")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 10
Clinical Results, Risk Factors, and Future Directions of Ultrasound-Guided Percutaneous Microwave Ablation for Hepatocellular Carcinoma
Authors Dong TT, Wang L, Li M, Yin C, Li YY, Nie F
Received 17 February 2023
Accepted for publication 9 May 2023
Published 15 May 2023 Volume 2023:10 Pages 733—743
DOI https://doi.org/10.2147/JHC.S409011
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ahmed Kaseb
Tian-Tian Dong,1– 3 Lan Wang,1– 3 Ming Li,1– 3 Ci Yin,1– 3 Yuan-Yuan Li,1– 3 Fang Nie1– 3
1Ultrasound Medical Center, Lanzhou University Second Hospital, Lanzhou, 730030, People’s Republic of China; 2Ultrasound Center, Gansu Province Clinical Research Center for Ultrasound, Lanzhou, 730030, People’s Republic of China; 3Intelligence Ultrasound Center, Gansu Province Medical Engineering Research Center for Intelligence Ultrasound, Lanzhou, 730030, People’s Republic of China
Correspondence: Fang Nie, Ultrasound Medical Center, Lanzhou University Second Hospital, Chengguan District, Lanzhou, Gansu, 730030, People’s Republic of China, Tel +86 13993163088, Email [email protected]
Abstract: Hepatocellular carcinoma (HCC) is one of the most common malignancies worldwide, with a relatively poor prognosis, especially for advanced HCC. With the availability of a variety of treatment options, the treatment strategies for HCC have become more and more diversified. Microwave ablation (MWA) has gradually been considered as a viable alternative to surgical resection (SR) owing to its comparable long-term survival, reduced complications, and greater preservation of hepatic parenchyma. However, clinical outcomes, tumor progression, and recurrence of HCC after MWA remain major concerns. Here, after reviewing the current therapeutic options for HCC, we focus on MWA, describing the advantages and challenges of MWA and the clinical results after treatment. We then focused on prognostic factors that influence post-ablation clinical outcomes and briefly presented the strategy of MWA for future clinical treatment.
Keywords: microwave ablation, hepatocellular carcinoma, clinical outcomes, progression
Introduction
Hepatocellular carcinoma (HCC) is the sixth most common cancer and the third-leading cause of cancer-related mortality worldwide and its incidence continues to rise1. Most HCCs usually develop in patients with a history of chronic hepatitis or cirrhosis. Chronic infection with hepatitis B virus (HBV) or hepatitis C virus (HCV) and aflatoxin-contaminated food are major risk factors for HCC.2 During the progression of HCC, there is continuous inflammation and regeneration of hepatocytes, the coexistence of inflammation and cirrhosis makes early diagnosis and treatment of HCC more difficult. This complexity highlights the importance of therapeutic strategy selection for HCC.
With the availability of multiple treatment options, treatment strategies for HCC have become increasingly diverse. Treatment of HCC is based on Barcelona Clinical Liver Cancer (BCLC) staging, including surgical resection (SR), liver transplantation (LT), and locoregional therapy (LRT). Traditionally, SR and LT are the most effective means of treating HCC, but these procedures are only available in <20% of patients due to the occurrence of high complication rates, which directly affects their postoperative morbidity and mortality.3
Current Therapeutic Options
In recent years, a number of different locoregional therapies for HCC have been performed, including transcatheter arterial chemoembolization (TACE), percutaneous ethanol injection, radiofrequency ablation (RFA), microwave ablation (MWA), high intensity-focus ultrasound, and irreversible electroporation (IRE).4
The selection of reasonable treatment method depends on the tumor burden, liver function, and performance status of patient, and the BCLC criteria are recommended for prognostic prediction and treatment allocation.5 Within the BCLC criteria, ablation is offered to patients with very early stage (single small tumors <2 cm) or early stage (Solitary or 2–3 nodules <3 cm) in Child–Turcotte–Pugh (CTP) grade A/B, for patients who are not candidates for SR or LT.6,7 Although not explicitly stated in the criteria, ablation can also be used as a bridging therapy for patients with early stage awaiting transplantation.8
In the past decade, local ablation has gradually become widely used because of its higher safety, lower treatment costs, and less invasive advantages, and has been suggested as the first-line treatment for early HCC, with satisfactory results for its efficiency.9 Studies have reported that for patients with early primary liver cancer, local ablative therapy can achieve the same effect as surgery, and the choice of multiple treatment options can effectively reduce the recurrence rate of liver cancer.10,11
Radiofrequency Ablation
Common clinically used ablation modalities are RFA and MWA. Each of these technologies has its own advantages and weaknesses when applied to treatment of tumors. RFA is considered a viable alternative to SR owing to its comparable long-term survival, reduced morbidity, and greater preservation of hepatic parenchyma. The survival rate of patients with solitary and small HCC (≤5cm) treated by RFA is comparable to that of patients treated by surgery.12,13 However, the overall efficacy of RFA is limited by local carbonized tissues, which increases the impedance and limits the ablation range, accompanied by an obvious “heat sink” effect, that is, the heat in the electrode is lost with the adjacent blood perfusion.14 The necrotic tissue generated by RFA is surrounded by liver tissue with chronic hypoxia at the edge, which easily leads to the invasive growth of residual cancer tissue.15,16 Hypoxic microenvironment contributes to the development of malignant phenotype of HCC, including local progression, recurrence, and chemotherapy resistance.17,18
Microwave Ablation
Technical Advantages
The MWA process is generally under anesthesia, the antenna is directly punctured into the tumor, the polar molecules in the tissue move at high speed under the action of the microwave field, rub each other to generate heat, and when the tumor rapidly heats up to 120°C~150°C (typically 5–20 min), the cancer cell protein is completely denatured and necrotic. The surrounding tissue is little or not damaged, achieving the purpose of “burning” tumor cells.19
The potential advantages of MWA over RFA are described as follows: 1) MWA can achieve higher temperature and faster ablation at 5, 10, and 15 mm in normal tissue without the limitations related to electric impedance compared to RFA;20 2) In tumor locations around large vessels and in highly perfused areas, where radio frequency energy is limited, MWA shows advantages because it is less affected by the “heat sink” effect of blood perfusion and can uniformly inactivate tumor targets close to the blood vessel; 3) In vivo, microwave conduction does not depend on the conductivity of tissues and is less affected by the carbonization and dehydration of tissues;21 4) The volume of ablation zones depends on the power and time used, antenna design, number and orientation of antennae, and microwave frequency, and multiple antennae can be used synchronously to create larger, more conformal and confluent ablation zones. In contrast to RFA current, microwave energy produces faster, hotter, and larger ablation zones in multiple tissue types;22 5) In addition, the updated MWA system is able to create predictable spherical zones of ablation by incorporating field control, thermal control, and wavelength control technology into the system.23
Technical Challenges
However, there are still some challenges in MWA treatment of tumors. Considering the tumor stage, liver function and physical condition, appropriate treatment should be planned after multidisciplinary evaluation.
