinoma. Int J Cancer. 2010;126:2164–2174.
42. Singh P, Toom S, Avula A, Kumar V, Rahma OE. The immune modulation effect of locoregional therapies and its potential synergy with immunotherapy in hepatocellular carcinoma. J Hepatocell Carcinoma. 2020;7:11–17.
43. Kim MJ, Jang JW, Oh BS, et al. Change in inflammatory cytokine profiles after transarterial chemotherapy in patients with hepatocellular carcinoma. Cytokine. 2013;64:516–522.
44. Zhao J, Li Q, Muktiali M, et al. Effect of microwave ablation treatment of hepatic malignancies on serum cytokine levels. BMC Cancer. 2020;20:812.
45. Ma B, Liu X, Yu Z. The effect of high intensity focused ultrasound on the treatment of liver cancer and patients’ immunity. Cancer Biomark. 2019;24:85–90.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.