Reasonable selection of indications to accurately evaluate the feasibility of MWA. Previous MWA was limited to treating small tumors, for patients with BCLC stage 0 and A HCC, MWA could be considered as curative therapy, but with the improvement of antennae and treatment strategies, MWA can also be used as palliative treatment for lesions >5 cm in diameter or multiple lesions with BCLC stage B HCC.24
The success of ablation technology is highly dependent on the experience of the operator, especially for multiple HCCs, the patient’s basic condition and ability to tolerate the operation, the location of lesions, and the duration of the procedure are all considered.
In addition, the routinely used two-dimensional ultrasound (2D US) is limited by its inability to provide adequate information about the spatial positioning of volumetric data for the target tumor and its adjacent structures during planning and guiding.25,26 Furthermore, a post-ablation evaluation of the success of the technique and the next step is planning when the tumor is incomplete ablation. These challenges increase the difficulty of creating a safe margin during ablation to achieve complete ablation, as well as the potential for damage to adjacent organs, especially for junior operators.
Treatment Efficacy
The overall survival (OS) of patients with HCC varies substantially around the world.27 Despite the many treatment options available over decades of research, survival remains poor for patients with HCC, the five-year survival rate is still less than 20% and the prognosis remained poor.28 For patients with HCC treated by thermal ablation, survival rate and tumor recurrence are the leading indicators to assess the prognosis.29 According to the literature, HCC patients treated with MWA have a complete ablation rate of higher than 90%, a complication rate of approximately 10%, a good disease-free survival (DFS) rate and OS rate, and a low local recurrence rate and mortality30–35 (Table 1), and the HCC near the major blood vessels, liver capsules and other organs also have good efficacy.36 Long-term follow-up observations from previous studies have shown that the success rate of MWA for oligonucleotide HCC ≤3cm was 88%–98%, and the 3-year DFS rate was 27%–91.7%.23
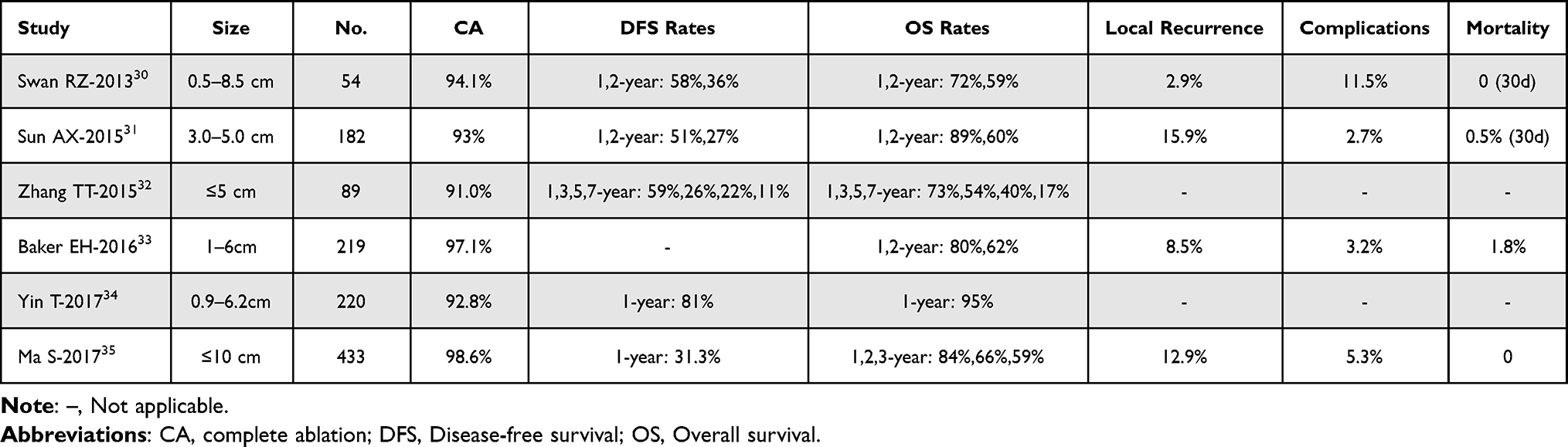 |
Table 1 Complete Ablation, Disease-Free Survival, Overall Survival, Local Recurrence, Complications, and Mortality in Patients with HCC Treated with MWA |
Compared with SR or laparoscopic resection (LR), MWA showed nearly equivalent oncological outcomes after treatment, and the methods of therapy do not affect the prognosis of HCC. Potretzke TA and Liang P reported that the 5-year survival rate of MWA is consistent with that of SR.37 For lesions <3 cm, multicenter studies showed that there was no significant difference in survival and effectiveness between MWA and SR.38 And operative MWA and SR provided nearly equivalent oncological outcomes for single HCC lesions <5 cm and proved to be a less invasive perioperative course39. Studies also showed that in contrast to SR, MWA exhibited less invasive perioperative course,38 shorter operation time, less amount of blood loss, and fewer complications.40,41 However, compared to SR, patients with HCC undergoing thermal ablation have a better long-term survival rate and a higher rate of tumor recurrence24,39,42–48 (Table 2).
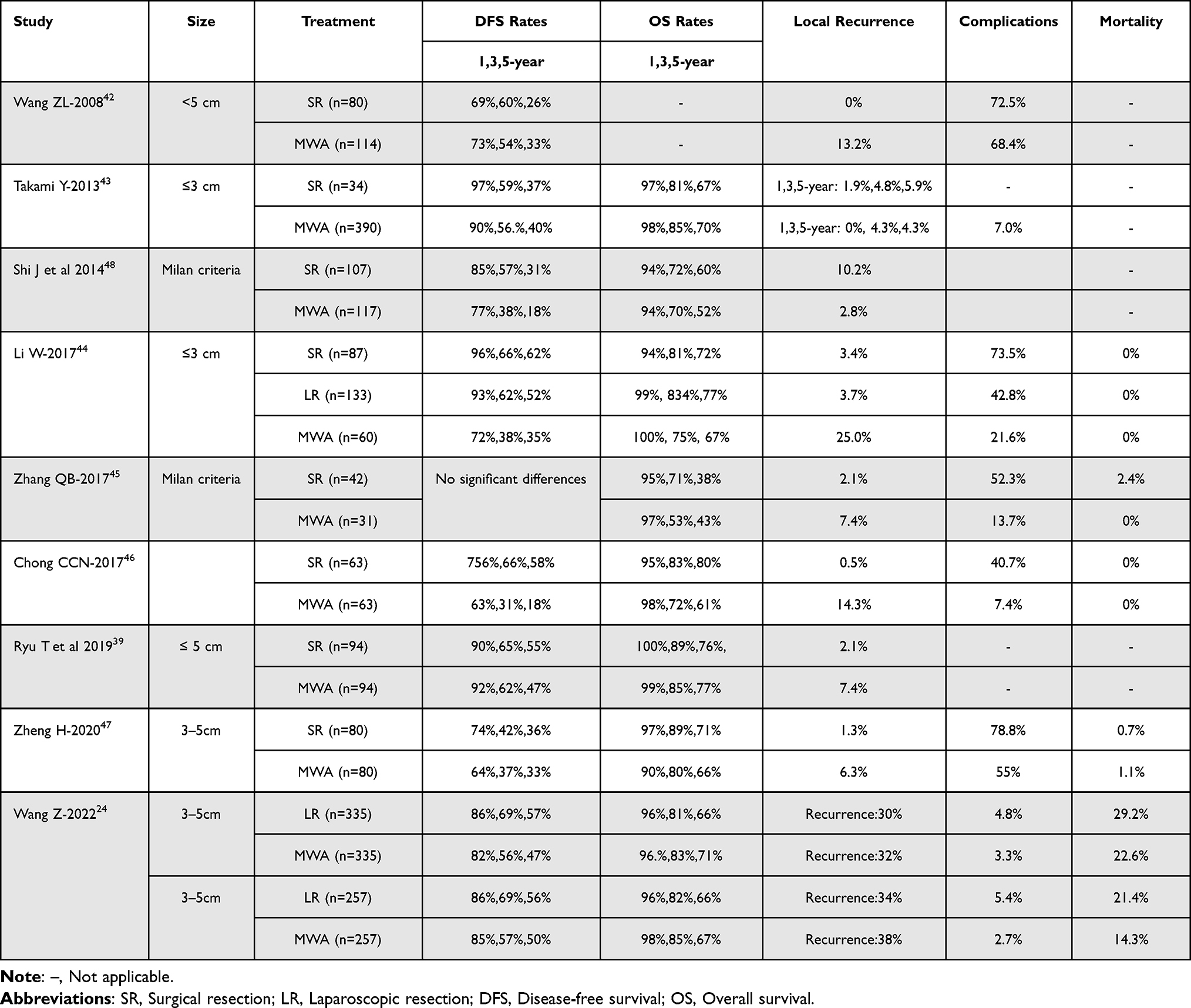 |
Table 2 Disease-Free Survival, Overall Survival, Local Recurrence, Complication Rates, and Mortality in Patients with HCC Treated with Microwave Ablation (vs. SR and LR) |
A research included a total of 26 studies with 4396 patients comparing the MWA group with the RFA group OS and DFS, and the results showed no statistical difference between the two groups.49 Spiliotis et al included 4 randomized trials and 11 observational studies with meta-analysis, and the overall analysis showed no significant difference in LTP between MWA and RFA.50 No significant differences were found between the two methods of ablation in IDR, complications, and tumor diameter less or larger than 3 cm37,51–61 (Table 3).
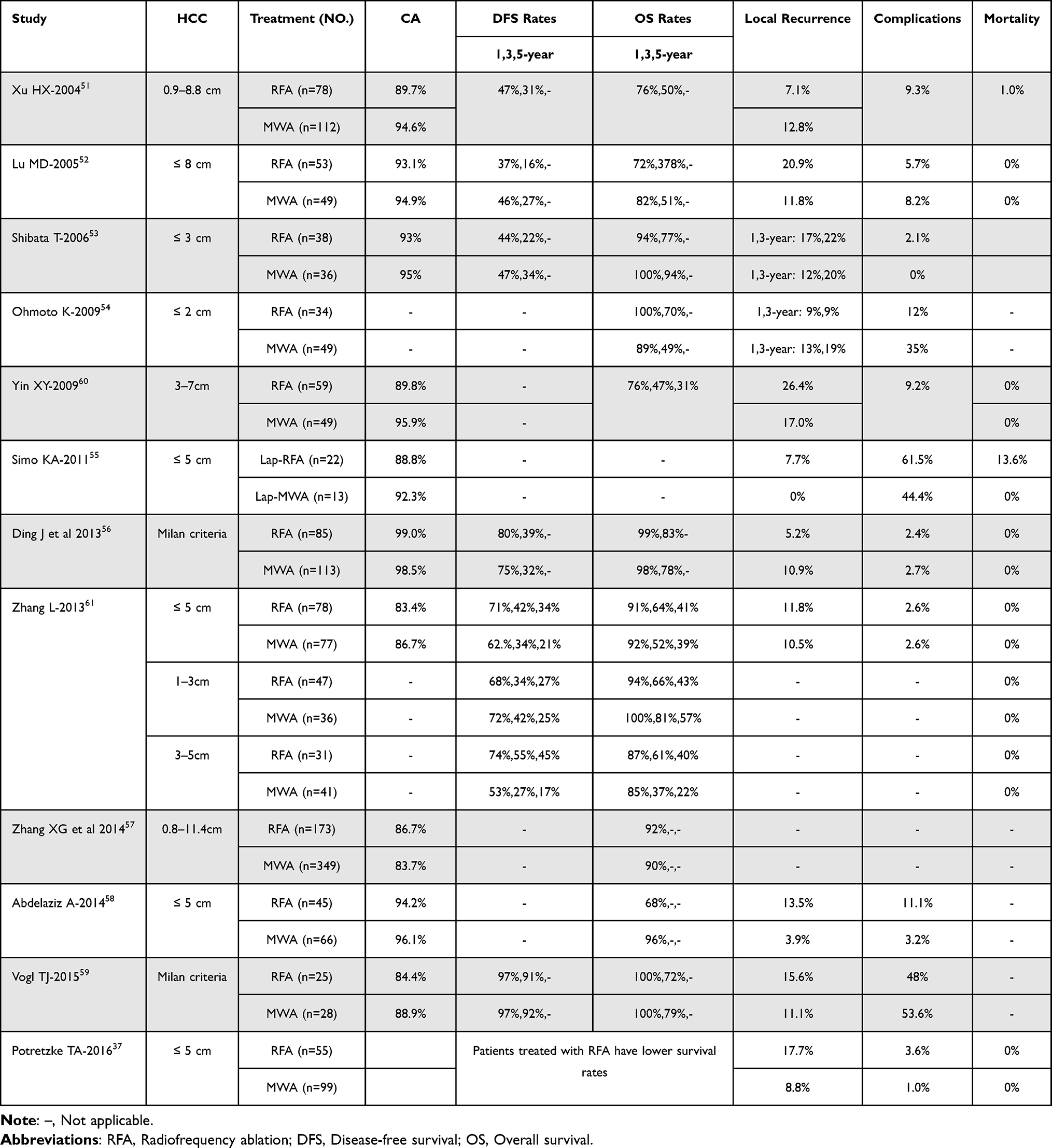 |
Table 3 Disease-Free Survival, Overall Survival, Local Recurrence, Complication Rates, and Mortality in Patients with HCC Treated with Microwave Ablation (vs. RFA) |
It has been reported in the literature that four different types of tumor progression (TP) occur after a period ablation.62,63 One of the most common is local tumor progression (LTP), which is defined as an abnormal imaging-enhanced nodule around the ablation site after MWA. The second is intrahepatic distant recurrence (IDR), which is described as abnormally enhanced nodules that appear further away from the ablation zone. In addition, there is aggressive intrasegmental recurrence (AIR), which is defined as the infiltrative recurrence of the treated liver segment with multiple abnormally enhancing nodules away from the edge of the ablation zone. The last one is extrahepatic distant recurrence (EDR), which is described as distant metastasis in the extrahepatic. Huang et al concluded that the occurrence rate of IDR was the highest and the occurrence rate of AIR was the lowest of all TPs following MWA of single HCC of ≤5 cm.62 Yoon et al showed that EDR occurred following multiple intrahepatic relapses after RFA, and the 10-year cumulative rates of HCC relapse and EDR were 92.7% and 33.7%, respectively.63 However, the incidence of these different TP after MWA is associated with multiple factors. Therefore, the study of risk factors in HCC patients treated by MWA provides a new reference for clinical management strategy prognosis.
Analysis of Influencing Factors
Treatment selection for HCC depends on tumor characteristics, BCLC stage, severity of liver dysfunction, age, other comorbidities, and available medical resources and local expertise,27 all of which have the potential to be independent risk factors for survival prognosis. Accumulated evidence demonstrates that various risk factors affecting LTP have been identified. Among them, tumor diameter, number, and degree of differentiation are well-known risk factors for recurrence after thermal ablation.64 In addition, recurrence and survival after MWA are also directly related to tumor location, pathological type, the underlying liver disease, and method used (percutaneous MWA, operative MWA)65 (Table 4).
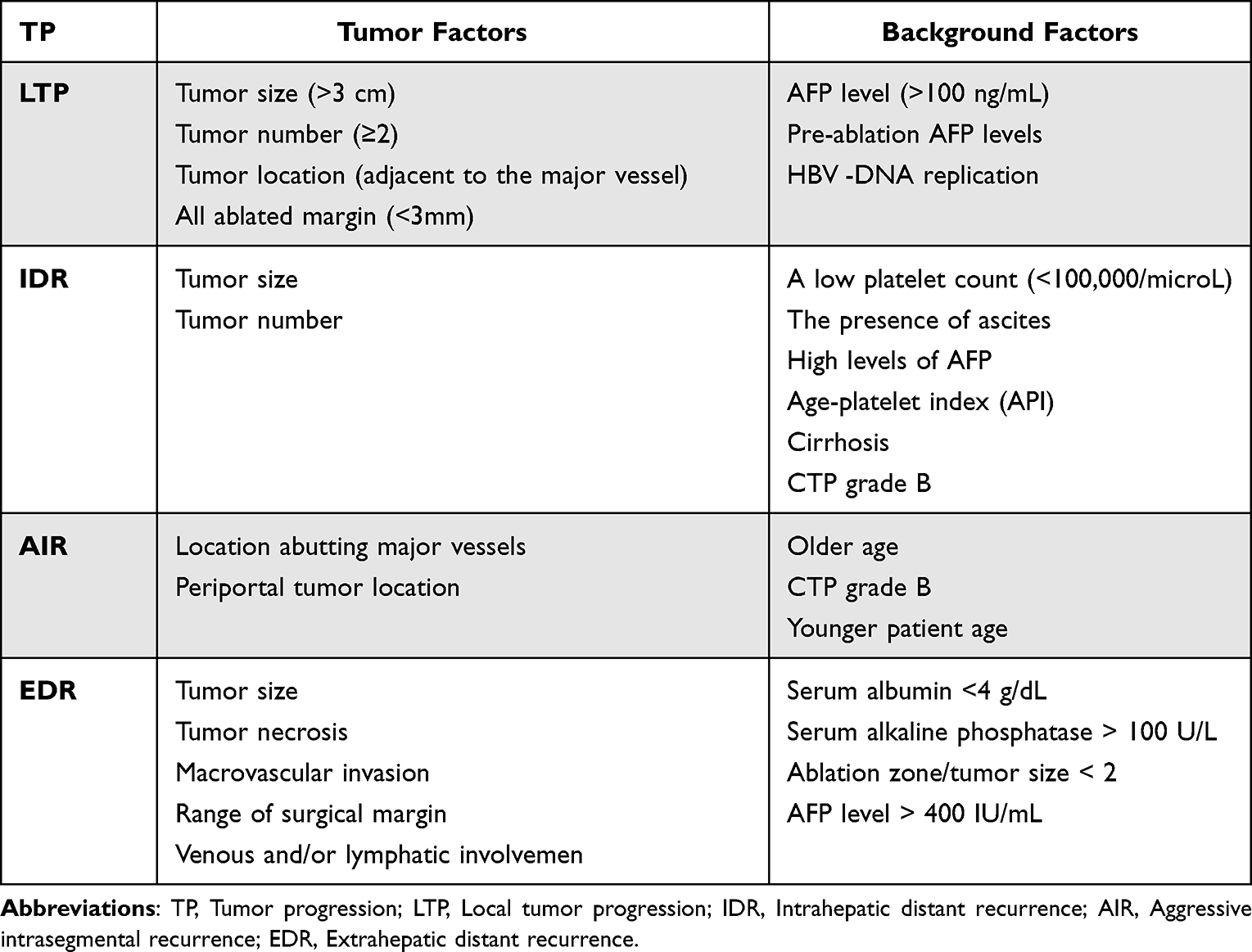 |
Table 4 The Factors of Influencing Tumor Progression |
Incidence and Risk Factors of LTP After Treatment
Research revealed that tumor size was a significant factor in terms of occurrence of LTP,62 and the degree of ablation margin is considered to be the most important factor in predicting LTP.66 Our team has previously confirmed HBV DNA replication, AFP level of pre-MWA (>200 ng/mL), tumor diameter (>30 mm), tumor location, and width of ablation zone were independent prognosis factors causing postoperative HCC recurrence,67 and Margaux also revealed that tumor size and ultrasound guidance independently predicted LTP, AFP (>100 ng/mL), and tumor size independently predicted IDR. DFS was independently predicted by multinodular HCC, treatment naivety, and AFP > 100 ng/mL.29
Zhang NN showed that a positive correlation existed between the number of lesions, proximity to the risk area, pre-ablation AFP levels, HBV-DNA replication and local recurrence, HBV-DNA, and proximity to the risk area as the independent prognosis factors causing postoperative HCC local recurrence.68
Incidence and Risk Factors of IDR After Treatment
While factors for local and distant recurrence were different, Yang69 revealed that 43.88% patients had IDR alone, male gender, multiple tumors, and cirrhosis were independent risk factors for late recurrence. A well-discriminated and calibrated nomogram was constructed to predict the probability of DFS. The predisposing factors for IDR and LTP of HCC differ and corresponding measures must be taken to prevent recurrence depending on the HCC status and background of liver disease.
Yang70 suggested that the independent risk factors for early recurrence were multiple tumors, AFP levels, gamma-glutamyl transferase (γ-GT), and serum albumin (ALB) levels. The incidence of IDR alone and IDR +EDR in early recurrence group was significantly higher than those in late recurrence group. Huang came to the conclusion that cirrhosis and CTP grade were significant factors in terms of occurrence of IDR, and cirrhosis and CTP grade B were independently associated with high occurrence rate of IDR.62
Incidence and Risk Factors of AIR After Treatment
Similar to the two TP above, CTP grade and location abutting major vessels were significant factors in terms of occurrence of AIR. Older age, CTP grade B, and location abutting major vessels were independently associated with high occurrence rate of AIR.62
A retrospective study71 of 539 patients concluded that the overall frequency of AIR after RFA for HCC was low, which was observed in 3.7% (20/539) of the patients, with the frequency increasing to 15% (11/72) in the subgroup of periportal HCC. AIRs could manifest as either multiple nodular type or diffusely infiltrative type with tumor thrombus formation. Periportal tumor location and younger patient age were significant risk factors for AIR. The occurrence of AIR had an adverse effect on OS rate. In contrast, AIR was rarely observed in Song’s study,72 the frequency of AIR was 1.4% (1/71) for all treated HCCs, and 4.5% (1/22) for the periportal HCCs. In view of these results, Song concluded that the combination of TACE and RFA can be considered as an effective strategy to reduce malignant segmental recurrence after treatment of HCC.
The tumor recurrence pattern after thermal ablation carries significant prognostic value in relation to OS. Long-term regular surveillance and aggressive treatment strategy are required for patients with different segment intrahepatic recurrence to optimize the benefits of ablation.
Incidence and Risk Factors of EDR After Treatment
It appears that proximity to major vessels is associated with a higher occurrence rate of EDR. A 15-year observational study73 analysed the factor of early extrahepatic recurrence for survival after HCC resection and concluded that serum ALB <4 g/dL, serum alkaline phosphatase >100 U/L, tumor diameter ≥7 cm, tumor necrosis, range of surgical margin, venous and/or lymphatic involvement, and macrovascular invasion were regarded as risk factors associated with early EDR. Early EHR was associated with substantially worse survival outcomes.
A retrospective study63 about the characteristics of extrahepatic metastases after RFA of HCC reported the 10-year cumulative rate of extrahepatic metastasis was 33.7%. Initial recurrence was most often intrahepatic after RFA, and the rate of EDR at initial recurrence was only 1.2%, and 68.2% of patients developed EDR within 2 years of the first recurrence. Regardless of DFS, 75.0% of patients developed EDR within 5 years after initial recurrence. Multivariate analysis showed DFS < 2 years, ablation zone/tumor size <2, and AFP level >400 IU/mL was associated with a high EDR risk.
Strategies for Challenges of Mwa
Fusion Navigation
With the development of imaging technology, image fusion can enable abdominal interventionalists to more accurately target challenging biopsy and ablation targets.74 Ultrasound contrast enhanced-guided or CT/MRI fusion guided ablation has achieved accurate localization and avoided bleeding and organ injury.75
Artificial Intelligence
Artificial intelligence (AI) is increasingly used in the field of surgery. AI is applied in the preoperative, intraoperative, postoperative, and long-term follow-up phases of surgical patient care in a safe and most cost-effective manner.76 Using machine learning models to analyze the predictors of outcome compared with the conventional multivariable logistic regression model, machine learning models showed better specificity, positive likelihood ratio, and positive predictive value, helping to identify high-risk patients more accurately and create opportunities for early in review and clinical intervention.
Preventive Treatment Strategy Prior to Progressivity of Recurrent HCC
BCLC staging has emerged as the standard classification system for the clinical management of HCC. However, the BCLC guidelines do not explicitly address early prevention strategies for recurrence or tumor progression. Thus, early detection and prevention of HCC development is, in principle, the most impactful strategy to improve patient prognosis.
This study77 proposes to evaluate the available clinical symptoms and laboratory variables to establish an HCC risk prediction score, however its performance is somewhat limited for HCC patients after local ablation. Cai78 suggested that personalized neoantigen vaccine is proved as a safe, feasible, and effective strategy for HCC anti-recurrence, and its progression could be sensitively monitored by corresponding neoantigen mutations in ctDNA, and thus provided solid information for individualized medicine in HCC, especially for HCC after radical surgery prophylaxis.
Schemmer P79 discussed the role of hepatitis B surface antigen for post-liver transplantation and resection, summarized that HBsAg has multiple implications for HCC development and postoperative recurrence, and speculated that HBsAg is key in the recurrence of HCC after LT, although its role in HCC recurrence post-resection is less clear. With the extensive application of HCC immunotherapy in clinic, combined immunotherapy with HBsAg-targeting hepatitis B immunoglobulin may have a potential role in the future management of liver transplantation or post-hepatectomy.
Zhou80 designed a multifunctional nanoparticle with a porous metal frame loaded with sorafenib, conjugated with HCC-specific targeting peptide and the near-infrared dye cyanine. The photothermal therapy and sorafenib therapy complement each other to reduce the side effects of sorafenib and achieve the therapeutic effect of non-local tumor recurrence. In addition, Catalase-like ability of NPs to relieve tumor hypoxia and its photothermal effects induce immunogenic cell death, resulting in the release of tumor-associated antigens. These actions together trigger an anti-tumor immune response; NPs also demonstrated a potential inhibitory effect on tumor metastasis and recurrence and produced abscopal effects and long-term immune memory when used in combination with anti-programmed death ligand 1 (PD-L1) immunotherapy.
Conclusions
In general, MWA is a first-line treatment for early liver cancer, and its advantages of safety and high efficiency have achieved satisfactory results. However, the clinical outcome, tumor progression, and recurrence of HCC after thermal ablation remain major concerns. Risk factors that influence clinical outcomes after ablation are currently the focus of research. Changes in treatment strategies and the development of assistive techniques are expected to reduce postoperative recurrence of MWA in the future, making it a clinically important treatment option. Future focus will be on using fusion navigation during local ablation therapy, the use of machine learning models before and after treatment to analyze outcome predictors, and finding strategies to prevent relapse after HCC treatment.
Abbreviations
2D US, Two-dimensional ultrasound; AFP, a-fetoprotein; AI, Artificial intelligence; AIR, Aggressive intrasegmental recurrence; API, Age-platelet index; BCLC, Barcelona clinic liver cancer; CA, Complete ablation; CT, Computed tomography; CEUS, Contrast-enhanced ultrasonography; CTP, Child–Turcotte–Pugh; DFS, Disease-free survival; ECOG, Eastern Cooperative Oncology Group; EDR, Extrahepatic distant recurrence; HBV, Hepatitis B virus; HCC, Hepatocellular carcinoma; HCV, Hepatitis C virus; IDR, Intrahepatic distant recurrence; IRE, Irreversible electroporation; LR, Laparoscopic resection; LRT, Locoregional therapy; LT, Liver transplantation; LTP, Local tumor progression; MRI, Magnetic resonance imaging; MWA, Microwave ablation; OLT, Orthotopic liver transplantation; OS, Overall survival; PLA, Percutaneous local ablation; PMWA, Percutaneous microwave ablation; RCT, Randomized controlled trial; RFA, Radiofrequency ablation; SMWA, Stereotactic image-guided microwave ablation; SR, Surgical resection; TACE, Transarterial chemoembolization; TP, Tumor progression; US, Ultrasonography.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Key Research and Development Project of Gansu Province, China [grant number 21YF5FA122]; The Youth Science and Technology Fund program of Gansu Province, China [grant numbers 22JR11RA074].
Disclosure
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391(10127):1301–1314. doi:10.1016/S0140-6736(18)30010-2
3. Sugawara Y, Inomata Y. Indications for living donor liver transplantation in patients with hepatocellular carcinoma. Hepatobiliary Surg Nutr. 2016;5(5):429–432. doi:10.21037/hbsn.2016.09.01
4. Simmerman E, Chung J, Lawson A, et al. Application of irreversible electroporation ablation as adjunctive treatment for margin enhancement: safety and efficacy. J Surg Res. 2020;246:260–268. doi:10.1016/j.jss.2019.06.010
5. Vitale A, Peck-Radosavljevic M, Giannini EG, et al. Personalized treatment of patients with very early hepatocellular carcinoma. J Hepatol. 2017;66(2):412–423. doi:10.1016/j.jhep.2016.09.012
6. Galle PR, Forner A, Llovet JM, et al. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236.
7. Raoul JL, Schirmacher P, Vilgrain V. Corrigendum to “EASL clinical practice guidelines: management of hepatocellular carcinoma” [J Hepatol 69 (2018) 182–236]. J Hepatol. 2019;70(4):817.
8. Habibollahi P, Sheth RA, Cressman ENK. Histological correlation for radiofrequency and microwave ablation in the local control of hepatocellular carcinoma (HCC) before liver transplantation: a comprehensive review. Cancers. 2020;13(1):104. doi:10.3390/cancers13010104
9. Bae SH, Park HC. Local modalities for inoperable hepatocellular carcinoma: radiofrequency ablation versus stereotactic body radiotherapy. Ann Transl Med. 2018;6(Suppl 1):S3. doi:10.21037/atm.2018.08.28
10. Donaldson K, Buchanich JM, Grigson PS. Abstracts of presentations at the association of clinical scientists 143rd meeting Louisville, KY May 11–14, 2022. Ann Clin Lab Sci. 2022;52(3):511–525.
11. Xu C, Li L, Xu W, et al. Ultrasound-guided percutaneous microwave ablation versus surgical resection for recurrent intrahepatic cholangiocarcinoma: intermediate-term results. Int J Hyperthermia. 2019;36(1):351–358. doi:10.1080/02656736.2019.1571247
12. Domini J, Makary MS. Single-center analysis of percutaneous ablation in the treatment of hepatocellular carcinoma: long-term outcomes of a 7-year experience. Abdom Radiol. 2023;48(3):1173–1180. doi:10.1007/s00261-023-03819-y
13. Majumdar A, Roccarina D, Thorburn D, et al. Management of people with early- or very early-stage hepatocellular carcinoma: an attempted network meta-analysis. Cochrane Database Syst Rev. 2017;3(3):CD011650. doi:10.1002/14651858.CD011650.pub2
14. Petre EN, Sofocleous C. Thermal ablation in the management of colorectal cancer patients with oligometastatic liver disease. Visc Med. 2017;33(1):62–68. doi:10.1159/000454697
15. Lee S, Kang TW, Song KD, et al. Effect of microvascular invasion risk on early recurrence of hepatocellular carcinoma after surgery and radiofrequency ablation. Ann Surg. 2021;273(3):564–571. doi:10.1097/SLA.0000000000003268
16. Shindoh J. Stratification of risk of recurrence after curative-intent treatment for small hepatocellular carcinoma. Hepatobiliary Surg Nutr. 2019;8(6):649–650. doi:10.21037/hbsn.2019.07.17
17. Yang Y, Chen W, Mai W, et al. HIF-2α regulates proliferation, invasion, and metastasis of hepatocellular carcinoma cells via VEGF/Notch1 signaling axis after insufficient radiofrequency ablation. Front Oncol. 2022;12:998295. doi:10.3389/fonc.2022.998295
18. Xiao C, Liu S, Ge G, et al. Roles of hypoxia-inducible factor in hepatocellular carcinoma under local ablation therapies. Front Pharmacol. 2023;14:1086813. doi:10.3389/fphar.2023.1086813
19. Pausch A-M, Ghali T, Wertheimer T, et al. Stereotactic microwave ablation of hepatocellular carcinoma: the impact of tumor size and minimal ablative margin on therapeutic success. Tomography. 2022;9(1):50–59. doi:10.3390/tomography9010005
20. Izzo F, Granata V, Grassi R, et al. Radiofrequency ablation and microwave ablation in liver tumors: an update. Oncologist. 2019;24(10):e990–e1005. doi:10.1634/theoncologist.2018-0337
21. Evans AL, Ma C, Hagness SC. Microwave-induced thermoacoustic signal characteristics in a dynamic temperature environment. Biomed Phys Eng Express. 2022;8(3):035020. doi:10.1088/2057-1976/ac60c6
22. Vietti Violi N, Duran R, Guiu B, et al. Efficacy of microwave ablation versus radiofrequency ablation for the treatment of hepatocellular carcinoma in patients with chronic liver disease: a randomised controlled Phase 2 trial. Lancet Gastroenterol Hepatol. 2018;3(5):317–325. doi:10.1016/S2468-1253(18)30029-3
23. Vogl TJ, Nour-Eldin N-EA, Hammerstingl RM, et al. Microwave ablation (MWA): basics, technique and results in primary and metastatic liver neoplasms - review article. RoFo. 2017;189(11):1055–1066. doi:10.1055/s-0043-117410
24. Wang Z, Liu M, Zhang D-Z, et al. Microwave ablation versus laparoscopic resection as first-line therapy for solitary 3–5-cm HCC. Hepatology. 2022;76(1):66–77. doi:10.1002/hep.32323
25. Makovich Z, Logemann J, Chen L, et al. Liver tumor ablation in difficult locations: microwave ablation of perivascular and subdiaphragmatic hepatocellular carcinoma. Clin Imaging. 2021;71:170–177. doi:10.1016/j.clinimag.2020.11.010
26. An C, Li X, Zhang M, et al. 3D visualization ablation planning system assisted microwave ablation for hepatocellular carcinoma (Diameter >3): a precise clinical application. BMC Cancer. 2020;20(1):44. doi:10.1186/s12885-020-6519-y
27. Yang JD, Hainaut P, Gores GJ, et al. A global view of hepatocellular carcinoma: trends, risk, prevention and management. Nat Rev Gastroenterol Hepatol. 2019;16(10):589–604. doi:10.1038/s41575-019-0186-y
28. Couri T, Pillai A. Goals and targets for personalized therapy for HCC. Hepatol Int. 2019;13(2):125–137. doi:10.1007/s12072-018-9919-1
29. Hermida M, Cassinotto C, Piron L, et al. Multimodal percutaneous thermal ablation of small hepatocellular carcinoma: predictive factors of recurrence and survival in western patients. Cancers. 2020;12(2):1.
30. Swan RZ, Sindram D, Martinie JB, et al. Operative microwave ablation for hepatocellular carcinoma: complications, recurrence, and long-term outcomes. J Gastrointest Surg. 2013;17(4):719–729. doi:10.1007/s11605-013-2164-y
31. Sun A-X, Cheng Z-L, Wu -P-P, et al. Clinical outcome of medium-sized hepatocellular carcinoma treated with microwave ablation. World J Gastroenterol. 2015;21(10):2997–3004. doi:10.3748/wjg.v21.i10.2997
32. Zhang -T-T, Luo H-C, Cui X, et al. Ultrasound-guided percutaneous microwave ablation treatment of initial recurrent hepatocellular carcinoma after hepatic resection: long-term outcomes. Ultrasound Med Biol. 2015;41(9):2391–2399. doi:10.1016/j.ultrasmedbio.2015.04.019
33. Baker EH, Thompson K, McKillop IH, et al. Operative microwave ablation for hepatocellular carcinoma: a single center retrospective review of 219 patients. J Gastrointest Oncol. 2017;8(2):337–346. doi:10.21037/jgo.2016.09.06
34. Yin T, Li W, Zhao P, et al. Treatment efficacy of CT-guided percutaneous microwave ablation for primary hepatocellular carcinoma. Clin Radiol. 2017;72(2):136–140. doi:10.1016/j.crad.2016.10.022
35. Ma S, Ding M, Li J, et al. Ultrasound-guided percutaneous microwave ablation for hepatocellular carcinoma: clinical outcomes and prognostic factors. J Cancer Res Clin Oncol. 2017;143(1):131–142. doi:10.1007/s00432-016-2266-5
36. Jin T, Liu X, Zhang H, et al. Ultrasound-guided percutaneous microwave ablation for hepatocellular carcinoma adjacent to large vessels: a propensity score matching analysis. Int J Hyperthermia. 2020;37(1):955–964. doi:10.1080/02656736.2020.1804076
37. Potretzke TA, Ziemlewicz TJ, Hinshaw JL, et al. Microwave versus radiofrequency ablation treatment for hepatocellular carcinoma: a comparison of efficacy at a single center. J Vasc Interv Radiol. 2016;27(5):631–638. doi:10.1016/j.jvir.2016.01.136
38. Feng H, Yang C, Xu F, et al. Therapeutic efficacy of microwave coagulation versus liver resection for hepatocellular carcinoma within the Milan criteria: a propensity score matching analysis. Eur J Surg Oncol. 2022;48(2):418–424. doi:10.1016/j.ejso.2021.08.035
39. Ryu T, Takami Y, Wada Y, et al. Hepatic resection versus operative microwave ablation for single hepatocellular carcinoma ≤5 cm: a propensity score-matched analysis. Surgery. 2019;166(3):254–262. doi:10.1016/j.surg.2019.05.007
40. Zhang M, Ma H, Zhang J, et al. Comparison of microwave ablation and hepatic resection for hepatocellular carcinoma: a meta-analysis. Onco Targets Ther. 2017;10:4829–4839. doi:10.2147/OTT.S141968
41. Glassberg MB, Ghosh S, Clymer JW, et al. Microwave ablation compared with hepatic resection for the treatment of hepatocellular carcinoma and liver metastases: a systematic review and meta-analysis. World J Surg Oncol. 2019;17(1):98. doi:10.1186/s12957-019-1632-6
42. Wang ZL, Liang P, Dong BW, et al. Prognostic factors and recurrence of small hepatocellular carcinoma after hepatic resection or microwave ablation: a retrospective study. J Gastrointest Surg. 2008;12(2):327–337. doi:10.1007/s11605-007-0310-0
43. Takami Y, Ryu T, Wada Y, et al. Evaluation of intraoperative microwave coagulo-necrotic therapy (MCN) for hepatocellular carcinoma: a single center experience of 719 consecutive cases. J Hepatobiliary Pancreat Sci. 2013;20(3):332–341. doi:10.1007/s00534-012-0527-5
44. Li W, Zhou X, Huang Z, et al. Short-term and long-term outcomes of laparoscopic hepatectomy, microwave ablation, and open hepatectomy for small hepatocellular carcinoma: a 5-year experience in a single center. Hepatol Res. 2017;47(7):650–657. doi:10.1111/hepr.12785
45. Zhang Q-B, Zhang X-G, Jiang R-D, et al. Microwave ablation versus hepatic resection for the treatment of hepatocellular carcinoma and oesophageal variceal bleeding in cirrhotic patients. Int J Hyperthermia. 2017;33(3):255–262. doi:10.1080/02656736.2016.1257824
46. Chong CCN, Lee K-F, Chu C-M, et al. Microwave ablation provides better survival than liver resection for hepatocellular carcinoma in patients with borderline liver function: application of ALBI score to patient selection. HPB. 2018;20(6):546–554. doi:10.1016/j.hpb.2017.12.001
47. Zheng H, Xu C, Wang X, et al. Microwave ablation shows similar survival outcomes compared with surgical resection for hepatocellular carcinoma between 3 and 5 cm. Int J Hyperthermia. 2020;37(1):1345–1353. doi:10.1080/02656736.2020.1849825
48. Shi J, Sun Q, Wang Y, et al. Comparison of microwave ablation and surgical resection for treatment of hepatocellular carcinomas conforming to Milan criteria. J Gastroenterol Hepatol. 2014;29(7):1500–1507. doi:10.1111/jgh.12572
49. Han J, Fan Y-C WK, Wang K. Radiofrequency ablation versus microwave ablation for early stage hepatocellular carcinoma: a PRISMA-compliant systematic review and meta-analysis. Medicine. 2020;99(43):e22703. doi:10.1097/MD.0000000000022703
50. Spiliotis AE, Gäbelein G, Holländer S, et al. Microwave ablation compared with radiofrequency ablation for the treatment of liver cancer: a systematic review and meta-analysis. Radiol Oncol. 2021;55(3):247–258. doi:10.2478/raon-2021-0030
51. Xu HX, Xie XY, Lu MD, et al. Ultrasound-guided percutaneous thermal ablation of hepatocellular carcinoma using microwave and radiofrequency ablation. Clin Radiol. 2004;59(1):53–61. doi:10.1016/j.crad.2003.09.006
52. Lu M-D, Xu H-X, Xie X-Y, et al. Percutaneous microwave and radiofrequency ablation for hepatocellular carcinoma: a retrospective comparative study. J Gastroenterol. 2005;40(11):1054–1060. doi:10.1007/s00535-005-1671-3
53. Shibata T, Shibata T, Maetani Y, et al. Radiofrequency ablation for small hepatocellular carcinoma: prospective comparison of internally cooled electrode and expandable electrode. Radiology. 2006;238(1):346–353. doi:10.1148/radiol.2381041848
54. Ohmoto K, Yoshioka N, Tomiyama Y, et al. Comparison of therapeutic effects between radiofrequency ablation and percutaneous microwave coagulation therapy for small hepatocellular carcinomas. J Gastroenterol Hepatol. 2009;24(2):223–227. doi:10.1111/j.1440-1746.2008.05596.x
55. Simo KA, Sereika SE, Newton KN, et al. Laparoscopic-assisted microwave ablation for hepatocellular carcinoma: safety and efficacy in comparison with radiofrequency ablation. J Surg Oncol. 2011;104(7):822–829. doi:10.1002/jso.21933
56. Ding J, Jing X, Liu J, et al. Comparison of two different thermal techniques for the treatment of hepatocellular carcinoma. Eur J Radiol. 2013;82(9):1379–1384. doi:10.1016/j.ejrad.2013.04.025
57. Zhang XG, Zhang ZL, Hu SY, et al. Ultrasound-guided ablative therapy for hepatic malignancies: a comparison of the therapeutic effects of microwave and radiofrequency ablation. Acta Chir Belg. 2014;114(1):40–45. doi:10.1080/00015458.2014.11680975
58. Abdelaziz A, Elbaz T, Shousha HI, et al. Efficacy and survival analysis of percutaneous radiofrequency versus microwave ablation for hepatocellular carcinoma: an Egyptian multidisciplinary clinic experience. Surg Endosc. 2014;28(12):3429–3434. doi:10.1007/s00464-014-3617-4
59. Vogl TJ, Farshid P, Naguib NNN, et al. Ablation therapy of hepatocellular carcinoma: a comparative study between radiofrequency and microwave ablation. Abdom Imaging. 2015;40(6):1829–1837. doi:10.1007/s00261-015-0355-6
60. Yin X-Y, Xie X-Y, Lu M-D, et al. Percutaneous thermal ablation of medium and large hepatocellular carcinoma: long-term outcome and prognostic factors. Cancer. 2009;115(9):1914–1923. doi:10.1002/cncr.24196
61. Zhang L, Wang N, Shen Q, et al. Therapeutic efficacy of percutaneous radiofrequency ablation versus microwave ablation for hepatocellular carcinoma. PLoS One. 2013;8(10):e76119. doi:10.1371/journal.pone.0076119
62. Huang Z, Guo Z, Ni J, et al. Four types of tumor progression after microwave ablation of single hepatocellular carcinoma of ≤5 cm: incidence, risk factors and clinical significance. Int J Hyperthermia. 2021;38(1):1164–1173. doi:10.1080/02656736.2021.1962548
63. Yoon JH, Goo YJ, Lim C-J, et al. Features of extrahepatic metastasis after radiofrequency ablation for hepatocellular carcinoma. World J Gastroenterol. 2020;26(32):4833–4845. doi:10.3748/wjg.v26.i32.4833
64. Lee SK, Lee SW, Jang JW, et al. Immunological markers, prognostic factors and challenges following curative treatments for hepatocellular carcinoma. Int J Mol Sci. 2021;22(19):1.
65. Yu J, Cheng Z-G, Han Z-Y, et al. Period-dependent survival benefit of percutaneous microwave ablation for hepatocellular carcinoma: a 12-year real-world, multicentric experience. Liver Cancer. 2022;11(4):341–353. doi:10.1159/000522134
66. Zhang Z, Yu J, Liu S, et al. Multiparametric liver MRI for predicting early recurrence of hepatocellular carcinoma after microwave ablation. Cancer Imaging. 2022;22(1):42. doi:10.1186/s40644-022-00471-5
67. Dong T, Nie F, Liu T, et al. Different power modes microwave ablation of hepatocellular carcinoma: evaluation of recurrence rate and factors related to recurrence. Asian J Surg. 2023. doi:10.1016/j.asjsur.2023.03.070
68. Zhang NN, Lu W, Cheng XJ, et al. High-powered microwave ablation of larger hepatocellular carcinoma: evaluation of recurrence rate and factors related to recurrence. Clin Radiol. 2015;70(11):1237–1243. doi:10.1016/j.crad.2015.06.092
69. Yang Y, Chen Y, Ye F, et al. Late recurrence of hepatocellular carcinoma after radiofrequency ablation: a multicenter study of risk factors, patterns, and survival. Eur Radiol. 2021;31(5):3053–3064. doi:10.1007/s00330-020-07460-x
70. Yang Y, Xin Y, Ye F, et al. Early recurrence after radiofrequency ablation for hepatocellular carcinoma: a multicenter retrospective study on definition, patterns and risk factors. Int J Hyperthermia. 2021;38(1):437–446. doi:10.1080/02656736.2020.1849828
71. Kang TW, Lim HK, Lee MW, et al. Aggressive intrasegmental recurrence of hepatocellular carcinoma after radiofrequency ablation: risk factors and clinical significance. Radiology. 2015;276(1):274–285. doi:10.1148/radiol.15141215
72. Song KD, Lee MW, Rhim H, et al. Aggressive intrasegmental recurrence of hepatocellular carcinoma after combined transarterial chemoembolization and radiofrequency ablation. Am J Roentgenol. 2016;207(5):1122–1127. doi:10.2214/AJR.16.16080
73. Yoon JH, Choi SK, Cho SB, et al. Early extrahepatic recurrence as a pivotal factor for survival after hepatocellular carcinoma resection: a 15-year observational study. World J Gastroenterol. 2022;28(36):5351–5363. doi:10.3748/wjg.v28.i36.5351
74. You Y, Zhang M, Li K, et al. Feasibility of 3D US/CEUS-US/CEUS fusion imaging-based ablation planning in liver tumors: a retrospective study. Abdom Radiol. 2021;46(6):2865–2874. doi:10.1007/s00261-020-02909-5
75. Floridi C, Radaelli A, Pesapane F, et al. Clinical impact of cone beam computed tomography on iterative treatment planning during ultrasound-guided percutaneous ablation of liver malignancies. Med Oncol. 2017;34(6):113. doi:10.1007/s12032-017-0954-x
76. Taher H, Grasso V, Tawfik S, et al. The challenges of deep learning in artificial intelligence and autonomous actions in surgery: a literature review. Artif Intell Surg. 2022;2(3):144–158. doi:10.20517/ais.2022.11
77. Fujiwara N, Friedman SL, Goossens N, et al. Risk factors and prevention of hepatocellular carcinoma in the era of precision medicine. J Hepatol. 2018;68(3):526–549. doi:10.1016/j.jhep.2017.09.016
78. Cai Z, Su X, Qiu L, et al. Personalized neoantigen vaccine prevents postoperative recurrence in hepatocellular carcinoma patients with vascular invasion. Mol Cancer. 2021;20(1):164. doi:10.1186/s12943-021-01467-8
79. Schemmer P, Burra P, Hu R-H, et al. State of the art treatment of hepatitis B virus hepatocellular carcinoma and the role of hepatitis B surface antigen post-liver transplantation and resection. Liver Int. 2022;42(2):288–298. doi:10.1111/liv.15124
80. Zhou T, Liang X, Wang P, et al. A hepatocellular carcinoma targeting nanostrategy with hypoxia-ameliorating and photothermal abilities that, combined with immunotherapy, inhibits metastasis and recurrence. ACS Nano. 2020;14(10):12679–12696. doi:10.1021/acsnano.0c01453
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.